
Abstract
The lived experiences of higher-weight people vary; homogenous samples may fail to capture this diversity. This study develops an in-depth understanding of the lived experiences of higher-weight (Body Mass Index ⩾ 30) older adults (⩾60 years of age) in a Canadian Atlantic province. Participants (n = 11) were interviewed face-to-face using a semi-structured interview guide twice at 2-to-3-month intervals regarding their perceived treatment in social and health situations; how positive and negative healthcare experiences affected their health, lifestyles and healthcare seeking-behaviour; and recommendations in terms of patient experiences, access and inclusion. Participants infrequently reported negative experiences; however, participants’ experiences were informed by uptake of moralistic, neoliberal discourses. Thematic content analysis identified two major themes: active citizenship (participants demonstrated internalisation of the imperative for weight loss, healthy lifestyles and active ageing) and bright-siding (participants expressed that a positive attitude could prevent/help cope with stigma). Results suggest that individualistic, rather than collective, political solutions to health and stigma have been taken up by higher-weight older adults in a Canadian Atlantic province, which may hinder attempts at structural reforms addressing stigma.
Introduction
Weight stigma is pervasive and associated with deleterious health outcomes (Chrisler and Barney, 2017; Puhl et al., 2008a, 2008b; Puhl and Heuer, 2010). Age-based stigmatisation is similarly associated with negative outcomes (Browning et al., 2020; Ebor et al., 2020; Hu et al., 2021). Growing evidence suggests there are racialised, classed, age, and gender-based differences in the experience of weight-based stigma (Decker et al., 2018; Himmelstein et al., 2017; Reece, 2019; Turan et al., 2019). While health and popular discourses concerning ‘obesity’ 1 often reconstitute gendered, racialised, and classist stereotypes (Crawford, 2006; LeBesco, 2004; Poudrier, 2007; Strings, 2019), there are gaps in understanding experiences of living at a higher weight and the internalisation of weight stigma among different populations (Himmelstein et al., 2017). Considering its pervasiveness, more qualitative research, diverse samples, and intersectional research on weight stigma is needed (Crenshaw, 1991; Himmelstein et al., 2017), including research incorporating higher-weight older adults. Similarly, to understand embodiment and combat stigmas affecting older adults, diversity, intersectionality, and multiple forms of marginalisation among older adults must be appreciated (Clarke and Korotchenko, 2011; Kum, 2017).
According to a 2013 nationally representative survey, the most common forms of self-reported, everyday discrimination among Canadian adults were based on race, gender, age, and other physical characteristics, followed by weight-based discrimination (Godley, 2018). Each one-point increase in Body Mass Index (BMI) increased the risk of experiencing any form of discrimination by 4% and the risk of experiencing weight discrimination by 23%. For those participants who reported another form of discrimination, weight and age were common forms of secondary discrimination, and weight and age-based discrimination overlapped (Godley, 2018).
This analysis is part of a larger project on the lived experiences of diverse and multiply-disadvantaged, higher-weight populations in a Canadian Atlantic province. This analysis focuses on the older adult subsample. Participants were interviewed twice regarding their treatment in social and health situations, effects of this treatment, and recommendations for health and inclusion. Participants infrequently reported negative experiences; however, they reproduced discourses emphasising neoliberal ideologies, including personal responsibility for health outcomes and remediation of stigma through individual positivity rather than politicised advocacy, which may have implications for addressing stigma through structural reforms.
Background
Critical weight studies
Critical weight scholars examine the science underlying ‘obesity’ epidemic discourse while exploring how this discourse affects individuals’ subjectivities and embodied, lived experiences (Bombak, 2014). The medicalisation of fatness into ‘obesity’ erases how fatness complexly affects health and instead reproduces simplistic notions of over-eating and laziness leading to bodies straining individuals’ and systems’ wellbeing (Bacon and Aphramor, 2011; Campos, 2011; Gard and Wright, 2005; Lupton, 2018). While fatness is frequently framed as unequivocally unhealthy (Kwan and Graves, 2013), there is uncertainty and inconsistencies in the ‘obesity’ literature often labelled ‘paradoxes’ (Lavie et al., 2016; Liu et al., 2020; McAuley and Blair, 2011). These paradoxes include individuals labelled ‘overweight’ on the BMI index having reduced mortality risk compared to those labelled ‘normal’ weight, individuals labelled ‘obese’ with certain conditions surviving longer than ‘normal weight’ counterparts, the substantial portion of ‘normal weight’ individuals with cardiometabolic risk and the large portion of ‘overweight’ and ‘obese’ individuals without said risk, and the important role of cardiorespiratory fitness in reducing the mortality risk associated with ‘obesity’ (Bacon and Aphramor, 2011; Flegal et al., 2013; Lavie et al., 2016; McAuley and Blair, 2011; Tomiyama et al., 2016).
