
Abstract
There is growing interest in menopause discrimination in healthcare, the workplace and beyond. However, there is a dearth of research on lesbian, gay, bisexual, transgender and queer (LGBTQ+) experiences of the menopause. This article reports on a scoping review of the recent literature which identified a very limited number of articles and a wide range of knowledge gaps. This is discussed in relation to LGBTQ+ wider health, healthcare and workplace inequalities, and heteronormative and cisnormative conceptualisations of the menopause. A research agenda is proposed. Research should: be intersectional; differentiate between LGBTQ+ sub-groups; aim to understand how menopause experiences impact and are impacted by minority sexuality/gender identities; and examine how menopause healthcare and workplace support can be LGBTQ+ inclusive. Such research is urgently needed to ensure that LGBTQ+ people are fully included in menopause justice discussions and solutions.
Introduction
There is growing interest in the menopause, which is when a biological female’s periods cease and she is no longer able to reproduce. The bulk of the literature so far comes from the UK and the US (Cahn, 2021; Crawford et al., 2021; Westwood, 2024). It mostly affects cisgender (cis) women (i.e. those born as biologically female, designated as female on their birth certificate, and who continue to identify as female) in their late 40s to early 50s. The menopause is often preceded by symptoms for several years (‘perimenopause’) and may be followed by symptoms afterwards (‘post-menopause’). Symptoms vary, including hot flushes; night sweats; anxiety; depression; difficulties with memory and concentration (‘brain fog’); irregular periods; excessive bleeding; vaginal dryness; and reduced/loss of libido (National Health Service (NHS), 2023). Research on the menopause is growing and so too is the array of supports available. For example, in the workplace there is a growing number of menopause policies, opportunities for reasonable adjustments (e.g. flexible working, environmental temperature control, different uniforms, counselling/ mental health support, etc.), although this remains highly variable among employers (Beck and Brewis, 2024). In the community, there is a range of supports available, via the NHS, such as hormone replacement therapy (HRT), individual/group support, written information and guidance, and alternative therapies. However, GP knowledge and understanding is patchy (Dintakurti et al., 2022), and there is often limited availability of a full spectrum of services.
Cis women affected by the menopause include those of all sexualities, that is, they may identify as heterosexual, bisexual, pansexual, lesbian, gay, queer, etc. It is not only cis women who are affected by the menopause and menopause-related symptoms. Some transgender women (‘trans women’), who were born biologically male, but identify as female, might experience menopausal symptoms if they undergo oestrogen reductions for clinical reasons in later life (Eismann et al., 2019) although whether they understand this in terms of menopause is contested. Additionally, ‘[s]ome trans men, gender nonbinary, and genderqueer individuals with at least one ovary and a uterus’ may also experience the menopause/menopause-type symptoms’ (Crawford et al., 2021: 1583).
According to a recent 27-country study by Ipsos, on average, 80% of people identify as heterosexual, ‘3% as gay, lesbian or homosexual, 4% as bisexual, 1% as pansexual or omnisexual, 1% as asexual, 1% as “other”, and 11% don’t know or won’t say’. Ipsos also found that ‘[o]n average, 1% of adults describe themselves identify as “transgender”, “non-binary/non-conforming/gender-fluid” or “in another way” rather than as “male” or “female”’ (Ipsos, 2023). Overall, non-heterosexual people form a sizeable sub-population. They, and trans people, are entitled to equitable health and healthcare support including in relation to the menopause not only based on scale, but also on the principles of equality, diversity and inclusion (Fish et al., 2021).
However, most of the current literature on the menopause relates only to white heterosexual cisgender women. As the UK Parliament’s Women and Equalities Committee (Women and Equalities Committee (WEC), 2022a) has observed,
Evidence to the inquiry and responses to our survey suggested that people with certain protected characteristics may experience specific challenges with menopause; witnesses pointed to LGBT+ people, younger women and ethnic minority women, in particular. Many people in these groups felt they were not included in a conversation which, when it happened at all, historically focussed on heterosexual, white, middle-class, ‘older’ women (para 11).
