
Abstract
Autistic children are less likely to participate in sport than non-autistic children, but we know little about how patterns of participation in team and individual sport change across childhood. Drawing on a nationally representative cohort of Australian children, this study analysed trajectories of participation in team and individual sport between the ages of 8 and 15 using a group-based multiple trajectory modelling approach. A five-group solution was found to be the best fit to the data, identifying distinct patterns of sport participation over time. In comparison with non-autistic children, autistic children were more likely to belong to the ‘sport avoider’ group with low participation in both team and individual sport at all ages. Conversely, autistic children were less likely to be classified in the ‘team sportsperson’, ‘ex-team sportsperson’ or ‘mixed sportsperson’ groups. No difference in the likelihood of belonging to the ‘individual sportsperson’ group was found. Risk factors for trajectory group membership were similar for autistic and non-autistic children. Our findings indicate that autistic children are particularly likely to experience exclusion from team sport environments, and this exclusion persists over time. Similar rates of participation in individual sport for autistic and non-autistic children indicate that these environments may be more supportive for autistic children.
Lay abstract
Autistic children are less likely to participate in sport than non-autistic children, but we know little about how patterns of participation in team and individual sport change across childhood. Drawing on data for a group of Australian children whose families were reinterviewed between ages 8 and 15, the present study patterns of participation in team and individual sport over time. Findings from the analysis suggested that children could be grouped into five patterns of participation in team and individual sport between the ages of 8 and 15. In comparison with non-autistic children, autistic children were more likely to belong to the ‘sport avoider’ group with low participation in both team and individual sport at all ages. Conversely, autistic children were less likely to belong to the ‘team sportsperson’, ‘ex-team sportsperson’ or ‘mixed sportsperson’ groups. Similar numbers of autistic and non-autistic children belonged to the ‘individual sportsperson’ group. Factors linked to patterns of participation over time were similar for autistic and non-autistic children. Our findings indicate that autistic children are particularly likely to experience exclusion from team sport environments, and this exclusion persists over time. Similar rates of participation in individual sport for autistic and non-autistic children indicate that these environments may be more supportive for autistic children.
The prevalence of autism has increased significantly over the past 10 years. For example, in 2015 it was estimated that one in 150 Australians were autistic (Australian Institute of Health and Welfare, 2017). In 2024, estimates suggest that these numbers have risen to approximately one in 40 (Autism Spectrum Australia, 2024). Autism is characterised by differences in the way the individual communicates, engages socially and processes their sensory environment (Dallman et al., 2022). It is widely acknowledged that autistic individuals experience poorer physical and mental health outcomes compared with non-autistic people (Bauman, 2010; Bradley & Bolton, 2006; Croen et al., 2015; de Bruin et al., 2007; Ghaziuddin et al., 1998; Levy et al., 2010; Leyfer et al., 2006). It is likely that a large component of the gaps in health and well-being between autistic and non-autistic populations is preventable and attributable to health behaviours. To address the health disparities experienced by autistic people, it is, therefore, crucial to understand patterns and determinants of health behaviour and determinants in this population.
Physical activity (PA) has a multitude of physical and mental health benefits while a lack of PA has been identified as a significant risk factor for many chronic health conditions (Noetel et al., 2024). Autistic individuals participate in less PA than their non-autistic peers with rates of participation decreasing from childhood to adulthood (Buchanan et al., 2017; Edwards et al., 2024). Reduced levels of PA participation across the lifespan has the potential to negatively contribute to the increased rates of chronic health conditions experienced by autistic individuals (Bauman, 2010; Bradley & Bolton, 2006; Croen et al., 2015; de Bruin et al., 2007; Ghaziuddin et al., 1998; Levy et al., 2010; Leyfer et al., 2006). Further research is required to explore ways to enhance PA participation in autistic children and support them to remain on a trajectory to become physically active adults.
For children and youth, sport is a primary context for PA participation with 70% Australian children and youth participating in sport each year (Department of Health and Aged Care, 2025). For autistic youth, when successful, sport participation has been found to be supportive of their physical health, their social and emotional functioning, and overall quality of life (May et al., 2018; Pan et al., 2011; Zborowska, 2024). Furthermore, sport has been suggested to provide autistic youth with positive social opportunities, providing a sense of connectedness with their peers (Zborowska, 2024). While seeming positive, these benefits are not guaranteed, as autistic children have lower rates of sport participation when compared with non-autistic children and are often faced with many barriers to participation (May et al., 2018; Pan et al., 2011; Zborowska, 2024).