Debates persist over the legitimacy of these paradoxes, their mechanisms, and whether they are merely methodological artefacts (e.g. Braun et al., 2015; Peeters, 2018; Stevens et al., 2015). However, there is increasing scientific recognition that these ‘paradoxes’ are persistently identified, and that weight research has frequently been characterised by assumptions, presumptions, and myths (Casazza et al., 2013; Hebert et al., 2013). Moreover, weight loss attempts result in pronounced homeostatic processes (Rosenbaum and Foster, 2023), which contribute to the low likelihood of sustainably losing weight (Mann et al., 2007). The potential harms of weight loss dieting, including perpetuating weight stigma; social justice concerns; and the mental, physical, and behavioural health benefits that can be achieved through non-dieting approaches have inspired a weight-neutral approach to health (Bacon and Aphramor, 2011; Bombak et al., 2019a, 2019b; Ingraham, 2021; Tylka et al., 2014).
The popular messaging that fatness is deadly and unsightly (Kwan and Graves, 2013), and a matter of personal responsibility, helps to generate weight stigma (Puhl and Heuer, 2010). This perpetuation of sizeism occurs within a neoliberal public health landscape that imposes responsibility on individuals for monitoring and mastering their health (Bell, 2017; Crawford, 1980, 2006; Lupton, 1995; Petersen and Lupton, 1996). As defined by Petersen and Lupton (1996), neoliberalism constructs individuals as ‘atomistic, rational agents whose existence and interests are prior to society’, and expresses ‘scepticism about the capacities of political authorities to properly govern; vigilance over attempts of such authorities to govern; [and] an emphasis on markets over planning as regulators of economic activity’ (p. 10). Charging individuals with personal responsibility for health was ‘particularly effective in establishing the “common sense” of neoliberalism’s essential tenets (Crawford, 2006, p. 410, emphasis in original). Individuals’ own lifestyles and lack of discipline are thereby perceived as especially dangerous to their health (Bell, 2017). Crawford (1980) termed this medicalisation and moralisation of lifestyle, ‘healthism’. Health and its pursuit have become an ‘unassailable’ (Bell, 2017) ‘supervalue’ (Crawford, 2006, p. 410), loaded with moral significance.
As Crawford (2006) states, people come to define themselves in part by how well they succeed or fail in adopting healthy practices and by the qualities of character or personality believed to support healthy behaviors. They assess others by the same criteria (p. 402)
One’s weight is a visible means through which these character qualities, particularly that of self-control, are assessed (Crawford, 2006), and a focus on ‘obesity’ can shift attention from social determinants of health and health inequities (Medvedyuk et al., 2018; Monaghan et al., 2022).
Weight stigma is prevalent in interpersonal encounters, mass media depictions, and inequities in employment and education (Puhl et al., 2008a, 2008b, 2016; Puhl and Heuer, 2010). Weight stigmatisation is frequently experienced in healthcare contexts (Puhl et al., 2008a, 2008b, 2016; Puhl and Heuer, 2010) and can include weight-centric dismissal of patient concerns, spending less time with patients, discriminatory communication, and ill-fitting equipment (Chrisler and Barney, 2017; Pausé, 2014a; Puhl and Heuer, 2010). In a 2013, nationally representative survey, 6.4% of Canadian adults reported experiencing weight discrimination in healthcare contexts (Gupta et al., 2020). Experiencing weight stigma has been linked to numerous health problems including healthcare avoidance, poor psychological outcomes, biological stress, and cardiovascular issues (Puhl and Heuer, 2010; Udo et al., 2016; Vadiveloo and Mattei, 2017). Importantly, weight stigma must be considered alongside other forms of marginalisation, including ageism (Himmelstein et al., 2017; Pausé, 2014b).
Ageism and Sizeism
Like weight stigma, ageism, stereotyping and discrimination based on age and related policies, is associated with negative outcomes (Browning et al., 2020; Ebor et al., 2020; Hu et al., 2021). For example, among patients undergoing cosmetic procedures, experiences of perceived ageism were associated with lower self-esteem, lower self-rated health, and greater anticipated age-based discrimination (Pearl and Percec, 2019). Age discrimination in healthcare is also associated with new or worsened disability among Americans over the age of 50 (Rogers et al., 2015). The social devaluation of older adults became especially apparent during the COVID-19 pandemic (Berridge and Hooyman, 2020; Lebrasseur et al., 2021). However, apocalyptic demography, popular alarm regarding an expensive ageing population, has circulated for decades compelling individuals to age ‘actively’ to reduce system strain (Gee and Gutman, 2000; Rozanova, 2006; Rozanova et al., 2006; Rozanova, 2010).