There is highly variable menopause healthcare in the UK, with the prescribing of HRT amounting to a ‘postcode lottery’ (Iacobucci, 2022). Women from lower socioeconomic backgrounds are far less likely to be prescribed HRT than women from higher ones. Research has also suggested that women from lower socioeconomic positions, and homeless women in particular, experience more severe menopause symptoms (De Mello et al., 2021). In terms of women in prison, their needs are less-well met than women not in prison, especially among older women, whose menopause-related issues often go unaddressed (Van Hout et al., 2022). Women from Black, Asian and minority ethnic backgrounds are disadvantaged in multiple ways at the intersection of the menopause with race and ethnicity (Cortés and Marginean, 2022; Prasad, 2023). For example, ‘menopause is still a social stigma and a taboo subject in many minority communities, many communities do not talk about it openly yet . . . [and] there may be a general expectation for women to stay silent and not complain about their ailments’ (Prasad, 2023: 236). Women of migrant/refugee status are more likely to experience precarity in access to menopause care particularly those who are on the legal borderlands (Ussher et al., 2019). Women with intellectual disabilities face heightened challenges communicating about their menopause symptoms and being provided with accessible information in relation to them (Moore et al., 2023; Moseley et al., 2020; Schupf et al., 1997). Women with autism encounter limited awareness about their needs (Groenman et al., 2022; Karavidas and de Visser, 2022; Moseley et al., 2020): there is ‘a lack of professional knowledge, understanding and communication about menopause for autistic people, and an absence of support’ (Moseley et al., 2020: 1243). Women with complex/chronic physical health problems can find it difficult to disentangle their pre-existing symptoms with their menopausal ones which can also interact to mutually inform one another (MacGregor, 2018; Mollard et al., 2018; Morales-Rodriguez et al., 2023).
However, while there is a growing awareness about how minority issues impact menopause experiences (Riach and Jack, 2021; Riach and Rees, 2022), (LGBTQ+) issues are rarely mentioned (Everett et al., 2021; Glyde, 2022a, 2022b, 2023; Throsby and Roberts, 2024). This is within the wider context of systemic LGBTQ+ health and healthcare inequalities, with LGBTQ+ people experiencing poorer health, and poorer health outcomes, than non-LGBTQ+ people (Fish et al., 2021; McDermott et al., 2021; Medina-Martínez et al., 2021; Zeeman et al., 2019; Westwood et al., 2020). Similarly, good practice guidance tends to exclude LGBTQ+ issues. For example, the European Menopause and Andropause Society (EMAS) position statement on the ‘essential menopause curriculum for healthcare professionals’, written by leading international authors (Rees et al., 2022), makes no mention of lesbian, gay and bisexual cis women’s healthcare needs in relation to the menopause and only mentions in passing that,
Some people require additional attention, with involvement of specialist services. These include women with chronic disease, premature ovarian insufficiency or early menopause or pre-existing disability, as well as transgender and gender-nonconforming people (p. 75).
Turning to the workplace, in recent years, a growing body of research has highlighted that workplace systems are often not menopause-friendly, menopausal women are often under-supported, and many are subject to bullying and harassment, often linked to the intersection of ageism and sexism (Beck and Brewis, 2024; Chartered Institute of Personnel and Development (CIPD), 2023; Jack et al., 2021). Some women have sought legal redress in the UK and the US, primarily drawing upon non-discrimination legislation, although there are concerns about the extent to which the law currently provides sufficient protection from menopause discrimination both within and beyond the workplace (Cahn, 2021; Cahn et al., 2024; Crawford et al., 2021). In the UK there has also been a burgeoning of employment guidance and policies aimed at improving menopause support (Hardy et al., 2018). Several contributors to the Women and Equality Committee’s consultation process highlighted the importance of workplace menopause policies (where they exist) being LGBTQ+ inclusive (Glyde, 2022b; Trade Union Congress (TUC), 2022; UNISON, 2022). However again, despite an emerging appreciation that menopause is ‘an intersectional experience’ (Riach and Jack, 2021: 10793) most of the literature on menopause in the workplace relates only to heterosexual cisgender women. For example, in the UK, the Chartered Institute of Personnel and Development (CIPD) recently surveyed 2000 women about their experiences of menopause in the workplace (Chartered Institute of Personnel and Development (CIPD), 2023). The study did not ask about sexual orientation or gender identity.
