
Abstract
This article contributes to social health research by presenting an analysis of the temporal dimensions of the “good” doctor-patient relationship as perceived and enacted by patients and general practitioners (GPs). The empirical data derive from ethnographic fieldwork comprising participant observation in four general practice clinics in Denmark, and semi-structured interviews with 27 patients and eight GPs. The analysis draws from Michael Flaherty’s sociology of time: notions of temporal agency and “time work” are used as analytical tools to demonstrate that the “good” doctor-patient relationship is constructed in a tension between external temporal structures and internal temporal experiences that are the result of GPs’ and patients’ agentic practices of “doing time.” Thus, the findings illustrate how temporal determinism and self-determinism are equally interwoven when GPs and patients talk about, enact and seek meaningful temporal experiences within the doctor-patient relationship, while resisting and avoiding others that undermine the relationship. The results challenge 1. deterministic conceptions of time demands in today’s healthcare systems that are said to control healthcare providers’ behavior and 2. the taken-for-granted understanding of continuity as a resource in itself.
Background
What constitutes a “good” doctor-patient relationship? In the effort to answer this question, researchers have scrutinized and specified ideal forms and components of the doctor-patient relationship, some of which have been turned into general descriptions and abstract typologies or models such as patient/person-centered medicine or relationship-centered care (Beach and Inui, 2006; Emanuel and Emanuel, 1992; Mead and Bower, 2000; Pellegrino, 2001; Stewart et al., 2003).
From a medical vantage point, studying what a “good” doctor-patient relationship is—and how it can be established, maintained and disrupted—is important since having a good relationship to one’s medical practitioner is shown to be crucial to patient well-being and health: it influences the patient to seek medical care in the first place, to disclose his/her symptoms, adhere to the prescribed biomedical treatment plan and attend treatment follow-ups (Dunn, 2019; Ridd et al., 2009). Thus, a good doctor-patient relationship has proven to have substantial albeit indirect biomedical effect on patients’ health (Mikesell, 2013). Finally, research tends to show that good doctor-patient interactions is good for physicians’ too, providing them with enhanced job satisfaction, better self-care and sense of meaningfulness (Beach and Inui, 2006; Derksen et al., 2015).
Determining the qualities attached to a good doctor-patient relationship patients’ and doctors’ perceptions of what constitutes a “good” doctor have been investigated. Several studies, conducted within Western contexts, show that from a patient perspective, a “good” doctor is someone who treats the patient with respect, as a fellow human being (“humaneness”), takes the patient seriously, listens without prejudice and provides sufficient time for information delivery and care (Anderson et al., 2007; Arborelius and Bremberg, 1992; Bensing et al., 2013; Carroll et al., 1998; Gérard et al., 2016; Wensing et al., 1998). From the doctors’ point of view, coordination -and continuity of care (mainly with patients suffering from serious and psychosocial conditions), technical expertise and knowledge along with interpersonal and communicative skills are emphasized as facilitators of a good doctor-patient relationship (Berger et al., 2020; Guthrie and Wyke, 2006; Jung et al., 1997; Ridd et al., 2006; Schers et al., 2006).
Bringing our attention to bear on the individual “desires” and “ideals” of patients and physicians in relation to the “good” doctor-patient relationship, these studies tend to ignore their temporal dimension and how the capacity of individuals to shape the doctor-patient relationship in good ways is intervowen with complex temporal structures- and logics that govern today’s healthcare delivery. Time as a concept has been central to medicine for decades, and social research has critically analyzed, for example, differences in patient/staff time conceptions (Roth, 1963), the symbolic construction and use of time in healthcare (Frankenberg, 1988) and the threats that a “time regime” presents to healthcare professionals’ work motivation and sense of meaningfulness (Balint and Norell, 1973; Deery, 2008). In recent years, the issue of time management in health care and patients’ and professionals’ responses hereto have gained much interest in academia and among practitioners. During the last decades, the healthcare systems in Western countries have experienced a steadily growing pressure to optimize their basic services and organizations of care and treatment through modernization processes that seek to rationalize and standardize work and place an economic value on time (the assumption that “time is money”) (Macbride-Stewart, 2013; Pedersen and Roelsgaard Obling, 2020). Time figures as a predominant discourse in health policy making, in the media and among clinicians themselves, for example, in macro-discourses about time efficiency and optimization through new and innovative health technologies (Sligo et al., 2017), and in calls from healthcare professionals about increased time deficiencies in patient care and high levels of stress and burnout as an individual response to environmental time constraints (Marchand and Peckham, 2017; Nettleton et al., 2008; Pedersen et al., 2021; Siegrist et al., 2010).
