
Abstract
This research aimed to better understand how institutions are maintained, and the role of materiality in this institutional work. More specifically, the present qualitative case study analyzed how different actors in a large academic hospital in Canada worked together (i.e. accomplished institutional work) to maintain the institution of medical record keeping as a new clinical information system (computerized physician order entry-the material entity) was enacted. The study reveals that, to maintain the institution at stake, the intertwinement of processes of creating and maintaining institutions took place. In fact, different forms of institutional work interact Results also strongly suggest that the design of computerized physician order entry and its implementation (i.e. the materiality involved in this institutional change) played an important role in the maintenance of the institution of medical record keeping: on the one hand, it was particularly present in three types of institutional work, namely enabling, policing, and deterring; on the other hand, it appeared to be an essential component of the routinization of work by allowing a better fit between the new technology and the organization of work
Introduction
In an institutional context that increasingly calls for a redefinition of the medical profession (Price et al., 2020; Sorensen and Iedema, 2008), it comes to not surprise that medical record keeping be unequivocally considered a key medical professional practice to be upheld. In line with applicable laws, medical associations have developed and disseminated guidelines for record keeping (Collège des médecins du Québec, 2005; College of Physicians and Surgeons of British Columbia, 2014; Royal College of Physicians, 2015). These guidelines emphasize the purpose of medical records (for communication, evaluation, legal protection, knowledge development, etc.), the types of information that must appear in the record, and the physician’s responsibility in record keeping. It is incumbent on physicians to include, among other things, their observation notes, medical orders, and progress notes. In this sense, record keeping and the rules governing the practice can be considered a veritable institution. Institutions are defined as “interrelated systems of rules that structure social interactions” (Hodgson, 2006: 2), with rules in turn being conceived as “norms of behaviors and social conventions, as well as legal rules.”
That said, a number of empirical studies have shown that respect for these rules cannot be taken for granted (Abdelrahman and Abdelmageed, 2014; Mann and Williams, 2003; Pullen and Loudon, 2006). Maintaining the institution requires work and effort by the actors involved to properly keep records. The introduction of information technologies (Goldschmidt, 2005; Institute of Medicine (US) Committee on Quality of Health Care in America, 1997) in the health sector is seen as a move that might facilitate the maintenance of this institution. However, information technologies are not being used to anywhere near their full potential, as has been demonstrated in numerous empirical studies (Audet et al., 2004; Berg, 2003; Gagnon et al., 2014; Greenhalgh et al., 2019; Håland, 2012; Mechanic, 2008; Miller and Sim, 2004; Petrakaki et al., 2016). Unfortunately, very few process studies have been undertaken to look at how, through the introduction of technologies, health care organizations ensure that physicians, who are particularly influential actors in health systems respect the rules related to record keeping.
From this starting point, the present study aimed to examine how different actors in a large academic hospital in Canada work together (i.e. accomplish institutional work) to maintain the institution of rules for medical record keeping through processes enacted to adopt a new clinical information system (the material entity). The investigation is guided by the following research question: How different hospital actors worked to maintain adherence to the rules of medical record keeping as they start using a new digital clinical information system?
Theoretical foundations: Institutional work and materiality
Since we focused on the maintenance of a medical institution, we considered that institutional theory was a well-suited theoretical foundation for this investigation. Moreover, several scholars who study information technology related change (Barrett, 2006; Greenhalgh et al., 2019; Hayes, 2008) have argued that new institutionalism provides a powerful framework for understanding the context within which organizational changes takes place. For instance, Greenhalgh et al. (2019) in their ethnographic case study of how health information infrastructure shapes and constrains technological innovation, added an institutional dimension to their analysis considering how institutional roles and identities generated particular agendas and priorities. Other scholars such as Hayes (2008), adopting a socio constructivist perspective, invite us to pay attention on how information technologies are implicated in institutionalization processes.
Until the 1990s, institutional scholars were primarily concerned with the way institutional context influenced organizations (Greenwood et al., 2008; Meyer and Rowan, 1977; Meyer and Scott, 1983; Powell and DiMaggio, 1983; Scott, 1995; Tolbert and Zucker, 1983). After DiMaggio’s (1988) remark that institutional theory should integrate agency, scholars became more interested in understanding how organizations shape their institutional context. This trend generated several new concepts, such as institutional work.
In their influential work, Lawrence and Suddaby (2006) define institutional work as “the purposive action of individuals and organizations aimed at creating, maintaining, and disrupting institutions” (p. 215). Founded in DiMaggio (1988) and Oliver’s (1991) emphasis on agency, and embedded in the so-called “practice turn” in social theory, Lawrence and Suddaby (2006) identify three interconnected elements important to understanding institutional work: (1) focus on the “awareness, skill and reflexivity of individual and collective actors” (p. 219) when creating, maintaining and disrupting institutions; (2) view institutions as coming into being through “the more or less conscious action of individual and collective actors” (p. 219); and (3) consider action as practice, which always occurs “within sets of institutional rules” (p. 210). Looking at the three stages in the life cycle of institutions as defined by Tolbert and Zucker (1996), Lawrence and Suddaby identify a taxonomy of forms of institutional work that individual and collective actors can undertake to create, maintain, and disrupt institutions.