Despite the expanding appreciation of menopause and diversity, and a growing interest in achieving ‘menopause justice’ (Cahn, 2021) by eradicating menopause inequalities, research on LGBTQ+ people experiencing the menopause remains ‘desperately needed’ (Riach and Rees, 2022: 100395). This is clearly an equality issue, with implications for the care and support of LGBTQ+ people in healthcare services, the workplace and beyond. The discursive silencing of LGBTQ+ individuals’ experiences of the menopause, obscured and occluded by heteronormative and cisnormative framing of it, not only prevents an understanding of those experiences, but it also paints a partial (heteronormative, cisnormative) picture of menopause, thus limiting full appreciation of its multiple, complex, intersectional meanings.
This article reports on a scoping literature review of recent articles based on empirical research about LGBTQ+ experiences of the menopause. It synthesises the available evidence reported in those articles, identifies knowledge gaps and sets a research agenda to improve much-needed knowledge and understanding.
Method
The research design was a scoping literature review (Arksey and O’Malley, 2005). The research questions were: (1) ‘How many empirical studies in the past ten years have been conducted specifically on lesbian, gay, bisexual, queer, transgender and/or gender non-binary persons’ experiences of the menopause, with particular focus on healthcare and the workplace?’; (2) ‘What did those studies find?’; and (3) ‘Which area(s) is/are under-addressed in the literature?’
The databases searched were Medline (Ovid), PsycInfo (Ovid), PubMed and Web of Science Core Collection. A general Google search (for grey literature) was also conducted. Literature was limited to English language publications, between January 2014 and December 2023. Additional references were searched by cross-checking references in selected literature. Search terms are listed in Figure 1. Exclusion criteria are listed in Figure 2. Other systematic reviews were examined (Sobel et al., 2024), and their reference lists hand-searched.
Search terms used.
Exclusion criteria.
Results
A total of 10 studies were identified. These are summarised in Table 1.
Selected studies.
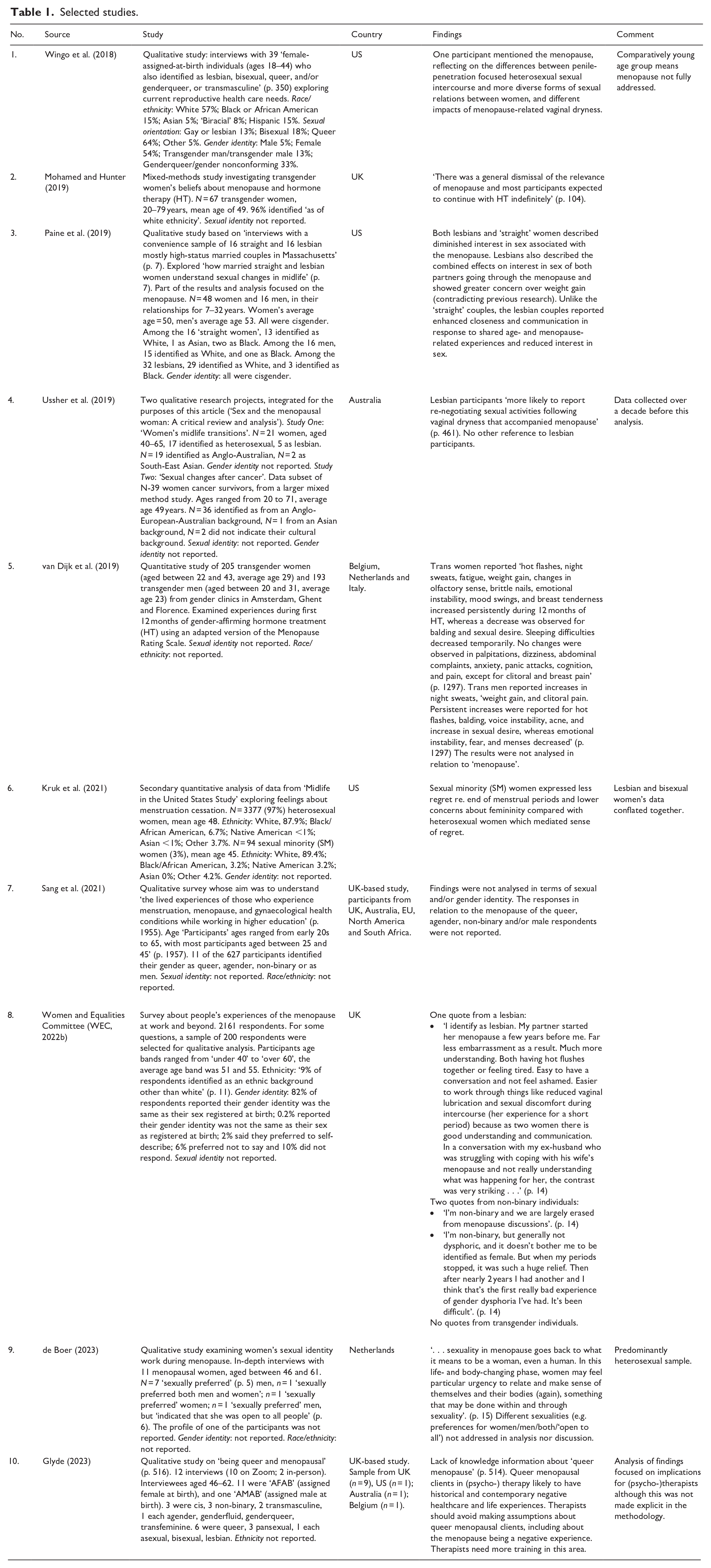
