
Abstract
Black caregivers of children with autism express that there are gaps in both knowledge and acceptance of disabilities within their communities. This lack of information and resources provided to Black communities can lead to tensions within families regarding autism diagnoses and how to support individuals with autism in their families. As part of a larger qualitative study, 23 Black caregivers of children with autism shared their experiences with the messages received from family members about their child’s autism diagnosis. Two overarching themes emerged regarding family messaging: Lack of Understanding and Denial of Autism and Supportive Acceptance and Inclusion. Six subthemes were identified that highlight the nuance within the messaging content. These findings can inform strategies to develop culturally tailored interventions to support Black caregivers in navigating the range of messages received from family members when their child receives a diagnosis of autism. Further research should build on these findings to investigate how directly this family messaging links to broader messaging in Black culture regarding autism, as well as how both family and cultural messaging may interact with factors such as awareness or use of autism resources, attitudes toward research, and long-term social and behavioral outcomes for Black children with autism.
Lay abstract
Black caregivers of children with autism say there are gaps in knowledge and acceptance of disabilities in their communities. This lack of information and resources can cause tensions in families about autism diagnoses and how to support their children. This study talked to 23 Black caregivers to learn about their experiences with the messages they received about their child’s autism diagnosis from family members. We found two main themes: Lack of Understanding and Denial of Autism, and Supportive Acceptance and Inclusion. Within these themes, parents shared different experiences, like family members denying autism exists, not wanting to learn about it, or being very supportive and inclusive. Black caregivers also talked about the emotional toll the negative messages take on them. This work is important because it can help create culturally tailored support for Black caregivers of children with autism, so that they can engage with family members in more supportive ways. Future research should look at how these messages affect the use of autism resources, attitudes toward research, and long-term outcomes for Black children with autism.
Early intervention for autism is believed to provide the greatest opportunity for improving outcomes and quality of life (Dawson et al., 2010; Kasari et al., 2010; Zwaigenbaum, Bauman, Choueiri, et al., 2015). Access to autism-specific early intervention typically relies on receipt of a diagnosis of autism spectrum disorder (ASD), which is often inaccessible to many families who are hindered by years-long waitlists and variable access to services based on geographic proximity and resources. For Black families, these delays are even greater, with Black children with autism experiencing delays in diagnosis on average 3–4 years after their parents’ first concern (Constantino et al., 2020). These delays to diagnosis and intervention lead to disparate functional outcomes for Black individuals with autism, who, according to population-level monitoring by the Autism and Developmental Disabilities Monitoring Network, experience intellectual disability almost two times as often as White individuals with autism (Baio et al., 2018; Hughes et al., 2023). Despite this documented history of delay, the prevalence of autism among Black children is currently higher than among White children. This shift may indicate a “catch-up” in previously missed diagnoses and underscores the need to improve the current framework for support and services (Maenner et al., 2023; Kasambira Fannin et al., 2024). In addition, although the number of Black children receiving diagnoses has increased, racial disparities persist regardless of whether the diagnoses occur early or late (Onovbiona et al., 2024).
Delays in diagnosis are not only detrimental to developmental outcomes but also have been correlated with increased parental stress (Zwaigenbaum, Bauman, Stone, et al., 2015). In a study by Dababnah et al. (2021), Black caregivers of children with autism reported key stressors such as feeling trapped in their role as a caregiver, fear of hyper-negative perceptions of their child’s behavior because of their race, and inadequate parental mental health support. In addition, caregivers reported feelings of isolation from their families, particularly in terms of generational and ideological differences in child-rearing. Relationships between Black caregivers and their families are particularly important for families of children with autism, as Black caregivers have reported that family support is a primary form of support when coping with the challenges of parenting a child with autism (Lewis et al., 2022).
Black caregivers of children with autism express gaps in both knowledge and acceptance of disabilities within their families and communities (Burkett et al., 2015), which impacts the messaging that they receive about their child’s behavior and diagnosis. In a qualitative study focused on cultural messaging, Black caregivers of autistic children reported that they experienced negative cultural messaging of denial, stigma, and shame related to having a child with autism (Dababnah et al., 2018). Other qualitative work reported that some Black caregivers felt that the messaging that they received from their family prior to receiving a diagnosis of autism minimized their concerns and delayed attainment of an autism diagnosis (Pearson & Meadan, 2018). Additional qualitative work by Lovelace et al. (2018) reported on three Black mothers’ experiences with their family’s messaging during the diagnostic journey. Their sample reported a universal lack of understanding of autism from family members, paired with messaging encouraging them to avoid seeking a diagnosis or treatment for their child, resulting in feelings of isolation.
Family messaging (i.e. the verbal and behavioral messages received by caregivers from their family members) is an integral contributor to the experiences of caregivers of children with autism. This study aims to expand on previously published work by deepening the examination of the range of family messages received by Black caregivers of children with autism throughout the diagnostic journey and beyond. This study reflects the collective experiences of 23 Black caregivers of autistic children, reporting both the strengths and challenges of family messaging they receive regarding autism. Family messaging can provide insight into how families conceptualize disability, how they engage with healthcare systems, and how they advocate for their child with autism. As the family unit is a critical tenet of support for Black families (Sarkisian & Gerstel, 2004), understanding familial and cultural dynamics is essential for clinicians to develop interventions that promote the well-being of Black children with autism and their caregivers. This article seeks to add to this body of knowledge by using qualitative methods to examine family messaging received by Black caregivers of autistic children about their child’s autism diagnosis. This study was designed to explore experiences of Black families specifically, and not to compare to other populations whose experiences may overlap or diverge.
