
Abstract
In the past few decades, photovoice research has gained prominence, providing context rich insights through participants’ photographs and narratives. Emergent within the field of photovoice research have been health studies embracing diverse illness issues. The goal of this scoping review article was to describe the use of photovoice in mental illness, paying particular attention to the following: (1) the study design and methods, (2) empirical findings, and (3) dissemination strategies. Nine qualitative studies (seven drawing from primary and two secondary analyses) featuring diverse approaches to analysis of data comprising individual and/or focus group interviews using participant-produced photographs were included in the review. Described were participant’s experiences of living with mental illness and/or substance overuse, including feelings of loneliness and being marginalized, along with their support care needs (e.g. physical, emotional, and spiritual) to garner self-confidence, respite, and/or recovery. Empirically, the reviewed articles confirmed the value of participant-produced photographs for obtaining in-depth understandings about individual’s mental illness experiences while a focus on stigma and recovery was prominent. In terms of dissemination, while most of the published articles shared some participants’ photographs and narratives, less evident were strategies to actively engage the public or policymakers with the images. Recommendations for future photovoice research include conducting formal analyses of participant photographs and strategically lobbying policymakers and raising public awareness through virtual and “in person” photo exhibitions while de-stigmatizing and affirming the experiences of those who are challenged by mental illness.
Introduction
Mental illness has become a leading cause of disease burden particularly within developed countries (National Institute of Mental Health, 2006; World Health Organization, 2010). However, as Ridge (2008) suggests, the interiority of mental illness challenges researchers and clinicians as well as those directly impacted to understand the diverse lived experiences that can emerge. One potential avenue to describe and address mental illness issues is the use of visual research methods (Emmison and Smith, 2000). Although visual methods have been somewhat under-valued in health research (Eisner, 2008), their capacity to provide powerful, nuanced accounts—critical to understanding health and illness issues—has also been evident (Bauer and Gaskell, 2000; Knowles and Cole, 2008). The purpose of the current scoping review article is to describe the use of photovoice visual methods in mental illness and to make recommendations for future research based on those findings.
Background
Photovoice and health research
Visual research addressing health and illness issues has used an array of data including photographs, drawings, diagrams, advertisements, and visual performances (Bauer and Gaskell, 2000; Emmison and Smith, 2000; Knowles and Cole, 2008). Among the visual data options, photographs have been prominent, and featured in a variety of photo-elicitation approaches (Harper, 2002), including photovoice (Wang et al., 1996), photo-essay (Corwin, 1985), autodriving (Heisley and Levy, 1991), and autophotography (Noland, 2006). Common to the aforementioned photo-elicitation methods is the soliciting of information within participant interviews and/or focus groups by inserting existing, researcher-sourced, and/or participant-produced images (Harper, 2002). While collecting participant narratives and visual data is also central to photovoice, the approach is differentiated by the exclusive use of participant-produced photographs (Harper, 2002; Wang and Redwood-Jones, 2001).
Photovoice also draws on participatory action research (PAR) to purposefully connect researchers and participants to design projects, to gather and interpret data, and to disseminate the findings from that work (Catalani and Minkler, 2010; Wang and Burris, 1994; Wang and Redwood-Jones, 2001). In “giving the lens to participants,” empowerment education, feminist theory, constructivism, and non-traditional approaches to documentary photography are central to photovoice: (1) enabling people to record and reflect their community’s strengths and concerns, (2) promoting critical dialogue and knowledge about important issues through large and small group discussion of photographs, and (3) reaching the public and policymakers (Wang and Burris, 1994). In terms of benefits, photovoice can facilitate dialogue and storytelling (Bauer and Gaskell, 2000; Foster-Fishman et al., 2005; Tinkler, 2013). Shared through photographs can be a wealth of information including contextual and symbolic representations (Harper, 2002) that serve to stimulate self-reflection and develop thick descriptions and nuanced meanings about participants’ experiences (Berman et al., 2001). In addition, when research processes message and lobby stakeholders and decision-makers, participants can witness how their insights and lived experiences prompt social, community, and political action (Wang and Burris, 1994).
