
Abstract
Nursing care work in Germany has been facing significant challenges, among them a steadily increasing shortage of nursing care workers. Funding programs promote the use of care robotics to mitigate these challenges’ negative effects and to support nursing care practice. However, most robotics research on the topic has so far followed a technology-centered approach that hardly considers nursing care experts’ distinct experiences, knowledge, or expertise. Drawing on interviews, focus groups, and workshops with nursing scientists, students, and practitioners, this study investigates the perspectives, evaluations, and imaginaries of German nursing care experts regarding care robotics. In their accounts, we found three salient themes that highlight care robotics as an open-ended, empirical concern for the nursing sciences; as a means for delineating between automatable and non-automatable nursing care activities; and as a potential remedy for nurses’ assistive and executive responsibilities. Each of these themes highlights a particular set of challenges that nursing care work currently faces in the context of German healthcare from the nursing care experts’ perspective and that shapes their perspectives on care robotics. We discuss the nursing care experts’ responses as a reference point to re-articulate deep-seated disciplinary and professional concerns along three distinct dimensions: a nursing-as-science, nursing-as-practice, and nursing-as-profession dimension. We further conceptualize these dimensions as matters of care that care robotics research should engage with to generate care for nursing care work and workers. We conclude by suggesting ways for incorporating these dimensions into care robotics research and development.
Introduction
The German healthcare system struggles with a set of challenges that question its long-term sustainability in the face of demographic change and a growing shortage of healthcare workers (Hinrichs, 2010; Neumann and Spöthe, 2015). In an attempt to address these challenges, the German government—similar to other European countries—has promoted the use of technology to support healthcare workers. These efforts have especially focused on professional nursing care workers, who make up the largest segment of Germany’s healthcare workforce and play a pivotal role in providing healthcare services to older adults (Böhm, 2021; Bundesministerium für Gesundheit, 2022; Hofmann, 2012).
As a result, healthcare and nursing-care-related research agendas have experienced a “technology-push” (Hülsken-Giesler and Daxberger, 2018; Krings et al., 2012) that substantially increased the number of funding programs that support the development of robots and other interactive or assistive technologies (Maibaum et al., 2022). This has made care robotics a rapidly expanding field of research (Bendel, 2018; Lipp, 2020), fueling policy-makers’ hopes that robots can become a tool for improving the working conditions of nursing care workers and the quality of care processes (Breuer and Müller, 2024). The resulting research and development efforts, however, often reflect a narrow set of engineering values and priorities, leaving open critical social science questions about how such technologies are designed, whose values they reflect, and how they reshape the work and responsibilities of nursing care workers in practice.
Addressing these gaps, this study explores how nursing care experts—including nursing care practitioners, scientists, and students—engage with and reflect on ongoing care robotics research. Drawing on interviews, focus groups, and workshops with German nursing care experts, we examine how they perceive and evaluate concrete examples of care robotics research and how they imagine possible futures with such technologies.
Specifically, we engaged participants with prototypes and scenarios drawn from a care robotics research project with which we have been closely collaborating. We invited them to reflect on these prototypes and scenarios, with a particular focus on whether and how they could imagine the integration of robotic technologies into their everyday nursing care work: Under what conditions does the use of robotics become meaningful or problematic? What roles might robotics play? How might nursing care practitioners’ own practices and responsibilities be affected? And what role do nursing care experts believe they should play in shaping the research, development, and implementation of such technologies?
We situate the nursing care experts’ perspectives, evaluations, and imaginaries within the broader social and political context of nursing care work in Germany—particularly its historical struggles for professional recognition, academic institutionalization, and equitable inclusion in healthcare decision-making. In this way, our study critically examines how care robotics research intersects with the professional, political, and historical conditions, and contributes a social science perspective that centers nursing care experts as key actors for future care robotics research.
Background
Nursing in Germany
Our research situates the nursing care experts’ perspectives, evaluations, and imaginaries regarding care robotics within the particular context of the German healthcare system, which has been marked by an ongoing transformation of nursing care work since the 1800s. Key aspects of this transformation include (1) an ongoing professionalization through political and regulatory reforms, (2) continued efforts to disentangle itself from its role as an assistive service to other healthcare professions (especially medicine), and (3) a relatively late academization of the nursing sciences at German universities compared to other countries. These interrelated developments formed an important backdrop to all conversations we had with nursing care experts on care robotics and significantly shaped how they perceived, evaluated, and imagined the role of care robotics in their field. 1
From a historical perspective, the current state of nursing care in Germany is caught in a structural conflict that emerged in the late 19th century and has persisted to the present day. In this conflict, two perspectives on care collide: The first views nursing care as a welfare-state service governed primarily by economic and administrative logics of cost efficiency. The second understands nursing care work as an increasingly institutionalized and professionalized domain, characterized by trained professionals who develop their own professional and ethical standards (Hergesell, 2018; Maibaum et al., 2022).
The professionalization of nursing in Germany is embedded in this structural conflict and began as care work started to transition from a family and partially clerical concern into the labor market it is today, where public, clerical, and private care suppliers offer professional nursing care services that are primarily funded by the German welfare state (Hofmann, 2012; Neumann and Spöthe, 2015). It was, however, not until the 1950s that nursing started to institutionalize itself as an independent healthcare profession by establishing training and education systems for nursing care workers independent of hospitals and the church (Theobald and Luppi, 2018). Since then, repeated regulatory reforms have responded to demographic change and increasing care needs.
The most recent reform, the Pflegeberufegesetz (2020), recognizes nursing as an academic healthcare profession and positions academic nursing training on equal footing with vocational training when it comes to the professional qualification for nursing positions (di Luzio, 2009; Wecht, 2020). At the same time, the expansion of dual academic-vocational nursing programs has further advanced the profession’s academic institutionalization, bringing “evidence-based” (Ingersoll, 2000) and “patient-centered” (Lusk and Fater, 2013) approaches to nursing practice. These reflect the profession’s expanded responsibilities and competencies, as introduced by recent political reforms, and challenge the “traditional model” of nursing as a profession subordinate to medicine (di Luzio, 2009).
