
Abstract
Research suggests autistic people experience greater post-traumatic stress disorder symptom severity than non-autistic people following traumatic events. Post-trauma appraisals are fundamental in cognitive models of post-traumatic stress disorder, but have not been explored in autistic people. We aimed to explore whether we could replicate effects of heightened trauma exposure and post-traumatic stress disorder symptom severity in autistic adults, and examine how post-traumatic appraisals affect the association between autism and post-traumatic stress disorder symptom severity. Two hundred forty-two autistic (n = 148) and non-autistic adults (n = 94) completed a survey measuring trauma exposure, post-traumatic stress disorder symptom severity and post-trauma appraisals. Exposure to types of traumatic events did not differ significantly between the groups, but the autistic group endorsed more events that ‘happened to me’ directly. Post-traumatic stress disorder symptom severity and endorsement of negative post-traumatic appraisals were significantly higher in the autistic group, specifically alienation, shame and fear appraisals. These appraisals mediated the association between autism and post-traumatic stress disorder symptom severity. Therefore, as in the general population, greater endorsement of negative post-traumatic appraisals may be a risk factor for post-traumatic stress disorder symptom development in autistic adults, particularly appraisals of shame, fear and alienation. Longitudinal designs are required to confirm the direction of these effects and to elucidate factors underlying these negative appraisals in autistic people.
Lay Summary
Many people experience intrusive memories and anxiety after a traumatic event. However, for some, these symptoms last longer and they might be diagnosed with post-traumatic stress disorder. Research suggests that autistic people might be more likely to develop post-traumatic stress disorder and experience more severe symptoms compared to non-autistic people after traumatic events. One factor that is important in post-traumatic stress disorder development is how people think about the trauma. These might be thoughts like ‘It was my fault’, ‘I’m not safe’, ‘I’m disconnected from other people’. There has not been research into how autistic people think about traumatic events compared to non-autistic people, and this could be important for making post-traumatic stress disorder treatments more effective for them, as many of these focus on thoughts. In this study, we asked 148 autistic people and 94 non-autistic people in the United Kingdom to complete an online survey about their trauma history, post-traumatic stress disorder symptoms and thoughts about a traumatic event. We found that autistic people experienced more types of traumatic events directly (it happened to them), but they did not experience more types of traumatic events overall. Interestingly, both groups reported events like bullying or the death of a loved one as traumatic, but these events would not meet the official diagnostic criteria for post-traumatic stress disorder. As expected, autistic people reported worse post-traumatic stress disorder symptoms than non-autistic people and were more likely to meet the cut-off for post-traumatic stress disorder diagnosis. Autistic people also reported more negative thoughts about the trauma, especially feeling unsafe, disconnected, ashamed or that the trauma was their fault. Having more thoughts like this was associated with being autistic and experiencing more severe post-traumatic stress disorder symptoms. Our findings suggest that therapies focusing on these negative thoughts could be helpful for autistic people with post-traumatic stress disorder. Future research should explore why autistic people have more of these thoughts after traumatic events and should use longitudinal or experimental designs to explore how these factors influence one another over time. Efforts to prevent negative experiences, challenge negative attitudes in society towards autism and support positive autistic identity and well-being will be helpful for changing this in the future. It is also important that mental health services offer support for post-traumatic stress disorder even when events do not meet the current diagnostic criteria, as this might prevent autistic and non-autistic people who need support with post-traumatic stress disorder getting help.
Post-traumatic stress disorder (PTSD) can occur following exposure to traumatic events, defined as events involving actual or threatened serious injury, death or sexual violence (PTSD Criterion-A; American Psychiatric Association (APA), 2013). PTSD is characterised by intrusive recollections and re-experiencing of trauma, avoidance of stimuli that are reminders of the event, hyperarousal and negative changes in mood and cognitions (APA, 2013). Many people experience these symptoms in the immediate aftermath of traumatic events, but for some, these persist for over a month and therefore constitute a diagnosis of PTSD. Lifetime prevalence of PTSD has been estimated at 8.9% for trauma-exposed adults (McManus et al., 2009).
Cognitive models of PTSD propose that PTSD occurs if individuals process traumatic events in ways that make the threat seem ‘current’ (Brewin et al., 1996; Ehlers & Clark, 2000). Two features are thought to cause and maintain this sense of current threat: (1) excessively negative appraisals about the trauma and/or its consequences, and (2) the nature of the trauma memories. Characteristics of traumatic events, cognitive processing during the trauma and prior traumatic experiences are suggested to influence the nature of appraisals and trauma memories. Strategies intended to reduce the perceived threat, like thought suppression, rumination, safety-seeking behaviours and avoidance, then maintain difficulties by inadvertently preventing change in appraisals or updating of trauma memories.
Much research in support of these models has focused on the general population. However, recent reviews suggest that prevalence of PTSD in autistic adults exposed to trauma may exceed that in the non-autistic general population, and they may develop PTSD symptoms with greater severity (Quinton et al., 2024). Autism is a neurodevelopmental difference, characterised by differences in social communication and interaction, sensory processing as well as restricted and repetitive interests and behaviours (APA, 2013). Approximately 0.82% of people in England are diagnosed autistic (O’Nions et al., 2023), although it is likely that autism is underdiagnosed, with an estimated true prevalence of 0.77%–2.12% (Huang et al., 2020; O’Nions et al., 2023). Rates of diagnosis of autism are higher among men, with an estimated 2.1:1 men-to-women ratio globally (Santomauro et al., 2025). Studies using self-report measures of PTSD symptoms have found that 32%–45% of trauma-exposed autistic adults exceeded cut-off scores for possible PTSD, significantly higher than non-autistic comparison groups (4%–4.5%; Haruvi-Lamdan et al., 2020; Rumball et al., 2020). PTSD symptom severity (PTSD-SS) is also consistently higher among autistic adults (Golan et al., 2022; Haruvi-Lamdan et al., 2019; Rumball, Brook, et al., 2021). However, in contrast, a recent systematic review and meta-analysis by Mansour and colleagues (2025) which pooled prevalence rates of PTSD using gold-standard diagnostic assessments reported that point and lifetime prevalence among autistic adults (2.06% and 2.72%, respectively) was comparable to rates in the general population. Given PTSD’s substantial impact on quality of life (Balayan et al., 2014), understanding reasons for autistic people’s possible heightened vulnerability and identifying intervention targets is essential.
One theory for increased PTSD-SS in autistic adults is that socio-communicative differences may render autistic people more vulnerable to victimisation (Haruvi-Lamdan et al., 2018; Kerns et al., 2015), increasing frequency of trauma exposure. Indeed, autistic people report greater trauma exposure compared to their non-autistic peers (Berg et al., 2016; Hartley et al., 2024; Haruvi-Lamdan et al., 2020; Rumball, Brook, et al., 2021), particularly physical and sexual abuse (Dike et al., 2022; Mandell et al., 2005) and maltreatment (McDonnell et al., 2019). This has also been observed in people with more autistic traits (Roberts et al., 2015; Stewart et al., 2021). In the general population, exposure to multiple traumas cumulatively increases risk of developing PTSD (Breslau et al., 1999) and PTSD-SS (Suliman et al., 2009), especially for traumas involving others (hereafter ‘interpersonal traumas’; Briere et al., 2016). In line with this, Rumball, Brook, et al. (2021) demonstrated that cumulative trauma exposure was associated with increased PTSD-SS in autistic adults. Consequently, exposure to multiple traumas may increase likelihood of autistic people developing PTSD symptoms, through their influence on the nature of trauma memories and post-traumatic appraisals.
In addition, research suggests that autistic individuals may subjectively experience a wider range of events as traumatic, including those not meeting DSM-5 Criterion-A, potentially increasing trauma exposure (Brewin et al., 2019; Haruvi-Lamdan et al., 2018; Kerns et al., 2015). Defining what constitutes a traumatic event is subject to debate (Weathers & Keane, 2007), and it is increasingly recognised that events which do not meet Criterion-A can result in PTSD symptoms (Brewin et al., 2019; Danese & Widom, 2020). Among autistic people, Rumball et al. (2020) found that experiences including social misperceptions, bullying and aversive sensory experiences were reported as ‘extremely unpleasant, stressful or traumatic’ and were associated with PTSD symptomatology as often as Criterion-A events. Furthermore, Haruvi-Lamdan et al. (2020) found that autistic adults were more likely than non-autistic adults to identify non-Criterion-A social experiences like bullying as most distressing, and only in the autistic group were these events significantly associated with PTSD-SS. Such experiences, like bullying (Cappadocia et al., 2011; Maïano et al., 2016; Van Roekel et al., 2010; Zeedyk et al., 2014), ostracisation and peer rejection (Chen & Schwartz, 2012; Paul et al., 2018) and sensory overload (Mandell et al., 2005), are more common for autistic people. The accumulation of both Criterion-A and non-Criterion-A experiences may significantly impact PTSD-SS; thus, adopting an inclusive definition of trauma is recommended when researching PTSD-SS in autistic people (Quinton et al., 2024). Indeed, in Mansour et al.’s (2025) meta-analysis which found comparable rates of PTSD in autistic compared to non-autistic population, they highlighted that their use of established diagnostic criteria may not capture the actual rates of post-traumatic symptoms or experiences within autistic populations, especially given that they overlook non-Criterion-A traumas (Mansour et al., 2025).
