
Abstract
The dominant notion that exercise is medicine puts a strong normative emphasis on individual responsibility for participation in sport and physical activity. The aim of this article was to explore how people with type 2 diabetes, a condition strongly linked to lifestyle behaviour both in origin and in management, translate this notion into their daily life. Based on a critical narrative analysis of stories of 18 Dutch people diagnosed with type 2 diabetes collected between 2012 and 2016, we found a range of meanings given to sport and physical activity. In addition, almost all respondents seemed to subscribe to the notion of exercise as medicine on a general level, either quite explicitly or in more subtle ways, for example, elicited by the interview setting. However, they employed different strategies to negotiate with the translation of this notion into their daily life, ranging from (almost) total acceptance to resistance. In addition, nearly all stories revealed mostly negative experiences with care and professional support regarding the uptake or continuation of sport or physical activity participation after diagnosis.
Introduction
Physical activity and exercise, including sports, 1 are considered important instrumental promises in relation to health. Based on numerous medical and epidemiological studies pointing towards the health benefits of regular physical activity (e.g. Pedersen and Saltin, 2015), this is increasingly translated into popular discourses, like ‘Exercise Is Medicine’, in healthcare settings and beyond (Cairney et al., 2018; Cheng and Mao, 2016). This medicalization of physical activity – a redefinition of a daily life aspect as medically essential (Malcolm, 2017) – is further supported by studies in leading medical journals about a so-called ‘physical inactivity pandemic’, warning for ‘harmful health consequences’ and increasing healthcare costs (Kohl et al., 2012; Pratt et al., 2012; see Piggin and Bairner, 2014).
A particularly interesting example is type 2 diabetes, a chronic condition that has become firmly linked to physical inactivity and overweight in both its origin and management (O’Donnell, 2015; World Health Organization (WHO), 2016). Consequently, all clinical type 2 diabetes guidelines emphasize the importance of exercise during treatment (Colberg et al., 2010; IDF, 2017; NHG, 2013). Therefore, it is to be expected that people with type 2 diabetes are frequently confronted with discourses emphasizing that regular exercise is good for them.
In their critical consideration, Cairney et al. (2018) argue that using or promoting exercise as medicine is ‘a practice of faith grounded in morality’ (p. 392). Supported by a firm body of scientific knowledge, exercise is framed as an effective means to live healthily. With this, the normative aspects often remain unstated or obscured because ‘the (in)decision to be physically (in)active is projected as an essentially personal and individual (ir)responsibility’ (Malcolm, 2017: 88). This resonates prevailing neoliberal discourses of healthism that place the responsibility to be(come) healthy at the level of the individual (Baum and Fisher, 2014; Crawford, 2006).
It is unknown how people with type 2 diabetes perceive and act upon discourses emphasizing the importance of regular exercise and individual responsibility in diabetes management (Kristensen et al., 2016; Wiest et al., 2015). Therefore, the aim of this article was to explore how Dutch people diagnosed with type 2 diabetes translate these discourses into their daily life.
A critical narrative approach
Storytelling offers people the opportunity to reflect on, make sense of and connect events to give experience meaning (Gubrium and Holstein, 2009; Riessman, 2008). Although embodied experiences of illness are unique to an individual, these are only made meaningful in the social context, where certain discourses and prominent types of narratives prevail (Abma, 1998; Gubrium and Holstein, 2009). In constructing their story, individuals are attracted more towards some narratives than others. These comprise a sort of inner library – a body of stories one is familiar with and shares with others – as part of a narrative habitus that serves as an unconscious basis for storytelling (Bourdieu, 1984; Frank, 2010).
Healthism, for example, is presented as a discourse that constrains and enables daily lives, albeit in largely unconscious ways because of its close alignment with the neoliberal emphasis on individual responsibility (Wiest et al., 2015). In this way, it is ingrained in the narrative habitus. However, as healthism, and the prescribed lifestyles, primarily fit with middle-class norms on health and healthy living (Greenhalgh and Wessely, 2004), it tends to privilege certain groups over others (Cairney et al., 2018; Jaye et al., 2018; Wiest et al., 2015).
Moreover, individual stories often resonate medical narratives, for instance, by the integration of jargon and science (Frank, 2013; Jaye et al., 2018; Kristensen et al., 2016). From the early 20th century onwards, when type 2 diabetes became increasingly common among the lower social strata instead of the higher, the accompanying medical lexicon became to centre on control and management and underlined diabetes management to be a private matter requiring strict adherence to lifestyle advice with physicians in control over diabetes outcome policies (O’Donnell, 2015). In addition, self-management education and support became important healthcare domains (e.g. Beck et al., 2017). Healthism echoes in this shift from the doctor as a protagonist in treatment (cf. Frank, 2013) towards the patient being responsible for diabetes control in daily life.
