
Abstract
This study examines disparities in autism identification rates and support needs between Māori and non-Māori populations in Aotearoa New Zealand. The research was conducted through a collaborative approach with autistic Māori. Population-level administrative data were analysed for all individuals aged 0–24 years (N = 1,565,505) as of 30 June 2018. Autism identification was determined through health service records from July 2010 to June 2018. Comparative analyses examined autism rates, intellectual disability (ID) co-occurrence, and Ongoing Resourcing Scheme (ORS; high-need education funding support) allocation between Māori and non-Māori populations. Autism identification rates were lower among Māori (70.9/10,000) compared to non-Māori (78.3/10,000). Autistic Māori had higher rates of ID diagnosis (OR = 1.12; 95% CI = 1.02, 1.24) and ORS funding allocation (OR = 1.35; 95% CI = 1.22, 1.48). The observed disparities in autism identification rates and diagnostic patterns suggest potential systemic barriers to autism identification among Māori, particularly for those with lower formal support needs. Future Kaupapa Māori, autistic-led research is warranted to better understand these disparities and inform culturally responsive diagnostic and support services.
Lay Abstract
In this study, autistic Māori collaborated with researchers to analyse autism identification in Aotearoa New Zealand using population-level administrative data. The research examined all children and young people (0–24 years) in the Aotearoa New Zealand population as of 30 June 2018, identifying autism through health service records between July 2010 and June 2018. The findings showed lower autism identification rates among Māori (70.9 per 10,000) compared to non-Māori (78.3 per 10,000). This difference in rates is likely to reflect ongoing inequities and systemic racism, not true prevalence differences. Autistic Māori were also more frequently diagnosed with intellectual disability (ID) and more likely to receive high-need education funding support than autistic non-Māori. While these patterns might suggest higher formal support needs among autistic Māori, it’s crucial to recognise that support requirements are highly individual and context-dependent, making them difficult to measure using broad indicators. The lower overall autism identification rate among Māori, combined with these findings, suggests that autistic Māori with lower formal support needs may be missing opportunities for diagnosis and not accessing the supports and services they are entitled to. Future Kaupapa Māori, autistic-led research is needed to gain a more nuanced understanding of autism identification and support needs among Māori.
A note on language
We have chosen to use identity first language (e.g. ‘autistic person’) in line with recommendations from autistic researchers and advocates regarding autistic preferred language (Monk et al., 2022). However, we acknowledge that preferences vary within and across different communities (Bottini et al., 2024) and, to date, no research has focused on the language preferences of autistic Māori.
We also acknowledge there are problems associated with some of the terminology used in this manuscript. For example, the term intellectual disability is underpinned by Western perspectives and presents a deficit-focused view which is at odds with te ao Māori (Māori worldview) perspectives (Ingham et al., 2022). In Aotearoa, the term ‘learning disability’ is increasingly being used in place of ‘intellectual disability’ (Benchmark, 2024) and is viewed as a more respectful term by those with such disabilities (People First NZ, 2024). However, we acknowledge that terminology varies across geographical and cultural contexts, and the term ‘learning disability’ is used to represent a distinct concept in some contexts. In addition, the data related to sex/gender included in this report are presented as binary (i.e. ‘male’ or ‘female’), but this does not reflect the many ways gender may be experienced and expressed (Hyde et al., 2019). These terms are used exclusively in relation to existing data; they are included to align with how data were originally collected and reflect living in the context of colonisation (Ingham et al., 2022). We use this terminology with caution so as not to reproduce it within autism research.
Introduction
Autism is a neurodevelopmental condition, clinically characterised by (a) differences in social communication and sensory experiences and (b) the presence of restricted and/or repetitive patterns of behaviour and special interests (American Psychiatric Association, 2013; Pellicano & den Houting, 2022). Māori (the Indigenous people of Aotearoa, New Zealand, from herein Aotearoa) understandings of autism may differ from Western understandings (Bevan-Brown, 2004). For example, te kura urupare, meaning gift of the senses (T. McDonnell, personal communication, 9 June 2021), is a Māori term for autism which acknowledges and celebrates autistic peoples’ unique sensory abilities and experiences. Similarly, takiwātanga, which means in one’s own time and space, was recently developed to capture a non-judgemental, te ao Māori (Māori worldview) perspective of autism (Altogether Autism, 2017; Te Pou o te Whakaaro Nui, 2019).
There is no systematically collected nationwide autism prevalence data in Aotearoa (Bowden et al., 2020). However, a recently developed method for identifying autism cases using administrative health data indicated a prevalence rate of 1 in 102 among 8 year olds (Bowden et al., 2020). In this same study, autism rates among Māori (the Indigenous people of Aotearoa) aged 0–24 years, were found to be substantively lower compared to New Zealand Europeans (49.2 per 10,000 people compared to 67.5 per 10,000). These differences are unlikely to indicate genuine differences in prevalence but may instead reflect underlying factors such as institutional racism and ongoing inequities (Bowden et al., 2020).