Alongside trauma exposure, cognitive models of PTSD (Brewin et al., 1996; Ehlers & Clark, 2000) emphasise the importance of peri-trauma factors like sensory and detail-focused processing, and post-trauma factors including memory and strategies to control perceived threat. Accordingly, differences in sensation, perception, detail-focused processing, memory and cognition associated with autism may influence the subjective experience of events as traumatic, and underpin susceptibility to PTSD symptoms and their maintenance (Brewin et al., 2019; Haruvi-Lamdan et al., 2018; Hoover, 2015; Kerns et al., 2015). Many of these factors are beginning to be investigated, with tendency towards ruminative thinking (Amatori et al., 2024; Golan et al., 2022), thought suppression (Rumball, Antal, et al., 2021), sensory hypersensitivity (Amatori et al., 2024) and memory differences (Rumball, Brook, et al., 2021) being implicated as mediators in the relationship between autism and PTSD-SS.
Despite increasing research into how PTSD-SS in autism might be understood through cognitive models, differences in negative post-traumatic in autistic adults remain unexplored. In the general population, negative post-traumatic appraisals are risk factors for PTSD (Gómez de La Cuesta et al., 2019). They are positively associated with PTSD-SS (DePrince et al., 2011; Duffy et al., 2013) and can prospectively predict PTSD-SS (Halligan et al., 2003). These effects persist even when accounting for frequency of trauma exposure (Andrews et al., 2000). Appraisals of fear, alienation, anger, betrayal, shame and self-blame mediate the relationship between childhood trauma, cumulative trauma and PTSD-SS, with alienation appraisals particularly emphasised (DePrince et al., 2011; McIlveen et al., 2022; Mitchell et al., 2020).
Appraisals are influenced by prior life experiences. We have highlighted that autistic people experience more traumatic events, especially victimisation by others which may or may not meet Criterion-A. Autistic people also experience high levels of stigma (Botha et al., 2022; Botha & Frost, 2018). Experiences of stigma, bullying and ostracisation may understandably result in autistic people feeling alienated, illustrated by qualitative reports that negative social experiences make autistic people feel ‘different’ in a negative way (for review see Williams et al., 2019). Internalisation of negative social experiences and stigma has been found to result in negative self-concepts that contribute to poorer mental health (Botha & Frost, 2018; Cooper et al., 2017). This may also increase the salience of negative appraisals following traumatic events, especially appraisals like self-blame, shame and alienation which are particularly associated with interpersonal traumas in the general population (Beierl et al., 2020; Moor & Farchi, 2011). Increased salience and endorsement of negative post-traumatic appraisals may contribute to the increased PTSD-SS observed in autistic people.
Given the theoretical importance of negative post-traumatic appraisals, and the focus on modification of appraisals in PTSD treatment (Gómez de La Cuesta et al., 2019; Jensen et al., 2018; Kleim et al., 2013), examining whether endorsement of appraisals differs between autistic and non-autistic trauma-exposed adults, and to what extent these mediate the relationship between autism and PTSD-SS, is important to further our understanding of differences which contribute to increased PTSD-SS in this group.
This study set out to evaluate whether self-reported trauma exposure, exposure to additional non-criterion-A traumas and PTSD-SS in response to a traumatic event was higher in autistic compared to non-autistic adults, in line with previous findings. We planned to review differences in the types of traumatic events reported. We then aimed to investigate how negative post-traumatic appraisals affect the association between autism and PTSD-SS. We hypothesised that
Method
Design
An online survey with a cross-sectional between-groups design was employed. The dependent variable was PTSD-SS. The independent variable was self-reporting being autistic or not (with the majority of the autistic group also reporting a formal diagnosis). Negative post-traumatic appraisals were investigated as possible mediators. This study was approved by the University of Oxford Medical Sciences ethics committee (R84859/RE001).
Participants
Participants were recruited through social media, autism charities and support groups through a study advert which asked ‘have you experienced an event in your life which you found traumatic?’ Participants were required to live in the United Kingdom, be aged ⩾ 18, report experiencing one or more events which they found ‘highly stressful or traumatic’, read and understand English, and not self-report diagnosis of an intellectual disability. No compensation was offered for participation.
Given the survey nature of the study, to check data validity and reduce the likelihood of automated responses, a CAPTCHA was included at the start of the survey, and response data were screened for unusually fast completion times combined with atypical or patterned responses and unusual free text responses. There was no compensation for participation. One response was excluded due to unusually fast response time and selection of the first option for every question. Two hundred forty-two people took part.
Participants were allocated to the autistic or non-autistic group according to self-report: 148 autistic and 94 non-autistic. For those who self-reported that they were autistic, they were asked to specify whether they had been formally diagnosed (121), were awaiting a diagnostic assessment (8) or self-identified as autistic (19). All participants completed the AQ (Autism Quotient; Baron-Cohen et al., 2001). Mann–Whitney U tests were run, which showed that there were not significant differences in AQ scores between autistic individuals who had a formal diagnosis, those who self-identified (U = 1072.0, z = 0.47, p = 0.637), and between those who had a formal diagnosis and those awaiting diagnosis (U = 391.0, z = 0.91, p = 0.363). The autistic group scored significantly higher on the AQ than the non-autistic group (p < 0.001; Table 1), and 86.5% of the autistic group scored ⩾ 32 on the AQ compared to 14.9% of the non-autistic group. This is in line with Baron-Cohen et al. (2001) expected rates for autistic individuals but above the expected rate of 2.0% for non-autistic individuals. Analyses were therefore run with and without those whose AQ score did not match their self-reported group; however, this did not qualitatively affect findings. All participants were therefore retained in their self-reported group. Table 1 presents demographic characteristics.
Demographic characteristics of the autistic (N = 148) and non-autistic (N = 94) groups.
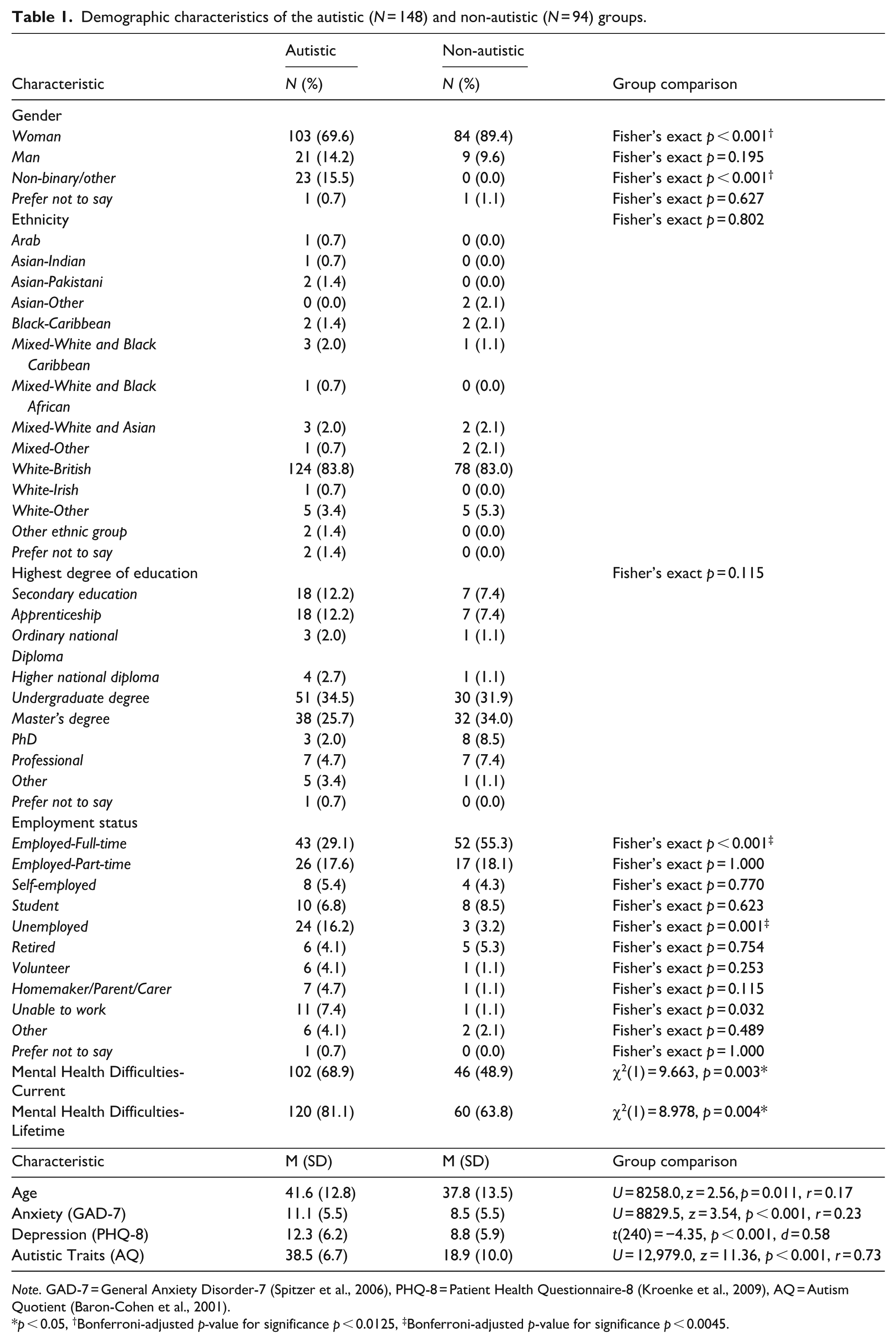
Note. GAD-7 = General Anxiety Disorder-7 (Spitzer et al., 2006), PHQ-8 = Patient Health Questionnaire-8 (Kroenke et al., 2009), AQ = Autism Quotient (Baron-Cohen et al., 2001).
