
Abstract
The ability of health-care professionals to understand the lived experiences of their patients has become increasingly important but has been a difficult topic to investigate empirically because it involves two distinctive research strands: interpretative phenomenological analysis and patient–provider communication. While interpretative phenomenological analysis focuses on experiences and illness narratives of patients, but not on therapist’s understanding of those, patient–provider communication surveys focus primarily on effective forms of communication without addressing the actual illness experiences of patients. There is a need for empirical research that combines both strands to investigate not only the experiences of patients but also whether professionals are able to understand these. This study combined both strands by means of a novel research method called the Imitation Game (combined with other qualitative methods). This sociological method was developed to investigate what different social groups know of each other’s lifeworld. It focused on the important domain of eating disorder treatment to investigate whether therapists were able to understand the experiences of their patients and vice versa. This study provides insights into the domains in which therapists and patients were able to develop insights into each other’s experiential knowledge (and where they had difficulties in doing so). The findings also implicate the high potential of the Imitation Game as an interdisciplinary research method. We propose that the Imitation Game may be particularly valuable as a ‘can opener’ that enables the development of in-depth, qualitative insights into the substantive themes that matter in the lifeworlds of patients and therapists.
Keywords
Introduction
The increasing prevalence of chronic illness has significant implications for relationships between patients and health-care professionals (Sullivan, 2003). Whereas acute patients are usually seen to treat a short-term illness or condition for a limited time period, the relationship between professionals and chronic patients (or other longitudinal patients in need of intensive treatment, such as those with an eating disorder) is more extended, developing over a longer time frame and focusing on managing symptoms in daily life (Thorne and Robinson, 1989). In such situations, it is crucial for health-care professionals to understand the lived experiences of patients: the ways in which individuals characterize and experience their condition, the meaning-making processes they attach to their condition and treatment, and the experiential knowledge of the condition and treatment that individuals gain over time (Greenhalgh, 2009; Thorne et al., 2003; Tyreman, 2005).
The doctor’s office is one of the primary locations in which patients can frame the experiences of their illness in the biomedical context. One of the main focuses of chronic illness research is communication between professionals and patients during medical encounters (Paterson, 2001; Scambler and Britten, 2001). A significant result of such research is the recognition of the importance of communication for effective care and the development of a well-functioning therapeutic alliance or relationship (Thorne, 2006). Recently, Britten and Maguire (2015) argued that interactions with professionals can be ‘profoundly damaging’ for patients if patients are not taken seriously (p. 2). Other scholars identified the provider’s sense of understanding of the patient’s lived experiences with an illness as a core condition for a well-functioning therapeutic relationship (Evans and Crocker, 2013; Thorne, 2006; Thorne and Paterson, 2000; Tyreman, 2005).
Although the ability of health-care professionals to understand the lived experiences and the experiential knowledge of their patients is highly important, it is a difficult topic to investigate empirically as the two-stranded topic has generally been addressed in different ways. The strand of illness experiences and experiential knowledge of patients is often investigated by means of interpretative phenomenological analysis (IPA). Using this approach, subjective processes of meaning-making are the primary focus, leading to rich, detailed insights into the lifeworld of patients (Bramley and Eatough, 2005; Osborn and Smith, 2015). While an important advantage of this approach is that it focuses on patients’ personal accounts of their illness and treatment experiences, it does not provide insight into how (health-care) professionals understand these experiences.
In contrast, the research strand of patient–provider communication (PPC) predominantly uses validated, patient-report surveys to measure items such as respectful treatment and ‘lay-friendly’ explanations of medical/treatment information (Gremigni et al., 2008; Haywood et al., 2014; Schillinger et al., 2004). While this research has put patient-centred health communication on many agendas, it does not reveal much about how well professionals are able to understand the experiences of patients, as the questionnaires often do not address the content of patient experiences.
Whereas IPA approaches address the experiences and illness narratives of patients, there is a gap in the literature in relation to how professionals are able to understand these experiences and connect to them in therapeutic encounters with patients. Alternatively, PPC literature does not focus on the actual content (e.g. the illness experiences) of patients. There is a clear need for empirical research that combines both strands to investigate the experiences and experiential knowledge of patients and in what ways professionals are able to understand patient experiences and experiential knowledge. The purpose of this article is to present such an empirical investigation by applying a novel research method: the Imitation Game. This method is ideally suitable to empirically investigate these important questions.
The Imitation Game is a blinded, computer-based experiment (often conducted on one location). Each Game consists of three participants in separate roles:
Judge: developing experience-based questions as member of a particular social/cultural group;
Non-pretender (NP): member of the same group, answering these questions naturally, from the experiences of being a member;
Pretender: not coming from this group but trying to formulate a plausible answer by pretending to be a member (Collins and Evans, 2014).
When the Pretender and the NP have formulated their answers to the Judge’s question, these are sent back (simultaneously and anonymously). The Judge then indicates which of the two answers (s)he believes to be from the Pretender and why. This process is repeated several times: the Judge can formulate a new question (or follow up an earlier question). The Imitation Game was developed as a sociological method to investigate what different social groups know of each other’s lifeworld (Collins and Evans, 2014). When applied to health care, the method allows for an investigation into the experiential knowledge of patients and into the degree and depth of knowledge that health-care professionals have into the experiential knowledge of patients, thereby combining the strands of research identified above (Wehrens, 2015).
This article investigates whether, how and to what degree therapists specialized in the treatment of eating disorders were able to understand the experiences of the young women in treatment. Simultaneously, this article investigates whether patients were able to understand the experiences of therapists. 1 For both questions, we used the Imitation Game method and focus groups. The second question has been surprisingly absent from the literature on patient–provider relationships, even though research has shown that patients often have distinct expectations about treatment and about therapists (Mahon, 2000) and that a large discrepancy between these expectations and eventual experiences is an important factor in treatment dropout (Clinton, 1996). Insights into these matters may bear important implications for future research, as we will explore in the ‘Discussion’ section.
Eating disorder treatment can be seen as an extremely relevant case study for empirically investigating what therapists know of the lived experiences of their patients by means of the Imitation Game. Patient–provider relationships in eating disorder treatment are often described as adversarial; interactions in treatment are considered highly complex and are often troubled by diverging perspectives and experiences of therapists and patients (Currin et al., 2009; Vitousek et al., 1998). There is a widely acknowledged need for therapists to gain a better understanding of the lived experiences of persons with an eating disorder (Darcy et al., 2010; Federici and Kaplan, 2008; Patching and Lawler, 2009). 2
The next section explores the theoretical concepts that are central to the Imitation Game method (‘contributory expertise’ and ‘interactional expertise’, the tacit dimension of both, and the process of socialization, which is at the core of acquiring expertise) and elaborates its applicability to eating disorders and eating disorder treatment. The ‘Methods’ section explores the Imitation Game method and the ways in which it has been applied as a method of understanding relationships and expertise; the ‘Methods’ section also discusses the focus groups, which were conducted to elicit insights into aspects of mutual understanding and lack of understanding. The results section is organized around the particular domains in which therapists were and were not able to articulate their understanding of their patient’s lived experiences and vice versa. In the discussion section, we interpret the empirical results in the light of existing research, offer reflections on the Imitation Game as an interdisciplinary approach and reflect on the particular strengths and limitations of the method. The conclusion summarizes the main findings.
Theoretical underpinnings
Contributory and interactional expertise
The Imitation Game has roots in the sociology of scientific knowledge (SSK) and its sub-field ‘studies of expertise and experience’ (SEE). Central to the field of SSK is the idea that knowledge is a collective and largely tacit phenomenon, which is acquired through a process of socialization into a particular community (Collins et al., 2017). In their studies on expertise and experience, Harry Collins and Rob Evans have conceptualized the acquisition of expertise as a thoroughly social process, involving a shared tacit dimension. It is through the actor’s socialization in the practices of expert groups that their expertise is established (Collins and Evans, 2008).
SEE has developed a rich taxonomy of the various forms of expertise. The most important theoretical concepts in relation to the Imitation Game are ‘contributory expertise’ and ‘interactional expertise’. Contributory expertise refers to the ability to perform a skilled practice. Someone who is a contributory expert in a domain is able to contribute to the domain to which this expertise pertains. For example, a surgeon can be seen as a contributory expert in the specialist domain of surgery, being able to conduct the specific, specialist tasks that belong to this domain. This ability requires both extensive formal knowledge and shared tacit knowledge.