Internationally, the rates of autism identification have historically been lower among underserved ethnic groups (Tromans et al., 2021), similar to patterns observed in the prevalence of chronic medical conditions such as diabetes and kidney disease (Kim et al., 2018). However, these gaps have not only closed over the past decade, but prevalence among minority groups in the United States now exceeds those among White Americans (Baio et al., 2018; Lau et al., 2024; Maenner et al., 2020, 2021, 2023; Shaw et al., 2025). Lower prevalence rates among underserved groups may reflect lower rates of interaction with health and social services that result in a recorded diagnosis. This may be in part due to health care barriers faced by underserved ethnic groups such as diagnostic biases, lack of culturally responsive services, systemic racism, a higher likelihood of living in geographically remote areas and mistrust of the health system/avoiding the health system as a safety strategy (Lau et al., 2024; Tromans et al., 2021). Indeed, Māori have a well-documented history of encountering institutional racism within the health and disability systems (Jones et al., 2024; Wilson et al., 2021). Another possibility is that, for underserved ethnic groups, lower-need cases of autism are being misdiagnosed or underdiagnosed relative to other groups. This would align with findings from Ruhe and colleagues (2022) regarding low rates of autism diagnosis among Pacific children in Aotearoa and with research from the United States regarding the under-identification of autism among Black children (Fombonne & Zuckerman, 2022). In contrast, a narrowing gap in autism diagnosis rates by ethnicity may reflect progress towards more equitable recognition and assessment practices (Harris, 2023; Yu et al., 2025).
There is limited existing research regarding Māori and autism diagnosis (Tupou et al., 2021). However, findings from two previous studies indicate that in general, Māori desire access to autism services, including diagnostic services (Bevan-Brown, 2004; Bevan-Brown et al., 2015). From the limited available data, it appears that Māori may face many of the same barriers to accessing autism services as non-Māori but may be less likely to live in large urban centres and/or may be more likely to have a lower socioeconomic status and therefore be more likely to face barriers associated with these factors (Whaikaha – Ministry of Disabled People and Ministry of Education, 2022). Autistic Māori may also face additional barriers such as negative attitudes from professionals and the public and a mistrust of the system (Bevan-Brown, 2004; Birkin et al., 2008; Whaikaha – Ministry of Disabled People and Ministry of Education, 2022). Furthermore, the intersectionality of autistic and Māori identities may lead autistic Māori to experience unique or compounded barriers that reflect the inequities faced by both underserved groups (Simpson, 2021). Overall, autistic Māori appear to have poorer access to services compared to non-Māori (Searing et al., 2015).
Research focussed on Māori and disability more broadly has highlighted the incongruence between Western diagnoses, which are often deficit-focussed and reductionist, and te ao Māori perspectives of hauora (health and well-being) which tend to be more holistic and strengths-focused (Jones et al., 2024). Despite this incongruence, disabled Māori report that diagnostic labels are often necessary for accessing disability support services (Jones et al., 2024). Indeed, access to support is the key reason that parents and families in Aotearoa pursue an autism diagnosis for their child (Autism NZ, 2024; Crane et al., 2016). The immediate and long-term benefits of early support for autistic individuals and their families have been highlighted across a large body of research (Whitehouse et al., 2020). Diagnosis may also play a crucial role in promoting acceptance, understanding and well-being among autistic people and their families, with earlier diagnoses associated with better outcomes than those received later in life (Atherton et al., 2022; Autism NZ, 2024; Bejarano-Martín et al., 2020).
Given the potential benefits associated with timely diagnosis and research indicating potential additional and unique barriers to diagnosis for Māori, it seems important to investigate autism identification in Māori. The current study builds upon earlier work from Bowden et al. (2020), which examined population-level administrative data covering the period from 2010 to 2016. Given the rapid changes in autism identification rates over time (Harris, 2023; Ministry of Health, 2025) and international evidence suggesting improved identification rates among minority groups (Baio et al., 2018; Lau et al., 2024; Maenner et al., 2020, 2021, 2023; Shaw et al., 2025), it seems valuable to examine how identification rates among Māori may have shifted in the two years between 2016 to 2018. A key strength of the current study is the inclusion of autistic Māori co-researchers who provide insight into data analysis and interpretation, drawing on their lived experience and expertise. This type of co-production is novel in autism prevalence/incidence research and is vital to ensuring that our analysis and interpretation of the data reflect the experiences and perspectives of autistic Māori. The specific aims of this paper are to use Aotearoa administrative data to examine whether (a) there are differences in the rate of autism diagnosis among rangatahi Māori (Māori youth) compared to non-Māori youth, and (b) whether identified cases of autism among rangatahi Māori vary in levels of formal support needs relative to non-Māori. Findings will be discussed in relation to implications for future research and service provision, including recommendations for how support needs can be better met.
Method
Study design
This was a national cross-sectional study using linked administrative health data contained within the Integrated Data Infrastructure (IDI). The IDI is a collection of administrative and survey data about people and households in Aotearoa, managed by Statistics New Zealand (Milne et al., 2019). These data are probabilistically linked by Statistics New Zealand at the individual level, using information such as name, sex, and date of birth, and then de-identified before being made available for research deemed to be for the public good. Statistics New Zealand’s linking methodology is designed to maximise linkage rates between data sources while keeping the false positive rate below 2% (Statistics New Zealand, 2021b). The study participants were a national cohort of children and young people in Aotearoa, aged 0–24 years. The cohort was defined as those in the Aotearoa estimated resident population (ERP) for the 2017/18 fiscal year (1 July 2017 until 30 June 2018) utilising an existing method for identifying the ERP using the IDI (Gibb et al., 2016). To be included in the IDI-based ERP, individuals must have used key government services in Aotearoa over the previous 2-year period. It also excludes those who died or moved overseas prior to the end of the 2017/18 fiscal year.
Community involvement
For this study, a Pou Herenga rōpū (anchoring group) of autistic Māori and whānau collaborated with the research team in the analysis and interpretation of data. Two of the rōpū (Ia Morrison-Young and Te Ahi Wi-Hongi) also contributed to writing up the study findings and are included as authors on this manuscript.