Methods
Research team positionality and community involvement
The authorship team of this article comprises a diverse group of researchers and collaborators, whose identities and experiences shape their perspectives and approaches to the study. The team includes authors who identify as Black (n = 2), Latina (n = 2), and White (n = 3). Among the authors, four are parents, one of whom has a child with autism and two of whom have children with other special healthcare needs or disabilities. In addition, one author has a sibling with autism. The team’s composition allowed for members who shared aspects of their identity with the participants to offer expertise and guidance in interpreting the data through their lived experiences, ensuring cultural responsiveness.
The study’s third author, Felicia Williams Brown, a Black mother of son with autism and an autism advocacy professional, served as a community/perspective consultant for the entirety of the project as a paid collaborator on the grant that funded this work. Prior to beginning data collection, Felicia contributed by collaborating on the development of the interview guide, consulting with the interviewer on interview style and approach, including co-developing a positionality statement to be used at the start of the interview. Felicia also participated in a mock interview with the interviewer to provide feedback on interview flow, length, and phrasing of questions. During data collection, Felicia provided ongoing consultation to the interviewer, for example, offering strategies to remain culturally responsive and reflective after a challenging interview. She also provided feedback after completion of the first five interviews, suggesting changes to interview question formats to garner more robust responses. During data coding, she reviewed and approved the final codebook. During the final stages of data analysis, we engaged with Felicia in a discussion of the identified themes and subthemes, which informed confirmation of the themes and interpretation of the results. In addition, she helped select illustrative quotations to include in the final publication. Finally, Felicia contributed as a co-author to the resulting article. A summary of the contributions of each author can be found in Table 1.
Chronology of qualitative methodology and team member contributions at each stage.

Note. Filled circles indicate that the team member was involved in that stage of the research.
Procedure
In this study, we utilized the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist to ensure the rigor and transparency of our qualitative research. The COREQ checklist, developed by Tong et al. (2007), comprises 32 items that guide the reporting of qualitative studies that utilize interviews and focus groups. By following these criteria, we aimed to provide a comprehensive and detailed account of our research process. The completed COREQ checklist is included in Supplemental Appendix 1.
Data for this study were collected as part of a larger qualitative study titled “Barriers to participation in autism infant sibling research for Black families: a qualitative and quantitative approach.” The study interviewed Black caregivers of children with autism to learn about their experiences and perspectives about autism research, including barriers, concerns, facilitators, and/or motivators that Black families might experience. In addition to these primary aims, the interviews also gathered information about participants’ experiences receiving a diagnosis of autism for their child and their perceptions of how their race and culture may have influenced their experiences. For this article, we focused on messages received by participants from their family members regarding their child’s diagnosis of autism and subsequent support needs.
Families were recruited through online and physical flyers that stated, “We want to hear from you! We are conducting interviews with Black/African American caregivers to learn about their opinions and experiences with autism research.” Online flyers were posted in subreddits focusing on ASD, such as “r/autism,” as well as Facebook groups such as “Autism Society of North Carolina,” “Black Proud Parents Children with Autism,” and “Autism and Asperger’s Awareness.” Families were also recruited through an existing registry at the University of North Carolina at Chapel Hill, consisting of families who had consented to be contacted about research opportunities. Interested families completed an eligibility screening survey. Eligible participants were 18 years or older, had at least one child diagnosed with autism, and identified as Black or African American. Participants consented to have their interviews recorded and utilized for the study. This study was approved by the University of North Carolina Institutional Review Board (IRB) (#21-3094).
Each participant completed one qualitative interview, which lasted between 60 and 90 minutes. Interviews were administered by the Principal Investigator (PI) of the parent study, a female, PhD-level licensed psychologist. The interviewer has over 10 years of experience working with families with autism and conducting clinical interviews. In addition, the interviewer attended multiple training courses on qualitative research interviewing, specifically, prior to conducting this study. The interviewer did not have any existing relationships with study participants prior to conducting study interviews. In acknowledgment of the racial mismatch between the interviewer and the participants (i.e. the interviewer is White), all interviews began with a positionality statement acknowledging the interviewer’s lack of expertise in the Black lived experience, and a desire to create an environment where participants could feel comfortable speaking candidly about their experiences. The study overview, research goals, and positionality statement used as part of the interview guide are included in Supplemental Appendix 2.
The interviews were conducted via phone (n = 22) or Zoom (n = 1, although video was not utilized) and followed a semi-structured interview guide with four primary content areas: family/community, opinions about research, reducing barriers in research, and future directions in research. Questions relevant to this article existed in the family/community section, such as “What were the feelings and responses of other members of your family [when your child was diagnosed with autism]?” and “Do you think these feelings and responses are unique to Black families with autism? Why or why not?” The interview guide was developed collaboratively with an expert in qualitative research methods (M.G.) as well as the study’s community consultant (F.W.B.). Interviews were audio- recorded for later transcription. After the interview, participants completed a brief electronic survey collecting demographic data (e.g. age, state of residence, family income).