In addition to thin idealization, the aging female body carries with it its own stigma (Chrisler, 2011; Clarke and Korotchenko, 2011). Older women describe somewhat less fixation on thinness than younger women but still display high levels of body dissatisfaction (Clarke and Korotchenko, 2011; Grippo and Hill, 2008; Pruis and Janowsky, 2010). Weight gain was previously thought to be a natural consequence of ageing, but such ‘licence’ has diminished over time (Veit, 2011). This may be particularly damaging to cis-gender women who experience involuntary changes in fat distribution (more fat around the mid-section) as they age or have children (Wells et al., 2010). While gaining weight may be particularly objectionable among older women, weight-related concerns pre-dated older age (Cameron et al., 2019). Qualitative research with older women suggests a conflation of health, youth, and appearance norms; youth and beauty equate to health, and health and thinness are interrelated. While one American study found younger women experienced and internalised more weight stigma (Himmelstein et al., 2017), body-image related issues generally appear to persist over the life course, even as some older women accept an ageing appearance as natural (Cameron et al., 2019). This is unsurprising, as individuals age within a discursive context rife with anti-ageing strategies and products (Cameron et al., 2019). Body dissatisfaction is also not uncommon among older men (Clarke and Korotchenko, 2011). Although compared with women, dissatisfaction among men may be more linked to muscularity than weight and more to functioning than appearance (Clarke and Korotchenko, 2011).
Despite the pervasiveness of anti-ageing and weight-loss discourses, appearance-modifications may not have the same social effects across the life course. Losing weight in later age may not be as valorised as doing so when young. The time for fulfilling certain social roles associated with thinness, heteronormative romance and biological reproduction, are thought to have passed (Weber, 2012). Furthermore, the gains in attractiveness that weight loss is meant to confer are thought to be cancelled out by sagging flesh (Weber, 2012).
The present study seeks to explore the experiences of those who may be especially affected by multiple, intersecting forms of stigma: higher-weight, older adults in an Atlantic Canadian province coping with considerable health inequities (Wang et al., 2016), including a declining, ageing, substantially rural population (Statistics Canada, 2011, 2017a, 2017b). While data collection was proceeding, the province was designated the poorest in Canada (Jones, 2019). The ageing population and poverty are leading to increases in cardiometabolic disease (Gupta, 2017). Qualitative work has illuminated pejorative social understandings of food and fatness in Atlantic and rural Canada (Beagan et al., 2015; McPhail, 2013; McPhail et al., 2013); however, the experience of being at a higher weight in these contexts is under-explored.
Methods
This analysis reports specifically on data from the older adult subsample (aged ⩾ 60 years) (n = 11) of a larger multi-sited micro-ethnography that explores the lived experiences of diverse higher-weight (ever had a BMI ⩾ 30) adults (n = 55) in an Atlantic Canadian province. Micro-ethnographies often involve multiple sites and shorter, focussed fieldwork than traditional ethnographic fieldwork (Bryman, 2012; Wolcott, 1990). A more problem-oriented and precise investigation of meaning-making is undertaken (LeCompte and Schensul, 2008; Wolcott, 1990), which reflects larger shifts in ethnography away from focussing on the holism of a culture (Marcus, 1998; Rabinow et al., 2008). In multi-sited ethnography, the ethnographer maps an object of study that emerges during research (Marcus, 1995). Deploying the multi-sited ethnographic technique of ‘following the people’ (Marcus, 1995), we visited multiple sites identified by participants as relevant to their lived experience across the province. Prior to data collection, the University of New Brunswick Research Ethics Board (REB File Number: 2019-035) reviewed and approved the study, and participants provided written informed consent.
We are critical of pathologizing fatness as ‘obesity’ (Meadows and Daníelsdóttir, 2016), and we recognise BMI is a clinically problematic measure (Hebert et al., 2013). However, we used BMI and the phrase ‘ever labelled obese’ in recruitment. We were interested in participants’ experiences in healthcare regarding weight including the pathologisation of weight, and it is unlikely one body-size relevant term would appeal to all participants (Meadows and Daníelsdóttir, 2016). Obvious obfuscations can generate suspicion, confusion, offence, and make fatness hyper-visible and shameful (Bombak et al., 2019a, 2019b; Warin and Gunson, 2013). During interviews, interviewers did not say ‘obesity’/‘obese’ unless they were mirroring participants. Apart from inclusion criteria, study materials used the term ‘higher-weight’.
Participants (see Table 1 for demographic characteristics) were recruited from radio and newspaper advertisements, posters, social media, email lists, and snowball sampling. This analysis is limited by the entirely White older adult subsample (although the larger study sample is racially diverse). This reflects the demographics of the region. Only 3.4% of the province’s population identified as a visible minority in the 2016 census (Statistics Canada, 2017c). Racial homogeneity prevents us from capturing potential racial differences and intersectional effects of racialised, weight-based, and aged-based forms of oppression. This is particularly relevant given the gaps in intersectional and racially diverse research in critical weight and stigma scholarship (Himmelstein et al., 2017; Pausé, 2014b).
Participant demographic characteristics.