p < 0.05, †Bonferroni-adjusted p-value for significance p < 0.0125, ‡Bonferroni-adjusted p-value for significance p < 0.0045.
Our minimum sample size (53 per group for Model 1, and 77 per group for Model 2) was determined using an a priori power analysis conducted in G*Power. This was based on a linear multiple regression model with two predictors in Model 1 and seven predictors in Model 2, assuming a medium effect size of autism group and overall post-trauma appraisals on PTSD-SS (f = 0.15), α = 0.05, 95% power and a two-tailed test.
Procedure and measures
Following confirmation of eligibility and informed consent, participants completed the survey via Qualtrics, beginning with a demographics form, then questionnaires in the order shown below, ending with a debrief. Signposting to support was available throughout the survey.
Trauma exposure
Life Events Checklist (LEC-5; Weathers, Blake, et al., 2013)
This is a 17-item measure of exposure to Criterion-A traumatic events, in which respondents report whether 16 types of traumatic events ‘happened to me’, were ‘witnessed’, ‘learnt about it’ happening to someone close to them, happened as ‘part of my job’ or ‘does not apply’. This measure is used extensively in PTSD research studies with neurotypical participants and has been shown to have good test re-test reliability (r = 0.82; Gray et al., 2004). Trauma exposure was calculated by summing the number of different traumatic event types endorsed in any way (i.e. happened to me, witnessed it, learnt about it, part of my job) by each participant, meaning a maximum score of 16. Trauma types endorsed as ‘happened to me’ were also summed separately, with a maximum score of 16 directly experienced traumatic event types. It should be noted that these scores do not reflect frequency of exposure. Item 17, which allows for ‘other’ traumatic events to be self-reported, was explored separately under the ‘non-Criterion-A Traumas’ section. If respondents self-reported ‘other’ traumatic events that met Criterion-A and therefore would have been captured by the LEC-5 traumatic event types, these were not counted as non-Criterion-A traumas.
Non-Criterion-A Traumas (based on Rumball, Brook, et al. (2021))
Participants were asked whether any other event had happened to them which ‘has felt like an extremely unpleasant, stressful or traumatic experience’, or ‘has caused you to have nightmares about it or think about it when you did not want to’, or ‘you have subsequently tried hard not to think about or go out or your way to avoid situations that remind you of it’. If affirmative to any of the above questions, the individual was asked to briefly detail the nature of the event(s). Participants were not explicitly instructed to report all the events that they had experienced that they found traumatic but were not covered by the LEC-5; thus, frequency of non-Criterion-A events cannot be reported. Qualitative descriptions were assessed by two clinicians and coded as meeting Criterion-A or not based on DSM-5 criteria (APA, 2013).
If participants reported more than one event which they found traumatic across the LEC-5 and/or non-Criterion-A events, they were asked to identify the event that caused them the most distress currently and complete measures in relation to this.
PTSD-SS
Post-Traumatic Stress Disorder Checklist for DSM-5 (Weathers, Litz, et al., 2013)
This 20-item measure assesses the severity of current PTSD symptoms according to DSM-5 criteria, with regard to the last month. Questions are answered on a 5-point Likert-type scale of 0 (‘not at all’) to 4 (‘extremely’). Scores range from 0 to 80. Higher scores indicate greater PTSD-SS, and a score of ⩾ 33 may indicate possible clinically significant PTSD symptoms (Blevins et al., 2015). This measure has been found to have excellent internal consistency in autistic (α = 0.94; Haruvi-Lamdan et al., 2020) and non-autistic adults (α = 0.94; Blevins et al., 2015). In the current sample, internal consistency was also excellent (α = 0.94; ω = 0.93).
Participants were then asked if there had been any time period since the trauma where they were a lot more troubled by the symptoms that they had just been asked about, than they were in the past month. If yes, and the symptoms lasted for more than 1 month, they were asked to complete another Post-Traumatic Stress Disorder Checklist for DSM-5 (PCL-5) in relation to that period of time. This is in line with previous use of the PCL-5 to explore lifetime PTSD-SS, as described by Rumball et al. (2020). In the current sample, internal consistency was excellent (α = 0.90; ω = 0.90).
Negative post-traumatic appraisals
Trauma Appraisals Questionnaire (DePrince et al., 2010)
This is a 54-item measure of negative post-traumatic appraisals, with six subscales assessing fear, alienation, anger, betrayal, shame and self-blame appraisals. Participants are asked to rate items on a 5-point Likert-type scale ranging from ‘strongly agree’ to ‘strongly disagree’ in relation to how they feel now when they think about the traumatic event that occurred. It includes items such as ‘I am disconnected from people’, ‘I was responsible for what happened’, ‘I felt humiliated’, ‘I am not safe’. Scores range from 54 to 270, with higher scores indicating greater endorsement of negative post-traumatic appraisals. This measure has been found to have excellent internal consistency (α = 0.84–0.93; DePrince et al., 2010) and good test–retest reliability (r = 0.73–0.88) in non-autistic adults. In the current sample, internal consistency was also excellent for the total score (α = 0.96; ω = 0.95) and was also strong at the subscale level (betrayal α = 0.91; ω = 0.90; self-blame α = 0.94; ω = 0.94; fear α = 0.91; ω = 0.91; alienation α = 0.90; ω = 0.90; anger α = 0.85; ω = 0.85; shame α = 0.89; ω = 0.89).
Anxiety and depression
General Anxiety Disorder-7 (Spitzer et al., 2006)
This 7-item measure assesses symptoms of anxiety. Items are rated on a 4-point Likert-type scale ranging from 0 (‘not at all’) to 3 (‘nearly every day’). Scores range from 0 to 21, with higher scores indicating more severe anxiety symptoms. This measure has shown excellent internal consistency (α = 0.90) and good test–retest reliability (r = 0.83) in non-autistic people (Spitzer et al., 2006), and good internal consistency and construct validity in autistic people (Robeson et al., 2024). In the current sample, internal consistency was good (α = 0.89; ω = 0.89).
Patient Health Questionnaire-8 (Kroenke & Spitzer, 2002)
This 8-item measure assesses symptoms of depression. Items are rated on a 4-point Likert-type scale ranging from 0 (‘not at all’) to 3 (‘nearly every day’). Scores range from 0 to 24, with higher scores indicating more severe depressive symptoms. This measure has shown excellent internal consistency and test–retest reliability in non-autistic people (Kroenke et al., 2010; Kroenke et al., 2009), and good internal consistency and construct validity in autistic people (Robeson et al., 2024). In the current sample, internal consistency was also good (α = 0.89; ω = 0.89).
Autistic traits
AQ (Baron-Cohen et al., 2001)
This 50-item measure assesses the presence of autistic traits. Questions are answered on a 4-point Likert-type scale ranging from ‘strongly agree’ to ‘strongly disagree’. Higher scores indicate higher presence of autistic traits. It is not a diagnostic measure; however, 80% of autistic people score ⩾32 compared to just 2% of controls (Baron-Cohen et al., 2001), and this cut-off is highly predictive of autism diagnosis (Ruzich et al., 2015). The AQ has good test–retest reliability (Baron-Cohen et al., 2001) and moderate-strong internal consistency in autistic (α = 0.81; Wakabayashi et al., 2006) and non-autistic samples (α = 0.67; Hurst et al., 2007). In the current sample, internal consistency was excellent (α = 0.95; ω = 0.95).
