
Abstract
Little is known as to what drives feelings of grief and relief observed following the late identification of neurodivergence, and its significance as it relates to sense of self and self-understanding. As such, this study considers how grief is understood and experienced by neurodivergent individuals in the context of late identification. This study used qualitative content analysis to identify themes from 225 public social media posts discussing grief and relief in relation to a late identification. With a sample focused mainly on autism, attention deficit hyperactivity disorder, and both co-occurring, four main themes, under an overarching theme and process, titled the Grief, Relief, and Belief Cycle, were identified: (1) The Life I Could Have Had; (2) Grieving for My Younger Self; (3) Feeling Gratitude; and (4) Post-Diagnosis Burnout. Overall, this study calls for a paradigm shift in how we understand and support neurodivergent individuals diagnosed in adulthood, seeing diagnosis as a first step, rather than a terminal component of a service, emphasising the need for comprehensive, individualised, wraparound care that addresses the emotional and practical aspects of their lives before, during, and beyond diagnosis.
Lay Abstract
Little is known as to why some individuals may experience feelings of grief and relief following late identification, by clinical diagnosis or self-identification, of neurodivergence (e.g. autism or attention deficit hyperactivity disorder), and how this relates to their sense of self. This study looks at how grief is understood and experienced by late-identified neurodivergent individuals using qualitative content analysis to analyse social media posts discussing grief in relation to late identification. A total of 225 public social media posts were analysed. These posts were mostly made by people who identified as autistic, having attention deficit hyperactivity disorder, or both. Four main themes and one overarching theme and process were identified. The overarching theme was named the Grief, Relief, and Belief Cycle, and the four themes were (1) The Life I Could Have Had; (2) Grieving for My Younger Self; (3) Feeling Gratitude; and (4) Post-Diagnosis Burnout. Theme 1 highlights the sense of loss and regret some late-identified neurodivergent individuals’ experience. Theme 2 explores the ways in which late identified neurodivergent individuals look at their past experiences with this newfound understanding of their neurodivergence. Theme 3 highlights the experiences of relief and gratitude these individuals have for the self-understanding that they discuss coming with their diagnosis. Theme 4 emphasises the intense emotional and physical toll and lack of available support that people can experience when their neurodivergence is identified later in life. Overall, this study emphasises the need for comprehensive, individualised, and ongoing care that addresses the emotional and practical aspects of individuals’ lives before, during, and beyond diagnosis.
Although there is a wealth of phenomenological research on neurodivergence (Green & Shaughnessy, 2023; Murray et al., 2023), there remains a dearth of phenomenological research as to the impact late identification can have on sense of self, relationships with others, and mental health (Corden et al., 2021). This gap persists despite evidence that late identification and/or missed diagnosis is associated with adverse outcomes, such as increased rates of offending behaviour (Young & Cocallis, 2021; Young et al., 2011) and lower self-esteem (Beresford & Mukherjee, 2024; Corden et al., 2021). Understanding the impact of late identification is also becoming more important given its increase over the last decade, accounting for the “lost generation” of neurodivergent adults (Lai & Baron-Cohen, 2015; Thapar et al., 2017). As such, this phenomenological study draws on a large qualitative social media data set on grief in the context of neurodivergence to explore grief reactions observed in response to late identification of neurodivergence.
It is important to note that several key terms are used throughout this study: grief, late identification, and neurodivergence. First, a phenomenological understanding of grief has been drawn upon to understand grief as the primarily affective reactions one has to the loss of a relationship defining of their practical identity in such a way that one cannot return to this relationship in the same way as before (Cholbi, 2021); this way of understanding grief has been taken to also consider the relationship one has with the self (Bertrand, 2021; Clifton, 2014; Plant, 2022) insofar as a late identification would significantly alter this relationship and one’s own practical identity. Second, late identification is used as an umbrella term throughout the study, referring to the recognition and labelling of one’s own neurodivergence in adulthood (i.e. ⩾ 18 years of age), either via clinical diagnosis or self-identification. This definitional approach has been taken for two main reasons: (1) it explicitly values self-identification; (2) it accounts for ambiguity in posts insofar as it is not always clear if the posts discussed in this study are recalling narratives of clinical diagnosis or informal accounts of self-identification. In this sense, late identification is used to describe the journeys individuals have undertaken in adulthood to understand their own neurodivergence. Moreover, where explicitly known in the results, the form this journey may take (e.g. clinical diagnosis or self-identification) for different individuals will be explicitly outlined. Finally, as with other studies in related areas (e.g. Dahan-Oliel et al., 2012; Gini et al., 2021; Mahjoob et al., 2024), experiences and understandings of neurodivergent individuals are being considered through a transdiagnostic lens, as there are broad overlaps and shared vulnerabilities between different neurodevelopmental profiles (American Psychiatric Association [APA], 2022; World Health Organization [WHO], 2019) and, for individuals with a neurodevelopmental condition, having more than one is the norm rather than the exception (APA, 2022; Francés et al., 2022). As such, although neurodivergent is generally a term with incredibly broad meaning in terms of mental health and neurodevelopment (Mahjoob et al., 2024; Mair et al., 2024), which is used to describe having a mind which operates in a significantly divergent way from dominant societal understandings of normalcy (Walker, 2026), for consistency, clarity, and focus within the context of this study, using a definitional approach applied within similar studies (e.g. Mahjoob et al., 2024; Mair et al., 2024), the term neurodivergent simply refers to having one or more neurodevelopmental conditions as defined by the current clinical literature (APA, 2022; WHO, 2019).
The transdiagnostic lens employed in this study is essential for capturing how neurodivergence is lived, negotiated, and made meaningful within and outwith discrete diagnostic categories, which has been increasingly highlighted in the context of co-occurring autism and attention deficit hyperactivity disorder (ADHD), commonly referred to as AuDHD (Craddock, 2024a, 2024b). For example, rather than treating autism and ADHD as discrete or additive conditions, a transdiagnostic approach foregrounds shared, overlapping, and dynamically interacting dimensions of the AuDHD experience(s), such as attentional variability, intensity, sensory processing, and identity formation, that are often rendered invisible within siloed diagnostic frameworks. This understanding resonates with the current phenomenological research on AuDHD (e.g. Craddock, 2024a, 2024b, 2025). In parallel, current understandings within critical ADHD studies also challenge deficit-based constructions of ADHD by (re)framing attention and intensity as contextual and variable differences, while also attending to the ways in which neurodivergent identities are actively named, negotiated, and politicised within everyday and institutional contexts (Rosqvist et al., 2023a, 2023b, 2025). As such, situated within this body of scholarship and aligned with broader calls for critical ADHD studies that emphasise phenomenological and transdiagnostic approaches (e.g. Jackson-Perry et al., 2025), this study adopts a transdiagnostic lens in order to critically examine how diagnostic categories are experienced, traversed, and resisted in lived experience(s), thereby centring complexity, plurality, and neurodivergent meaning-making. In this sense, this study views neurodevelopmental concepts, which have been traditionally regarded within the academy and medicine as distinct clinical categories of neurodevelopmental deficit, as whole ways of being and engaging with the world, and as forms of life and identity formation which can be known and lived without being reduced into clinical categorical siloes of being less than that which is neurotypical (Chapman, 2019, 2020; Foucault, 1988a).