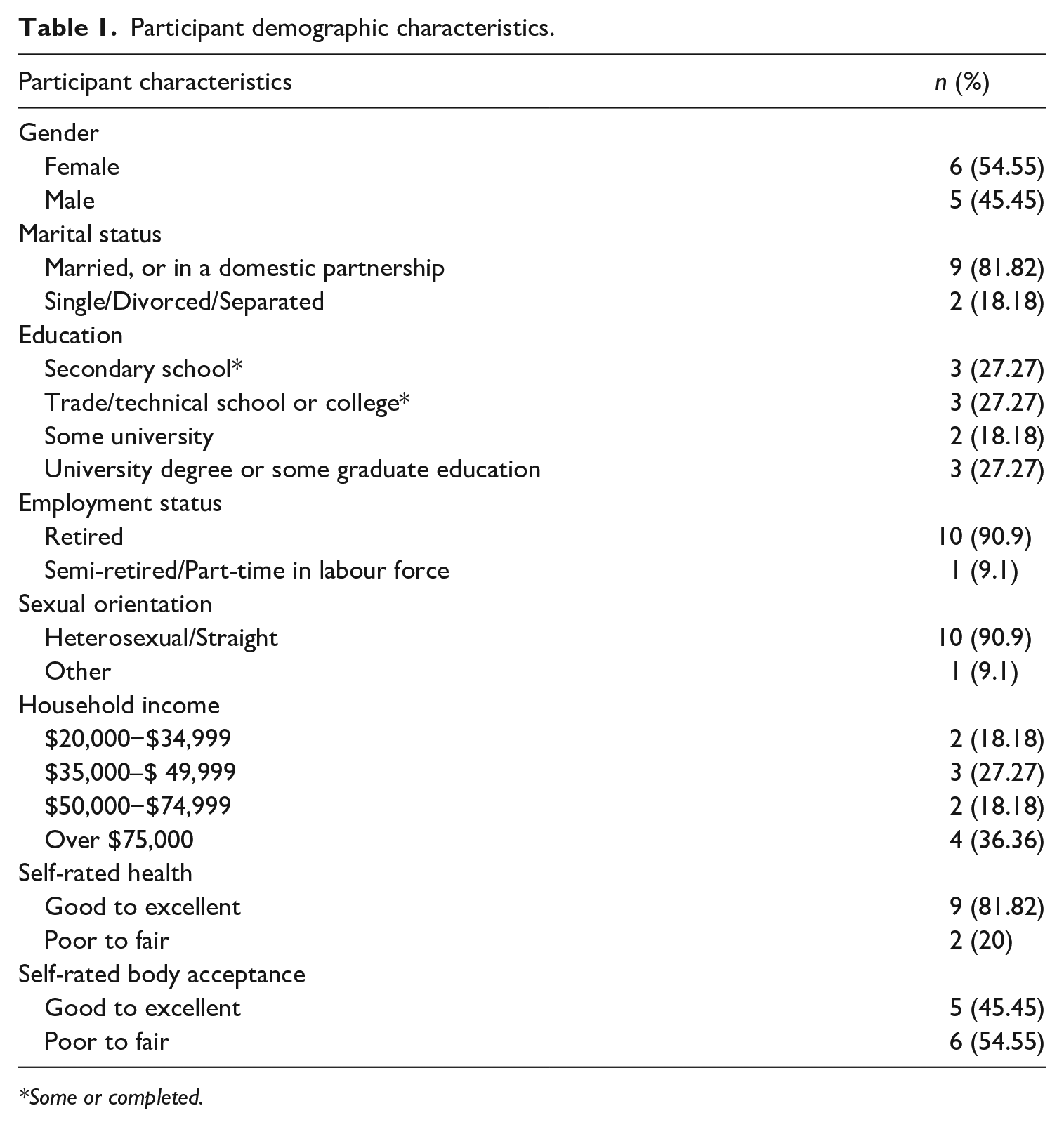
Some or completed.
The age range of the sample was 60–75 years of age. Participants were interviewed twice at 2-to-3-month intervals in 2019. Interviewers accompanied each participant to a public site identified as relevant to their health for observation (data to be published elsewhere). In one instance, a participant was interviewed at home because of health-related restrictions and reported insights about a space subsequently visited by the interviewer. Over the course of both interviews, participants were asked about how weight and age affected their treatment in healthcare and social contexts; positive and negative experiences in healthcare; places they felt most or least accepted; how healthcare experiences affected health, lifestyles, and healthcare seeking-behaviour; their access to healthcare and other participant-identified sites and related facilitators and barriers to accessibility; consequences of (in)accessibility/(non) inclusivity; and recommendations for the health system, accessibility, safety, and inclusion.
All participants but one completed both sets of interviews. Interviews were completed face-to-face, audio-taped, and transcribed professionally verbatim. Field notes documenting the interview process and field site observation were undertaken following each interview. Interviewers placed a particular emphasis on documenting interactions, non-verbal cues, body language, setting, appearance, and researcher biases (Emerson et al., 2011).
Thematic content analysis (Elo and Kyngäs, 2008) was applied to interview transcripts, uploaded into NVivo (QSR International) software, to identify recurring concepts, language, and meaning units in the data. Field notes provided important supplementary data on tone and emotional tenor of interviews. Rigour was ensured through multiple means (Creswell, 2007; Kaczynski et al., 2014), including documenting reflexive memos and audit trails and on-going peer-debriefing. Multiple coders reviewed each interview and summarised the analysis; any discrepancies were addressed by the lead author. Use of multiple investigators and data sources ensured investigator and data triangulation.