Data analysis
Interviews were transcribed through a multistep process to ensure accuracy. First, interviews were auto- transcribed using Microsoft Word. Each transcription was then reviewed alongside the audio recording by a member of the study team to correct any errors accrued during auto-transcription. All transcripts were then reviewed by a second team member, different from the original transcriber. Any remaining discrepancies were resolved by the PI.
Qualitative content analysis was employed to systematically code and categorize the data, allowing for the identification of key themes. The initial codebook was derived from the interview guide through negotiated consensus by four members of the team, including the PI (K.E.C.), the study coordinator (K.M.), a senior research assistant/first author of this article (D.M.), and the qualitative consultant (M.G.). A hybrid coding framework was used, with a combination of a priori codes based on the study’s primary research questions (i.e. barriers and facilitators to participating in autism research for Black families) and codes that emerged from the interview data. Each team member coded two transcripts independently and then met to develop consensus codes. A third transcript was coded by K.E.C, D.M., and K.M. to confirm established codes and add any additional codes, which resulted in the final codebook. The final codebook was reviewed by the study’s qualitative consultant (M.G.) and approved by the study’s community consultant (F.W.B.), who did not suggest any changes. The remaining transcripts were coded by D.M. and K.M. using the qualitative coding software Dedoose (2021).
For this study, participant responses coded under “family views on autism” were analyzed. According to the established codebook, coders were instructed to use this code “when participants describe the opinions, experiences and beliefs of their family members about autism spectrum disorder or having a family member with autism spectrum disorder.” The code report from the “family views on autism” code was generated. We then used an iterative team-based process to identify and summarize themes within the code report. After a team discussion of the content, one analyst (D.M.) conducted an initial analysis of the code report, labeling each excerpt with the applicable theme. This work was reviewed with a second analyst (K.C.) to refine and finalize themes. D.M. and