While earlier institutional scholars were much less interested in the institutional work involved in maintaining an institution than in its creation, Lawrence and Suddaby’s taxonomy points to enabling, policing, deterring, valorizing and demonizing, mythologizing and embedding, and routinizing as forms of work that serve to maintain an institution. The first three involve assuring adherence to institutionalized rule systems, whereas the latter three focus on reproducing norms and beliefs.
Inspired by this taxonomy, a growing body of literature highlights the different strategies actors take to maintain an institution. First, these strategies include micro and macro level processes sustaining institutional stability (Dacin et al., 2010; Quinn Trank and Washington, 2009; Zilber, 2009). For example, Dacin et al. (2010) illustrate how formal dining at the University of Cambridge contribute to the maintenance of the British class system. Trank and Washington (2009) showed how a legitimating organization undertook actions to reinforce the normative foundations of the institutional arrangements in the field of management education (cf. accreditation).
Second, maintenance work can emerge when change threatens institutional arrangements. In these contexts, active incumbents enact activities to secure their occupations. For example, in their case study of NHS, Currie et al. (2012) shed light on the tactics employed by specialist doctors (educating, theorizing to assume a delegation role) to maintain their professional dominance, after the introduction of a new labor policy. In another study, Micelotta and Washington (2013) illustrated how Italian legal professions, after a reform introduced by the government depriving them of their privilege to self-regulate, engaged in institutional work aiming at repairing institutional arrangements.
Third, strategies to maintain institutions correspond also to less intentional micro-processes undertaken by institutional inhabitants to restore breakdowns in institutionalized practice. For example, Heaphy (2013) study in a hospital shows how patient advocates skillfully used rules—or formal policies and procedures—to restore, clarify, or initiate organizational changes in rules, all to maintain institutionalized role expectations (p. 1). Lok and de Rond’s (2013) study reveal that the different forms of institutional work vary depending on the nature and process history of practice breakdowns, contributing to a “plasticity” of institutions capable of self-repair.
Whereas there is no doubt that the aforementioned works deepen our understanding of maintenance work, there is still a dearth of research on material work, as has been highlighted in a relatively recent knowledge synthesis on institutional work (Hampel et al., 2017). As explained by the authors, material work “draws on the physical elements of the institutional environment, such objects or places, to influence institutions” (p. 27). The material turn in organization studies, championed by renowned scholars such as Carlile (2002), Orlikowski (2007), Nicolini et al. (2012), and de Vaujany et al. (2019) emerged following the linguistic focus that was predominant in the 1980s and 1990s. As Monteiro and Nicolini (2014) note, this approach combines “the idea that materials (e.g. objects and spaces) are part of the way in which social processes and organizations are enacted and stabilized with the widely held position that institutional agency is better conceived as both emergent and distributed” (p. 1).
Hampel et al. (2017) stress the importance of conducting further empirical studies to better understand the role of materiality in institutional work. The present study seeks to answer this call. To our knowledge, it is the first study to consider the interplay between technology and institutional work in order to understand the maintenance of an enduring institution such as the keeping of medical records in hospitals. The technology considered here is the computerized provider entry system (CPOE), which enables providers to submit orders electronically. The majority of existing studies concerning CPOE have focused on physicians’ beliefs and concerns (Georgiou et al., 2009; Holden, 2010), patterns of use (Niazkhani et al., 2011), impacts on workflows (Aarts et al., 2007), and on the quality of care (Brown et al., 2016). Rare are studies that focus on implementation issues, except Aarts et al.’s (2004). We were particularly interested in understanding how concerned actors work together to maintain the institution of medical record keeping in a context of materiality change. Our analysis was guided (see Table 1) by the taxonomy of forms of institutional maintenance proposed (Lawrence and Suddaby, 2006):
• Enabling refers to the creation of rules that will further support the institution in place. This form of institutional work includes the creation of new roles to ensure survival of the institution.
• Policing aims to ensure compliance with rules through enforcement, auditing, and monitoring.
• Deterrence establishes coercive barriers to institutional change.
• Valorizing and demonizing involve presenting illustrations of the normative underpinnings of the institution, both positive and negative.
• Embedding and routinizing integrate the normative underpinnings of the institution into actors’ day-to-day practices and routines.
Forms of institutional work: definitions.