Although the narrative habitus sets certain limits, individuals can take various approaches to stories, interpret them differently and challenge or resist dominant narratives in artful and creative ways (Bourdieu, 1984; Fleetwood, 2016; Frank, 2006, 2010). For instance, individuals are found to blend their interpretations and perceptions of healthism in manners that work for them in their daily life, using strategies like negotiation, resistance, ambivalence and zealousness (Jaye et al., 2018; Kristensen et al., 2016: 487; Wiest et al., 2015).
Moreover, the process of defining which story does (not) fit is shaped by embodied experiences, and vice versa: embodied experiences are dependent on the stories one selects and rejects, and, at the same time, these affect embodiment, producing more stories that further predispose someone towards certain stories and not others (Frank, 2006). For instance, exercise can offer a means of controlling diabetes and hence reinforce the appeal of the dominant narrative. However, embodied experiences with diabetes may also challenge physical abilities that were formerly taken for granted (Corbin, 2003; Frank, 2013) and prevent someone from continuing sport participation. These experiences impact the story a person tells.
Methodology
This study is part of a larger research project, Sport in Times of Illness, for which the requirement of full medical ethical approval was waived by the Institutional Review Board of the VU Medical Centre in Amsterdam. This article is based on a narrative analysis of interviews with 18 Dutch people diagnosed with type 2 diabetes (see Table 1). All names are fictitious.
Characteristics of the respondents.
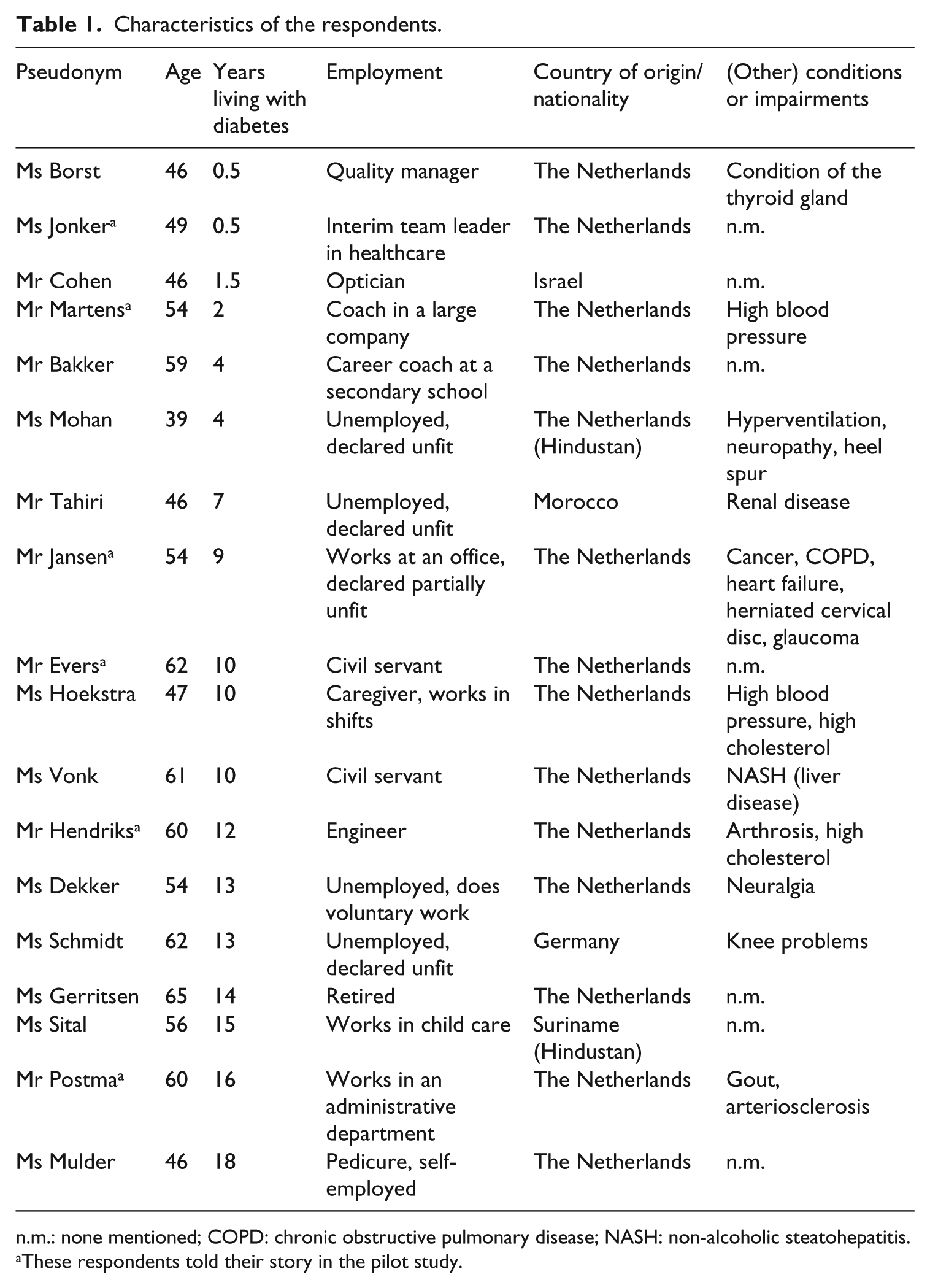
n.m.: none mentioned; COPD: chronic obstructive pulmonary disease; NASH: non-alcoholic steatohepatitis.
