
Abstract
Autism is increasingly understood from a neurodiversity-affirmative perspective recognising the unique contributions of autistic individuals. Despite this shift, the specific experiences of autistic healthcare students in clinical placements remain underexplored. This scoping review aims to map existing literature on this topic, identifying both barriers and enablers to learning in clinical environments. Using Arksey and O’Malley’s framework, with methodological updates, a comprehensive search was conducted across databases including CINAHL, Medline, APA PsychInfo, Education Research Complete PubMed, Google Scholar, ProQuest and grey literature. Studies were included if they focused on the perspectives of autistic undergraduate healthcare students in clinical practice. Six studies met the inclusion criteria, which were synthesised into four overarching analytical categories: autistic profiles, sensory environments, disclosure and support and belonging and inclusion. Students reported strengths including empathy and attention to detail, alongside challenges like sensory sensitivities and social communication difficulties. Disclosure experiences varied, and a strong sense of belonging was linked to improved mental health and academic success. This review highlights the urgent need for inclusive educational practices, including tailored support, autism training for educators and a culture of acceptance. It also reveals a significant gap in the literature, underscoring the need for further research in this area.
Lay Abstract
This study explores what it is like to be an autistic student training in healthcare, particularly during clinical placements. While we know autistic people are entering higher education and healthcare professions, there is still very little research about their specific experiences in clinical learning environments. These placements are a key part of training for careers like nursing, midwifery and medicine, but they can be especially challenging for autistic students. To better understand this, a scoping review was carried out. This means the researcher searched for and reviewed existing studies and articles on the topic. Only six relevant articles were found, all written in the UK, and were based on personal experiences shared by autistic students themselves. The review grouped findings into four main areas: the unique strengths and challenges of autistic students, the impact of sensory environments, the difficulties around disclosing an autism diagnosis and the importance of feeling included and supported. The findings show that while autistic students bring valuable qualities to healthcare, like empathy and attention to detail, they often face barriers such as sensory overload, stigma and a lack of tailored support. Many students feel they must mask their autism to fit in, which can affect their mental health and sense of belonging. This study highlights the urgent need for more inclusive and supportive clinical learning environments. It calls for better training for educators and supervisors, more awareness of autism and practical changes to help autistic students thrive. More research is needed to fully understand and support this group of students.
Background
Autism has historically been framed through a medical model that emphasises deficit and disorder. In contrast, increasing research and advocacy support a neurodiversity-affirmative approach, which recognises autism as a natural variation in cognitive functioning rather than a pathology (Botha et al., 2024; Shaughnessy et al., 2024; Sonuga-Barke & Thapar, 2021). This evolving perspective aligns with the social model of disability, which highlights how structural barriers and social exclusion contribute to disabling experiences (Dwyer, 2022; Fletcher-Watson & Happé, 2019). The neurodiversity paradigm builds on this by (2006, 2022) asserting that neurodivergent individuals should be accepted and supported regardless of their level of disability (Rosqvist et al., 2020). Although debates persist around terminology and models (Bailin, 2019; Ballou, 2018; Kapp, 2020), many in the autistic community advocate for identity-first language and the principle of ‘nothing about us, without us’ (Botha et al., 2021; Taboas et al., 2022). Reflecting these values, this review is led by an autistic midwifery researcher and contributes to the growing body of work by neurodivergent scholars.
Over the past 5 years, the number of students with a declared disability studying in UK higher education has risen from 340,420 to 484,270 (HESA, 2024), reflecting a growing recognition of neurodiversity within academic institutions. This trend of increasing neurodivergent representation and associated challenges is evident across various academic fields, including among research students (Tan, Rabuka et al., 2025; Tan, Edwards et al., 2025). A report by Unite Students (2023) found that over 14% of students surveyed identified as being neurodivergent or multiply neurodivergent. Although data on autistic students in healthcare remains limited, some insight into the prevalence of neurodivergent traits can be drawn from other neurotypes. For example, Wray et al. (2012) found that 29% of nursing students met the criteria for a dyslexia diagnosis, suggesting that neurodivergence may be particularly common in healthcare disciplines. This raises important questions about the representation and support of autistic students, whose experiences in clinical practice are notably under-researched.
In addition, the National Health Service (NHS), the UK government-funded healthcare system, published the Longterm Workforce Plan promoting a vision of a compassionate and inclusive NHS yet acknowledged that disabled staff report higher levels of bullying and harassment (NHS England, 2023). Moreover, the Institute of Leadership and Management (2020) found that 50% of managers would not employ someone from at least one neurominority group, with the greatest bias directed towards autism, attention-deficit/hyperactivity disorder (ADHD) and Tourette’s. These findings suggest that discriminatory attitudes may extend into educational settings, a concern amplified by reports that medical education contexts may be regarded as unwelcoming to disabled students and faculty, citing negative attitudes, inaccessible environments and struggles to receive reasonable adjustments (Aitken et al., 2025). The incidence of different neurotypes may be higher within healthcare, as these professions often attract individuals with traits such as attention to detail, pattern recognition and a conscientious work ethic (McCowan et al., 2021). In surveys aimed at identifying and supporting autistic patients, approximately 1% of GPs and psychiatrists identified as autistic (Crane et al., 2019), although this figure is likely an underestimation (McCowan et al., 2021) and does not provide insight into student populations.
Despite these developments and the rising number of autistic students in UK higher education, the exact number of autistic healthcare students remains unknown. This lack of visibility is also highlighted in reviews specific to medical education and may be attributed to several intersecting factors (Aitken et al., 2025). Many students choose not to disclose their diagnosis due to fears of stigma (Cinarbas & Hos, 2022), previous negative experiences (Svendby, 2020) or concerns that disclosure could negatively impact their academic progress or future career (Dolmage, 2017; Grimes et al., 2019). Beyond individual concerns, autistic students may face challenges in help-seeking, particularly in environments that lack neurodiversity-affirmative practices. Furthermore, institutional systems for data collection, whether at university or national levels, may also be inadequate for capturing the full spectrum of autistic student participation, especially when diagnoses are delayed or students self-identify without formal recognition. While existing research has explored the general educational experiences of autistic students (Davis et al., 2021; Nuske et al., 2019), there is limited understanding of how these challenges manifest within healthcare education, which uniquely combines academic rigour with clinical practice. Moreover, although the literature on disabled healthcare professionals is expanding, the specific perspectives of autistic healthcare students remain underrepresented (Bulk et al., 2020; Lindsay et al., 2023). This gap is particularly concerning given the distinct demands of clinical learning environments, which can significantly influence both educational outcomes and professional development.