Four studies were conducted solely with sub-groups of LGBTQ+ people. Wingo et al.’s (2018) study on reproductive health care needs comprised ‘female-assigned-at-birth individuals (ages 18–44) who also identified as lesbian, bisexual, queer, and/or genderqueer, or transmasculine’ (p. 350). Van Dijk et al.’s (2019) study examining experiences during the first 12 months of gender-affirming hormone treatment (HT) comprised both transgender women and men. Glyde’s (2023) study of ‘being queer and menopausal’ (p. 516) comprised 12 interviewees, 11 of whom were ‘AFAB’ (assigned female at birth), and one ‘AMAB’ (assigned male at birth). Three were cisgender, three non-binary, two transmasculine, one each agender, genderfluid, genderqueer, transfeminine. Six were queer, three pansexual, one each asexual, bisexual, lesbian. Mohamed and Hunter’s (2019) study comprised solely transgender women, exploring their beliefs about menopause and hormone therapy (HT).
Six were mixed studies. Paine et al.’s (2019) study of sexual changes in midlife comprised 16 ‘straight’ couples and 16 lesbian couples. Ussher et al.’s (2019) article on sex and the menopausal woman drew upon two studies, one of which comprised 17 heterosexual women and five lesbians. Kruk et al.’s (2021) study on feelings about menstruation cessation. comprised 97% heterosexual women and 3% ‘sexual minority women’. Sang et al.’s (2021) study of ‘the lived experiences of those who experience menstruation, menopause, and gynaecological health conditions while working in higher education’ (p. 1955) comprised 627 participants, 11 of whom (2%) identified as queer, agender, non-binary or as men. However, the findings were not analysed by sexual identity or gender identity. De Boer’s (2023) study examining women’s sexual identity work during menopause comprised 11 participants, seven of whom ‘sexually preferred’ men, one who ‘sexually preferred both men and women’; one who ‘sexually preferred’ women; and one ‘sexually preferred’ men, but ‘indicated that she was open to all people’ (p. 6). The profile of the eleventh participant was not reported and the findings were not reported/analysed according to sexual identity nor gender identity. The Women and Equalities Committee’s (WEC, 2022b) survey on the impact of the menopause in the workplace and beyond comprised 82% of participants whose gender identity was the same as their sex registered at birth while 0.2% reported their gender identity was not the same as their sex as registered at birth and 2%. 16% of respondents preferred not to say/did not respond. Sexual identity was not reported.