It will take time until we know whether and how the effects of these developments will fully unfold in nursing care practice, and in the meantime, working conditions are expected to remain challenging (Schmucker, 2020). This has prompted political and research interest in technological solutions such as care robotics, which, however, now must contend with the dynamic and contested situation of German nursing care work highlighted above. This includes the ongoing tension between ensuring the financial viability of nursing care on the one side and delivering high-quality care in line with current professional standards on the other (Hergesell, 2018).
Drawing from the field of Science and Technology Studies (STS), our study investigates how nursing care experts’ perceptions, evaluations, and imaginaries are linked to the historical, social, and political developments around nursing care in Germany and how they envision care robotics within nursing care’s evolving professional landscape.
STS perspectives on nursing and care robotics
STS research demonstrates that the adoption of technology in nursing care practice is shaped by its social and political context (Lindén and Lydahl, 2021). Studies have shown how power hierarchies, economic pressures, and institutional norms influence how technologies are implemented and interpreted in practice. For example, the introduction of a wireless nursing call system in a Canadian hospital was shaped by cost-saving imperatives and hierarchical divisions of responsibility (Bruun Jensen, 2007). A Danish study on an electronic medication system revealed how implementation processes reproduced existing expectations that doctors instruct nurses rather than the other way around (Markussen and Olesen, 2007).
Studies like these show that the introduction of novel technologies to digitize or automate certain aspects of nursing care work is rarely a neutral or purely technical act. Such interventions inevitably interfere with existing social and organizational structures and potentially challenge or reaffirm prevailing assumptions, ideas, expectations, and power dynamics in nursing care work environments. This raises questions about whether the current political efforts to integrate care robotics into nursing care practice will yield the anticipated benefits. In this regard, STS research has highlighted the important role that nursing care workers play in making robots operational in complex social environments, such as healthcare (Chang and Šabanović, 2015; Chevallier, 2023).
However, the literature also highlights that robotics research has often had “barely any or no interaction” with experts from nursing care (Nieto Agraz et al., 2022: 13). In those studies that do engage nursing care workers, the focus tends to remain on the technology itself and its perceived usefulness or acceptance rather than foregrounding the experiences, knowledge, and expertise of the nursing care workers involved (Kang et al., 2023; Parviainen et al., 2019; Saadatzi et al., 2020). A scoping review from 2018 identifies 19 such studies on socially assistive humanoid or animal-like robotics (Papadopoulos et al., 2018). While the review yields some overarching insights—such as a generally more positive than negative attitude among care workers toward robotics—it also emphasizes that the studies usually conflate nursing care workers with other health or social care workers. This points us to a persistent gap in care robotics research: the insufficient attention to the context of use and the perspectives of those affected by these technologies. Care robotics research has often tended to approach nursing care as “an object of robotic engineering” (Bischof and Graf, 2022), rather than consistently mobilizing robotics as a resource for addressing the needs, concerns, and epistemic agendas of nursing care itself.
Researchers from STS have begun to address this imbalance by more directly engaging nursing care workers’ perspectives. A notable example is the work by Nettleton et al. (2025) that involved practicing nurses in an on-site trial of a teleoperated care robot in a Finnish hospital. Their analysis sheds light on nurses’ expectations and imaginaries of care robotics and highlights how these expectations and imaginaries change once nurses interact with the technologies. Crucially, their analysis moves beyond merely assessing or evaluating the success of a particular care robotics system and instead raises more fundamental questions about how the introduction of robots in nursing care settings might reconfigure existing schedules, roles, hierarchies, relationships, and practices from the perspective of nurses and other affected stakeholders in the hospital.
Our study follows these lines of inquiry, addresses the aforementioned gap by focusing on the perspective of nursing care experts, and asks the following research questions: How do nursing care experts perceive and evaluate care robotics based on their particular experiences, knowledge, and expertise? And how do their perspectives, evaluations, and imaginaries 2 relate to the wider social and political context of nursing care work in Germany?
Study design and methods
This study was conducted within the context of an interdisciplinary research project titled Responsible Robotics (RR-AI), which focused on the research and application of robotics in healthcare settings. Our interdisciplinary project team brought together expertise from STS, ethics, law, and engineering and adopted an “Embedded Ethics and Social Science” (Breuer et al., 2024) approach that aims at including “the consideration of social, ethical and legal issues into the entire development process in a deeply integrated, collaborative and interdisciplinary way” (McLennan et al., 2020: 1). Within this approach, the present study aims to make nursing care experts’ insights available for the shaping of early technology development for a care robotics initiative and for including their voices in the design and direction of the research (Breuer et al., 2024; Willem et al., 2024).
Data collection and participants
We combined multiple data collection methods to engage a diverse group of nursing care experts with varying levels of practical experience, different educational backgrounds, and partially overlapping professional identities, including nursing scientists, nursing students, and nursing care practitioners. Our data were collected between February 2021 and June 2023 and comprise transcripts from (1) six open-ended, semi-structured interviews with nursing scientists; (2) four scenario-based focus groups with nursing students, nursing care practitioners, and nursing scientists; and (3) an interdisciplinary LEGO® Serious Play® workshop with nursing care experts and robotics researchers (see Figure 1 and Table 1 for an overview). None of our participants participated in more than one of the methods. 3 Across all formats, we ensured balanced participation and focused on eliciting reflexive, experience-based insights.