Current research on late identification has framed the experience in terms of difficulty (both affective and practical), self-understanding, and relief (Huang et al., 2020; Leedham et al., 2020; Nayyar et al., 2024). Difficulty in this sense relates to the events precipitating identification and/or clinical diagnosis, navigating diagnostic pathways and the lack of wrap-around support, the accessibility of diagnosis in terms of cost and socio-cultural biases, and the potential stigma associated with a diagnosis (Huang et al., 2020; Lockwood Estrin et al., 2021; Nayyar et al., 2024). Difficulty has also been identified in terms of grief reactions observed (Beresford & Mukherjee, 2024; Corden et al., 2021; Leedham et al., 2020), with late identification typically marking a juncture in assumptions one has made about their life and significant reappraisals of one’s identity and relationships (Corden et al., 2021; Leedham et al., 2020; Lupindo et al., 2023). This juncture between trying to cope with perceived loss in terms of sense of self and what this means for one’s life may be reflected in the dual process model of coping with grief (Fiore, 2021; Stroebe & Schut, 2010), which sees oscillations between loss-orientated coping states (e.g. acknowledging lost opportunities for earlier intervention/support and feeling regret/sadness) and restoration-orientated coping states (e.g. seeking information/support and developing new strategies). Overall, this model describes individuals oscillating between states of trying to cope with issues directly linked to the loss and living life in the context of secondary changes, brought on because of the loss itself.
Moreover, reappraisals in response to a late identification have generally been noted in a past-present-future orientated observation of self and other, which considers one’s sense of self, their narrative of the past, and their reframed perception of their future based upon a new self-understanding found in their diagnosis (Beresford & Mukherjee, 2024; Leedham et al., 2020; Stagg & Belcher, 2019). Although often tied to grief, self-understanding and relief in the context of late identification have been noted in relation to more positive affective reactions to the diagnosis and its impact on self-understanding and self-identity (Huang et al., 2020; Lupindo et al., 2023; Nayyar et al., 2024; Stagg & Belcher, 2019). These positive reactions ultimately appear to be reflected under a post-traumatic growth model of grief, where individuals demonstrate positive psychosocial change and growth following a significant stressor (Calhoun et al., 2010; Tedeschi & Calhoun, 2004).
It is also important to note factors which may influence age of diagnosis, as these may influence how one responds to the diagnosis and their experiences before, during, and after the diagnosis (Crane et al., 2016; Leedham et al., 2020; Lockwood Estrin et al., 2021). For example, factors related to broader neurodevelopmental profiles, rather than singular diagnoses, have been noted to impact upon age of clinical diagnosis; for instance, autism is typically diagnosed later when it co-occurs with ADHD (Sainsbury et al., 2023) and those with a communication disorder diagnosed in childhood have a higher likelihood of receiving an autism diagnosis in adulthood than those without (Huang et al., 2020; Mouridsen & Hauschild, 2009). There is also a dearth of high-quality research on the needs and experiences of adults with intellectual disabilities being diagnosed with co-occurring autism, as such, despite the high rate of co-occurrence, adults with intellectual disabilities are still likely to be under-represented/identified in adult autism pathways (Huang et al., 2020). Moreover, although there may be an awareness of a child’s difficulties related to their neurodivergence, a range of social, cultural, and economic factors can influence the age at which a diagnosis is provided or even assessed for, such as biases and reproductions of neuronormativity by parents, caregivers, and teachers who may prefer to avoid labelling the child in order to avoid perceived stigma which comes with a diagnosis (Crane et al., 2016). In addition, race and/or gender-based stereotypes which discount presentations of neurodivergence that do not align with normative assumptions and stereotypes (Huang et al., 2020; Lockwood Estrin et al., 2021), and the cost of a diagnosis and/or waiting times for assessment (Nayyar et al., 2024) can also impact upon age of diagnosis. Thus, many of these factors may contribute to poorer mental health outcomes and negatively influence how individuals relate to their own diagnosis; this occurs through the reinforcement of stigma and neuronormative practices, which can give rise to biases in assessment and diagnosis (Beresford & Mukherjee, 2024; Corden et al., 2021).
Another key reason which may account for late identification stems from individuals’ abilities to mask, camouflage, and employ compensatory strategies to avoid stigma for their neurodivergence (Beresford & Mukherjee, 2024; Nayyar et al., 2024), which has been highlighted in autism research, specifically in women and girls (Huang et al., 2020; Leedham et al., 2020; Lockwood Estrin et al., 2021). However, the use of specific compensation strategies is not identified across all late identifications of specific neurodivergences, such as in dyslexia (de Bree et al., 2022), and compensation is not unique to only those who are diagnosed later in life (APA, 2022; Chapman et al., 2022), though the reasoning behind employing compensatory strategies and minimisation of difficulties experienced may be qualitatively distinct (Asherson et al., 2012; Cook et al., 2021). Moreover, masking and compensation are energy intensive strategies (Cook et al., 2021; Pearson & Rose, 2021). As such, for those who effectively employ these coping strategies, their neurodivergence may only be outwardly apparent when demands exceed their ability to compensate (Asherson et al., 2012; Nayyar et al., 2024). This juncture has been linked with poorer mental health (Cook et al., 2021; Leedham et al., 2020; Lupindo et al., 2023), autistic burnout (Cook et al., 2021; Raymaker et al., 2020), and increased difficulty in school, employment, and social relations (Chapman et al., 2022; Leedham et al., 2020; Pearson & Rose, 2021).
Furthermore, late identification appears to be associated with specific mental health outcomes related to self-esteem (Beresford & Mukherjee, 2024; Corden et al., 2021). For example, those with a later clinical diagnosis of dyslexia tend to regard themselves as less competent and are less forgiving of the difficulties associated with their dyslexia than their peers with earlier identification (Battistutta et al., 2018; de Bree et al., 2022). This is also seen in those who developed self-blame and shame in relation to traits associated with their neurodivergence as a result of bullying and social isolation (Chou et al., 2018; Maïano et al., 2016), such as in depression and anxiety in late-identified autistic adults (Leedham et al., 2020; Lupindo et al., 2023; Stagg & Belcher, 2019). Therefore, late identification is also linked with increased perception, experiences, and internalisation of stigma related to neurodivergence (Battistutta et al., 2018; Nayyar et al., 2024).
Overall, late identification of neurodivergence is associated with many different challenges, including navigating diagnostic pathways, stigma, and the role of masking (Asherson et al., 2012; Beresford & Mukherjee, 2024; Corden et al., 2021). Although late identification has been linked with specific protective factors, such as an increase in self-understanding, self-compassion, and feelings of relief (Corden et al., 2021; Huang et al., 2020; Nayyar et al., 2024; Young et al., 2008; Zener, 2019), it is also associated with poor mental health outcomes related to stigma and self-esteem, grief, and burnout (Beresford & Mukherjee, 2024; Corden et al., 2021; Huang et al., 2020). However, little is known about what drives these feelings of grief and relief and the significance of late identification as it relates to sense of self and self-understanding. As such, this study explores grief reactions observed following late diagnosis, with the main research question being: how is grief understood and experienced by neurodivergent individuals upon late identification of their neurodivergence?
Methods
Search Strategy/Criteria
A protocol outlining the search strategy for data collection was written a priori and submitted alongside this study’s ethics application, which was granted favourable approval by the Clinical Psychology Ethics Committee at the University of Edinburgh. Data collected was taken from and indexed on a publicly available search engine to ensure (1) closed groups were not accessed; (2) data were indexed in such a way that it is accessible to the general public without any specific knowledge of the social media platform itself; and (3) rather than web scraping the data, the data used is reflective of that which is easily accessible to the general public and avoids accidentally or purposively mining more data and considering this public data just because it is obtainable using a specialised skillset.
Six different social media platforms were searched via Google in March/April 2023: Instagram, Reddit, TikTok, Tumblr, Twitter (now X), and WordPress. A series of search strings were run for each platform (Table 1). These strings were developed via personal knowledge of online neurodivergent communities, the use of hashtag generators, and piloting and refining the search strategy.
Development & Application of Search Strategy.