Participatory methods
Three experts-by-experience who are autistic and/or had PTSD were consulted prior to seeking ethical approval. Their guidance was sought about choice of outcome measures, and how these were explained, as well as ways to reduce the burden of the survey on respondents. They reviewed all study materials and were invited to make changes to wording and structure throughout. They also provided suggestions for improvements to signposting throughout the study. They were paid for their time spent independently reviewing materials and time discussing these with the researchers.
Analysis
Descriptions of ‘worst’ traumatic events were examined independently by two clinicians to determine whether they met Criterion-A (coded ‘Criterion-A’ or ‘non-Criterion-A’, according to DSM-5 criteria (APA, 2013)) and whether they were interpersonal (traumatic because of the actions or words of another person or people) or not. Coding criteria are provided in Appendix 1.
Statistical analysis was conducted using SPSS version 28 (IBM Corp., 2021). Frequencies, chi-square and t-tests (or non-parametric equivalents) were used to compare the groups on trauma exposure, PTSD-SS and negative post-traumatic appraisals. Bivariate Pearson’s correlations (and point-biserial correlations for autism group) were conducted among primary study variables to summarise the strength and direction of their associations across the full sample. Mediation models using PROCESS for SPSS (Hayes, 2012) were used to assess the role of appraisals in the association between autism and PTSD-SS. Model 1 had a single mediator (Trauma Appraisals Questionnaire (TAQ) total), with autism group as a binary predictor variable and PTSD symptoms as the outcome variable. In Model 2, TAQ subscales were included as mediators, permitting the calculation of the indirect effect of each appraisal type while others were controlled. Five thousand bias-corrected bootstrap samples were used to generate 95% confidence intervals (CIs) and point estimates for indirect effects.
For group comparisons, variables were tested for normality, variance homogeneity and outliers to determine appropriate analyses. For mediation models, residuals met assumptions of normality, homoscedasticity and linearity, and there were no problems with multicollinearity. Outliers were assessed within the autistic and non-autistic groups separately as recommended by Sullivan et al. (2021), identifying three outliers in studentised deleted residuals in Model 1, and four in Model 2, but none with high leverage based on Mahalanobis distance, so these were retained.
Results
Descriptive statistics
The autistic and non-autistic groups differed significantly by age (p = 0.011) and in the proportion of the autistic group who identified as women or non-binary compared to the non-autistic group (Fisher’s exact p < 0.001), as shown in Table 1. Differences in the proportions of each group identifying as men were not significant. The autistic and non-autistic groups differed significantly in the proportion of each group describing themselves as employed full-time (Fisher’s exact p < 0.001) and unemployed (Fisher’s exact p = 0.001) but not in other employment types. The groups also differed significantly in the proportion of each group reporting current (p = 0.003) and lifetime (p = 0.004) diagnoses of mental health difficulties. The multinomial probability distributions were equal between the two groups for ethnicity (p = 0.802) and highest degree of education (p = 0.115).
Age was not associated with PTSD-SS or TAQ score in the autistic (r = 0.13, p = 0.117; r = 0.02, p = 0.822) or non-autistic group (r = 0.06, p = 0.549; r = 0.01, p = 0.945). The three-level variable for gender (man, woman, non-binary/other) also did not predict PTSD-SS or TAQ in the autistic (F(2, 146) = 0.05, p = 0.948; F(2, 146) = 1.29, p = 0.280) or non-autistic group (F(1, 92) = 2.95, p = 0.089; F(1, 92) = 1.15, p = 0.286). As age and gender were not related to these key outcome variables, they were not controlled for in our main analyses.
Trauma exposure
The number of Criterion-A traumatic life event types exposed to overall, as categorised and measured by the LEC-5 (see method ‘Trauma Exposure’ section), did not differ significantly between the autistic and non-autistic group. However, the number of event types exposed to directly (‘happened to me’) was significantly higher in the autistic group (p = 0.002; Table 2).
Descriptive statistics and effect sizes for group differences in Criterion-A trauma exposure, PTSD-SS and appraisals.
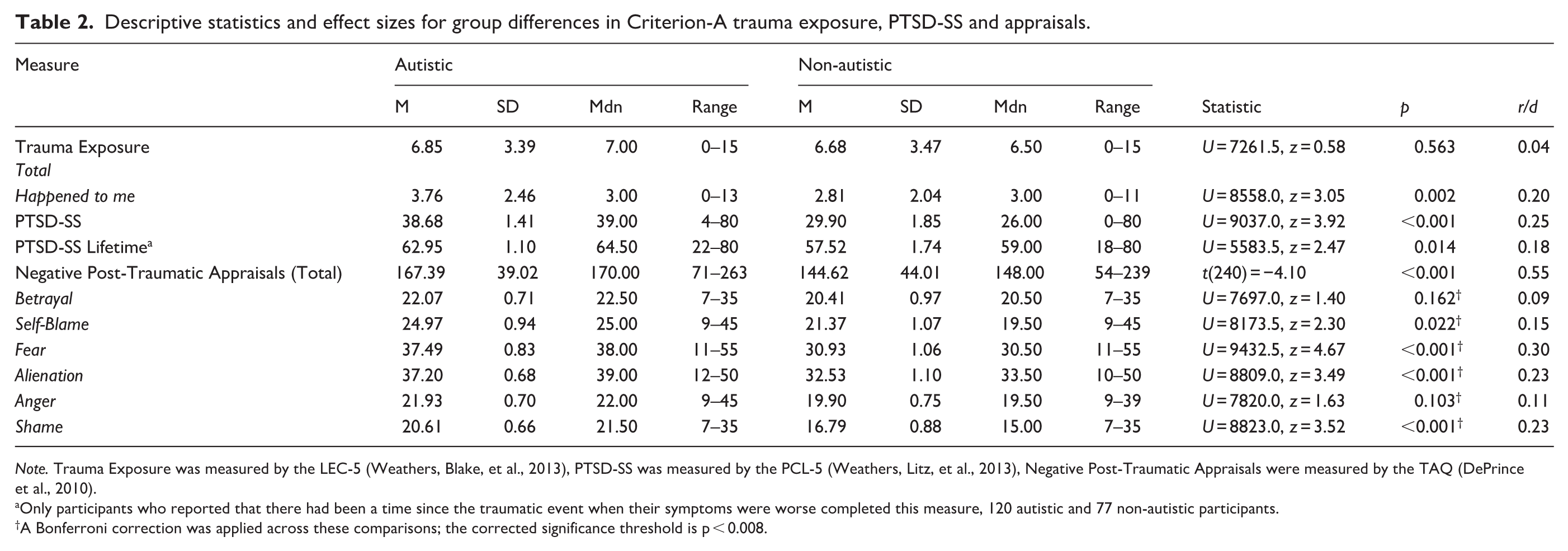
Note. Trauma Exposure was measured by the LEC-5 (Weathers, Blake, et al., 2013), PTSD-SS was measured by the PCL-5 (Weathers, Litz, et al., 2013), Negative Post-Traumatic Appraisals were measured by the TAQ (DePrince et al., 2010).
Only participants who reported that there had been a time since the traumatic event when their symptoms were worse completed this measure, 120 autistic and 77 non-autistic participants.
A Bonferroni correction was applied across these comparisons; the corrected significance threshold is p < 0.008.
One hundred three autistic (69.6%) and 61 non-autistic participants (64.9%) reported experiencing ‘other’ traumatic events which did not meet Criterion-A. This difference was not statistically significant (p = 0.491). A further four participants (two per group) reported experiencing ‘other’ traumatic events but provided no details so could not be coded.
PTSD-SS
Current PTSD-SS was significantly higher in the autistic group (p < 0.001; Table 2). A significantly greater proportion of the autistic group (62.8%), compared to the non-autistic group (40.4%), reached the cut-off for current probable PTSD on the PCL-5 (p < 0.001).
Of participants who reported that there had been a time since the trauma where their symptoms were worse, lifetime PTSD-SS was significantly higher in the autistic group (n = 120) than the non-autistic group (n = 77; p = 0.014; Table 2). Of the autistic group, 79.7% crossed the cut-off for probable PTSD in their lifetime compared to 76.6% of the non-autistic group. This difference was not statistically significant (p = 0.074).
Nature of traumas endorsed
Similar proportions of the autistic (43.2%) and non-autistic group (37.2%) identified non-Criterion-A traumas as their ‘worst’ event (p = 0.389), and reported a ‘worst’ traumatic life event which was coded as ‘interpersonal’ (autistic 54.1%, non-autistic 53.2%; p = 0.813). Removal of traumas which were ‘uncertain’ to code did not affect these findings. Details of the nature of the ‘worst’ trauma by group are available in Appendix 2.
