
Abstract
As interlocutors in national level discourse with the power to influence public opinion and inform policy, the news media are an important data source in understanding the constitutive roles played by culture and discourse in shaping health experiences and outcomes. This paper reports on a critical discourse analysis of news media coverage of HIV in the Republic of Ireland between 2006 and 2016. This period is significant because of the considerable increase in new HIV diagnoses that occurred in Ireland after the 2008 recession. Analysis of articles (n = 103) demonstrated a pattern of dividing practices whereby people living with or affected by HIV were frequently positioned as somatically and morally deficient via discourses of risk and responsibility. Little focus was given over to examination of the structural drivers of HIV, occluding the social context of the epidemic. The findings suggest that media discourses on HIV have the potential to other people living with HIV and generate stigma by invoking a dynamic of blame and shame frequently implicated in the stigma process.
Introduction
In spite of vast improvements to treatment and prevention technologies in recent years, HIV remains a significant public health concern in the Republic of Ireland. Around 7200 people live with HIV in the Republic of Ireland (Health Protection Surveillance Centre [HPSC], 2019), and significant increases in the rate of new diagnoses have been reported recently, with the highest number ever recorded in 2018 (HPSC, 2019). The current notification rate stands at 11.0 per 100,000 of population, notably higher than the European average of 6.2 (HPSC, 2019). These increases have occurred in the context of considerable social stigmatisation of HIV. A survey conducted in 2017 found that among people living with HIV (PLHIV) (n = 168), 30% reported feeling stigmatised by family, and 23% by friends (HIV Ireland, 2017). Stigma is also a problem frequently experienced by PLHIV in many healthcare settings (Vaughan et al., 2020). The rise in HIV rates coincided with an era of economic austerity precipitated by the 2008 recession, during which time funding for the health system overall was reduced by 22% (Health Service Executive [HSE], 2013). Funding for the Gay Men’s Health Service (GMHS) was hit especially hard, and was halved between 2009 and 2014 (Donohue, 2017). Over the same period diagnoses of HIV among gay men almost doubled (HPSC, 2017). While funding for the health service has since been restored, and indeed increased, on pre-2008 levels (HSE, 2019), HIV rates have continued to increase.
Critical public health and the media
As Lupton (1994) has remarked, health and illness states are, in large part, ‘products of social systems and ideological processes’ (p. 58). Critical public health scholars have made the case for a reflexive, interdisciplinary and politically aware scholarship (Dutta, 2010). Print media reporting is especially relevant in such a pursuit because of the role of journalism in setting and framing social, political and policy agendas (McCombs, 2005). In this sense, the media is not just an observer of social and political phenomena, but rather a participant that plays a key function in shaping and constraining public attitudes and political and policy debates. Print media act as gatekeepers of social and political discourse, choosing which topics to cover and exercising editorial power over how such topics are framed. The media thus have a dual function, serving as a conduit to disseminate information, but also acting as institutional players in their own right with the power to construct and frame discourse as they see fit. Consequently, the discourse that is reproduced will often be contingent on who has access to the media, and institutional/editorial choices about which voices to prioritise. Such discourses become impactful then, in the way in which they come to create meaning, define problems, and propose solutions that circulate in the wider community.
Such influence has become all the more powerful given the active role of the media in disseminating information about health and illness (Picard and Yeo, 2011). Moreover, as Hallin et al. (2013) have argued, ‘the production and circulation of biomedical knowledge have increasingly moved from what was construed as a private sphere of doctor/patient communication . . . into the public sphere, where the communicative norms of biomedicine compete and combine with those of marketing, journalism and political debate’ (p. 121). The media remains the main source of information for lay people about health matters (Gould et al., 2009). How health and illness issues are framed by media sources are thus relevant in appreciating how lay knowledge of health matters and health policy is constituted and reproduced. Consequently, print news media is an important data source in social, political and health research (Baumgarten and Grauel, 2009). Print news media is highly consumed in Ireland, with over 80% of the population of approximately 4.9 million people regularly reading news in print and online (Newman et al., 2020). By comparison, only 29% of the population are Twitter account holders, with only 37% of them being active users of the platform (IPSOS/MRBI, 2020).
HIV and media reporting
Given the initial association of the illness with gay men, much of the early coverage of AIDS characterised the epidemic as a ‘gay plague’ (Treichler, 1999). Emerging at a time when the world was becoming ever more inter-connected and neoliberal policies were re-shaping societies, AIDS was the first pandemic in human history to reach a global audience via mass media. The ascendency of Ronald Reagan and Margaret Thatcher had re-invigorated a social conservatism which, aligned with the Christian Right, endorsed a potent anti-gay message. The use of the term GRID (gay-related immune deficiency) at the outset of the epidemic helped in part to construct future conceptualisations of the illness as a disease that was intrinsically linked to gay identities. This was reinforced by early medical speculation that AIDS was caused by something particular to gay life-styles (Greene, 2007). The media, particularly the tabloid press, were keen to capitalise on such accounts of AIDS to bolster the renewed ideological agenda. Roy Greenslade, assistant features editor at The Sun newspaper in the UK from 1981 to 1986 recalled that among executives at The Sun ‘the consensus that informed the debate . . . was that all homosexuals are perverts . . . AIDS appeared to be just desserts for being involved in deviant sexual behaviour’ (Garfield, 1994: 44–45).