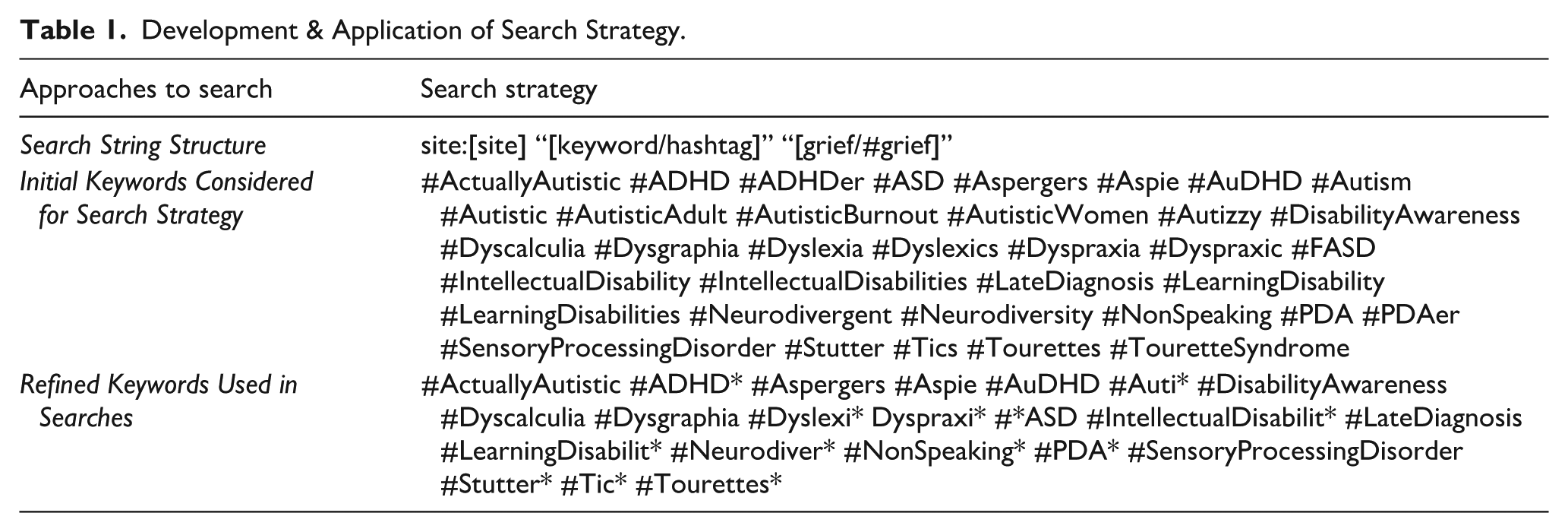
Data used in this study met the following criteria: (1) explicitly discusses grief and late identification of neurodivergence; (2) made by/with a neurodivergent individual, as explicitly indicated by the content of the post, and directly includes their voice (i.e. written by or directly quoting the neurodivergent person); and (3) the user did not indicate a wish to opt out, following the study’s intentions being communicated via a post with a link to indicate a wish to not have posts by a specific user accessed in this study, as this strategy was advised by the Data Protection Officer at the School of Health in Social Science at the University of Edinburgh. Although searches were only run in English, posts in all languages were considered.
Ethical Considerations
This study employed a social media ethics framework (Townsend & Wallace, 2016), following UK government (Social Media Research Group, 2016) and British Psychological Society (Kaye et al., 2021) guidance. Moreover, although this study involved no active participation, a system was set up to allow users to indicate they did not wish their posts accessed as part of this study and a Study Information Sheet (Supplementary Material 1) was used to communicate research intentions across platforms accessed.
Furthermore, to ensure anonymity and provide appropriate attribution of content (i.e. quoted content), a mode of delineating content which is authored, posted or private was established (Figure 1). Authored content is considered public and remains attributable to the individual who produced it, which is reflective of quotes used in results section (Supplementary Material 2). Authored content is considered as such if it is produced by a social media influencer (SMI) and/or professionals, activists, and/or advocates explicitly communicating in this role (Figure 2). Posted content is content which, although easily accessible to the general public, is posted in a context where privacy would be reasonably expected (i.e. not as an SMI or through a professional capacity); these data were collected for analysis but was anonymised and no direct quotes from posted content have been used in this article, as these would be easily retraceable. Finally, private content was not collected for analysis, this was any data in closed groups or from a private account.
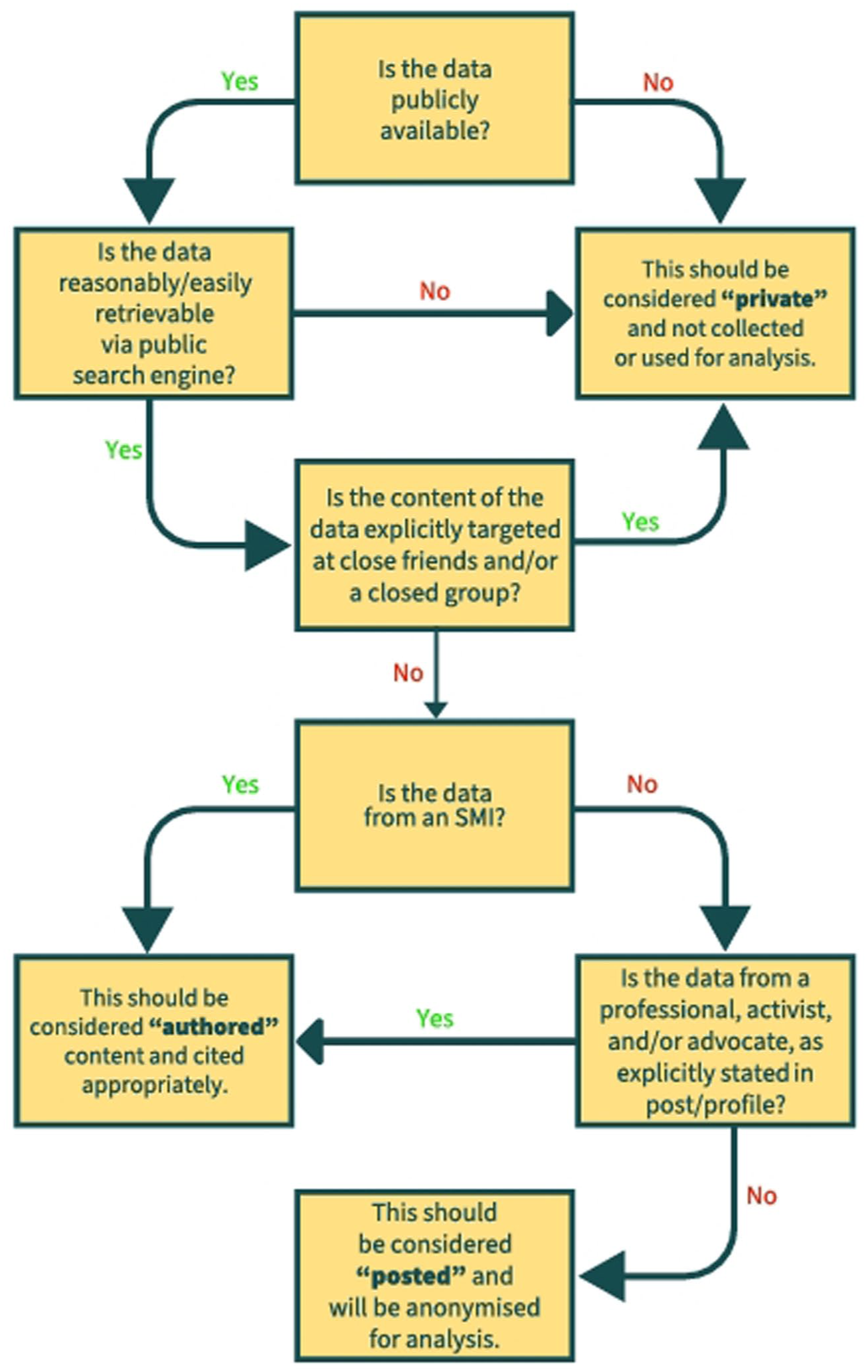
Flowchart of Authored, Posted or Private Content.