In health research, photovoice methods have purposefully engaged participants to reflect upon and illustrate their experiences about an array of issues including smoking (Oliffe et al., 2010), grief associated with the loss of a male peer to an accident (Creighton et al., 2013), unintentional childhood injuries (Brussoni et al., 2013), and prostate cancer (Oliffe and Bottorff, 2007). Prevailing across much of the photovoice health research are processes wherein participants are interviewed (e.g. individual and/or focus groups) and invited to discuss their photographs and reflect upon the issues most relevant to them. Some studies have also used participant photographs and narratives to lobby health and social change with broader communities and policymakers. For example, Seitz et al. (2014) used a public photovoice exhibit to advocate for change to a campus smoking policy, and Mitchell et al. (2005) reached out to the teachers and community health workers in South Africa to educate and raise awareness about youth HIV and AIDS. The emancipatory qualities of photovoice are well suited to exploring and de-stigmatizing an array of diseases including mental illness (Lysaker et al., 2007; Schnittker, 2013; Stevens, 2004). Although one in four people suffer mental illness (World Health Organization, 2010), it remains deeply stigmatized, inhibiting individuals from expressing their feelings and/or seeking professional help (Lysaker et al., 2007). The purpose of the current scoping review article is to describe the use of photovoice visual methods in mental illness and to make recommendations for future research based on those findings.
Methods
Scoping reviews can be used to determine the value of undertaking a full systematic review or as a means to providing a summary of research findings drawn from existing literature wherein the primary aim is to identify research gaps and make recommendations for future studies. The current scoping review is informed by the latter aim, focused on identifying broad themes and patterns, mapping the most common photovoice approaches for examining mental illness, amid offering suggestions for future photovoice research (Armstrong et al., 2011; Levac et al., 2010; Rumrill et al., 2010). The decision to conduct a scoping review was also informed by our suspicion that there was not enough literature or evidence to conduct a full synthesis, and that further primary research was likely needed (Canadian Institutes of Health Research (CIHR), 2014).
A search of the literature using online electronic databases was conducted in December 2013. The literature search terms and processes mirrored Catalani and Minkler’s (2010) approach to reviewing photovoice and public health research. In brief, Catalani and Minkler (2010) used keywords including “photovoice” OR “photo novella” OR “participatory research” AND “photography” OR “photo” to retrieve 37 photovoice articles addressing public health issues. In this study, Catalani and Minkler’s (2010) aforementioned keywords were used, not limited by any field (e.g. abstract, keywords) or time frame, to search PsycINFO, PubMed, Web of Science, and MEDLINE/PubMed. Retrieved and exported to RefWorksTM were 382 peer-reviewed articles published in English. After reviewing 382 article abstracts, 373 articles were excluded because they were duplicates or did not focus on people’s experiences of mental illness.
Mental illness was defined in the current scoping review as a self-identified and/or clinically significant syndrome affecting cognition, emotion, and/or behaviors (Kecmanovic, 2013; Manderscheid et al., 2010). Studies that did not explicitly focus on mental illness within the parameters of the aforementioned definition were excluded. For example, mental illness issues may have been present in Denov et al.’s (2012) article, ‘Engaging war affected youth through photography: Photovoice with former child soldiers in Sierra Leone’; however, it was excluded because the study focused on the participant’s post-war re-integration experiences to civilian life.