In a general practice setting, increased demand for primary care worldwide has created concern among primary care physicians about the impact of shorter consultation length on patient healthcare and physician workload and stress (Irving et al., 2017; Macbride-Stewart, 2013; Mercer et al., 2002; Osborn et al., 2015). Research shows that the pervasiveness of the institutional logics of efficiency influences patients’ health care seeking with patients being concerned about wasting the GP’s time in a primary care context of constrained resources and government calls for cautious healthcare spending (Andersen and Vedsted, 2015; Llanwarne et al., 2017). Furthermore, doctors’ moral judgments about the appropriateness of patients’ health service use creates a pressure on consulting appropriately or legitimizing the patient’s decision to consult (Cromme et al., 2016; Llanwarne et al., 2017).
The conceptual framework in relation to time of the above research leads us to think about time in terms of deterministic causation, focusing on what (lack of) time does to us and not what we do with time, hereby ignoring the agentic practices of patients and health care professionals to shape their own and each other’s temporal experiences. Notable exceptions can be found in research investigating the interrelationship between “real time” (clock time) in consultations, patient-perceived time (how time is felt by patients) and level of patient satisfaction with consultation length (Cape, 2002; Ogden et al., 2004; Pollock and Grime, 2002). One study shows that there is a discrepancy between actual consultation time length (clock time) and patients’ estimations of consultation duration (perceived time) and that patient preferences for more consultation time is correlated with dissatisfaction with the emotional aspects of the consultation and a lower compliance rate (Cape, 2002). This research suggests that an investigation of what constitutes a “good” doctor-patient relationship can be insightfully approached by analyzing the interrelationship between how time is spent in the doctor-patient relationship and temporal experiences. The aim of this paper is to bring attention to the temporal dimensions of the “good” doctor-patient relationship as perceived and enacted by patients and general practitioners (GPs). The subject arose from ethnographic fieldwork in a general practice context exploring what patients and GPs experience as constituting a “good” doctor-patient relationship. The time theme as inextricably linked to the perceptions and enactments of a “good” doctor-patient relationship arose during data collection and analyses of the data: experiences of how time should be spent, efforts to construct certain temporal experiences, resistance to time circumstances, etc. Flaherty’s sociological study on how human beings in everyday life strive to control and customize time through temporal agency, what he calls “time work,” was found to be resonating with the pervasiveness of time found in the data. Before continuing with Flaherty’s thoughts on temporal agency, it will be useful to look to the general practice context in Denmark as the backdrop against which the subjective temporal experiences and practices found in the data unfold.
The context of general practice in Denmark
As part of the Nordic healthcare system, general practice in Denmark aims to deliver timely and equal access to high-quality health care for the Danish population (Oxholm et al., 2022). The Danish healthcare system is financed by taxes offering almost all services free of charge to its citizens. General practice is the first access point for patients to the health care system and GPs may refer patients to another specialist treatment in the primary or secondary health care sector. About 98% of all Danish citizens are listed with a GP (in most cases of their own choosing), and a GP usually has a patient list of around 1600 patients (OECD, 2017; Pedersen et al., 2012). Over the years, demands for services in general practice in Denmark from both patients and health authorities have increased (Oxholm et al., 2022). In addition to handling pressures due to an aging population, an increase in the number of chronically ill people, and a decline in the GP workforce, GPs are expected to deliver primary prevention and to treat patients who have been early discharged from the hospitals. Moreover, recent mandatory implementation of quality- and patient safety initiatives as well as quality inspections- and controls from The Danish Patient Safety Authorities have added to feelings of pressure (Pedersen et al., 2021). The GPs work as private contractors and are remunerated by the public health authorities through a mixed capitation and fee-for-service system (Olsen et al., 2016). Standard consultation time in Denmark for routine booked appointments is 10 minutes, which is approximately half the consultation length compared to neighboring Nordic countries such as Norway, Finland and Sweden (topping with 22.5 minutes) (Irving et al., 2017).
Without consideration for the prevailing circumstances, general practice has generally been said to have a privileged position in terms of time (Jeffers and Baker, 2016). GPs are said to have abundant time in the longitudinal perspective via continuity of care as many patients are seen to return again and again to the GP as their “family doctor” (Macbride-Stewart, 2013). A large body of primary care research has investigated the significance of a continuing doctor-patient relationship, providing an extensive account of how the longitudinal continuity provides the foundations for relational qualities and for quality of care via accumulated knowledge of the patient (Gérard et al., 2016; Ridd et al., 2009; Salisbury et al., 2009). Research on the influence of time continuity on relationship-building (Baker et al., 2003; Guthrie and Wyke, 2006; Haggerty et al., 2003; Rhodes et al., 2014), suggests a certain causality between many consultations over time and the establishment of a “good” doctor-patient relationship as part of the identity building and core value set of general practice. While this relationship between longitudinal care and the “good” doctor-patient relationship thus seems well established, some studies nevertheless suggest that from the patient’s perspective, longitudinal continuity within the doctor-patient relationship is only appreciated by patients when it consists of interpersonal qualities such as trust and recognition (Frederiksen et al., 2009; Rhodes et al., 2014), indicating that a linear and sequential time allocation is only valued by patients when spent meaningfully. Flaherty’s sociology of time (Flaherty, 2011), pointing to the tight connection between time and human agency, helps toward further exploring this perspective.