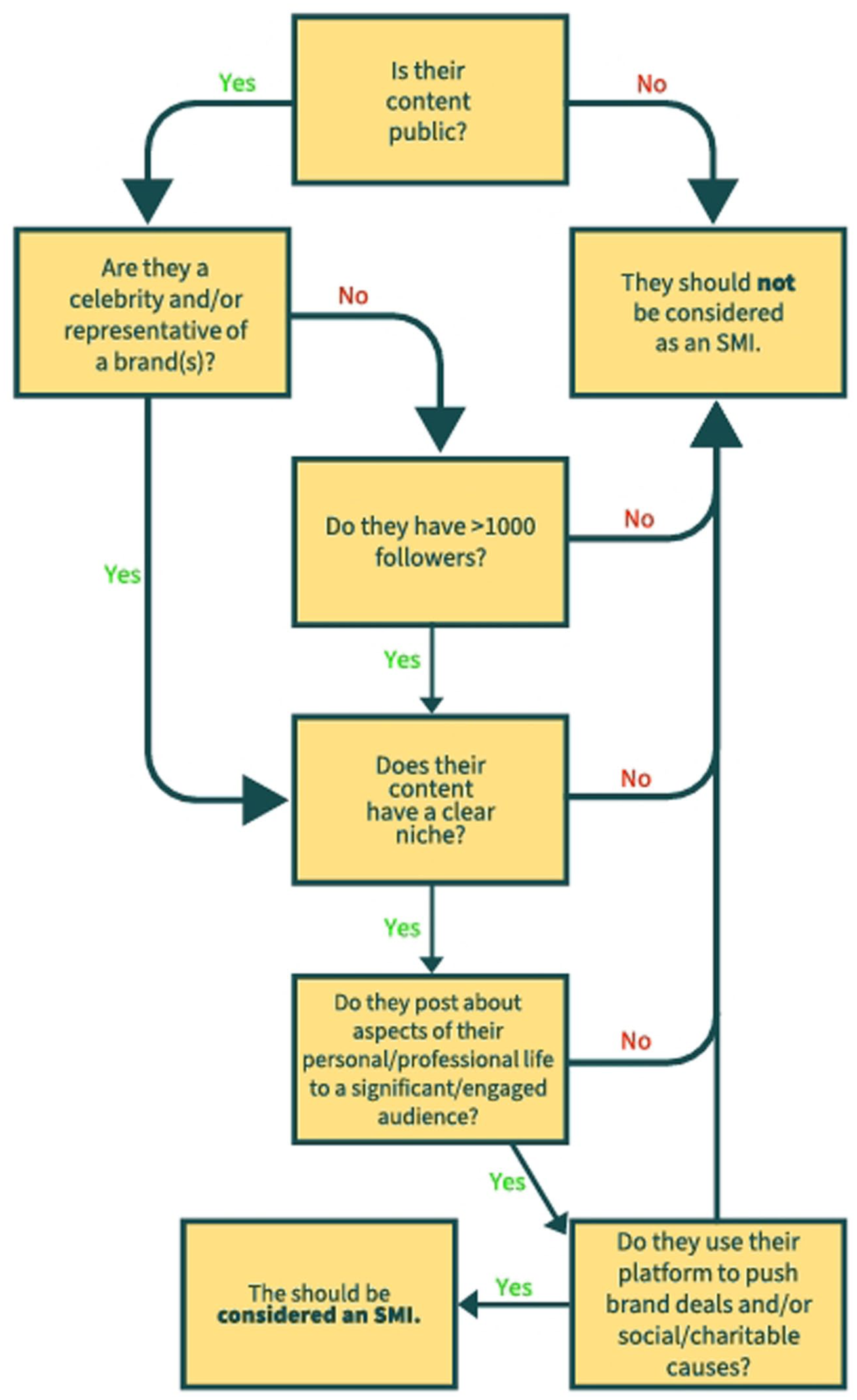
Social Media Influencer Flowchart.
Analysis
The data accessed in this study was taken from a larger social media study, which accessed 731 posts related to grief and neurodivergence across six social media platforms during March/April 2023: Instagram (n = 31), Reddit (n = 256), TikTok (n = 131), Tumblr (n = 64), Twitter (n = 58), WordPress (n = 103), and YouTube (n = 88). Of these posts, 31% (n = 225) observed grief and relief in relation to a late identification: Instagram (n = 7), Reddit (n = 91), TikTok (n = 39), Tumblr (n = 5), Twitter (n = 27), WordPress (n = 18), and YouTube (n = 38). These posts were analysed via a mixed-procedures inductive qualitative analysis using content structuring/theme analysis following Mayring’s (2022) 8-step approach to content analysis (see Supplementary Material 3 for full detail on analysis).
Positionality
When engaging in critical neurodivergent research, it is essential to present a sense of thereness, that which is the context, situatedness, and relationships which (in)form the research (Yergeau, 2018). This notion of thereness should extend beyond the researchers’ own (re)presentations of reflexivity and positionality, to also recognise how neurodivergent people actively (re)shape academic discourse, spaces from which they have long been excluded from (Rosqvist, Botha, et al., 2023; Yergeau, 2018). As such, this article, authored by a neurodivergent researcher, with analysis supported and validated by a neurodivergent peer researcher and in a team whose members hold personal and/or professional connections to neurodivergence (e.g. through family relationships or clinical practice), aims to foreground a neurodivergent thereness in research by recognising and validating diverse sources of knowledge (e.g. recognising the epistemic agency of neurodivergent individuals and regarding discussions produced by neurodivergent communities as genuine sites of knowledge production) and prioritising the voices of neurodivergent individuals sharing their own lived experiences and expertise.