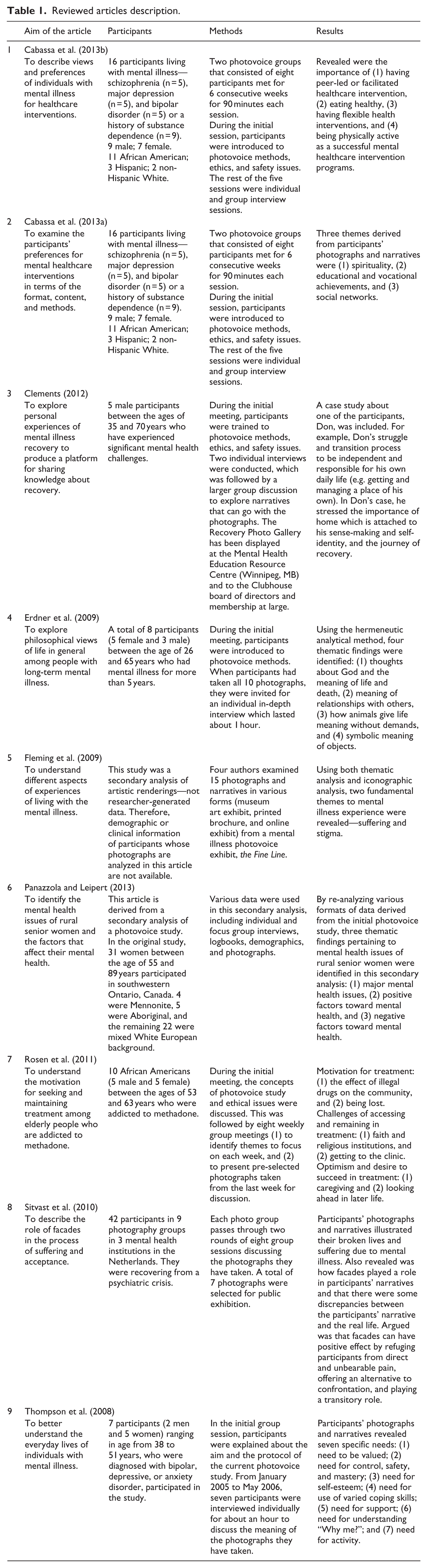
A total of nine articles were positively evaluated for qualitative quality (Tracy, 2010) and subsequently reviewed for the current scoping review (Table 1). The nine articles were read multiple times by the two authors and memos were made to summarize and categorize each article. The authors focused on (1) study design and methods, (2) empirical findings, and (3) dissemination strategies to detail each of the studies, and met to compare interpretations to inductively derive preliminary themes within each of the aforementioned categories. The analytic approach employed was constant comparison (Strauss and Corbin, 1998) wherein specific aspects of each study were examined to distill similarities and patterns as well as contextualize differences in the reviewed articles. Consensus about the findings within each category was reached through discussion, and in the writing up of the results. Within these analyses, we were ethical and reflexive in acknowledging potential biases and staying focused on thoughtfully and thoroughly synthesizing patterns reflecting what had been done (as distinct from belaboring what had not been done).
Reviewed articles description.
Results
Informed by the overarching research question, how has photovoice been used to research mental illness? the current scoping review describes (1) the study design and methods, (2) the empirical findings, and (3) dissemination strategies. Within the empirical findings, two sub-themes, (a) living with mental illness and (b) recovery from mental illness, are used to describe the most common study results. Based on the overall findings drawn from the scoping review, also provided are directions for future mental illness photovoice research.
Study design and methods
Of nine reviewed articles, seven were primary data studies (Cabassa et al., 2013a, 2013b; Clements, 2012; Erdner et al., 2009; Rosen et al., 2011; Sitvast et al., 2010; Thompson et al., 2008) and two were derived from secondary analyses of existing photovoice data (Fleming et al., 2009; Panazzola and Leipert, 2013). Authors of all nine reviewed articles claimed photovoice as a novel and effective methodology as well as a method of “knowing” beyond traditional quantitative and qualitative research approaches. In particular, central was PAR approaches involving participants throughout the photovoice process (i.e. formulation of research questions, design, implementation, analysis, and dissemination). Aside from the two secondary analysis studies, the reviewed study articles affirmed participants’ contribution to data collection and subsequent discussions (i.e. taking photographs and participating in interviews or group sessions). Clements (2012) also described actively involving participants in the research design, implementation, and dissemination stages (e.g. photo exhibits). Most studies also collaborated with community partners. For example, the Clubhouse of Winnipeg (an independent community-based mental health rehabilitation agency; Clements, 2012), a housing agency in New York City (Cabassa et al., 2013a, 2013b), a Midwestern teaching hospital’s psychiatric outpatient clinic (Thompson et al., 2008), mental health institutions in the Netherlands, (Sitvast et al., 2010), a methadone clinic (Rosen et al., 2011), and a community day center for people with long-term mental illness (Erdner et al., 2009) were featured study partners, all of whom played a pivotal role in participant recruitment.
Collaboration between researchers, participants experiencing mental illness, and/or agencies invested in advancing their well-being yielded two key benefits. First, the feasibility of conducting the research was likely enhanced because there was input to the study design and buy-in from stakeholders and gatekeepers. Second, the emancipatory goals of the studies were explicit and evident in that community partners and participants were involved from the outset in determining what as well as how their stories would be shared. Embedded in such collaboration and inclusion were epistemological and ontological overtures privileging and affirming the knowledge of those experiencing mental illness as key to understanding and addressing the needs of vulnerable sub-groups.