Determining ethnicity
An indicator for Māori ethnicity was extracted from the personal details table of the IDI. Ethnicity data in the personal represents total ethnicity, meaning each person can identify with multiple ethnicities. All those who identified as Māori were included as Māori, regardless of the other ethnic groups they identify with. For the purposes of this study, rangatahi Māori (Māori children and young people) were compared to non-Māori (all individuals in the ERP who did not identify as Māori). This group is comprised of those from level 1 major ethnic groups of: European,; Asian; Pasifika; Middle Eastern, Latin American, African (MELAA); and other (not listed).
Identifying autism
Autism status was determined using an existing IDI-based case identification method (Bowden et al., 2020). This method draws on diagnosis information from three health datasets: hospital admissions information from the National Minimum Dataset (NMDS); specialist mental health services data from the Programme for the Integration of Mental Health (PRIMHD), and needs assessment information from Socrates, the Ministry of Health’s disability support services (DSS) dataset. Individuals were identified as autistic utilising appropriate coding from within each dataset. Specifically: Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) codes for autistic disorder (299.00), childhood disintegrative disorder (299.10), and Asperger’s disorder/pervasive development disorder NOS (299.80) from PRIMHD; ICD-10-AM codes for autistic disorder (F84.0), atypical autism (F84.1), other childhood disintegrative disorder (F84.3), Asperger’s syndrome (F84.5) other pervasive developmental disorders (F84.8), and pervasive developmental disorder, unspecified (F84.9) from NMDS and PRIMHD; and assigned diagnosis codes of autism (1211), Asperger’s syndrome (1206) and other autism spectrum disorders (1207) from Socrates. Autism was identified among the participant population if at least one of the above-listed diagnostic codes, in any of the datasets was present, across 8 years of data from 1 July 2010 until 30 June 2018. As described in Bowden et al. (2020), the majority (77%) of autism cases identified are via DSS data, and diagnosis information is recorded upon referral for a needs assessment. These are formal diagnoses, from qualified clinicians, or team of clinicians, including developmental paediatricians, child and adolescent psychiatrists, general practitioner, or psychologist. Under the current system in Aotearoa, all individuals who receive an autism diagnosis should be referred to a Needs Assessment and Service Coordination provider for a needs assessment to facilitate access to DSS. Cases identified via NMDS and PRIMHD have been coded by trained coding specialists, recorded only if the autism diagnosis is material to the health care of the child, and should therefore have a high degree of accuracy, although this method has not been formally validated.
Primary outcome variable: level of formal support need
Two separate indicators were created as proxies for higher levels of formal support needs among those with an autism diagnosis: intellectual disability and ongoing resourcing scheme (ORS) funding.
Intellectual Disability (ID)
As noted at the beginning of this manuscript, the conceptualisation of ID is problematic from a te ao Māori perspective. Our use of the term ‘intellectual disability’ here is in line with how the data were originally collected.
ID is commonly associated with autism and is estimated to affect 31% of autistic people (Baio et al., 2018). Autistic individuals with co-occurring ID often face additional challenges including social and emotional difficulties as well as increased rates of co-occurring psychopathology (Matson & Shoemaker, 2009), typically leading to higher levels of formal support needs. In the present study, ID was identified in much the same way as autism, using an existing IDI-based case identification method (Bowden et al., 2020). Specifically, ID was identified from the presence of any of the following codes over the 8 year period: DSM-IV codes 317* 319*, 3180, 3181, 3182 in PRIMHD; ICD-10-AM codes, F70-F79 in NMDS or PRIMHD; team type code, 12 (Intellectual Disability Dual Diagnosis Team) in PRIMHD; and assigned diagnosis codes, 1208 (intellectual disability, type not specified), 1209 (learning disability, type not specified), 1210 (developmental delay, type not specified) and 1299 (other intellectual, learning or developmental disorder) in Socrates.
Ongoing Resource Scheme (ORS) funding
ORS funding information was extracted from the Ministry of Education student interventions table. ORS is a needs-based funding support provided via the Ministry of Education (Smith, 2016). ORS typically provides support to 1% of school-aged children, meaning only those considered to have the highest level of needs receive funding. For this reason, we believe the presence of ORS funding provides a robust indication for high needs cases of autism, while acknowledging that ORS funding is not always available to those who need it. An indicator reflecting whether or not an individual had received ORS funding was constructed. An individual was recorded as having received ORS funding if an intervention for ORS (intervention code = 25) was present in the student interventions table. Analysis of ORS was restricted to those who were at least school-aged, 5 years and over.
Sociodemographic measures
Sex (‘male’/‘female’) and age (0–4, 5–9, 10–14, 15–19, and 20–24 years), chosen to align with previous studies, were extracted from the IDI personal details table. As highlighted at the beginning of this manuscript, a significant limitation of the current data is the presentation of gender as a male/female binary at the exclusion of other expressions and experiences of gender. This is based on statistical standards for sex at the time of analysis, which predominantly reflects assigned sex, rather than self-reported sex (Statistics New Zealand, 2021a). A local neighbourhood indicator of socioeconomic deprivation was also established using the New Zealand Deprivation Index (NZDep) 2018 (Atkinson et al., 2020). Urban/rural profile of residence was measured using Statistics New Zealand’s classifications (Statistics New Zealand, 2016). NZDep and urban/rural are each based on the meshblock (neighbourhood) an individual lives in as at 30 June 2018. Meshblocks were determined using the address notification table in the IDI. NZDep scores were collapsed into quintiles with 1 representing the least deprivation and 5 the greatest. A binary variable was created reflecting urban/rural profile of residence was determined using the Urban Rural Indicator 2018, which is based on factors such as resident population, population density, and the extent of built physical structures (Statistics New Zealand, 2017). It can be conceptualised as reflecting urban areas (populations of 1000 or more), and rural areas (less than 1000 people).
