
Abstract
Previous research has suggested potential phenotypic similarities between autism and borderline personality disorder (BPD). We aimed to identify overlapping and differentiating characteristics of the two diagnostic groups in women and people assigned female at birth (PAFAB). Women and PAFAB with an autism diagnosis (n = 51) or a BPD diagnosis (n = 51), who had few or subclinical traits of the comparator diagnosis, completed a range of self-report questionnaires. Emotional reactivity, emotional dysregulation, identity disruption, difficulties being alone and rejection sensitivity were significantly more characteristic of BPD-diagnosed participants, with identity disruption representing the biggest difference from autistic participants (d = −1.36, 95% confidence interval [CI] = [−1.79, −0.92]). Autistic participants scored significantly more highly on measures of sensory processing, social cognition and behaviour, preference for sameness and repetitive motor behaviour, with sensory processing representing the biggest difference from BPD-diagnosed participants (d = 1.19, 95% CI = [0.76, 1.60]). Group differences in social cognition, social camouflaging, identity disruption, impulsivity and coping with being alone, together correctly classified 95.1% of participants (area under the curve [AUC] = 0.98). However, comparison with measure scores in previous research suggests more complex phenotypic similarities, whereby autistic individuals may show more BPD-aligned characteristics than the general population and vice versa.
Lay Abstract
Autism can look similar to borderline personality disorder (BPD), leading to misdiagnosis. For example, both diagnostic groups may experience difficulties in regulating their emotions. To improve diagnosis, we wanted to understand similarities and differences between autism and BPD in adult women and people assigned female at birth (PAFAB). We asked two groups of people to complete online questionnaires: (1) 51 women/PAFAB with an autism diagnosis, who do not meet diagnostic criteria for BPD and (2) 51 women/PAFAB diagnosed with and meeting diagnostic criteria for BPD, who are not autistic. The questionnaires asked participants how they experience their emotions, how they interact and relate with other people, how they experience their identity and self-concept, how they react to sensory input, for example, sounds and smells, and how they use repetitive movements, as well as their preferences for sticking to familiar ways of doing things. We found more differences than we expected between autistic people and people meeting diagnostic criteria for BPD. For example, autistic people described being more sensitive to sensory input, described ‘masking’ more during social interactions and described more challenges in understanding the social behaviour of non-autistic people, compared to people meeting diagnostic criteria for BPD. People meeting diagnostic criteria for BPD described more difficulties with emotion regulation and with their sense of self (‘knowing who I am’), were more likely to behave impulsively and found being on their own more difficult, compared to autistic people. Clinicians, and people with a BPD diagnosis who think they may be autistic, can use these findings to better understand the differences between the two diagnoses. Even though we found lots of differences, it is still likely that autistic people experience more similarities with BPD than non-autistic people do and vice versa.
Keywords
Introduction
Borderline personality disorder (BPD) is one of the most frequent diagnoses given prior to adult autism diagnosis and is the most commonly perceived misdiagnosis reported by autistic people (Kentrou et al., 2024). Recognising critical stances on this diagnostic construct (Watts, 2024), we refer throughout to people diagnosed with or meeting diagnostic criteria for BPD, rather than to people ‘with’ or ‘having’ BPD. Missed autism may be particularly prevalent among BPD-diagnosed women and people assigned female at birth (PAFAB), since there are known sex differences and biases resulting in underdiagnosis of autism and overdiagnosis of BPD (Braamhorst et al., 2015; Lai & Baron-Cohen, 2015).
Clinicians say that shared characteristics of autism and BPD may contribute to misdiagnosis, including emotional dysregulation, alexithymia and identity disruption (Aves, 2022; Cumin et al., 2022; Gordon et al., 2020; Lai & Baron-Cohen, 2015; McQuaid, Strang, & Jack, 2024; Sarr et al., 2025). Research conducted separately in each diagnostic group suggests both groups experience higher levels of these characteristics than the general population do (Carpenter & Trull, 2013; Hull et al., 2017; Kinnaird et al., 2019; McQuaid, Strang, & Jack, 2024; New et al., 2012; Ritzl et al., 2018; Roberts et al., 2015; Samson et al., 2014; Weiner et al., 2023; Weiss et al., 2014). Emotional dysregulation and identity disruption are core diagnostic criteria for BPD. By contrast, emotional overwhelm in autistic people may relate primarily to the distressing effects of sensory overload, social demands and managing unpredictability, while identity disruption may result from social camouflaging of autistic characteristics (McQuaid, Strang, & Jack, 2024). Heightened trauma exposure among autistic people is also a complicating factor (Cazalis et al., 2022; Cumin et al., 2022), since trauma is strongly associated with developing the coping strategies and internal experiences characteristic of BPD (Porter et al., 2020). A few studies directly comparing autism and BPD diagnostic groups have found similarities in aspects of social, emotional and cognitive functioning (Dudas et al., 2017; Duijkers et al., 2014; Insua-Summerhays, 2021; López-Pérez et al., 2017). These findings add to the contention that autism and BPD may be phenotypically similar.
However, existing studies did not assess key domains potentially important for differential diagnosis, such as sensory processing or rejection sensitivity. Furthermore, they did not screen BPD-diagnosed participants to check whether any had undiagnosed autism, nor whether their autistic participants had significant features of BPD, likely increasing the apparent similarities between the diagnostic groups. To better establish any phenotypic similarities and differences, it is important to exclude individuals in each diagnostic group who are likely to meet full diagnostic criteria for the other diagnosis, while also allowing inclusion of individuals with some subclinical traits of the other diagnosis, given the overlap identified in previous studies (Dudas et al., 2017).