Healthcare studies such as midwifery, nursing and medicine are viewed as practice-orientated professions, which require students to complete clinical hours alongside theoretical learning before being added to a professional register (NMC, 2018, 2019). Training within healthcare settings is widely recognised as a demanding experience; the Royal College of Nursing (2024) reports an average attrition rate of 21% among nursing students, who also face elevated risks of stress, burnout and depression compared to peers in other disciplines (Sassoon et al., 2025). Although data on university attrition rates among autistic students is limited, existing studies indicate that they are less likely to complete their degrees than non-autistic students (Anderson et al., 2017; Newman et al., 2011). Given this context and the heightened likelihood of unmet support needs among autistic students, it can be postulated that these factors may contribute to disproportionately higher attrition rates within this group. It is vital to explore the current evidence base to better understand and address their experiences and support needs. Yet, the literature remains sparse and fragmented. This aligns with other reviews confirming that the experiences of autistic medical students are under-researched, underscoring the necessity of reviews like this one to map existing knowledge (Aitken et al., 2025).
Accordingly, the purpose of this review is to use a scoping methodology to explore what is known about the experiences of autistic students in healthcare education in a clinical setting. Arksey and O’Malley (2005) describe this approach as aiming to identify gaps in the evidence base where little research has already been undertaken. Scoping studies are relevant in areas with emerging evidence where randomised controlled trials have not yet been conducted and where a range of study designs can be included (Levac et al., 2010). This methodology also allows researchers to explore complex concepts, which in turn may lead to new lines of enquiry (Davis et al., 2009). This review will be guided by Arksey and O’Malley’s methodological framework and will also take methodological advancements into account (Levac et al., 2010; Peters et al., 2020). Importantly, this review is shaped by the perspective of the first author, an autistic midwifery researcher, bringing an insider’s perspective to an area in need of neurodivergent-authored research. This scoping review aims to address this gap by systematically mapping the existing literature on the experiences of autistic healthcare students in clinical practice. By examining studies that focus on this specific population, the review seeks to provide a comprehensive overview of the experiences of autistic healthcare students in clinical practice. The findings will contribute to the development of more inclusive healthcare education practices and policies that support autistic students.
Method
This scoping review was conducted according to the Joanna Briggs Institute (JBI) scoping review methodology (Peters et al., 2020) and the methods described by Arksey and O’Malley (2005) and Levac et al. (2010). The PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews Checklist) (Tricco et al., 2018) was used to ensure the study was reported in a transparent and rigorous manner. The use of scoping review methodology allows the author to map out and clarify the main concepts, definitions and features found in existing literature, offering a broad overview (Munn et al., 2018). Unlike systematic reviews, scoping studies do not typically appraise the quality of evidence or seek to produce aggregated effect estimates but may involve descriptive or analytical synthesis to map patterns across the literature (Arksey and O’Malley, 2005). Scoping review methodology was chosen in view of the quality and sparsity of the literature available, allowing the authors to determine gaps in the literature and areas for future study. The stages in this methodology include (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) analysis and synthesis. The protocol for the search was developed in January 2025 and amended in September 2025.
Identifying the Research Question
The research question was developed using Levac et al.’s (2010) recommendation of pairing a wide-ranging research question with a well-defined scope of investigation. Focusing on this enquiry required defining the concept (neurodivergence within healthcare education), target population (autistic healthcare students) and outcomes (student perspectives on clinical placement experiences) to ensure the search strategy was effective. Healthcare students were defined as those enrolled in pre-registration or undergraduate degree programmes that include clinical placements and lead to regulated healthcare qualifications (e.g. medicine, nursing, midwifery, radiography). The purpose of this study was to identify the facilitators and barriers to learning in a clinical environment from the perspective of autistic healthcare students, with the underpinning rationale to contribute to the literature supporting more inclusive healthcare education. This process prompted the development of the research question: ‘What are the experiences of autistic healthcare students in a clinical learning environment?’
Identifying Relevant Studies
For this scoping review, it was necessary to ensure that the studies were identified from a broad and comprehensive range of sources. No restrictions were placed on publication dates to ensure a comprehensive view of the research progression in this field. The strategy was refined through discussion with collaborators. On 01/09/2025, the first author searched four databases CINAHL, Medline, APA Psychinfo and Education Research complete via EBSCO host. Searches were also undertaken on PubMed, Google scholar and ProQuest. The terms used were variable to account for differences in the indexing of the different databases. Additional sources of grey literature including pre-prints, websites and other academic thesis databases were reviewed but yielded no relevant material. As per guidance for JBI reviews (Peters et al., 2020), the sources included all primary research studies and grey literature sources, to ensure autistic student accounts were systematically captured. Studies were included if they met the defined criteria for concept, target population and outcomes defined. The inclusion and exclusion criteria are defined below:
Inclusion:
Studies published in the English language
Full text available
Studies examining autistic undergraduate healthcare students
Studies examining qualified staff reflection on their experience as a student
Articles detailing the perspectives of students in clinical practice/placement.
Exclusion:
Population examined was qualified healthcare professionals with no mention of student experience
Studies that positioned the perceptions of healthcare educators
Studies that made no mention of a student’s experience in clinical practice
Study Selection
The study-selection process is summarised in Figure 2, in line with PRISMA-ScR recommendations. The initial search yielded 33,304 results, and 1085 results were uploaded into a shared file in Zotero. An iterative approach was used to select studies for inclusion. Titles and abstracts were screened by two independent reviewers, with 18 articles retained at this step. They were joined by a third researcher as they independently examined the full texts. The three researchers then met to discuss these articles, and any disagreements or uncertainties regarding inclusion were resolved through discussion among all three researchers to reach consensus. Two made no mention of healthcare students and focused on the general university or college population, eight lacked a focus on autistic student experiences and two made no mention of firsthand experiences. Six studies were included in the final review. The reference lists of the included studies were then searched; nine studies were identified, but no further references were included.