Studies of media coverage of HIV since the early days of AIDS suggest that this legacy continues to shape news reporting on HIV and AIDS. Studies in Australia in the 1990s showed how media representations of HIV circumscribed ‘innocent’ victims and ‘guilty’ perpetrators, constructed discourses that presented AIDS as a ‘hidden danger’ (Brown et al., 1996: 1694) and evoked typologies of PLHIV as archetypes of infection that suggested a moral hierarchy premised on the relative risk they were deemed to pose to others (Lupton, 1999). Other studies have noted the decline in reporting on HIV globally throughout the 2000s (Gao et al., 2013; Stevens and Hull, 2013), likely due to the development of antiretroviral (ARV) medications and the growing biomedical normalisation of the condition in the West. In the United States, Stevens and Hull (2013) identified a shift in newspaper coverage of HIV from a domestic issue to an ‘African problem’ (p. 6). They further point out that the disproportionate impact of HIV on African Americans remains under-reported, with existing reporting focussing on individual risk behaviours, rather than on structural determinants. In the UK, analysis of media coverage of post-exposure prophylaxis (PEP) has demonstrated a dichotomisation of social representations of this prevention tool and those that require it – with gay men positioned as careless and undeserving, while healthcare workers were framed as responsible and deserving (Jaspal and Nerlich, 2016). A study on representations of pre-exposure prophylaxis (PrEP), showed a similar dichotomisation, with a discourse of hope at the public health possibilities afforded by PrEP and a competing discourse that constructed gay men as irresponsible, premised on assumptions that this prevention tool would exacerbate and increase risky behaviours among this population specifically (Jaspal and Nerlich, 2017).
This article seeks to contribute to the scholarship on the representation of HIV in the print media outlined above. The aim of this research was to identify and analyse the dominant discourses of HIV found in the print media in Ireland. The research questions that informed the investigation were ‘what discourses exist in relation to press coverage of HIV in Ireland today and how does the media frame people living with HIV?’, and ‘how do these discourses frame understandings of HIV and the nature of the HIV epidemic in the Irish context?’ Using a critical discourse analysis framework, this paper explores how media discourses position HIV and people affected by it, and discusses the public health implications arising from this.
Methods
Data collection
Data collection comprised sampling newspaper articles published in Irish print media over a 10 year period from 2006 to 2016. This period was selected because it is contemporaneous with key developments in HIV research and treatment that have led to a biomedical ‘normalisation’ of HIV, as well as being concurrent with the aforementioned increases in Irish HIV diagnoses, and the economic austerity measures that impacted the health system. The sample of newspaper articles was collected via the LexisNexis database. Inclusion criteria required that articles must:
– contain the word ‘HIV’ or ‘AIDS’ in the headline, so as to be reasonably assured that HIV was the main topic of the article;
– be published in a national Irish publication, so as to be of national significance and therefore part of macro-level discourse;
– be no fewer than 500 words, to have pieces of reasonable length in order to perform analysis.
A total sample of 103 articles that satisfied inclusion criteria was retrieved and included articles from national broadsheet, tabloid and Sunday newspapers (see Figure 1), which had a combined weekly hard-copy circulation figure of 803,180 at the midpoint of the sampling period (News Brands Ireland, 2010). Of the total sample, 73 articles dealt with HIV in a domestic context (Ireland or the UK), and 30 had an international focus, with 14 articles on HIV in Africa and an additional 13 on Russia, China, Thailand and the US, among others. The majority of the sampled articles were derived from the news (n = 29), features (n = 18), health (n = 15) and ‘Ireland’ (n = 14) sections of the newspapers (see Figure 2).
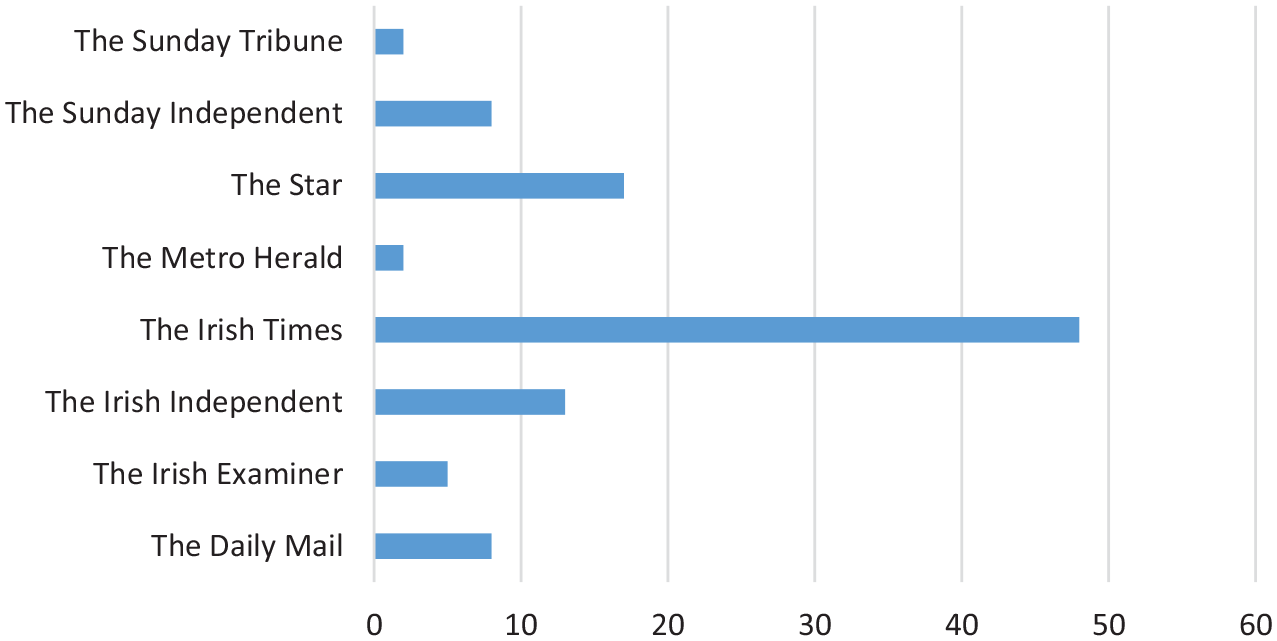
Newspaper titles.