Results
Two main themes, active citizenship and bright-siding emerged that suggest participants had internalised an individualistic, neoliberal approach to health, weight, and stigma, and these perspectives informed their lived experiences. While negative experiences were infrequently recounted, participants frequently spoke of individuals’ role and obligation in maintaining health through limited lifestyle choices (active citizenship) and indicated their positive outlook determined their experience of stigma and capacity to cope (bright-siding). Themes were similar across genders. Themes with exemplary quotes are discussed below.
Active citizenship
Many participants were seeking to control their health and weight. Participants expressed frustration with overly simplistic understandings of weight, health, and lifestyle, which did not fully capture their experience and were frustrated by stigma, judgement, and insensitivity; however, they generally endorsed dominant views that higher-weight was damaging to health, and weight loss would be beneficial. Participant 1 was a woman who felt she was ‘rushed’ by healthcare workers as a higher-weight older woman. She was trying to lose weight but felt healthcare workers may not understand how difficult this process could be. She also described an active life as a community member, taking classes, volunteering, and playing games. She described some other older adults with whom she interacted as follows: Having seen a lot of those seniors who don’t do anything- I think it’s really important, 'cause. . . I’ve met some of them and I. . . asked what they do and what they’re involved in and they said, ‘Oh no, we just live by the beach and we enjoy the summer and in the winter we kind of hibernate’. Oh my God, that’s not a way to live. . .I think it’s important to me for all those aspects to be healthy.
In the quote above, Participant 1 reproduces the expectations placed on older adults to embody a vigorous degree of health and activity, and having a ‘purpose’, by critiquing what she perceives as her peers’ sedentary and aimless lifestyles.
While participants did describe socialising and community engagement as important, in other ways they tended to describe relatively narrow healthy lifestyles. For example, healthy food choices, according to participants drew from a very narrow selection of options, particularly, salads, which were repeatedly brought up.
Participants used morally charged language as they discussed ‘junk [food]’, ‘eat[ing] their feelings, (not) ‘doing something right’ regarding health behaviours and ‘trying very hard’.
Participant 8 was devoted to learning as much as possible about health, alternative medicine, and active transportation. He consumed large amounts of health and food related online videos and was sceptical of biomedicine. Even while describing scepticism of neoliberal tenets and noting an underfunded and inaccessible healthcare system, with respect to his own behaviours, he was self-critical. He described a desire to be more disciplined regarding his diet when asked about potential health changes: . . .just be more motivated to. . . be more strict with my diet. . .I guess that would just be the thing that I would have is be more motivated. That’s just me. That’s on me.
Above, Participant 8 directly takes responsibility for not eating ‘strict[ly]’, suggesting a personal internalisation of neoliberal health tenets, despite a more political and critical overall perspective. Similarly, Participant 11, who was hoping to lose weight and did not perceive his friends’ teasing or doctors’ exhortations to lose weight as stigma, reflected on how eating chips disrupted the ‘well[ness]’ of his eating habits.
. . .when I think I’m doing well, I’m not really doing well. You know, you think you’re doing well with your eating habits . . .Then you eat a bag of chips or something.
The moralising of food was particularly apparent in the above quotes from Participants 8 and 11. Both participants expressed their frustration with themselves when they veered off this strict path to healthy eating. Later in the interview, Participant 11 states, ‘I don’t have any, I have no food discipline, I guess’.
Participant 5 had a chronic health problem and described positive experiences in healthcare except for inaccessibility. Having quit smoking and drinking alcohol, he was currently dedicated to losing weight, which he characterised several times as a ‘battle’. He discussed exercising for 50–60 minutes every day and careful regulation of blood pressure and other biometrics, including weighing himself daily, ‘So if I go up one day, I try to balance it out the next day’.
Participant 3 did not perceive negative experiences in healthcare despite being told by a doctor after surgery that another physician was required to ‘hold [his] fat’, although he did feel ‘looked down [upon]’ more generally. He did recount stigmatising treatment experienced by his wife. He discussed his determination after his surgery to lose weight and his subsequent weight loss: I’m the type of guy . . . I was quite overweight. . . years ago, I was over 300 pound. . . I started walking at, at work. I walked every day, and every time I’d get a break I’d walk and walk. And. . . lost a lot of weight that way. . .when we came down here, I’m gaining a little bit of weight, so I thought, well, I’ve got to do something. So, I. . . bought a couple of bikes and I started biking. And, uh, I loved it.
Regarding weight loss, Participant 7, who had a chronic disease and recounted a traumatic surgical experience but otherwise ‘exceptional’ care, expressed laughingly how, ‘sitting on your fat arse doesn’t help but I do it so well’. In Participant 7’s case, this was especially interesting given the limitations imposed by her illness and her enthusiasm and dedication to physical activity. Such statements reaffirm an individual’s primary responsibility for health and body. However, participants’ admission of their own fallibility (i.e. that no one can achieve healthist standards), humour, as well as references to others’ problematic ‘obsessiveness’ regarding health behaviours, such as going to the gym every day for 2 hours, and occasional referral to genetics, or more fatalistic perspectives on disease aetiology or ageing, demonstrated participants’ capacity for resistance to healthist discourses. Similarly, participants occasionally did refer to socioeconomic or accessibility challenges that may impede someone’s capacity to follow health, weight, and ageing prescriptions. Participant 9 came from a low-income family and had frequently weight cycled. She described overt weight stigma and dismissal as an older woman in healthcare. She referenced the complexity of trying to eat a healthy diet including changing, rigid, nutritional advice and the cost of food: If you were to eat what you should be eating, just stop and think how much it is to buy a box of macaroni, compared to a head of lettuce. Go buy celery right now, you know. That was always one of those things you had in the fridge that if you got the munchies, go grab a celery stick. A little cheese whiz on it if you want to. Sometimes you couldn’t, you know it’s cheaper to go buy a big bag of potato chips and put that on the table.