These respondents told their story in the pilot study.
Data collection
Six interviews were conducted during a pilot study in 2012 (Van den Berg, 2012). Their transcripts were included during analysis. The other interviews were carried out by the first author (M.S.) between 2014 and 2016. Eight participants were recruited through an advertisement in a local newspaper in Amsterdam (over 400,000 households) asking for people with type 2 diabetes who wanted to tell about their experiences. A gift voucher of €15 was offered as an incentive. With this, we aimed to include respondents with different cultural, socioeconomic and sport/exercise backgrounds in order to collect a broad range of stories. Four participants were included through our network. All were informed about the study’s aims and ethical aspects – such as confidentiality and the possibility to withdraw – in writing and face-to-face before they provided informed consent.
The interviewer started by saying, ‘You have diabetes, can you tell me what happened?’ Some topics, such as living with diabetes, healthcare experiences and the role of sport/physical activity before and after diagnosis, were asked later if the respondent did not mention them spontaneously. Respondents were encouraged to take their time in telling their story and not to expect many questions (Nijhof, 2000). Near the end, respondents were asked to visualize their life at different moments, to reflect on what they had just told. This allowed the interviewer to ask further questions.
Most conversations took place at the respondents’ home. One arranged for a private room at his work and another wanted to meet in a public area. The mean duration was an hour (30–180 minutes). The interviewer wrote a reflexive account after each interview, describing the setting, atmosphere and interaction; what was said off the record; and her feelings about the conversation. All sessions were audiotaped and transcribed verbatim by the interviewer.
Data analysis
Data analysis started at the level of each interview. The interviewer wrote the story down in the narrator’s words and order. This was concluded by an initial interpretation and, together with the transcript, discussed with another researcher (A.E. and/or T.A.). This account was sent to the respondent as a member check. A few did not respond after a reminder, some made some minor textual corrections, but most stated that the account reflected their story well.
We were aware of certain complexities in member checking. For instance, respondents might not be interested or reluctant to disagree (Sandelowsky, 2008). Therefore, we were careful in our descriptions, tried to write comprehensible theoretical informed interpretations and added that reactions were not obliged. We strongly feel that this extensive procedure strengthens our analysis, as it prevented us from ‘simply gather[ing] data on others to fit into our own paradigms once we [were] safely ensconced in our university libraries ready to do interpretation’ (Borland, 1991: 73). More importantly, we wanted to ‘take our work back’ to the respondents because of ethical reasons (Riessman, 2008: 198) and offer them an outsider reflection on their story. 2
In our narrative approach, we studied each story as a whole, including its tensions, complexities and contradictions (Riessman, 2008). We paid attention to the plot structure by looking at character, acts, context and goals (Murray and Sools, 2015), with a focus on the integration of sport/physical activity practices and embodied experiences. Moreover, we were attentive to emotion, phrasing, temporal orientation and co-construction of the story (Riessman, 2008; Sparkes and Smith, 2005).
During data collection and analysis, we met regularly to discuss the stories and consider them from our perspectives of medical and sport sociology (M.S.), critical sport scholarship (A.E.) and medical humanities and care ethics (T.A.). Moreover, we reflected intensively on how our social positions might impact the analysis (Stuij et al., 2019). We gradually moved from individual stories to an overall analysis, in which the transcripts of the pilot study were included. In this process, we tried to understand the different plot structures to illuminate how the respondents related to and negotiated with the notion of exercise as medicine.