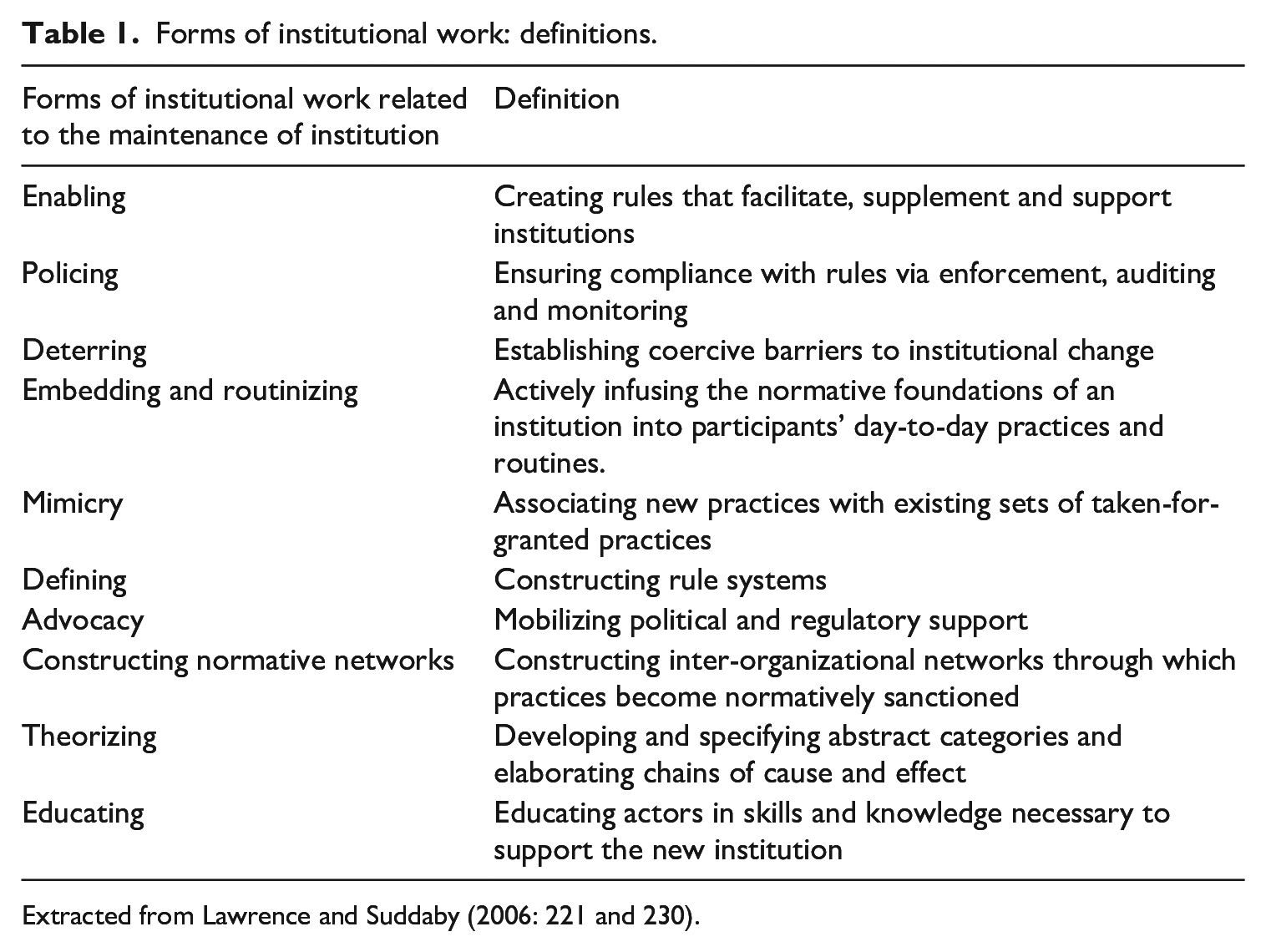
Extracted from Lawrence and Suddaby (2006: 221 and 230).
Study context
This research was conducted in an academic hospital within the Quebec health network. To meet the population’s needs for health and social services, Quebec built, starting in the 1970s, a network of public establishments employing different types of health professional. Physicians remain self-employed workers in this system, and are mostly paid by fee for service. In line with the principle of public management, these physicians are subject to a number of laws, including the Medical Act (1973) that stipulates norms for medical record keeping. Based on this law, in 2005 the College of Physicians of Quebec produced a guide for members, reminding them of the importance of proper record keeping and the principles that should guide practice.
The academic hospital in this study is a super hospital created in 1997 through the merger of five academic hospitals. The publication in the USA of the report To Err is Human: building a safer health system was the catalyst that prompted the hospital to look into the acquisition of a new clinical information system. The report claims that between 75,000 and 100,000 deaths in the US each year are due to medical errors, a third of which could be avoided by introducing electronic orders. At that time, the hospital already had a system for radiology and laboratory requisitions, which were entered into the medical record by clerical staff. The goal was to acquire a comprehensive clinical information system that included (CPOE), where the physician would directly enter requisitions for radiology and laboratory tests, and prescriptions for medications. The system would therefore encourage use of recognized standards in record keeping, while also improving the quality of care (see Introduction). It promised a number of benefits, such as preventing the duplication of tests.