Interactional expertise refers to expertise in the language of a specialization in the absence of expertise in its practice. This also requires a degree of enculturation into the expert group but not necessarily requiring full-blown immersion (Collins and Evans, 2008). Persons spending a significant amount of time within a group of contributory experts, becoming ‘socialized’, may be able to learn the language pertaining to the (contributory) expertise of this group, even without being able to contribute directly to this domain. Building on the surgeon example, an ethnographic researcher could develop interactional expertise in surgery through long-term observations. The ethnographer would be able to understand the tacit components and experiences of surgeons, the nuances in their work, without being able to actually complete a (successful) surgery.
The concepts of contributory and interactional expertise offer an interesting new conceptualization of both the lived experiences of chronically ill patients and of therapeutic work. Those with a chronic illness or condition have developed the tacit knowledge necessary to deal with their illness in daily life. They ‘contribute’ to this domain in various ways, such as acting on subtle bodily cues and testing out disease management strategies. Similarly, the ability of health-care professionals to understand the lived experiences of these patients can be conceptualized in terms of interactional expertise: while many professionals do not have the same actual experiences and do not have to act on this illness the way patients do, they, nevertheless, need to be able to understand the tacit components and experiences of their patients.
In a similar sense, these concepts allow us to explore therapeutic work in terms of contributory expertise as well. Therapeutic work does not only consist of propositional knowledge but also has a tacit, experience-based component (i.e. therapists exchanging tips on how to approach particular patients, what to say or not to say, how to behave, etc.). Although patients may have developed some understanding of these aspects of therapeutic work through their sustained interactions (i.e. ‘interactional expertise’), they do not have the experience of doing therapeutic work themselves (i.e. they do not have contributory expertise in this domain).
Based on this framework, it is clear that both patients and therapists have developed experiential knowledge (in ‘living with an eating disorder’ and in ‘providing therapy’). Both can be conceptualized as forms of ‘contributory expertise’. Through their sustained interactions in the therapeutic encounter, both therapists and patients become ‘socialized’ into each other’s community (the assumption being that the therapist becomes more socialized into the eating disorder community than the patient as the main focus of the relationship is to help the patient recover and manage an eating disorder). The Imitation Game allows for an investigation into the extent in which therapists and patients developed an understanding of each other’s experiential knowledge.
Eating disorders: complicated relationships and ‘irrational’ experiences?
Such mutual understanding is a particularly relevant topic for eating disorder treatment. Eating disorder patients perceive therapists to be unable to understand what the disorder means in their lived experiences (Dawson et al., 2014); such understanding has consistently proved to be highly important in how patients perceived the quality of their treatment (De La Rie et al., 2008). When this understanding is missing, it often leads to discontent, frustration and detrimental effects on how treatment is perceived (Darcy et al., 2010; Dawson et al., 2014).
A range of critical feminist and discourse analytic studies have pointed to a further complication. Within therapeutic encounters, the lived experiences of those with an eating disorder are often depicted as symptomatic of the illness, thereby neglecting and trivializing them a priori (Bell, 2009; Gooldin, 2008; Lester, 1997). This vein of scholarship has been persistent and persuasive in contextualizing (and problematizing) why the relationships between therapists and patients in eating disorder treatment are often perceived as adverse. Developing and testing ways, such as the Imitation Game, for therapists to understand the lived experiences of those with an eating disorder has the potential to improve eating disorder care and the relationships between patients and therapists.
Explanatory models of illness
Feminist literature on eating disorders elucidates that the lived experiences of persons with an eating disorder are not simply the irrational expressions of various individuals but form a coherent frame of sense-making processes that need to be understood in their social and cultural context (Bordo, 1997; King, 2004; Malson, 2004). Simply dismissing such experiences as irrational expressions of the illness is likely to be extremely problematic in terms of establishing a workable therapeutic relationship. Instead, it becomes more important to understand such – often shared – systems of understanding.
A useful theoretical framework for this purpose is provided by Fox et al. (2005), who built on Kleinman’s concept of explanatory models, understood as narrative frameworks used by lay and professional people to make sense of disease. This concept enables us to understand the lived experiences of patients as a ‘lay construction of an illness grounded firmly in the experiential and contextual reflections of [its] participants’ (Fox et al., 2005: 963). Such lay constructions emerge ‘as a coherent system of understanding, grounded in […] shared experiences […], as opposed to externally-imposed models of disease’ (Fox et al., 2005: 965). The notion of ‘explanatory models’ provides a frame for understanding differences between medical understandings of eating disorders and the experiences of patients, while sensitizing us to the need for therapists to acquire understanding of the explanatory models constructed by their patients.
The notion of ‘explanatory models’ clearly resonates with the concepts of ‘contributory’ and ‘interactional expertise’. Together, they emphasize two important points. First, the lived experiences of persons with an eating disorder should not be read as irrational expressions of the illness but need to be understood as sense-making processes. Second, these experiences and sense-making processes are not (only) individual but often shared through socialization.
When taking these points together, they harbour important implications for both professionals and researchers. Professionals are encouraged to acquire a frame of reference that can help them understand the experiences of persons with eating disorders (cf. Vitousek et al., 1998). For researchers, the implication is that investigating whether professionals are able to acquire such frames becomes an important empirical topic. The remainder of this article focuses on the results of an empirical study in which this topic was investigated through the utilization of the novel Imitation Game method.
Methods
The history of the Imitation Game can be traced back to the Turing (1950) test for artificial intelligence. More recently, it was developed as a social science research method to compare what different social or cultural groups know about each other (Evans and Collins, 2010). As outlined in the introduction, the Imitation Game is a blinded, computer-based experiment with three distinctive roles:
Judge: developing experience-based questions as member of a particular social/cultural group;
NP: drawn from the same group, answering these questions naturally, from the experiences of being a member of this group;
Pretender: not coming from this group but trying to formulate a plausible answer by pretending to be a member of this group (Collins and Evans, 2014).
What follows is a recursive cycle in which the two participants (Pretender and NP) formulate answers, which are evaluated by the Judge, who formulates a new question, which is sent to both participants again. Judges formulate their own questions.
Two different Imitation Game set-ups were used. In ‘Set-up 1’, the roles of Judge and NP were played by persons with an eating disorder. Therapists were playing the role of Pretender: they were asked to answer the questions they received as if they had an eating disorder themselves. In ‘Set-up 2’, therapists played the role of Judge and NP. Patients were playing the role of Pretender: in this set-up, they were answering questions regarding experiences of therapists in providing care as if they were therapists themselves.
Because the goal of the Judge is to identify the Pretender, it was emphasized that Judges should try to think of questions they regarded to be particularly informative about their own experiential knowledge (i.e. regarding their experiences with an eating disorder or their experiences as a therapist treating those with an eating disorder). The two designs of the method aim to provide insights into how well therapists are able to understand the experiential knowledge of their patients and how well patients are able to understand the experiential knowledge of their therapists. Figures 1 and 2 show how the Imitation Game has been utilized.
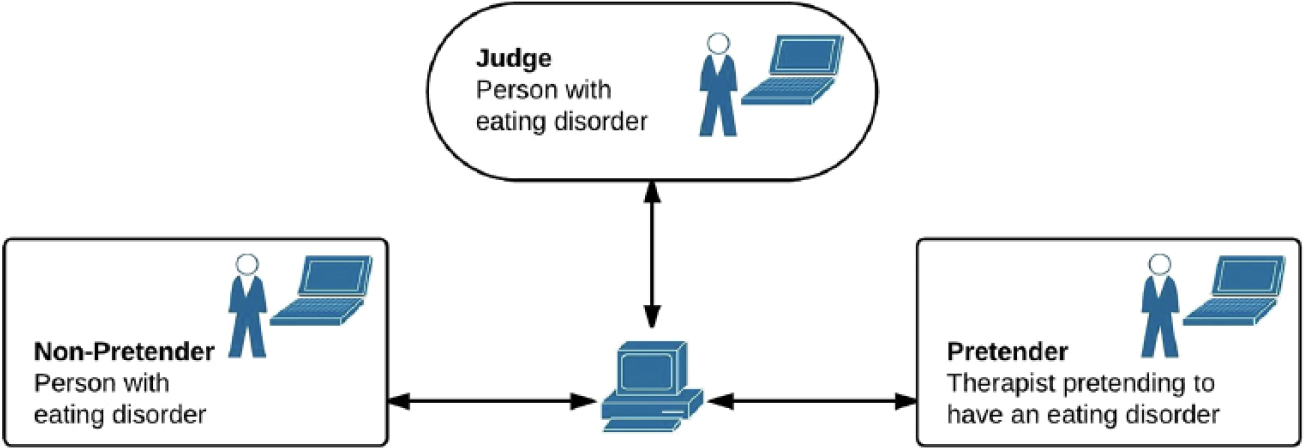
Imitation Game set-up with patient as Judge.