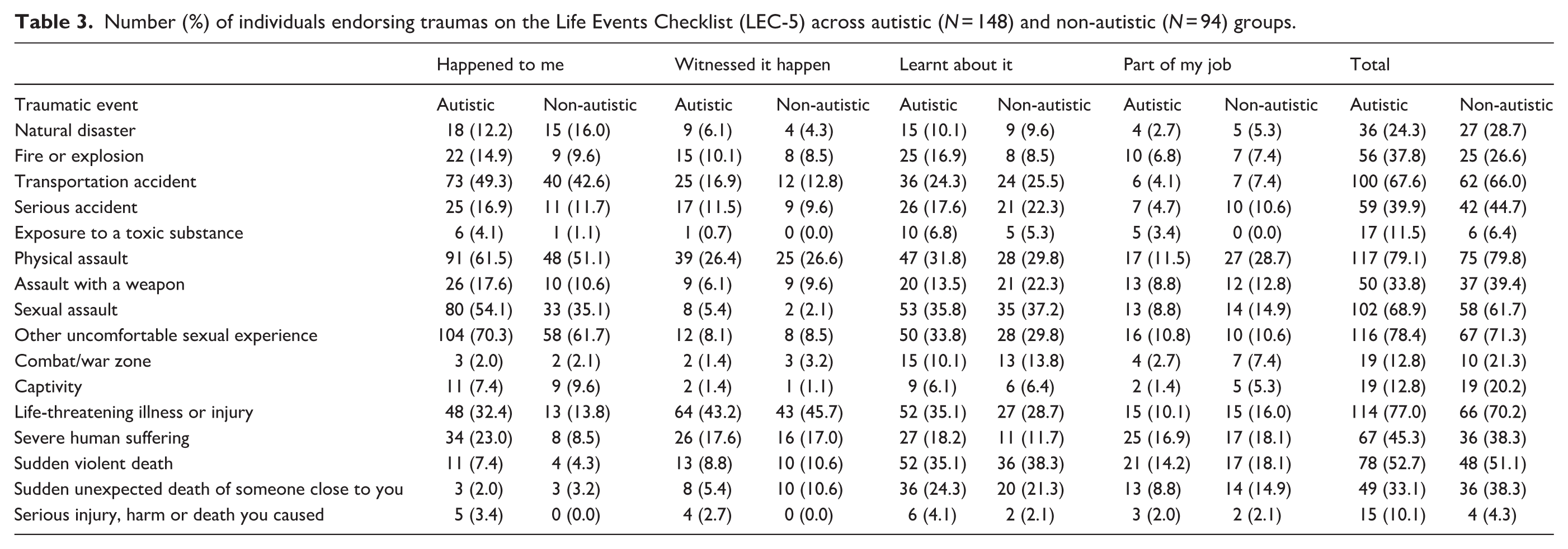
For Criterion-A traumatic event types overall, measured and categorised by the LEC-5, both groups most frequently endorsed physical assault, unwanted sexual experiences, life-threatening illness or injury, sexual assault and transportation accidents. For events that ‘happened to me’ directly, uncomfortable sexual experiences were reported by the highest proportion of each group, followed by physical assault. Except for natural disaster, exposure to war/combat, captivity and sudden unexpected death of someone close to you, a higher proportion of the autistic group directly experienced each trauma type than the non-autistic group. The Criterion-A traumatic events endorsed by each group are shown in Table 3.
Number (%) of individuals endorsing traumas on the Life Events Checklist (LEC-5) across autistic (N = 148) and non-autistic (N = 94) groups.
Of 103 autistic and 61 non-autistic participants who reported additional non-Criterion-A traumatic events, the autistic group most frequently reported bullying (26.2%, n = 27), bereavement (21.4%, n = 22) and emotional abuse (14.6%, n = 15). The non-autistic group most frequently reported bereavement (18.0%, n = 11), illness, medical procedures and hospitalisation (16.4%, n = 10), pregnancy and childbirth (11.5%, n = 7), and illness or injury of a family member or friend (11.5%, n = 7). The non-Criterion-A traumatic events reported by each group are shown in Table 4.
Non-Criterion-A traumas reported by the autistic and non-autistic groups.
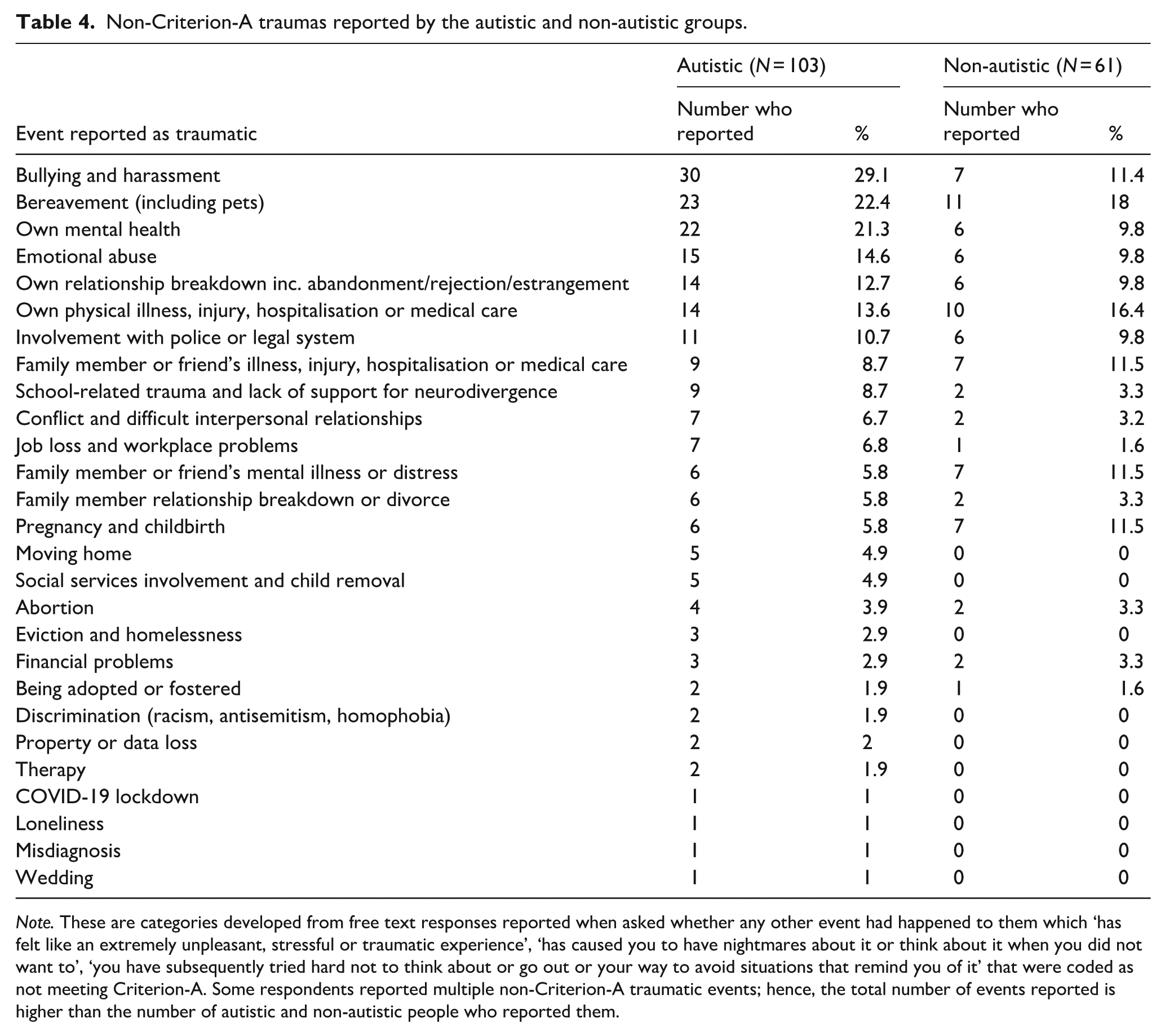
Note. These are categories developed from free text responses reported when asked whether any other event had happened to them which ‘has felt like an extremely unpleasant, stressful or traumatic experience’, ‘has caused you to have nightmares about it or think about it when you did not want to’, ‘you have subsequently tried hard not to think about or go out or your way to avoid situations that remind you of it’ that were coded as not meeting Criterion-A. Some respondents reported multiple non-Criterion-A traumatic events; hence, the total number of events reported is higher than the number of autistic and non-autistic people who reported them.
Bivariate correlations
A correlation matrix of study variables is shown in Table 5. PTSD-SS, depression and anxiety symptoms were highly intercorrelated. TAQ subscales were positively correlated with PTSD-SS, Depression and Anxiety Symptoms, and these associations were all statistically significant.
Correlations between autism group, PTSD-SS, appraisals, anxiety and depression.