Statistical analysis
Reporting of analyses were informed by the REporting of Studies Conducted using Observational Routinely-collected health Data (RECORD) guidelines (Benchimol et al., 2015). The autistic cohort, as at 2017/18, was described descriptively by sociodemographic sub-group. Comparisons of crude autism identification rates – the number of autistic people identified with an autism diagnosis in the data as a proportion of the NZ population – were made between Māori and non-Māori. Crude rates of ID and ORS funding were then derived at both the population level and among autistics, stratified by Māori/non-Māori. Among the autistic population, the association between each of the support need measures and Māori ethnicity were estimated separately using logistic regression models. Unadjusted and adjusted odds ratios (OR) were estimated, and variables in the adjusted models included sex, age, NZDep2018, and urban/rural profile. Two-tailed α = 0.05 is the threshold adopted in the study to determine significance.
Procedure
The June 2020 refresh of the IDI was used to access all data. These data were extracted using SAS version 7.1 (SAS Institute Inc., 2014) and analysed in Stata MP version 15 (StataCorp, 2017). All Statistics New Zealand confidentiality requirements were adhered to, including rounding to base 3, and suppression of any data where counts were less than 6.
Ethical approval
The University of Otago Human Research Ethics Committee reviewed the study for ethics consideration. The study was reviewed as a ‘Minimal Risk Health Research – Audit and Audit related studies’ proposal and was approved (reference: HD17/004). Clearance for this study and access to data was also approved by Statistics New Zealand (MAA2017-16).
Results
Participant population
The full Aotearoa ERP of 0- to 24-year olds for the 2017/2018 fiscal year contains 1,565,505 children and young people. Of those, 405,966 identified as Māori, and 1,159,539 as non-Māori; 2877 rangatahi Māori were identified as autistic, reflecting an administrative data-based prevalence rate (from herein identification rate) of 70.9 per 10,000 population. In contrast, 9084 non-Māori young people were identified as autistic, yielding a higher identification rate of 78.3 per 10,000 people. The sociodemographic characteristics of these children are presented in Table 1 alongside associated population identification rates.
Sociodemographic characteristics and autism case identification rates of the 405,966 Māori and 1,159,539 non-Māori children and young people (per 10,000 people), 2017/2018.
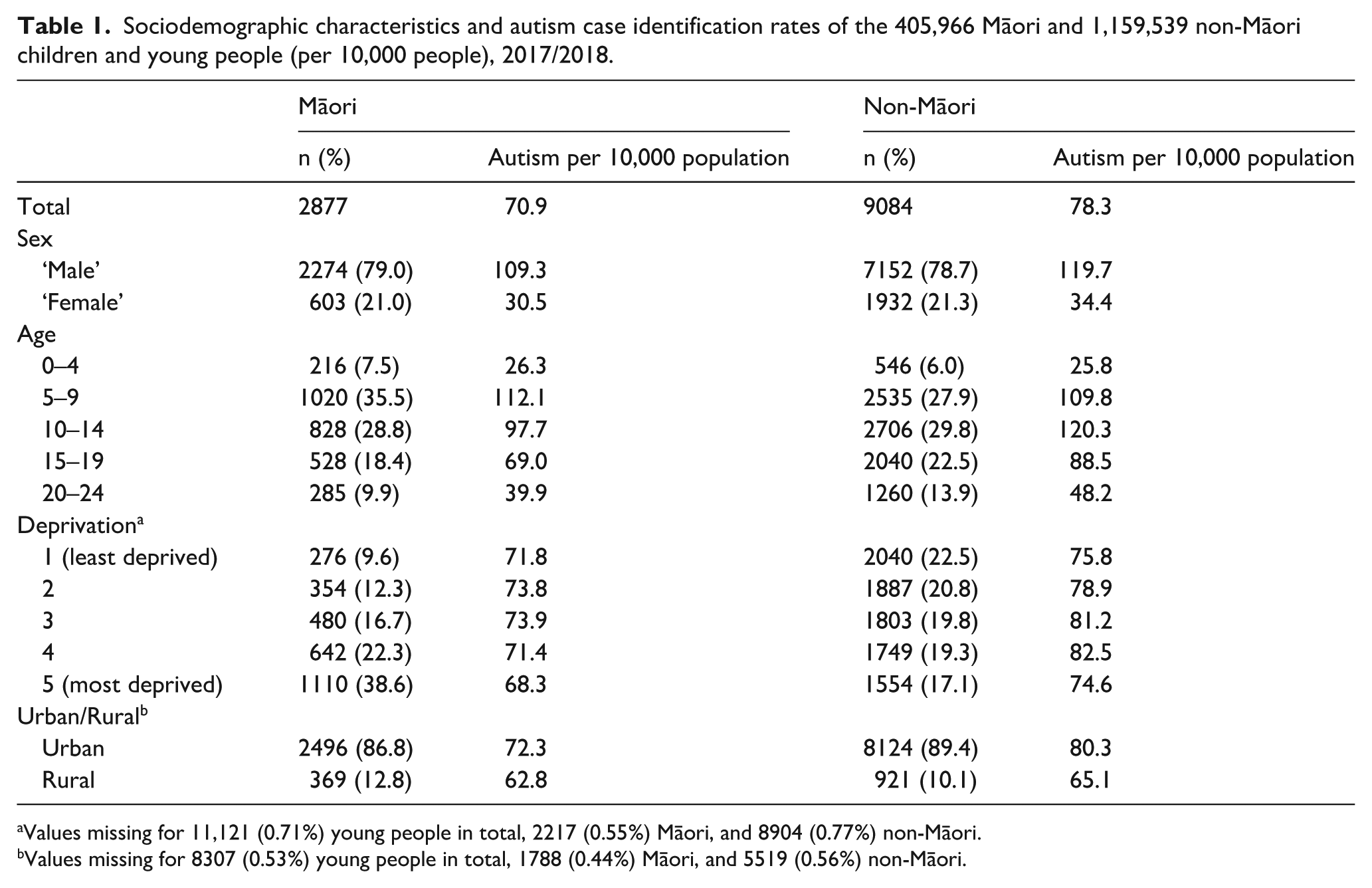
Values missing for 11,121 (0.71%) young people in total, 2217 (0.55%) Māori, and 8904 (0.77%) non-Māori.