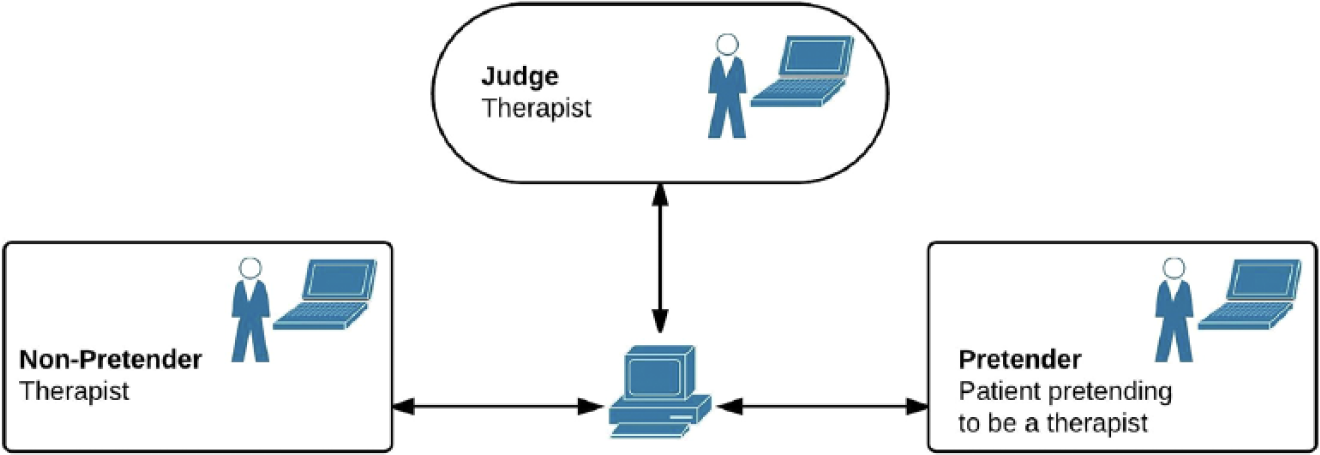
Imitation Game set-up with therapist as Judge.
In total, 12 Imitation Games were played in one afternoon session, with a total of 14 participants (8 persons with an eating disorder and 6 therapists), ranging on average 90 minutes per game. The data produced by these games (automatically recorded by specialized software) consisted of the full dialogues (Judges’ questions, Pretender and NP’ answers, the Judges’ decisions and their rationale for the decision). The games were conducted on laptops set up in one large room in the centre. 3
Although the developers of the Imitation Game have emphasized the quantitative potential of the method (Collins and Evans, 2014), the way in which we apply the method is methodologically most closely linked to an interpretative qualitative research approach. It is tied to phenomenological approaches through its emphasis on the lifeworld and experiential knowledge, as well as harbouring characteristics of ethnographic research through its focus on the ‘culture’ of the ‘contributory experts’. In addition, there is a clear similarity to participatory research approaches (as it is the Judges rather than the researchers who develop the questions).
Other methods
In order to generate additional qualitative insights into aspects of understanding and to elaborate on the results of the Imitation Games, three focus groups were organized immediately after the Imitation Games. First, two separate focus groups were organized (one for patients and the other for therapists). The first focus group was coordinated by a therapist working as an ‘experience worker’. 4 The first author coordinated the therapist focus group. Both focus groups had a length of approximately 45 minutes. They consisted of 8 and 6 participants. After these separate focus groups, a combined focus group (14 participants) of approximately 1 hour was held. All focus groups were recorded and transcribed verbatim.
The focus groups were semi-structured around the following themes: experiences with the game, motivations behind the questions asked as Judges, strategies for answering questions as pretenders and general suggestions about the method. The joint focus group focused on facilitating discussion among both groups of participants, in order to generate participant explanations for why understanding each other’s experiences was perceived as challenging or easy.
Research context
This study took place in a specialist centre for eating disorder treatment in the Netherlands. The centre offers outpatient treatment and part-time treatments, both on individual and group levels. The therapists involved in this centre all had long-term, specialized knowledge in the treatment of eating disorders. In total, six therapists (one male and five female therapists) and eight persons diagnosed with an eating disorder (all female) participated in the research. Tables 1 and 2 provide more detailed information about the most important characteristics of both groups.
Participating patients: age, type of treatment and details of eating disorder.
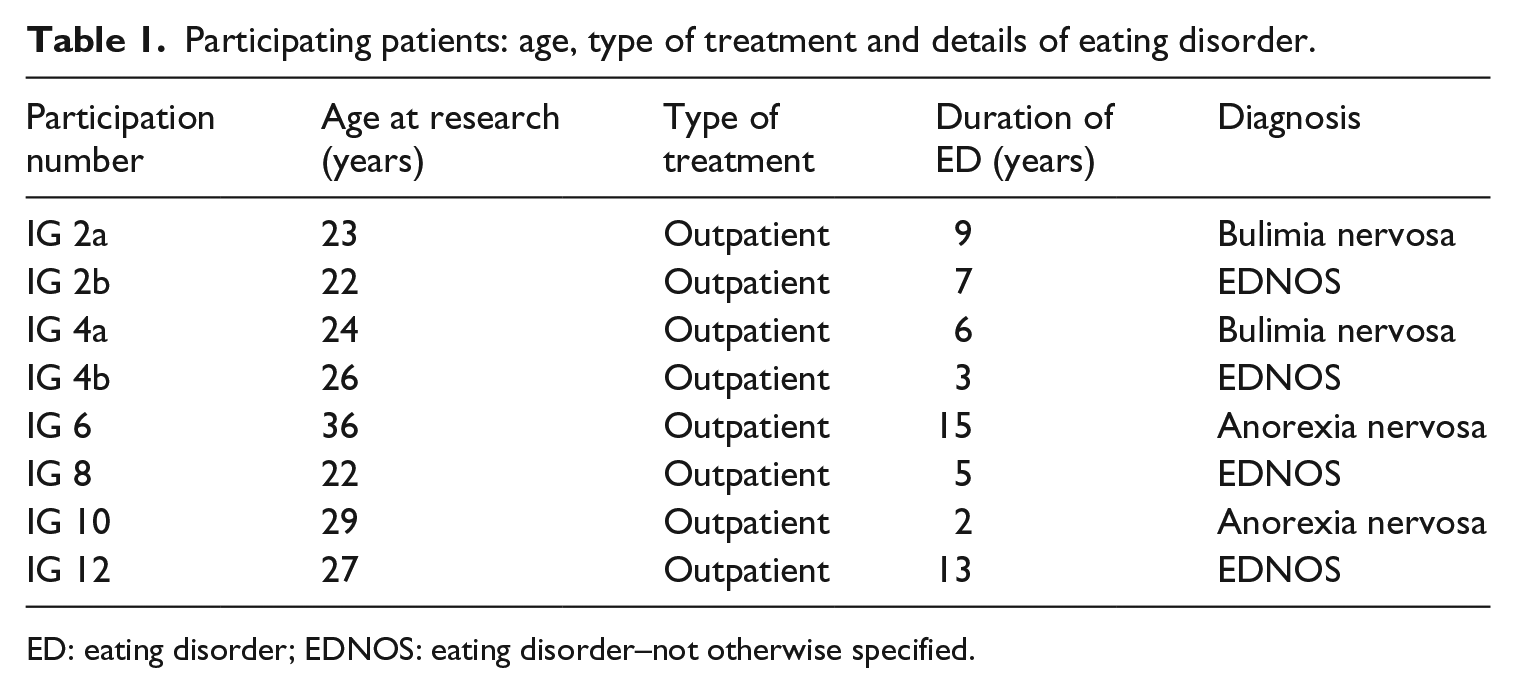
ED: eating disorder; EDNOS: eating disorder–not otherwise specified.