Results
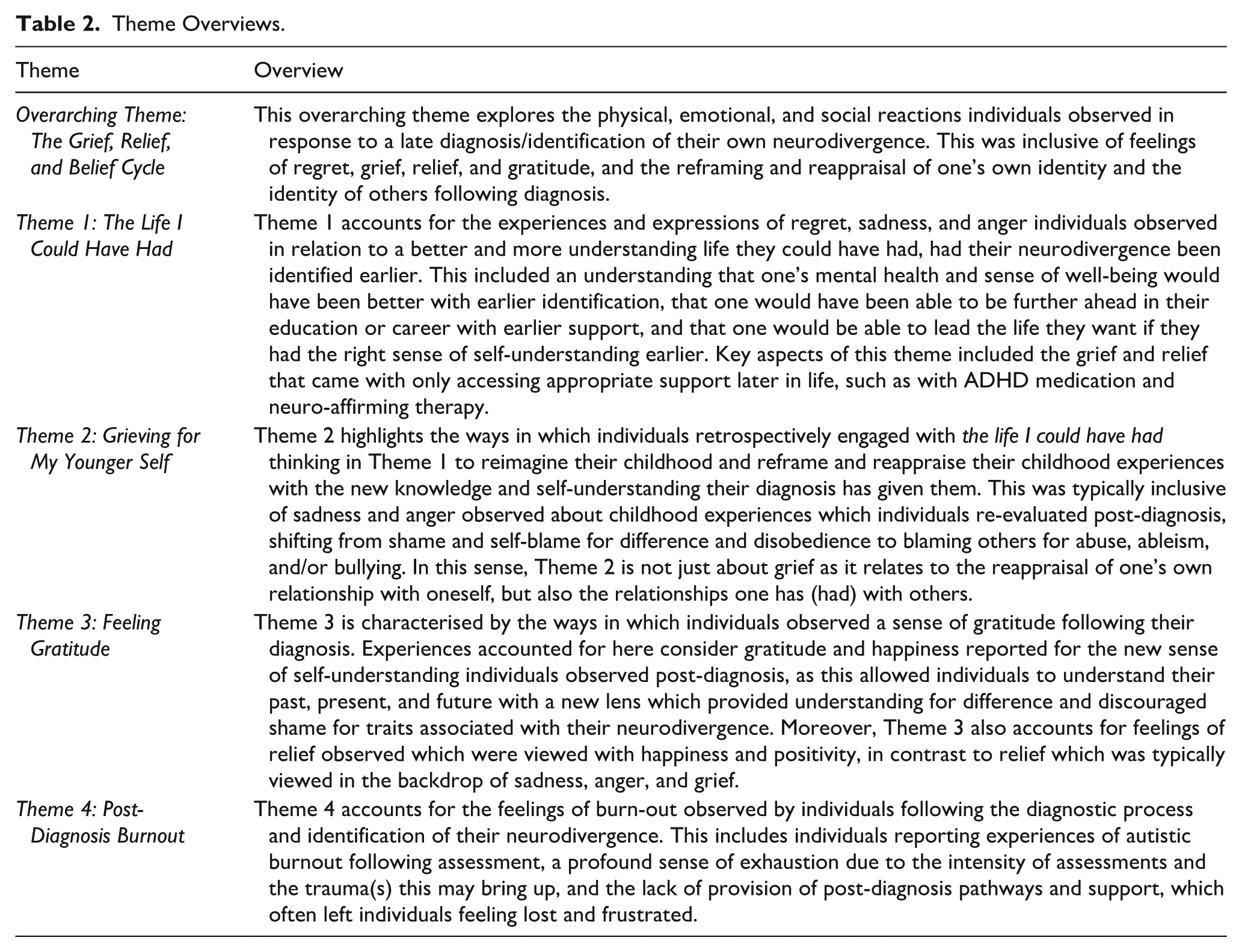
Four main themes under an overarching theme, titled the Grief, Relief, and Belief Cycle, were identified: (1) The Life I Could Have Had (n = 221), (2) Grieving for My Younger Self (n = 216), (3) Feeling Gratitude (n = 66), and (4) Post-Diagnosis Burnout (n = 188) (Table 2).
Theme Overviews.
The sample is representative of a broad range of neurodivergences, though mainly comprised of autistic individuals (n = 130), those with ADHD (n = 119), and those with both co-occurring (n = 46). The term neurodivergent was also used by several posts (n = 48), as well as different modes of describing different autistic profiles, like Asperger’s/Aspie (n = 16) and pathological demand avoidance (n = 6). A minority of posts identified with other forms of neurodivergence: communication disorder (n = 6), developmental co-ordination disorder (n = 6), Tourette syndrome (n = 3), and specific learning disorders (n = 16) (for more detailed results, see Supplementary Material 4).
Overarching Theme: Grief, Relief, and Belief Cycle
The overarching theme explores physical, emotional, and social reactions observed in response to late identification, which formed an oscillating cycle of grief, relief, and (self-)belief (Figure 3).
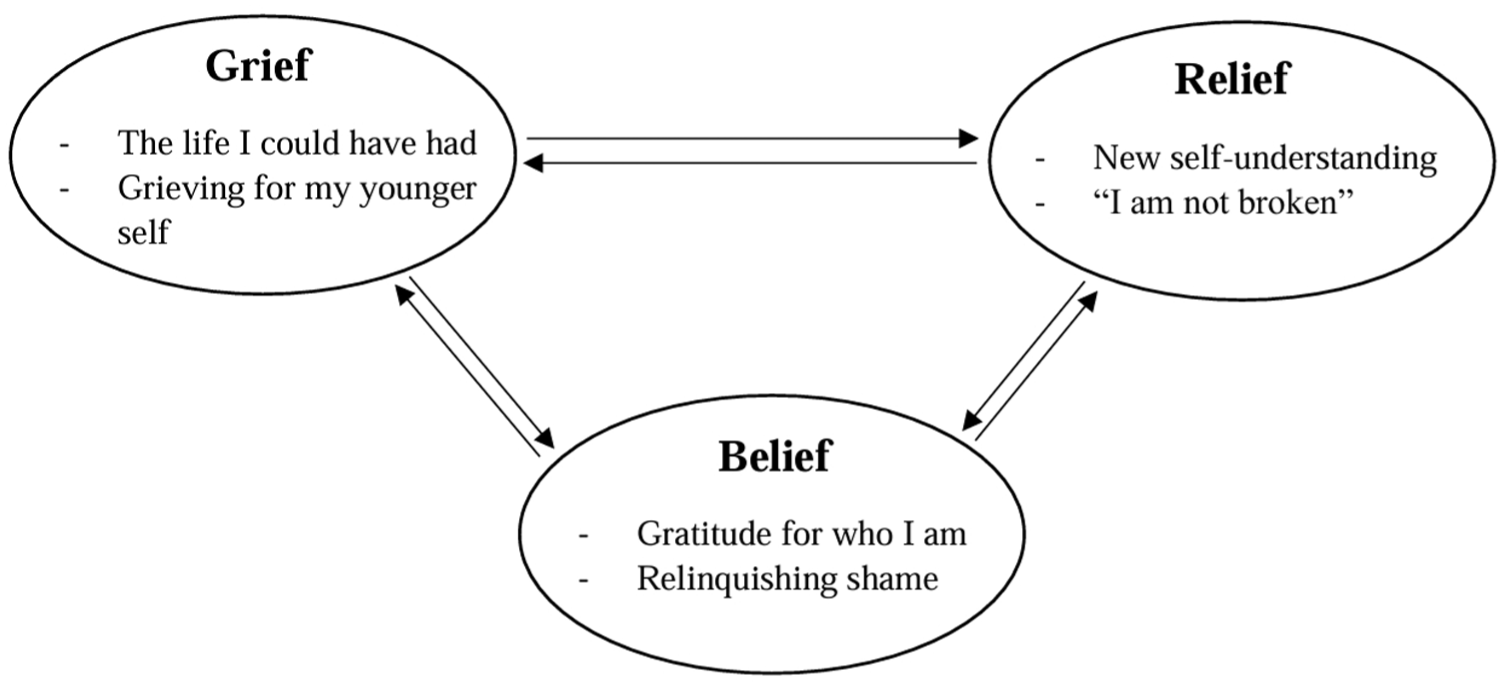
The Grief, Relief, and Belief Cycle.
This was inclusive of a range of feelings identified across themes, which were typically centred on distressing emotions related to grief, as well as positive experiences of gratitude and relief in response to the diagnosis running in contradistinction to the grief observed: [Following late diagnosis] we often go into a phase of anger, questioning, and even grief, that lives side by side the joy and relief that we feel. (Matthew)
Moreover, reappraisals of one’s own relationship with oneself and their relationships with others were observed in a Grief, Relief, and Belief Cycle identified following a diagnosis: It’s like a grief and relief response . . . many of us are over the age of 18 [when diagnosed], so we have a lot of grief for the fact that we went through our entire educational career with little to no supports, but also relief that we now understand that we are not . . . whatever label some horrible teacher tried to put on us. (Halliwell)
Overall, this overarching theme identifies a grief and relief cycle which was observed across posts and ties together the main themes by means of reframing and reappraising one’s sense of self, relation to others, and perception of life before, during, and after diagnosis.