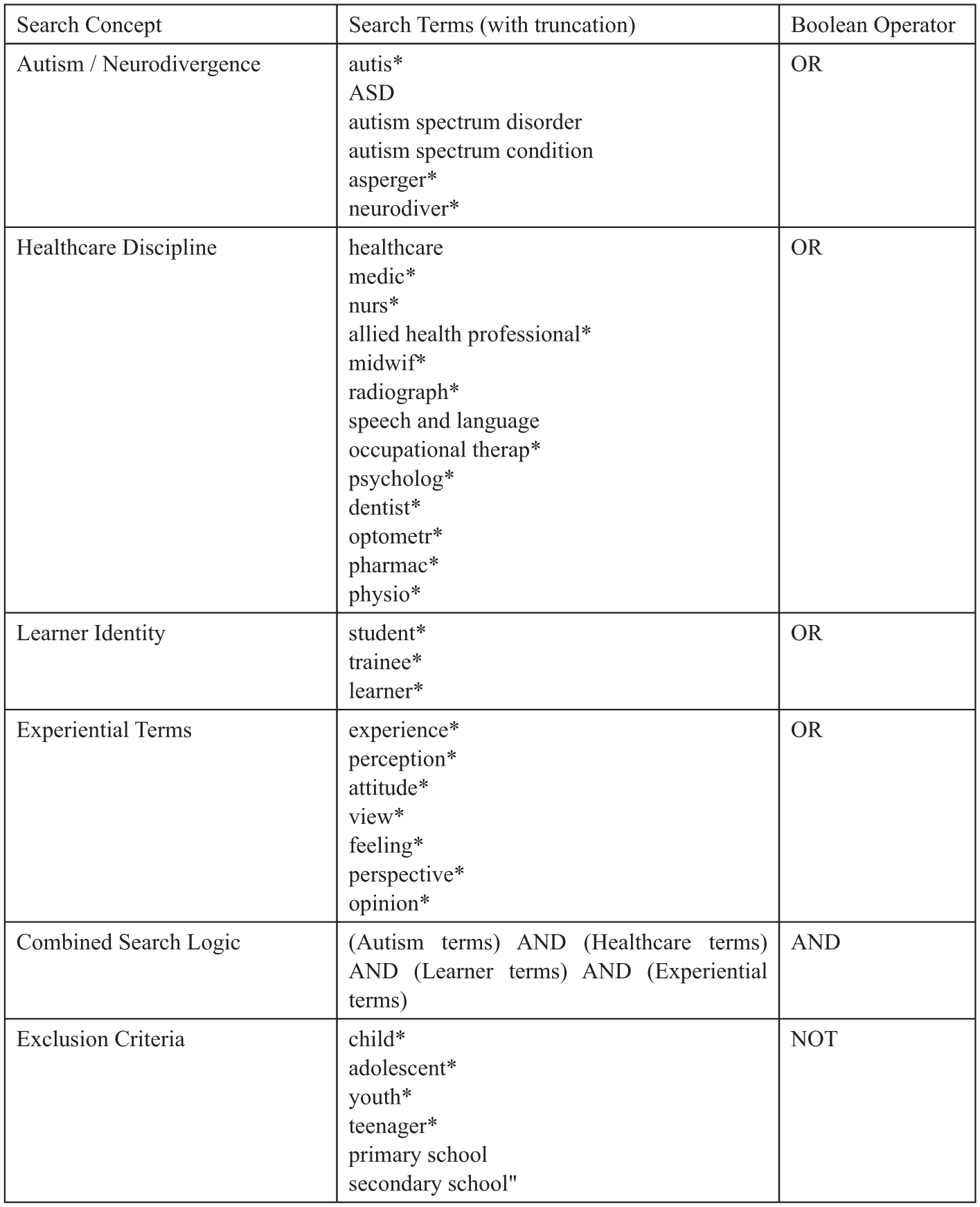
A Table Showing the Search Terms Used on EBSCO Host With the Combination of the Boolean Operators ‘OR’, ‘AND’ and ‘NOT’.
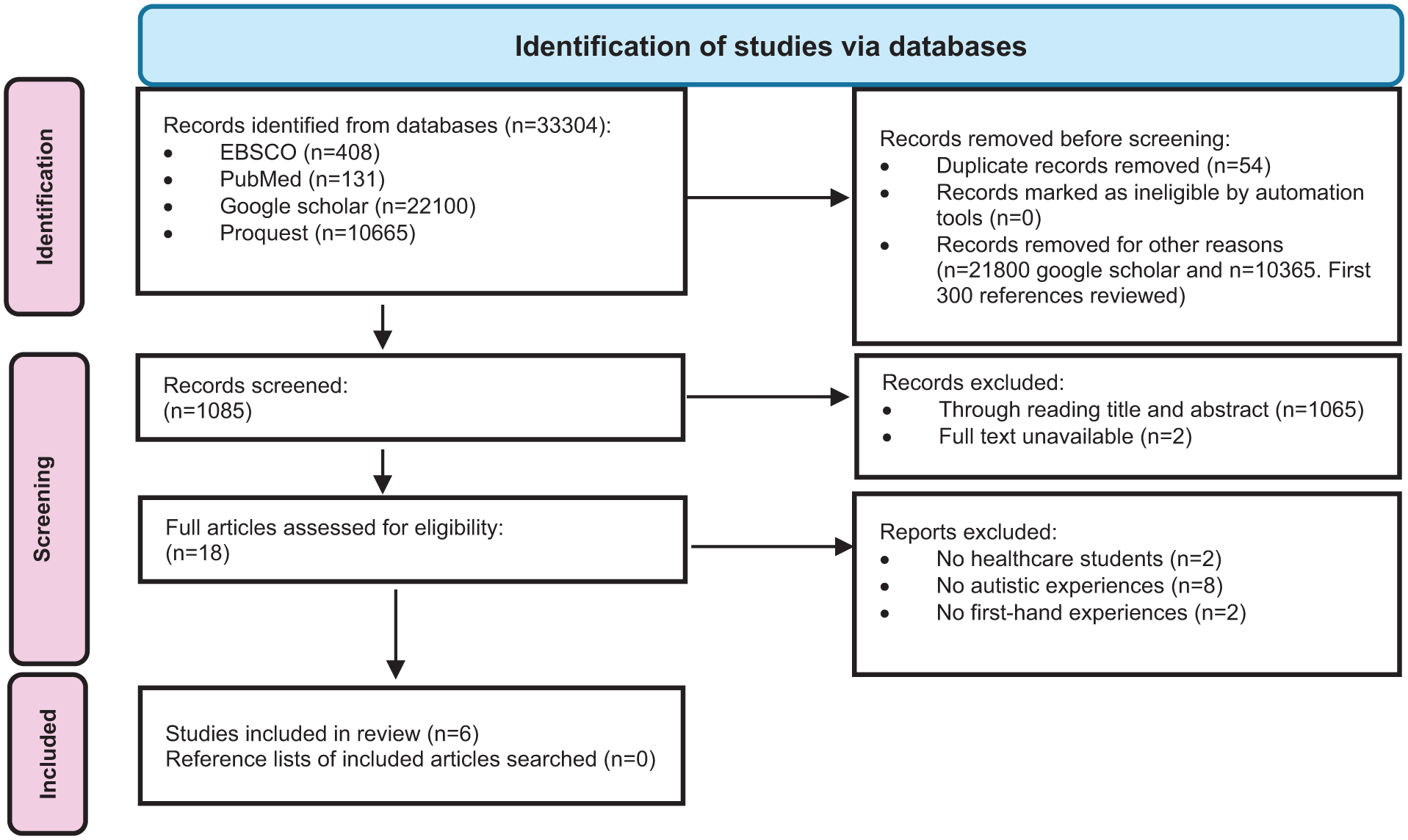
Study-Selection Strategy.
Given that one of the included studies was authored by the lead researcher, additional steps were taken to ensure reflexivity and minimise bias in the selection and appraisal process. The study was assessed against the same inclusion criteria as all other articles, with no preferential treatment. To enhance objectivity, the screening and data-extraction processes were conducted collaboratively with co-authors. Specifically, titles and abstracts were screened independently, and the self-authored article was critically appraised and discussed within the team to ensure its relevance and alignment with the research question. This collaborative and transparent approach aimed to uphold the integrity of the review and ensure that the inclusion of the self-authored study was justified by its contribution to the evidence base.