K.C. then reviewed all excerpts for each theme identified within the code report to describe themes and identify salient quotes. Thematic saturation of our coding of the “family views on autism” content was confirmed through the analysis process, where no new subthemes were identified after interview number 11, and the established six subthemes became recurrent. Results of the analysis were reviewed with F.W.B. (i.e. validation) before finalization, who approved the results and did not suggest changes.
Results
Participants
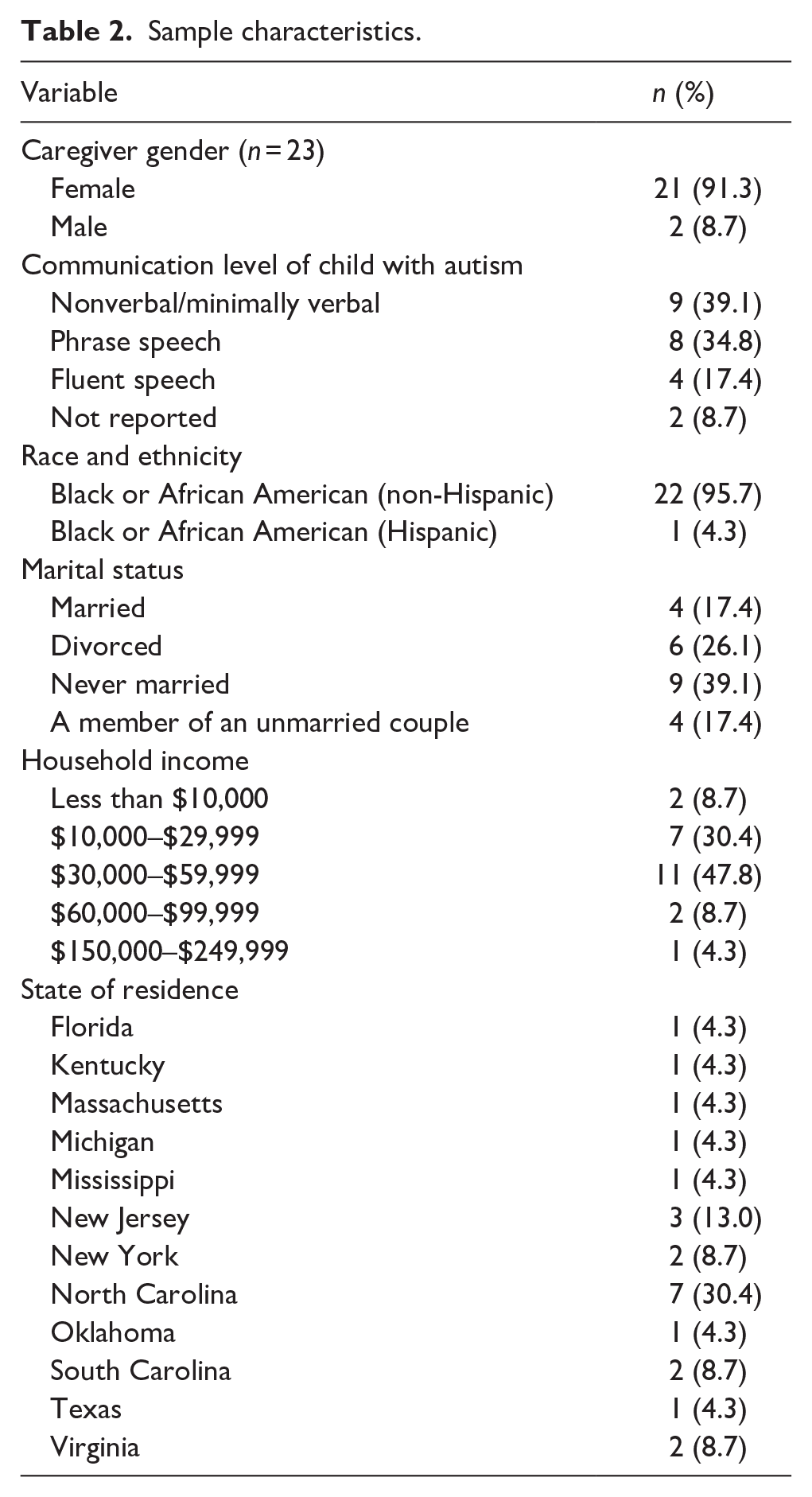
Caregivers (n = 23) participated in this study between August 2022 and February 2023 (91.3% female, 8.7% male). In total, 25 participants consented to participate in the study; however, two were lost to follow-up after requesting to reschedule their initial interview appointment. All participants identified as Black or African American caregivers of at least one child with autism. Two caregivers had two children with autism. One participant also identified as Hispanic. Given that the caregiver’s experience was the focus of the study, participants were not asked to report their child’s racial or ethnic identity. The greatest proportion (30.4%) of participants lived in North Carolina, with the remaining participants residing in 11 states across the US. participants were aged 31–50 years (m = 38.2 years) and had household incomes that ranged from less than $10,000–$250,000. Participants were compensated for their time with a $50 gift card. Communication level of the caregiver’s child with autism (or the oldest child with autism in multiplex families) was determined based on qualitative parent report of current language level (i.e. caregivers were asked open-ended questions about their child’s current communication level and support needs around communication). Participant demographics are summarized in Table 2.
Sample characteristics.
Two primary themes and six subthemes emerged from the interview data (see Figure 1). The two primary themes included (1) Lack of Understanding and Denial of Autism (reported by 11 caregivers), and (2) Supportive Acceptance and Inclusion (reported by 5 caregivers). Three caregivers reported family messaging under both themes, and four participants did not share experiences with family messaging in their interview.
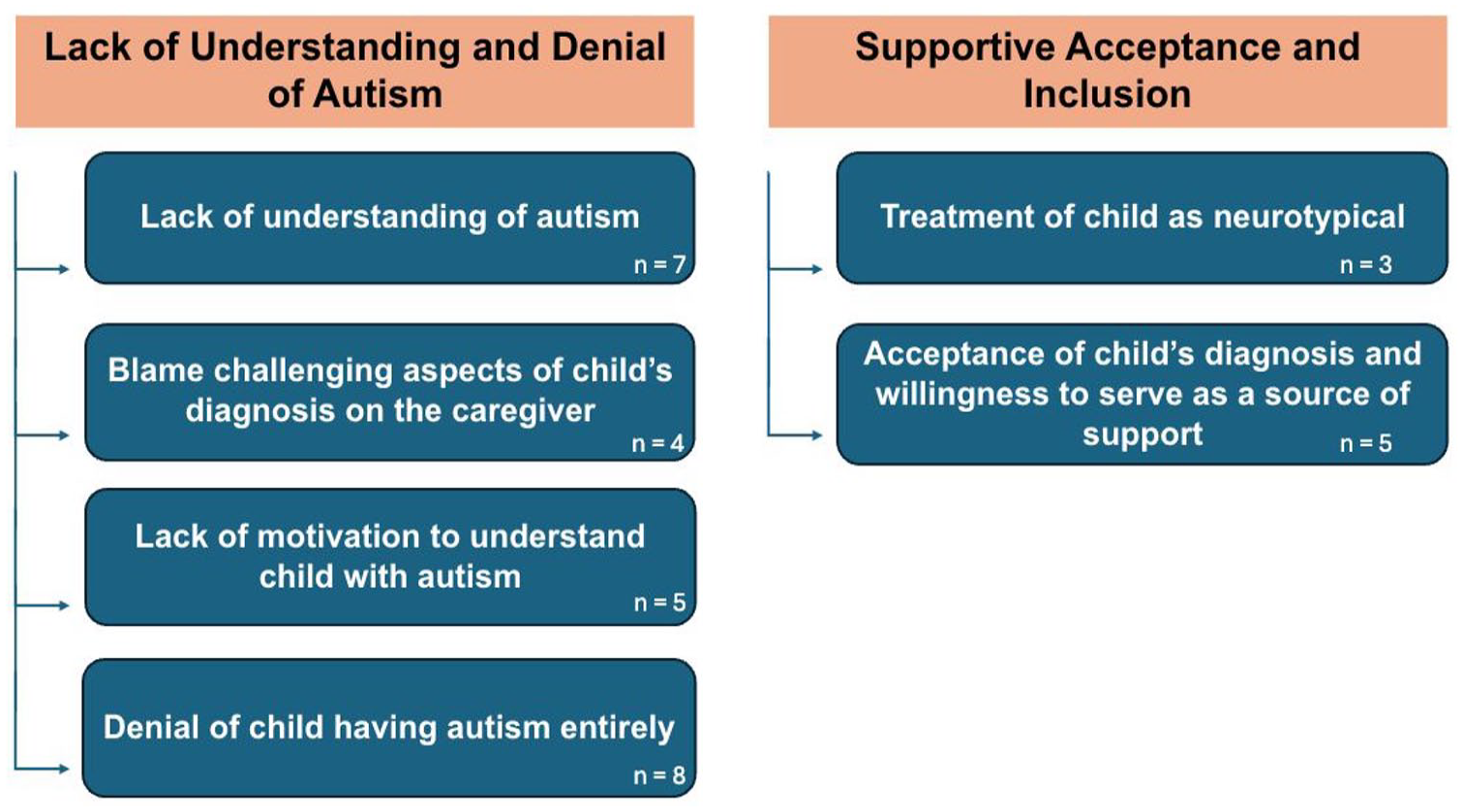
Family messaging themes and subthemes.