The social-ecological approach provides a well-established framework for understanding these barriers (e.g. Buchanan et al., 2017; Okkenhaug et al., 2024). Originally described by Bronfenbrenner (1979) and elucidated for PA specifically by Sallis et al. (2008), the social-ecological framework describes the dynamic interaction between the person and the environment over time. Based on this framework, barriers to, and facilitators of, PA participation for autistic people include intrapersonal (factors relating to the individual, for example, diagnosis, motivation, motor skills), interpersonal (factors relating to social relationships, for example, family, coaches and teammates), institutional (places with rules and regulations, for example, sporting clubs, physical education), community (the relationship between institutions, for example, the availability of inclusive programmes and accessible facilities), public policy (state and national laws, for example, national PA strategies), and physical environment (factors from the physical environment, for example, temperature, sensory properties) factors. These factors may represent either barriers or facilitators to PA participation for autistic people. For example, within their recent scoping review, Okkenhaug et al. (2024) identified intrapersonal barriers to PA participation for autistic children to include lack of motivation, difficulty with motor skills, sensory preferences and behaviours of concern. Interpersonal barriers included bullying, exclusion and lack of coach support. Institutional barriers related to how programmes were delivered, specifically with a lack of perceived structure and without clear explanation to the individual of why and how to participate. Similarly, within community factors authors identified the barriers presented by the competitive environments of many PA opportunities, as well as rigid expectations in relation to performance. While few studies were identified relating to public policy, authors noted that lack of funding and prioritisation of PA on a government level presented as a barrier for many. Finally, barriers relating to the physical environment included the weather, and the surrounding auditory environment, such as noises of crowds of people were also identified.
While research has highlighted the low sport participation rates of autistic children, as well as the specific barriers to engagement, previous research has not examined patterns of sport participation over time within this group. Similarly, we lack clear evidence on how autism is associated with team or individual sport participation. The distinction between team and individual sport is likely important for autistic youth due to the distinct social and sensory environments of team sport in comparison to individual sport (Hill et al., 2024; O’Flaherty et al., 2025). For instance, while evidence generally suggests stronger benefits of team sport than individual sport for mental health (Eime et al., 2013), a recent study found that autistic children gained no benefit from team sport participation and in fact experienced increased externalising behaviour (O’Flaherty et al., 2025). Individual sport participation was, conversely, found to have more benefit for physical health–related quality of life among autistic children than among non-autistic children (O’Flaherty et al., 2025). Insights gained from developing a deeper understanding into the trajectory of sport participation for autistic children may provide relevant health, fitness and education professionals guidance on how to address the barriers faced by many autistic young people. Furthermore, evidence generally indicates declining rates of sport participation and PA over childhood and adolescence on average (Corder et al., 2019; Dumith et al., 2011). However, studies also show that there exist diverse patterns of participation over time, with some groups maintaining consistent levels of participation and others decreasing or exhibiting continuing low participation (Howie et al., 2020; Lounassalo et al., 2019; Pate et al., 2019). Understanding factors associated with trajectories of either sustained sport participation or desistance from participation has important implications for efforts to prevent formation of sedentary behaviour patterns.
Therefore, this study adopted a group-based trajectory modelling approach to answer the following research questions:
What is the association between autism and trajectories of youth participation in team and individual sport?
What intrapersonal, interpersonal (family) and community factors predict trajectories of team and individual sport participation, and does the association between these factors and participation differ for autistic and non-autistic youth?
Methods
The data for this analysis were sourced from the Longitudinal Study of Australian Children (LSAC) (Soloff et al., 2005). LSAC includes two groups of children: those born between March 2003 and February 2004 (‘B’ cohort) and those born between March 1999 and February 2000 (‘K’ cohort). Initial data collection occurred from March to November 2004 when the children in ‘B’ cohort were 0 to 1 years old and children in K cohort were 4 to 5 years old. The sampling method used a two-stage cluster design, starting with a stratified sample of 311 postcodes, followed by random selection of children from Medicare records within those postcodes. A total of 18,800 children were invited, with baseline data collected from 10,090 children (54% response rate). Data collection has continued every 2 years, with the most recent data available from 2020. For this article, data up to ages 14 to 15 are used: wave 8 (2018) for the ‘B’ cohort and wave 6 (2014) for the ‘K’ cohort. We exclude a total of 1405 (14%) children who dropped out prior to wave 4 when autism was first ascertained. Cases with less than two non-missing observations for both team and individual sport participation (630 children) or missing data on covariates (815 children) were also excluded from analysis. The final analytic sample comprises 7240 children (72% of baseline sample), including 316 autistic children and 6924 non-autistic children. A total of 5611 children contributed four waves of data, 998 contributed three waves, and 631 contributed two waves.