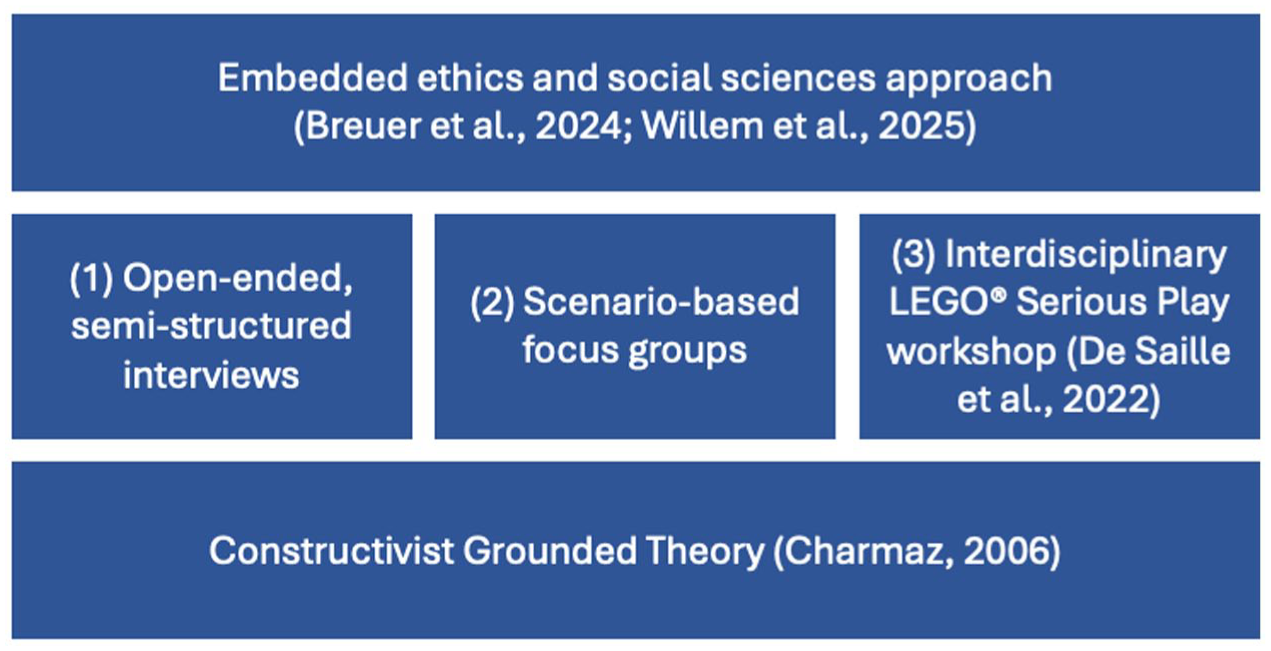
Methodology and research design.
Overview of methods and target groups.

We began with interviews with nursing scientists. Participants were selected for their topical expertise; three were affiliated with universities of applied sciences and three with universities linked to university hospitals. Interviews lasted 1–2 hours and were conducted as open-ended semi-structured conversations. They covered a range of topics, including the role of nursing science in German society, experiences with care robotics, the public discourse on robotics, the political and legal context, factors that might help nursing staff in the adoption of robotic technologies, and overall impressions and opinions on recent developments in nursing care and care robotics.
Insights from these interviews informed the design of subsequent scenario-based focus groups, which lasted 2–3.5 hours. We conducted three online focus groups with nursing students in the sixth semester of a dual nursing program at a German university of applied sciences that combines vocational training and academic studies. Their training spanned diverse care domains, including childcare, outpatient care, elderly care facilities, and various clinical settings, which enabled them to contribute detailed, context-rich perspectives. We also included material from a fourth focus group that invited healthcare practitioners more generally, which two nurses attended, along with three physicians.
All focus groups were centered around application scenarios developed in collaboration with care robotics researchers and based on prototypes under current development. Scenarios included (1) a humanoid robot for telemedicine, (2) a robotic telemedicine station for isolated patients, (3) an early mobilization therapy system for ICU patients, and (4) the Care-o-Bot system developed by Fraunhofer IPA for everyday assistance. Scenarios were illustrated using already published or internet-accessible video or image material to spark open discussions about the use of robotics in nursing care. Each session included questions about participants’ views on robot use in specific scenarios and tasks, their ideas of other nursing care activities suitable for the use of robots, areas where robots should not be used, and implications for work routines (see also Table 2 for more details).
Structure and content of the scenario-based focus groups.

https://www.youtube.com/watch?v=6ymaQlnnSSY (accessed 04.02.2026, 1:32–2:30).
https://www.youtube.com/watch?v=4wpIvt9BPuY (accessed 04.02.2026; we did not use this video in particular, but instead a shorter one containing the same footage, which is however not accessible online).
https://www.youtube.com/watch?v=GhZxVVgiyKA (accessed 04.02.2026, 19:04–19:59).
https://www.youtube.com/watch?v=nJj8wJg6jNM (accessed 04.02.2026, 1:54–2:50).
In the interdisciplinary LEGO® Serious Play® workshop (de Saille et al., 2022), we facilitated a dialog between nursing care experts and care robotics researchers. We invited all researchers from the care robotics research initiative we collaborated with, of which three participated. The nursing care experts were invited based on prior contacts with interviewees or focus group participants and included a nursing researcher and former nursing care practitioner, a nursing professor, and a nursing student and former nursing care practitioner from different German nursing institutions.
The workshop involved hands-on model-building with LEGO® bricks. Participants first built models representing their professional responsibilities and discussed the values embedded in them (e.g. participation, privacy, autonomy). They then constructed models of robots that they could imagine supporting the care of an older adult. The facilitator then asked them to modify their models and reflect on how these changes might positively or negatively influence aspects of responsibility. We paid special attention to how nursing care experts evaluated proposed models and roboticists’ imaginaries against their lived experiences in nursing care work. Figure 2 provides a few impressions of the workshop.