While the nine studies had institutional ethics approval, the specificities related to photovoice and the use of photographs were not detailed. Participant inclusion criteria comprised adults (i.e. >18 years) who experienced mental illness(es) and/or were in the process of recovering (Cabassa et al., 2013a, 2013b; Erdner et al., 2009; Rosen et al., 2011; Sitvast et al., 2010; Thompson et al., 2008). Purposive sampling, aided by community collaborations (Clements, 2012; Erdner et al., 2009; Panazzola and Leipert, 2013; Rosen et al., 2011), optimized the collection of information-rich cases (Cabassa et al., 2013a, 2013b; Fleming et al., 2009; Sitvast et al., 2010; Thompson et al., 2008). The number of study participants ranged from 5 to 42 (M = 18). 1 Assurances that participants had the cognitive capacity to provide informed consent were made, and some studies provided specific details about participants formally diagnosed with mental illness(es) (Erdner et al., 2009; Rosen et al., 2011; Sitvast et al., 2010; Thompson et al., 2008), while others used the term mental illness to detail the sample (Cabassa et al., 2013a, 2013b; Clements, 2012; Fleming et al., 2009; Panazzola and Leipert, 2013).
All the studies were grounded in the tradition of qualitative research methods, although Sitvast et al. (2010) adopted a mixed-methods design comparing participants’ self-reports against their official health records. In terms of study procedures, at the initial researcher–participant meeting, researchers typically assessed potential participants’ capacity to consent, explained the study, obtained written consent, collected demographic and other information, gave out cameras, and discussed safety and ethics measures. During the subsequent individual and/or group interview sessions, participants shared their stories by talking about their photographs. For example, Sitvast et al. (2010) met with participants for two rounds of eight sessions, focusing on participants’ emotional experiences as well as visualization of their life goals in the photographs. Also noteworthy was the use of a semi-structured interview guide “SHOWED” 2 in Cabassa et al.’s (2013a, 2013b) study, a tool used to direct the focus group dialogue in discussing participants’ photographs. The participant interviews were all transcribed verbatim, and focused on photographs selected by participants.
Diverse qualitative and visual data analyses were operationalized to interpret participants’ narratives and meanings attributed to their photographs. The array of approaches used reflects Wang and Burris’ (1997) assertion that photovoice is intentionally eclectic in how the data are analyzed. That said, constant comparison (Cabassa et al., 2013a, 2013b; Thompson et al., 2008) synonymous with grounded theory (Strauss and Corbin, 1998) was the most commonly cited analytic frame. Consistent with PAR, Clements (2012) and Rosen et al. (2011) invited their study participants to the analysis phase. Clements’ (2012) researcher–participant group discussed the concept of recovery using thematic analysis techniques, while Rosen et al.’s (2011) discussed the meaning of the older African American methadone clients’ images. However, most studies (n = 7) were researcher-centric in detailing “their” data analyses procedures. For example, references were made to listed authors of these seven studies independently reading interview transcripts, examining photographs and other relevant documents (e.g. participant observation, field notes, and health records) to develop preliminary codes (Cabassa et al., 2013a, 2013b; Erdner et al., 2009; Fleming et al., 2009; Panazzola and Leipert, 2013; Sitvast et al., 2010; Thompson et al., 2008). Some researchers also met to discuss their independent interpretations of the data to shape codes and categories and develop and theorize overarching themes and sub-themes (Cabassa et al., 2013a, 2013b; Fleming et al., 2009; Sitvast et al., 2010; Thompson et al., 2008). Implicit to these procedures is that the researchers are best credentialed to analyze the data and summarize the predominant participant viewpoints. While it can be reasonably argued that this approach breaks with the empowerment ideals underpinning PAR, it is important to note that in most studies, the findings were shared with the participants to ensure the representativeness of the findings (Cabassa et al., 2013a, 2013b; Clements, 2012; Rosen et al., 2011; Sitvast et al., 2010).