A study on the experiences of doctors was included as a portion of the data reflected their retrospective accounts of medical school and clinical placements. Although the participants were qualified professionals at the time of the study, the survey instrument was specifically designed to capture their experiences as students, including challenges encountered during clinical education. This retrospective lens offers valuable insights into the long-term impact of clinical learning environments on autistic individuals and aligns with the review’s focus on student experiences. The study was included following careful appraisal and discussion among co-authors, and its relevance was confirmed based on the presence of detailed data pertaining to clinical placements during undergraduate training. Including this study enhances the depth of the review by providing longitudinal perspectives that are otherwise absent in the current literature.
Results
Charting the Data
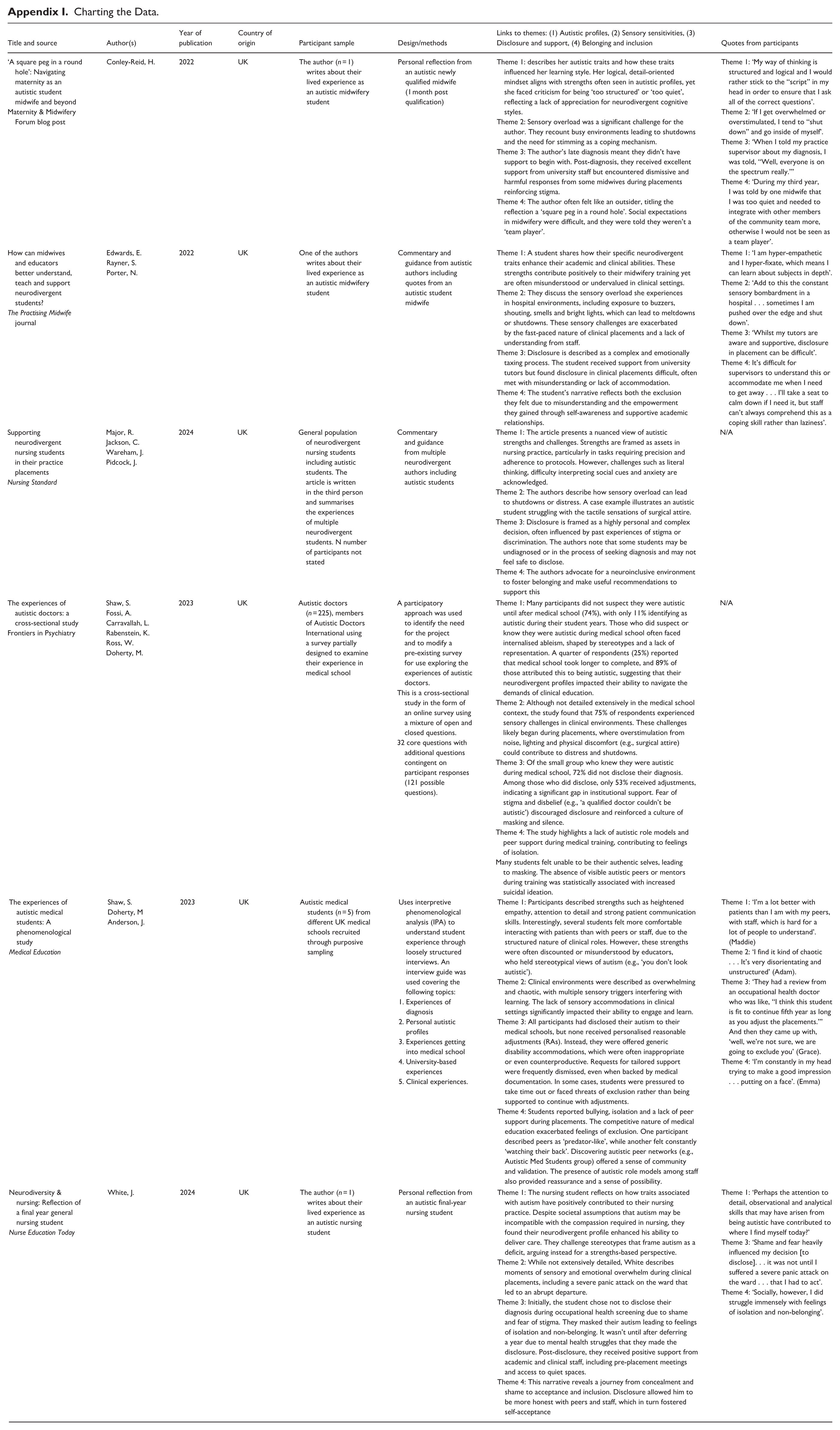
Six articles were identified and selected for scoping review, and the data was charted independently by the first and second authors in a data-extraction form (Appendix 1) established using a JBI template (Peters et al., 2020). The data included in the final table was then discussed with co-authors to ensure the data extraction was consistent with the research question and purpose.
The six studies included in this scoping review varied in design, methodological rigour and depth of analysis. Two studies (Shaw, Doherty, et al., 2023; Shaw, Fossi, et al., 2023) employed empirical methodologies, including phenomenological and cross-sectional designs, offering structured data collection and thematic analysis. These studies demonstrated high reliability through transparent methods and participant sampling, although Shaw, Doherty, et al. (2023) relied on retrospective accounts, which may introduce recall bias. Shaw, Fossi, et al. (2023) used purposive sampling and interpretive phenomenological analysis, providing rich insights but with limited generalisability due to the small sample size (n = 5). White (2024) and Conley-Reid (2022) presented reflective, first-person narratives. While these accounts offer authentic and nuanced perspectives, they are anecdotal and lack a methodological structure, limiting their reliability and validity. Nonetheless, their inclusion is justified by the review’s aim to centre lived experience. Edwards et al. (2022) and Major et al. (2024) provided commentary and guidance based on personal experience and professional practice. These articles blended reflective testimony with practical recommendations but did not employ formal research designs.
All studies included were published between 2022 and 2024 and were written by UK authors discussing the experiences of UK healthcare students. The sparsity of the articles found reflects the limited research available on the specific experiences of autistic healthcare students. However, the six articles were written by one or more neurodivergent authors, bringing authenticity, lived experience and nuanced understanding of the challenges faced by neurodivergent students.
Analysis and Synthesis
Levac et al. (2010) criticise the Arksey and O’Malley (2005) framework for its lack of detail in the process of collating, summarising and reporting the results from a scoping study. This study therefore undertook a more systematic approach to this step utilising NVIVO software providing a structured framework for organising, managing and analysing the data. Following study selection and data charting, a qualitative, framework-based synthesis was undertaken to organise and interpret patterns across the included studies. Consistent with the aims of a scoping review, the analysis focused on the reported findings and experiential accounts within each publication, rather than primary participant-level data. This allowed a systematic comparison across heterogeneous study designs, including empirical studies, reflective narratives and commentary articles.