The LSAC study received ethics approval from the Australian Institute of Family Studies Human Ethics Review Board. Parents or guardians provided informed consent for themselves and their child. The current study was deemed exempt from ethics review by The University of Queensland Human Research Ethics Committee. Although autistic community members were not involved in designing or conducting the research, several authors are family members of autistic individuals.
Measures
Sport participation
Sport participation was reported by the child’s primary carer from ages 8–9 to 14–15 years. For ages 8–9 and 10–11 years, parents were asked, ‘In the last 12 months, has the child regularly participated in any of the following activities (outside school hours even if organised by the school)?’ This question was revised for ages 12–13 and 14–15 years to ‘Considering any out-of-school activities the child regularly engages in, has the child participated in any of the following activities in the past week?’ Participation in ‘team sport’ and ‘individual sport’ was recorded separately (yes/no) at each time point.
Autism
Starting from wave 4, parents were asked, ‘Does the child have any of these ongoing conditions?’ which included ‘Autism, Aspergers, or other autism spectrum disorders’. Given that autism is a long-lasting condition that may not be identified right away, we classified children who were ever reported to have autism as ‘autistic’, while those who were never reported to have autism were categorised as ‘non-autistic’.
Covariates
We included a range of intrapersonal-, interpersonal- and community-level covariates in analysis that may predict sport participation trajectories. Intrapersonal-level covariates included child sex in addition to summary indices of physical development, socio-emotional development, and learning outcomes at age 4 to 5 years (Sanson, Hawkins, et al., 2010; Sanson, Misson, et al., 2010). Interpersonal-level covariates included a summary measure of family socioeconomic position constructed from parental income, education, and occupation data (Baker et al., 2017), cultural background (whether the child speaks a language other than English at home), maternal age at the child’s birth, number of siblings, family structure (both biological parents present vs other family structures) and whether the child was taken by family to parks/pools in the past week. A summary measure of area advantage (Socioeconomic Indexes for Areas [SEIFA]) was included to capture contextual factors affecting sport participation. Continuous covariates with no natural metric (socio-economic position, SEIFA, indices of physical development, socio-emotional development, and learning outcomes) are standardised to mean zero and standard deviation one.
Analysis
Group based multi-trajectory modelling (GBMTM) (Nagin et al., 2018) using the traj Stata plugin was used to analyse trajectories of participation in team and individual sport. GBMTM is a finite mixture modelling technique and represents an extension of group-based trajectory models (GBTM) (Nagin, 2009) to allow for multiple parallel trajectories. The GBMTM approach divides the analytic sample into a number of latent subgroups which follow similar patterns of team and individual sport participation between ages 8 and 9 years and 14 and 15 years. The resulting groups are not thought to represent literally distinct subpopulations (at least in the current application), but nonetheless may offer a useful approximation of a complex joint distribution of sport participation over time (Nagin, 2009). Maximum likelihood estimation is employed (Jones & Nagin, 2013), meaning that model parameters are unbiased under the assumption of missing at random (MAR) (Nagin & Odgers, 2010).