Theme 1: The Life I Could Have Had
Theme 1 accounts for the experiences and expressions of regret, sadness, and anger individuals observed in relation to a better/more understanding life they perceive they could have had, had their neurodivergence been identified earlier. This included an understanding that one’s mental health and sense of well-being would have been better with earlier identification. Posts also identified a perception that individuals believed that they would have been able to be further ahead in their education and/or career with earlier formal support for their neurodivergence(s): I had no friends, higher qualifications or career prospects and was housebound with crippling anxiety. How could I view my brain wiring positively . . .? (BA)
It is important to note that a general sense of grief due to disability was also noted for the life one could have had without disability. Moreover, despite the desire for earlier identification, several posts admitted that they could not actually know if this would have made their life better. Posts also observed the notion of an inauthentic life prior to identification, due to a combination of social factors, such as masking, ableism, and feeling/being misunderstood. Individuals highlighted that they felt they would have been able to lead a life they, “wanted to lead” had they had the right sense of self-understanding and appropriate support earlier: [With the right support/medication] the realisation sets in that you were never lazy, that you’d forced yourself to live a lie and lost so much time, so much of the person you could have been, and that is real grief. (210mgs)
Aspects of self-understanding included an understanding of why one felt different from their peers and engaged in particular behaviours (e.g. stimming and echolalia), as well as understanding why previous therapeutic interventions had not been of benefit, as these were not mindful of key difficulties particular neurodivergences may raise for engagement with and understanding of the intervention: I had the realisation that I spent a lot of my life thinking I was depressed or sad and not understanding why, and it was that I was over-stimulated, and I didn’t understand what that meant. (Rys)
Finally, key aspects of this theme included the grief and relief that came with only accessing appropriate support later in life, such as with ADHD medication and neuro-affirming therapy. Overall, Theme 1 highlights a range of reactions to diagnosis which were typically future and present focused insofar as they centred on where individuals felt they “should” be with their lives, and what they think they “should” be able to do and “could” have been able to achieve with appropriate support and understanding. However, it is important to note that these perspectives were typically predicated on thoughts of their younger self, as posts observed grieving for what they perceived they lost in their youth due to not being diagnosed.
Theme 2: Grieving for My Younger Self
Theme 2 is characterised by the ways in which individuals retrospectively engaged with the life I could have had thinking in Theme 1: I felt so sad for me as a child. That lonely little girl that wanted to be part of life . . . What could I have achieved if the odds weren’t stacked-up against me? (Sam)
This retrospective thinking was typically observed as a reimagination of childhood centred on a reframing and reappraisal of specific experiences, generally centred on school, family life, teenage mental health, and social relationships. These reappraisals of the past were marked by grief for one’s younger self in terms of loss of opportunity, social relationships, health, and sense of self, and were (in)formed by new knowledge and (self-)understanding that the identification of one’s neurodivergence was observed to provide: Coming out of denial involves both grief and relief. I’m relieved to know I’m not alone; however, I’m grieved I felt alone for so long. (AACW)
Affective reactions to these reappraisals were typically focused on sadness and anger observed about childhood experiences which individuals re-evaluated post-diagnosis, shifting from shame and self-blame for difference and disobedience to blaming others for abuse, ableism, bullying, and/or misunderstanding. In this sense, Theme 2 is not just about grief as it relates to reappraisal(s) of one’s own relationship with oneself, but also the relationships one has (had) with others: When I was first diagnosed, I felt vindicated. I wanted to yell ‘See? I wasn’t faking!’ into my parents faces. (ZP)
Overall, Theme 2 highlights a past-/present-focused re-evaluation of oneself and one’s own experiences and social relationships insofar as posts observed the present knowledge and self-understanding afforded by the diagnosis to offer a new lens through which to view and understand their childhood. It is important to note that although past experiences were typically reframed in a negative light, the knowledge afforded by the diagnosis was welcomed in a present sense and often met with more positive feelings in among the grief.
Theme 3: Feeling Gratitude
Theme 3 is characterised by the ways individuals observed a sense of gratitude following their diagnosis, with happiness reported for the new sense of self-understanding individuals reported post-diagnosis: When I finally got a diagnosis that made sense. I bawled. Not because I was sad. But because I could finally heal. (Power)
This new sense of self-understanding afforded by the diagnosis was observed as a tool for individuals to understand their past, present, and future: There was before my diagnosis. The imposter syndrome, grief and denial during my diagnosis. And after [my diagnosis] I accepted and embraced it. (Sue)
Although posts observed feeling shame and embarrassment for traits associated with their neurodivergence prior to their diagnosis, this new lens to view these traits afforded by the diagnostic label was identified to provide understanding for difference while discouraging shame for traits associated with their neurodivergence. This understanding which countered shame also accounts for feelings of relief observed which were viewed with happiness and positivity, in contrast to relief which was typically viewed in the backdrop of sadness, anger, and grief, as identified in other themes: Superheroes, we see their powers first, and their challenges after. And we empathise with their struggles as they embrace their powers . . . I want others to see their assets first too. So that they can embrace their superpowers to not only survive and better manage their diagnoses but to thrive and succeed because of them, not despite them. (Blady)
Overall, Theme 3 highlights a present/past-focused reappraisal following diagnosis which was typically centred on gratitude and compassion. This ultimately helped to foster a new sense of self-understanding and identity which sought to relinquish shame for characteristics related to one’s neurodivergence and was a moment of positivity, often framed as relief, following a diagnosis. However, the post-diagnosis period was not just considered in terms of relief, rather these positive re-evaluations of the past/present were typically framed as exhausting experiences which led to a sense of burnout.
Theme 4: Post-Diagnosis Burnout
Theme 4 accounts for the feelings of burnout observed by individuals following the diagnostic process and identification of their neurodivergence. This includes individuals reporting experiences specifically of autistic burnout following assessment, as well as a more general sense of burnout and grief which was observed in relation to the intensity of the diagnostic process. This intensity was typically framed in terms of its social demands and the taxing and tiring nature of family involvement in assessment pathways too. Moreover, some posts observed exhaustion as the result of discussing emotive events and trauma(s) from their past during assessment: When you are 30, 40, 50 years old, and you realise you are neurodivergent, there is so much to unpack, and looking back on all of the memories and all of the trauma is really hard, and you grieve. (Lindsey)
Finally, the lack of provision of post-diagnosis pathways and support were identified as significant gaps in wrap-around support, which often left individuals feeling lost, frustrated, and angry: How would autistic people fare if we were all given the option to undergo counselling post-diagnosis? If we were given space to voice our traumas, to come to terms with our lives and develop the thinking skills & coping strategies needed to forge a positive future? (BA)
Discussion
The analysis indicates that late identification can be met with grief, as the posts identified grieving for the life that they “could have had,” as well as grieving for their younger self and associated loss of identity. However, it is important to note that this study was specifically looking at experiences of grief and there may exist a multitude of non-grief related responses to late identification which were not identified through the methods employed in this study. Nevertheless, it is important to note that, when other reactions to late identification were noted, grief remained central to these experiences; for example, although most posts discussed a grief and relief cycle, they typically solely focused on the grief aspect. This cycle aligns with current phenomenological research on late identification of neurodivergence (Leedham et al., 2020; Young et al., 2008; Zener, 2019), which highlights grief and joy in one’s own journey to accepting their neurodivergence. The grief individuals observe also aligns with parent-focused research, which discusses a perceived sense of ambiguous loss when a child is identified as autistic (Bravo-Benítez et al., 2019; Fernańdez-Alcántara et al., 2016).