Flaherty’s time conceptualizations
Flaherty argues that human beings’ relationship to time is not a passive one. Instead, on the basis of a large study in which Flaherty has scrutinized the experiential qualities of lived-time (how time is thought, seen, remembered, and felt) in hundreds of people’s narratives, he builds the argument that when relating to time, we are not passive observers of time passing by in a linear continuum, in which case time is conceived as something independent from us (Flaherty, 2011: 132). Rather, he argues, human beings’ relationship to time is based on action and reaction by active and creative agents who influence temporal experiences by “doing time” in various ways through acts of self-agency and self-determination (Flaherty, 2011: 11). This, he calls “time work” referring to all those efforts undertaken every day by people to construct their own and others’ temporal experiences, for example, speeding up time, killing it or slowing it down (Flaherty, 2003). According to Flaherty, this time work is done either to foster a valued self-identity, for example, one that spends “quality time” with the family, or to experience a sense of one’s own self-efficacy, for example, that one is in control of one’s life or uses time well. Flaherty thus takes issue with the viewpoint that time is objective, linear and unaffected by human beings’ individual intentions and interventions. Rather, he argues that time can be dealt with in various ways through one’s modes of being and therefore time exists in an alternation between something “out there” (objective time) and “in here” (subjective time), and thus as both determined by external structures and enacted through individual agentic practices and intentionalities.
Applying these time conceptualizations to the empirical data challenges the deterministic conceptions of the “objective” temporality dominating today’s healthcare system and makes us question, first, why specific temporal experiences arise in us, and second, whether these experiences are beyond our control or in fact invite us to constitute time differently.
Methods
The study
The empirical study was conducted by a team of three persons: a senior researcher together with two junior researchers (graduate students). Data generation took place through three consecutive substudies. This approach, with multiple researchers generating data within the same overall research project, was inspired by team-based ethnography which is a method for generating data at different sites within a relatively short time span (Bikker et al., 2017).
The first substudy was designed as ethnographic fieldwork conducted by the author between January and June 2019, involving participant observation and informal and formal interviews with GPs and patients. Four clinics were selected to reflect a spread of practice characteristics including practice type (group and one-man practices), geographical location (urban and rural) and patient population (a mix of ethnicity and socioeconomic backgrounds). All four clinics were situated in one out of Denmark’s five regions. Before participation in the study, the clinic personnel gave their written, informed consent. Both doctor and nurse-led consultations were observed by the author, who also spent time in lunchrooms and waiting rooms. Before each medical consultation in the clinic, the patients filled out a written consent form. Approximately 50 hours of observation were conducted, and field notes were taken during observations (DeWalt and DeWalt, 2011).
Five of the GPs in the above clinics (two women and three men, between 35 and 70 years of age) were interviewed during working hours (audio-recorded interviews with a duration of 20–30 minutes), using a semi-structured interview guide containing open-ended questions relating to their reflections on the interaction taking place in the recently observed consultations, and their general reflections on which characteristics are constitutive to the “good” doctor-patient relationship (see Table 1). Seven patients, who had been observed during consultations with the above GPs, were interviewed immediately after the consultations, and asked to reflect on the interaction taking place in the observed consultations and provide descriptions of which characteristics are constitutive of the “good” doctor-patient relationship (see Table 1). Three additional semi-structured interviews with GPs (two men and one woman, between 43 and 70 years of age) were conducted without participant observation, using the above general question concerning constitutive characteristics of the “good” doctor-patient relationship as the opening question. In selecting GPs for these interviews, variation was sought regarding GPs’ age, gender, practice type, geographical location and years of practice. The three interviews were audio-recorded and lasted from 45 to 60 minutes.
Interview guide: The “good” doctor-patient relationship in general practice: GP- and patient.