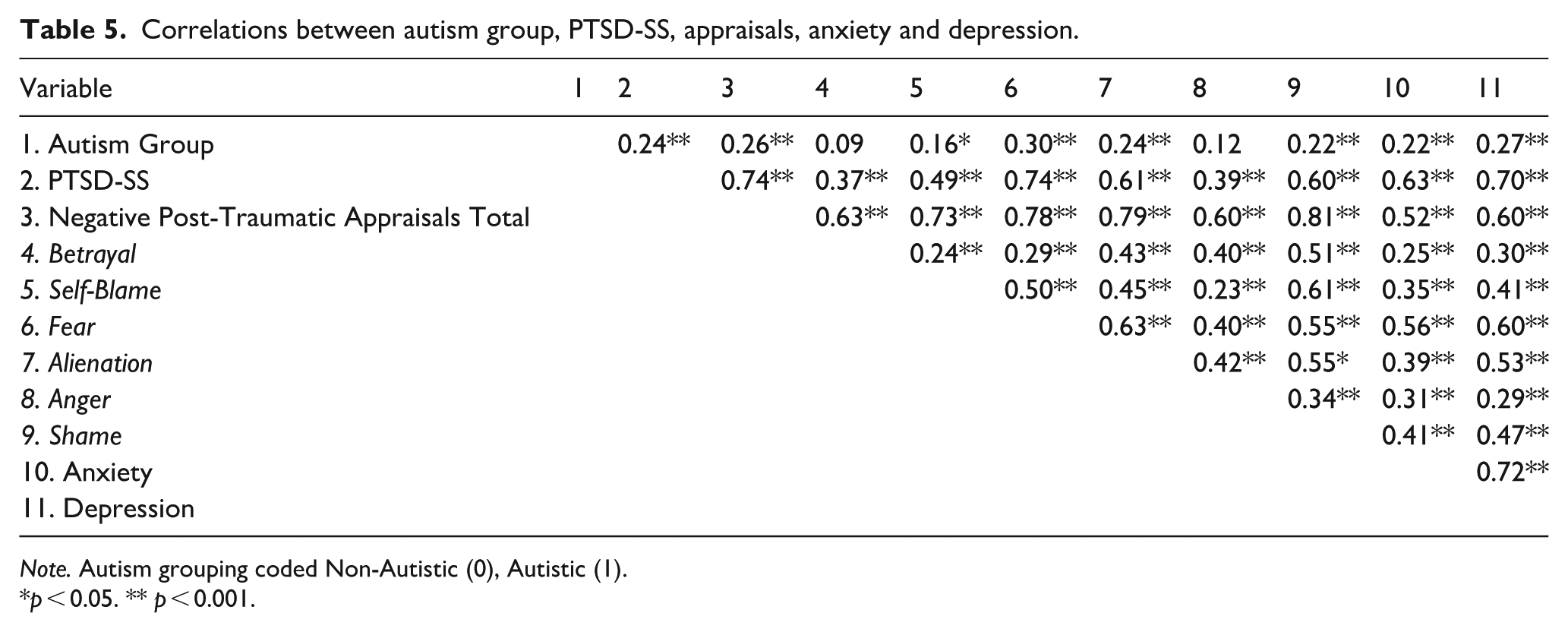
Note. Autism grouping coded Non-Autistic (0), Autistic (1).
p < 0.05. ** p < 0.001.
H1: The autistic group will endorse significantly more negative post-traumatic appraisals than the non-autistic group
The autistic group reported higher scores on the TAQ overall than the non-autistic group, a statistically significant difference (p < 0.001; Table 2).
H2: The autistic group will endorse significantly more shame, self-blame and alienation appraisals than the non-autistic group
The autistic group had higher scores across all TAQ subscales than the non-autistic group. However, after applying a Bonferroni correction for multiple comparisons (adjusted significance threshold p < 0.008), this difference was statistically significant for alienation (p < 0.001) and shame (p < 0.001), as hypothesised, and also for fear (p < 0.001; Table 2). Although the autistic group also reported higher self-blame scores, this difference did not reach the corrected threshold for significance (p = 0.022). Betrayal and anger did not differ significantly between the groups.
H3: The association between autism group and PTSD-SS will be significantly mediated by negative post-trauma appraisals, with more negative post-traumatic appraisals being associated with higher PTSD-SS
Model 1 explored the effect of negative post-trauma appraisals on the association between group and PTSD-SS following a traumatic event. Results based on 5000 bootstrapped samples indicated that TAQ total score significantly mediated the association between group and PTSD-SS (Table 6); significant total effects were found between autism group and PTSD-SS, and when TAQ total scores were entered as a mediator of this association, a significant indirect effect was observed. The direct effect was no longer significant and the bias-corrected 95% CI for the indirect effects did not pass through 0. Autistic adults had more negative appraisals following a traumatic event, which was statistically associated with higher PTSD-SS compared to non-autistic adults (Figure 1).
Appraisal mediation models based on 5000 bootstrapped samples for the association between group (autistic/non-autistic) and PTSD-SS.
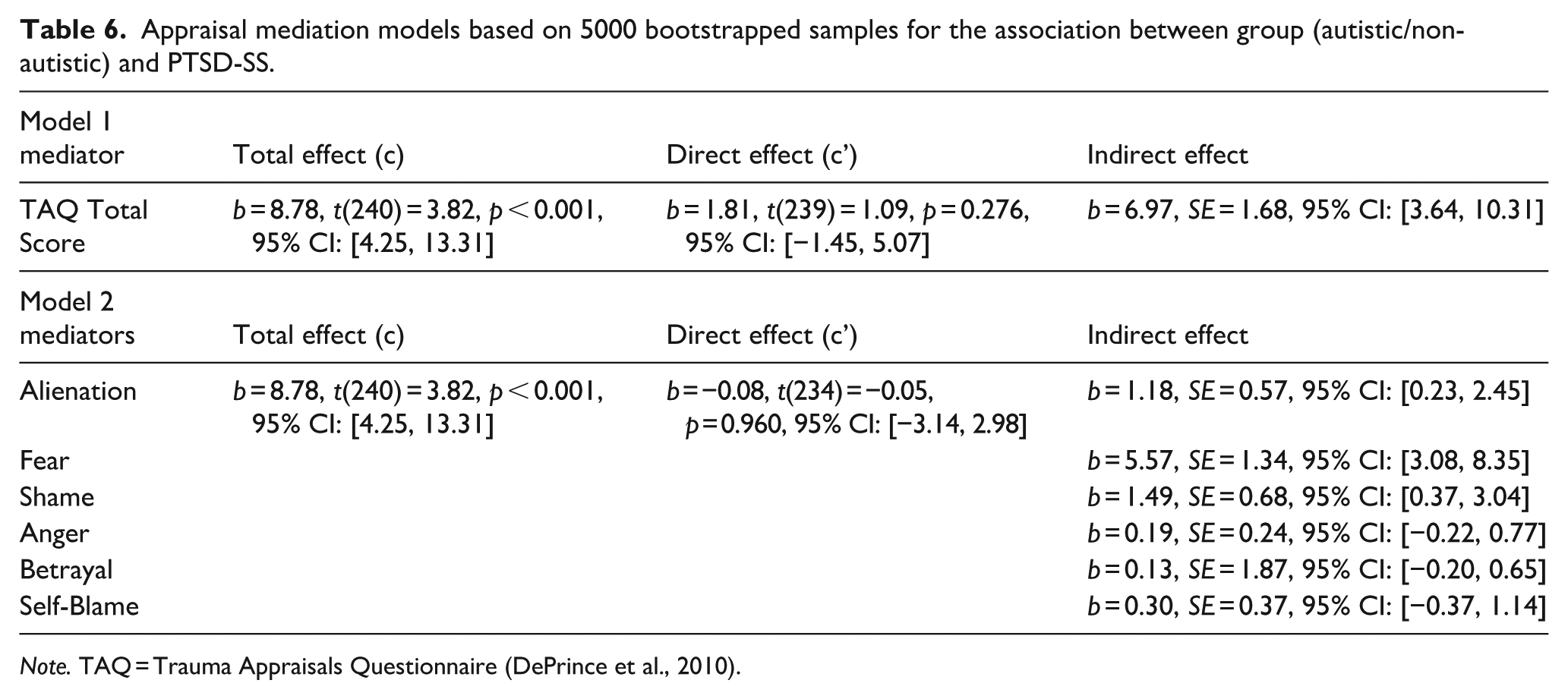
Note. TAQ = Trauma Appraisals Questionnaire (DePrince et al., 2010).