Findings
Many respondents told about a period after diagnosis when they searched for the right type and amount of medication before they felt able to more or less control their blood sugar level without excessive side effects. Most of them also made some lifestyle changes, especially regarding their diet and exercise. These stories were about finding a new balance in a life with diabetes and strongly preoccupied with control and management (Karas Montez and Karner, 2005). For more than half of the respondents, this resulted in a life in which diabetes was always there, but not as a real impediment, as Ms Gerritsen (65/14y: 65 years, 14 years with diabetes) explained: ‘Diabetes is part of my life, but it doesn’t have a real impact anymore. I know I have it, and I need to take it into account, but apart from that, it’s in the background’. Nonetheless, what this required varied from person to person.
Almost all respondents considered sport and/or exercise means ‘to take diabetes into account’ on a general level, subscribing to dominant discourses emphasizing that exercise is a type 2 diabetes medicine and individual responsibility. However, the stories illustrated many different ways of translating these discourses into daily life, ranging from (almost) total acceptance to resistance and subtler gradations in between. These are captured in seven different storylines below. Intertwining these storylines, nearly all stories revealed mostly negative experiences with healthcare and support in becoming active (again) after diagnosis.
1. Appropriating exercise as medicine, but not the prescribed standard
Ms Borst (46/0.5y) felt uncomfortable with the message of her healthcare professionals after she was diagnosed: she had to start on medication, and this would doubtless increase in the future because ‘diabetes was in [her] family’. She also could no longer continue her fitness routine and asked her gym manager for advice. Based on a scientific study, they developed a schedule that worked for her: three weight training sessions a week ‘to increase the insulin-like growth factor 1 (IGF-1) hormone levels, which sort of replaces the insulin and helps to stabilize your sugar’ and a training session on an empty stomach once every 2 weeks to ‘clean [the] liver for the rest of the week’. To ensure that her body ‘continued to respond to training’, she changed her weight lifting programme every 4 weeks: By training the opposite muscles and changing the tempo, your body is used differently and with this training, my sugar is stable throughout the weeks. […] For me, it’s exercise as medicine. Instead of medication with side-effects, I do a work-out three times a week.
Ms Borst trained five times a week before her diagnosis, and it took her little effort to adjust her schedule. She used a scientific, systematic approach to get the results she wanted: she kept track of her blood glucose levels before and after training, experimented with different loads and used an app to note her exercise and eating behaviour. She adopted quite a mechanistic view of the body in which exercise – through the production of IGF-1 hormone – ‘fixed’ a failure of the pancreas (Frank, 2013). This approach seemed to fit with what Jaye et al. (2018) call zealousness. The embodied experiences of Ms Borst matched with the notion of exercise as medicine: The way I live now, I live like I did before I was ill: being active and able to do the things I want’. Furthermore, she expressed a feeling of certainty regarding her approach: ‘as long as I can keep on like this, my diabetes won’t trouble me.
Ms Borst was the only respondent who fully embraced the exercise is (the only) medicine thesis. However, she resisted the standard exercise advice for diabetes prevention: ‘[Many people] are just on the cross trainer, three times a week for an hour, and think they do great. Just like I did, but I got very ill nonetheless’. With this, Ms Borst questioned and appropriated the standard advice.
2. Exercise is too demanding to implement as medicine permanently
The requirements of diabetes management were not easily fulfilled by everyone. This is illustrated by the story of Ms Hoekstra (47/10y), who alternated between greater and less control. She lost 11 kg through a 6-month fitness programme, which enabled her to cut her medication in half. She hated the gym but noted the positive effects. However, when the programme ended, she was unable to continue the four intensive training sessions a week on her own, with her irregular shifts at her physically demanding work as a caregiver and adolescent daughter at home. She also noticed she was active during work all day: ‘Sitting down is out of the question. You would expect I get my exercise, but apparently, this is not the exercise you need’. This illustrates a further refinement of the exercise as medicine notion.
By the time of the interview, Ms Hoekstra had regained 6 kg and her ‘sugar level was way too high’ again, but she felt unable to do anything about it. She did not feel she had found a balance after 10 years of living with diabetes: ‘Sometimes I’m doing reasonably well, sometimes totally not’. Because her internist always seemed to have so little time, she did not talk about this with him or dare to ask for help. Her living conditions, previous exercise experiences and socioeconomic status seemed to interfere with her wish to manage her diabetes by doing exercise (Baum and Fisher, 2014). Therefore, exercise seemed to be an impossible necessity for her.