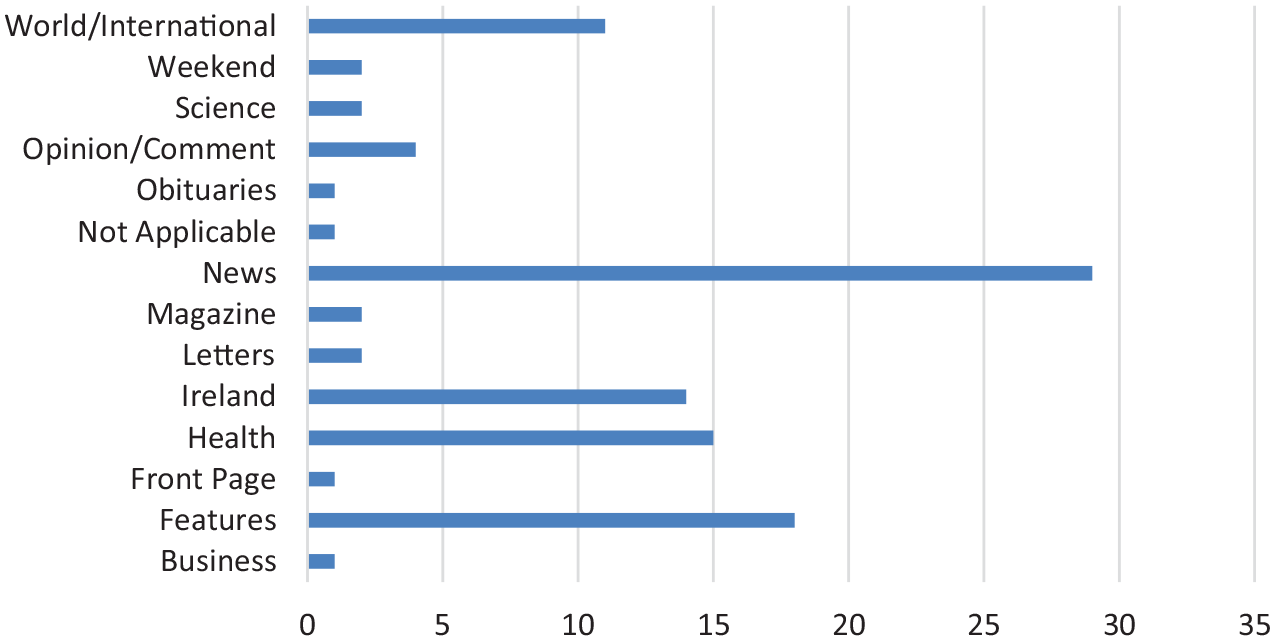
Newspaper sections.
Critical discourse analysis
Critical discourse analysis (CDA) is concerned with examining discourse as social practice and entails a close scrutiny of the formal, contextual and intertextual properties of texts to reveal underlying power relations (Fairclough, 2003). The CDA approach used in this study was derived and adapted from Fairclough (1989). The aim of CDA is to examine and uncover the often subtle ways in which language circumscribes subject positions for social actors, and reproduces and sustains structurally embedded systems of inequality and hegemonic frameworks of knowledge. This method acknowledges the constitutive role of language in shaping social identities, subject positions, social relationships and systems of belief and knowledge (Fairclough, 1989; Foucault, 1982). CDA also recognises that processes of symbolic violence can legitimate and facilitate the reification of norms and practices that implicitly favour the dominant group and marginalise other groups (Bourdieu, 1991).
In this sense, CDA is not a value-free method, nor does it claim to be. As a critical approach, CDA is inherently political and advocates that ‘critical discourse analysts (should) take an explicit socio-political stance: they spell out their point of view, perspective, principles and aims, both within their discipline and within society at large’ (Van Dijk, 1993: 252). This is not discordant with the aims and objectives of public health scholarship more broadly. Like CDA, critical public health approaches challenge and question existing orthodoxies and advocate for structural changes that would facilitate greater social equality and better health outcomes for all (Green and Labonte, 2008). As Schrecker (2016) has argued, what is needed ‘is a political science of health inequalities . . . capable of identifying the relevant macro-micro connections’ (p. 479). As scholars working in the disciplines of Health Promotion [EV] and Social Care [MP] respectively, this approach aligns with our own epistemological and ontological perspectives, and our work continually strives to draw attention to the social and structural determinants that underpin health inequalities. Indeed, the foundational document of Health Promotion, the Ottawa Charter acknowledges the need to recognise obstacles to achieving health parity and to advocate and mediate for actions that will address this (World Health Organization, 1986). Consequently, we agree with Dutta (2010) that ‘. . . the emancipatory politics of healing are embedded in the capacity of health scholarship to challenge and transform structural violence’ (p. 538).