Lack of understanding and denial of autism
Lack of understanding of autism
Many caregivers expressed concerns regarding a lack of understanding from family members of the child with autism and their diagnosis. Most commonly, caregivers expressed passivity from their families regarding their child, in that although their family members are involved in the lives of their child and their views are not directly harmful, autism remains an uncomfortable topic in their household and is difficult for the caregiver to navigate. One caregiver expressed that their family has the mindset that “it ain’t their child so they don’t have to deal with it.” Another caregiver stated that talking about autism is a “sensitive, touchy conversation,” due to a lack of understanding of autism. This lack of understanding sometimes perpetuates a lack of emotional and logistical support from family members. One caregiver attributes this lack of understanding to a lack of formal education of her family members.
I have a lot of aunties and uncles that didn’t finish high school and stuff. They don’t really understand it. So when I’m around them and my son is doing certain stuff, they don’t understand. Like, “Oh, this is what people do with autism.” Like, “No, you need to whoop him.” Like, no . . . I don’t. I don’t. He doesn’t understand. This is why he’s doing that. So, they don’t really understand. (Mother, 33 years old)
A few caregivers who did not have a theory regarding why this lack of understanding occurs, however, expressed that their family members have an incorrect perception of autism, such as family members using the word “retarded” to refer to their child’s developmental disability. Another caregiver who has multiple children with autism expressed that it was difficult for her father to understand her children’s diagnoses because of the phenotypical variability in autism:
My father, it’s hard for him. He can see [CHILD]’s diagnosis very easily and so it’s not hard for him to accept [CHILD]’s diagnosis . . . but for my other kids since they’re more high functioning, it’s hard for him to see it. So, he doesn’t believe so much that they have autism. (Mother, 43 years old)
Lack of motivation to understand child with autism
Several caregivers reported a lack of motivation of family members to understand their child with autism. This is distinctive from the prior theme as this messaging highlights that family members lack both the understanding of autism and the motivation to expand their knowledge. Caregivers described that family members do not “care to understand” or that family members “never took the time” to understand their child. One caregiver explained this through the analogizing of developmental disabilities and a blood disorder:
We were in a car going somewhere and the girls were in the car as well and my mother said something, it was a little disrespectful or whatever, and I said, hey, if [CHILD] had sickle cell, you would research it. If she had some other kind of, like say disease or illness you would look it up. . . . I said though, because she has autism. You’ve never gone to a workshop about autism. You’ve never gone. (Mother, 51 years old)
Some caregivers also emphasized the frustration of continuously trying to demonstrate how to best love, support, and care for their child, eventually “giving up” on repeated explanations. One caregiver stated that “after that first attempt and I see there’s no, you know, trying to understand, we just, we stop coming around.” Another caregiver highlighted her own efforts in stating that if she had to educate herself on autism, her family members can too:
. . . [CHILD] had a whole full meltdown and everybody was like, “Oh my God. Why didn’t you tell us he had a bad temper. Why didn’t you tell us this?” I told y’all he had autism . . . I don’t know if y’all researched autism and see what that’s about, but if you haven’t, I encourage you to. I’m not gonna do your research for you. I had to do my own research and you need to do the same. (Mother, 35 years old)
Blame of challenging aspects of child’s diagnosis on the caregiver
Some caregivers shared experiences of feeling blamed for their child’s autism diagnosis, as well as for challenging behaviors they associate with their child’s diagnosis such as “talking out” and “making a mess of things.” One caregiver described family members questioning the caregiver for seeking a diagnosis, stating, “People look at me funny because I did get him tested” and questioned why the caregiver would “let them put that label on him.” One caregiver stated that her parents expressed feelings that she and her partner “weren’t being good parents to [their] son.” Another caregiver experienced similar messaging from the child’s grandparents on both sides:
All I have to say is, as a Black family with a son that’s autistic, it was a horrible experience. Not just on a social level as far as like, outside of the home, as far as like school and stuff. But even within the family. For the longest time his grandparents on both sides—they tried to blame his condition on me and my husband by saying that we wasn’t raising him right. Especially when he would have a tantrum. (Mother, 42 years old)
One caregiver highlighted that her racial identity has affected her experience in how her family perceives her parenting:
I think basically, me being Black with a child with autism, I feel like sometimes, people don’t take you seriously about autism. Sometimes I feel like if I go to a person of another race with my concerns, they understand me. But, you know, my family, for one, they’ll say like, “nothing is wrong with him,” ‘he’s just a boy.’ It’s just, ‘he’s the first child, first child syndrome,’ and ‘you don’t have him around other kids.’ (Mother, 33 years old)