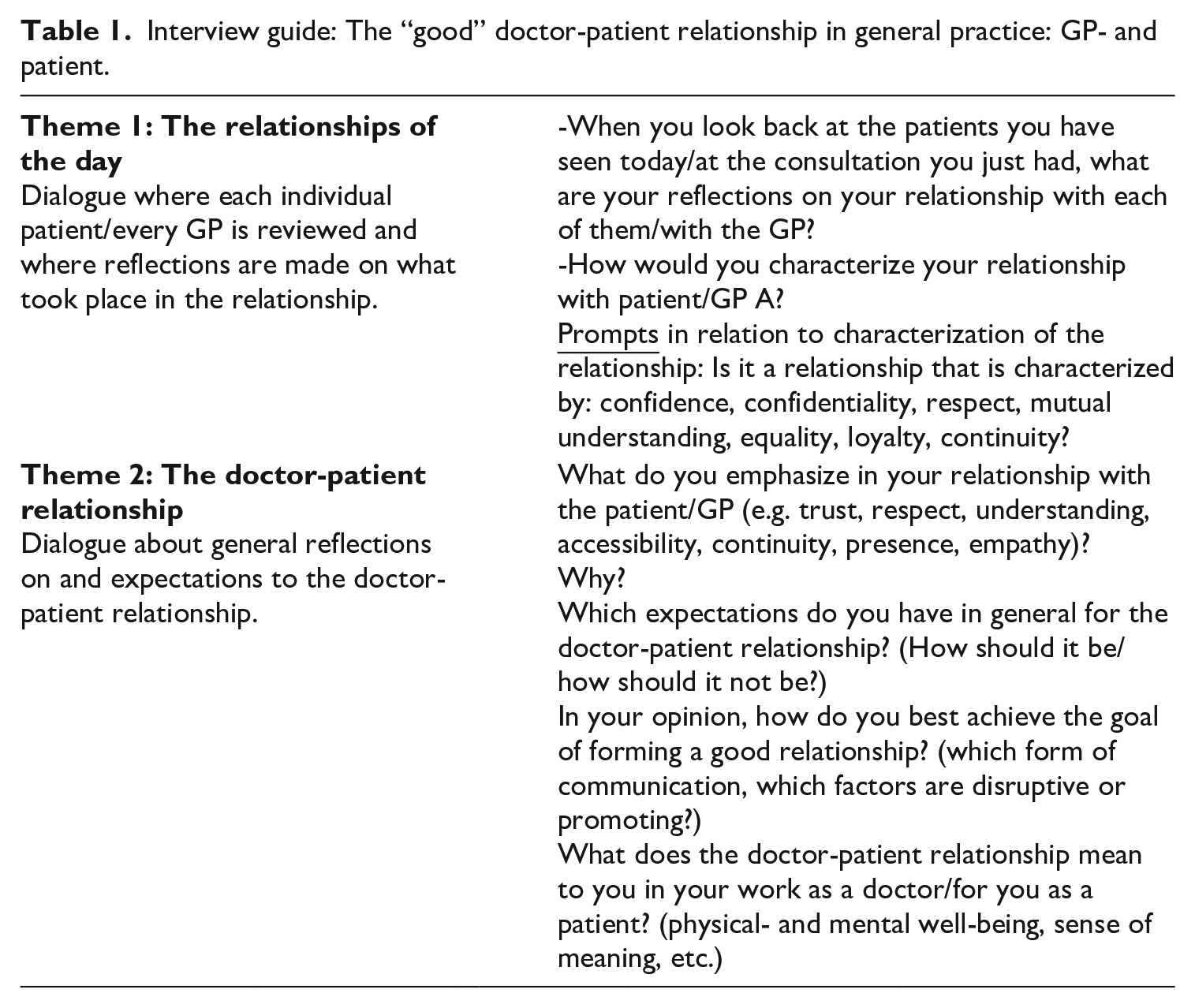
In the second substudy, 10 patients were interviewed by a junior researcher (and graduate student as part of a master’s thesis) about their experiences of the “good” doctor-patient relationship (using an adapted version of the above interview guide). A further objective of this sub study was to investigate the usability and perceived relevance of a short patient questionnaire translated into Danish on the doctor’s communication skills and empathy display: the Consultation And Relational Empathy (CARE) measure (Mercer et al., 2004). The stimulus afforded by the questionnaire, and the focus on how the patients’ experiences related to each questionnaire item, allowed for in-depth exploration of personal experiences with the doctor-patient relationship and perceived characteristic traits of a “good” doctor-patient relationship. A convenience sampling strategy was used. All interviews were audio-recorded and lasted from 40 to 70 minutes.