A number of specific discursive features of texts provide insight into how text producers construct knowledge about the world and delineate subject positions for actors represented in discourse (Fairclough, 1989). The key features we examined included: propositional assumptions, or assumptions about what is, can be or will be the case; dialogicality, concerning the presence of specific ‘voices’ in texts; intertextuality, concerning the presence of other texts within a text; ideologies, concerning aspects of text embodying particular world views or perspectives; and modality, concerning the use of modal auxiliary verbs such as ‘may’, ‘might’, or ‘could’ to hedge statements, speculate or introduce elements of doubt or possibility.
NVivo software was used to organise and code data. The analytical process was as follows: First we conducted iterative readings, during which we took notes and discussed the organisation of information in texts, broader themes arising and use of language. Two rounds of coding were subsequently carried out in which texts were coded thematically and then for the discursive and linguistic features outlined above. Initial coding and analyses were carried out by the lead author and reviewed by and discussed analytically with the second author, with any differences in interpretation resolved by consensus. A final round of coding to refine codes and consolidate thematic and discursive analysis was then carried out.
It is worth highlighting a number of methodological challenges that arose in analysing the data and how we addressed these: Firstly, CDA demands that texts are scrutinised for what is not said and who is not included in the discourse, as well as for what is said and by whom. This presented a methodological dilemma as clearly coding for absences is not possible. To overcome this we instead took detailed memos of observations and linked these to the individual texts under analysis. Another methodological challenge we encountered was how to synthesise findings across the relatively large corpus of texts in the sample. We were further wary of potential for confirmation bias given our knowledge and understanding of HIV as a stigmatising condition. In order to address both these concerns, software assisted technique triangulation (Humble, 2009) and limited content analysis (Hsieh and Shannon, 2005) were employed. Certain features of NVivo allowed us to introduce additional analytical techniques to explore and represent the patterns that we observed and, in the process, increase rigour. For example, by exploring the frequency and usage of key terms and nomenclature, to generate visualisations and to cross-reference coding of themes against discursive features using coding matrix queries.
Results
Discourse of risk and responsibility
The dominant discourse identified was of risk and responsibility. Risk was more likely to be associated with biomedical voices and perspectives. Biomedical voices were also more likely to be drawn upon intertextually. The theme of risk was identifiable in just under half of the articles coded (50/103), with 147 direct references to the concept of risk. Biomedical ‘voice’ was the voice most prominently identified, with medical professionals, researchers and scientists most likely to be drawn upon for expert opinion. This was followed by people living with HIV (PLHIV), advocacy/NGO and then official/political (Figure 3).
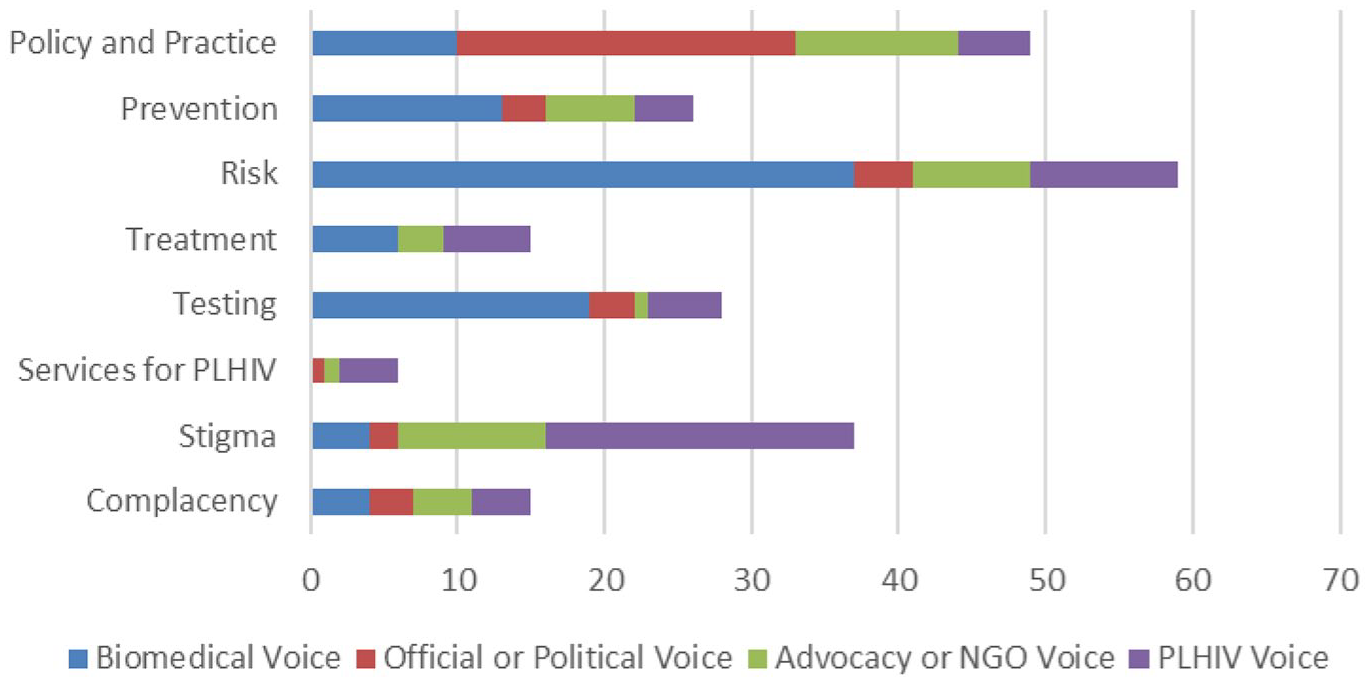
Proportion of voices in a sample of coded themes.