Aims and Hypotheses
We aimed to identify overlapping and differentiating clinical features, characteristic of autistic women/PAFAB and women/PAFAB meeting diagnostic criteria for BPD in people with few or subclinical traits of the other diagnosis.
We hypothesised that:
Differences relating to sensory processing, social camouflaging, social cognition, social awareness, social communication, social avoidance, need for time alone, repetitive motor behaviour and preference for sameness will be more characteristic of autistic people than of people who meet diagnostic criteria for BPD. These hypotheses were based on these characteristics being diagnostic criteria for autism, not previously shown to be characteristic of people meeting diagnostic criteria for BPD, and identified by clinicians and/or our lived experience advisory panel as potentially differentiating autism from BPD (Cumin et al., 2022; Gordon et al., 2020; Sarr et al., 2025).
Distress and difficulty coping when alone, and rejection sensitivity, will be more characteristic of people meeting diagnostic criteria for BPD than of autistic people (Cumin et al., 2022; Gordon et al., 2020; Sarr et al., 2025). These hypotheses were based on these characteristics being closely related to a diagnostic criterion for BPD (fear of abandonment), not previously shown to be characteristic of autistic people, and identified by clinicians as core to understanding the attachment-related difficulties that may underlie BPD and potentially differentiate BPD from autism (Cumin et al., 2022; Gordon et al., 2020; Sarr et al., 2025).
Emotional reactivity, emotional dysregulation, alexithymia, identity disruption and experiences of childhood trauma will not differentiate between diagnostic groups. These hypotheses were based on these characteristics being identified by clinicians, by our lived experience advisory panel and by previous empirical studies as being characteristic of both autistic and BPD-diagnosed people (Carpenter & Trull, 2013; Cazalis et al., 2022; Hull et al., 2017; Kinnaird et al., 2019; Lai & Baron-Cohen, 2015; McQuaid, Strang, & Jack, 2024; New et al., 2012; Porter et al., 2020; Ritzl et al., 2018; Roberts et al., 2015; Samson et al., 2014; Weiner et al., 2023; Weiss et al., 2014).
Other potential areas of difference, such as intense interests and differences in non-verbal communication (autism), emptiness, idealisation and devaluation, and dissociation (BPD), have been less well discussed in extant literature and were not evaluated in this study.
Method
Design
This was a cross-sectional survey using self-report questionnaires to compare the clinical features of autistic participants and participants meeting diagnostic criteria for BPD, with screening measures used to eliminate undiagnosed comorbidity between the diagnostic groups while including individuals with few or subclinical traits of the other diagnosis.
Participatory Methods
The study was co-led by an autistic researcher with experience of BPD diagnosis and co-designed with another autistic researcher. They co-designed the research question, study design, measure selection, recruitment, data collection, analysis, interpretation and dissemination of the findings. A panel of people with lived experience of autism and/or BPD diagnosis, and a panel of mental health clinicians, advised on all aspects of study design and methodology. All autistic people involved in project co-design were women or people assigned female at birth.
Positionality
Two of the study authors are autistic researchers with experience of BPD diagnosis. Their experiences informed the study team’s neurodiversity-affirming approach to autistic traits and critical stance regarding the BPD diagnostic construct.
Inclusion Criteria
All inclusion and exclusion criteria were assessed by participant self-report.
All participants were as follows:
Aged ≥ 18 years.
Assigned female at birth (AFAB) or identifying as a woman. This included any AFAB people regardless of their gender identity (e.g. non-binary individuals and trans males were included as well as cisgender females), and anyone currently identifying as a woman, regardless of their sex assigned at birth (e.g. people assigned male at birth [AMAB] were included if they identified as a woman). We included these groups because cisgender women and gender-diverse individuals are diagnosed with autism later in life, are more likely to receive psychiatric diagnoses prior to autism diagnosis and are more likely to be diagnosed with BPD than cisgender men (Abu-Ramadan et al., 2025; Braamhorst et al., 2015; Graham-Holmes et al., 2026; Kentrou et al., 2021; McQuaid, Ratto, et al., 2024; Posserud et al., 2021; Rodriguez-Seijas et al., 2024; Zimmerman et al., 2022). Consequently, these are the groups for whom difficulties in differential diagnosis of autism and BPD are likely to be most prevalent. Cisgender men were excluded because sex differences in the socio-communicative and repetitive motor behaviour domains of autism mean that findings from cisgender autistic men may not generalise to cisgender autistic women or gender-diverse groups (Wilson et al., 2016).
Currently resident in the United Kingdom.
Autistic participants (Group 1) were additionally required to meet the following criteria:
Current diagnosis of an autism spectrum disorder.
Has never been diagnosed with a personality disorder.
Unlikely to meet full diagnostic criteria for BPD as indicated by a score below 7 on the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD). Each of the 10 items on this measure corresponds to one of the 10 diagnostic criteria for BPD, of which 5 are needed to make a diagnosis. A cut-off score of 7 thus allowed for autistic individuals in our study to experience subclinical BPD characteristics while providing the best combination of sensitivity (0.81) and specificity (0.85) for distinguishing psychiatric patients who do versus do not meet full diagnostic criteria for BPD (Zanarini et al., 2003).
Participants meeting diagnostic criteria for BPD (Group 2) were required to meet the following criteria:
Current diagnosis of BPD.