Full texts were imported into NVivo and read iteratively by the lead author. Initial inductive coding captured recurrent areas of focus across results, discussion and reflective sections. These codes represented common experiential topics and were then grouped into broader analytical categories through iterative comparison and refinement, supported by team discussion.
While informed by Braun and Clarke’s (2006, 2022) work on analytic reflexivity, the resulting themes function as organising categories that synthesise patterns across the literature, consistent with framework-based and thematic synthesis approaches. They represent topic-based groupings rather than meaning-making themes derived from primary qualitative data. Through this process, four overarching themes were identified:
(a) Theme 1 – Autistic profiles: explores the distinctive cognitive, emotional and behavioural traits that shape the experiences of autistic healthcare students.
(b) Theme 2 – Sensory sensitivities: explores students’ perceptions of the sensory processing differences they experience in clinical environments. It also highlights the lack of sensory accommodations and the emotional toll of masking sensory discomfort, which can exacerbate mental health difficulties.
(c) Theme 3 – Disclosure and support: addresses the factors influencing disclosure. While some students benefit from disclosure, others report discrimination or a lack of appropriate adjustments. The theme underscores systemic gaps in understanding autism within clinical education and the need for tailored, neurodiversity-affirmative support strategies.
(d) Theme 4 – Belonging and inclusion: explores how autistic healthcare students experience inclusion or indeed exclusion within clinical learning environments
These categories provide an analytical framework for mapping the existing evidence base and identifying gaps in the literature relating to autistic healthcare students’ experiences of clinical learning environments. The data pertaining to each of these themes has been summarised in the table in Appendix 1.
Discussion
Throughout the discussion, references to the six studies included in the scoping review are marked by italicised titles to distinguish them from broader literature. These studies are Shaw, Doherty, et al. (2023), Shaw, Fossi, et al. (2023), White (2024), Edwards et al. (2022), Major et al. (2024) and Conley-Reid (2022).
How Do Autistic Individuals Experience Clinical Placements?
Theme 1 – Autistic Profiles
While the medical model has historically pathologised autism, Shaw, Doherty, et al. (2023) challenge this view by discussing the rising acceptance of neurodiversity. Many autistic individuals present with a ‘spiky profile’, a pattern of uneven cognitive or functional abilities in which pronounced strengths coexist with significant challenges (Doyle, 2017; Pollak, 2009). Despite this, diagnostic criteria still centre autism as a ‘disorder’, highlighting deficits in social-emotional reciprocity and communication. White (2024) argues that this framing may contradict qualities expected of healthcare professionals, such as empathy and effective communication.
Neurodivergent scholars have criticised research portraying autistic people as lacking empathy or communication skills, suggesting such studies are methodologically flawed (Fletcher-Watson & Bird, 2019). Shaw, Doherty, et al. (2023) further explore the ‘double empathy problem’, which posits that communication breakdowns between autistic and non-autistic individuals are mutual rather than located within autistic people alone (Milton, 2012). This reframing challenges deficit-based assumptions and highlights the importance of reciprocal understanding.
Conley-Reid (2022) offers a first-person account of how autistic traits such as structured, detail-oriented thinking can function as strengths yet also invite misunderstanding in clinical education. Her experiences of being criticised for being ‘too quiet’ or ‘too structured’ illustrate how neurodivergent cognitive styles are misinterpreted within healthcare environments and how external judgement shapes identity formation.
Recent literature suggests healthcare roles may attract individuals with traits commonly associated with autism, including conscientiousness, pattern recognition and attention to detail (McCowan et al., 2021, 2022). Medical students in Shaw, Doherty, et al. (2023) reported strengths such as attention to detail, motivation to help others, organisational skills and empathy, qualities also emphasised in Major et al. (2024). Similarly, Edwards et al. (2022) include a midwifery student’s account of ‘hyper-empathy’ and ‘hyper-fixation’, which supported deep learning and clinical performance. Across these studies, autistic students consistently demonstrate motivation to use their strengths in caring roles, often persevering despite significant challenges.
However, these strengths are frequently overshadowed by social difficulties and stigma. Shaw, Doherty, et al. (2023) detail challenges such as interpreting unspoken rules and managing social anxiety, exacerbated by negative experiences with peers and supervisors. Such interactions reinforce stereotypes and contribute to internalised shame, as described by White (2024), who reflects on struggling with self-acceptance in the face of misunderstanding and judgement.
Theme 2 – Sensory Environment
Sensory challenges are well documented in the autism literature, with atypical sensory processing frequently observed among autistic individuals. Many experience the world through sensory perceptions that differ significantly from the general population, with prevalence estimates between 69% and 93% (Green et al., 2015; Horder et al., 2014; Robertson & Simmons, 2013). All six studies in this review referenced sensory-related difficulties in clinical environments.
Major et al. (2024) note that students with sensory processing differences often find clinical placements overwhelming. Edwards et al. (2022) describe ‘sensory bombardment’ in hospital settings, while Shaw, Doherty, et al. (2023) report that medical students found clinical environments ‘disorientating’, with sensory challenges compounded by social and structural stressors. Although White (2024) does not explicitly name sensory sensitivities, his deteriorating mental health during placement suggests they may have contributed. Conley-Reid (2022) provides a personal account of sensory overload in maternity care, describing busy environments leading to shutdowns and the need for stimming as a coping mechanism. Her reflection adds depth to the theme by linking sensory distress to emotional regulation and highlighting discipline-specific challenges.
Masking, or camouflaging, is closely tied to sensory overwhelm. It involves suppressing autistic traits to avoid stigma or rejection (Cook et al., 2021; Miller et al., 2021). Shaw, Doherty, et al. (2023) describe students masking to cope in chaotic environments, resulting in emotional exhaustion and withdrawal. Research likens this to draining a ‘social battery’ (Øverland et al., 2024). Conley-Reid (2022) echoes this analogy, describing masking as a ‘complex survival strategy’ that left her battery ‘well and truly empty’, while White (2024) recounts masking becoming harder when expected to socialise.
The cumulative impact of sensory overload and masking can be profound. Edwards et al. (2022) report a student being ‘pushed over the edge’ by placement experiences, and research links masking to increased mental health difficulties, including suicidality (Cassidy et al., 2020; Hull et al., 2021). These findings underscore the need for sensory-aware, neurodiversity-affirmative approaches in clinical education.
Theme 3 – Disclosure and Barriers to Support
Research indicates that autistic students often struggle to disclose their diagnosis due to past negative experiences, stigma and a perceived lack of support (Cai & Richdale, 2016). Major et al. (2024) describe how fear of discrimination in clinical placements can deter students from disclosing, even when doing so might lead to accommodations.