News reports framed rising HIV and STI rates as a consequence of individual risk behaviours, particularly among younger people. The moral positioning of people in relation to the concept of risk was a recurring feature of many texts. Sexual risk-taking was often described in hyperbolised terms, where condomless sex was framed as an act of hubris and recklessness. The dialogicality of such pieces was low, with individuals from these population groups rarely interviewed about their perspectives. Rather journalists relied on expert opinion from physicians, who made assumptions about the motivations and decision-making processes of those framed as sexual risk-takers (emphasis added throughout sample quotes): The recent resurgence of STIs in Ireland indicates that people are taking greater risks, particularly in the younger generation. ‘What we surmise to some extent is that they have grown up in this era of HIV/Aids and either they believe that they are invincible or that it is worth the risk,’ he [clinician] says.
1
One of Ireland’s leading specialists on STIs, has painted a frightening picture of Ireland’s current one-night stand culture where many are regularly indulging in high-risk sexual behaviour.
2
Risk-taking was frequently linked to a lack of personal responsibility, which was often tethered to and operationalised as ‘complacency’. This emerged as a ‘common sense’ explanation in reporting on HIV in the Republic of Ireland to account for the growth in HIV rates. Such assertions appeared to be speculative however, with statements asserting that complacency among individuals was a driving factor frequently hedged, through the inclusion of modal verbs such as ‘seems’, ‘appears’ or ‘might’, or, for example, by posing statements as questions: ‘We have gone from one extreme to another, but has a dangerous complacency set in?’ 3
Two features to emerge from closer analysis of articles that drew on the risk/responsibility frame showed that (i) complacency was attributed to individuals and sub-populations, with young people and gay men especially singled out; and (ii) complacency was linked to a lack of fear of HIV due to the availability of medications, with the assumption that this resulted in cavalier attitudes to sex. Claims included that ‘the message about safe sex . . . no longer seems relevant to a younger generation’
4
and that ‘the successful development of anti-retroviral drug treatments appears to have encouraged many young men to take the sort of risks which only 4 or 5 years ago their counterparts would have thought twice about’.
5
Such messaging was reinforced with quotes from authoritative figures who agreed that ‘. . . there’s no scare factor out there . . . which means less people are worried about it’.
6
Responsibility for acquiring HIV was thus shifted to lie solely with the individual and their lifestyle choices, rather than on social or structural factors: But we must all face the consequences of the choices we have made. And if prevention is better than cure, then surely it’s rational to explain that HIV/AIDS arises because of a choice made, just as lung cancer or COPD may be the penalty for a similar form of recklessness.
7
Young gay men in particular were identified as engaging in risky and irresponsible behaviour. It is worthy of note that two lengthy articles in the sample were centred on the phenomenon of ‘bug-chasing’ – a practice in which people seek to purposefully acquire HIV. While studies have shown that this subculture does exist in the US, there is little evidence to suggest that it is in any way a common or wide-spread practice (Moskowitz and Roloff, 2007). There is no evidence to suggest that it is practiced at all in the Republic of Ireland. Nevertheless, two long reports were carried in sister publications The Irish Independent and The Sunday Independent, two of the best-selling papers in the country. Neither one interviewed participants in this sub-culture, although The Irish Independent article did cite a study on the practice. The authors suggested that such research had ‘only skimmed the surface’ and that future research needed to ‘carry it further afield, especially into areas like Africa’. 8 The Sunday Independent article, titled ‘Ignorant youth deliberately seek twisted “gift” of HIV’, claimed that ‘warped bug-hunters’ were engaging in a ‘worrying new trend’. The same article also drew attention to the risks of HIV to the wider public, stating that: ‘All the old myths that HIV and Aids (sic) are the exclusive preserve of gay men and intravenous drug users are nothing but fairy tales to give the common upstanding citizen a sense of security’, while claiming (erroneously) that ‘the rates of heterosexual infection [in Ireland] have risen by over 400pc in the past five years’. 9 Despite being more apocryphal tale than common practice, both these articles substantially over-state the extent of this as a problem, while implicitly suggesting, rather improbably, that such practices may help to explain high levels of HIV elsewhere and among diverse populations.
Notably, on the rare occasions young gay men’s voices were included, these challenged the idea that young people were wilfully reckless or complacent, rather hinting at a prevalence of misinformation, a lack of knowledge and a lack of visibility: ‘People think it’s like leprosy or something, that you can tell if people have it’ [Declan, 19]. ‘After getting tested, I’ll never do it [have unprotected sex] again. But I didn’t know. I’m not stupid, but no one ever told me . . . I’ve never seen an ad in the mainstream media about gay men and protection’ [John, 21].