Denial of child having autism entirely
The final subtheme under lack of understanding and denial of autism is family members’ denial of the child having autism entirely. Four different caregivers expressed family members using the specific phrase that there is “nothing wrong with” the child with autism, occasionally with the addition that symptoms would alleviate with time and a “typical” parenting approach. For example, one caregiver shared,
Well, I would say my family kind of like look past it. They kind of have this, this idea like if we treat [CHILD] normally then he’ll just be a normal kid. (Mother, 35 years old)
Other caregivers described their family members labeling autism as “a White people disease,” that they think autism is “a bunch of crap,” or that they “kind of [act] like it doesn’t exist.” A variety of different phrases were used to deny that a diagnosis of autism is real or accurate. Some caregivers acknowledged that this denial of autism also occurs in other racial groups. For example, a participant shared,
Even in the very beginning with my son, you know, “ain’t nothing wrong with that boy he’ll be able to talk.” And once again, that does come with a level of denial which I have learned is across the board, regardless of race. (Mother, 46 years old)
Finally, caregivers whose quotes fell under the theme Lack of Understanding and Denial of Autism sometimes reported how this messaging impacts their well-being by concluding experiences with statements referencing their own emotions, such as “that was tough,” “nobody understood where I was coming from,” and “it was a horrible experience.”
Supportive acceptance and inclusion
Acceptance of child’s diagnosis and willingness to serve as a source of support
Several caregivers expressed that they had family members who were accepting of their child’s diagnosis and functioned as a source of support. This support includes asking questions such as “What can we do to support?” or “being really engaged in wanting to learn more about [autism].” Other forms of support include family members “[understanding] the situation” and helping with logistics such as providing childcare. One caregiver emphasized that the professions of her family members have a positive influence on how they assist the caregiver with navigating her child’s diagnosis:
I have a lot of nurses in my family and things like therapists and psychologists—‘cause I’m a nurse. So they kind of understand where I’m coming at. They helped me a lot with telling me stuff I can do for him or, certain foods I shouldn’t give him and what makes it worser and stuff and what studies have shown. (Mother, 33 years old)
Treatment of child as neurotypical
The last subtheme encompassed the desire of the caregiver’s family, and occasionally by the caregiver themselves, to treat the child with autism as a neurotypical child. For example, a caregiver shared,
They don’t treat him any differently just because he has autism because that’s not how it works in the real world. They love him though, but we don’t treat him any differently; I treat him just as I would if he was a normal functioning child. (Mother, 38 years old)
One caregiver noted that they “are the difference” regarding educating their family about developmental disabilities and views their family treating the child as any other child as an indication of success. Although similar to the sentiment that there is “nothing wrong with” the child, these caregivers are expressing that family members accept the autism diagnosis and view their child in a positive light. Another caregiver emphasized,
Everybody is pretty much on track. They have to get on track. We all treat him the same way. We all allow him to have his independence. We all try to allow him to be his own person, so I don’t feel like anybody directly around me, treats him any different or does not have the same feelings or the same concerns as I do. Everybody’s pretty much the same as far as like in my family, immediate family, grandparents. (Mother, 36 years old)
Discussion
This study contributes to the literature by focusing on the content and valence of the messages about autism communicated by family members of Black caregivers of children with autism. We identified two recurring themes regarding the content of this family messaging described by caregivers who participated in our study: Lack of Understanding and Denial of Autism and Supportive Acceptance and Inclusion. Within each theme, we identified multiple subthemes that encompass a variety of family messages. In reporting on these themes, we propose next steps for practitioners in supporting Black caregivers of children with autism aimed at improving well-being derived directly from community partners’ shared experiences.
Themes of denial and lack of understanding have emerged in other qualitative interview studies with Black caregivers of children with autism (Dababnah et al., 2022; Fisher et al., 2022; Pearson & Meadan, 2018). Black families report high levels of this stigma (Rivera-Figueroa et al., 2022) as well as a vital dependence on their families for support (Burkett et al., 2015). Discrimination and systemic racism in the United States has necessitated a strong reliance on family and community for Black Americans (Dilworth-Anderson, 1992), and Black families have expressed the importance of clinicians who understand these aspects of their cultural background and values (D. R. Jones et al., 2020).