Values missing for 8307 (0.53%) young people in total, 1788 (0.44%) Māori, and 5519 (0.56%) non-Māori.
‘Males’ comprised just under 80% of the sample of autistic rangatahi Māori, slightly more than non-Māori. The majority (64.3%) of the Māori sample were aged 5–14, while only 7.5% were aged 0–4 years, 18.4% 15–19 years, and 9.9% 20–24 years. In contrast, the age distribution among the non-Māori group was older. The vast majority of autistic rangatahi Māori (86.8%) resided in urban areas, compared to 89.4% of non-Māori.
Autism identification rates were lower among Māori across all sociodemographic subgroups except among those aged 0–4 years and 5–9 years where rates among Māori were marginally higher. In contrast, the largest difference in autism identification rates between Māori and non-Māori was in the older age groups, where Māori rates were approximately 20% lower. Identification rates among Māori were also notably lower relative to non-Māori among ‘females’ (11.3% lower).
Formal support needs
In crude analyses, among the autistic cohort, observed rates of ID and ORS funding, measures that reflect higher need, were substantively higher, 18 and 33% higher respectively, among autistic Māori compared to autistic non-Māori. For reference, observed rates among the full ERP are also presented in Table 2.
Formal support need indicators for Māori and non-Māori, under 25 years of age: All young people and autistic young people, 2017/2018.
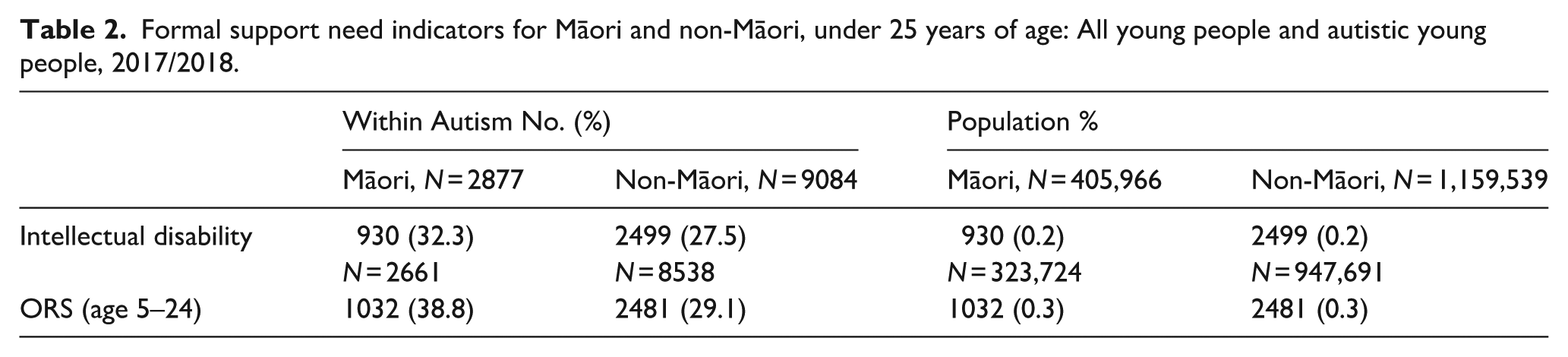
Table 3 presents unadjusted and adjusted (sex, age, deprivation and urban/rural profile) odds ratios (OR) for autistic Māori on each of the formal support need measures. After adjusting for socioeconomic differences, autistic Māori had significantly higher odds of having an ID (OR = 1.12; 95% CI = 1.02, 1.24) and being ORS funded (OR = 1.35; 95% CI = 1.22, 1.48) compared to autistic non-Māori.
Comparative odds ratios (ORs) across proxies for formal support needs in autistic rangatahi Māori young people, 2017/18.