Impressions of the LEGO® Serious Play® Workshop (clockwise, from top-left): (a) The set of LEGO® bricks each participant received, (b) a model of a care robot built by one of the participants, (c) an overview of the models and their associated values, documented with yellow post-its, and (d) participants presenting their models.
Analytical framework
We used a qualitative, inductive, and interpretivist study design based on a constructivist grounded theory (Charmaz, 2006) approach, which aims to develop theory out of close empirical observations. This approach was particularly well-suited to our exploratory aim of understanding nursing care experts’ perspectives on the evolving integration of care robotics into nursing care work. Grounded theory enabled us to remain open to unexpected insights and to develop concepts closely tied to participants’ experiences and concerns.
Following the principles of theoretical sampling, early insights from our data analysis informed subsequent data collection, allowing us to refine our focus iteratively. This approach also supported the integration of diverse empirical materials into a coherent analytical framework. We determined that theoretical saturation was reached when no new theoretical insights for the core categories emerged from the most recent data.
All data were audio-recorded, transcribed, and analyzed using the MAXQDA software. We conducted initial line-by-line coding followed by focused coding, developing core categories in an iterative process and using memo writing as an additional means of reflection. Following the grounded theory commitment to treating data symmetrically as laid out in Charmaz (2006), we considered all data sources—interviews, focus groups, and workshops—as well as participants’ different professional backgrounds equally when developing analytical themes. We approached interpretation as an active, situated process of meaning-making, while remaining critically aware of the theoretical and experiential lenses we brought to the data (Charmaz, 2006). Coding and interpretation were developed collaboratively within the research team through ongoing reflexive discussions.
The three empirical themes presented in this paper emerged early in the analytical process and were refined through multiple cycles of comparison across our material. We noticed that nursing care experts often made sense of care robotics by viewing it through the lens of existing challenges and responsibilities within their daily work, rather than discussing robots primarily as technical artifacts or tools to be used in nursing care practice. In doing so, they frequently related care robotics to epistemic practices, forms of relational and affective work, or existing professional standards characterizing contemporary nursing care environments. Our focused coding centered on these concerns and led us to refine our analysis around three ways in which nursing care experts characterize care robotics, which also structure our empirical analysis: (1) as an open-ended, empirical concern for nursing science, (2) a means to delineate non-automatable from automatable nursing care practices, and (3) a potential remedy for nurses’ assistive and executive responsibilities.
Our scholarly background in feminist STS sensitized us to these dynamics and led us to further develop our analysis using the conceptual lens of “matters of care” (Puig de la Bellacasa, 2011: 85). This focus emerged from our observation that nursing experts consistently articulated care robotics through concerns, attachments, and responsibilities that resonate with a “matter of care” perspective. Their accounts foregrounded the ethical, affective, and relational dimensions of nursing care, alongside a shared concern that care robotics might disrupt these dimensions if insufficiently attended to. Through iterative cycles of focused and theoretical coding, we used the matters of care lens to examine how nursing experts framed care robotics as something that demands ethical attention and responsibility because it directly affects what they understand as good nursing care—scientifically, practically, and professionally.
All quotes from interviews and focus groups presented in this article were translated by the authors from German to English.
Results
Based on our analysis, we will present three key themes in this section that show how the nursing care experts perceive, evaluate, and imagine care robotics as (1) an open-ended, empirical concern for the nursing sciences, (2) a means for delineating between automatable and non-automatable nursing care activities, and (3) a potential remedy for nurses’ assistive and executive responsibilities.
Care robotics as an open-ended, empirical concern for the nursing sciences
The nursing care experts consistently stressed that care robotics is an open-ended empirical concern—one in which they envision a significant and active role for the nursing sciences. We found this theme especially often in our interviews with nursing scientists. The theme is closely related to discussions surrounding the ongoing institutionalization of nursing as an independent scientific discipline in Germany and the nursing care experts’ concern that current care robotics research does not sufficiently reflect and incorporate the epistemic values, methodological approaches, and professional insights of the German nursing sciences. Nevertheless, the nursing care experts exhibited a high degree of openness to using robotic technologies in nursing care practice, provided such technologies are assessed according to the methodological frameworks and standards established by the nursing sciences and their development involves nursing care experts from the earliest stages.
Our participants saw nursing science as underrepresented in Germany, especially compared to other countries such as the USA and Scandinavia. They attributed this to its limited institutionalization as an independent scientific discipline at German universities, and its marginal involvement in research and health policy at the federal and state level. One nursing scientist described how resources were allocated to research during the COVID pandemic as an outcome of this underrepresentation: There is this corona task force from the DFG, no one from nursing science is on it. Where do we have the biggest problems? In elderly care wards. All the funding that has been provided now, billions in funding on the subject of COVID-19, has been distributed to university medicine. (nursing scientist 3)
This account highlights the institutional logic behind the allocation of resources for nursing research, where nursing remains subsumed under the umbrella of medicine. While the most significant challenges in the pandemic were emerging in (clinical) elderly care, resources were not allocated directly to nursing research but instead to “university medicine,” as clinical elderly care’s institutional representative in Germany. This puts medicine in the role of an essential gatekeeper for the nursing sciences in terms of access to funding.
As the nursing scientist continued, this situation makes it generally challenging for German nursing science to formulate and address healthcare issues as an independent scientific discipline, since research priorities often favor medical and economic concerns. As a result, many empirical research gaps in the nursing sciences would persist, waiting to be addressed: for example, the actual needs of older adults receiving nursing care, the heterogeneous composition of the nursing profession, and the impacts of specific care interventions on patient outcomes. In this light, the nursing scientists viewed the rise and support for care robotics as a strategic opportunity. It presents a potential avenue to enhance the visibility and recognition of German nursing science as an independent academic discipline. The focus on nursing care work in care robotics research was very much welcomed, as this could provide opportunities for more direct collaboration between technology researchers and nursing researchers, thus improving the allocation of resources for nursing research without having to rely on the role of medicine as a gatekeeper.