A score of 4 or above on the MSI-BPD (Zanarini et al., 2003). This cut-off score was chosen to optimise sensitivity (0.98) at the expense of specificity (0.32) (Zanarini et al., 2003), as it is known that endorsement of BPD criteria can fluctuate over time (Zanarini et al., 2007).
Has never been diagnosed with an autism spectrum disorder, does not believe themselves to be autistic or possibly autistic and is not referred for an autism assessment.
Unlikely to meet full diagnostic criteria for autism as indicated by scoring <23 on the Ritvo Autism and Asperger Diagnostic Scale-Revised (RAADS-14) (Eriksson et al., 2013) and/or <6 on the Autism Spectrum Quotient-10 (AQ-10) (Allison et al., 2012). To enable participation of individuals with subclinical autistic traits, we used a high cut-off for the RAADS-14 (14 is recommended as the usual cut-off, whereas 23 may offer a better combination of sensitivity and specificity in psychiatric populations, Eriksson et al., 2013), and we allowed participants with RAADS-14 scores over 23 to participate as long as their AQ-10 scores were under 6.
Exclusion Criteria
We excluded participants who were:
Diagnosed with a schizophrenia-spectrum disorder.
Had moderate to severe learning difficulties.
Sample Size Calculation
We aimed to recruit 51 autistic people and 51 people meeting diagnostic criteria for BPD, enabling us to detect clinically useful group differences with a medium effect size of d = 0.6 with 85% power at alpha = 0.05.
Recruitment
Participants were recruited between January 2023 and July 2023. Staff in adult autism, personality disorder and research and development (R&D) services in seven NHS Trusts in the North-West, North-East, Midlands and South-East regions of England identified potentially eligible service users. The research and R&D teams advertised the study through flyers in NHS waiting rooms, social media, the National Institute for Health Research Be Part of Research website and the Scottish Women’s Autistic Network.
Procedure
Clinical staff and study adverts directed potential participants to a Qualtrics-hosted website, where they could give informed consent and complete eligibility checks. The survey algorithm then automatically provided eligible participants with the study questionnaires to complete online. At each stage, potential participants could instead choose to complete informed consent, eligibility checks or the questionnaires in person, over the phone or over video call, with a member of the research team or with staff from NHS R&D teams. Participants who completed the questionnaires were sent a £25 voucher.
Measures
Total or subscale scores were used to measure constructs of interest, in line with our hypotheses. The measures completed by participants to compare the clinical features of the diagnostic groups were:
Adult Repetitive Behaviours Questionnaire 2 (ARBQ-2) subscales to assess repetitive motor behaviour and insistence on sameness (Barrett et al., 2015).
Adverse Childhood Experiences International Questionnaire (ACE-IQ) (World Health Organisation, 2011). This optional questionnaire assessed childhood experiences of parental/caregiver emotional abuse, parental/caregiver physical abuse, sexual assault and bullying. Details of how we operationalised these variables are given in Supplementary Online Information Box 1.
Camouflaging Autistic Traits Questionnaire (CAT-Q) to assess strategies used to compensate for or mask autistic characteristics (Hull et al., 2019).
Difficulties in Emotion Regulation Scale (DERS) subscales to assess non-acceptance of emotional responses, difficulties in goal-directed behaviour, impulse control difficulties, limited access to emotion regulation strategies, lack of emotional awareness and lack of emotional clarity (Gratz & Roemer, 2004).
Emotional Reactivity Scale to assess emotional reactivity (Nock et al., 2008).
Experience of Time Alone Scale (ETAS) subscales to assess the need to escape by being alone, difficulty coping when alone and intolerable distress when alone (Vardy et al., 2019).
Glasgow Sensory Questionnaire (GSQ) to assess hyper- and hypo-sensory sensitivities (Robertson & Simmons, 2013).
Inventory of Interpersonal Problems–Personality Disorder scale-25: Interpersonal Sensitivity subscale (IIP-PD-25-IS) assessing rejection sensitivity (Kim & Pilkonis, 1999).
Self-concept and Identity Measure (SCIM) to assess identity difficulties (Kaufman et al., 2015).
Social Responsiveness Scale Version 2 Adult Self-Report (SRS-2-ASR) subscales to assess social cognition, social awareness, social communication and social motivation (Constantino & Gruber, 2012).
For all measures, higher scores indicate greater differences/difficulties compared to population norms. All measures have good evidence of reliability, construct validity and concurrent/convergent validity (Barrett et al., 2015; Bölte, 2012; Borges et al., 2023; Gratz & Roemer, 2004; Hallion et al., 2018; Hull et al., 2019; Kaufman et al., 2015; Kerr-Gaffney et al., 2020; Kim & Pilkonis, 1999; Mandell et al., 2012; Meinck et al., 2022; Nock et al., 2008; Ritschel et al., 2015; Robertson & Simmons, 2013; Stern et al., 2000; Vardy et al., 2019). The internal consistency of all measures in our sample was acceptable (IIP-PD-25-IS alpha = 0.79), good (ARBQ-2 alpha = 0.88) or excellent (all other measures, alpha range = 0.92–0.95).