Participating therapists: age and details of work experience.
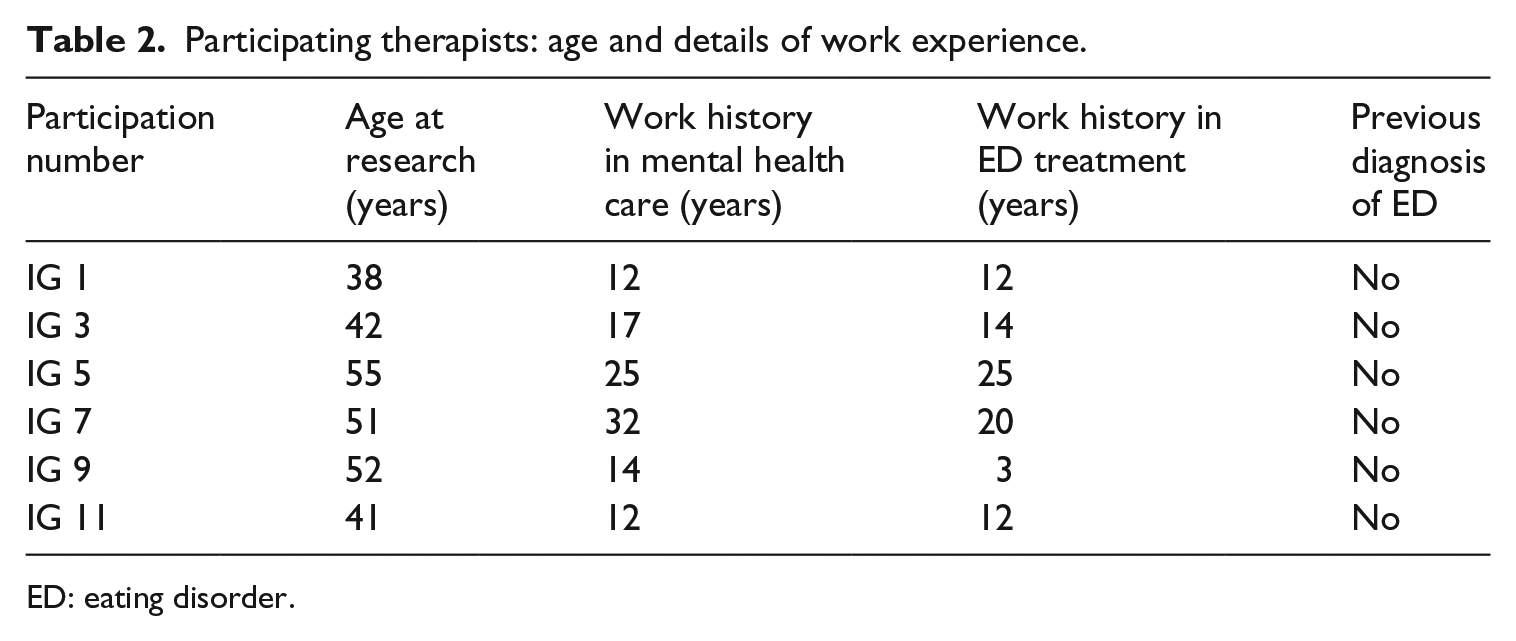
ED: eating disorder.
Participants have been recruited by means of various information flyers provided to them by therapists (the flyers were developed together with the centre) and by means of informal communication.
Ethics
Research ethics formed an important part of the study. Ethical approvals have been obtained at the relevant ethical review committee. 5 The experience worker informally assessed which participants would be suitable to participate. Only persons involved in the outpatient programme of the centre could participate. Much care was taken to ensure informed consent: all participants have been informed thoroughly in advance about the aims and methods of the research. The voluntary character of participation has also been stressed. All participants were over 18 years of age. All data have been anonymized.
Analytical procedure
A thematic content analysis (Guest et al., 2012) was conducted by the first author. All material (the Imitation Game dialogues and focus groups) has been coded in three substantive steps. No distinction was made between Imitation Game analysis and focus group coding process to allow for comparability of the results. A process of open coding allowed for a line-by-line analysis of all transcripts. The process of axial coding then enabled a more detailed investigation into the main themes that were emerging from these transcripts (e.g. ‘dealing with weight changes’). Finally, the process of selective coding allowed for establishing an order and relation between these main themes (e.g. ‘dealing with weight changes’ as a sub-theme of ‘fear of losing control’; Mortelmans, 2007). The emerging themes were discussed between the two authors until consensus was reached. The analysis was done inductively, although theoretical insights were used as ‘sensitizing concepts’ (Mortelmans, 2007). The research was conducted in Dutch. All quotes have been translated by the first author and checked by the second author, who is a native English speaker.
Results
The thematic analysis led to the identification of various domains in regard to patient’s and therapist’s understanding and lack of understanding of each other’s experiences. The inductively identified domains have been categorized along two axes: ‘therapist–patient’ and ‘showing knowledgeability–lacking knowledgeability’ (of each other’s experiences), drawing on material from the Imitation Games and the focus groups:
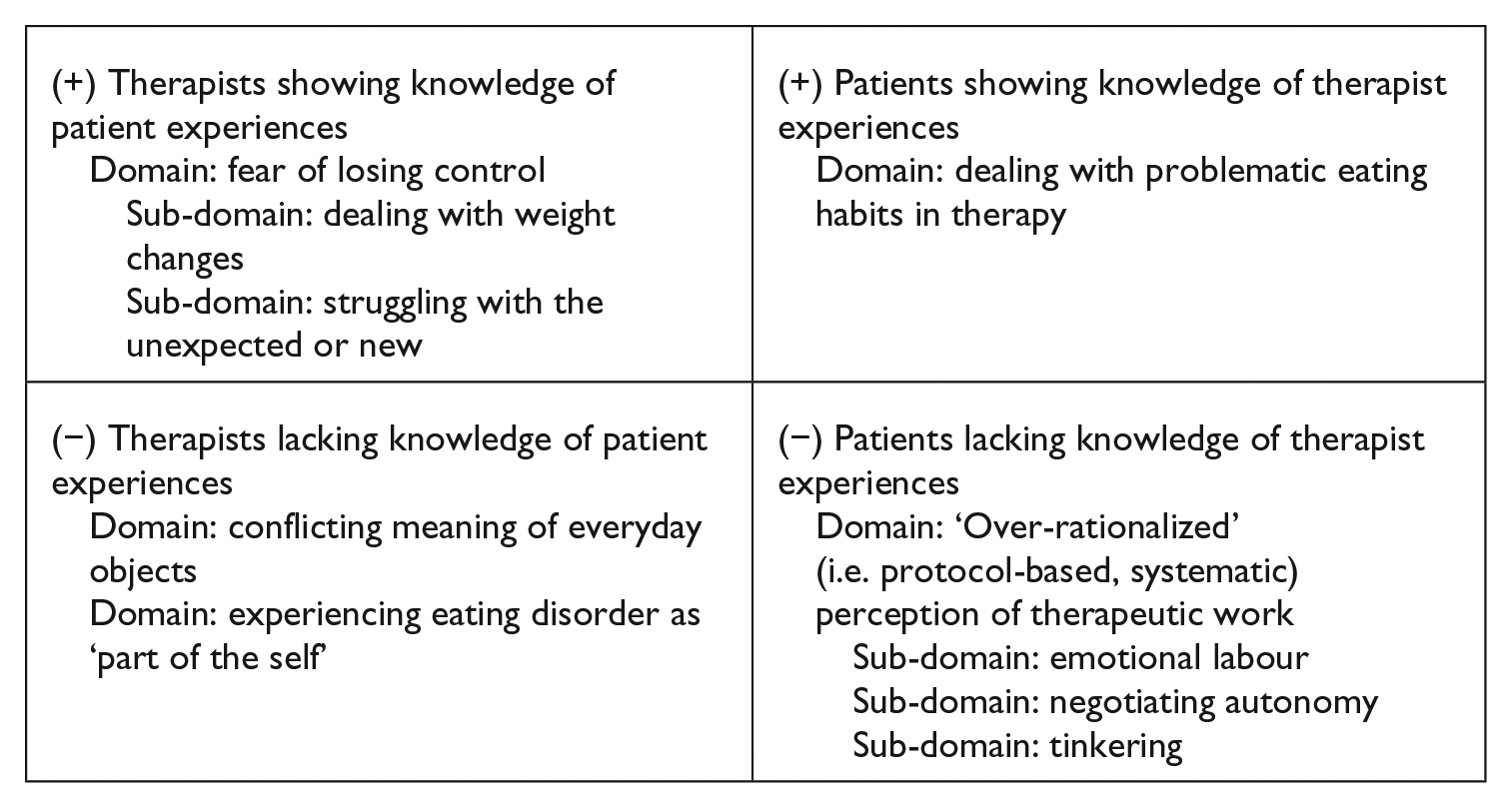
Therapists showing knowledge of patient experiences
Therapists convincingly expressed knowledge of the patient experience in several domains. The fear of losing control was one overarching theme. Therapists recognized that the fear of losing control is a key underlying experience for many patients with an eating disorder. This fear of losing control becomes clear in two sub-domains (dealing with weight changes and struggling with the unexpected or new).