Most of the studies reported on either participants’ sexual identity or their gender identity but not both. Wingo et al. (2018), Paine et al. (2019) and Glyde (2023) reported on both sexual identity and gender identity. Mohamed and Hunter (2019), van Dijk et al. (2019), Kruk et al. (2012), Sang et al. (2021) and the Women and Equalities Committee (WEC, 2022b) reported on gender identity but not sexual identity. De Boer (2023) reported on sexual identity but not gender identity. Ussher et al. (2015) reported on sexual identity but not gender identity in one of the two studies analysed and reported on neither sexual identity nor gender identity in the other study analysed.
The identified studies offer very limited insights on LGBTQ+ experiences of the menopause. There was some suggestion that lesbian same-sex sexual activity, relationship- and communication styles might act as a buffer to issues associated with reduced sexual desire and/or vaginal lubrication (Paine et al., 2019; Ussher et al., 2015; Wingo et al., 2018; Women and Equalities Committee (WEC), 2022b). This echoes Winterich’s (2003) earlier study of heterosexual and lesbian women’s accounts about sex after menopause (which suggested that heterosexual women were ‘more constrained by cultural ideas about menopause, gender and heterosexuality’, less likely than lesbians to talk openly about sex and about their desires, and more likely to experience menopause-related sexual difficulties). It also resonates with Kelly’s (2005) study, which suggested that some lesbian identities might act as buffers to internalised gendered ageism. This needs to be better understood in relation to other research which suggests lesbians experience earlier onset and comparatively worse symptoms (Everett et al., 2021).
It was also suggested that ‘sexual minority women’ might experience less of a sense of loss and fewer concerns about femininity than heterosexual women (Kruk et al., 2021). However this was undifferentiated by different minority sexualities and conflicts with earlier research which suggested that lesbians experienced greater grief/loss associated with the menopause than heterosexual women (Hyde et al., 2011).
Non-binary individuals reported feeling excluded from menopause discussions (Glyde, 2023; Women and Equalities Committee (WEC), 2022b). Mohamed and Hunter (2019) reported that the transgender women in their study did not consider the menopause to be relevant to them. However, Glyde’s (2023: 524) study found that some trans and gender non-binary people do think it is relevant and are concerned about a lack of knowledge and information about ‘queer menopause’.
Several studies were tokenistic in their inclusion of LGBTQ+ issues, either including LGBTQ+ people in their sample (often in small numbers) but then not analysing data by sexual identity/gender identity, or only mentioning them in passing. The UK Women and Equalities Committee (WEC, 2022b) report on its survey of over 2000 women in relation to their experiences of menopause in the workplace, claimed it included LGBTQ+ people. However it only provided data on transgender status, but not sexual identity. It included a single quote from a lesbian and two quotes from gender non-binary individuals, and its survey findings were not discussed in relation to either sexual or gender identity.
Discussion
Limitations
The review was conducted by a single researcher and may have been informed by her particular standpoint (white, lesbian, older woman, intersectional feminist, social gerontologist, socio-legal scholar). The review did not examine the full spectrum of menopause studies (e.g. clinical, bio-medical) and it is possible that such studies may have included an LGBTQ+ sample. However, it is unlikely, as they tend not to profile sexual/gender identity in their demographics. Some studies with transgender women and men and gender non-binary people may not have been identified, if the language of ‘menopause’ was not used in those studies (Cheung et al., 2023; Mohamed and Hunter, 2019). The evidence solely comes from wealthy nations and may have limited implications globally, especially as so many LGBTQ+ people remain legally, politically and structurally oppressed around the world.