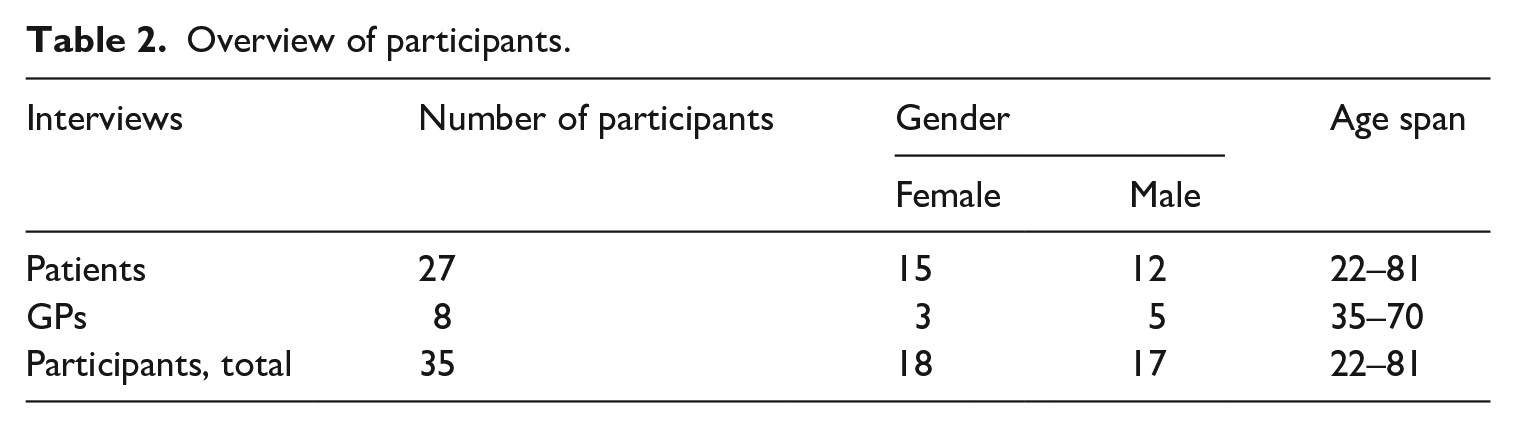
In the third substudy, 10 patients, all from another ethnic background than Danish, were interviewed by a second junior researcher (and graduate student as part of a master’s thesis) about their experiences of the characteristics of a “good” doctor-patient relationship. All interviews were audio-recorded and lasted from 15 to 55 minutes. In total, 27 patients (15 women, 12 men, age span: 22–81), 8 GPs (three women, five men, age span: 35–70) participated in the study (Table 2).
Overview of participants.
Data analysis
Notes from the fieldwork (substudy 1) were worked up by the senior researcher into detailed, descriptive, first-person field notes, including informal conversations. All formal interviews were transcribed verbatim by a student assistant and the two junior researchers. Both interview transcripts and reports with fieldwork notes were analyzed using the software program NVivo 12 pro. The senior researcher coded the transcripts following an initial open (inductive) coding strategy, using a node structure that reflected identified themes and subthemes that allowed for expansion and reduction along the way (Braun and Clarke, 2006). Time was identified as a prominent feature in the participants’ accounts, thus qualifying as a sensitizing concept, that is, a concept that is useful for starting and orienting a more focused coding in a subsequent analytic step (Bowen, 2006). Using the concept of time as guidance for further analysis, an interwovenness of being and time was identified: time allocation was perceived as an important element of the “good” doctor-patient relationship, but the meaning and value of the time allocated by the GP was dependent on the GP’s way of being during the allocated time. The literature was reviewed on perceived and actual time in the doctor-patient relationship to identify temporal categories and refine and concretize the analysis. Michael Flaherty’s analysis of the experiential qualities of time was moving the analysis toward identifying differences in temporal understandings, different time logics and how individual agentic practices are played out in respect to time management. This analytic process led to the identification of the following subthemes: (1) Making time – controlled by time, (2) Time allocation, and (3) Compensatory time work. In the below results section, data extracts are used to illustrate and develop the analytical arguments.
Findings
Making time—controlled by time
In conversation about their experience of what constitutes a “good” doctor-patient relationship, many of the interviewed patients used expressions that underlined the value of a doctor-patient relationship in which the doctor “gives you time” (“to be”). It became apparent that this expression concerned the subjective experience of temporality including being given time to tell their story and being listened to with an attentive presence during that time. In the following excerpt a married couple, both in their fifties, described it thus:
It’s important that they give you time.
Yes, that they give you time to be, and that they don’t rush things or already have a preconception or something they want to say. It’s important that they give you time. I mean, sometimes doctors can be busy, I mean, I think so, and you need to understand that, but, ehm, but it’s important to be given time to tell your story, because if that doesn’t happen, then it’ll be a problem for the relationship.
A young female patient explained it thus:
It’s very important that you feel that the doctor has time for you - and that you feel that you’re allowed to be worried or scared so that he doesn’t go like: “argh. . . I’ve looked at this a hundred times,” but that there’s room for you. The thing about not feeling that they have to hurry or that they are in a hurry. That they have time to figure out what to do about this, so that you are not seen as a patient but as a human being. (Patient 5)
Seen through Flaherty’s temporal agentic perspective, the time that the patients in the above excerpts desire to be given by their GP is in fact a customized time for them in particular such that the GPs “make” time for them during which they feel taken seriously and valued. The GPs’ act of making time (“time work”) seemingly takes precedence over everything else since it is experienced as a gesture that counters the experience of being just another patient on the conveyor belt. Another patient with non-Danish ethnic background explains:
Because then I have three other things that I need to ask her [the GP] about, now that I am finally there. And I have experienced her saying: “No, we don’t have time for that. You have to book another appointment.” And I get it, I mean, there is only allocated 10 minutes. But sometimes doctors are so busy that they forget that we are humans, who sometimes just need five more minutes. . .