Mr Martens (54/2y) also alternated between being in and out of control, although he ascribed this to his dietary habits mostly. At the moment of diagnosis, he was not active, but the spectre of his mother who died from diabetes-related complications made him change his lifestyle: [I did not like exercise,] but that has changed! I started to lose weight and got on that home trainer and cross trainer [that I kept in the attic]. And I still do so six days a week. Still. At a certain moment I started to lose weight. But I gained weight as well. So I wanted to take it up again. That’s why I made another appointment with [a dietician]. So, I started to do exercise and I felt I was losing weight quite quickly, but my sugar level also plummeted because of the exercise. So I knew, with the Sword of Damocles of my [diabetic] mother above my head, I thought: darn it, that won’t happen to me. Look, if something happens, it happens. But something that you can control yourself, I try to prevent.
Exercise seemed to have become a new necessity in the life of Mr Martens, who clearly subscribed to the notion of individual responsibility. However, his whole story was imbued with the difficulty of maintaining constant control over his glucose level and weight. His use of both past and present tense underlined this and made it difficult to follow his exercise notions and actual behaviour. He systematically kept track of his behaviour, weight, glucose levels and feelings in a diary he showed during the interview. After losing more than 10 kg, he could do without medication for a while, but then ‘things sneaked in, that’s purely my own doing’, and he noticed the symptoms – thirst, fatigue – himself. He repeatedly emphasized his need for support: ‘I know for sure, when I have a good dietician, I will get rid of those medicines again’. But at the moment of the interview, such support was not covered by his health insurance.
At times, both Mr Martens and Ms Hoekstra managed to control their diabetes, offering hope for a more balanced life. But their stories also radiated despair and fragility, mostly because they were not able to successfully self-manage their diabetes at all times. Both acknowledged they could not keep control over their diabetes on their own; however, there seemed to be no prospect of long-term professional support, and they seemed not able to organize such support themselves as Ms Borst did. This emphasizes their individual responsibility.
3. When exercise used to be more than medicine
The notion that exercise is medicine frames exercise as a means to (re)gain health, but leaves other meanings, like enjoyment, performance or social aspects, largely aside (Cairney et al., 2018; Malcolm, 2017; Wiest et al., 2015). Indeed, the ‘Exercise Is Medicine’ proponents put it the other way around by stating that ‘regular exercise can be fun, if you let it be fun!’ (Jonas, 2009: 7), implying that exercise is more important than or comes before fun. However, embodied experiences with diabetes can also interfere with taken-for-granted physical abilities (Corbin, 2003), hindering someone from continuing sport participation. This might result in a confrontation with formerly important meanings of sport, like fun. Ms Dekker (54/13y), for instance, recently had too much pain in her legs to continue horse riding, something that made her emotional during the interview: That is what hurts most […] you don’t have the fun anymore, but I also have to do some extra effort to make up for that part of my body [i.e. glucose regulation], you know? And it will never be that fun anymore. That is the pain, it really is pain.
She told about the present with references to the future and past. Throughout her story, feelings of loss clearly emerged, for instance, related to physical abilities and activities that used to be important for her. However, she did not ask her healthcare professionals for help because she had overall negative experiences with them: ‘You have to be lucky to meet the right professional’. 3
For Mr Jansen (54/9y), who also had cancer, chronic obstructive pulmonary disease and heart failure, meanings and possibilities also changed. He used to be a member of a cycling club, but resigned because he could not keep up with them – as ‘that would not be wise’ – and still missed the company. For him, sport is a ‘nice addiction’, especially related to performance. In fact, he was particularly angry about and resisted the widespread image of the ‘lazy, fat diabetic, that does not do sport’, because he used to run marathons and participated in the Dutch Elfstedentocht, a 200-km ice-skating tour. However, at the moment of the interview, he experienced a kick when doctors were astonished about his performance in the bike test. Although he participated in sport all his life, its meaning seemed to have shifted from sport-related to exercise-related performance, with health promotion as a major goal now.
4. Exercise as an unfulfilled promise
Besides a shift in meanings, there was another layer in the story of Mr Jansen, one that challenged the promise of exercise as a medicine. Although his diabetes was under control now, he said, Sporty [all my life], yes, and still all those problems. […] It’s a matter of time. Your pancreas is going to do its work less and less. You can say: go on doing sport. But in the end, you lose and have to give in. I know this time is coming, but I postponed it for quite a long time [by being sporty].
This quotation clearly illustrates the unpredictability or even the predictable decline of the body. Mr Jansen directly referred to a time in the future when loss seemed inevitable. For him, sport offered a means of postponing this. However, he received contradictory advice from his doctors: one told him to do less, another that he could do more. He concluded by saying he had to work this out for himself ‘because in the end, nobody knows’.