Results implications
The results support the concerns which have been raised about the paucity of research on LGBTQ+ experiences of the menopause. There are, first and foremost, strikingly few studies on LGBTQ+ experiences of the menopause. The narratives of cis bisexual women are particularly obscured in the selected studies, either not being mentioned at all or conflated, as is so often the case, with those of cis lesbians (as in, e.g. Kruk et al.’s (2021) study of ‘sexual minority’ women). The significance (or not) of menopause and menopause discourse for transgender people remains open to question, with competing narratives. For example while some research suggests trans women consider symptoms associated with reductions in gender-affirming hormones (generally for clinical reasons), to constitute the menopause (Glyde, 2023) other research indicates that for trans women ‘menopause was generally not considered to be particularly relevant’ (Mohamed and Hunter, 2019: 105). Similarly, for trans men, changes associated with gender-affirming hormone treatment may be more likely to be associated with adolescence/puberty rather than the menopause (Toze and Westwood, in press).
The comparative lack of research about LGBTQ+ issues is located within current heteronormative, cisnormative and binary-based constructions of the menopause. While the literature on other aspects of intersections relating to the menopause is expanding, there remains a dearth of literature in relation to minority sexualities and minority gender identities. This is inequitable (Fish et al., 2021). There needs to be much more research conducted on how those with non-heterosexual and non-cisgender identities experience and navigate the menopause, so that their respective issues and concerns can be understood and addressed.
The rhetorical silencing about LGBTQ+ issues also means that concepts and theories about the social contexts of the menopause are presently only partial ones. As Throsby and Roberts (2024) observe,
. . . the dominant historical framing of menopause has led to a research focus on cohorts of white heterosexual cisgendered women with teenage or adult children. . . If we want to understand the impacts of menopause both within and outside of the workplace. . . we need to widen the research frame and ask new questions about menopause as a mid-life, generative process. (23)
Achieving a better understanding of LGBTQ+ menopause experiences will not only benefit LGBTQ+ people. It will also support wider and more nuanced understandings of the menopause, its contexts, and its meanings, and broader understandings of menopause-related issues. The ‘postcode lottery’ of access to HRT experienced by many cisgender menopausal women (Iacobucci, 2022), for example, has parallels with the ‘postcode lottery’ of access to gender-affirming hormone therapy among trans people (Cheung et al., 2023; Oktaba et al., 2023; Toze, 2020). Similarly, the positive impacts of menopause for both trans men and some cis women also offer the opportunity to understand menopause beyond narratives of decline to those of freedom and liberation (Throsby and Roberts, 2024). It is therefore essential to expand normative understandings of menopause (Crawford et al., 2021; Glyde, 2022a, 2022b, 2023; Jack et al., 2021; Throsby and Roberts, 2024).
In terms of health and healthcare, LGBTQ+ healthcare disadvantages are now well-recognised. LGBTQ+ people experience worse physical and mental health, primarily caused by minority stress (Frost and Meyer, 2023), and greater healthcare dissatisfaction than heterosexual and/or cisgender people (Fish et al., 2021; McDermott et al., 2021; McNeill et al., 2023; Zeeman et al., 2019; Westwood et al., 2020). We know that reproductive healthcare is problematic for cis lesbians and bisexual women (Everett et al., 2021), where they face barriers associated with their respective sexual identities, and for transgender women and men and gender non-binary individuals (Norris and Borneskog, 2022; Rodriguez-Wallberg et al., 2023), where they face barriers associated with their respective gender identities. As Mohamed and Hunter (2019: 100) have observed, there are ‘gaps in knowledge about transgender health within the UK medical system, with few specialists in the area and reports of transgender people feeling dissatisfied’ particularly in relation to gender-affirming treatment and support.