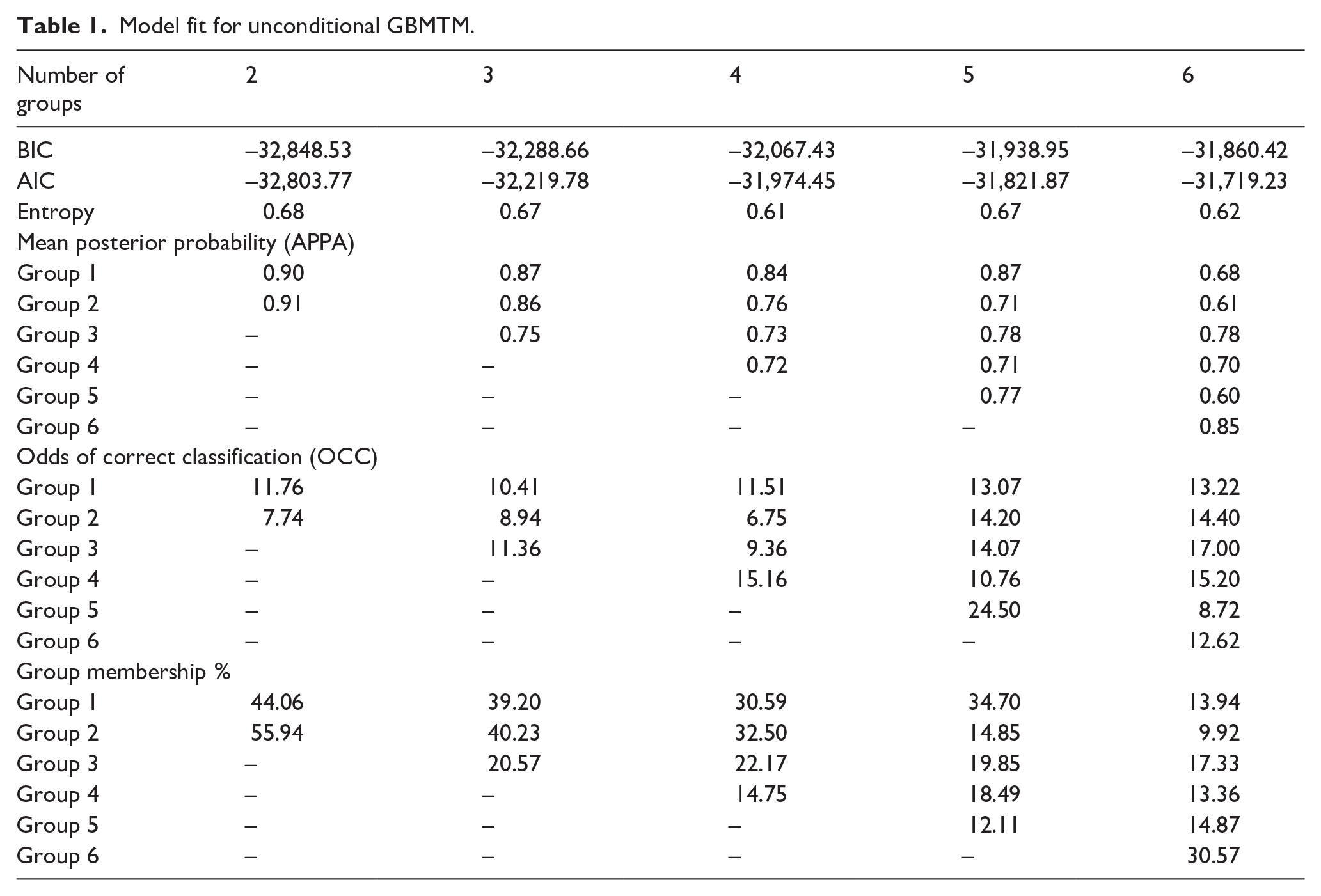
To examine trajectories of sport participation between ages 8 and 15, we first fit a series of unconditional GBMTM from two to six groups, allowing quadratic trajectories in all groups. Fit statistics, including the Bayesian information criterion (BIC), Akaike information criterion (AIC), entropy, the average posterior probability of assignment (APPA) (Nagin, 2009), and the odds of correct classification (OCC; Nagin, 2009), were compared to determine an optimal number of groups for further analysis. Substantive relevance of the groups to the research questions was also considered. Noting that ‘traj’ reports an alternative formulation of AIC and BIC such that higher (closer to zero) values are preferable (Nagin, 2009), fit statistics shown in Table 1 indicated support for either a five- or six-group model. Both BIC and AIC indicated the six-group model, but APPA for the six-group model fell below the recommended lower bound of 0.7 (Nagin, 2009), indicating that some groups may not be clearly distinguished from other groups when more than five groups were estimated. Entropy similarly indicated that the five-group model (0.67) provided better classification than either the four (0.61) or six (0.62) group models, although all models exhibit only moderate classification quality. Nagin (2009) recommends minimum OCC values of 5 for all groups, with higher values representing better classification accuracy. All solutions exceed the recommended minimum value for all groups; however, the five-group solution appears to exhibit slightly higher OCC values. Substantively, the six-group solution identified a pattern of exiting individual sport (while continuing to play team sport) which was not apparent in the five-group solution. For our analysis, we focussed on the five-group solution because the additional complexity of the six-group solution, while improving BIC/AIC and conveying substantively relevant additional information, may not result in clear distinctions between children.