And how does this affect the doctor-patient relationship you think?
Well, I just feel like she’s signaling to me: “next! [patient] – I need to get the next patient in, otherwise the whole system will break down.” Of course, it has an effect on the relationship, no doubt about that.
Underlying the need of the patients to experience time with the GP as a human being, explicitly articulated in the above accounts, is the awareness of a healthcare system and general practice as a pressured setting: waiting time on the telephone, time-pressured GPs and sometimes rushed consultations. What the GP chooses to do with that time in acts of self-determination, is what gives the whole situation meaning: for example, the patients who note that the GP chooses to do this instead of that, to be like this instead of like that. In so doing, the patients discern between an objective time framing in the manner of measuring and timing (clock time) and another that allows patients to exist and express themselves as temporal beings. On a further note, there seems to be a powerful potential for relationship building- and strengthening in the tension between how time reveals itself to the patient, in this case between external time constraints within the organization, and the action of “giving one time to be.”
Thus, the effect of what GPs choose to do with time, and how they enact time, play an active role in determining patients’ consultation experiences and the doctor-patient relationship, and this was observed in various consultations. For example, patients described the opposite temporal experience as “undesirable,” where the GP does not “make” time for listening and rushes consultations. In one of the clinics a GP abruptly interrupted a young female patient from a non-Danish ethnic background who was in the middle of presenting her reasons for consulting. Seemingly overwhelmed by being presented with more than one issue, the GP said: “You have to choose one single issue! We only have 10 minutes.” In this particular example the patient’s lack of adherence to appointment structures (one issue per visit) provoked a feeling in the GP of “losing” time, prompting her to take defensive agency toward mastering the organizational time circumstances in which she found herself, inducing a certain kind of unpleasant temporal experience in the patient. On the patient side, some of the interviewed patients from non-Danish ethnic backgrounds believed that common-held cultural stereotypes about them, for example, that they tend to show up late to consultations or do not respect the one-issue-per-visit policy, affected the temporal agency of the GP, which impacted the doctor-patient relationship. A patient said:
It’s commonly known that immigrants tend to be late for their appointments and the doctor can get like: “Argh, that’s just so typical for that group of patients.” So I always arrive ahead of time. . .And I think that should I be late for an appointment, it wouldn’t mean anything, because I have never been late. But here the other day, I was waiting in the waiting room and I overheard her say to an Arabic couple: “Well, you are 10 minutes late, so you have to book a new appointment.” And her tone was very harsch.
Although Flaherty with his idea of time agency emphasizes that the constitution of time is to a large extent accomplished through interpersonal interaction and agency—for example, in the doctor-patient interaction referred to above—he also points to the fact that it happens on an intra-personal level as interaction with regulating political and social norms that have come to control us. According to Flaherty, with the institutionalization of time, including the demand to control time efficiently, time can begin to inform, and eventually deform, our own personal ideals and wishes. The result can be that we end up doing exactly that which is expected of us, for example, making work more efficient but at the same time undermining our ethical standards and ideas of a “right” moral conduct. This might be the mechanism that we see illustrated in the above data when the GP rushes the consultation, educating patients about the organizationally-imposed time structures in order to experience a sense of time control and self-efficacy.
Time allocation
According to Flaherty, no “time work” is more agentic than the deliberate allocation of time (setting time aside) for our desires (Flaherty, 2011: 98). Allocating more time to the consultation in Danish general practice than the standardized amount of time (10 minutes) is unusual, although, in principle, every GP is in fact free to allocate the amount of minutes he/she wishes working in their own private practices.
Only one doctor in the study made efforts to increase the clock time for consultations, allocating 30 minutes to each consultation. Proceeding from Flaherty’s point that time is a resource that people actively and creatively manipulate, the GP’s choice of increasing the consultation length can be seen as a piece of “time work” (Flaherty, 2003) directed toward creating positive temporal experiences for his patients and himself, mastering and modifying the tempo in his activities (decelerate rather than accelerate). Talking with him about his priority, and the organizational implications hereof, he told me that in the beginning the clinic had a financial deficit. However, a long work life had taught him that sufficient time allocation for each patient would bring about the best solutions to the patients’ problems and thus “pay off” in the long run. Observing the interactions in the consultation room between the GP and patient provoked thoughts about whether the temporal experiences that the GPs’ time agency provoked were indeed aligned with those of the patients. Within the time available, the GP was observed to allocate a great deal of time to regulating medicine lists, looking away from the patient at the computer, filling in the electronic patient journal and applying a predominantly biomedical mindset to respond to health problems that might have needed a psychosocial or existential exploration, for example, feelings of grief, sleep disorder and stress. In a GP’s job there are many demands for which time must be made. From an array of obligations and demands, the individual GP’s allocation of time for different tasks reflects personal and professional decisions concerning the appropriate allocation of a precious time resource.