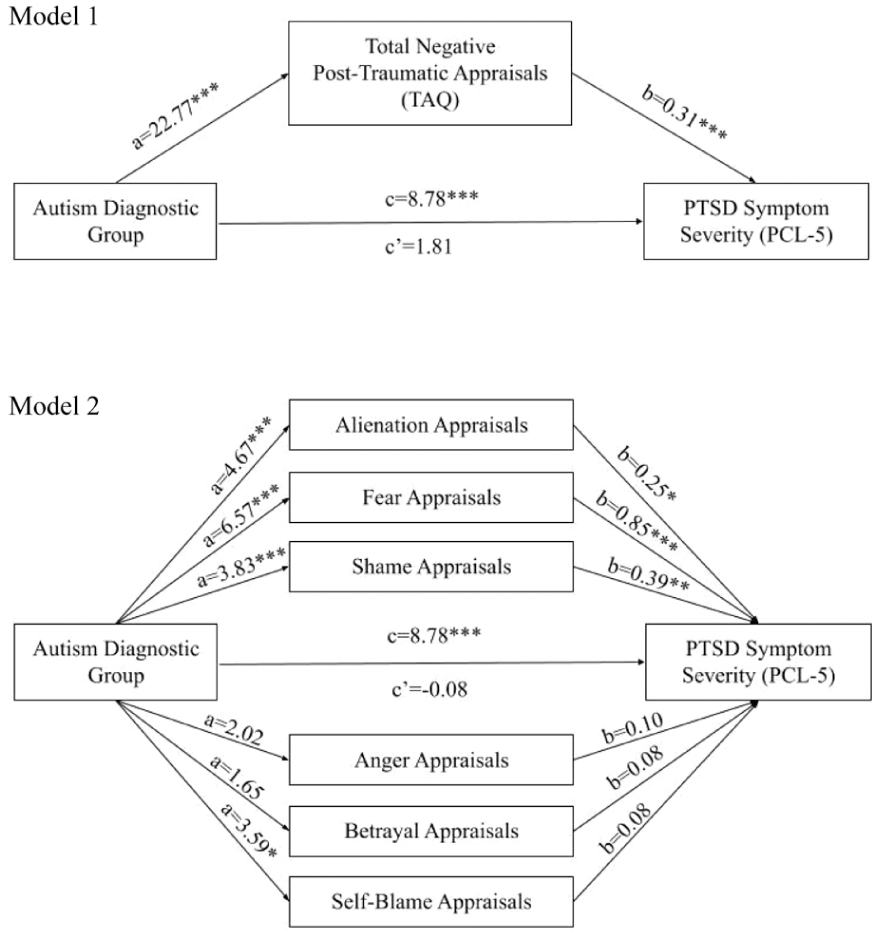
Mediation models showing the unstandardised regression coefficients for the association between autism diagnostic group and PTSD-SS, via total negative post-traumatic appraisals (Model 1), appraisal subscales (Model 2).
In Model 2, the six TAQ subscales were included as parallel mediators. Results based on 5000 bootstrapped samples showed that alienation, fear and shame appraisals mediated the association between autism group and PTSD-SS; there was a significant total effect, and significant indirect effects were observed for alienation, fear and shame appraisals, suggesting these appraisals mediate the association between group and PTSD-SS when other appraisals are controlled for. The direct effect was not significant and the bias-corrected 95% CIs for the indirect effects did not pass through 0, suggesting these appraisals mediated the association between autism and PTSD-SS (Figure 1). Autistic adults had more alienation, fear and shame appraisals following a traumatic event, and these were statistically associated with higher PTSD-SS compared to non-autistic adults.
Given the high intercorrelation observed between TAQ subscales, and measures of depression and anxiety symptomatology, two further exploratory mediation models were run with depression and anxiety scores as outcomes with the six TAQ subscales as parallel mediators. Total effects were significant for both outcomes (anxiety c: b = 2.56, t(240) = 3.53, p < 0.001, 95% CI: [1.13, 3.99]; depression c: b = 3.48, t(240) = 4.34, p < 0.001, 95% CI: [1.90, 5.06]). For anxiety, a significant indirect effect was observed for fear appraisals (b = 1.50, SE = 0.41, 95% CI: [0.77, 2.36]). For depression, significant indirect effects were observed for fear (b = 1.42, SE = 0.42, 95% CI: [0.68, 2.31]) and alienation (b = 0.56, SE = 0.27, 95% CI: [0.11, 1.15]) appraisals. The direct effects were not significant (anxiety c’: b = 0.63, t(240) = 0.97, p = 0.334, 95% CI: [−0.65, 1.90]; depression c’: b = 1.07, t(240) = 1.58, p = 0.115, 95% CI: [−0.26, 2.40]) and the bias-corrected 95% CIs for the indirect effects did not pass through 0, suggesting fear appraisals mediated the association between autism and anxiety, and that fear and alienation appraisals mediated the association between autism and depression. Autistic adults had more alienation and fear appraisals following a traumatic event, and these were statistically associated with higher depression and anxiety symptomatology compared to non-autistic adults.
Discussion
This study aimed to evaluate whether, compared to trauma-exposed non-autistic adults, autistic adults are exposed to more traumatic life events, find a broader range of events traumatic and report greater PTSD-SS, in line with existing findings. We then aimed to explore whether negative post-traumatic appraisals differed between the groups, and whether these mediated the association between autism and PTSD-SS.
In line with previous findings, PTSD-SS was significantly higher in the autistic compared to the non-autistic group, and autistic people were more likely to meet the threshold for PTSD diagnosis following traumatic life events. Although on the LEC-5 autistic people did not report exposure to significantly more types of Criterion-A traumatic life events overall, they reported that more types of Criterion-A event had happened to them directly. These findings suggest that while autistic individuals may not experience a greater number of trauma types per se, they appear more likely to be directly exposed to those events. This is an important distinction, as direct exposure has been shown to be more strongly associated with PTSD symptom severity than indirectly experienced events (Anders et al., 2011). Concerningly, incidence of physical assault, sexual assault, uncomfortable sexual experiences, bullying and emotional abuse was very high in the autistic group, higher than the non-autistic group, in line with previous studies (Rumball et al., 2020; Rumball, Antal, et al., 2021; Rumball, Brook, et al., 2021). Despite this, contrary to our predictions based on past research, the groups did not differ in overall Criterion-A trauma exposure, as assessed by the LEC-5, or nature of their ‘worst’ trauma (whether it was interpersonal or not, or met DSM-5 Criterion-A). It is important to acknowledge that this may be the product of limitations of the LEC-5 in this context, which is not designed to quantify trauma frequency. As such, while we report the number of trauma types, we were unable to assess how often each trauma occurred, seriously limiting this measure of trauma exposure. Nevertheless, while trauma is a necessary antecedent, these findings suggest that trauma type and frequency are not the only relevant risk factors for increased PTSD-SS in autistic people. As is known in the general population, there are a range of pre-, peri- and post-trauma factors which impart risk of PTSD development (Brewin et al., 2000), which may increase risk of PTSD development for autistic people even when levels of trauma exposure appear comparable.
Similar proportions of each group completed the PCL-5 in relation to non-Criterion-A events, in line with research which repeatedly demonstrates that people can experience PTSD symptoms following non-Criterion-A events (Brewin et al., 2019; Hyland et al., 2021; Larsen & Pacella, 2016; Nielsen et al., 2015). This challenges the clinical utility of the DSM-5 conceptualisation of traumatic events and supports research which has called for the need to critically reassess how PTSD is defined and diagnosed (e.g. Brewin et al., 2019; Mansour et al., 2025). The International Classification of Diseases, 11th Revision (ICD-11; World Health Organization, 2022) definition of trauma as ‘an extremely threatening or horrific event or series of events’ may be preferable in PTSD assessment to ensure that people who would benefit from support receive a diagnosis.
We extend knowledge in the field by showing that autistic people reported higher levels of negative post-traumatic appraisals, in particular alienation, shame, self-blame and fear appraisals. Negative appraisals statistically mediated the positive association between autism and PTSD-SS, suggesting a plausible statistical pathway between experiencing trauma, to PTSD-SS, via negative appraisals, consistent with cognitive models of PTSD (Brewin et al., 1996; Ehlers & Clark, 2000). To our knowledge, this has not been previously demonstrated in autistic people.
Increased propensity to negatively appraise traumatic experiences may be influenced by several factors in autistic people. Exposure to stigma and traumatic experiences throughout life may understandably lead to development of negative beliefs about themselves and the threat posed by the world and other people, which may prime autistic people to more negative appraisals following traumatic events which are seen as a confirmation of these beliefs. Sensory sensitivity may additionally result in the world feeling more overwhelming and dangerous. Furthermore, tendency towards perseverative thinking and thought suppression observed in autistic people and associated with PTSD-SS (Crane et al., 2013; Rumball, Antal, et al., 2021) may result in difficulty disengaging from negative appraisals, or their more frequent intrusion due to ‘bounce back’ effect of suppression (Davies & Clark, 1998), increasing their intensity. Sensitivity analyses suggested that while appraisals such as shame may be more PTSD-specific, others such as fear and alienation may represent broader mechanisms linking trauma exposure to multiple forms of distress.