10
Interestingly, whereas there was a lack of focus on structural explanations for rising HIV rates in the Irish context, the opposite was true of articles that had a focus on HIV in an international context. This was particularly noted in respect of reporting on the HIV epidemic in Africa, where responsibility for high numbers of infections was rather attributed to ‘a lack of political commitment by past governments’. 11 Topics covered in the international articles included funding for prevention programmes, access to treatment and prevention, 12 legal and policy frameworks 13 for addressing the HIV epidemic, the impact and effects of inequality, stigma and harm reduction measures 14 and the roles of government, 15 the media and aid agencies. 16 Consequently, while lack of personal responsibility was posited as the primary cause of the rise in new diagnoses in the Irish context, political and institutional failings 17 and a lack of coherent policy frameworks were frequently attributed as the drivers of epidemics in Africa, Russia and elsewhere. 18
Constructing the ‘other’
Within both domestic and non-domestic articles, there was a tendency towards constructing people living with and affected by HIV as ‘other’. One way in which this occurred was through implicitly framing people living with HIV as unhealthy and vectorising them as potential sources of disease. An article on pre-exposure prophylaxis (PrEP) in Ireland described candidates for PrEP as ‘healthy, but high risk’, framing HIV negative people in a way that sets up a dichotomy that necessarily draws on the reader’s assumptions that people living with HIV are ‘unhealthy’. 19 Such framings suggested and reinforced a hegemonic biomedical understanding of health, which privileges the absence of disease as the gold standard for what it means to be healthy, rather than overall well-being. Similarly, a feature piece described a pregnant woman living with HIV as looking ‘like any other healthy mother’, before stating she is ‘a carrier of a potentially deadly virus which might be passed onto her unborn child’, and implying that her pregnancy is a ‘reckless’ act. 20 The use of such language, in addition to suggesting that the mother was lacking in sound moral judgement, further perpetuated an anachronistic representation of HIV that posited the bodies of people living with HIV as sites of disease and contagion.
This othering was also apparent in non-domestic articles on HIV. One such piece, which ostensibly explored the role of the media in reporting HIV in Zambia opened with a paragraph in which the writer described the difficulties of engaging readers on the topic of HIV in Africa. 21 She writes: ‘the subject and location seem so distant from us in every sense’ (emphasis added). In the following paragraph she questions what HIV looks like in ‘the place where it is a daily reality?’ This raises questions: who is the collective indicated in the pronoun ‘us’? Is the subject matter really that irrelevant to a Western readership or just some members of that readership? Who then is included and who is excluded from this ‘us’? Is the West not a place where HIV is a ‘daily reality’ also? With her statements the writer is making both propositional and existential assumptions about her readership, about who is and who is not affected by HIV, about how and where HIV occurs and about who counts in the collective ‘we’ or ‘us’.
Similarly, a piece in The Irish Times 22 quite clearly illustrated how HIV-positive identities may be positioned in relation to the ‘other’ in ways that emphasise their somatic and moral deficiencies. The writer describes receiving a positive HIV test while he was living in Africa, recounting his thoughts and feelings as he awaited results of a confirmatory test, which turned out to be negative. In considering how he may have acquired the virus, the writer positions himself passively, rather attributing agency to his [African] girlfriend, stating: ‘It has to be her. She has infected me’. He imagines the reaction of his family back home, saying: ‘I feel ashamed. I’ve let them down’, indicating his diagnosis represents a moral failure. He jokes with his friend that he is ‘no Mick Jagger’, a joke that draws on assumptions about male sexuality and the stereotype that HIV is acquired via prolific and promiscuous sexual behaviour. When he finally receives the news that he is in fact HIV negative, he is relieved and elated, stating: ‘For three days I was HIV-positive, and now I am healthy. I am normal. I am free’, with the clear implication that such things are not possible if living with HIV.
Anachronisms and ambiguity – HIV through the lens of AIDS
Another feature identified was a tendency to reflect HIV through an historical AIDS lens. This had the effect of producing conflicting or ambiguous messages. Many of the longer domestic feature pieces and reports sought to provide a comprehensive overview of the condition. This would typically include providing epidemiological information specific to the Irish context, the history of HIV, and its current status as a treatable condition. However, beyond mentioning that HIV was now a treatable chronic condition, little or no detail was provided on other contemporary positive biomedical developments. For example, in the sample as a whole, there were only four references to treatment as prevention (TasP),23–25 only one specific reference to post-exposure prophylaxis (PEP), 26 and only one article on PrEP. 27 Rather than focus on the positive aspects of current daily realities of life with HIV, writers frequently employed language that implicitly conflated HIV with AIDS, reproducing obsolete portrayals of HIV. One way in which this occurred was using negative frames to describe HIV in terms of what it is not. Phrases that were used commonly in this context were the collocations ‘death sentence’ 28 or ‘fatal 29 or ‘terminal’ 30 condition. The ‘death sentence’ metaphor in particular is rather loaded for its connotations with crime and punishment. Additionally there is the implicit suggestion that if HIV ‘might no longer mean a death sentence’ 31 then it must be a life sentence. Indeed, in two of the texts this exact phrase was used.32,33
Another way in which this occurred was via often graphic descriptions of symptoms that people with AIDS experienced, 34 with expositions on ‘agonising deaths’ that were suffered in the past 35 and doom-laden descriptions, such as that in the headline of an article about singer-songwriter John Grant, described as ‘living with the spectre of being diagnosed HIV positive’. 36 Certainly, descriptions of HIV as a condition that people can live well with were rare by comparison and were often minimised elsewhere. Largely absent of other frames of reference to describe the contemporary reality of life for the majority of people with HIV and, given the tendency to position people living with HIV as ‘unhealthy’, this created a sense of doubt and ambiguity as to the potential to live well with the virus. This was compounded by a pattern of conflicting and contradictory messages, observable, for example, in a long feature in The Irish Times. The writer states in the third paragraph that HIV is ‘no longer a death sentence’, yet ends the piece with the quote: ‘People think, “Ah, I’ll do it just the once,” but taking that one chance could be your last’. 37
The frame of AIDS as moral failure alluded to above was exacerbated by the constitution of HIV positive identities as reformed subjects. A HIV diagnosis was positioned as a ‘turning point’ in the lives of people affected.38,39 Many of the people living with HIV who were featured or interviewed as part of stories on HIV were often volunteering or otherwise working to support other people living with HIV and to educate others about HIV prevention – practices which facilitated the creation of a certain narrative about their lives.