Theme 1 highlights the profound sense of loss and regret observed by neurodivergent individuals who received their diagnosis in adulthood. Thus, Theme 1 centres on a common narrative of missed opportunities and the perception of a life that might have been significantly improved upon with earlier identification, support, and understanding. This aligns with existing literature that documents the benefits of earlier identification and support in improving social (Beresford & Mukherjee, 2024; Corden et al., 2021; Gabbay-Dizdar et al., 2022), academic (Asherson et al., 2012; Battistutta et al., 2018), and mental health outcomes (Leedham et al., 2020; Lupindo et al., 2023; Stagg & Belcher, 2019). Moreover, it also supports the growing body of literature which observes the sense of regret late identified neurodivergent individuals have for a life they perceived would have been better had they received earlier diagnosis, (self-)understanding, and support (Beresford & Mukherjee, 2024; Nayyar et al., 2024; Young et al., 2008). However, it is crucial to acknowledge the complexity and variability of individual experience(s), as several posts did identify that there is no certainty that an earlier diagnosis would universally lead to better outcomes, and acknowledge the increased social stigma (Huang et al., 2020; Nayyar et al., 2024), potential family difficulties (Crane et al., 2016; Fernańdez-Alcántara et al., 2016), and social and legal vulnerability an early diagnosis can bring, and the associated traumas and losses linked to this. This includes increased rates of parental divorce when parents do not develop adaptive coping strategies and/or have access to appropriate support for their neurodivergent child(ren) (Anchesi et al., 2023; S. L. Hartley et al., 2010). Overall, this uncertainty indicates the need for more personalised approaches to diagnostic pathways and post-diagnosis support (Rutherford et al., 2023).
Theme 2 indicates a retrospective grief and reappraisal of past experiences through the new lens of their neurodivergence. This re-evaluation was often observed in a process which shifts from self-blame to recognising external factors, such as stigma, bullying, and ableism, have informed many significant life experiences. This is consistent with the current literature which suggests that neurodivergent children experience increased levels of stigma (Aubé et al., 2021; Mazumder & Thompson-Hodgetts, 2019), involvement with bullying as victim and/or perpetrator (Chou et al., 2018; Maïano et al., 2016), negative comments from adults (Furukawa et al., 2017; Musser et al., 2016), and risk of adverse childhood experiences (G. Hartley et al., 2024; Lugo-Candelas et al., 2021) than their neurotypical peers. The emotional weight of this re-evaluation of past experiences through this new lens fits with a grief-orientated re-evaluation of the self, which is documented in adult diagnoses of disabilities (Bertrand, 2021; Clifton, 2014). This also lends to the need for trauma-informed diagnostic pathways, post-diagnostic support, and distinct neuro-affirming post-diagnosis therapeutic interventions to address past traumas and foster self-compassion (Beresford & Mukherjee, 2024; Chapman & Botha, 2023; Corden et al., 2021; Rutherford et al., 2023).
Theme 3 centres on a sense of relief and gratitude for the self-understanding that comes with their diagnosis. This positive reappraisal is crucial in highlighting the merit of late identification, as, despite the challenges it raises, the diagnosis itself serves as a pivotal and defining moment of self-understanding and acceptance (Corden et al., 2021; Crane et al., 2016; Leedham et al., 2020). The transformative shift from shame and self-blame to gratitude, self-compassion, and self-acceptance corresponds with the emerging literature on late identification, which highlights that late identification of neurodivergence is often met with joy and relief (Huang et al., 2020; Nayyar et al., 2024; Young et al., 2008). This also provides a framework for compassionate self-understanding (Corden et al., 2021; de Bree et al., 2022) and the necessary vocabulary to understand who they are, the challenges they face, and how to better navigate these (Leedham et al., 2020; Lupindo et al., 2023; Stagg & Belcher, 2019). These findings also align with post-traumatic growth theories, where individuals experience positive psychological change following highly stressful events (Tedeschi & Calhoun, 2004), and the link between grief, relief, and belief is suggestive of a more specific post-grief growth (PGG) phenomena, where grieving individuals experience positive psychosocial change in response to their grief. This PGG understanding has been identified in different areas of grief research, such as in growing around grief (Tonkin, 1996), the grief to personal growth model (Hogan & Schmidt, 2002), and the use of a post-traumatic growth framework to develop an understanding of post-bereavement growth (Calhoun et al., 2010). However, the associated sense of burnout also observed, suggests that PGG in this context is an exhausting process, which indicates the need for comprehensive wrap-around support built into diagnostic pathways (Beresford & Mukherjee, 2024; Rutherford et al., 2023).
Theme 4 emphasises the intense emotional and physical toll of the diagnostic process and a subsequent lack of support, as highlighted in emerging literature on late identification (Huang et al., 2020; Nayyar et al., 2024; Young et al., 2008). However, despite long-standing awareness of the taxing nature of neurodevelopmental diagnostic pathways for children and their primary caregivers (Bravo-Benítez et al., 2019; Crane et al., 2016), and an increasing awareness of the taxing nature of these diagnostic pathways for adults (Lockwood Estrin et al., 2021; Stagg & Belcher, 2019; Zener, 2019), the findings still reflect a significant gap in healthcare post-diagnosis. This indicates a need for increased wrap-around support offered and an understanding that diagnosis provision should not be regarded as an endpoint in of itself, rather it should be viewed with greater continuity of care (Beresford & Mukherjee, 2024). Furthermore, burnout in the context of late identification is observed in line with established conceptualisations of autistic burnout (Raymaker et al., 2020), in terms of experiences of profound exhaustion, loss of skills, and increased sensitivity to stimulus in response to life stressors, cumulative load, and barriers to support. Experiences of burnout were typically identified as being exacerbated by the social, familial, practical, and clinical demands of the diagnostic process and recounting past traumas, which are key points of difficulty and stress identified across the late identification literature for both autism and ADHD (Leedham et al., 2020; Nayyar et al., 2024; Young et al., 2008). Therefore, addressing this gap would require the development of comprehensive and compassionate post-diagnosis pathways which are, “relevant, proportional, and individualised” (Rutherford et al., 2023), involving both health and social care and practical resources (Beresford & Mukherjee, 2024; Rutherford et al., 2023).
The results of this study offer a comprehensive view of the psychosocial grief experienced by neurodivergent individuals (specifically those who are autistic, have ADHD, or both) following a late identification and highlight the complex process of the Grief, Relief, and Belief Cycle. This cycle forms a dynamic process that evolves as individuals come to terms with their diagnosis and builds an understanding of PGG which furthers current research of late neurodivergent identification, which addresses reactions involving grief and relief (Leedham et al., 2020; Nayyar et al., 2024; Young et al., 2008) but has not yet presented a non-linear, evolving, and individual process through which this may be understood. It is important to note that although this study also considers PGG aspects of (self-)belief, the Grief & Relief Cycle of late identification is a concept already identified in the language used within the posts analysed in this study. As such, using the Grief, Relief, and Belief Cycle to frame the ways in which neurodivergent individuals may process and integrate a diagnosis into their sense of self, is a framework that remains true to neurodivergent individuals’ own language, discourse, and understanding(s). As such, in (re)presenting this framework, the authors seek to value the epistemic agency and epistemological contributions of online neurodivergent communities in developing and conceptualising the Grief & Relief Cycle of Late Identification. Overall, the authors acknowledge that the study (re)presents terminology used for describing experiences of late identification already used within online neurodivergent communities themselves, as identified in the analysis. This article, therefore, makes no claim to coining the term or originating its conceptualisation; rather, this article has provided a comprehensive overview of grief in relation to late identification and (re)presents a community-produced framework as to how this may be conceptualised as a Grief, Relief, and Belief Cycle.