Analysis
We used STATA/SE version 14.2. We identified and removed bot responses using published criteria (Storozuk et al., 2020), alongside our own indicators (Supplementary Online Information Box 2). Measure distributions were assessed using the sktest command to evaluate skewness and kurtosis. Cohen’s d effect sizes and independent sample t-tests were calculated to compare scores for autistic participants and participants meeting diagnostic criteria for BPD. For non-normally distributed variables, sensitivity analyses using Mann–Whitney U-tests and between-groups Z-score comparison were conducted. Stepwise binary logistic regression was then conducted to predict group membership [dependent variable = autistic (1)/BPD (0)]. Each questionnaire total/subscale score differing significantly between the groups was added to the model, one by one, in order of Cohen’s d effect size. Variables that did not significantly predict group membership and/or did not improve model fit were removed. Models were compared using both likelihood ratio tests and area under the curve (AUC) analysis derived from the models’ receiver operating characteristic curve (ROC). For each model, sensitivity, specificity, the positive likelihood ratio, the negative likelihood ratio and the percentage of cases correctly classified was calculated, with observations classified as positive if their predicted probability was greater than 0.5. Sensitivity analyses were undertaken to ascertain how childhood trauma, and other potentially confounding variables (clinical and demographic characteristics differing in frequency between diagnostic groups by at least 10%), affected the best-performing model for predicting group membership.
Results
Description of the Sample
A total of 102 individuals consented to participate, met the eligibility criteria and completed all compulsory study measures, comprising 51 autistic individuals (Group 1) and 51 individuals meeting diagnostic criteria for BPD (Group 2). A further 140 potential participants did not meet the eligibility criteria, and 38 participants met the eligibility criteria but did not complete all compulsory study measures, so they were excluded. Further detail is shown in Figure 1 in the Supplementary Online Information. Key participant characteristics are summarised in Table 1, with further detail given in the Supplementary Online Information Table 1. While unlikely to meet full diagnostic criteria for BPD due to scoring below 7 on the MSI-BPD, 21 (41%) of our autistic participants scored between 5 and 6 on this measure, indicating likely subclinical BPD traits. Similarly, 17 (33%) of our BPD-diagnosed participants had RAADS-14 scores over 14 (the cut-off usually recommended) but under 23 (the cut-off that offers better specificity in a psychiatric population) (Eriksson et al., 2013), and 8 (16%) scored over 23 on the RAADS-14 but under 6 on the AQ-10, indicating likely subclinical autistic traits while being highly unlikely to meet full diagnostic criteria for autism.
Key Participant Characteristics.
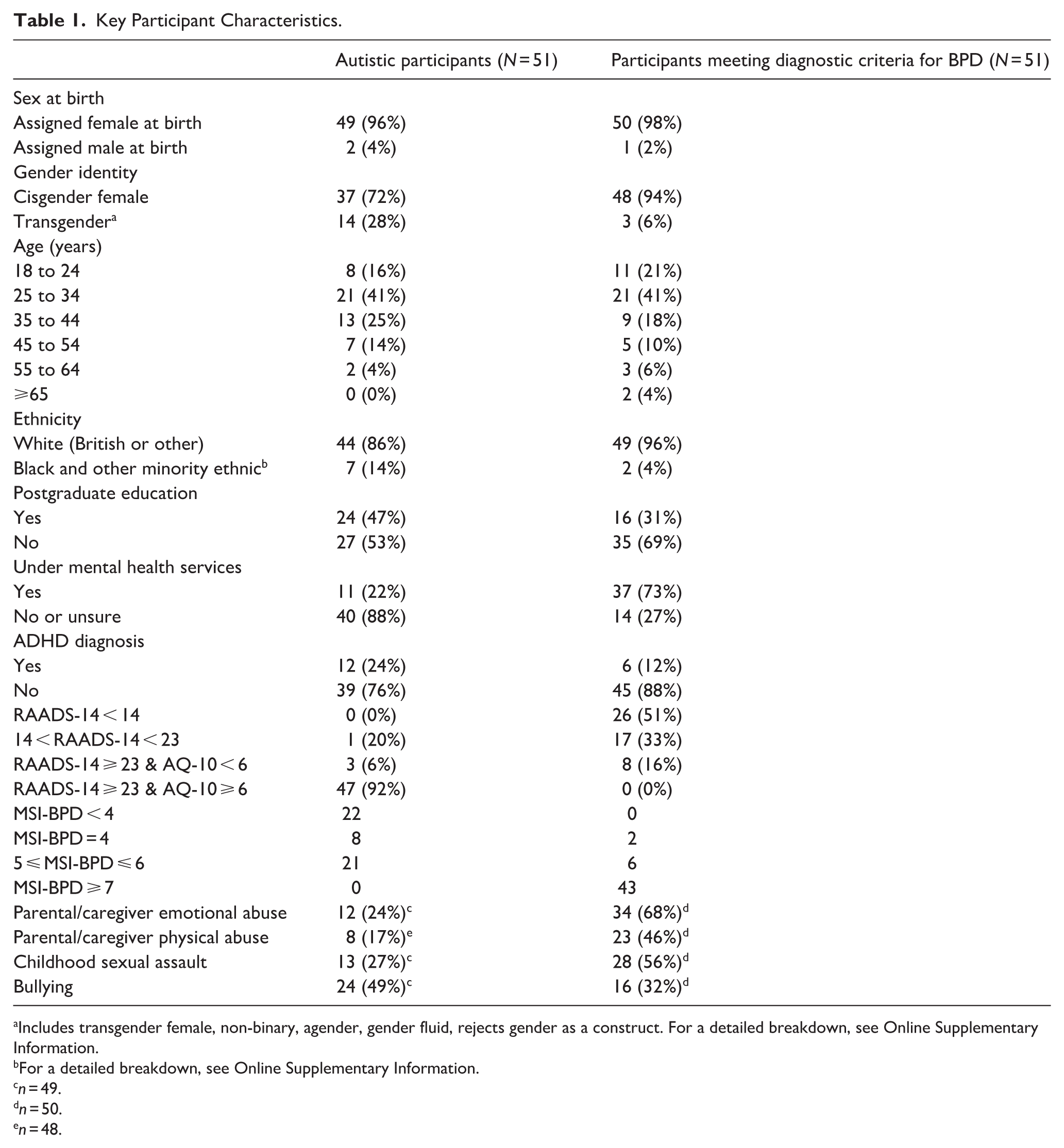
Includes transgender female, non-binary, agender, gender fluid, rejects gender as a construct. For a detailed breakdown, see Online Supplementary Information.