This work expands on the previous literature in two important ways. First, it focuses specifically on messaging received from family members, in contrast to previous qualitative work that focuses on broader perspectives from Black caregivers of children with autism such as views on religion, coping, stress, and services surrounding their child’s diagnosis (Crais et al., 2020; Dababnah et al., 2018, 2021; Lewis et al., 2022; Lovelace et al., 2018; Pearson & Meadan, 2018; Pearson et al., 2021). Second, our analysis distinguished between lack of understanding from family members (i.e. limited or no content knowledge about ASD) and lack of motivation to understand from family members (i.e. rejection of information, declinations to further their knowledge). In the former (i.e. lack of understanding), caregivers report uneasiness from their families regarding their child’s autism diagnosis. They express that autism is a “touchy conversation” as well as a source of confusion for family members, of which caregivers cite theories such as lack of education and difficulty perceiving the heterogeneity in behavioral phenotypes of the autism spectrum. In contrast, caregivers who receive lack of motivation to understand messaging directly express frustration when family members either do not care to understand or repeatedly ignore their efforts to explain their child’s diagnosis and support needs.
Caregivers who express lack of motivation to understand family messaging highlight the difficulty of motivating their family members to take the time to learn about their child. There is a sense of fatigue associated with this subtheme; some caregivers report giving up on educating their family about autism, something that is not discussed as part of the lack of understanding subtheme. This distinction is especially important in considering the role of clinicians, as the efficacy of interventions may differ based on family dynamics. Approaches to supporting Black caregivers may need to be individualized based on the type of messaging they are receiving. For example, caregivers who express receiving lack of understanding messaging may benefit from resources that they can share with family members to improve understanding. These families may also be ready to engage in family support services or interventions that include extended family members. In contrast, caregivers who express receiving lack of motivation to understand messaging may require more support from clinicians in building skills to engage with family members to increase motivation to learn. In addition, these caregivers may find culturally specific support groups (e.g. The Color of Autism, Black Autism Moms) especially helpful in coping with this type of family messaging, as it was reported to be associated with more negative emotional impacts on caregivers.
This study highlights the emotional toll that receiving negative family messaging can have on caregivers of Black autistic children, especially during the time of receiving a new autism diagnosis, which as Crais et al. (2020) report, caregivers consistently describe as overwhelming. Though we did not inquire specifically about how the reception of negatively valanced family messaging impacts their well-being, caregivers spontaneously described feeling negatively affected. Improving caregiver well-being is essential, for both the caregiver and their child. A caregiver’s well-being is entangled with the well-being of their child (ten Hoopen et al., 2020), and Black caregivers are at a double disadvantage as caregivers of a child with a disability and coping with stress related to systemic racism and discrimination (S.C.T. Jones et al., 2020). With this knowledge, clinicians can implement preventive care by normalizing the range of family messages and offering coping support to promote positive mental health. In addition, an essential means of coping with family messaging lies in family support groups for Black caregivers with children with autism. They serve as a support system and a way to exchange resources and information about caring for their child with autism based on lived experience. These groups can also address feelings of isolation often reported by Black caregivers (Stahmer et al., 2019) and foster community.
A common family message that participants reported receiving was that there is “nothing wrong with” the autistic child. Although this phrase was typically captured under the Lack of Understanding and Denial of Autism theme, we see similar messaging under the Supportive Acceptance and Inclusion theme. Caregivers expressed that they feel supported by their families when they treat their child as they would a neurotypical child. However, in an effort for inclusion and acceptance, treating an autistic child as “normal” may, in effect, be denial through a different lens. This messaging of intentioned equality in treatment (e.g. “They don’t treat him any differently just because he has autism because that’s not how it works in the real world”) may be directly linked to fear of discrimination and repercussions in a racialized society. By centralizing equality in their treatment of children with autism, family members may unintentionally impact equity by minimizing the need for supports or accommodations necessitated by their autism diagnosis. To prevent this possible barrier to interventions for children with autism, clinicians may want to discuss that aiming toward “normalcy” rather than tailoring interventions to the child’s specific needs may hinder their development and independence. Clinicians should also emphasize that an autism diagnosis is not solely attributed to negative characteristics and take care to focus on their child’s strengths.
Caregivers who expressed experiences under the Supportive Acceptance and Inclusion theme reported inclusive and understanding family members that transcend passive acceptance into actions that improve the well-being of both the caregiver and their child. For example, though one caregiver expressed she believes her family’s lack of understanding is rooted in a lack of education, another caregiver expressed how grateful she is to have a family full of scientists who support her and her child. Families are adaptive and capable of change, and because of this, there is a critical need for programs focused on empowering and educating the Black community on supporting families with autism. One example of this is FACES, a 6-week parent-training intervention for Black parents of children with autism (Pearson & Meadan, 2021). The FACES program seeks to increase advocacy and empowerment in Black caregivers of children with autism while increasing feelings of community. Understanding family messaging within Black families regarding autism aids in creating culturally tailored programs, such as FACES, that effectively address disparities in autism diagnoses and interventions.