The psychosocial processes identified, which (in)form this cycle, can be viewed in an oscillating nature, which appears to align with the dual process model of coping with grief (Stroebe & Schut, 2010), as this model centres on oscillations between loss-oriented and restoration-oriented modes of coping following a loss, which in this case is in reference to loss and reappraisal of one’s own sense of self and their relationships with others (Fiore, 2021; Stroebe & Schut, 2010). Moreover, the framing of this cycle in terms of PGG is crucial, as it acknowledges the grief, traumas, difficulties, and stressors involved in receiving and, consequently, reframing one’s own self-understanding following a diagnosis, as is identified in neurodevelopmental (Leedham et al., 2020; Nayyar et al., 2024) and broader disability (Bertrand, 2021; Clifton, 2014) research, but also highlights the potentiality for growth and compassion that this new found self-understanding and lens to view one’s life with serves (Chapman & Botha, 2023; Corden et al., 2021; Stagg & Belcher, 2019).
This cycle also echoes similar narratives of identity formation and sense of self discussed in the broader literature of on disclosure, identity integration, and self-refiguration, which conceptualise identity as narratively constituted, relational, and continually reinterpreted across the life course (Butler, 2006; Goffman, 1990; McAdams, 1997). For example, within queer studies, early models of coming out employed linear frameworks of disclosure and acceptance (e.g. Cass, 1979; Troiden, 1989); however, critiques of and developments of this understanding emphasise the ongoing, context-dependent, and the non-linear nature of coming out, thus highlighting the limitations of linear teleological framings of identity negotiation (McDonald, 1982; Newman & Muzzonigro, 1993). As such, the oscillatory nature of the psychosocial processes identified in this study resonate with these more nuanced coming out narratives, which view the gradual acceptance and integration of an identity in terms of a continually negotiated process of meaning-making, disclosure, concealment, and integration across the life course, rather than a singular event or linear process.
These processes may also be situated within broader theoretical accounts of identity formation, which conceptualise the self as being dynamically (re)produced through discourse, reflexivity, and social practice (Butler, 2006; Foucault, 1991). From a Foucauldian perspective, late identification can be understood as a process of subjectivation, whereby individuals come to know and (re)constitute themselves, and be known and (re)constituted by others, as particular kinds of subjects through historically and culturally situated discourses of neurodivergence and neuronormativity (Foucault, 1982, 1988a). This involves the use of categorical language and forms of reflexive self-work (i.e. technologies of the self), through which individuals (re)interpret past experiences, (re)negotiate disclosure, and (re)integrate new understandings of their sense of self across social contexts (Foucault, 1988b). Ultimately, such processes resonate with narrative and psychosocial theories that conceptualise identity as continually (re)authored and (re)produced across the life course, particularly following moments of disruption or re-interpretation (Butler, 2006; McAdams, 1997). Overall, this understanding aligns with the current literature on late identification, which emphasises complex and continual re-evaluations of sense of self following late identification of one’s neurodivergence (Leedham et al., 2020; Nayyar et al., 2024; Young et al., 2008), as well as the dynamic, non-linear process(es) of (re)appraisal, (re)interpretation, gradual acceptance associated with PGG, and integration conceptualised in the Grief, Relief, and Belief Cycle presented in this study.
Strengths and Limitations
Due to the specific data set through which these posts were identified and analysed, this study only explored the reactions to late identification of those who observed experiences of grief. As such, findings are not representative of those who do not experience grief in response to late identification. It is important to note, that given the role of stigma in the Grief, Relief, and Belief Cycle, variations in grief reactions or lack thereof may be associated with different cultural understandings of neurodivergence and neurodiversity, prior self-identification, and/or the type, availability, and attitudes of social support systems (Chapman et al., 2022; Nayyar et al., 2024; Rutherford et al., 2023). As such, although a key strength of this study is its nuanced exploration of a particular aspect of neurodivergent individuals’ reactions to late identification, this study calls for further research which explores these experiences more broadly.
Moreover, while most posts account for lived experience(s) in terms of autistic individuals, people with ADHD, and those with both co-occurring, only a small minority of posts considered other forms of neurodivergence. Although this is likely to be due to specific presentations of different neurodevelopmental profiles in the data set, which were typically representative of those with lower support needs who are speaking, and other more outwardly discernible forms of neurodivergence tending to be exclusively identified in childhood/adolescence, such as intellectual disabilities and Tourette syndrome (APA, 2022; WHO, 2019). As such, this study is limited in scope in terms of experiences of late identification of neurodivergence it may account for, with the main focus being on autism and ADHD. Moreover, with dual-diagnosis of autism and ADHD only clinically being considered from 2013 onwards (APA, 2013, 2022), it is unclear if experiences of late identification in those with a dual-diagnosis was influenced by this, either as the reporting on their late identification centring on one of these or their late identification stemming from a more complex neurodevelopmental profile where features from each masked features from the other and only became apparent in adulthood as social demands exceeded ability to mask (APA, 2022; Hartman et al., 2016; Rau et al., 2020). However, given that the majority of individuals with one form of neurodivergence will have another co-occurring (Francés et al., 2022), it is important to note that even when those posting only explicitly identified with one form of neurodivergence, it is likely that another form of neurodivergence will also inform their lived experiences (APA, 2022; Francés et al., 2022; WHO, 2019). Therefore, despite being limited in scope, the broad transdiagnostic intentionality of this study is a key strength, as it provides an understanding of late identification, while being mindful of individual differences which (in)form these lived experiences.
Clinical Implications & Future Research
The sample accessed in this study is typically reflective of the reactions of individuals who received a diagnosis, as such this research is limited in scope in terms of understanding the experiences of those who were not given a diagnosis, were (mis)diagnosed, or were unable to access assessment in the first place. This is important to note, as diagnosis was often observed in terms of reframing feelings of self-blame in relation to difference into an understanding that others had unfairly treated the individual for traits they cannot help. This is tentatively suggestive that being unable to access a diagnosis through inaccessible services may ultimately compound feelings of shame and self-blame. Therefore, this study calls for future research that accounts for the experiences of those who were misdiagnosed and/or unable to access assessment pathways. Overall, this study calls for a paradigm shift in how we understand and support neurodivergent individuals, seeing diagnosis as a first step, rather than a terminal component of a service, emphasising the need for comprehensive, individualised, wrap-around care that addresses both the emotional and practical aspects of their lives before, during, and beyond diagnosis.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261437916 – Supplemental material for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence
Supplemental material, sj-docx-1-aut-10.1177_13623613261437916 for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence by Ally Pax Arcari Mair, Marina Gonzalez-Figueroa, Doug McConachie, Karen Goodall and Karri Gillespie-Smith in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613261437916 – Supplemental material for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence
Supplemental material, sj-docx-2-aut-10.1177_13623613261437916 for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence by Ally Pax Arcari Mair, Marina Gonzalez-Figueroa, Doug McConachie, Karen Goodall and Karri Gillespie-Smith in Autism
Supplemental Material
sj-docx-3-aut-10.1177_13623613261437916 – Supplemental material for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence
Supplemental material, sj-docx-3-aut-10.1177_13623613261437916 for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence by Ally Pax Arcari Mair, Marina Gonzalez-Figueroa, Doug McConachie, Karen Goodall and Karri Gillespie-Smith in Autism
Supplemental Material
sj-docx-4-aut-10.1177_13623613261437916 – Supplemental material for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence
Supplemental material, sj-docx-4-aut-10.1177_13623613261437916 for Grief, Relief, and Belief: A Social Media Study on Late Identification of Neurodivergence by Ally Pax Arcari Mair, Marina Gonzalez-Figueroa, Doug McConachie, Karen Goodall and Karri Gillespie-Smith in Autism
Footnotes
Ethical Considerations
This study was granted favourable ethical approval by the School of Health in Social Science Ethics Committee at the University of Edinburgh and an ethical framework based on UK government and the British Psychological Society guidance on social media research was employed.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was carried out as part of a PhD funded by the University of Edinburgh’s College Research Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.