For a detailed breakdown, see Online Supplementary Information.
n = 49.
n = 50.
n = 48.
Differences between Diagnostic Groups
Differences between our autistic participants and our participants meeting criteria for BPD are presented in Table 2 in order of effect size.
Similarities and Differences between Autism and Borderline Personality Disorder Diagnostic Groups.
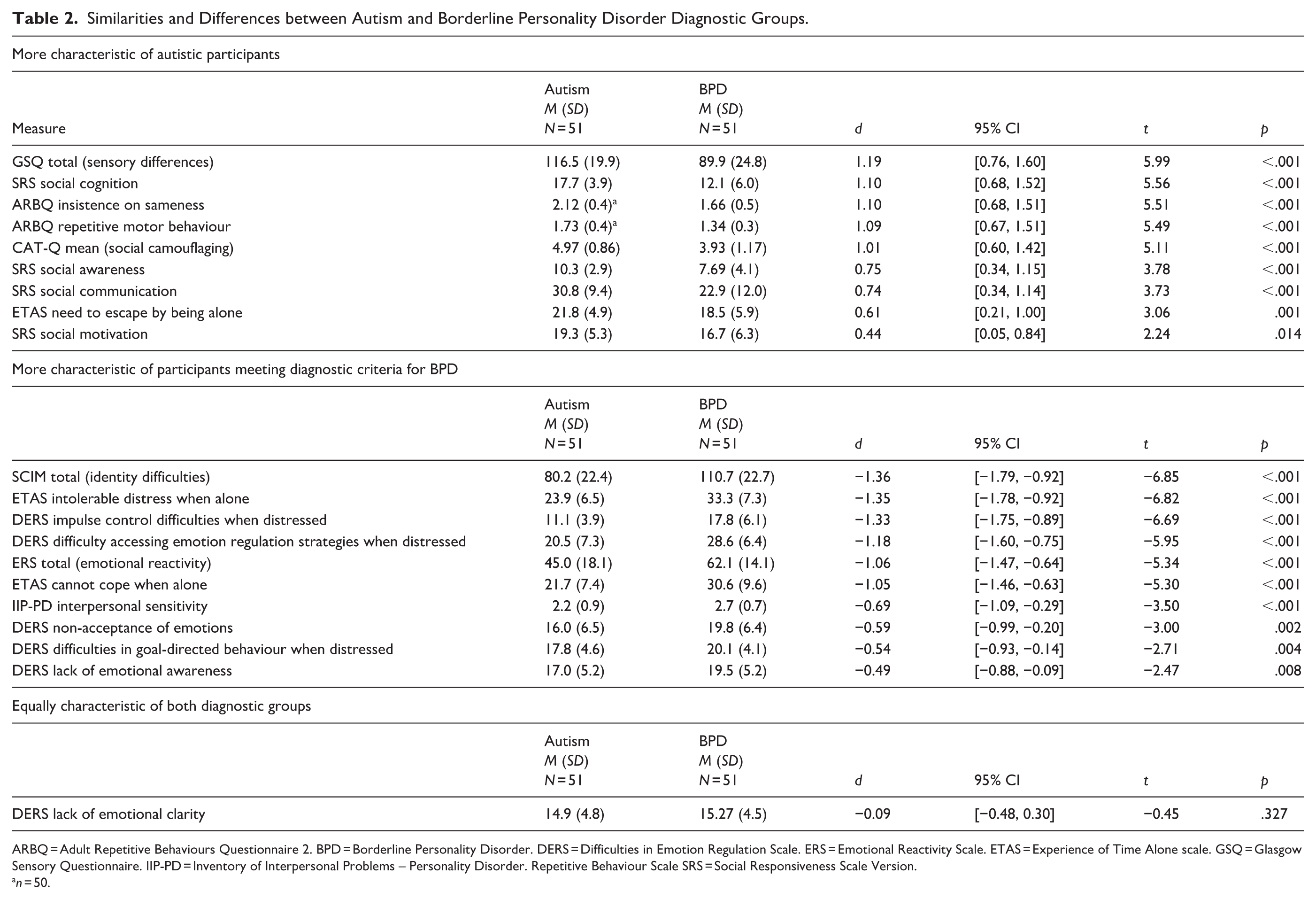
ARBQ = Adult Repetitive Behaviours Questionnaire 2. BPD = Borderline Personality Disorder. DERS = Difficulties in Emotion Regulation Scale. ERS = Emotional Reactivity Scale. ETAS = Experience of Time Alone scale. GSQ = Glasgow Sensory Questionnaire. IIP-PD = Inventory of Interpersonal Problems – Personality Disorder. Repetitive Behaviour Scale SRS = Social Responsiveness Scale Version.
n = 50.