What we do not yet know, as this review has highlighted, is how these inequities apply in relation to menopause healthcare. This is especially important as recent studies have suggested that cis women with pre-existing physical and mental health problems are more likely to experience worse symptoms and greater distress than cis women who do not have these pre-existing conditions (MacGregor, 2018; Mollard et al., 2018; Perich and Ussher, 2022; Stute et al., 2020). Given that research already indicates that cis lesbians and bisexual woman, have comparatively worse physical and mental health than cis heterosexual women, and that transgender and gender non-binary individuals have comparatively worse physical and mental health than cisgender individuals, LGBTQ+ people could be more likely to be negatively affected by the menopause. There may be mitigating factors, such as the buffering impact of reciprocal support among lesbian couples suggested by the studies identified in this review, and also that for some trans people – trans men, for example – the menopause (which they may not even call the menopause) may be a time of liberation, self-determination and even a new adolescence associated with gender identity affirmative bio-medical and/or legal interventions (Glyde, 2023). We simply do not yet know or understand sufficiently well how the physical and/or mental wellbeing of LGBTQ+ people – across all the various sub-groups – is affected by the menopause.
With increasing demands for LGBTQ+ health equity in many parts of the world, particularly where LGBTQ+ people are legally entitled to equality in healthcare delivery, LGBTQ+ people will be looking to see whether healthcare services are LGBTQ+-inclusive (Kenner et al., 2023; Rullo and Faubion, 2017), and this includes menopause healthcare provision. If those services are neither aware of, nor understand, LGBTQ+ needs issues and concerns in relation to the menopause it is unlikely they will deliver LGBTQ+-inclusive care and support. It is essential, therefore, that research is conducted which can inform healthcare providers in their provision of services to LGBTQ+ patients. It is also important providers understand these issues within regulatory frameworks, that is, healthcare laws, healthcare professional regulations, equality and human rights laws, and health and social care policies, in order to ensure compliance with them.
With regards to employment, despite the increase in inclusive workplaces in some parts of the world, LGBTQ+ people continue to face discrimination, exclusion and barriers at work (Mara et al., 2021; Stonewall, 2018). It is important to understand this in relation to menopause in the workplace and in relation to menopause workplace support. Concerns about LGBTQ+-related discrimination on top of menopause discrimination may pose additional barriers for some LGBTQ+ people in seeking menopause support at work. As the International Menopause Work Consortium (2022) has observed, this also intersects across employment contexts: ‘[c]are should be taken when generalising LGBTQI+ experiences across different types of work such as professional and entry level work’ (para 34). It is again important to understand these issues within regulatory frameworks, that is, employment laws, health and safety laws, equality and human rights laws and social policies.
Research agenda
To address the knowledge gaps identified in this review, the following research agenda is proposed:
Mainstream menopause research should routinely include representative samples of LGBTQ+ individuals, and include an analysis of sexual and gender identity in its findings.
There should be dedicated LGBTQ+ research on the menopause, its experience, and healthcare and workplace support.
Dedicated LGBTQ+ research should differentiate between the experiences of lesbian, gay, bisexual, transgender and gender non-binary/genderfluid individuals and individuals of other sexual/gender identities.
Key questions which need to be answered include:
a. Health, well-being and relationships
i. How and in what way is sexual identity relevant to the age of menopause onset, the type and severity of menopause-related symptoms, and the health, well-being and relationships of (a) lesbians, (b) bisexual individuals and (c) individual with other minority sexual identities? ii. How, in what way and with what contingencies is the concept/language of ‘menopause’ relevant to/for (a) trans women, (b) trans men, (c) gender non-binary/gender fluid individuals and (d) those with other minority gender identities? iii. Where applicable, how and in what way are minority gender identities relevant in relation to the age of menopause onset, the type and severity of menopause-related symptoms, and the health, well-being and relationships of (a) trans women, (b) trans men, (c) gender non-binary/gender fluid individuals and (vd) those with other minority gender identities?