The unfulfilled promise of exercise was particularly marked in the story of Ms Mulder (46/18y), who experienced completely uncontrollable blood glucose levels during her periods: You can wake up with the wrong sugar and do whatever you want all day, but it’s just going to be a terrible day. […] I can go to the gym: my sugar won’t fall. I can go for a walk: my sugar won’t fall. Nothing helps, until the week is over.
This story shows an alternation between the disciplined and the chaotic body: outside her periods, Ms Mulder was able to control her diabetes with insulin, healthy food and exercise – a lifestyle she established herself, as food and exercise were not a topic during her consultations. Moreover, her doctors could not explain her uncontrollable glucose levels and told her to wait for the menopause. In this sense, she hoped for a better future. However, this was mixed with fear of future complications: ‘You know it only gets worse: your eyes will deteriorate, you get neuropathy, there are so many things in your body that break down. That frightens me enormously’. Overall, Ms Mulder’s story radiated a great deal of despair: You are occupied with it all day long: how much exercise? What to eat? How much insulin? But I did it all
The story of Ms Mulder clearly countered the dominant narrative of the individual’s ability to discipline the body. As she experienced little support, she had been left to her own devices with this.
5. Be put on the defensive by presenting exercise as a medicine
The message that exercise is a medicine might be experienced as a confrontation with current behaviour and result in a defensive reaction. For instance, Mr Hendriks (60/12y) and Ms Sital (56/15y) both felt annoyed by the steady stream of messages of their healthcare professionals. The latter explained, They ask me what I do, and what I don’t do. I still smoke, [so they ask] if I don’t want to quit smoking. That sort of stuff. How I eat. That I need to do a lot of physical activity, something I already do. That I need to quit drinking alcohol. Just a little while and I’m ready to go to the convent.
Mr Hendriks – who told he did not do ‘any real exercise at the moment’ – even seemed to be annoyed by the questions of the interviewer:
You sometimes hear that people’s toes die. Well, I don’t have that problem yet. And I hope I never will. I don’t have problems with my eyes or something either.
And what are you doing to make sure things stay that way?
Well, not that much. Are you trying to convince me I should do more?
No, that’s absolutely not…
Because the practice nurse asks me exactly the same thing.
This excerpt reflects the presence of the Exercise Is Medicine discourse in the interview setting and, more implicitly, how this might be experienced in the consultation room.
Mr Evers (62/10y) also seemed to be put on the defensive during the interview. Although he was told by his healthcare professional that his sugar levels and blood pressure were ‘good’, he said, I am not sport-minded at all, there you go, physical activity. I cycle every day, to and from work. That’s about 15 or 16 kilometres daily, there and back. That’s my exercise, actually. And then the diabetes nurse says: that’s enough, that amount in a day. So, what can I do more? [They offer fitness classes at my work.] I did try that, but I need guidance if I’m going […] to do that much [exercise], and I don’t get any guidance at all. I need to do it myself, and that’s a bit difficult for me. It’s also a matter of discipline. I don’t want to shirk my responsibility, but still.
This quotation also gives a glimpse of how the dominant discourse affected the interview setting at times as Mr Evers seemed to feel that he had to justify his level of exercise behaviour although his nurse told him he was active enough. This was mixed with feelings of uncertainty regarding the right thing to do; he admitted that it would be good if he lost 10 kg, but mentioned that his brother – who also had diabetes – was very slim, while some of his colleagues at work were ‘very fat and had no problem at all’. This seemed to make him feel guilty, on the one hand, and unwilling or not knowing how to do more without support, on the other.
6. Resisting exercise as medicine
Some respondents resisted the idea of exercise as a medicine in their own life. Mr Cohen (46/1.5y), for instance, told about the time after his diagnosis: In the beginning, I secretly didn’t participate […]. You are examined, but for those people working in the hospital […] it is all self-evident, because they do this for a long time already. [I’m just another person with diabetes.] They say: ‘You have to lose weight and do more exercise’. […] They check your information, fill in a questionnaire and that’s it. And then, three months later [they say]: ‘It’s not good, isn’t it? Well, do your best!’ That’s it.
He talked about ‘the diabetes world’ he felt he entered, a world in which ‘healthy living is something obvious’, but a world he did not feel part of. This illustrates a possible distance between patients and their healthcare professionals in their degree of (unconscious) acceptance of dominant health discourses, which is also experienced by the latter at times and intertwined with their personal sport/exercise experiences (Stuij, 2018).