At the same time, many nursing care experts remained concerned about the current orientation and motivations of existing care robotics research. They painted a picture of care robotics as still too focused on fundamental technical challenges in robotics itself instead of focusing on challenges related to nursing care work. They also criticized the tendency of robotics research to overpromise about the capabilities and potential benefits of its prototypes. Some nursing scientists questioned whether the challenges that ostensibly motivate care robotics research (e.g. the increasing shortage of nursing care workers) are even problems that can be solved through the development and implementation of new technologies in any case. In these accounts, German research policy became a common reference point, especially its strong prioritization of the development of technical products and prototypes within care robotics research programs: [T]he engineering country Germany is simply looking for a technological solution to a social problem and the fact that the technological solution may not be a good solution or a satisfactory solution is not taken into consideration at all. (nursing scientist 3)
This nursing scientist emphasizes the social and political nature of the current challenges in nursing care work, suggesting that technological solutions might be too limited to address its problems. Yet, social solutions remain marginalized in Germany’s current, technology-centered high-tech policy and research agendas. These agendas tend to prioritize engineering-oriented criteria—such as safety, efficiency, and functional robustness—while largely overlooking epistemic standards and methods from nursing science. As a result, nursing scientists are often relegated to the limited role of validators in the final phases of research projects, without being granted a more substantial involvement early in the process. In such constrained positions, nursing scientists struggle to contribute effectively to care robotics research, missing opportunities to shape care robotics as the empirical, open-ended concern they believe it must necessarily remain.
To counter these current tendencies, nursing scientists argued that care robotics research should increase its focus on assessing and measuring the specific outcomes that result from using care robotics systems in a particular context of nursing care. For the context of clinical environments, for instance, nursing scientists recommended adopting criteria from evidence-based nursing, such as feasibility and effectiveness, or the common research framework of “complex interventions” (Corry et al., 2013: 2366) for accommodating the complexity of nursing care work in the hospital. Importantly, these suggestions did not involve a wholesale rejection of the development and use of care robotics systems. Rather, they called for readjusting current research agendas to better align with the epistemic commitments of nursing science and for opening the research process to all relevant stakeholders.
Care robotics as a means to delineate (non)automatable nursing care practices
This hopeful attitude toward care robotics was more difficult to sustain when discussions turned to the push for greater efficiency in nursing care through automation. Nursing care experts emphasized that care work is inherently relational and multifunctional, qualities that resist the neat division of tasks into the “automatable” and “non-automatable” categories often assumed in robotics research. This theme surfaced most prominently in the focus groups with nursing students, in which we showed them videos and images from ongoing care robotics research that rely on such a logic of delineation. Their responses highlighted three intertwined concerns: defining the core of nursing care, preserving its multifunctional character, and sustaining nursing care practitioners’ capacity to build meaningful relationships with patients.
Even though most nursing care experts themselves attempted to delineate between automatable and non-automatable nursing care practices, they continuously highlighted the difficulty—and at times the impossibility—of establishing such a clear-cut difference. When discussing which existing practices might be suitable for automation, participants generally shared the view that there is a fundamental core of nursing care work that should not be delegated to robots. A primary criterion for gaging whether a specific existing practice would belong to this core was its relevance for building trusting patient relationships. This was seen as a necessary prerequisite for good patient outcomes and good nursing care in general.
Consequently, the most frequently mentioned non-automatable practices involved direct interactions with patients. These include formal and informal conversations, practices that involve body contact with patients, and other activities that offer opportunities for communication, such as administering food or water. Consider this comment from a nursing student responding to the question of whether they could imagine using teleoperated robots to conduct nursing rounds in the clinical setting: So now, perhaps specifically about nursing rounds, I have to say that I can only imagine this in an assisting function at best, because one of the core tasks is also somehow the relational work, that is, simply the personal interaction with the patient. (focus group 2)
The quote provides a clear example of how the nursing care experts described relational work as essential to nursing care practice. It is portrayed as a fundamental building block of nursing care practice, emphasizing the importance of “personal interaction” with patients. Therefore, care robotics systems are expected to play a strictly “assisting” role in the relational “core tasks,” which should remain undisturbed and reserved for human nursing care practitioners. Examples of tasks for robots in such an assisting role include stocking dressing trolleys in the operating room, reminding visitors to wear masks during the COVID-19 pandemic, preparing medication, measuring vital parameters, providing directions to visitors and patients within the healthcare facility, interpreting for international patients, and documentation.
However, this clear-cut logic of delineation was regularly contested by a shared understanding among nursing care experts that nursing care practices are largely multifunctional. This made the border between automatable and non-automatable practices more fluid, sometimes resulting in heated debates about whether a particular practice could or should be automated. One example was the preparation of hospital beds, a task frequently mentioned as automatable in focus group discussions. However, one nursing expert stressed that it creates important affordances for social interaction: So I can put a cover on a pillow even if I don’t fully concentrate on it, but I don’t stand around stupidly either, so [patients] don’t have the feeling that they’re hindering me from doing my work, but they realize that I hear them, that I can listen to them. (. . .) And that’s why, although it’s a recurring and idiotic activity, i.e., very unspecific, I wouldn’t give it up because, as I said, this offer to talk is something that’s simply there. (nursing scientist 6)
Despite being “unspecific” and lacking the direct relational qualities, the preparation of beds becomes, in this account, a valuable practice for nurses. It satisfies a particular social expectation among patients, namely, not to keep time-pressured nurses from doing their work or taking too much of their time, while still allowing them to enjoy a nurse’s attention and share with them, for instance, how they are feeling. This makes it an activity conducive to building caring relationships with patients. The isolated functionality of “making beds” is seen as multifunctional: not restricted to providing a necessary infrastructure for clinical healthcare in the form of a clean and disinfected bed, but instead extending to an opportunity to talk and practice care.