Methodology
Research strategy
We adopted a qualitative case study approach as this research design appears particularly suited to understanding complex phenomena in context (Stake, 1995). Qualitative methodology that aims to “reveal the sense or meaning that the phenomenon under study holds for individuals” (Fortin and Gagnon, 2016: 25, our translation), enables research to answer how and why questions (Creswell, 2014). The case was the project to implement the CPOE module in this hospital. Two elements make the case especially interesting: (1) Adherence to best practice norms for medical record keeping is essential in an academic hospital. Through its teaching mission, the organization must set the example for the physicians it trains. As well, its research mission requires high quality data, and thus impeccable record keeping. (2) The hospital in question was, at the time, one of the few hospitals in Canada to adopt a clinical information system that included the CPOE module, which was expected to play a key role in proper record-keeping.
Description of the case
Joining forces with another academic hospital, in 2004 the hospital under study acquired a clinical information system (OACIS) with configurable technology (Fleck, 1994). Considerable work was required to develop the system’s functionalities. Three phases of deployment were planned: (1) A first phase, begun in 2006, dealt with the visualization of imaging and laboratory test results. (2) A second phase (2010–2011) focused on developing the clinical documentation module (vital signs, height, weight, pain assessment, etc.) needed for deployment of the prescription modules. This module was pilot-tested in 2010–2011. During this same phase, the imaging module was implemented in 2011–2012. (3) Finally, the module for laboratory/microbiology requisitions was deployed progressively starting in 2013, and more rapidly after 2014 in order to close the contract with the old system’s provider. Each of the three modules was deployed first as a pilot project and then throughout the hospital. The present study focuses on the processes of pilot testing and deploying the imaging and laboratory requisition modules.
Study participants
Thirty-one respondents with different roles in the hospital participated in the study: members of the executive, clinical consultants, a representative of the technology supplier, members of the project team, members of the support team, physicians, directors of nursing, and other hospital personnel. All participants provided a written informed consent.
Data sources and methods of analysis
Data were collected between 2012 and 2016, with a first certificate from the ethics committee of the faculty of medicine affiliated with the hospital delivered on May 25, 2012, then renewed each year until the end of the study (IRB study number A05-E43-12B).
This study had two sources of data: observations and individual interviews. We conducted non-participant observation of all meetings of the “champions” committee (56 hours of observation) and the “acceleration” sub-committee (32 hours) in order to discover the challenges associated with the implementation and utilization of the new clinical information system, and the solutions proposed by actors participating in these spaces. We also observed use of the new clinical information system in the daily operations of clinical units. The objective was to observe the use of the different modules, the day-to-day problems encountered, how (and by whom) these problems were solved, interactions between actors around the circulation of information, etc. Three care units with different operational contexts were observed: a pediatric care unit (18 hours of observation), a neurologic unit in a general hospital (13 hours), and a general surgery and transplantation unit (16 hours). Each unit revealed specific challenges related to harmonizing the technology and work routines. For example, the functioning of the pediatric unit required a catalog of specific laboratory tests that was different from the adult catalog.
Semi-structured interviews were conducted to more deeply understand actors’ realities (Lutton, 2010). Interviews addressed a number of themes: perceptions of the new clinical information system, the deployment process, system utilization modalities, difficulties encountered during deployment, adaptations made to the system, modifications brought to work routines. All interviews were transcribed and coded with NVivo software.
Analysis involved a constant dialog between data and theory (Collins and Stockton, 2018). As a first step, we assembled the various data sources to produce thick descriptions of how the actions undertaken by different actors enabled the maintenance, throughout the appropriation of the new technology, of the institution involving adherence to best practices in medical record-keeping. In complement to this analytical approach, we also employed a strategy of temporal bracketing (Langley, 1999): the decomposition of data into successive adjacent periods to enable explicit examination of how actions in one period lead to changes in the context that will affect action in subsequent periods. This technique enabled us to identify three consecutive phases in the maintenance of the institution of proper medical record keeping following the adoption of the CPOE.
Moving to a more abstract analysis, we then associated results of the descriptive analysis with the different forms of institutional work identified by Lawrence and Suddaby (2006) that correspond to the goal of maintaining institutions, while staying attuned to forms of institutional work corresponding to other goals, such as creating institutions. The abstraction was accomplished in several iterations: the two first authors of the paper challenged each other’s interpretations and discussed differences until consensus was reached, aided by a reexamination of theoretical works. This interpretation was then validated with the other authors.
Results
Phase 1: Starting with the simple stuff
The phase begins with a change at the level of materiality, in this case the decision, and subsequent action, to move from paper records to a digital system. When records were in paper form, physicians simply wrote down what they prescribed or ordered in the paper chart. The organization then delegated to a clerk the task of entering the order in the requisition system.