Limitations and implications
While a critical addition to the literature, this study has a few inherent limitations. First, like other qualitative studies, the results presented in this article are not intended to be generalizable. Therefore, while they illustrate the experience of the Black families we interviewed, these themes may not apply to all Black families. In addition, caregivers of autistic children of different races may have similar or different experiences; however, those were not examined in this study and we do not intend for our results to be interpreted through a comparative lens. Second, while we documented caregivers’ self-reported racial and ethnic identity (with only one participant identifying as Black Hispanic), we did not document culture of origin across participants and their family members. Therefore, we are not able to differentiate across cultural nuance within the US Census umbrella term of Black. For example, caregivers whose parents are African immigrants may receive different messaging than caregivers who are from multigenerational American families. In addition, both groups may receive different messaging than caregivers who come from a mixed-race or ethnically diverse family. Our study also lacks representation from Black male caregivers, as only two participants identified as male. Finally, the interviewer in this study was not Black. Although the interviewer acknowledged this racial discordance in an effort to increase comfort and build rapport during the interviews, the effects of this racial mismatch may have impacted the participants’ comfort speaking with complete candor and authenticity to their lived experience (Marcucci, 2024). We have attempted to mitigate this limitation by collaborating with a racially matched community partner (F.W.B.) and research team members (D.M.) through each stage of the research process (i.e. study design through dissemination). In addition, our findings are consistent with previous qualitative work in this area conducted with racially matched interviewers (e.g. Lovelace et al., 2018; Pearson & Meadan, 2018), suggesting that the racial mismatch between interviewer and interviewees in our study may have had minimal impact on our findings. Finally, we did not collect racial identities of the autistic children of the caregivers. Therefore, we have not been able to address nuance that may exist in the messaging received in multi-racial or multi-ethic Black families.
Building on these findings, future work should focus specifically on how family messaging translates into caregiver behaviors and thus impacts developmental outcomes and family well-being. It should continue to engage community partners to design culturally tailored interventions to support Black caregivers in coping with and responding to negative family messaging. This work should also build on the individual strengths reported by these caregivers, combined with known strengths within the Black community at large. Furthermore, studies should seek to explore the heterogeneity within the Black racial identity, recruit additional male caregivers, and consider having a Black interviewer to assess for possible variability in results. Finally, these findings would be well suited to inform a quantitative examination of these themes to determine whether these findings can be generalized, and whether they may be shared across racial groups.
Community partner reflection
I am Felicia Williams Brown, a dedicated Black mother to a son with autism, a perspective consultant for this exceptional research project and third author on this article. Utilizing my personal experiences and professional background in intellectual developmental disabilities, this endeavor has shed light on the complex challenges faced by Black families dealing with autism. The findings were not only insightful but also encouraging.
Our community is keenly aware of the unique struggles Black families encounter, yet this project has further revealed the harm caused by negative narratives within our own community. It highlights how societal pressures promoting Black excellence clash with the reluctance to accept an autism diagnosis. It also affirms that the Black community is more aware of autism, but the pain is further exacerbated by a lack of inclusivity or commitment to make needed adjustments for accommodation.
The heartbreaking stories these families share deeply resonate with my own experiences, exposing layers of difficulty and obstacles unique to our community. From facing skepticism about their concerns to advocating for their child’s needs in various settings, the isolation, pain, and exhaustion felt by our families are tangible. It seems that our community and society often question our knowledge about our own journey, making us doubt our intentions or efforts in seeking help for our children. Despite this, we are more than just caregivers—we are pioneers, innovators, and resilient individuals navigating through systemic challenges and enduring cultural traumas ingrained in our history. This innovative research not only uncovers some of the underlying barriers hindering progress within the Black autistic community, but it also sets an example for fostering understanding moving forward. The integrity of this initiative is commendable, providing valuable insights that will empower and uplift the Black autistic community amid its struggles.
Active inclusion of Black families in autism research is essential for progress in diagnostic methods and treatments for autism. As a proud Black mother of an autistic child, I am hopeful for a better future through initiatives like this research project. It has recognized and has overcome cultural challenges while still embracing the enthusiasm of Black families striving for positive outcomes within the autistic community. Thank you so very much for the privilege to witness and participate in such a wonderful opportunity.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251361604 – Supplemental material for Navigating family messaging: Qualitative experiences of Black caregivers of children with autism
Supplemental material, sj-docx-1-aut-10.1177_13623613251361604 for Navigating family messaging: Qualitative experiences of Black caregivers of children with autism by Dalia Marquez, Kattia Mata, Felicia Williams Brown, Mary E Grewe, Joseph Piven and Kelly E Caravella in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613251361604 – Supplemental material for Navigating family messaging: Qualitative experiences of Black caregivers of children with autism
Supplemental material, sj-docx-2-aut-10.1177_13623613251361604 for Navigating family messaging: Qualitative experiences of Black caregivers of children with autism by Dalia Marquez, Kattia Mata, Felicia Williams Brown, Mary E Grewe, Joseph Piven and Kelly E Caravella in Autism
Footnotes
Ethical considerations
This study was approved by the University of North Carolina Institutional Review Board (IRB).
Consent to participate
Informed consent to participate was both written and verbal.
Author contributions
Felicia Williams Brown: Formal analysis; Methodology; Writing—review & editing.
Mary E Grewe: Formal analysis; Methodology; Supervision; Writing—review & editing.
Joseph Piven: Conceptualization; Funding acquisition; Writing—review & editing.
Kelly E Caravella: Conceptualization; Formal analysis; Funding acquisition; Investigation; Methodology; Writing—original draft; Writing—review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UM1TR004406. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Deidentified data utilized in this manuscript are available via direct request to the senior author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.