In terms of the specific data analyzed, most studies provided interpretations about participant narratives, and only two studies included formal analyses of photographs as well. For example, Fleming et al. (2009) employed an iconographic approach from visual anthropology to analyze participant photographs, focusing on the levels of abstraction. Specifically, the first stage considered was the “everyday recognition of the subject and surroundings,” while the second level included abstracting patterns including cultural symbolic features. Similar to constant comparative analyses applied to the participant narratives, thematic content analysis on the photographs was conducted to identify key elements and impressions, which were eventually clustered into themes (Fleming et al., 2009). Sitvast et al. (2010) used a semiotic approach to interpret the photographs as an arbitrary sign, paying particular attention to perspective, focus, tone, setting, and themes, and these symbolic meanings were subsequently targeted to understand the context. Evident by the absence of a formal analysis in seven studies was the positioning of the photographs as conduits to promote participants talk in interviews.
Empirical findings
While the articles engaged a range of mental illnesses among participants from diverse backgrounds, the findings drawn from the studies tended toward two themes. First, thick description prevailed wherein participants’ experiences of living with a mental illness featured. Balanced with this were narratives and images depicting recovery from mental illness. Of course, these findings were not mutually exclusive but instead intertwined highlighting the stigma accompanying mental illness amid chronicling potential remedies. The two sub-themes also served to provide hope in what could have emerged as our first-hand accounts of living with a mental illness.
Living with mental illness
Five studies described personal experiences of everyday life among participants with mental illness (Erdner et al., 2009; Fleming et al., 2009; Panazzola and Leipert, 2013; Sitvast et al., 2010; Thompson et al., 2008). Central to these studies was a focus on chronicling the day-to-day challenges accompanying mental illness including specific feelings and the internal and external origins (i.e. self and society) of those experiences. For example, Thompson et al.’s (2008) study of seven participants diagnosed with depressive and/or anxiety disorders described how participants needed to be valued juxtaposing that they frequently felt invisible and misunderstood in society. Craved also was control, safety, and mastery—both physical and emotional—along with participant narratives lamenting why they had a mental illness (Thompson et al., 2008). Similarly, Erdner et al.’s (2009) study of eight participants detailed how a lack of interpersonal contact and closeness fueled mistrust in others and created “existential loneliness” which exacerbated some participants’ mental illness. Fleming et al. (2009) featured 15 photographs and narratives in a mental illness photovoice exhibit called the Fine Line Art, revealing two themes—suffering and stigma. Participant accounts of depression, anxiety, irritability, and fear summed up the experiences of emotional suffering of individuals living with mental illnesses, and these experiences were strongly represented in their photographs (Fleming et al., 2009). Discussed was how stigma outcast participants, damaging their identities and confidence—leading them to further isolate (Fleming et al., 2009). The absence of, or negative sense of, self was also discussed in Panazzola and Leipert’s (2013) study of 31 women ranging in age from 55 to 89 years old. The findings described participants’ feelings of loneliness and being unable to appreciate themselves (e.g. negative self-concept) as the major contributor to mental illness (Panazzola and Leipert, 2013). Also detailed were inadequate community resources along with participant stories about how being devalued—due to their living environments (i.e. rurality), ethnicity, and gender—was detrimental to the mental health of the women (Panazzola and Leipert, 2013).
Across all the aforementioned studies was evidence for how external and internalized stigma flowed to and from mental illness to marginalize, “other,” and ostracize the participants. The overall findings depicting experience were particularly powerful for connecting the interiority of participants’ mental illnesses with other factors to signal an array of potential triggers. While Sitvast et al.’s (2010) study also did this, it differed in that participant’s strategies for dealing with mental illness symptoms were also described, and to some extent critiqued. Specifically, participants’ broken lives were explained in the context of how facades 3 permeated their narratives and the handling of suffering in their storytelling (Sitvast et al., 2010). Specifically, 10 of the 42 participants were suggested to embody facades by denying and/or blunting painful feelings associated with their mental illness. While facades could offer individuals an alternative to confrontation reducing suffering from emotional and psychological pain, Sitvast et al. (2010) suggested that these facades needed to be surpassed to effectively overcome suffering.