Model fit for unconditional GBMTM.
Results
Table 2 presents summary statistics for the analytic sample, separately for non-autistic and autistic and the total sample. The sample included 7240 youth (6924 non-autistic and 316 autistic). Autistic children were much less likely to participate in team sport at all ages, with bivariate differences of 17 to 23 percentage points. Differences in individual sport participation were less marked (2–6 percentage points) but slightly lower among autistic children. Bivariate tests (available on request) show that these differences are uniformly statistically significant for team sport and not statistically significant for individual sport. About three-quarters of the autistic sample were male. At age 4 to 5, autistic children scored lower on the physical development, socio-emotional development and learning outcomes. Otherwise, there were minor demographic differences between autistic and non-autistic children (autistic children less likely to reside with both biological parents or to speak a language other than English). There were no apparent differences in rates of attendance at parks/pools or the frequency of outdoor play.
Sample summary statistics.
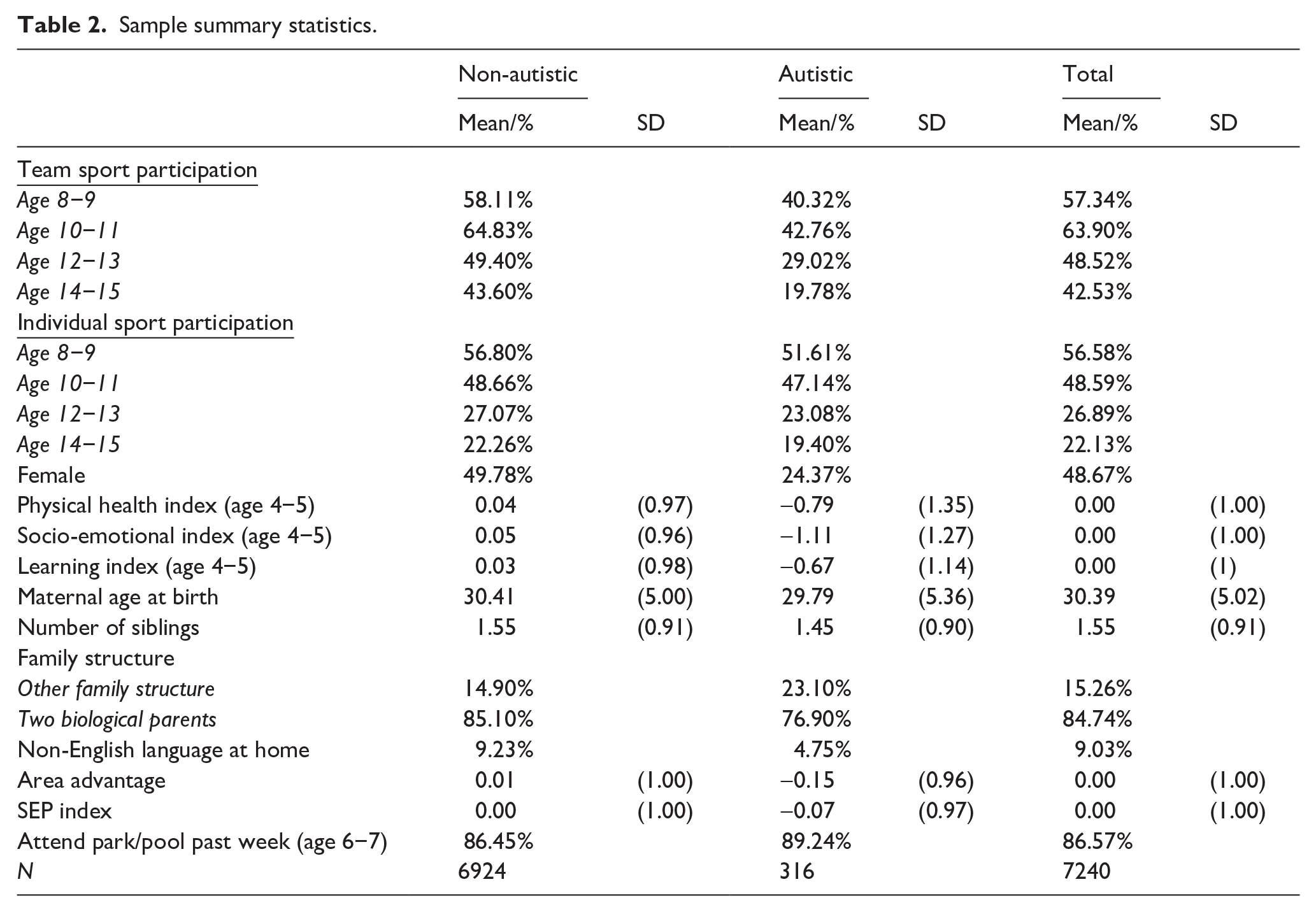