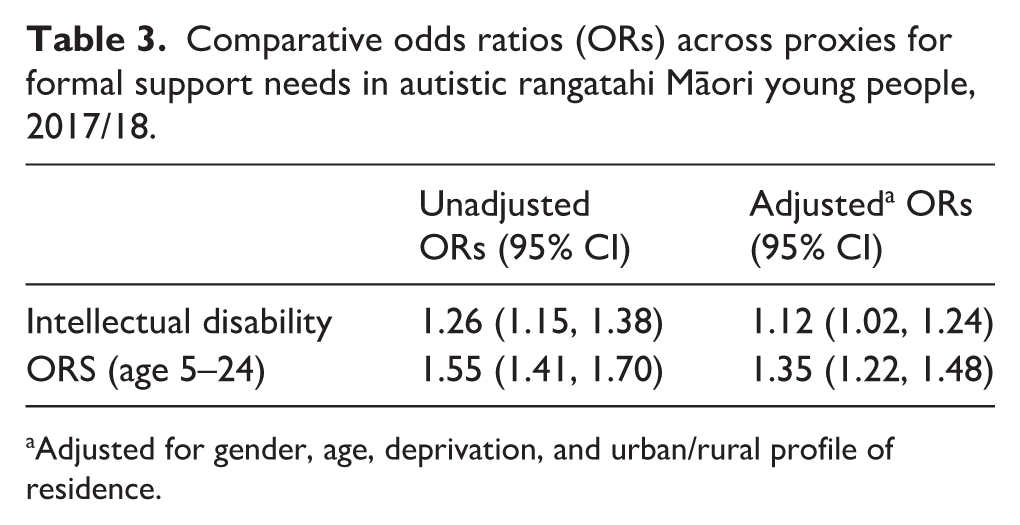
Adjusted for gender, age, deprivation, and urban/rural profile of residence.
Discussion
This study, which was co-produced with autistic Māori adults, aimed to investigate autism identification among rangatahi Māori and whether the formal support needs of autistic rangatahi Māori differ from those of their non-Māori counterparts. By employing a previously established case identification method (Bowden et al., 2020) and analysing linked population-level administrative data, we identified 2877 rangatahi Māori as autistic, resulting in an identification rate of 70.9 per 10,000 individuals. In contrast, 9084 non-Māori young people were identified as autistic, reflecting a higher identification rate of 78.3 per 10,000 individuals. Formal support needs were compared using two indicators associated with higher levels of formal support need (co-occurring ID, and receipt of ORS funding). After adjusting for socioeconomic differences, Māori had significantly higher odds of having a co-occurring ID (OR = 1.13) and being ORS funded (OR = 1.35).
Overall, autism identification rates from the current study (70.9–78.3 per 10,000 for Māori and non-Māori, respectively) are substantially higher than those reported in earlier research using the same case identification method and data until 2015/2016 (49.2–60.1 per 10,000; Bowden et al., 2020). These higher rates may reflect improvements in autism identification and diagnosis pathways in Aotearoa, enabling more children to access diagnosis. Alternatively, this increase may also be driven by expanded data coverage in the IDI captured in the present study, providing a broader window in which diagnoses can be captured. As it is not possible to disentangle these factors, this represents an important focus for future research.
The finding of a lower autism identification rate among Māori compared to non-Māori is consistent with Bowden et al.’s (2020) previous research. However, the identification rate for Māori in the current study (70.9 per 10,000) is substantially higher than the rate from Bowden et al’.s study (49.2 per 10,000). This suggests that Māori autism identification rates have increased, and the gap compared to non-Māori has somewhat closed. International literature also indicates lower rates of autism identification among underserved ethnic groups (Lau et al., 2024; Tromans et al., 2021), and a recent Aotearoa-based study found lower autism identification rates in Pasifika youth compared to non-Pasifika youth (Ruhe et al., 2022). Suggested reasons for lower identification rates typically focus on barriers to diagnosis encountered by underserved groups such as lack of culturally responsive services, systemic racism and mistrust of the health system/avoiding the health system as a safety strategy (Ruhe et al., 2022; Tromans et al., 2021).
Indeed, in Aotearoa, gaining an autism diagnosis typically requires high levels of engagement with government systems which may pose safety risks for Māori who have a long history of unfair treatment within these systems (Harris et al., 2006; Jones et al., 2024; Wilson et al., 2021). This may mean that autistic Māori who seek out a formal autism diagnosis are unable to gain one due to systemic barriers and racism. It may also solidify the resolve to adhere to a safety strategy of avoiding a racist system, and leave some Māori less likely to engage and seek a formal diagnosis for themselves or their child. It is also possible that historical trauma and ongoing racism towards Māori (Moewaka Barnes & McCreanor, 2019; Salahshour, 2021) leads some autistic Māori to feel so stigmatised that they strategically choose to mask or ‘pass as neurotypical’ to avoid further oppression and stigma. This masking often comes at a significant cost to the well-being of the autistic person (Beck et al., 2020; Cage & Troxell-Whitman, 2019; Milner et al., 2019). When autistic Māori do seek formal diagnosis, the same racial discrimination and unfair treatment may result in the inability to obtain a diagnosis.
Furthermore, current autism diagnostic practices are often grounded in the medical paradigm which takes a deficit-focussed approach to autism (Masi et al., 2017; O’Dell et al., 2016). This may not fit with a te ao Māori perspective where people are viewed holistically, as part of a wider whānau, hapū and iwi context (Bevan-Brown, 2004; Tupou et al., 2024). In a te ao Māori context, individuals who are ‘different’ are still valued and given a place and purpose, they still belong (Bevan-Brown, 2013). From this perspective, whānau Māori may not want to receive a deficit-focussed autism diagnosis. Similarly, lower rates of autism diagnosis among Māori could reflect a rejection of te ao Pākehā (Western world) understandings and diagnostic labels that are perceived as Pākehā (non-Māori; Jones et al., 2024).