“In the past there was a practice where some things were - for better or worse - delegated to intermediaries who, when you think about it, were not the right people from, I don’t know, a legal perspective or even level of responsibility, to do these things. So we started with an electronic requisition system that was. . . look, it was absolutely fantastic in its time, and was even quite advanced compared to other establishments, but where clerks operated requisitions and, over time, that meant some people. . . developed a degree of autonomy around that, becoming somewhat disassociated from the doctor’s initial order”. A manager
The CPOE, as conceived, required physicians to enter their requisitions and prescriptions in the system themselves. It was clear to the organization that physician entry of prescriptions for medications would bring the greatest added value in terms of quality of care. That said, they could not implement this module directly. Facilitating uptake required proceeding with small steps: “But the biggest problem is with medications. Will they take the time to enter them? And of course that’s where the benefit lies. But I think once you’ve developed the habit of entering lab and imaging requisitions, it will come more naturally, it won’t be so scary. The psychological block will be gone.” A manager
In this gradual approach to appropriating practice changes, physicians were placed at the heart of the process, participating in various committees alongside other stakeholders. This was accomplished by putting in place multiple structures (project management team, “champions” committee, working groups) that constructed
As well, still in the perspective of promoting the adoption of new practices, the project leads used an “We reached out for support at the political level, we reached out for support from professional services. We communicated messages through them, and it was they who officially announced the start of deployment “From now on, you have to enter your prescriptions in OACIS, and while it may be hard at first, it will work out well in time.” (Communications officer)
Considering that physicians in one constituent part of Hospital X, a pediatric hospital, had, in the past, used a clinical information system where physicians entered medication prescriptions—a system that had since been abandoned—the project team sought to build on this experience to encourage physicians in the pediatric hospital to enter prescriptions in the new modules. This strategy is related to “And that is when we focused on medical imaging, because doctors. . .. and they knew it from their responsibilities and because it was demanded by the radiology department – and by imaging – were obliged to produce a paper requisition detailing the conditions of the exam, the patient history, etc. . . . the indications and all that. So, one way or another, each time doctors ordered an imaging test, they were obliged to produce something. They couldn’t just state: tomorrow an echo, or tomorrow an x-ray. . .” A manager “That’s it. It was a choice to say let’s start with an area, a form of prescription that will right away offer tangible benefits to the doctor, and is simple to do because a catalogue of imaging is pretty standard; while some learning was needed, there wasn’t much complexity to capturing in OACIS an x-ray or a scan or whatever based on a catalogue.” A manager
That said, despite the apparent “simplicity” of changing these practices, efforts were needed to convince doctors of the benefits of making requisitions in this new way. This
“We insisted that we had to demonstrate and teach people that it wasn’t just an electronic requisition system, but really a prescription management system. So, who manages prescriptions? That would be clinicians with prescribing privileges. So it’s not like a clerk can take their place, or second them or act as the physician’s backup.” A manager “So we said, look, rather than have the doctor order the prescription, complete the requisition, and give it to the clerk to enter into the system, we’re going to take the fast track, and the clerk’s role is no longer needed, except to operate the mode of transportation and ensure the order has reached the imaging system. Good. But you will go directly into OACIS to enter the order, enter the clinical information, and when you press ‘send’ the radiology department receives your requisition that second. Before, the requisition could spend three days in the mail’s envelope or waiting for someone to deliver it. . .” A manager
To proceed with this change aimed at maintaining the institution of medical record keeping, the organization formalized rules around record keeping and around each person’s role, which relates to institutional work of
Control over access to the system (material work) became a crucial means of enforcing adherence to the rules: “I think it starts to make sense from the moment you have a way to really control its evolution and always focus back on the rules of best practice, on who are the different people who can interact with the system, with the right rules of conduct and the right privileges.” A manager
Changing medical practices also required institutional work around “The transition to electronic prescribing forced harmonization, standardization and use of the same nomenclature everywhere. That’s also somewhat difficult. . .” Information technology (IT) team member
This standardization obviously required significant learning among physicians. As one example, using the system required that physicians know the precise names of all the exams, something they did not need to know when the clerk was entering the request: “The other thing is around learning. When doctors prescribe on paper, they write it however they want. Or they’ll verbally tell someone “do me a lung for the patient in 3”; the catalogue doesn’t have an entry for just ‘lung’. . . you have lung, anteroposterior or lateral; one view, two views, three views, you have everything. . . a ‘lung’ is like nine different tests. Before, when the doctors said “do me a lung for the patient in 3”, the nurse or clerical staff knew that on that unit, when a doctor says they want a lung, that means an AP-lateral. Clerical and clinical personnel were interpreting what the doctor was ordering.” IT team member
Bringing about this learning required considerable work in “Hey, what do you call that? pulmonary? respiratory?’ So right away for all the tests that involved lung, we put CXR as a synonym. It’s this type of gap between the machine’s language, the catalogue and,,, the clinician’s language. That’s the gap that in clinical analyses we need to bridge with synonyms or groupings of prescriptions or other things.” IT team member
Each time the imaging module was introduced in a care unit, the paper format was eliminated, thus preventing physicians from reverting to old work habits in record keeping. They had no choice but to enter the orders in the new system. In other words, we witnessed implementation of a “The implementation team was the first to notice it (entry of orders in paper form) because they assured surveillance of the system. They would contact the physician: ‘Have you been trained? Can we set up a meeting?’ And on like that. If that didn’t work, the physician’s name was passed on to the Director of Professional Services. So it followed its course.” Communications officer
Phase 2: Gradually introducing the more complicated modules in some care units
After having tackled the simplest module, Hospital X proceeded with the gradual introduction of the laboratory module, as per the original plan. This deployment was more complicated, because treatment of the physician’s order involved a number of actors (nurses who take the samples, clerks, laboratory personnel, etc.) and greater interdependence. The specificities of medical orders in some units, notably in pediatrics (nomenclature of tests, quantity of blood required) created challenges around the fit between the technology and work routines. Finally, physicians usually ordered groups of exams and found it intolerable to enter them one by one.