Figure 1 presents the predicted trajectories of individual sport (top panel) and team sport (bottom panel) for the selected unconditional five-group solution. Each subplot shows the probability of team and individual sport participation over time within trajectory groups. Approximately one-third of children (34.7%) were classified as sport avoiders. These children had low and declining rates of participation in both team and individual sport. The second group (14.8%) was classified as team sportspeople. Among children in this group, rates of individual sport participation were similar to the sport avoiders group, but participation in team sport was much higher at between 80% and 100%. The third group (19.8%) can be described as ex team sportspeople – this group, while exhibiting consistently low rates of individual sport participation, played team sport at very high rates at ages 8 to 9 and 10 to 11 before decreasing sharply at older ages. A fourth group of children (18.5%) are characterised by mixed sportspeople. This group was likely to play team sport at all ages, similar to the team sportspeople group. However, they were also very likely to also play individual sport at younger ages, before declining participation at older ages. Finally, the fifth group (12.1%) represents individual sportspeople. Children in this group were likely to play individual sport (albeit at declining rates) but were unlikely to be involved in team sport at all ages.
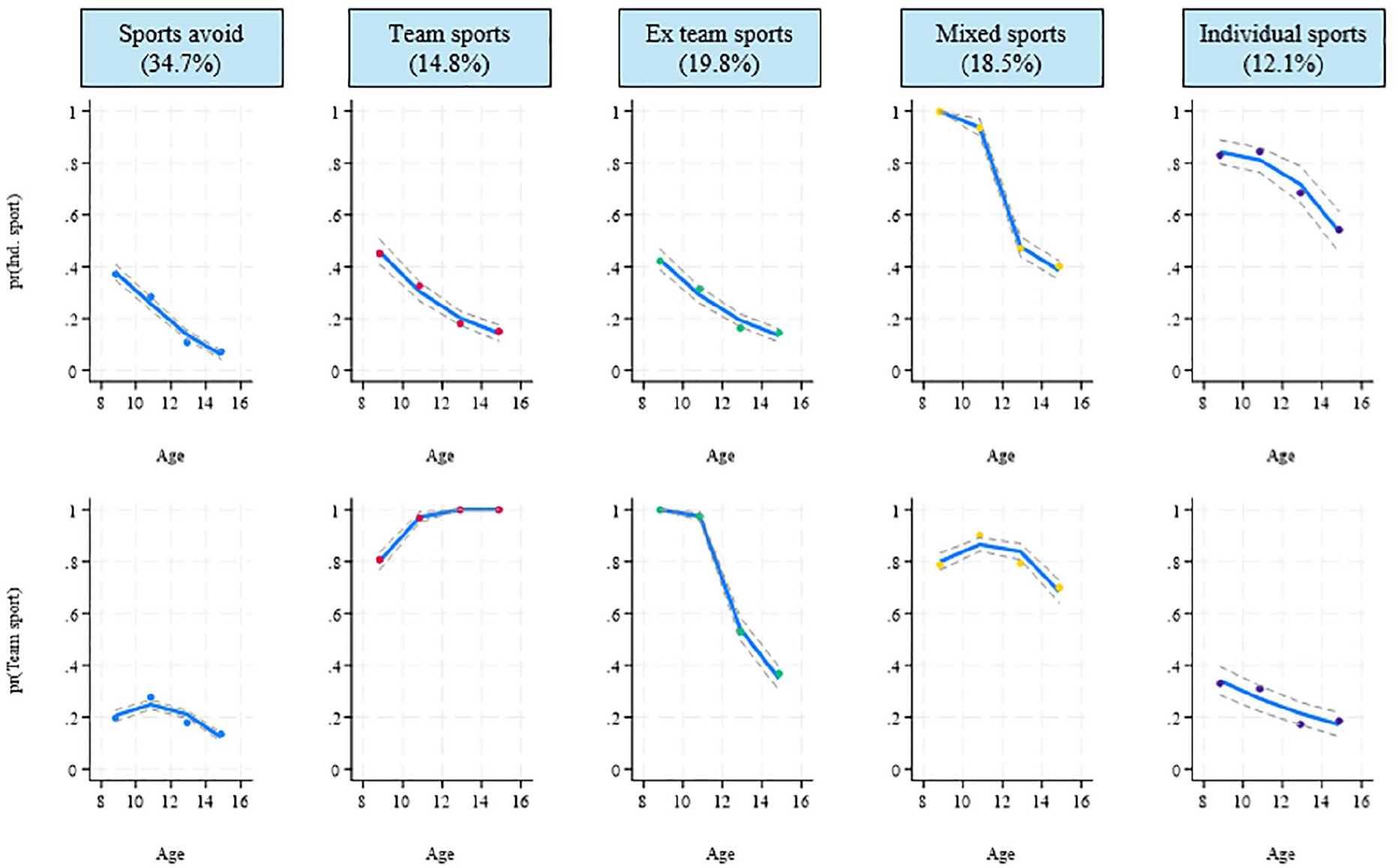
Five-group GBMTM solution. Probability of individual sport (top)/team sport (bottom) participation, age in years (approximately 8–14).
Appendix Table 4 shows the proportions of children classified into each group by child autism. To assess the relationship between autism and trajectories of sport participation, participants were classified into groups using the maximum probability assignment rule and multinomial logistic regression was used to investigate associations. Table 3 presents adjusted relative risk ratios (RRRs) derived from this analysis. The RRR for each group is compared with the largest (sport avoiders) group and analyses are adjusted for child, family and contextual characteristics. Autism was associated with substantially lower likelihood of being a team sportsperson (RRR = 0.29, p < 0.001), an ex team sportsperson (RRR = 0.47, p < 0.001) or mixed sportsperson (RRR = 0.39, p < 0.001), but was not significantly associated with the likelihood of being an individual sportsperson (RRR = 0.84, ns). To ease interpretation, adjusted marginal effects of autism (on the probability scale) are presented in Figure 2. Autistic children were approximately 