Interestingly, for the cohort included in this study, comparative Māori and non-Māori identification rates varied according to age group. In the younger age groups (0–4 years and 5–9 years) autism identification rates were higher for Māori compared to non-Māori. While for the older age groups (10–14 years, 15–19 years and 20–24 years), Māori identification rates were lower than those of non-Māori. This is further evidence that the gap between identification rates for Māori and non-Māori is closing and that, over time, it has become easier for Māori to obtain an autism diagnosis. This would align with international research suggesting improved identification rates for underserved ethnic groups (Baio et al., 2018; Lau et al., 2024; Maenner et al., 2020, 2021, 2023). However, further research using a broader range of data is required to better understand any trends in identification rates over time. Ongoing monitoring using administrative data may also be useful to enable identification of any inequities and to track measures designed to reduce ethnic inequality. It also seems important to explore the pathway into autism diagnosis, both quantitatively and qualitatively, and how this might differ for Māori compared to non-Māori. This could include an analysis of the different sources of diagnosis in the IDI and whether source of diagnosis is a significant co-variate.
It is also interesting to note that identification rates among Māori differed according to geographical location with higher rates for Māori living in urban areas (72.3 per 10,000 people) compared to Māori living in rural areas (62.8 per 10,000 people). A similar pattern was also observed among non-Māori. Access to diagnostic services may be more challenging for people living rurally. Indeed, there is a substantial body of research suggesting that people who live in geographically isolated locations, such as many rural locations in Aotearoa, may face additional barriers to accessing autism services (Aylward et al., 2021; Drahota et al., 2020). This may lead autistic Māori and their whānau to relocate to urban areas to access diagnosis and support. It is also possible that rural environments better meet the needs of autistic Māori, minimising the need for a formal diagnosis. For example, living rurally may allow individuals to have closer connections with te taiao (the environment) and alignment with māramataka (the phases of the moon; Warbrick et al., 2023). It is also important to note that health services tend to be centralised in larger urban areas and the threshold used for classifying locations as ‘urban’ is very low, so current findings may underestimate the impact of rurality.
Notably, the autism identification rate among people recorded as ‘female’ was 11.3% lower for Māori compared to non-Māori. This gap suggests that Māori who were recorded as ‘female’ may have faced additional barriers to accessing an autism diagnosis. This disparity may stem from multiple overlapping factors related to the intersectionality of autistic, Māori and female/non-male identities leading to unique and compounded barriers to accessing services. Identification with multiple marginalised groups can make accessing services more challenging for autistic people yet intersectionality among autistic people is a traditionally overlooked area of research (Simpson, 2021). While the current data don’t allow for analysis of identification rates among transmasculine and transfeminine people specifically, these groups are likely to experience unique or additional barriers to autism identification and diagnosis. This is a priority area for future research.
Overall, current findings indicate that rangatahi Māori with a diagnosis of autism are more likely than their non-Māori peers to have higher formal support needs. Māori with an autism diagnosis were significantly more likely to receive ORS funding and have an ID diagnosis. Cultural values for Māori may play a role in autism identification and diagnosis (Bevan-Brown, 2004; Whaikaha – Ministry of Disabled People and Ministry of Education, 2022). For example, Māori may be more accepting of diversity and therefore more likely to include and overlook differences that don’t require high levels of formal support. There may also be bias in identification and diagnosis where lower needs cases in Māori may be overlooked, explained as ‘bad parenting’ or misdiagnosed as another condition. This would align with research from the United States indicating that Black children who present with less complex autism are at higher risk of under-identification compared to their White counterparts (Fombonne & Zuckerman, 2022). Similarly, Ruhe and colleagues (2022) found higher levels of autism complexity in Pasifika youth in Aotearoa compared to non-Pasifika youth.
The finding of comparatively higher rates of ORS funding in the current study could be perceived as positive in that it may indicate autistic rangatahi Māori and their whānau are accessing the educational support they are entitled to. Indeed, previous research has suggested that ORS funding may be more accessible than other funding such as disability support services (DSS) because education providers facilitate the application process. ORS funding goes directly to schools to enable them to create an inclusive, supportive environment for the student (Ministry of Education, 2024), so schools have a vested interest in supporting whānau to obtain ORS funding. However, it is also important to acknowledge the well-documented shortage in culturally responsive specialist supports for Māori (Berryman et al., 2015; Bevan-Brown, 2006; Tupou et al., 2024), indicating that even when rangatahi Māori receive ORS funding, it may not lead to them accessing culturally responsive educational supports. It is also worth noting that rangatahi Māori represent approximately 27% of all students receiving ORS funding (Education Counts, 2024), which aligns with their proportion in the general population (Statistics New Zealand, 2024). Thus, further research examining the underlying reasons for higher rates of ORS funding among autistic Māori is needed. Similarly, it may be useful to examine the rate of unsuccessful ORS funding applications for autistic rangatahi Māori (Noakes-Duncan, 2023).
Implications for practice and research
Several important implications for practice can be drawn from the current findings. First, lower identification rates among Māori underscore the need for more accessible, culturally responsive diagnostic services for Māori. These services should account for differences in te ao Māori and Western understandings and framings of autism. The higher rates of formal support needs observed in Māori compared to non-Māori may also indicate gaps in identifying Autism associated with lower support needs in Māori. Clinicians and other professionals should undertake cultural safety training and be educated in autism identification among Māori, with a particular focus on cases associated with lower formal support needs. It is also possible that some Māori do not desire a formal autism diagnosis for themselves or their child. It is therefore important to ensure that access to effective, culturally responsive, and timely support is not dependent upon formal diagnoses.