Another GP explained with great conviction that consultation time need not be longer than standard time allocation of 10 minutes. To make patients feel “seen and heard,” he argued for the decisive role of a certain sequence of actions (and thus timing of events), involving a routine rhythm and use of body language. This sequence consisted of the following three steps: first, when the patient was seated on the chair in the surgery, he would roll toward the patient bending his upper body slightly forward toward the patient, a body language that he would use in order to invite the patient to talk (tell his/her story). Then, when the patient started talking, he would lean his upper body toward the back of the chair as a sign of giving the patient time without interrupting (another GP described this as the “two minutes of emptying the patient”). Lastly, when having responded to the patient’s story and agreeing on an action plan, he would roll determinately back to the front of his desk, ready to look into the computer and schedule a new appointment. It was apparent that, by virtue of a self-conscious rhythm of activity, this GP was “doing time,” a piece of work directed toward provoking and/or preventing various temporal experiences.
In both of the above cases, the GPs were accustomed to being in authority and thus assumed the responsibility of organizing time. As Flaherty argues, all of us have agency in our daily lives to create different experiences of time. The interviews with patients also brought attention to the possibility of patient agency: when experiencing that time allocated to them was used inappropriately, in keeping with our previous finding concerning the value of being “given time to be,” they would allocate their time to another GP (switch the GP). The following excerpts illustrate this pattern:
If I just feel like I’m part of her daily routine because she has to fill out her work day to raise her salary, well, then I wouldn’t feel welcome either. And then I would also feel that I shouldn’t come here anymore. If it repeats itself. (Patient 1)
If you feel he’s sitting there, being superficial, if he has this empty look in his eyes. . .and you just feel like he’s thinking: “Isn’t she soon done talking so that I can move on?” then I don’t bother wasting my time on him anymore, no way. No, then I’ll just switch doctor. (Patient 5)
The experience of social and emotional disengagement described by the patients in the above excerpts can be compared to situations where we notice that the person we are in conversation with is looking at his/her watch in our presence. This usually gives the unpleasant feeling that the time that was dedicated to us here and now is turned into an absent presence and being exchanged for someone, something or somewhere else. As seen in the above excerpts, the judgments about how the allocated time can be spent inappropriately are also linked to a concern about wasting the patients’ own time and taking action should this feeling of wasted time arise. For the patients above withdrawing from spending time with a GP is based on the experience of him/her taking their time (time theft) which creates resistance. In the above excerpts the patients’ agentic resistance is related to the practice of switching doctors, thereby seeking meaningful temporal experiences within the doctor-patient relationship and resisting and avoiding others.
Compensatory “time work.”
The GPs, like the patients, showed an awareness of the time-pressured context in which they worked, with scarce temporal resources. Despite this, most of the GPs seemed unwilling to represent the doctor-patient relationship as constrained by limited time. Rather, they implied that the longitudinal time aspect inherent in the organization provided them with a privilege in terms of relationship-building and recurrently GPs were saying the sentence: “you have to remember, we GPs know our patients.” One GP explained:
It’s the continuity that turns our relationships into what they are. In other words, the knowledge of the patient’s prehistory, family history, background, etc. That’s for sure. And that’s our strength here in general practice in relation to our consultation process. Because we don’t have to start from scratch every time. And that makes it easier, that you can kind of build on a frame of reference. (GP 7)
As the above excerpt illustrates, the GP considers the relationship with the patient in a pragmatic manner stressing the central role of continuity, and the knowledge built over time of the patient, as a diagnostic tool and thus as something increasing competence and performance. Using Flaherty’s notion of “time work,” it seems that the knowledge that the GP has accumulated of the patient is connected and synthesized with the present in an effort to exert some control over the patient’s future, what Flaherty describes as timing (Flaherty, 2011: 82).
The longitudinal time dimension was also perceived as coming to the GPs’ “rescue,” since this could sometimes compensate for lack of time in the individual situation. The GPs used expressions such as “saving up time” or “having time on the account,” reflecting logics such as: “what we cannot do today, we have done yesterday” or “what we cannot do today, we can do tomorrow.” Talking with a GP at the end of a busy work day (being behind of schedule, barely any time for lunch or other breaks) about her reflections on the day (including consultation lengths), she commented: “But it’s also easier to have these short consultations if you know the patient well. Then you know, well, we’ve had a longer conversation another day. So now, today, it’s something quick.” (GP 4). In this excerpt time work is in evidence: finding herself in undesirable time circumstances in general practice, reference to longitudinal care and the “good” doctor-patient relationship as built upon a sequence of consultations in the past, present and future, can be seen as oriented toward customizing or manipulating her own temporal perceptions and desires. Whether continuity does in itself create a “good” relationship is of less interest in this context. Instead, to be noticed, were the efforts done with varying degrees of self-consciousness to arrange or manipulate one’s time circumstances such that time will be experienced in a certain, more positive way, achieving a persistent sense of professional identity.