Recovery from mental illness
Six articles discussed individuals’ recovery from mental illness (Cabassa et al., 2013a, 2013b; Clements, 2012; Panazzola and Leipert, 2013; Rosen et al., 2011; Thompson et al., 2008). The centrality of peer and community supports predominated in the studies addressing recovery from mental illness. For example, Panazzola and Leipert (2013) highlighted how social support from family and friends could catalyze an array of positive personal characteristics including resilience to bolster mental health. Evident also was the effectiveness of social networks and supports for initiating change and maintaining a healthy lifestyle. Rosen et al.’s (2011) study of 10 senior African Americans described how the use of illegal drugs had invaded and destroyed their lives and communities in asserting they were “sick of being sick” and signaling their collective desire to re-build their community by being “clean” and sober. Also revealed was how faith- and community-based religious institutions could help garner and sustain their recovery proving a “second chance” (Rosen et al., 2011). The Our Photos, Our Voices study chronicled the importance of community in describing the recovery efforts of five male participants (Clements, 2012). One participant, Don, provided an especially compelling account of his struggle and transition to becoming independent and responsible for his own life (e.g. getting and managing a place of his own). Evident in Don and the other participants’ interviews was the importance of having a home to bolster self-identity and anchor their efforts toward recovery (Clements, 2012).
Some studies provided evaluations of existing programs in detailing positive influences aiding recovery from mental illness. Cabassa et al.’s (2013b) study examining 16 individuals with serious mental illness suggested that effective mental healthcare programs (1) were peer-led or facilitated, (2) flexible, and (3) included healthy eating and physical activity. In addition, the interactive qualities of the program were the lynchpin to remedy as well as to prevent depression from reoccurring. In the subsequent article drawn from the same dataset, Cabassa et al. (2013a) elaborated on participants’ preferences for mental healthcare programs across three themes: (1) spirituality, (2) educational and vocational achievements, and (3) social networks. Detailed was how participants drew strength and meaning-making through spirituality (e.g. faith, prayers, meditation, and reading the Bible) making functional gains through life achievements (e.g. formal credentials, jobs, hobbies). Participants in Thompson et al.’s (2008) study also identified the need for activity and the benefits of being busy as well as the need for coping skills and physical and emotional supports to effectively manage their mental illness. The aforementioned studies explicitly connected community-based and professional programs to participant’s recovery from mental illness. By distilling key ingredients from end-user perspectives, these studies also had the potential to inform other mental health programs and those who attended them.
Dissemination strategies
While photovoice offered two distinct but connected data—photographs and narratives—the participant-produced photographs were less visible than their narratives in the published articles. For example, only four articles included participant-produced photographs accompanied by the corresponding captions/narratives to share participants’ experiences and perspectives about recovery from mental illness (Cabassa et al., 2013b; Clements, 2012; Panazzola and Leipert, 2013; Thompson et al., 2008). This trend may have been influenced by specific journal regulations governing the use and/or number of images included in the published articles. As well, ethics and copyright issues related to publishing participants’ photographs may have underpinned these editorial decisions. Hierarchies may have also privileged the written word and narratives to convey the qualitative findings implying greater empirical weight for the written word compared to images. Three articles did not include photographs or narratives (Cabassa et al., 2013b; Erdner et al., 2009; Fleming et al., 2009). Instead offered were the researchers’ analyses without illustrative examples drawn from the empirical data. This approach might be argued as traversing the emancipatory goals of PAR by relying on the researchers to reliably share the overarching story. Inversely, this approach might purposefully refute the need to convince readers of a single truth or scientifically prove their findings.
In terms of other dissemination strategies, only three studies included photographic exhibitions to share the data and/or results with the public. Collaborating with the Clubhouse of Winnipeg and the study participants, Clements (2012) hosted a series of photographic exhibitions, the Recovery Photo Gallery. Featuring 18 selected photographs and corresponding narratives, the exhibit toured and is currently on permanent display at the Clubhouse of Winnipeg. Similarly, Cabassa et al. (2013b, 2013a) and Sitvast et al. (2010) showcased selected photographs and narratives in public exhibitions. These exhibitions attracted diverse audiences with the intent of raising public awareness and de-stigmatizing mental illness.
In summary, few details about dissemination were shared in the articles we reviewed. Perhaps this reflects understandings that dissemination is the central motivation for publishing journal articles. Some studies may have had the budget to host other dissemination events such as exhibitions and/or the published articles may have been de-linked from such activities.
Discussion
Overall, the findings drawn from the current scoping review confirm the potential of photovoice for eliciting and connecting visual and narrative data to advance understandings of people’s “lived experiences” (Plunkett et al., 2013). From ontological and epistemological standpoints, affirmed is the value of sharing multiple truths and realities in chronicling an array of mental illness experiences across particular themes. Evident also is the therapeutic value of providing participants opportunities to positively reframe meanings in their mental illness and lives (Sitvast and Abma, 2012). Elaborating on these points, the following discussion synthesizes key design, empirical and dissemination issues in making recommendations for future photovoice research addressing mental illness.