Mr Tahiri (46/7y) found a solution in the combination of medication and cutting out sugar. He used to go to the gym, quite often, but quit about 12 years ago because he became a father and worked in irregular shifts, leaving too little time. Therefore, certain life-changing events already impacted his exercise behaviour (Allender et al., 2008), before he was diagnosed with diabetes. Moreover, as a Muslim, Mr Tahiri believed that people have to become ill and that one can prevent worse by avoiding stress and fear. This moral claim clearly counters healthism and Exercise Is Medicine discourses (Pitaloka and Hsieh, 2015). Mr Tahiri added, ‘I have a good life. I am ill, but I’m fine’, indicating that he found a balance in living with diabetes.
Interestingly, both Mr Cohen and Mr Tahiri emphasized the importance of physical activity in their lives during the interview, but, at the same time, were a bit vague about their actual practices and also admitted they did not do much. ‘This has always been a problem for me’, Mr Cohen added. Their comments seemed to be motivated by a feeling that being active was socially desirable and, again, the presence of the dominant discourse in the interview setting. They seemed to acknowledge the norm that exercise is a medicine on a general level, but not in their own lives.
Another form of resistance is illustrated by the story of Mr Postma (60/16y), who found another way of managing his diabetes: When you start eating, your pancreas says: ‘Hey, carbohydrates are coming in. That many? Then I need to make that much insulin’. So, for me, it works exactly the same way. […] When I eat a bag of crisps, I check the amount of carbohydrates on the bag. And while I eat these crisps, I inject myself with the corresponding amount of insulin. […] You need to know how to handle this. And in 10, 15 years we’ll find out if I did it the right way, is the only thing I can say. But for now, I can live like I want to. And that’s the most important thing for me.
He told a story about a broken body, unable to make insulin itself. When he injected exogenous insulin, his body functioned like a normal, non-diabetic, body again. As a result, exercise was not needed as a medicine. Mr Postma used to do a lot of sport when he was young: he took part in the Dutch Swimming Championship and wanted to become a physical education teacher, but had to stop his education because of knee problems: In the course of time, this [sport participation] went from 100 percent to nothing, basically. And really, I know that if I were more active now, it helps to lose weight. And the lower your weight, the less trouble you have with this sugar. But yes, then it is a matter of: do you want that? If I can control it the way I do now, I don’t need to lose weight. Because I can control my sugar precisely.
On the one hand, Mr Postma acknowledged the Exercise Is Medicine discourse, but on the other, he resisted the idea of exercise in his current life. Given his previous athlete career and relatively privileged social position, one might have expected a different story.
7. When exercise cannot be medicine
Finally, there is a storyline in which exercise cannot be a medicine. This is illustrated by the story of Ms Mohan (39/4y), whose story was chaotic (Frank, 2013), both in content and in structure as she rambled from one subject to the other and from past to present. This also seemed her way of storytelling, something she admitted near the end of the interview. Despite this, she concluded that she experienced a lot of stress – she had no job, a lot of health problems and her mother was ill – but did not feel able to reduce it. Diabetes was something ‘large’ in her life, and her glucose levels remained high. She confirmed that her diabetes nurse touched on the subject of physical activity sometimes, but because of a heel spur, this was not an option for her. And this set her of telling about medical issues during its treatment and her current status: I couldn’t anymore, I was just completely worn out. I do not feel anything, in my foot, not anymore. So yeah, that’s my impairment. I have special shoes as well. So yeah, it is very difficult with me, at the moment. I also have many, look, I’ve all those spots. That’s because of my sugar. They also said I have a diabetic foot, because I have neuropathy […].
In sum, her circumstances left no room for physical activity in her life.
Discussion
In this article, we presented a wide variety of meanings of sport and physical activity in the lives of people diagnosed with type 2 diabetes, ranging from an instrumental sense where exercise was used to manage diabetes (Ms Borst) to loss of or change in meanings because diabetes interfered with former physical abilities and sport practices (Ms Dekker, Mr Jansen); from a new to an impossible necessity (resp. Mr Martens, Ms Hoekstra); from something to feel guilty or annoyed about (Mr Evers, Ms Sital, Mr Hendriks) to something unable to fulfil its promise (Ms Mulder); from something not needed (Mr Cohen, Mr Tahiri, Mr Postma) to something impossible to integrate in daily life (Ms Mohan).
Notwithstanding these differences, our findings illustrate that the normative notion of exercise as medicine is ingrained in the narrative habitus related to living with type 2 diabetes. It permeated all stories, either quite explicitly or in more subtle ways, for example, elicited by the interview setting. However, people employed different strategies to translate this norm into their daily life, in ways that confirmed, challenged or resisted this.