The first sub-domain is about dealing with weight changes:
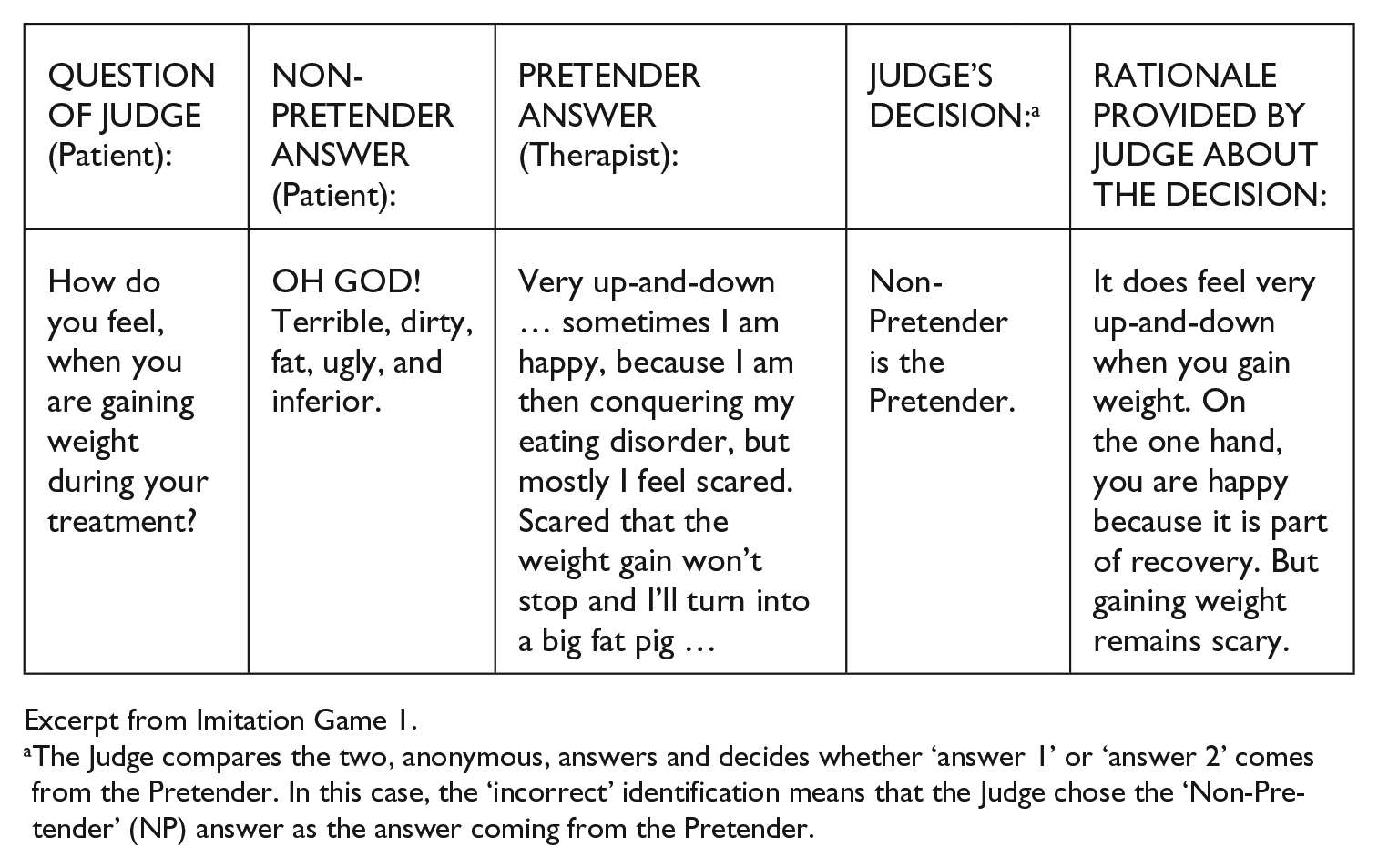
Excerpt from Imitation Game 1.
The Judge compares the two, anonymous, answers and decides whether ‘answer 1’ or ‘answer 2’ comes from the Pretender. In this case, the ‘incorrect’ identification means that the Judge chose the ‘Non-Pretender’ (NP) answer as the answer coming from the Pretender.
This excerpt shows the therapist’s ability to express the ambivalent experiences of the patient in relation to gaining weight during treatment: perceiving it as something good but, nonetheless, scary. Furthermore, the therapist recognizes that this patient’s primary fear is not the weight gain per se but the fear of not being able to control this weight gain.
The second sub-domain can be labelled ‘struggling with the unexpected or new’. Many questions of patient Judges focused on experiences of unusual or new events, such as going on vacation or joining in for Christmas dinner. Fear of losing control is also of great concern. The excerpt below illustrates how one therapist is able to convincingly express this (i.e. the answer is recognized as valid by the Judge): 6
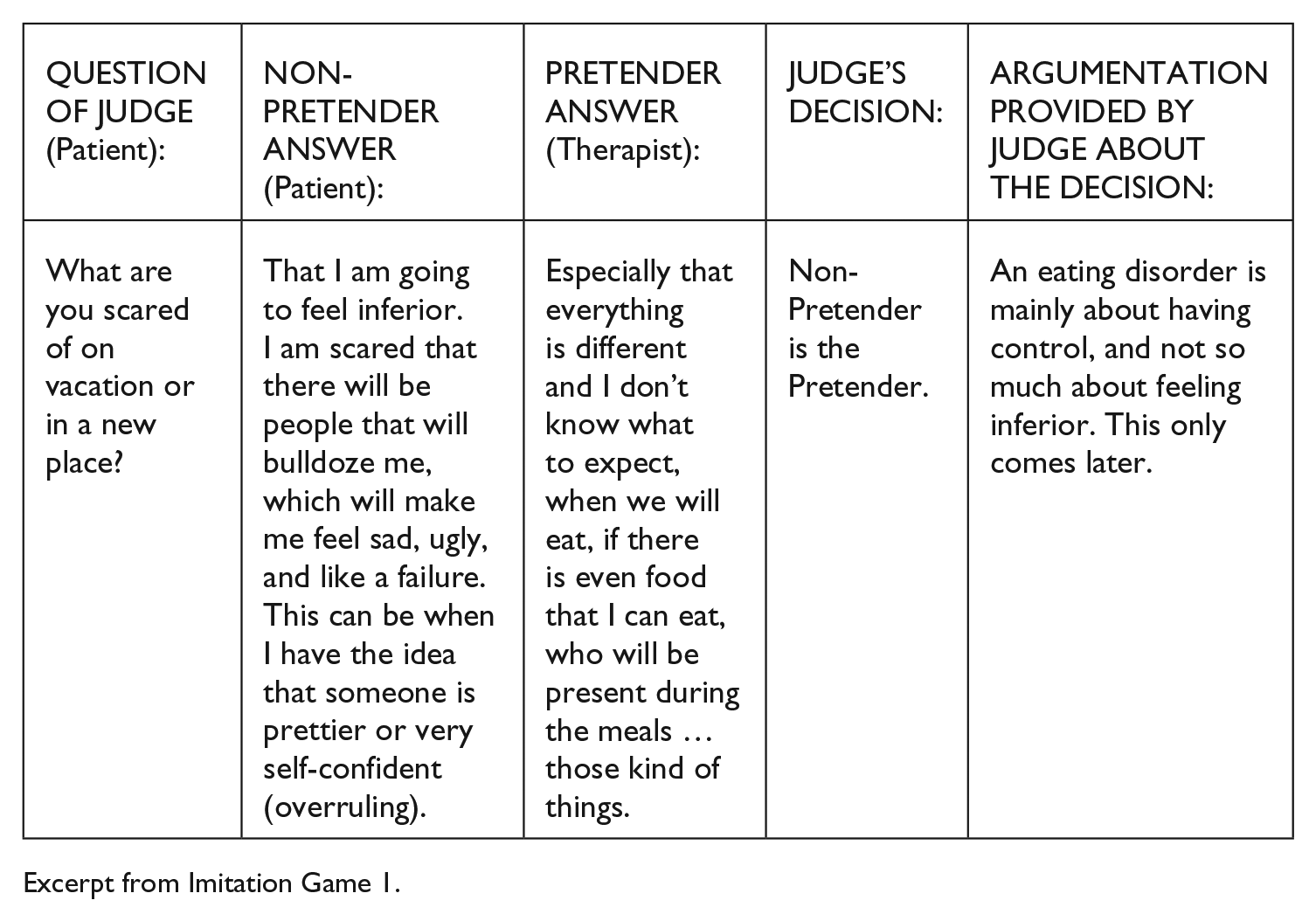
Excerpt from Imitation Game 1.