40
For example, an obituary for a prominent AIDS activist described her ‘journey from a comfortable middle-class background in south Dublin into hell, then back again to a form of redemption which inspired thousands of others’.
41
At the same time, there was an implication that such practices acted as a form of penance, with the author of the obituary employing an interesting syncretism of religiously-inflected discourse with the sterile, clinical language of bio-medicine, disclosing that the woman had acquired HIV through ‘extra-marital heterosexual intercourse’. Such a framing is suggestive of a sinner or saint dichotomy, mirroring earlier HIV media discourses that circumscribed guilty and innocent victims. Certainly, this framing reinforced the concept of HIV as a moral failing, particularly given the discursive legacy of AIDS, as well as the contemporary tendency towards representing HIV within discourses of risk and responsibility. Ironically, one of the clearest articulations of this ‘redemption’ theme in the sample was found in a piece on actor Charlie Sheen, specifically positioning him diametrically to it: Not that he intends to become a reformed character. No . . . Charlie Sheen doesn’t believe that HIV has the power to make him a better person. Nor does he seem to want it to. And he knows that this flies in the face of the modern belief that bad luck and disease and disability and tragedy are given to us in order that we do some good with them.
42
Discussion
Analysis of the texts in our sample demonstrated how HIV was constructed through discursive lenses that emphasised risk and invoked notions of personal responsibility. The discourse of risk and responsibility was largely focussed on young people and gay men, for whom subject positions as complacent and irresponsible social actors were textually delineated. This echoes findings by Jaspal and Nerlich (2017), whose analysis of PrEP in the UK press found similar social representations of gay men which drew on and reproduced stereotypical characterisations of gay lifestyles as sexually promiscuous. Such representations implicitly invite judgement and stigmatisation, particularly in a place such as Ireland where social and cultural values have historically been grounded in conservative Catholic traditions (Ferriter, 2009). Furthermore, this discourse also aligns with what Clarke et al. (2003) have termed ‘biomedicalisation’ – a process that describes the social transformation of health and medicine from around the early Eighties. Among the key aspects highlighted by biomedicalisation is an emphasis on health in terms of risk and surveillance. Within this paradigm health is reproduced as a moral obligation, accompanied by attendant responsibilities for increasingly complex rituals of maintenance, self-regulation and safe-guarding against risks. Where acquiring HIV is constructed as the consequence for neglecting to be vigilant of one’s health, this signals an additional and discrete moral failure in the care of oneself (Foucault, 1984). Such representations have clear implications for public health, given the stigmatising impact they may have both for young gay men and for people living with HIV. HIV-related stigma is, for example, associated with decreased rates of testing and higher life-time risk of acquiring HIV (Pitpitan et al., 2012), while stereotypes about HIV are known to decrease perceptions of risk (Earnshaw et al., 2012). Adherence to ARV medication is also negatively affected by HIV-related stigma, resulting in adverse health outcomes for PLHIV (Kingori et al., 2012), as well as having implications for onward transmission of the virus (Katz et al., 2013). Healthcare professionals should therefore be cognisant of the potential of media discourses on HIV to invoke stigma among people living with and affected by HIV, and seek ways to counteract this.
As Douglas (1994) has observed, ‘the modern risk concept, parsed now as danger, is invoked to protect individuals against encroachments of others. It is part of the system of thought that upholds the type of individualist culture which sustains an expanding industrial system’ (p. 28). It is perhaps unsurprising therefore that the discourse of risk was tethered to a discourse that emphasised individual personal responsibility, aligning with findings of similar studies in the UK and the US (Mowlabocus, 2020; Stevens and Hull, 2013). It is significant, however, that coverage of HIV internationally drew attention to structural issues driving the epidemic, whilst coverage of HIV in the domestic context eschewed such critiques. The disparity in reporting is remarkable given that Irish journalism is not generally shy of levelling criticism at the government or the health system, and there is ample information in the public domain to support such analysis. Policy and practice evaluations over several decades have found coordination of services to be ‘erratic’ (Seery, 1999: 10), with professionals reporting ‘ad hoc and inequitable’ delivery (Lynch, 2009: npn). Despite this, a mid-term review of the 2008 National HIV Education and Prevention Plan noted ‘no progress in the implementation of actions to expand opportunities for HIV screening and testing’ (National AIDS Strategy Committee [NASC], 2010: 4). More recent reports show Ireland was one of only three countries in the European Union/European Economic Area with major gaps in testing for all key affected populations, including young gay men (European Centre for Disease Prevention and Control [ECDC], 2017) and one of only eight countries reporting no national testing guidelines (ECDC, 2019).