As hypothesised, in order of effect size, the following features were significantly more characteristic of autistic participants than of those meeting criteria for BPD: sensory processing differences, social cognition differences, preference for sameness, repetitive motor behaviour, social camouflaging, differences in social awareness, differences in social communication, need for time alone and low social motivation. As hypothesised, distress and difficulty coping when alone and rejection sensitivity were significantly more characteristic of people meeting diagnostic criteria for BPD than of autistic people. Contrary to hypothesis, emotional reactivity, emotional dysregulation and identity disturbance were also significantly more characteristic of people meeting diagnostic criteria for BPD, with identity disturbance representing the biggest difference from autistic participants. As hypothesised, the emotional clarity subscale of the DERS was equally impaired in both groups. The effect sizes for the majority of identified differences were either large (d ≥ 0.8) or moderate (0.5 ≤ d > 0.8). Sensitivity analysis using Mann–Whitney U-tests for non-parametric data showed that all between-groups differences remained statistically significant, and the ordering of group differences by Z-score did not differ from the ranking by Cohen’s d effect size (Supplementary Online Information Table 2).
What Combination of Characteristics Provides the Best Prediction of Diagnostic Group?
A summary of the model fit statistics for the forward entry binary logistic regression models predicting membership of Group 1 (autistic participants) versus Group 2 (meeting diagnostic criteria for BPD), entered in order of effect size, is shown in Online Supplementary Information Table 3. Variance Inflation Factors were low at every step (range = 1.02–2.85). The full models, and details of the process for selecting the optimal model, can be found in the Supplementary Online Information Box 3 and Table 4.
Total self-concept and identity difficulties (SCIM score) were entered first and improved explanatory power versus the null model (Supplementary Online Information Table 3 Model 1), correctly classifying 71.6% of participants. While ETAS intolerable distress when alone and the GSQ total sensory sensitivity score were initially significant additions to the model, they became non-significant once the SRS social cognition subscale score was added (Supplementary Table 3 Model 5b; Supplementary Table 4) and so were removed. The final model, considered to offer the best and most parsimonious fit to the data, consisted of the following variables, each of which significantly independently predicted group membership: SCIM identity disturbance total (odds ratio [OR] = 0.91, 95% confidence interval [CI] = [0.87, 0.96], p < .01); DERS impulse control (OR = 0.68, 95% CI = [0.54, 0.87], p < .01); SRS social cognition (OR = 1.62, 95% CI = [1.22, 2.16], p < .01); ETAS cannot cope when alone (OR = 0.86, 95% CI = [0.76, 0.99], p = .03); CAT-Q social camouflaging total (OR = 1.05, 95% CI = [1.01, 1.09], p = .01). This model had an AUC of 0.98 (95% CI = [0.97, 1.00]), a sensitivity of 94.12%, a specificity of 96.08%, a positive likelihood ratio (LR+) of 24.01 and a negative likelihood ratio (LR−) of 0.06 for differentiating between Group 1 and Group 2 and correctly classified 95.10% of participants (Supplementary Online Information Table 3 Model 8).
Assessment of Possible Confounders
As shown in Table 1, childhood experiences of parental/caregiver emotional abuse, parental/caregiver physical abuse, sexual assault and bullying were common in both diagnostic groups. Other than bullying, each of these experiences was significantly more common in the group meeting diagnostic criteria for BPD [parental/caregiver emotional abuse χ2(1, 99) = 18.83, p < .001; parental/caregiver physical abuse χ2(1, 98) = 9.74, p = .002; childhood sexual assault χ2(1, 99) = 8.86, p = .003; bullying χ2 (1, 99) = 2.96, p = .085]. Non-cisgender, postgraduate education and co-occurring attention-deficit/hyperactivity disorder (ADHD) diagnoses were substantially more prevalent in the autism group (Group 1) than in the BPD group (Group 2) while being under mental health services was substantially more prevalent in the BPD group (Table 1). When added to the model of characteristics best predicting group membership (Supplementary Online Information Table 3 Model 8), these variables were not independent predictors, excepting parental/caregiver physical abuse (OR = 0.06, 95% CI = [0.00, 0.94], p = .045). However, the model including this variable resulted in reduced sensitivity (93.75%), specificity (94.00%) and correct classification (93.88%) (Supplementary Online Information Tables 3 and 4).
Discussion
Through a robust and comprehensive comparison of the diagnostic groups, we found more differences than we expected between autism and BPD. The differences we found were apparent despite including individuals with subclinical traits of the comparator diagnosis, and aligned with each diagnostic construct.
Interpretation of Findings and Comparison with Previous Research
Comparison to the General Population
To better contextualise our findings, it is important to understand how our participants’ scores on the measures compare to the scores of general population (i.e. non-clinical) samples. We conducted literature searches to identify the largest available studies using our study measures among general population samples. A comparison of our sample scores with those in general population samples is shown in Table 3.
Comparison of Our Sample Measure Scores with Published Research in General Population Samples.