The aspect of multifunctionality even extended to a practice that most nursing care experts viewed as the most tedious part of their work: documentation. In our material, documentation consistently appeared at the top of the list of nursing care practices perceived as suitable for automation. Making documentation more efficient, comfortable, and enforceable is also an ongoing concern in nursing research (Graham et al., 2018; Heartfield, 1996). Yet, one nursing scientist emphasized a more nuanced perspective, highlighting documentation’s “meaningful” role beyond the legal, budgetary, and regulatory functions it is mainly associated with. They described how documentation serves as a valuable source of knowledge about past “clinical decisions” and their outcomes, highlighting its importance as a critical tool for informed decision-making in everyday care (nursing scientist 3).
To sum up, although the nursing care experts actively discussed whether or not certain nursing care practices could be automated, the logic of automation itself often remained incompatible with their shared understanding of nursing care as a relational and multifunctional practice. This understanding puts into question existing approaches in care robotics research that attempt to delineate automatable from non-automatable practices by modularizing nursing care practice into singular, stand-alone functions that robots can perform (Vallès-Peris and Domènech, 2020). Underlying this theme were also broader reflections on the existing professional responsibilities of nurses, which we explore further in the third theme.
Care robotics as a potential remedy for nurses’ assistive and executive responsibilities
This theme emerged from the nursing care experts’ reflections on the traditional self-understanding of nursing as an assistive healthcare profession and the staging of care robotics as an assistive technology. It builds on nursing care workers’ everyday experiences and collective reflections about a future in which some of their current professional responsibilities might be delegated to technology. The nursing care experts supported the idea of care robotics as an assistive technology, provided it can enhance, preserve, or sustain the autonomy of the nursing profession.
While the nursing care experts understood nursing as “a profession in its own right” and themselves as “experts” in that profession (focus group 1), the daily reality of nursing care practice often stood in sharp contrast to this understanding, positioning them as assistive and executive agents under the authority of other healthcare professions. Many emphasized their struggles in dealing with these dynamics, noting that despite recent reforms in nursing education and regulation aimed at enhancing the professional autonomy of nursing care practitioners, meaningful change in everyday nursing care work remains limited.
A typical reference point was the recent reform of the nursing professions regulation, which formally elevated nursing into a curative profession (dt. “Heilberuf”), a legally defined status in the German healthcare system associated with therapeutic responsibility and autonomous clinical decision-making. This status grants expanded decision-making authority but also increased accountability for these decisions and their consequences. A nursing scientist described the results of this reform for nursing care practice in the following way, using the example of writing prescriptions for support stockings: [Support stockings] are aids, doctors have nothing to do with them, and yet they used to have to prescribe them. So [nurses used to] get a patient in a hospital and realize that he probably needs support stockings, but they had to hope that the doctor sees it the same way as they do, although they nurse and care for [the patient] for a week and notice that his circulation keeps derailing. . . Today, [nurses] are allowed to do these things themselves, as these things have become the responsibility of the nursing staff. (nursing scientist 1)
The account provides an example of how the recent reform is supposed to enable a better allocation of decision-making competencies in the clinical context. Based on their daily interactions with patients, nurses often have the experiential knowledge needed to prescribe specific health interventions that doctors lack. With the current reform, they can now also act upon this knowledge on their own behalf and without having to rely on other healthcare professions.
However, many nursing care experts pointed to the mismatch between this formal enhancement of decision-making capacities and their experiences in actual nursing care practice. Many of our nursing care experts found themselves between a rock and a hard place in which they, on the one hand, tried to embrace the increased autonomy and responsibility provided by the reform of the nursing professions regulation, but on the other hand, could hardly live up to their old, existing responsibilities, especially in the clinical context. Consider this account of a nursing student on how the long-existing responsibility for changing beds is currently handled in a hospital: If a patient has a certain germ, the hygiene plan stipulates that the bed linen must be changed every time before this patient is collected for an examination. So it’s simply impossible to do this in terms of time and logistics. He can have three examinations a day. (. . .) I don’t notice this at all as a nurse, I don’t delegate anything here, but it’s still my responsibility to change the bed linen, and if anything happens (. . .) then I’m liable. (focus group 1)
The student highlights the executive responsibility of nurses to change the bedding of patients with infectious diseases between medical examinations. They find that this responsibility is often difficult to fulfill under the current working conditions. Compounding the issue, nurses are not involved in the planning or scheduling of these examinations, leaving them without the ability to influence the timing or coordination of related tasks. This problematic situation negatively affects both patients and nurses: beds might remain unchanged, posing health risks, and nurses are liable for it, although they find themselves unable to improve the situation.
In this divergence between aspiration and reality, care robotics was seen as an assistive resource that could take over some of nurses’ current assistive and executive tasks—provided it supports rather than undermines their professional autonomy. While roboticists often promote “assistive” care robotics (i.e. assistive to nurses rather than patients) to ease concerns about robots replacing nurses (Breuer et al., 2023), our nursing care experts accepted this framing only when the technology truly assists their work. Consider this quote: Where I see the robots as assistance is, for example: some patients are post-operative, they have to have their blood pressure measured regularly, and we nurses, we just don’t always manage to measure the blood pressure on time after an hour, or after half an hour, or depending on how the doctor wants it—that there is a robot that really simply measures the pressure every half hour or hour. (focus group 3)
This nursing student reflects on the practice of measuring patients’ blood pressure according to the instructions of doctors. In the account above, “the robot” appears as an alternative assistive agent that can fulfill the requirements for blood measurement set by “the doctor,” which “we nurses” cannot cope with under the current conditions. The nursing student’s statement therefore combines both the difficult work conditions in nursing practice and the assistive nature of the task (“how the doctor wants it”) to propose that robots could take it over.