Characterisation of the HIV epidemic in Ireland as a matter of individual responsibility and complacency is thus divorced from a structural context in which the capacity of citizens to take care of their sexual health is considerably reduced. Responsibility both for acquiring HIV and for the burgeoning epidemic is disproportionately shifted towards the actions and behaviours of individuals and specific populations, rather than on policy-makers and healthcare providers. Refracted through this lens, the framing of the epidemic and the individual acquisition of HIV reconfigures the rhetoric of guilt and innocence that characterised much of the media reporting of AIDS earlier in the epidemic, rather reflecting a specific ideological position that seeks ‘to focus blame on those who are “guilty” for their illness’ and thus ‘deflect attention away from the social context of the spread of disease’ (Sacks, 1996: 70). Such a discourse occludes the structural underpinnings of pandemics in which structural violence, social inequality, gender-based violence, poverty and stigma are key drivers and the reason why HIV diagnoses are differentially distributed along lines of class, race, gender and sexuality (Farmer et al., 2006; Gruskin et al., 2014). Given the role of the media in agenda setting, obscuring this reality may have a negative effect on decision-makers tasked with crafting policy solutions to effectively address the HIV epidemic. This highlights the need for researchers working on HIV and other infectious diseases, to engage constructively with policy- and decision-makers and seek new ways to translate knowledge to maximum effect.
Throughout the data, various strategies of othering were observed. These included drawing delineations between HIV positive and HIV negative people as ‘unhealthy’ and ‘healthy’ respectively. This was reinforced by tethering the idea of HIV positivity to anachronistic representations of living with HIV via imagery of sickness, infectiousness and death. In this way the results mirror those of Jaspal and Nerlich (2020), whose study of media narratives of the Daryl Rowe case in the UK, showed how media representations of HIV in that context engendered fear and stigma by reproducing fatalistic impressions of HIV as an inevitably ‘destructive disease’ (p. 14). While such representations have public health implications specifically for HIV in respect of creating barriers across the HIV care continuum (Gesesew et al., 2017), there is also a broader question around the function of discourses that assert a singular biomedical conceptualisation of health and the impact that these may have on people with disabilities or people that live with health conditions other than HIV. The Covid-19 crisis, for instance, has seen much news reporting on deaths associated with this new virus occurring in people with ‘underlying conditions’. As has been pointed out by scholars of disability studies, the ‘casual brutality’ of these discourses implicitly signals that such lives are ‘expendable’ (Abrams and Abbott, 2020: 169). This has clear bioethical implications in the context of a pandemic where policy-makers and healthcare providers must make decisions regarding allocation of resources in often over-burdened and under-resourced health systems. Viewed through this perspective, discourses that dichotomise the ‘healthy’ from the ‘unhealthy’, cease to be merely descriptive accounts of a material biomedical reality and rather become a moral taxonomy of which bodies are disposable. This raises the question that Judith Butler has posed about forms of political exclusion and who counts as ‘the people’. A reformulation of this question in the context of HIV – or the Covid-19 pandemic – might be whose ‘health’ counts in a politics ‘that produce conditions of systematic negligence’, which disproportionately affect individuals with less access to power (Butler, 2015: 11)?
Limitations
There are some limitations to our study to which we wish to draw attention, and which may help to inform future research. Firstly, our sample drew entirely on articles from the print media. While many of these publications do have an online presence, we omitted from our sample publications that operate solely online. It should be noted that a strength of the research is that the majority of the articles were derived from the most highly circulated and influential papers. However, as print media declines, future research on media discourse and HIV (or health more broadly) may wish to consider the additional inclusion of online publications. We also chose not to include analysis of discourse on online platforms such as Twitter and Facebook. This was in part because the influence of these platforms in agenda setting in the Irish context is unclear. Nevertheless, given that audiences are increasingly consuming news media via these platforms, as well as the documented role of social media in disseminating false and misleading information about the Covid-19 pandemic (Allington et al., 2020), this would seem a fruitful place for future analysis of HIV and other health-related discourses. A final limitation is that findings may not be applicable to other contexts, as analysis of texts was limited to those published in the Republic of Ireland only. Future research may wish to explore if similar discursive regimes exist elsewhere.
Conclusion
As an important cultural and political actor, the print media play a key role both as the conduit through which dominant societal views are disseminated and as interlocutors in their own right. This article argues that in unpacking the discourses of HIV that occur in the print media, a pattern emerges in which PLHIV are frequently positioned as somatically and morally deficient via discourses of risk and responsibility. This is reinforced by anachronistic representations of HIV and AIDS and through constructions of the ‘other’. Furthermore, it is clear that the epidemic itself is framed in ways that reflect a dominant ideological paradigm in which health becomes a matter of individual responsibility and the role and function of the State in creating the right conditions for citizens to attain good sexual health is set aside. Inasmuch as dominant biomedical and neoliberal discourses circumscribe HIV positive subjectivities in ways that emphasise the otherness of the HIV-positive body, this reflects and reproduces a social arena in which the stigmatisation of certain groups of people is a fundamental component. By discursively enshrining the notion of hierarchical differences between social groupings into the cultural/discursive fabric in such a way that it appears natural and taken-for-granted, processes of stigma and discrimination are (mis)recognised as ordinary and legitimate rather than arbitrary – but necessary – operations of power that facilitate the existence of an asymmetrical social order. With the emergence of a new ‘mythological menace’ (Sontag, 1988: 148) in the shape of Covid-19, we may expect these processes will continue in reconfigured, yet familiar, forms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.