This excerpt provides another example of a therapist expressing understanding of the lived experiences of this patient: for the patient, the fear of situations and experiences out of their control is frequently perceived as the most frightening aspect of dealing with a new situation. The review by the patient Judge affirms this concern.
Therapists lacking knowledge of patient experiences
Our research has revealed the domains in which therapists faced difficulties in convincingly expressing knowledge of patient experiences. These two domains were identified: conflicting meanings of everyday objects and the eating disorder as ‘part of the self’. The conflicting meanings of everyday objects can be seen in the following excerpt from the joint focus group; the therapists and patients reflected on how a therapist provided a rather surprising answer about the ‘functionality’ of a mirror in one of the Imitation Games:
What was also remarkable was that many questions were asked about ‘what does it do [with you] when you look into the mirror?’, ‘how does that feel?’, and those kinds of questions (…)
Yes, how does that make you feel? (Laughter) The mirror, which was supposedly very functional (ironic emphasis). Who was that? (Loud laughter)
I didn’t do so well, did I? (Laughs)
But what was your reasoning then? Why was that question so important for you all?
Well, (…) this is more from my own perspective, but what it does for us (…) for me the mirror greatly influences my day, for example. And also that you can use a mirror for positive ends, making yourself pretty (…) but I also looked in the mirror for a long time to see that I was too fat, so seeking negative affirmations, and that was not from my ‘healthy me’, but it is a large influence the mirror can have in a given moment. And of course [they are] my thoughts but it is also the burden carried by the mirror. (Excerpt of joint focus group, 12 September 2013)
This excerpt centres on how one of the patients expressed her surprise about a particular answer about mirrors that was given during one of the Imitation Games. The way in which the patient reacted during the focus group and her subsequent elaboration highlight how this particular therapist seemed to lack knowledge about the ambivalent but very large impact that mirrors have for many patients. As well, the elaboration of this patient provided a detailed understanding of the role of this everyday object (the mirror) in her own lived experience.
The second domain in which therapists experienced difficulties is about how patients experience the eating disorder as ‘part of the self’. The excerpt below from the focus group with therapists illustrates this:
Can you remember more questions from clients of which you all thought ‘that is a good question; I had difficulties in answering that one’?
Yes: ‘what did you find the most difficult to share from the point of view of your eating disorder?’
Oh yes, yes, that is a very good question indeed.
But it is also a question like … ‘from the point of view of your eating disorder’, that is so much … what does that mean then?
Yes I also noticed that in the [therapy] sometimes they talk about ‘my eating disorder’. But what is that then? Is that only the part about eating or also all the other shit that accompanies it? They usually only talk about eating. (Therapist focus group, 12 September 2013).
This quote shows how difficult it can be for therapists to understand what a patient means when referring to their eating disorder, whether it ‘only’ refers to eating-related matters or whether it is experienced as a broader part of the patient’s identity. As the earlier quote concerning the mirror makes clear, patients also view aspects such as ‘seeking negative affirmations’ (by obsessively looking in the mirror) as part of their identity as someone with an eating disorder.
Patients showing knowledge of therapist experiences
The Imitation Games with therapist Judges revealed the differences in the knowledge of patients and therapists in regard to each other’s experiences. Overall, patients found it harder to show knowledge of the experiences of therapists. 7 One domain could be identified in which a patient succeeded in understanding the knowledge and experiences of therapists: dealing with problematic eating habits in therapy. The next excerpt discusses how to deal with veganism in therapy:
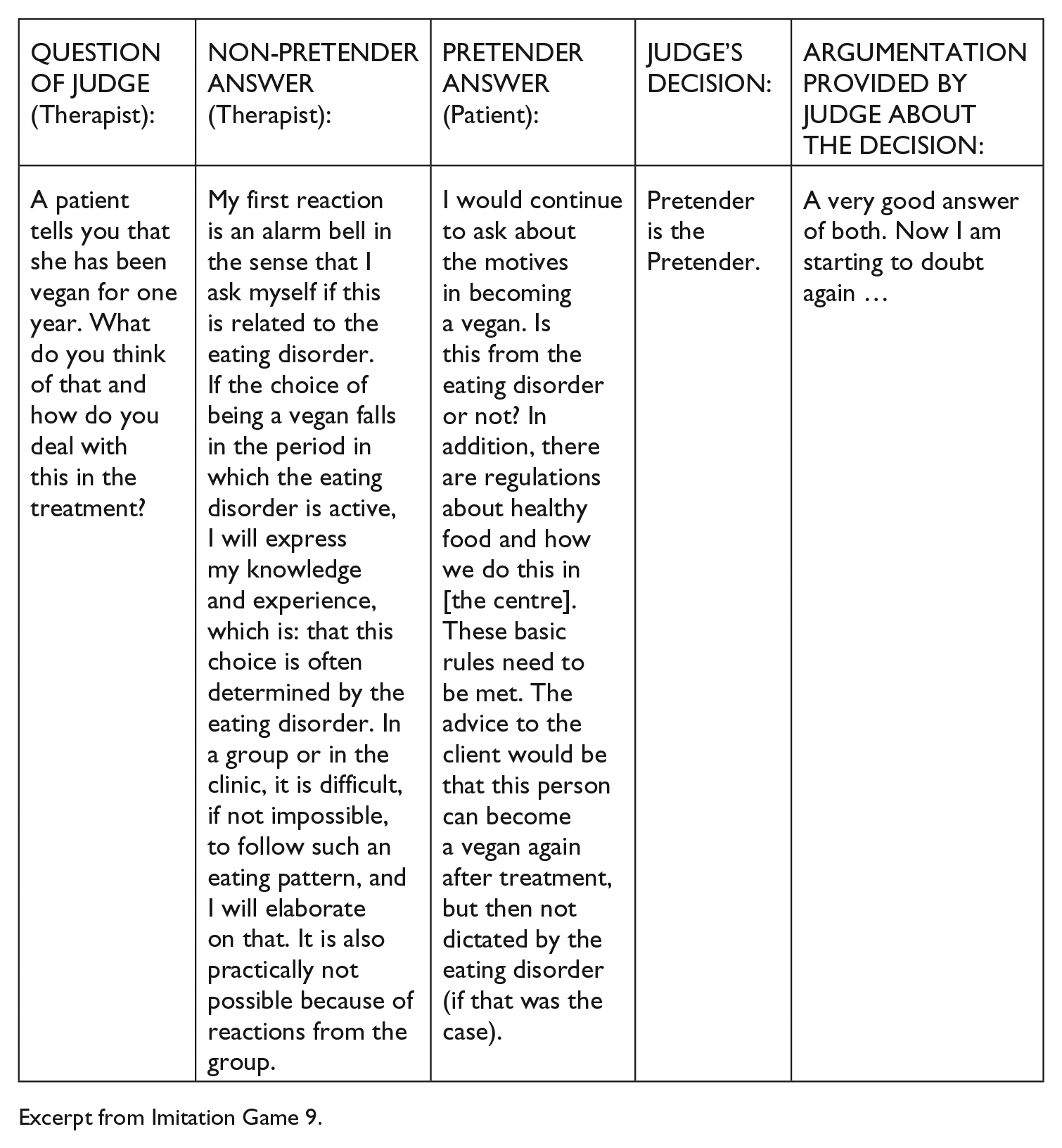
Excerpt from Imitation Game 9.