In terms of study design, well documented in the literature are the theoretical, methodological, and practical challenges for developing in-depth understandings about the lived experiences of marginalized sub-groups (Dadich and Muir, 2009; Parr, 1998). This is due, at least in part, to the struggles individuals can experience in disclosing and/or conveying their emotions using conventional interviews or survey methods that rely on the spoken word and/or responses to specific questions (Cabassa et al., 2013a; Green and Thorogood, 2009). In particular, people experiencing mental illness are often accustomed to concealing and/or disguising their illness as a means to avoid the stigma and shame that so often accompany such conditions (Schnittker, 2013; Stevens, 2004). Therefore, essential are efforts to provide mechanisms and explicit permission for participants to access, reflect upon, and authentically reveal their mental illness experiences.
By taking photographs of their everyday life and reflecting on events that can go unnoticed, a therapeutic effect through participants’ self-enlightenment or new perspectives may also have been garnered (Sitvast et al., 2010). Similarly, in chronicling recovery processes, participants’ lived experiences can provide important insights to guide the efforts of mental healthcare providers and the families and friends of those individuals experiencing mental illness (Demerouti et al., 2011). These benefits reveal photovoice as a robust method ideally suited to describing mental illness issues while affording some important therapeutic value. In this respect, evident in the current scoping review was the potential for photovoice to be an elixir promoting participants’ talk as well as medium to illustrate what was felt and experienced in and around mental illness. Ever present also was the capacity of photovoice methods to empower marginalized sub-groups who endure mental illness (Wang and Burris, 1994).
The collective empirical findings drawn from the studies featured in the current scoping review are powerful both in what is said and how it is represented by words and images. The findings confirm the challenges faced by those experiencing mental illness while providing hope and direction in detailing strategies toward recovery. While the findings in and of themselves are not necessarily “new,” affirmed is the significant burden imposed by the internal and external stigma accompanying mental illness. In terms of future steps, repackaging the empirical findings or purposefully building strategies to privilege participant-produced photographs might find a wider audience to increase public awareness and de-stigmatize mental illness. In addition, while the focus of the reviewed studies was direct mental illness experiences, investigating the perspectives of family members and friends of individuals with mental illness may also be an important future research area. Extending beyond mental illness to more fully apprehend specific illnesses, including depression, anxiety, and suicidal behaviors, and where feasible stratifying by age, gender, and socioeconomic status might enable us to more fully understand the diversity and patterns within and across specific sub-groups.
A central mandate in photovoice research is to raise public awareness and influence policymakers (Wang and Burris, 1994). Although traditional ways of disseminating research findings through scientific journals and conferences engage academics and some clinicians, photovoice offers unique opportunities to innovatively message a range of stakeholders including the public and policymakers (Rynes et al., 2001). Given the accessibility and acceptability of photographs (Knowles and Cole, 2008; Liamputtong and Rumbold, 2008), participant-produced photographs can reach out to the public and contribute to rewriting social attitudes and beliefs about mental illness (Clements, 2012). In that sense, wider use of public photo exhibitions might strategically promote such changes. While public photographic exhibitions can be powerful dissemination platforms, budget implications as well as challenges accessing spaces to host “in person” exhibits are key issues. Therefore, augmenting and/or replacing in person exhibitions with online photo-exhibits and promoting these through social media channels might increase the reach of photovoice studies (Chung et al., 2009).
In sum, photovoice research can solicit and share insider’s views of mental illness, and this knowledge can influence clinical practice, raise public awareness, and guide policy amid empowering and affirming individuals in their quest for recovery. In line with the assertions of other researchers (Fleming et al., 2009; Plunkett et al., 2013), the findings from the current scoping review confirm photovoice as a means to de-stigmatize mental illness and design services to aid the well-being of those experiencing mental illness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research and the open access of this article were funded by Movember Canada (Men’s Mental Health Initiative) for the Masculinities and Men’s Depression and Suicide Network ![]() (Grant No. 11R18296). John Oliffe is supported by a 2014-2015 UBC Peter Wall Distinguished Scholar in Residence award.
(Grant No. 11R18296). John Oliffe is supported by a 2014-2015 UBC Peter Wall Distinguished Scholar in Residence award.