All this meant that institutional work to
“Sometimes, there are things that still appear as “ordered” when they have already been collected, but because they were sent to another hospital, it still says “ordered.” So I have no way of telling the difference between what has and has not been collected. So there should be additional steps, like “ordered” to mean I requested it, then “collected,” but maybe not sent, and after that “in progress” when the lab has received it, if we want to make the distinction.” A Resident
“We had a technical team of analysts and the lab team and we worked together to define the needs of the lab, what had to be entered in the lab system as required information. On the one hand, there’s the information needed to interpret results or for the lab machines to conduct their analyses.” IT team member
This institutional work was demanding and continued for quite some time. As a result, during the first months of deploying the module, there were persistent difficulties that created considerable resistance among physicians in some units. Faced with a crisis, the nurses agreed to enter orders for the physicians. But at one point, they refused to continue this practice, and were united in doing so, thus preventing physicians from reverting to former habits (
Phase 3: Accelerating deployment of the modules across the hospital
The move to the new hospital site triggered phase 3, as hospital leadership decided to proceed with the accelerated deployment (over just a few months) of imaging and laboratory modules across the entire hospital starting in Fall 2014. The decision was motivated by a desire to save on the costs associated with the old requisition system. From that point on, the hospital would keep only the clinical information system. This transition (
The accelerated deployment required particular efforts related to different forms of institutional work. First, an accelerated deployment committee was created, involving all actors needed to contribute to change ( “To sum it all up, I think there was a disciplinary committee, at a high enough level in the hierarchy, dedicated to accelerating deployment that could ensure deployment was successful. Because it enabled things to move more quickly, to access all levels of decision-making, offer much tighter support. Sometimes just the fact. . . there was a unit that lacked computers, it had two but would need five, six, seven, eight. . . well just the fact of having the director of IT, who was able to look into the budget and find computers quickly, well, that helped with deployment.” Communications officer
As well, thanks to “. . .each week, Ms. X received new trainers. You had a core of three or four OACIS trainers, who didn’t have time to train the new trainers, so trainers were sort of paired. They attended training sessions, read everything there was to read about OACIS and all that until they felt comfortable enough to provide support, then one-on-one training, and then classroom training. And there were all sorts of people doing that; it was amazing. That amazing thing was like a kind of mirage in the situation.” Communications officer
These efforts resulted in significant changes in practice. In 2015, data collected suggest that medical residents were increasingly using the new system, entering orders themselves. However, a number of physicians were not doing so. As well, there was a persistent major problem in that verbal orders made by nurses were not being counter-signed. Formal procedures were introduced to partly resolve the problem, while still respecting the rules, by using collective prescriptions to give nurses the right to prescribe. These prescriptions are specifically attached to a particular unit and are formally created with approval from the physicians (authorizing nurses to enter the prescription) and the nurses (accepting to enter this type of prescription). The intensive care unit opted for conditional prescriptions entered into the system by the physician: nurses are allowed, for example, to order laboratory tests if certain clinical conditions arise (i.e. increase in a patient’s temperature).
Discussion and conclusion
This research aims to better understand how institutions are maintained, especially in professional milieus. The work contributes to a relatively recent trend in institutional studies that goes beyond regarding institutions as self-reproducing, and reveals the work undertaken by actors to ensure their stability. Our research takes place in a context where actors’ dynamics which have motivated efforts for institutional maintenance are not triggered by a perceived threat to the survival of the institutional arrangement, but rather by a change in the institution’s materiality that creates an opportunity to update how actors mobilize and adhere to institutional norms. The institution maintained in our case is the keeping of medical records. As a leading academic hospital, the organization sees the change in material support for medical record keeping as imperative to preserve its legitimacy in the institutional field. As well, the pressure on the medical profession described in the introduction to this paper means that maintaining the institution of standardized medical record-keeping is a real issue for the profession’s legitimacy.