The quote shows that the Pretender (patient) was able to communicate a convincing answer to this question; she was able to make the Judge doubtful about the previous choice. This may be because of experiences with other patients (e.g. in treatment groups) trying to ‘use’ veganism as a strategy for restricting food intake. In the large majority of the cases, however, patients experienced difficulties in understanding the experiences of therapists.
Patients lacking knowledge of therapist experiences
The study revealed one main domain in which patients consistently experienced a lack of knowledge regarding the experiences of therapists: the over-rationalized image of therapeutic work. Many patients had a very protocol-based and systematic view of therapeutic work and did not understand the large tacit dimension involved in the daily work of therapists. Within this domain, three sub-domains can be identified: emotional labour, negotiating autonomy and tinkering (Mol et al., 2010).
An example of emotional labour is the considerations that go beyond therapy protocols:
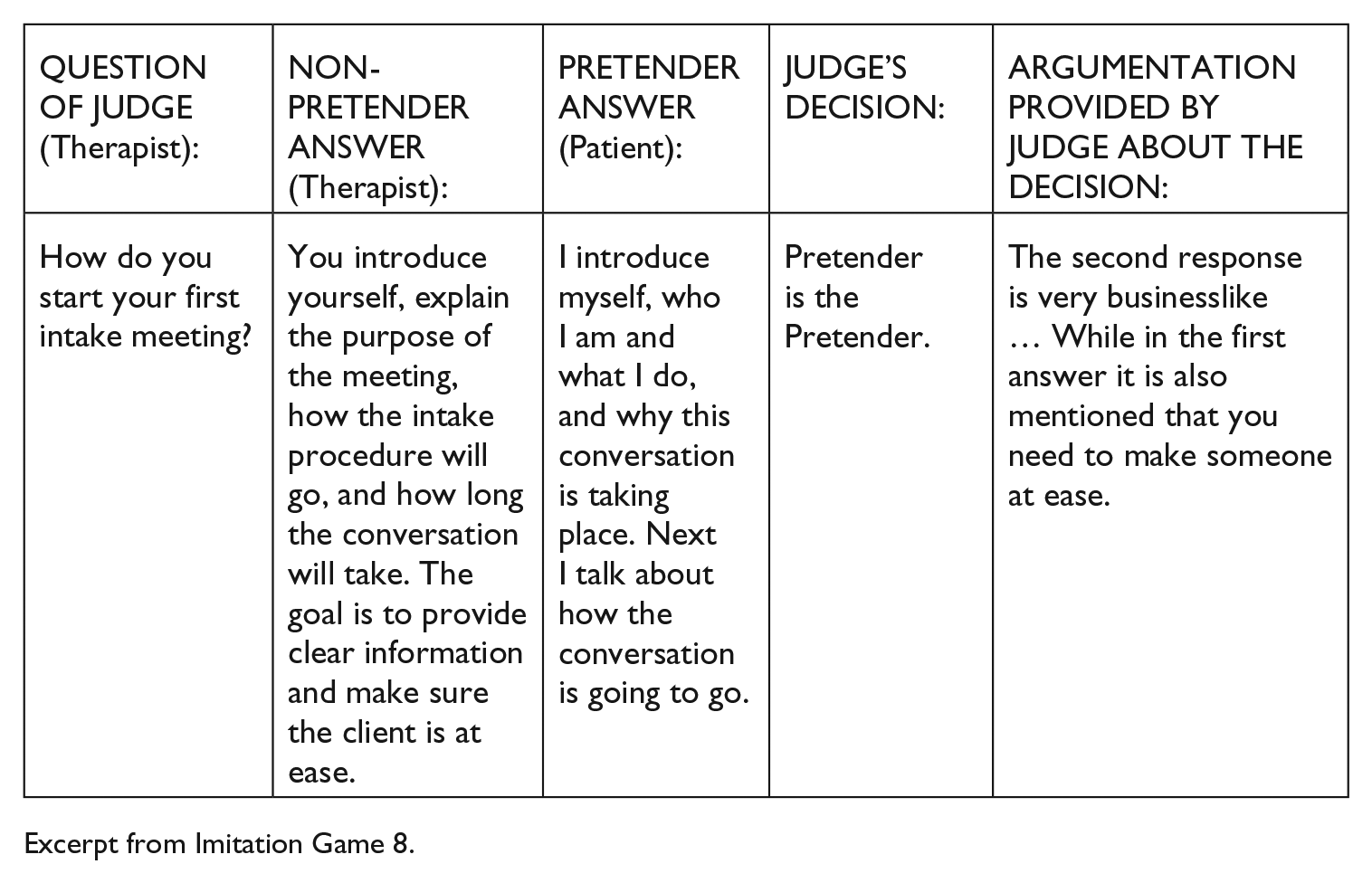
Excerpt from Imitation Game 8.
During intake meetings, therapists need to do more than simply discussing the steps of therapy at the centre, such as how to make a patient feel at ease. This more tacit dimension is not recognized by this patient.
The second sub-domain is about negotiating autonomy. This is another implicit aspect of therapeutic work that is often missing from the more rationalized view that patients have of therapists, such as when considering hospitalizing a patient:
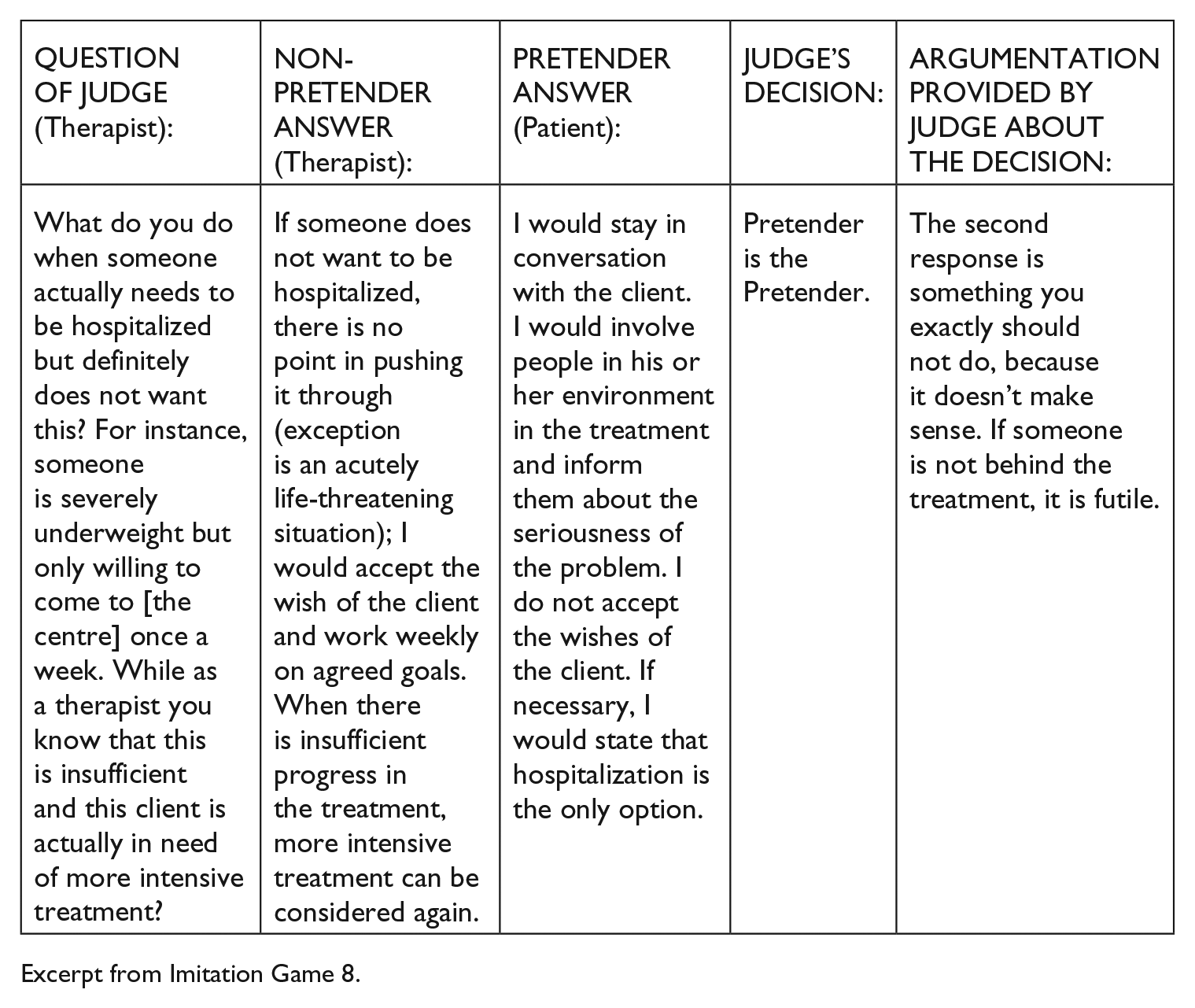
Excerpt from Imitation Game 8.