Despite these challenges, she persisted in the weight-loss ‘battle’, which she characterised as a ‘constant struggle’.
In-depth discussions of cost of living occurred infrequently in interviews. Participants occasionally referenced fiscal policy when discussing healthcare, calling for more funding and incentives for healthcare workers, but others challenged the expediency of these reforms, such as Participant 10: ‘Deficits are significant and they need to be managed. And, you need to be very. . . (laughs) careful where you allocate funds and. . .what can we do?’
Moralism sometimes played out in participants’ communications with healthcare professionals. For instance, like other participants, Participant 2, a former healthcare worker who was involved in community and volunteer work, described herself as ‘active’ and had a positive relationship with her doctor, expressed doubt and exasperation throughout her interview regarding the omnipresent elision of weight and health. But she also expressed that a ‘slap in the face’ might be needed from doctors regarding weight loss: . . .then once I tell them. . . ‘I’m healthy. I know I’m overweight, but I’m still very healthy. I’m in here for, for whatever else. It has nothing to do with my weight’. I saw an orthopaedic doctor once with my knee, and he was very upfront with me and saying, ‘You need to lose a hundred and some pounds, because I’m not going to touch your knee’. And, of course, I understood that. . .Because, it was the way he said it wasn’t nice, but it was the truth, and sometimes you need that slap in the face.
While Participant 2 considered herself healthy and ‘young’ for her age, she still felt there was recourse to confrontational communication regarding her weight from healthcare providers. Participants tended to default to doctors’ presumed expertise. Critique was levelled at delivery of health information – but not necessarily substance of the messages imparted by health professionals.
Bright-siding
Similar to an individualising outlook on maintaining health, many participants frequently emphasised the importance of a positive outlook, implying that this outlook determines their lived experiences and helps them cope with their reportedly infrequent negative encounters. Some participants contrasted themselves with ‘others’ who failed to do this.
Participant 4 was trying to lose weight, coping with a chronic condition, and described herself as ‘active’. While describing previous healthcare experiences in another province as being more dismissive based on her weight, and a family member being stigmatised for age, she described only positive local healthcare experiences. She believed that her personality was the reason she did not experience negativity from others in social settings, although she did recount one insensitive weight-related joke at a family occasion: I don’t want to sound conceited in this aspect, but because of my personality . . . and the way that I deal with people and everything, I really don’t get a lot of negativity.
Further, Participant 4 implied that a positive outlook can potentially ‘keep the door closed’ to the effects of negativity including treatment from others: I find if someone is concerned about their weight and they’re putting themselves down and it’s like if you’re opening the door for negativity and you have to be positive, and if you’re positive, then you don’t get any of the negative. . . shit going on, right?
Participant 2 also attributed having a non-‘obese’ self-image to her personality and is only reminded of her stigmatised size when she sees her reflection.
I think it’s just my personality. Yeah, it’s just my personality. . . It’s really weird, but I don’t see myself as being obese until I walk in front of a mirror half naked or something.
Importantly, Participant 2 did talk about feeling that others were watching when she ate ‘garbage’ food. This feeling led her to eat in her car or at home.
. . .if I go to town, and I order a doughnut. . .or something like that, then I might feel like people are watching me and saying, ‘are you crazy?’, so, I. . . can be maybe sometimes a little bit of a closet eater. It’s like when I want that garbage I’ll stay home and eat it, or in the car when we’re going out for a drive or something. That would probably be about the only time that I feel that is when people watch what I’m eating.
Participant 2’s ‘personality’ was insufficient to compensate for her self-consciousness during public food consumption and the assumption others were watching and judging her. Personality was not effective in offering protection from feelings of self-censure when experiencing particularly weight-salient situations, such as publicly eating ‘garbage’ foods or seeing oneself naked.
During her interview, Participant 6, had a background in education and healthcare. She was hoping to lose weight, suffered from ‘physical problems’ and ‘chronic pain’, and attributed the fact that she was rarely treated poorly as an older adult to her confidence, assertiveness, and sense of entitlement to good service. She felt that stigma probably resulted from (misplaced) moral assumptions over lifestyles and may especially accrue to those who did not present as ‘well-educated’ and did not ‘assert themselves’, which was occasionally expressed by other participants. As she specified, . . .that’s what I think happens with some people . . . they kind of let people treat them badly and don’t speak up. And then, you know, they have a bad experience . . .they kind of don’t feel that confident to speak up.