Across the studies reviewed, the decision to disclose varied significantly. White (2024) describes concealing his diagnosis for several years due to fear of judgement, while Shaw, Doherty, et al. (2023) found that 72% of autistic medical students who were aware of their diagnosis at entry chose not to disclose. In contrast, all participants in Shaw, Fossi, et al. (2023) had disclosed to their institutions. For some, disclosure led to positive outcomes; White (2024), for example, reported feeling supported both at university and in practice. However, others described disclosure as a risk, with students in Shaw, Fossi et al. (2023) reporting a perceived ‘weaponisation’ of their diagnosis, including being pressured to interrupt or leave their studies.
Conley-Reid (2022) discusses the impact of late diagnosis. She received excellent support from university staff post-diagnosis, but her clinical placements were marked by dismissive and stigmatising responses from midwives. She was told she was ‘too quiet’ to be a team player and warned she would ‘struggle when qualified’, comments that undermined her confidence and reinforced feelings of exclusion. Her practice supervisor downplayed her diagnosis and advised her to ‘come up with coping mechanisms’, placing the burden of adaptation solely on her. This contrast between supportive academic environments and unsupportive clinical settings highlights the inconsistency in neurodiversity-affirmative practice and the risks associated with disclosure.
The need for tailored support in clinical placements is emphasised by Major et al. (2024) and Edwards et al. (2022), both of whom advocate for adjustments that reflect individual needs. Yet, none of the students in Shaw, Doherty, et al. (2023) reported receiving personalised accommodations, and Edwards et al. (2022) describe an environment where staff lacked understanding of autistic behaviours, suggesting a broader issue of inadequate training.
Although UK legislation such as the Equality Act (2010) appear to support disclosure and reasonable adjustments, the reality is more complex. Shaw, Doherty, et al. (2023) report ongoing stigma and discrimination from supervisors and peers, and Conley-Reid (2022) similarly recounts being marginalised in placement. One student in Shaw, Fossi, et al. (2023) described being dismissed after disclosing their diagnosis, reinforcing the risk of invalidation. These accounts illustrate how disclosure can lead to stereotyping and exclusion, particularly in clinical environments where neurodivergent traits are poorly understood.
Theme 4 – Belonging and Inclusion
Belonging and inclusion are critical components of a positive educational experience, particularly for autistic healthcare students (Tan et al., 2025). A strong sense of belonging has been consistently linked to improved wellbeing, academic achievement and mental health (Kahu et al., 2022; Veldman et al., 2022). This theme explores how belonging and inclusion manifest in the experiences of autistic students within clinical learning environments.
Across the six studies reviewed, recurring language points to feelings of non-inclusion. Autistic students often feel compelled to mask their traits in clinical settings to fit in or make a good impression (Shaw, Doherty, et al., 2023). However, masking can lead to internal conflict, emotional exhaustion and burnout, as noted in Conley-Reid (2022), Major et al. (2024), Shaw, Doherty, et al. (2023) and Shaw, Fossi, et al. (2023). These harms are compounded by stigmatising behaviours, which may stem from autistic stereotyping (Shaw, Fossi, et al., 2023), unconscious bias (Major et al., 2024) or negative interpersonal experiences (Shaw, Doherty, et al., 2023). Conley-Reid (2022) captures this sense of exclusion by describing herself as a ‘square peg in a round hole’.
The concept of ‘belonging uncertainty’ (Walton & Cohen, 2007) helps explain how transitions into new academic or clinical environments, often rotational and unpredictable, can heighten anxiety and undermine a sense of inclusion. For autistic students, intolerance of uncertainty (Boulter et al., 2014; Jenkinson et al., 2020) may intensify these challenges. White (2024) describes how feelings of isolation and non-belonging coincided with poor mental health during placements, while Edwards et al. (2022) report autistic burnout and meltdowns following clinical shifts. These accounts reinforce the protective role of inclusion in supporting mental health (Gopalan et al., 2021).
Community of Practice (CoP) theory suggests that learning occurs within social groups united by shared interests (Lave & Wenger, 1991). Membership in such communities is essential for developing professional identity and competence. Yet, for autistic students, inclusion in these communities can be complex. Shaw, Doherty, et al. (2023) note that although the UK’s General Medical Council has introduced goals around equality and inclusion, these remain largely aspirational and have yet to translate into meaningful change. Participants in their study reported having their autistic identities discounted by clinical supervisors, while Major et al. (2024) describe students being questioned about their ability to qualify due to their diagnosis. Shaw, Fossi, et al. (2023) and Shaw, Doherty, et al. (2023) also document experiences of bullying and judgement from non-autistic peers, further undermining students’ sense of belonging.
Despite these challenges, some studies highlight the value of supportive communities. Shaw, Doherty, et al. (2023) found that connection with others who share lived experiences can foster belonging. However, many autistic students lack access to autistic role models or peers within their discipline. Shaw, Fossi, et al. (2023) report that students felt isolated and misunderstood, with communication difficulties often explained by the double empathy problem (Milton, 2012). Conley-Reid (2022) reflects on how social expectations in midwifery, such as being a ‘team player’, conflicted with her communication style, illustrating that belonging is not only about peer relationships but also about cultural fit within specific healthcare disciplines.
How Can More Inclusive Healthcare Education Be Developed?
Across the literature, autistic healthcare students are shown to bring valuable traits to clinical practice yet face barriers arising not from autism itself but from environments poorly adapted to neurodivergent needs. Belonging is shaped by emotional, spatial, social and structural factors (Pesonen et al., 2023). The findings align with wider neurodiversity-affirmative literature, which emphasises recognising autistic strengths and providing tailored support (Botha et al., 2020; Fletcher-Watson et al., 2019). Despite legislation such as the Equality Act (2010), disclosure often results in stigma rather than support. Clinical placements remain physically and socially inaccessible for many students, with limited sensory accommodations, inconsistent adjustments and insufficient staff training contributing to exclusion.
The six included studies highlight practical routes towards improvement. Shaw, Doherty, et al. (2023) underscore the value of autistic role models, while Shaw, Fossi, et al. (2023) show how peer networks foster self-efficacy and belonging. Although networks such as Autistic Doctors International are not universally available, identity-affirming communities play an important role (Shaw, Doherty, et al., 2023). Major et al. (2024) and Edwards et al. (2022) further outline strategies, including discipline-specific autism training and adjustments that acknowledge neurological differences.
To develop more inclusive healthcare education, institutions must:
Embed neurodiversity-affirmative practices (e.g. strengths-based approaches, sensory-aware placement planning, co-designed support plans).
Train educators and supervisors through autistic-led or autistic-informed content addressing sensory differences, masking and the double empathy problem.
Create identity-affirming networks and visible role models, such as peer mentoring or access to openly autistic clinicians.
Ensure consistent support across university and placement settings, including shared support plans and clear communication channels.
Involve autistic students in co-design, including support plans, placement-preparation resources and alternative feedback mechanisms.
Ultimately, inclusion must go beyond compliance. A cultural shift that values neurodivergent contributions and removes structural barriers is needed for autistic students to thrive.