This excerpt shows that therapeutic work is not only based on the ‘rational’ decision of the therapist (as assumed here by the pretending patient). Instead, therapeutic work is a delicate process of negotiating the patient’s autonomy: trying to determine when someone is ready to change while recognizing the patient’s autonomy in this change process.
The third sub-domain could be described as tinkering (a term coined by Mol et al., 2010, to describe the ‘attentive experimentation’ done by caregivers in order to adapt to specific situations). Many patients viewed therapeutic work as only protocol based, whereas therapists emphasized the continuous balancing, experimenting and compromising involved in providing therapy. However, an excerpt from the joint focus group reveals how the patient understands therapeutic work:
What did you find hard about pretending to be a therapist?
I think I tried too hard about … using protocols and fancy terms and such. […] I really tried to pretend to be someone with a systematic approach. (Joint focus group, 12 September 2013, emphasis added)
It was primarily this strategy of overemphasizing the systematic approach that revealed most patients as pretenders. While patients had some knowledge of the work of therapists, they did not have a ‘feel’ for it.
In sum, there are many implicit aspects of how therapists experience their work that are not well understood by patients. In contrast, therapists were able to express knowledge of particular aspects of the lived experiences of those with an eating disorder (the fear of losing control) but had difficulties in relation to more subtle aspects (the conflicting meanings patients experienced in objects such as mirrors or the identification of the eating disorder as ‘part of the self’).
Discussion
This research investigated the ways in which patients and therapists involved in eating disorder treatment were or were not knowledgeable of each other’s experiences. The Imitation Game was a valuable method for unravelling the domains in which such substantive understanding did or did not develop. This discussion interprets the empirical results in the light of existing research on eating disorder experiences and the therapeutic relationship. Given the novel character of the method and the new application of this method to the context of health research, the discussion also reflects on the strengths and limitations of the Imitation Game as an interdisciplinary method.
Interpreting the results
The empirical results resonate with phenomenological literature on eating disorder experiences and with ethnographic accounts on therapeutic work. Both the importance of ‘control’ and the view that the eating disorder constitutes a ‘part of the self’ have been noted in previous literature (Rich, 2006; Tiggemann and Raven, 1998; Walters et al., 2015; Warin, 2005). The large tacit dimensions of therapeutic work have also been regularly discussed in ethnographic literature (Mol et al., 2010; Welsh and Lyons, 2001). Most research in the eating disorder field focuses solely on the lack of understanding therapists have about the experiences of patients. The results of this study indicate, however, that there are also many aspects in which patients lack understanding of therapist’s experiences and the implicit aspects of therapeutic work. This points to important new directions for research; this could include researching how such differences in understanding contribute to the complicated relationships between therapists and patients and whether increased insights into the tacit dimensions of therapeutic work can lead to improved mutual understanding and, ultimately, better outcomes for both the patients and their therapists.
The Imitation Game and interdisciplinarity
The complex nature of many health problems, including eating disorders, necessitates interdisciplinary approaches. When exploring health concerns such as eating disorders, it is important to utilize concepts, insights and methodological approaches from other fields. While previously used in the sociology of knowledge, the Imitation Game is a useful methodology for exploring patients’ and therapists’ experiences. Based on this empirical study, two beneficial aspects of applying this novel method can be identified.
First, the Imitation Game is able to connect strands of research that have been mostly separate. Although numerous studies investigated the lived experiences of patients, they seldom investigate whether professionals are able to understand these experiences. However, literature in the domain of PPC focuses primarily on effective forms of PPC, while largely neglecting the actual content of patients’ illness experiences. As an innovative methodological approach, the Imitation Game is able to connect these different strands and deliver clear data on both PPC and the content of illness and treatment experiences.
Second, although the notion ‘explanatory models’ sensitizes us to differences between medical understandings of illness and the lived experiences of patients, the core concepts underlying the Imitation Game (‘contributory expertise’ and ‘interactional expertise’) can offer a broader interpretative frame for understanding the experiential knowledge of patients, its shared component (socialization) and the various ‘explanatory models’ of illness. The notion of ‘contributory expertise’ offers an interpretative frame to understand the experiential knowledge chronically ill patients develop through their lived experiences with a specific condition (an eating disorder, in this case). Similarly, the notion of ‘interactional expertise’ offers a frame to understand (and empirically investigate) the ability of health care professionals related to understanding the lived experiences of patients with eating disorders.
The Imitation Game as ‘can opener’
This is one of the first studies worldwide that utilizes the Imitation Game method in a health-care context. Through this approach, the study was able to provide an in-depth understanding of therapists’ and patients’ understanding of each other’s lived experiences in the context of eating disorder treatment.
As an innovative method, the Imitation Game also raises questions. One question is how in-group variety can be taken into account, as not every patient has similar experiences. While this could become problematic when the Imitation Game is utilized only as a quantitative test to find out the percentage of therapists able to ‘pass’ as pretender, 8 such issues are much less problematic when the Imitation Game is used for qualitative purposes. As such, it can render these differences visible through a detailed analysis of the dialogues.
Second, as the Imitation Game is a form of written communication, this raises the question of how much language skills (how well someone is able to express himself/herself) influence the Judge’s decision. However, the influence of language skills is likely to be mostly problematic for a quantitative comparison (as it may be read as a ‘contamination’ of the results), whereas for a qualitative analysis, the content of dialogues is most relevant.
Based on this study, we propose that the Imitation Game can best be conceptualized as a ‘can opener’ that enables the development of in-depth, qualitative insights into the substantive themes that matter in the lifeworlds of patients and therapists.
Conclusion
The question of whether health-care professionals are able to understand the lived experiences of their patients is very important but is under-investigated empirically. While interpretive phenomenological analyses focus on patient experiences and illness narratives (but not on therapist’s understanding), PPC surveys focus primarily on effective forms of communication without addressing the actual illness experiences of patients. There is a need for empirical research that combines both strands of research to investigate not only the experiences of patients but also whether professionals are able to understand these experiences. This study combined both strands by means of a novel research method called the Imitation Game. It focused on eating disorder treatment to investigate whether therapists were able to understand the experiences of their patients and vice versa. This study showed that there are not only domains in which therapists developed substantive knowledge about the lived experiences of patients but also domains in which they had more difficulties. Furthermore, patients were able to develop substantive knowledge about the experiences of their therapists but overall had a rather rationalized understanding of therapeutic work.
The application of the Imitation Game to research patient experiences and PPC proved advantageous in two ways. First, the method was able to connect strands of research that have hitherto been mostly separate. Second, the core concepts underlying the Imitation Game offered a broader interpretative frame for understanding the experiential knowledge of patients and the various ‘explanatory models’ of illness. Based on this study, we propose that the Imitation Game may be particularly valuable as a ‘can opener’ that enables the development of in-depth, qualitative insights into themes that matter in the lifeworlds of patients and therapists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.