Participant 6, above, contrasted her expectations and attitudes to others without her attitude and to her younger self when she didn’t feel ‘important enough’. While this approach suggests an acquired sense of self-worth, it also implies that proper treatment is predicated on individuals’ outlook, behaviour, and not being a ‘doormat’.
Participant 10, who had a chronic disease, was participating in an exercise programme and hoping to lose weight, did not describe stigmatisation in his own healthcare; however, he did describe being made aware his size was a burden to healthcare workers, healthcare workers’ impatience with his older father, and disorganisation and miscommunication among healthcare workers in his wife’s care. He attributed his non-stigmatising experiences in healthcare to his forbearance. The implication may be that others’ negative experiences were, in part, a product of their demanding attitudes.
My experiences have always been positive. I. . . can’t think of a negative experience. I’m also a very tolerant individual. Like a very patient individual. . .I don’t expect to snap my finger and. . . have somebody arrive at my beck and call.
When reflecting on their positive and negative experiences as higher-weight older adults, most participants tended to individualise such occurrences as a product of their own outlook and behaviour. By being accommodating, affirmative, and/or assertive, participants perceived themselves as inviting only positive experiences. The inverse follows then that negative, demanding, or passive individuals allowed for negativity in their lives. When all else failed, participants tended to opt to avoid stigmatising places. Participant 6 avoids public exercise for fear of judgement due to her size: I have this belief that . . . I would be judged if I’m going to the gym. . . So these are all. . .obviously pre-judgements. . . So that maybe . . . keep me from. . . doing some things . . . I still can do some things that. . . maybe other people at my weight or level couldn’t. But yeah. . .I do kind of think that way.
Discussion
How older adults in an Atlantic Canadian province described their experiences at a higher weight was captured in the following themes: active citizenship (that one’s health and weight can be controlled through lifestyle behaviours) and bright-siding (that attitude and positivity could counter stigma). Their individualist orientation to health may hinder attempts to recognise and address weight stigma as a structural social determinant of health and enact upstream reforms that could reduce stigma (Hatzenbuehler et al., 2013), and it unfairly burden individuals, such as the participants of this study.
Participants exhibited some resistance to health moralising and individualistic neoliberal discourses, such as disputing that fatness necessarily equated to unhealthiness or expressing frustration or incredulity regarding frequently changing or ever more stringent health advice. Interestingly, one participant who most frequently referenced socioeconomic issues (even when endorsing other neoliberal conceptions of weight), was one of the only participants who did not mention what we have termed a ‘bright-siding’ perspective on stigma. Instead, the participant suggested children needed to be prevented from gaining weight to prevent stigma – again, a neoliberal framing of oppression.
Taken together, these themes demonstrate how participants’ focus tends to largely discount the role of structural forces on health and lifestyles. The themes reveal an individualistic orientation with a concentration on assuming responsibility for health, abiding by expert advice, and managing the experience of negativity/stigma. While it may seem intuitive that participants shared certain generational (Baby Boomer) values, international research suggests Baby Boomers cannot be pigeon-holed with holding certain values – including regarding individualism, obligations to others, and collectivism (Airey et al., 2021; Guberman et al., 2011, 2012; Sirias et al., 2007).
Healthy dietary and activity behaviours have long been touted as an antidote to the ageing process; a process which individuals should delay, slowdown, and resist. Most participants reproduced, neoliberal, healthist, and ‘successful ageing’ discourses, which place the onus on individuals to monitor and maintain activity and health – including into old age (Bell, 2017; Crawford, 1980, 2006; Lupton, 1995; Petersen and Lupton, 1996; Rozanova, 2006; Rozanova et al., 2006; Rozanova, 2010). For participants, actions to overcome the effects of ageing included consuming the ‘right’ food/portions; engaging in physical activity; and seeking out alternative treatments, supplements, and therapies to age well. Viewing health behaviours as prophylaxis for ageing, while expressing occasional resistance to, frustration with, and ambivalence regarding health behaviour expectations is similar to other international studies (Pond et al., 2010; Spoel et al., 2012; Stephens et al., 2015). This ambivalence was evident when participants mentioned the challenges of living in a poor, rural province; affordability and inaccessibility of food, housing, transportation, healthcare, and size inclusive-clothing; and the value of free and discounted programming. Some participants contextualised these concerns when mentioning government fiscal policies, but participants held government culpable to various degrees, and these discussions were relatively limited.
Some participants contrasted their embodiment of moral, healthy citizenship with less active others, or distinguished themselves from people who did experience harmful effects from stigma because of their personal attitudes. For example, participants referenced other older adults who did not maintain themselves through diet and exercise and who may experience an acceleration into frailty and passivity (Higgs and Gilleard, 2014: 10). This process of defencive othering may be magnified by participants’ higher-weight bodies (Schwalbe et al., 2000). For higher-weight individuals, cultural pressures exist to conform to particular ‘good fatty’ behaviours and rationalities such as being active, pursing weight loss, or having a socially acceptable justification for their size (Pausé, 2015). As some participants framed themselves as fairly immune to stigma, so targets of racism may be socialised into ignoring or emotionally distancing from oppression and more politicised or ‘deviant’ others (Froyum, 2010; Wilkins, 2012). A compulsion to distinguish oneself from other, less active, positive, or health conscious higher-weight and older adults may compromise solidarity that could help in anti-stigma advocacy. Some participants suggested that there may be a class component to ‘bright-siding’ in which less educated (or those presenting as less well-educated) may be especially vulnerable to stigma due to a lack of assertiveness, entitlement, or articulation, but this would need to be studied more specifically.