It may be valuable for future research to examine autism identification data from a broader time period to more closely examine any shifts in identification rates over time. Investigating the crossroads of autism, gender, and Māori identity presents a complex and valuable area for future research. This is especially relevant given the high prevalence of autistic individuals who are transgender, within a culture that traditionally values and respects the mana of both.
Furthermore, it may be interesting to explore how co-occurring diagnoses and misdiagnoses affect autistic Māori. This could include investigating rates of diagnosis among Māori for other conditions which commonly co-occur and/or share common characteristics with autism (e.g. attention deficit hyperactivity disorder, bipolar disorder, specific learning difficulties, depression, and anxiety). Co-diagnosis is not captured in the current data, and this may have important implications regarding support needs. Furthermore, there are likely to be important differences between the experiences of being undiagnosed and misdiagnosed. The current data doesn’t include this distinction and it may be valuable for future research to explore these differences.
Future qualitative research is needed to gain a more nuanced understanding of the needs and experiences of autistic Māori. Such research could include an exploration of the experiences of autistic Māori and their whānau in accessing and/or choosing not to access an autism diagnosis. Kaupapa Māori research exploring what identity means to autistic Māori and their whānau is also needed. Similarly, qualitative research is needed to better understand the support needs and preferences of autistic Māori. All future research must be conducted in collaboration with autistic Māori to ensure that it is relevant and responsive to their needs. A key strength of the current study is the inclusion of autistic Māori adults as co-researchers. This approach provides an example of how Māori autism research can be enhanced through the inclusion of Māori autistic voices. Furthermore, a broad range of autistic voices and experiences must be represented including diverse ages, genders, and backgrounds. It is also essential that non-speaking autistic people be given an opportunity to contribute using their preferred means of communication so that their perspectives can also be included.
Limitations
Several limitations should be considered when interpreting the findings of this study. First, the method used to identify the autistic population has not been validated and may not accurately capture the true number of cases of autism. Similarly, the codes we used to identify autism reflect DSM-IV codes. When the DSM-V was introduced in 2013, Pervasive Developmental Disorders, Autistic Disorder, Childhood Disintegrative Disorder, and Asperger’s disorder were combined under Autism Spectrum Disorder (Ehreta & Berkingb, 2013). Recently, questions have been raised regarding whether conditions such as Childhood Disintegrative Disorder should be considered distinct diagnostic entities, separate from autism (Mehra et al., 2019). Nevertheless, our inclusion of these codes reflects the diagnostic practices in place prior to 2013 and those available in the IDI for the present study. Furthermore, by focusing specifically on the 0- to 24-year old population, current findings only reflect autism identification rates and patterns among children and youth. Including a wider age range may have led to different findings. However, there is currently insufficient data in the IDI to enable this kind of analysis for an older age group.
In addition, the use of administrative data means that we only have access to officially recorded cases and instances of service use. The extent of our identification of Māori autism cases may be limited by the barriers to engagement with those services. This is especially true for autistic Māori who may face inequitable access to formal diagnosis and culturally responsive services and may therefore be undercounted in the current research (Bowden et al., 2020). Moreover, the case identification method, which derives the majority of its cases from for a needs assessment via disability support services, may introduce a selection bias towards those with the greatest level of need, if lower need autistic individuals are disproportionately more likely to not receive a referral. Nevertheless, the methods used in the current research have been used successfully across other studies with strong face validity (e.g. Bowden et al., 2020; Bowden, Gibb, et al., 2022; Bowden, Milne, et al., 2022; McLay et al., 2024; Mujoo et al., 2023).
It is also important to acknowledge the limitations associated with using data from the IDI for research involving Māori. First, IDI data are primarily collected for administrative, not research, purposes, often during vulnerable times for Māori such as during interactions with the criminal justice system or hospitalisation, potentially affecting data reliability and validity (Greaves, et al., 2023). In addition, there are issues with ethnicity indicators and a lack of consistency regarding how Māori ethnicity is identified (Greaves et al., 2023). This may lead to inaccuracies in identifying Māori individuals within the data. Furthermore, the data have been gathered using Pākehā concepts and measures which are mostly deficit framed, and poorly aligned to either Indigenous value systems or strengths-based analytic approaches (Thurber et al., 2020; Walter et al., 2021).
Finally, measures of formal support need used in this study should be considered proxies. Support requirements vary greatly across autistic individuals and are therefore difficult to accurately capture and measure using broad indicators such as those employed in the current study. ORS funding is arguably the best proxy as it is needs-based and involves various stakeholders in the application process which is a much more equitable process with respect to ethnicity than other forms of funding.
Conclusion
The current findings indicate that rangatahi Māori may be less likely to be identified as autistic. They also suggest that among Māori, autism cases are more likely to be associated with higher levels of formal support need compared to non-Māori. Together these findings may indicate inequities in access to autism diagnostic services for Māori. Further research is necessary to gain contextual understanding, particularly through the stories and lived experiences of autistic Māori, and to identify culturally relevant solutions from within te ao Māori. This research should be co-designed or led by autistic Māori using a Kaupapa Māori approach where the needs and priorities of the community are privileged. The current study, which included a Pou Herenga rōpū of autistic Māori ‘co-researchers’, may present one framework for this kind of approach.
Footnotes
Acknowledgements
We are hugely grateful to Susan Haldane and Matthew Matamua for their contributions to this project. This work has been enriched through your mātauranga (knowledge) and whakaaro (ideas). Aku mihi ki a kōrua (thank you to you both). Thank you also to Dr Kirsten Smiler for your contributions in the initial stages of this project.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Health Delivery Research Activation Grant from the Health Research Council of New Zealand.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.