b. Menopause healthcare
i. How and in what way is sexual identity relevant to the menopause healthcare experiences of (a) lesbians, (b) bisexual individuals and (c) individual with other minority sexual identities? ii. How does/would good menopause healthcare support look like for people with minority sexual identities? iii. Where applicable, how is gender identity relevant to the menopause healthcare experiences of (a) trans women, (b) trans men, (c) gender non-binary/gender fluid individuals and (d) those with other minority gender identities? iv. How does/would good menopause healthcare support look like for people with minority gender identities? v. What are the regulatory (e.g. non-discrimination, health equity, patient rights, etc.) implications of LGBTQ+ experiences of menopause healthcare support?
c. Menopause in the workplace
i. How and in what way is sexual identity relevant to menopause in the workplace with regards to (a) lesbians, (b) bisexual individuals and (c) individual with other minority sexual identities? ii. How does/would good workplace menopause support look like for people with minority sexual identities? iii. How and in what way is gender identity relevant to menopause in the workplace, with regards to (a) trans women, (b) trans men, (c) gender non-binary/gender fluid individuals and (d) those with other minority gender identities? iv. How does/would good workplace menopause support look like for people with minority gender identities? v. What are the regulatory (e.g. non-discrimination, employee rights, health and safety, etc.) implications of LGBTQ+ experiences of menopause in the workplace?
d. Comparing sexualities, gender identities and their intersections
i. How do the menopause experiences of cis lesbian, gay, bisexual and other sexuality minority women menopause compare with those of cis heterosexual women? ii. Where applicable, how do transgender, gender non-binary and other gender minority individuals’ menopause experiences compare with those of cis heterosexual women? How does this compare between (a) heterosexual and (b) sexual minority transgender, gender non-binary and other gender minority individuals? iii. Where applicable, how do transgender, gender non-binary and other gender minority individuals’ menopause experiences compare with those of cis lesbian, gay, bisexual and other sexuality minority women? How does this compare between (a) heterosexual and (b) sexual minority transgender, gender non-binary and other gender minority individuals? iv. What do these insights offer conceptual and theoretical framings of sexual and/or gender identity and the menopause?
Research measures should not presume heterosexuality or cisgender identities. For example, the Female Sexual Functioning Index (FSFI) is often used to measure sexual functioning, including in relation to the menopause. The scale is presently framed in relation to heterosexual sexual function, referring to ‘penetration’ and male sexual partners. It should be adapted to reflect non-penetrative same sex-sexual activities and female sexual partners as well (Everett et al., 2021).
All research on LGBTQ+ experiences of the menopause should be intersectional. There should be differentiation among the L, the G, the B, the T and the Q+ to avoid the conflation of diverse issues into one homogenised ‘LGBTQ+’ whole (Westwood, 2020). It is also important to recognise diversity within a sub-group. For example, there is great diversity among and between current cohorts of ageing lesbians and gay women particularly in terms of when and how they engaged with a lesbian/gay identity (Traies, 2016; Westwood, 2013, 2016). At the same time, it is also important to consider overlaps between sub-groups. For example, there is a significant overlap between bisexual and transgender identities (Jen and Jones, 2019). The different meanings and understandings of menopause among trans women, trans men, gender non-binary and other gender minority should be explored, including how this varies according to sexual identity (Vincent, 2020). Across all these issues other intersections – including race/ethnicity, disability and socioeconomic status – must be addressed.
Conclusion
This review has highlighted the paucity of research on LGBTQ+ experiences of the menopause and menopause support. As Cahn et al. (2024) have observed, advocacy for menopause equity requires considering justice for all people impacted by the menopause not only heterosexual cisgender women. It is essential that the wide range of knowledge gaps identified in this article are addressed to ensure that understanding and responding to menopause-related issues encompasses the needs and concerns of all who are affected. It is to be hoped that the research agenda proposed in this article will serve as a launch pad for more inclusive and diversity-responsive menopause research, healthcare and support in the future.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.