Participants’ use of a ‘personality’ or similar individualist characteristics to counteract the effects of stigma align with an internalized neoliberal orientation to health and a strong North American emphasis on positive thinking, which is reinforced by positive psychology, related ‘sciences’, and industry, what Ehrenreich (2009) termed ‘bright-sid[ing]’. A normative positive ethos can reinforce victim-blaming with its focus on the controllability of emotions and subsequent outcomes (Ehrenreich, 2009). Experiencing and being emotionally affected by stigma may become invisible/objectionable in the presence of resilience discourses that ‘authenticate and idealise’ certain ‘experience[s], thinking, and feeling’ and demands the performance of certain forms of ‘self-actualising/improving’ labour (Gill and Orgad, 2018: 6). Rather than recognising conflict, oppression, power differentials, and the need for negative emotions (i.e. rage at injustice) and radical challenges to the status quo, individuals and their attitudes and thoughts are blamed for unhappiness or a lack of fulfillment (Schwarz, 2018; Yakushko and Blodgett, 2021). This apolitical, decontextualised approach can reinforce and exacerbate existing oppressions (Schwarz, 2018; Yakushko and Blodgett, 2021). It may fail to hold perpetrators of stigma to account; result in counterproductive reactions, such as avoidance or self-blame; or inhibit progressive, inclusionary reforms.
Rather than personal positivity, what is needed to ensure people of all ages and sizes are treated with respect and dignity is a weight-inclusive approach to health (Tylka et al., 2014), which would help remedy some of the frustration participants felt when healthcare providers adopted an overly reductive view of the relationship between weight and health. Weight-inclusive physical spaces, and greater representation of diverse, higher-weight bodies participating in a range of activities, including exercise, could help ameliorate some of the concerns participants expressed regarding eating and exercising publicly (Bombak et al., 2019a, 2019b; Meadows and Bombak, 2019; Pearl, 2018). A decreased focus on ‘personal responsibility’ for health in media, a shift in focus from weight to health, an elimination of biased portrayals, and greater awareness of weight stigma may also help reduce stigmatisation and shift the focus on individual responsibility for wellbeing that participants frequently reproduced (Bombak et al., 2019a, 2019b; Pearl, 2018; Tylka et al., 2014). Lastly, increased legislation and policies prohibiting discrimination/bullying founded on weight are essential social justice aims (Pearl, 2018).
Strength and limitations
This study used repeated interviews to explore the experiences of Canadian Atlantic higher-weight older adults’ experiences. Retention was high. Conducting two interviews and iterative analysis with a team of analysts, who recorded a detailed audit trail, allowed for the developing of strong rapport, investigator triangulation, and the gathering and analysis of rich data that were contextualised in the lives of participants (Creswell, 2007; Kaczynski et al., 2014; Saldaña, 2003). Furthermore, we had the means to clarify findings and emergent themes over the interviews. Although the sample was small, homogenous, and cannot allow for generalisability, the intent of the study was to gather rich, particular data within a specific locale. Nevertheless, the findings should be tested for transferability in other settings and among more racially, sexually, or ethnically diverse populations and across the gender spectrum. Indeed, this study is part of a larger study looking at experiences of higher-weight among diverse populations (older-adult, Canadian newcomers, sexual and gender minorities, lower-income Canadians and Francophones), which can help reveal convergences and differences across sociocultural, structural, and demographic subgroups.
Conclusion
In a Canadian Atlantic province, higher-weight older adults reproduced individualist neoliberal health discourses emphasising the value of positive attitudes and taking responsibility for one’s health. While participants infrequently described negative experiences, discourses that present positivity as a means of coping with stigma may ‘sugar-coat’ problematic situations, impede collective action to improve inclusivity, and reinforce moralising fragmentation of marginalised groups into responsible citizens and irresponsible others (Pausé, 2015). More radical discourses must be amplified (Bombak et al., 2019a, 2019b). Structural advances such as anti-weight discrimination legislation, which have been found to boost individuals’ affect and reduce weight internalisation (Pearl et al., 2017), are necessary and do not burden individuals with ‘grinning and bearing’ unfair treatment or disengaging from activities, people, or places out of fear of injustice.
Footnotes
Acknowledgements
The authors are grateful to participants for their engagement, to Julia Sheehan for assistance in data collection early in the project, and to Bailey George and Anne Waugh for formatting assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported an Establishment Grant awarded to AB from the New Brunswick Health Research Foundation and a Banting Discovery Award awarded to AB.