Future Research Directions
This review highlights a limited evidence base despite a clear need for improved understanding and support. Future work should prioritise primary qualitative studies centring autistic students’ perspectives across healthcare disciplines, stages of training and outcomes such as attrition, deferral and fitness-to-practise processes. Research should also include students who have withdrawn to avoid survivorship bias. There is strong justification for participatory, co-produced approaches involving autistic students and professionals.
Further work is needed to examine clinical placement cultures, including supervisors’ understanding of autism, responses to disclosure and attitudes towards adjustments. Studies should extend beyond descriptive accounts to evaluate neuroinclusive interventions such as sensory-aware environments, structured supervision, flexible assessment and autism-specific staff training. Finally, longitudinal, intersectional and international research is required to understand the longer-term impact of clinical education on wellbeing, retention and workforce participation and how structural and policy contexts shape inclusion.
Limitations of this Review
This review is subject to several limitations. First, the small number of included studies (n = 6) restricts the breadth and generalisability of the findings. Although the search strategy was comprehensive and included grey literature, relevant studies, particularly those in non-indexed or informal formats, may have been missed. This reflects a broader underrepresentation of autistic voices in healthcare education research.
The inclusion of reflective commentaries and opinion pieces, while valuable for capturing lived experience, introduces variability in methodological rigour. These sources are anecdotal and may not reflect broader trends. While rich in insight, they are limited in scope and generalisability. All six studies were UK-based, further limiting applicability to international contexts with differing educational and cultural systems.
Two studies (Shaw, Doherty, et al., 2023, Shaw, Fossi, et al., 2023) feature prominently, which may have influenced the thematic balance. The lead author’s involvement in one included study also introduces potential bias, though steps were taken to ensure reflexivity and rigour.
Conclusion
This review highlights the complex and often underrepresented experiences of autistic healthcare students in clinical learning environments. While students demonstrated strengths such as empathy, attention to detail and professional commitment, they also faced significant barriers, often stemming not from autism itself, but from environments not designed with neurodivergent needs in mind. A key theme was the importance of belonging and inclusion. Students who felt understood and supported were more likely to thrive. However, many reported isolation, masking and a lack of neurodivergent role models. These findings underscore the need for systemic change in healthcare education to foster environments that are not only accessible but also neurodiversity-affirming. Significant gaps remain in the literature. Future studies should centre autistic voices, adopt participatory methods and explore diverse disciplines and international contexts. Ultimately, embedding inclusive values and practical support into clinical education can better enable autistic students to succeed and contribute meaningfully to the healthcare workforce.
Positionality Statement
The lead researcher is an autistic midwife and academic and brings a lived experience perspective to this study. Her personal journey through healthcare education has informed the research focus, design and interpretation of findings. She brings an insider position to the research and is uniquely positioned to identify and explore the nuanced challenges and strengths experienced by autistic healthcare students in clinical environments.
She acknowledges that her experiences are not representative of all autistic individuals and has approached the research with reflexivity and critical awareness. To mitigate potential bias, the study was conducted in collaboration with both neurodivergent and neurotypical co-authors and followed a structured methodological framework. This collaborative approach ensured that interpretations were grounded in the data and not solely shaped by personal perspective. The inclusion of neurodivergent-authored literature and the centring of autistic voices reflect her commitment to neurodiversity-affirmative research. This study aims to challenge deficit-based narratives and contribute to a more inclusive understanding of autism within healthcare education. By highlighting both barriers and strengths, the research seeks to inform practice and policy that better supports autistic students and promotes a culture of acceptance and belonging.
Footnotes
Appendix
Charting the Data.
| Title and source | Author(s) | Year of publication | Country of origin | Participant sample | Design/methods | Links to themes: (1) Autistic profiles, (2) Sensory sensitivities, (3) Disclosure and support, (4) Belonging and inclusion | Quotes from participants |
|---|---|---|---|---|---|---|---|
| ‘A square peg in a round hole’: Navigating maternity as an autistic student midwife and beyond Maternity & Midwifery Forum blog post |
Conley-Reid, H. | 2022 | UK | The author (n = 1) writes about their lived experience as an autistic midwifery student | Personal reflection from an autistic newly qualified midwife (1 month post qualification) | Theme 1: describes her autistic traits and how these traits influenced her learning style. Her logical, detail-oriented mindset aligns with strengths often seen in autistic profiles, yet she faced criticism for being ‘too structured’ or ‘too quiet’, reflecting a lack of appreciation for neurodivergent cognitive styles. Theme 2: Sensory overload was a significant challenge for the author. They recount busy environments leading to shutdowns and the need for stimming as a coping mechanism. Theme 3: The author’s late diagnosis meant they didn’t have support to begin with. Post-diagnosis, they received excellent support from university staff but encountered dismissive and harmful responses from some midwives during placements reinforcing stigma. Theme 4: The author often felt like an outsider, titling the reflection a ‘square peg in a round hole’. Social expectations in midwifery were difficult, and they were told they weren’t a ‘team player’. |
Theme 1: ‘My way of thinking is structured and logical and I would rather stick to the “script” in my head in order to ensure that I ask all of the correct questions’. Theme 2: ‘If I get overwhelmed or overstimulated, I tend to “shut down” and go inside of myself’. Theme 3: ‘When I told my practice supervisor about my diagnosis, I was told, “Well, everyone is on the spectrum really.”’ Theme 4: ‘During my third year, I was told by one midwife that I was too quiet and needed to integrate with other members of the community team more, otherwise I would not be seen as a team player’. |
| How can midwives and educators better understand, teach and support neurodivergent students? The Practising Midwife journal |
Edwards, E. Rayner, S. Porter, N. |
2022 | UK | One of the authors writes about their lived experience as an autistic midwifery student | Commentary and guidance from autistic authors including quotes from an autistic student midwife | Theme 1: A student shares how their specific neurodivergent traits enhance their academic and clinical abilities. These strengths contribute positively to their midwifery training yet are often misunderstood or undervalued in clinical settings. Theme 2: They discuss the sensory overload she experiences in hospital environments, including exposure to buzzers, shouting, smells and bright lights, which can lead to meltdowns or shutdowns. These sensory challenges are exacerbated by the fast-paced nature of clinical placements and a lack of understanding from staff. Theme 3: Disclosure is described as a complex and emotionally taxing process. The student received support from university tutors but found disclosure in clinical placements difficult, often met with misunderstanding or lack of accommodation. Theme 4: The student’s narrative reflects both the exclusion they felt due to misunderstanding and the empowerment they gained through self-awareness and supportive academic relationships. |
Theme 1: ‘I am hyper-empathetic and I hyper-fixate, which means I can learn about subjects in depth’. Theme 2: ‘Add to this the constant sensory bombardment in a hospital . . . sometimes I am pushed over the edge and shut down’. Theme 3: ‘Whilst my tutors are aware and supportive, disclosure in placement can be difficult’. Theme 4: It’s difficult for supervisors to understand this or accommodate me when I need to get away . . . I’ll take a seat to calm down if I need it, but staff can’t always comprehend this as a coping skill rather than laziness’. |