Consider also this quote from another nursing student who likewise reflects on the responsibilities of the nursing profession generally, also referring to the less-than-ideal conditions under which it currently operates: I don’t want to call it mass processing care (Ger. “Massenabfertigungspflege”), but at the moment it is simply that, because it can’t be done any other way. Regardless of whether robotics or not, if we simply supported the nursing staff with either more employees, ha-ha, or just robotics or other aids, we could also ensure more human care again, which is actually part of the profession of nursing. (focus group 3)
In this quote, the nursing student describes the responsibility to “ensure humane care” as a fundamental part of nursing. However, meeting this responsibility is threatened by the challenging conditions under which nursing care practice is suffering. Care robotics is mentioned here as one, but not necessarily the preferred, way of counteracting this situation, given that the possibility of hiring more nursing care staff is dismissed as unrealistic (“ha-ha”). Thus, care robotics becomes a placeholder for all kinds of changes that could help nursing into a better future in which it can eventually live up to its professional responsibilities.
Discussion and conclusion
This paper has examined how nursing care experts perceive, evaluate, and imagine care robotics by engaging the nursing care experts with examples from ongoing care robotics research and exploring their own visions for its future. By focusing on the nursing care experts’ experiences, knowledge, and expertise, our study addresses an important gap in the largely technology-centered literature on care robotics. Our results shed light on the current conditions and challenges in the German healthcare system, showing how they shape nursing care experts’ ability to practice nursing care work, conduct nursing research, and handle professional relationships. They also reveal a strong desire among nursing care experts to be involved in the political decision-making process regarding these conditions, the role of care robotics in nursing care work, and the future of nursing in German healthcare overall.
Based on these insights, we now discuss the normative commitments implied in the nursing care experts’ accounts of care robotics, turning to the challenges these accounts emphasize as “matters of care” (Puig de la Bellacasa, 2011: 85). Puig de la Bellacasa’s notion of matters of care invites us to think about these challenges as “undervalued and neglected issues” (Puig de la Bellacasa, 2011: 85) for which we can generate care by articulating, engaging with, and relating to them. By linking care robotics to these challenges, the nursing care experts effectively turned these challenges into matters of care. They created an imaginary in which care robotics became a vehicle for change with the potential to address these challenges—provided care robotics remains committed to engaging with them and, thereby, generates care for them. Accordingly, the concrete examples of care robotics research we shared were most positively received when they remained attuned to the challenges that nursing care experts face in their own professional field.
Three dimensions to care for: Nursing as science, practice, and profession
In this section, we discuss and conceptualize our findings as three distinct dimensions that capture the main themes of our analysis in relation to the conditions of nursing care work in Germany and explore how care robotics is seen as possibly able to address these challenges. We propose nursing-as-science, nursing-as-practice, and nursing-as-profession dimensions. Each dimension highlights how the nursing care experts’ perspectives, evaluations, and imaginaries are deeply shaped by the very logics of how robotics is currently promoted: as a viable means to address the challenging conditions of nursing care work. At the same time, these logics become fragile and unstable when greater attention is paid to the specificities of these conditions and how care robotics could really help transform and care for them.
The nursing-as-science dimension builds on nursing care experts’ view of care robotics as an open-ended, empirical concern for the nursing sciences. When articulating this dimension, nursing care experts build on the tradition of other health sciences to argue that care robotics should be assessed by measuring patient outcomes. At the same time, they present the importance of measuring the effects of care robotics as motivated by desires to overcome the current, technology-centered modes of research and allow the nursing sciences to participate in developing technologies that can and should be used in their professional context. Therefore, an important matter of care in this dimension was less the production of new, “evidence-based” (Ingersoll, 2000) nursing science knowledge about the use of care robotics in nursing practice, but instead, more meaningful participation in care robotics research as well as continuous engagement of relevant stakeholders as a better way for understanding how care robotics can usefully improve nursing care experts’ and patient wellbeing.
The nursing-as-practice dimension is reflected in the nursing care experts’ view of care robotics as a means to delineate (non)automatable nursing care practices. This dimension arose from nursing care experts’ engagement with the logic of automation, which breaks down nursing care practices into smaller, isolated tasks amenable to being delegated to robotic systems. This logic stood in tension with the relational and multifunctional nature of nursing care practice. The nursing care experts highlighted the relevance that certain nursing care practices might gain in a specific care situation that cannot be foreseen, evaluated, or defined in advance. An important matter of care in this dimension was that care robotics research should remain open to emerging situational needs and avoid dismissing them by adhering too rigidly to taskifying research approaches (Vallès-Peris and Domènech, 2020).
The nursing-as-profession dimension becomes evident in the nursing care experts’ hope that care robotics can support the autonomy of nursing care work and its professional responsibilities. It reflects on the introduction of care robotics from the perspective of executive and assistive healthcare professionals, who are expected to exercise greater formal autonomy granted through recent political reforms, yet struggle to do so within the constraints of everyday workflows. While our nursing care experts were primarily academically trained professionals who understood nursing as a standalone profession and discipline, they frequently found themselves confronted with a version of everyday nursing care work that did not align with this vision. The central matter of care, then, became the future of nursing itself—its evolving role as a curative profession and the uncertainty surrounding how that role might unfold. A key question emerged: Could the assistive capacities of care robotics help reconcile the professional self-understanding of nursing care experts with the practical realities they face? Or would it further entrench the misalignment between the (self-)expectations of nursing care work and its everyday enactment?
Preserving care in nursing care: Turning care robotics into a matter of care
All of these matters of care reflect an understanding of nursing care work that highlights its specific, unruly, and experiential nature, in contrast to the orderly, uniform, and impersonal vision of nursing care work that care robotics research currently often implies. While this underlines once more the need to reconsider existing understandings of nursing care work that drive care robotics research (Breuer et al., 2023), it also leads to critical ethical concerns, such as: what can a good future for nursing care work look like? What role could care robotics play in shaping this future? And how do we best care for nursing care work itself?