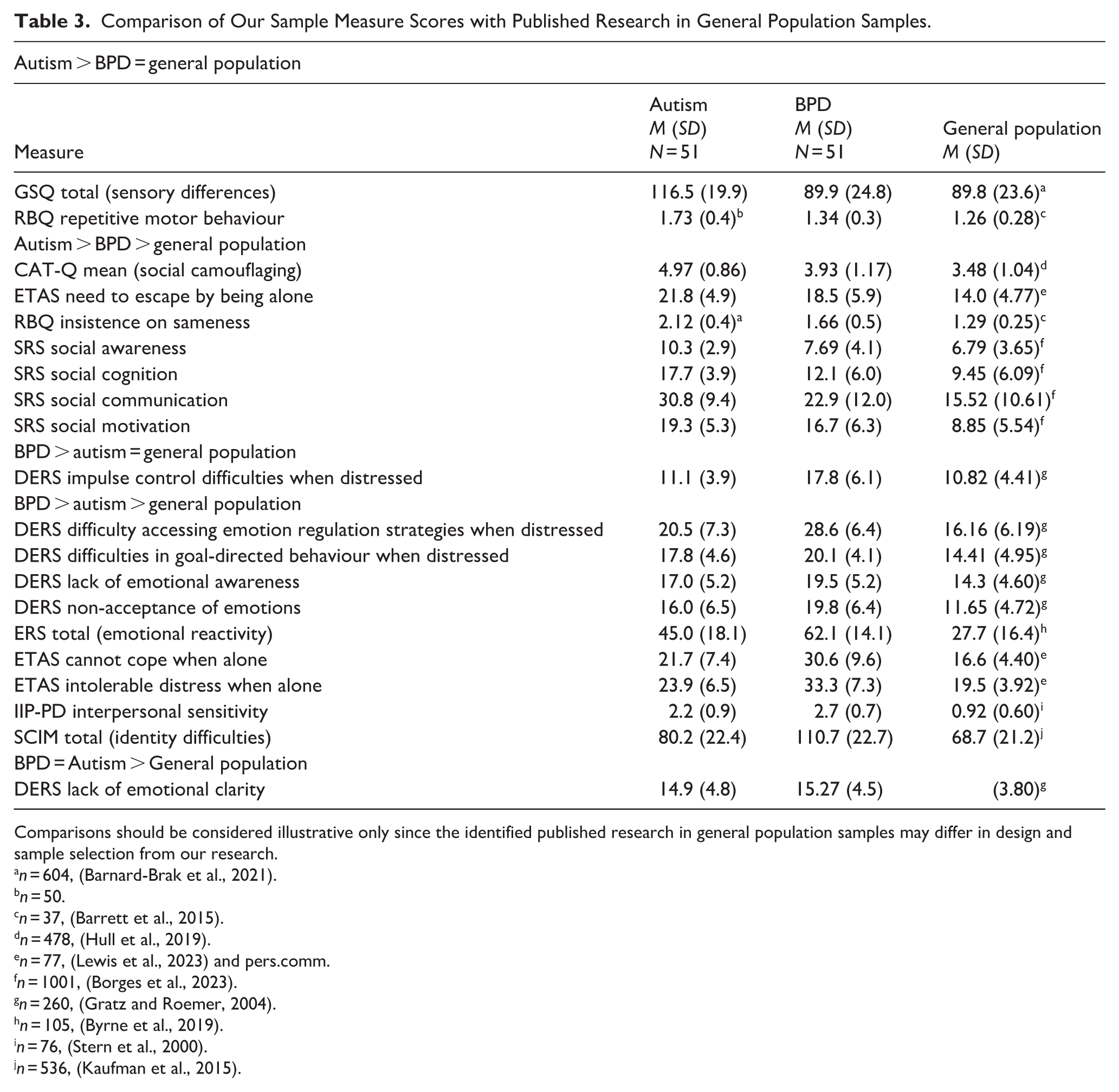
Comparisons should be considered illustrative only since the identified published research in general population samples may differ in design and sample selection from our research.
n = 604, (Barnard-Brak et al., 2021).
n = 50.
n = 37, (Barrett et al., 2015).
n = 478, (Hull et al., 2019).
n = 77, (Lewis et al., 2023) and pers.comm.
n = 1001, (Borges et al., 2023).
n = 260, (Gratz and Roemer, 2004).
n = 105, (Byrne et al., 2019).
n = 76, (Stern et al., 2000).
n = 536, (Kaufman et al., 2015).
Characteristics Typically Associated with Bpd
There were moderate-to-large differences suggesting heightened emotional reactivity and dysregulation, identity difficulties, difficulty being alone and rejection sensitivity among our BPD participants compared to our autistic participants. However, comparison of our sample scores with previous research using the same measures suggests that autistic individuals may still experience increased difficulties in all of these areas compared to the general population (Table 3). Previous research has found a similar pattern of heightened emotional dysregulation in autistic adults compared to non-clinical samples, but even more heightened emotional dysregulation among BPD-diagnosed people (Bemmouna et al., 2023). The mild level of identity disruption seen in our autistic sample may relate to the effects of social camouflaging, while mild levels of rejection-sensitive dysphoria, and distress and difficulty coping with being alone, may stem from experiences of social rejection, alienation and loneliness (Aves, 2022; Hull et al., 2017; Kiehl et al., 2024; McQuaid, Strang, & Jack, 2024). Since an autism diagnosis can reduce emotional distress and increase identity consolidation (Gray et al., 2024; Kiehl et al., 2024), potentially undiagnosed autistic individuals may experience more severe difficulties than our post-diagnosis sample.
Lack of emotional clarity was the sole variable found not to differentiate the diagnostic groups. This contradicts some clinicians’ views that BPD-diagnosed people have less difficulty in identifying their emotions than autistic people (Cumin et al., 2022). Alexithymia may relate to trauma-linked dissociation in people meeting diagnostic criteria for BPD and to sensory processing differences in autistic people (Chaim et al., 2024; Kinnaird et al., 2019).