| Supporting neurodivergent nursing students in their practice placements Nursing Standard |
Major, R. Jackson, C. Wareham, J. Pidcock, J. |
2024 | UK | General population of neurodivergent nursing students including autistic students. The article is written in the third person and summarises the experiences of multiple neurodivergent students. N number of participants not stated | Commentary and guidance from multiple neurodivergent authors including autistic students | Theme 1: The article presents a nuanced view of autistic strengths and challenges. Strengths are framed as assets in nursing practice, particularly in tasks requiring precision and adherence to protocols. However, challenges such as literal thinking, difficulty interpreting social cues and anxiety are acknowledged. Theme 2: The authors describe how sensory overload can lead to shutdowns or distress. A case example illustrates an autistic student struggling with the tactile sensations of surgical attire. Theme 3: Disclosure is framed as a highly personal and complex decision, often influenced by past experiences of stigma or discrimination. The authors note that some students may be undiagnosed or in the process of seeking diagnosis and may not feel safe to disclose. Theme 4: The authors advocate for a neuroinclusive environment to foster belonging and make useful recommendations to support this |
N/A |
| The experiences of autistic doctors: a cross-sectional study Frontiers in Psychiatry |
Shaw, S. Fossi, A. Carravallah, L. Rabenstein, K. Ross, W. Doherty, M. |
2023 | UK | Autistic doctors (n = 225), members of Autistic Doctors International using a survey partially designed to examine their experience in medical school | A participatory approach was used to identify the need for the project and to modify a pre-existing survey for use exploring the experiences of autistic doctors. This is a cross-sectional study in the form of an online survey using a mixture of open and closed questions. 32 core questions with additional questions contingent on participant responses (121 possible questions). |
Theme 1: Many participants did not suspect they were autistic until after medical school (74%), with only 11% identifying as autistic during their student years. Those who did suspect or know they were autistic during medical school often faced internalised ableism, shaped by stereotypes and a lack of representation. A quarter of respondents (25%) reported that medical school took longer to complete, and 89% of those attributed this to being autistic, suggesting that their neurodivergent profiles impacted their ability to navigate the demands of clinical education. Theme 2: Although not detailed extensively in the medical school context, the study found that 75% of respondents experienced sensory challenges in clinical environments. These challenges likely began during placements, where overstimulation from noise, lighting and physical discomfort (e.g., surgical attire) could contribute to distress and shutdowns. Theme 3: Of the small group who knew they were autistic during medical school, 72% did not disclose their diagnosis. Among those who did disclose, only 53% received adjustments, indicating a significant gap in institutional support. Fear of stigma and disbelief (e.g., ‘a qualified doctor couldn’t be autistic’) discouraged disclosure and reinforced a culture of masking and silence. Theme 4: The study highlights a lack of autistic role models and peer support during medical training, contributing to feelings of isolation. Many students felt unable to be their authentic selves, leading to masking. The absence of visible autistic peers or mentors during training was statistically associated with increased suicidal ideation. |
N/A |
| The experiences of autistic medical students: A phenomenological study Medical Education |
Shaw, S. Doherty, M Anderson, J. |
2023 | UK | Autistic medical students (n = 5) from different UK medical schools recruited through purposive sampling | Uses interpretive phenomenological analysis (IPA) to understand student experience through loosely structured interviews. An interview guide was used covering the following topics: 1. Experiences of diagnosis 2. Personal autistic profiles 3. Experiences getting into medical school 4. University-based experiences 5. Clinical experiences. |
Theme 1: Participants described strengths such as heightened empathy, attention to detail and strong patient communication skills. Interestingly, several students felt more comfortable interacting with patients than with peers or staff, due to the structured nature of clinical roles. However, these strengths were often discounted or misunderstood by educators, who held stereotypical views of autism (e.g., ‘you don’t look autistic’). Theme 2: Clinical environments were described as overwhelming and chaotic, with multiple sensory triggers interfering with learning. The lack of sensory accommodations in clinical settings significantly impacted their ability to engage and learn. Theme 3: All participants had disclosed their autism to their medical schools, but none received personalised reasonable adjustments (RAs). Instead, they were offered generic disability accommodations, which were often inappropriate or even counterproductive. Requests for tailored support were frequently dismissed, even when backed by medical documentation. In some cases, students were pressured to take time out or faced threats of exclusion rather than being supported to continue with adjustments. Theme 4: Students reported bullying, isolation and a lack of peer support during placements. The competitive nature of medical education exacerbated feelings of exclusion. One participant described peers as ‘predator-like’, while another felt constantly ‘watching their back’. Discovering autistic peer networks (e.g., Autistic Med Students group) offered a sense of community and validation. The presence of autistic role models among staff also provided reassurance and a sense of possibility. |
Theme 1: ‘I’m a lot better with patients than I am with my peers, with staff, which is hard for a lot of people to understand’. (Maddie) Theme 2: ‘I find it kind of chaotic . . . It’s very disorientating and unstructured’ (Adam). Theme 3: ‘They had a review from an occupational health doctor who was like, “I think this student is fit to continue fifth year as long as you adjust the placements.”’ And then they came up with, ‘well, we’re not sure, we are going to exclude you’ (Grace). Theme 4: ‘I’m constantly in my head trying to make a good impression . . . putting on a face’. (Emma) |
| Neurodiversity & nursing: Reflection of a final year general nursing student Nurse Education Today |
White, J. | 2024 | UK | The author (n = 1) writes about their lived experience as an autistic nursing student | Personal reflection from an autistic final-year nursing student | Theme 1: The nursing student reflects on how traits associated with autism have positively contributed to their nursing practice. Despite societal assumptions that autism may be incompatible with the compassion required in nursing, they found their neurodivergent profile enhanced his ability to deliver care. They challenge stereotypes that frame autism as a deficit, arguing instead for a strengths-based perspective. Theme 2: While not extensively detailed, White describes moments of sensory and emotional overwhelm during clinical placements, including a severe panic attack on the ward that led to an abrupt departure. Theme 3: Initially, the student chose not to disclose their diagnosis during occupational health screening due to shame and fear of stigma. They masked their autism leading to feelings of isolation and non-belonging. It wasn’t until after deferring a year due to mental health struggles that they made the disclosure. Post-disclosure, they received positive support from academic and clinical staff, including pre-placement meetings and access to quiet spaces. Theme 4: This narrative reveals a journey from concealment and shame to acceptance and inclusion. Disclosure allowed him to be more honest with peers and staff, which in turn fostered self-acceptance |
Theme 1: ‘Perhaps the attention to detail, observational and analytical skills that may have arisen from being autistic have contributed to where I find myself today?’ Theme 3: ‘Shame and fear heavily influenced my decision [to disclose]. . . it was not until I suffered a severe panic attack on the ward . . . that I had to act’. Theme 4: ‘Socially, however, I did struggle immensely with feelings of isolation and non-belonging’. |
Ethical Considerations
None required
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.