Going back to the work of Puig de la Bellacasa (2011), these concerns turn care robotics into a matter of care in itself. Should it become part of the future of nursing care work, the research and development of care robotics must remain committed to attending to the tensions and frictions revealed by our analysis, and attuned to the ongoing challenge of preserving care in nursing care practice. In this sense, care robotics researchers are called upon to become allies of nurses—working with, rather than on, nursing care work—by aligning their research agendas, design practices, and evaluative criteria with the situated knowledge, values, and concerns of those who carry responsibility for nursing care in practice.
Possible solutions are manifold and include, first, the better involvement and representation of stakeholders from nursing in care robotics research and policymaking. This could bridge the current gap between technology-driven research agendas and the actual needs of nursing care practitioners, fostering the development of technologies that align with these needs and creating more inclusive and socially robust processes for deciding whether and which robotics systems should be integrated into nursing care practice. These processes would position nursing scientists as important contributors in a currently highly-prioritized and well-funded research domain, potentially reshaping the representation and influence of the nursing sciences in the German research landscape over the long term. Without such processes in place, care robotics research runs the risk of turning into a hammer looking for nails (Bischof and Graf, 2022), that is, pursuing research that is driven by robotics disciplinary priorities and technical affordances, rather than the actual needs of those affected by it.
Second, we should rethink current approaches to care robotics to better represent nursing based on how it could be, under improved circumstances, rather than on the grounds of its current mode of constantly coping with structurally deficient healthcare systems. While the nursing care experts were generally open to the use of care robotic systems as assistive devices, care robotics should not become a mere band-aid solution that risks reinforcing existing structural deficiencies instead of addressing them. If care robotics is designed primarily to compensate for systemic shortfalls, it may inadvertently solidify a narrow and diminished view of care—as a set of mechanical tasks, devalued labor, or a burden to be offloaded (DeFalco, 2020)—rather than as skilled, relational, and context-sensitive work. Instead, it should create a solid understanding of how care robotics can contribute usefully to a more desirable future for nursing care work, in which its professional aspirations, standards, and values are upheld.
Overall, this work demonstrates the importance of providing space and time for actors from nursing to contribute their perspectives on the potential uses of care robotics and other emerging technologies in research and development early in the process. Care robotics research is still far from living up to its aspirations (Nettleton et al., 2025): prototypes abound, and significant technical challenges persist. This leaves it open whether and to what extent robots will become a practical reality in nursing care practice—not only from a nursing perspective but also from a technical standpoint (Yang et al., 2018).
Analyzes like ours can inform care robotics research by challenging overly narrow understandings of the professional and practical contexts in which care robotics are meant to be implemented. This can help find ways that encourage care robotics researchers to “care with” (Imrie and Kullman, 2016: 1) nursing care; to create research practices that are inclusive, “response-able” (Haraway, 2008: 71; Haraway, 2016: 20), and engage all relevant expertise and stakeholders in shaping the future role of care robotics in nursing care work.
Limitations
There are some limitations to this work that we would like to address. Our data collection was focused on nursing care experts with academic nursing training; non-academic nursing care practitioners who solely underwent vocational training at nursing care schools (Pflegeschulen) within the German vocational education system are not represented in our sample. Our study does not assess the differences or similarities among the various groups of health professionals or the socio-demographic characteristics (age, gender, socioeconomic background etc.) of our participants in further detail. It should also be noted that the results of our analysis are situated in a particular local context—German healthcare, and particularly within the federal state of Bavaria. To examine how these insights might translate to or differ from international contexts, further research would be needed.
Footnotes
Acknowledgements
We would like to thank the Lighthouse Initiative Geriatronics and, in particular, Prof. Dr. Sami Haddadin, Dr. Abdeldjallil Naceri, Jon Skerlj, and Konstantin Ritt for their invaluable support. We would like to thank Dr. Stevienna de Saille for conceptualizing and facilitating the Lego Serious Play® Workshop. We also thank our interviewees and focus group participants for sharing their perspectives, opinions, and ideas with us. We thank the Bavarian Research Institute for Digital Transformation (bidt) for funding the research that led to this article. Finally, we also thank Dr. Mallory James for the language editing of the manuscript.
Ethical considerations
The research project Responsible Robotics (RR-AI) received ethics approval (344/20 S-SR) from the ethics committee of the Technical University of Munich.
Consent to participate
Informed consent to participate was obtained in written form.
Author contributions
As the senior author, author 3 conceptualized the study, acquired project funding, and supervised the research this article is based on. Author 1 and 2 prepared, conducted, and analyzed the interviews, focus groups, and workshops. Author 1 wrote the first draft of the manuscript. Authors 2 and 3 read and commented extensively on the first and subsequent drafts before initial submission. All authors discussed and conceptualized how to address reviewer comments. Author 1 revised the manuscript for resubmission. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research presented in this article was primarily funded by the Bavarian Research Institute for Digital Transformation (bidt) as part of the project “Responsible Robotics (RR-AI).” Authors 2 and 3 further received relevant financial support from the Robotics Institute Germany (RIG), funded by the Federal Ministry of Research, Technology and Space (BMFTR) under grant 16ME0997K and the Center for Responsible AI Technologies (CReAITech), which is co-funded by the University of Augsburg, The Munich School of Philosophy and the Technical University of Munich.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data have been gathered according to the existing standards of the European General Data Protection Regulation (GDPR) and the ethical standards set by the ethics committee of the Technical University of Munich. To avoid compromising the individual privacy of our participants, it is not possible to share our interviews and focus group transcripts publicly. The data are stored in the university database system at the Technical University of Munich.