Characteristics Typically Associated with Autism
There were moderate-to-large differences in social avoidance, social cognition, social awareness, social motivation and social camouflaging, and heightened preference for sameness, among our autistic participants compared to our participants meeting diagnostic criteria for BPD. The identified social differences can be understood in relation to the double empathy problem, whereby autistic and non-autistic individuals experience mutual difficulties in understanding each other (Milton et al., 2022). However, comparison of our sample scores with previous research using the same measures in non-clinical samples, suggests that people meeting diagnostic criteria for BPD may still experience increased difficulties in many of these areas compared to the general population (Table 3). Mild autism-aligned differences in aspects of social interaction could be explained by social anxiety, trauma-related shame and difficulties with trust in people meeting diagnostic criteria for BPD (Hull et al., 2019; Jørgensen & Bøye, 2024; South et al., 2017). Some degree of preference for sameness could be linked to safety-seeking and cognitive rigidity following trauma (Al-Attar et al., 2024).
Differentiating Autism and Bpd
While we identified many diagnosis-aligned differences between our autistic and BPD-diagnosed participants, our tentative comparison of our findings to general population scores in previous research suggests that many of these characteristics are present to some extent transdiagnostically, relative to the general population (Table 3). This suggests it is important to take into account the severity/extent of difficulties in these areas when making a differential diagnosis. An exception was impulsivity, on which our autistic sample scored very similarly to a general population sample (Table 3) (Gratz & Roemer, 2004). This fits with views of autism as characterised by behavioural over-control rather than disinhibition (Lynch, 2018). In addition, our BPD sample scored very similarly on the GSQ sensory sensitivity questionnaire and on the repetitive motor behaviour RBQ subscale to general population samples (Table 3) (Barnard-Brak et al., 2021; Barrett et al., 2015). This contradicts a Delphi study of clinicians who felt they did encounter sensory differences among people with BPD (Sarr et al., 2025).
Strengths and Limitations
The study sample was drawn from across the United Kingdom, represented a range of ages, and was gender diverse. However, most of the sample were educated to degree level or above, and ethnic diversity was lacking (Tromans et al., 2021). We used carefully specified thresholds on our screening measures to include individuals with subclinical traits of the comparator diagnosis, as long as they were unlikely to meet full diagnostic criteria. However, carrying out diagnostic interviews would have represented a more robust method of establishing this. We do not know whether excluded participants actually had undiagnosed comorbidity. If not, then screening them out could have reduced sample variance relative to the wider diagnostic populations and made our groups more dissimilar. The accessibility of the included measures for autistic people – which may be threatened by terms or language structures that are ambiguous, imprecise or metaphorical – has not been evaluated (Nicolaidis et al., 2020). Our comparisons with previous research using these measures in the general population may be affected by differences in sample characteristics and study design. Furthermore, while this study represents the most comprehensive comparison of the diagnostic groups to date, some potential additional areas of difference, such as intense interests and differences in non-verbal communication (autism); emptiness, idealisation and devaluation, and dissociation (BPD), were not evaluated in this study.
Conclusion
Previous research indicates that screening measures alone may be insufficient to differentiate between autism and BPD, given that half of BPD-diagnosed individuals score above the cut-off on the AQ-50 (Dudas et al., 2017). Based on our findings in women and PAFAB, it may additionally be useful to administer self-report questionnaires or clinical interviews assessing social cognition, social camouflaging, identity difficulties, impulsivity, difficulties coping with being alone, sensory processing and repetitive motor behaviour. These additional measures may help to guide clinical decision-making about onwards referral for fuller personality and/or autism diagnostic assessments. To aid clinicians, examples of the questions used to assess these domains in our study are given in Supplementary Online Information Box 4. However, differences in many of these areas may be present to some extent transdiagnostically, suggesting that it is important to take into account the severity/extent of difficulties in these areas when making a differential diagnosis.
Future research should identify a smaller subset of items that are most useful for guiding referral decisions. These should be tested in larger samples, including a matched general population comparison arm, with sufficient AFAB, AMAB and gender-diverse individuals to investigate any differences by sex assigned at birth or gender identity. Diagnostic interviews should be used to establish who does and does not meet full diagnostic criteria for each condition. Subgroups of people with a BPD diagnosis who show high levels of autistic traits and vice versa, should also be included to help us better understand these clinical groups.
Supplemental Material
sj-docx-1-aut-10.1177_13623613261431309 – Supplemental material for Overlapping And Differentiating Clinical Features of Autism and Borderline Personality Disorder in Women and People Assigned Female at Birth: A Cross-Sectional Study
Supplemental material, sj-docx-1-aut-10.1177_13623613261431309 for Overlapping And Differentiating Clinical Features of Autism and Borderline Personality Disorder in Women and People Assigned Female at Birth: A Cross-Sectional Study by Kirsten Barnicot, Elissa Thompson, Sally Turner, Will Mandy, Rose McCabe, Eloise Stark and Jennie Parker in Autism
Footnotes
Acknowledgements
We would like to thank all of our participants for their time and expertise, and we are grateful for the advice and feedback received from our lived experience advisory panel (Jenn Layton Annable, Jo Barnes, Eva Broeckelmann, Eloise Curtis, Peg Digitalis, Sarah Labovitch, Sheena Dean) and our clinician advisory panel (Mike Crawford, Tennyson Lee, Silvia Murguia, Rachael Line, Richard Smith, Richard Pender, Harriet Fletcher, Simon Graham).
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the West Midlands–South Birmingham National Health Service (NHS) Research Ethics Committee on January 14, 2022 (REC ref. 21/WM/0287, IRAS 307912).
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by a grant from Words That Carry On through the McPin Foundation (ref. WTCO Research Award).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The pseudonymised data that support the findings of this study are available from the corresponding author, KB, upon reasonable request.
Informed Consent
Written informed consent was obtained from all participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.