Generally, nearly all respondents considered exercise a useful means to manage blood glucose levels and postpone possible complications – this meaning was shared by those who practised it, wanted or intended to practice it (more), or did not want to. Even the latter did not doubt the promise of exercise. In other words, they seemed to subscribe to the message on a general level, but this did not correspond to their own daily life informed notions and experiences (Malcolm, 2017; Wiest et al., 2015). However, as the promise of exercise as medicine is strongly related to control over diabetes, and hence feeling well – at least in theory – it might be questionable whether it is possible to resist this discourse on a general level.
Nearly all respondents in the present study talked about rather negative experiences with ‘physical activity care’, despite its given importance as a topic throughout treatment in clinical guidelines (IDF, 2017; NHG, 2013). In a way, this further emphasizes the individual’s responsibility in the uptake or continuation of exercise after diagnosis. It clearly illustrates the close intertwinement between the neoliberal discourses of healthism and the notion of exercise as a type 2 diabetes medicine (Cairney et al., 2018).
These negative care experiences might be explained by the diabetes medical environment, which is highly protocolled, limited by a strict time frame, and has a strong focus on blood glucose levels, other measurable parameters and self-management support (Karas Montez and Karner, 2005; O’Donnell, 2015; Stuij, 2018). A translation from exercise advice as a standardized healthy lifestyle recommendation into person-centred care and support might be difficult in this medical setting.
Our findings suggest that people with type 2 diabetes might experience certain differences between themselves and their healthcare professionals. This is illustrated by the stories of Ms Sital, Mr Hendriks and Mr Evers, who at times felt the need to defend their behaviour or became annoyed by the messages about the importance of exercise. Mr Cohen summarized this in his image of the ‘diabetes world’ of which he did not feel part. Healthcare professionals are also found to ‘feel’ this and to acknowledge these differences to some extent (Stuij, 2018).
This experienced distance might be better understood in the light of other differences between (mostly ‘White’ and higher educated) healthcare professionals and a share of their patients, for instance, in socioeconomic and cultural living circumstances, notions on healthy living, and their sport, exercise and illness biographies (Greenhalgh and Wessely, 2004; Stuij, 2018). For instance, people from the higher social strata have a lower risk to get type 2 diabetes (Agardh et al., 2011; Ujcic-Voortman et al., 2009) and tend to participate more in leisure-time physical activity (Beenackers et al., 2012). 4
To improve the connection between healthcare professionals and patients, an acknowledgement that the notion of exercise as medicine is not merely a neutral and evidence-based message but an inherently normative one seems necessary. This normativity primarily lies in the emphasis on individual responsibility, although this mostly remains unstated because of the close alignment with neoliberal healthism notions (Wiest et al., 2015). These are, as Mr Cohen explained, notions from a world in which healthy living is something obvious.
This seems more urgent given the increasing emphasis on exercise as medicine, illustrated, for example, by the publication of a Dutch ‘Physical Activity Care Standard’ for healthcare professionals (NHG, 2015) and the foundation of the Dutch Lifestyle Medicine Innovation Centre (NILG, 2018). These developments might lead to a further obscuration of the normative aspects and, in the end, increase inequalities (Baum and Fisher, 2014). This also might result in the norm that exercise is the best medicine for type 2 diabetes.
Therefore, reflexivity on the normative aspects of the notion that exercise is a type 2 diabetes medicine seems a prerequisite for the provision of ‘good’ physical activity care. This normativity is shaped in practices and depends on the context and persons involved. It might include, for instance, reflexivity of healthcare professionals on their personal sport and exercise/physical activity biographies, notions on healthy living, relatively privileged positions and on how these impact relationships with their patients.
This requires attention to other ways of knowing besides the medicalized views on illness and exercise that include more lifeworld-led care (Dahlberg et al., 2009) and attention to the broader socio-cultural and economic contexts people live in (Jaye et al., 2018). This article illustrated a great variety of (embodied) experiences and living circumstances, resulting in different (im)possibilities and wishes regarding sport and exercise. Getting to know someone’s story and critical reflection on its co-construction, both in face-to-face interaction and in relation to prominent narratives, might add to ‘good’ physical activity care.
Footnotes
Acknowledgements
The authors are grateful to the respondents for sharing their stories and to Majorie van den Berg for conducting the pilot study. We also thank Andrew Sparkes for his helpful comments on an earlier draft of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by NWO, the Netherlands Organization for Scientific Research, as part of their research programme Sport: Participation. The funding party was not involved in the study or its publication.
Research ethics and patient consent
According to the Medical Research Ethics Committee of the VU University Medical Centre, the study does not fall under the scope of the Medical Research Involving Human Subjects Act (WMO), reference number 2013.413. After written and oral information, the respondents provided informed consent.