Integrating Flaherty’s thoughts, embracing continuity as a core value of general practice can be seen as evidence for compensatory “time work,” provoked by the time-pressured circumstances in which most health professionals find themselves and as a reactive adaptation to a reality in which there are greater demands on the GPs’ time than there is time to give. It can also be seen, however, as something that is done in order to avoid challenging the status quo, contributing to the reinforcement of existing organizational, market-driven time structures.
Conclusion
Drawing on Flaherty’s sociology of time and different notions of time agency (Flaherty, 2011), this study documents how the “good” doctor-patient relationship is perceived and enacted in a tension between external temporal structures and internal temporal experiences that are the result of GPs’ and patients’ agentic practices of “doing time.” The use of agentic practices, by Flaherty called “time work,” is done in an effort to modify and manipulate various dimensions of temporal experience in the everyday life in general practice. In the “good” doctor-patient relationship patients desire and value to be “given time to be,” that is, that GPs use self-determination in order to customize patients’ internal time experiences, making them feel at ease and “human.” The accounts of the patients in this study relating to the “good” doctor-patient relationship can be seen to reflect a reaction to the “time regime” and “logic of acceleration” of our modern digital capitalist society (Rosa, 2010; Wajcman, 2015). In continuation hereof, seeking experiences of “being given time to be” in the encounters with the doctor can be interpreted as a result of an increase in dehumanizing developments, and a focus on clock time, in our healthcare system. As Arthur Frank points out in his book The renewal of generosity; illness, medicine and how to live (Frankel, 2004), modern medicine as a profession suffers from a loss of moralization as an inevitable result of an economic rationality that imposes regulation and monitoring on healthcare professionals, turning medicine into an economic enterprise. Frank sees a renewal of generosity as the answer to this growing demoralization. Generosity is here understood as a resonant, moral capacity of giving a human response to suffering that goes beyond the “job’s” biomedical and technical significance. Generosity here resonates with the kinds of doctor-patient relationships that patients want, namely those in which the GP does not only treat doctoring as a job but also as a human (relational and social) enterprise. This, we have seen, is related to how time is spent affectively and whether or not the time available is spent as open to resonance (as Rosa describes it). Thus, anticipating a pressured healthcare system makes for a compensatory desire among patients for “being given time to be” and among GPs for manipulating one’s time circumstances.
Our findings has also documented how “time work” can be used to undermine the “good” doctor-patient relationship through agentic practices that adhere to efficiency -and productivity logics (e.g. “time is money”). Thus, our findings show that GPs and patients on a micro-level can create the sense of more (and less) time through agentic practices in regard to time modulation, allocation, timing, and modification. GPs actively modify the reality of limited time that, apart from endangering their temporal experiences, might also weaken their sense of professional identity and self-efficacy.
The analysis highlights and challenges two things: First, rather than looking upon time as a situational given (i.e. a product of macro-structural determinism), individuals construct strategies for modulating their own and other’s temporal experiences, showing self-determination. Furthermore, showing how time experiences are actively constructed through “time work” offer new perspectives on the discourses of time in today’s healthcare systems that tend to focus on how healthcare providers have fallen victim to the time tyrannies of the modernization agenda, pressured into work situations beyond individual agency (Nettleton et al., 2008; Watt et al., 2008). While these findings are essential in understanding how the macro structure- and context in which health care professionals operate impact their ability to act in certain ways, as well as how they shape their beliefs about how they ought to act, it should not be forgotten that subjects are also agentically driven, shaping the world in accordance with priorities and parameters (Wajcman, 2015). Second, highlighting how patients’ assessments of the “good” doctor-patient relationship rest on subjective temporal experiences puts the stereotypical understanding of continuity, understood as continued, repeated contacts, as an a priori resource in general practice into relief. The unidimensional focus on time continuity as a resource thus needs to be supplemented by attention to how time is enacted. In continuation hereof, and drawing on Flaherty’s (2011) sociology of time, GPs and other health professionals might need to ask themselves: What kind of temporal experience do I want the patient and myself to have? Asking this question, and even better to act on it, one ceases to be regulated entirely by external time demands beyond ones’ control and instead exercises a measure of self-determination and agency in relation to time.
Footnotes
Acknowledgements
I thank all the research participants for their time and commitment to the study and former graduate students Anne Ulsø and Sebastian Bach Fiege for research collaboration.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I thank the Research Foundation of General Practice for funding this research project (grant number: EMN -2019-00719/A1835).
Ethics approval
All participants provided informed written consent. The study was accepted by the institutional review board of the University of Southern Denmark, The Research and Innovation Organization (RIO) (Journal no. 10.154.) and conducted in accordance with the GDPR and Declaration of Helsinki.