Our in-depth analysis of the forms of institutional work (see Table 2) employed to maintain this institution allows us to make two contributions to the current state of knowledge. First, the study reveals that in situations characterized by changes in the materiality of an institution—in this case, replacing paper by digital technology—the maintenance of institutional norms requires the creation of new practices and, consequently, a change in professional practices. To our knowledge, these insights regarding the maintenance of institutions in a context of change in materiality have not previously been identified. That said, the phenomenon of overlap between processes of creating and maintaining institutions has been noted in other contexts. Dahlmann and Grosvold (2017) showed that in complex environments, characterized by the juxtaposition of a variety of institutional logics, managers sometimes negotiate tensions by trying to integrate logics, and do so by combining different forms of institutional work to create, maintain, or destabilize institutions. As well, in their study of the creation of a new institution (new standards for managing enterprise risks), Hayne and Free (2014) showed that different forms of institutional work were involved in the creation and maintenance of these new standards. Our research, in turn, reveals that efforts to maintain norms, in the context of changed materiality, involve overlap between processes of creation and maintenance.
Forms of institutional work employed over time.
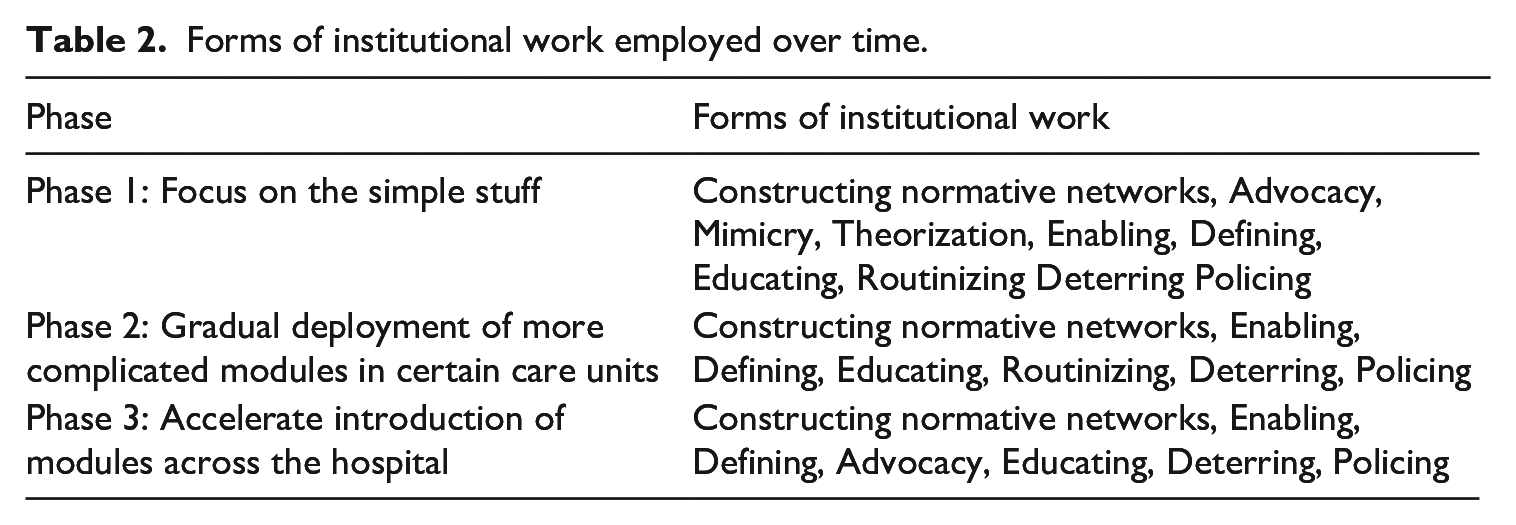
Physicians are major actors in the institution of medical record keeping. With the new digital platform, physicians in this study were responsible for entering and following up on requisitions and prescriptions themselves. Likewise, they had to know the exact names of tests included in the CPOE catalog and learn how to operate the computer system. These demands met initially with considerable resistance from physicians, who were expected to make major changes to their usual behavior. In this context, several forms of institutional work related to creating an institution (mimicry, theorizing, advocacy, constructing normative networks, defining, educating) were needed to facilitate the transition from paper to digital record-keeping. The timing of different forms of institutional work also appears important: while educating continued throughout the deployment, mimicry (“associating new practices with existing sets of taken-for-granted practices, technologies and rules in order to ease adoption”) and theorizing (“the development and specification of abstract categories and the elaboration of chains of cause and effects”) (Lawrence and Suddaby, 2006: 221) were particularly useful during the first phases of the transition. This being said, all these efforts resulted in partial success. As outlined. medical residents, the next generation of physicians, have adopted new ways of working. This is a very promising change. Older physicians have not adopted CPOE, but there was not an outcry, and the CPOE implementation continues. Other studies confirm that the adoption of CPOE is challenging (Cresswell et al., 2016; Muslin et al., 2014; Poon, 2006), especially for more senior physicians. These latter often reject dirty work (Håland, 2012; Hughes, 1962). Dirty work refers to tasks that are perceived as degrading, disgusting, such as secretarial work.