Alienation appraisals, related to feelings of disconnectedness from self and other people, are implicated as important for PTSD development in general population samples (Mitchell et al., 2020) and mediated the association between autism and PTSD-SS in this study. Research has highlighted that autistic people are aware of their differences from non-autistic people and that these are often perceived negatively (Botha et al., 2022; Han et al., 2022). Internalisation of stigma, reflected in qualitative research in which autistic people describe themselves as ‘weird’ (Botha et al., 2022, p. 10), may increase sense of ‘otherness’, increasing salience of alienation appraisals following trauma. Alienation appraisals may alternatively reflect a mismatch between neurotypical and neurodivergent communication styles, resulting in difficulties with understanding and being misunderstood, termed the double-empathy problem (Milton, 2012). This may contribute to feeling disconnected, and possibly to actual reduced accessibility of social support observed in autistic people (Tobin et al., 2014), which contributes to PTSD in the general population (Shallcross et al., 2016), and worsened mental health in autistic people (Moseley et al., 2021). Exploratory analyses indicated that alienation appraisals also mediated associations between autism and depression symptoms, consistent with research that feelings of disconnection may underpin both PTSD and broader emotional distress (DePrince et al., 2011; Mitchell et al., 2020).
Shame-based appraisals are implicated in PTSD-SS in the general population (DePrince et al., 2011) and were higher in our autistic group and mediated PTSD-SS. These may also be related to internalised stigma, which has been associated with feelings of shame about being autistic, identified as a reason for camouflaging of autistic characteristics (Cage & Troxell-Whitman, 2019). Furthermore, if autistic people perceive that traumatic experiences occurred due to being autistic (e.g. bullying), this may be particularly likely to result in shame appraisals as an aspect of the self is implicated in the traumatic event. This may be especially relevant following interpersonal traumas, associated with more shame-based appraisals in the general population (Beierl et al., 2020). Although the ‘worst’ events reported by autistic people were not more likely to be interpersonal, there was higher incidence of interpersonal traumas like physical and sexual abuse and bullying in the autistic group. Elevated self-blame appraisals were also observed in the autistic group, as hypothesised, however, these did not mediate PTSD-SS.
We had not hypothesised that fear appraisals would be higher in the autistic group; however, it is plausible that these are developed and reinforced through repeated experiences of the world not being safe or supportive for autistic people. In addition, factors like intolerance of uncertainty and alexithymia which are elevated in autistic people (Maisel et al., 2016; South & Rodgers, 2017) may predispose them to fear appraisals. Intolerance of uncertainty is robustly linked with increased anxiety in autistic people (Jenkinson et al., 2020) and may reinforce appraisals that the world is unpredictable and thus unsafe following trauma. Furthermore, if some autistic people have difficulties recognising their own or others’ emotional states as explored by Maisel and colleagues (2016), processing feelings of fear or safety may be more difficult. These individuals may also experience more uncertainty and fear appraisals in social situations if other people have been experienced as dangerous before and are hard to read. Future research could examine these possible autism-related vulnerability factors for PTSD. Sensitivity analyses showed that fear appraisals similarly mediated links between autism and both anxiety and depression, suggesting that fear-based interpretations of the world as unsafe may contribute to general affective vulnerability in autistic adults, rather than being specific to PTSD.
The current findings tentatively imply that trauma-focused therapeutic approaches that focus on negative appraisals in PTSD, with enquiry about appraisals of alienation, shame and fear, are supported for autistic people. Interventions must prioritise initially building a strong therapeutic relationship focused on shared understanding. Compassion-focused approaches may be indicated in the context of increased shame (Goffnett et al., 2020), and approaches to support positive autistic social identity may also be helpful to improve well-being (Cooper et al., 2017). It is also important that measures are put in place to protect autistic people from trauma exposure and tackle societal stigmatising attitudes towards autism which can negatively impact well-being if internalised (Botha & Frost, 2018; Perry et al., 2022).
Limitations
Several factors influence the generalisability and validity of our current results. Most significantly, the use of a cross-sectional methodology limits our ability to draw conclusions about the directionality or causality of the observed relationships. The mediations presented identify statistical associations consistent with our hypotheses, but do not confirm that one variable causes changes in another. Prospective longitudinal studies examining the temporal sequence of trauma exposure, appraisals and later development of PTSD symptoms are required to provide stronger evidence for causal mechanisms.
It should be noted that rates participants exceeding the threshold for probable PTSD on the PCL-5 were high in both groups, particularly for probable lifetime PTSD, exceeding those observed in previous research with trauma-exposed individuals. In addition, rates of exposure to specific trauma types like sexual assault are significantly higher in both groups than general population prevalence rates (McManus et al., 2009) and large-scale epidemiological studies of trauma exposure (Kessler et al., 1995). This may reflect a self-selection bias inherent to online research, whereby individuals experiencing heightened severity of trauma experiences or PTSD symptoms, may be more motivated to participate, resulting in elevated symptom reports across both groups. However, as both groups self-selected, group comparisons remain valid. In addition, recruitment materials intentionally did not refer to PTSD or PTSD symptoms with the hope that this reduced the risk of this. High rates of probable lifetime PTSD may also reflect the reliance of the adapted lifetime version of the PCL-5 on participants’ retrospective recall of symptoms, which can introduce recall bias and inflate estimates of symptom severity (Pacheco-Romero et al., 2025). The lifetime version of the PCL-5 was included to provide an estimate of past symptom burden, but is not validated for this purpose, so these rates should be interpreted cautiously.
Regarding representativeness of the sample, participants were also predominately White British, women and university educated, and individuals with an intellectual disability were excluded. Consequently, the experiences of some autistic and non-autistic people, especially those with additional support needs and from ethnic minority groups, are not reflected. People with multiple minoritised identities may experience heightened stigma and victimisation (Budge et al., 2016); thus, more effort is needed to reach these groups in future studies.
A notable feature of this study is the large sample size and relatively high number of autistic women and non-binary participants, groups that have historically been underrepresented in autism research and experience higher rates of PTSD in the general population (Marchi et al., 2023; Olff, 2017). However, the high proportion of respondents identifying as women may have influenced our findings, as gender has been identified as a risk factor for PTSD (Brewin et al., 2000). Gender differences in PTSD-SS were not found in either group so gender-disaggregated analyses were not conducted. Nonetheless, gender differences in exposure to specific trauma types among autistic people, like sexual assault which is more frequent in women and is associated with risk of PTSD (Creamer et al., 2001), may warrant further investigation. A strength of this study is that similar proportions of each group reported interpersonal traumas as their ‘worst’, as these are more likely to result in PTSD (Brewin et al., 2000). However, trauma type is also implicated; thus, future studies could match for trauma type across autistic and non-autistic groups.
By determining autism grouping by self-report, we reduced bias towards including only those who have the means to access an autism diagnosis in our sample. However, this may mean that some participants were not accurately grouped as we did not verify diagnoses. AQ scores were higher than expected in the non-autistic group, which may be a product of recruitment through autism charities, with family members of autistic people who may have more traits possibly being recruited. However, this may alternatively be an artefact of measurement, with some studies suggesting that the AQ poorly differentiates autism from constructs like attention deficit hyperactivity disorder (ADHD) and Personality Disorders (Dudas et al., 2017; Sizoo et al., 2009), although this has not been explored in relation to PTSD symptomatology. We also did not record the age at which people were diagnosed as autistic. It may be interesting for future research to explore whether there are differences in the variables and associations explored in this study between people with and without formal diagnoses, and between those diagnosed in childhood compared to adulthood.
Finally, the PCL-5 and TAQ have not been validated in autistic individuals; indeed, there are currently no PTSD or post-traumatic appraisal scales validated for use with autistic people. In this study, we included only limited qualitative exploration of the nature of autistic people’s traumatic experiences. Future qualitative research in this area is needed to elucidate the autistic experience of trauma and PTSD and inform the development of appropriate measures. Research is then needed to validate or develop tools to assess PTSD symptoms and appraisals for autistic people, with consideration of possible autism-specific presentations. In addition, the LEC-5 was not designed to measure trauma frequency, nor did we record frequency of non-Criterion-A traumas, limiting the validity of our findings in relation to frequency of trauma exposure.
Conclusion
These findings add to the growing literature highlighting increased PTSD-SS experienced by autistic adults following traumatic events. The mediating effect of negative post-traumatic appraisals is in line with cognitive models of PTSD in the general population, suggesting that similar mechanisms are involved in the development of PTSD for autistic adults. Negative appraisals of shame, fear and alienation are particularly implicated. Longitudinal designs are now required to confirm the direction of these effects and understand factors precipitating more negative appraisals in autistic people in order to identify possible therapy targets and strategies to reduce the risk of PTSD development.
Footnotes
Appendix 1
Appendix 2
Ethical Considerations
This study was approved by the University of Oxford Medical Sciences ethics committee (R84859/RE001).
Consent to Participate
Written informed consent to participate was obtained from all participants.
Consent for Publication
Written informed consent to publish was obtained from all participants.
Author Contributions
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The data from this study is not publicly available as participants’ consent for this to be shared was not sought.