Furthermore, for institutional norms to be upheld during the transition to the new digital platform, our study reveals that concomitant forms of institutional work to maintain an institution are needed. In this case, these involved enabling (the creation of rules that support institutions), policing (fostering compliance through enforcement, auditing, and monitoring), deterring (establishing barriers to institutional change), and routinizing (actively supporting the normative foundations of day-to-day organizational practices) (Lawrence and Suddaby, 2006). These forms of institutional work were essential at all phases of implementation.
Interestingly, our study also shows that some forms of institutional work involved in creating institutions are complementary not only amongst each other, but also with forms of institutional work related to maintaining institutions. For instance, policing work in the initial phases of the transition would have had a very limited impact without concurrent education. Likewise, the lobbying work to obtain resources was essential to carry out the education work, and was particularly important during the accelerated deployment in Step 3. Furthermore, without the construction of normative networks in the initial phases of transition, routinization, which requires commitment from various actors, would have been very difficult to achieve. Routinization was also facilitated by mimicry, as seen in the decision to conduct the early pilot deployment in a unit where physicians were already familiar with the use of an earlier iteration of digital requisitions. Like Hayne and Free (2014) and Currie et al. (2012), we see a very fluid process where different forms of institutional work interact. By addressing the temporal aspects of the phenomenon under study, we also see that some forms of institutional work persist over time (such as routinization and education), while others disappear (such as theorization), and still others re-emerge (such as advocacy).
Our second contribution deals with the role of materiality in different forms of institutional work (see Table 3). Our results suggest that materiality plays an essential role in three types of institutional work (enabling, policing, deterring). More precisely, it contributes to preserving institutional arrangements by relying on a pillar of institutions, in this case, rules. As just one example, monitoring physicians’ practices through databases produced by the clinical information system enabled the identification of possible misconduct. Similarly, controlling the right to access the clinical information system by assigning codes to clinicians enforced the rules underlying each of their roles (i.e. who has the right to prescribe). Withdrawing paper forms after each phase of deployment in a care unit gave doctors no choice but to follow the rules around entering orders in the system. At another level, material work, in this case the design of computerized physician order entry, is, to the extent that design improves the fit between the technology and the organization of work, an essential component of the routinization of work, and thus contributes to maintaining the institution.
In sum, this investigation rejoins recent works (Boutinot and Delacour, 2022; Colombero and Boxenbaum, 2019) that enrich our understanding of how materiality plays a role in different forms of institutional work aiming to maintain institutions. It also enriches the state of knowledge concerning CPOE. As Aarts et al. (2004) argue, the introduction of CPOE can be understood only if we consider the social and technical aspects of the story (p. 215). Our study deepens our understanding of these socio-material practices.
Role of materiality in the different forms of institutional work.
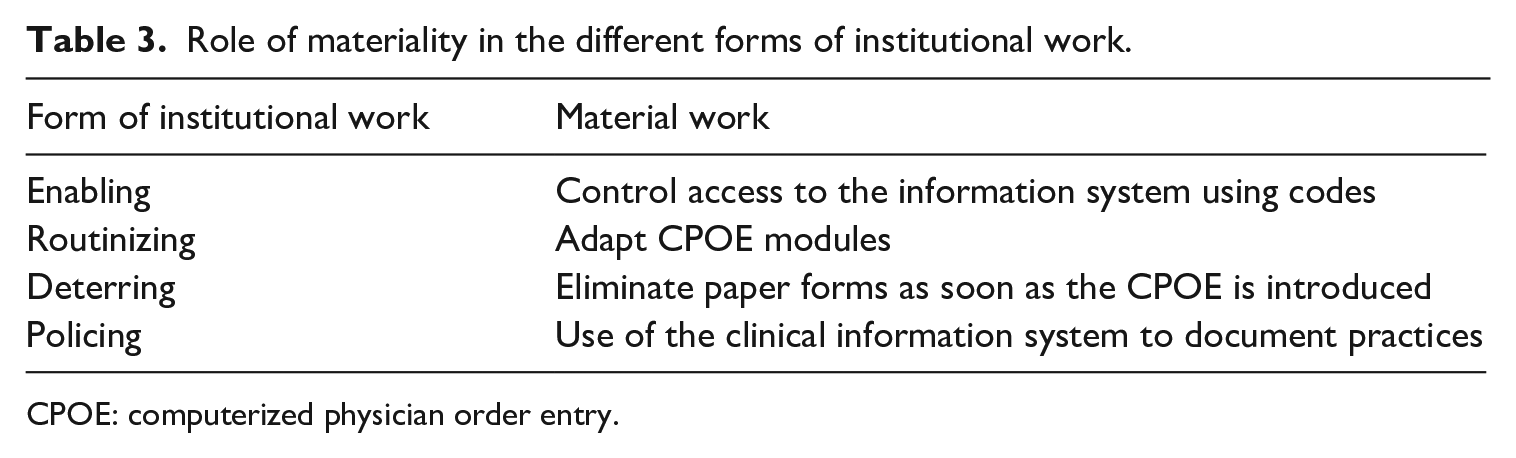
CPOE: computerized physician order entry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received a funding from Social Sciences and Humanities Research Council for this research.