17 percentage points more likely than non-autistic children to be sport avoiders. Correspondingly, autistic children were eight percentage points less likely to be team sportspeople, four percentage points less likely to be ex team sportspeople, and eight percentage points less likely to be mixed sportspeople. Autistic children were slightly more likely (three percentage points) than non-autistic children to be an individual sportsperson, although this difference was not statistically significant.
Predictors of trajectory group membership.
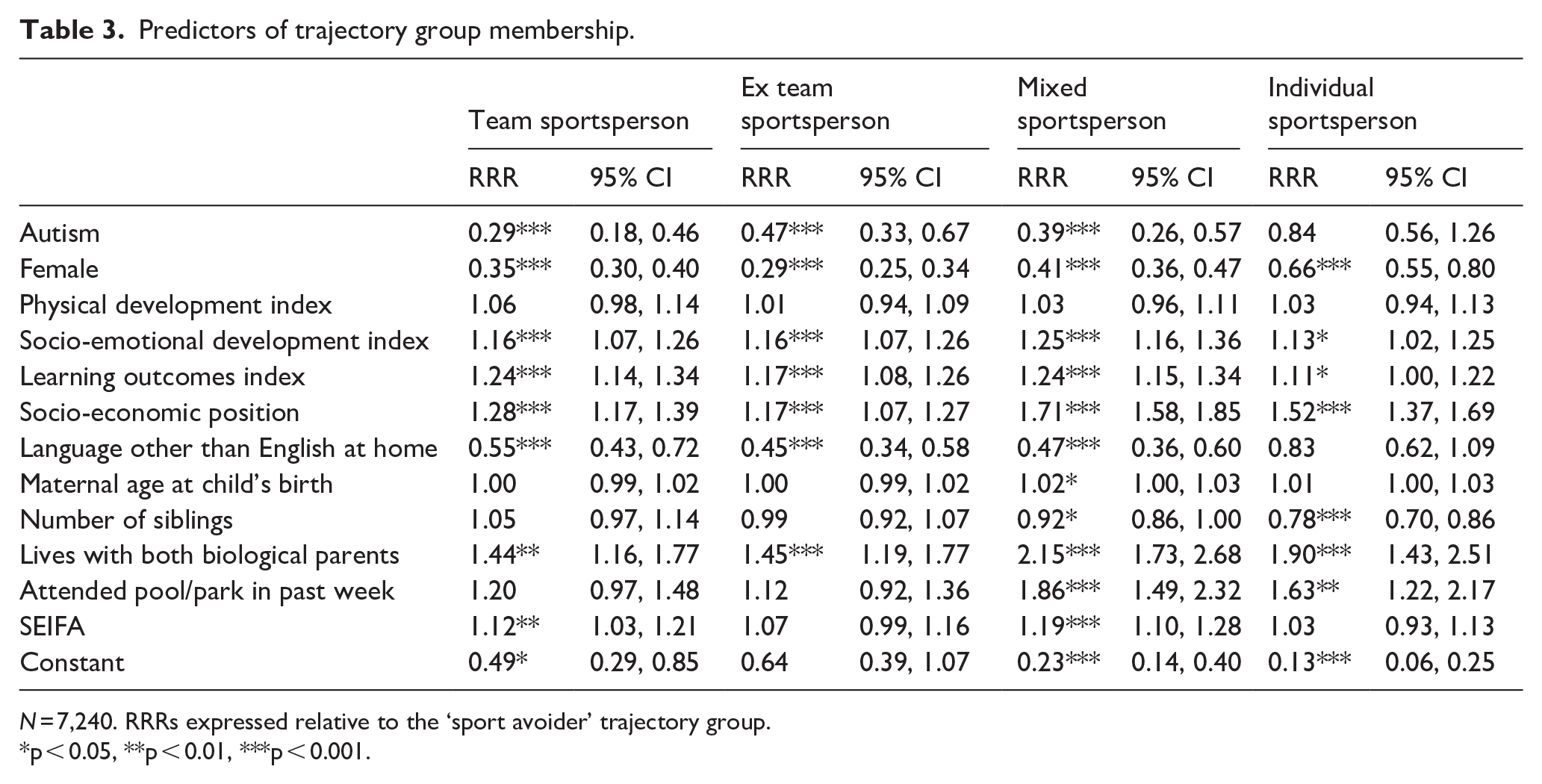
N = 7,240. RRRs expressed relative to the ‘sport avoider’ trajectory group.
p < 0.05, **p < 0.01, ***p < 0.001.
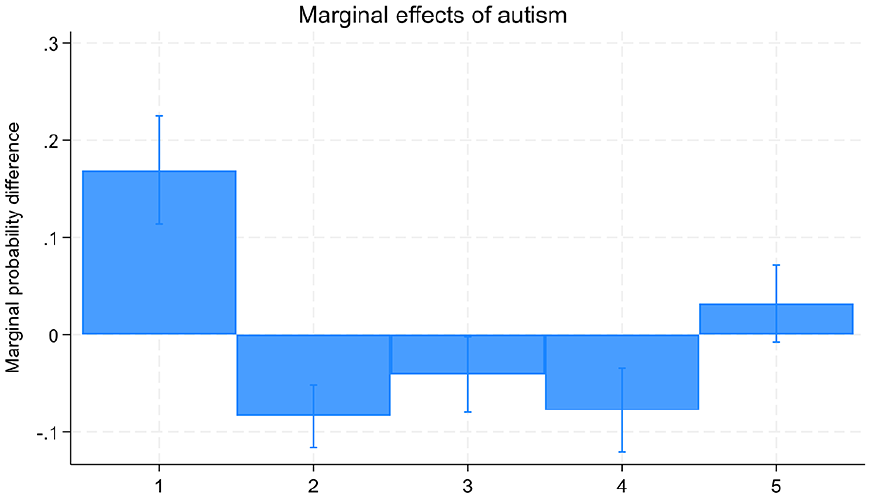
Marginal effects of autism. 1 ‘sport avoider’, 2 ‘team sportsperson’, 3 ‘ex team sportsperson’, 4 ‘mixed sportsperson’, 5 ‘individual sportsperson’.
For covariates, female children were much more likely to be sport avoiders relative to any other group compared to boys. Children’s physical development (at age 4–5 years) was, perhaps surprisingly, not associated with patterns of subsequent sport participation. Better socio-emotional development and learning outcomes at age 4 to 5 years were, however, positively associated with all trajectories of sport participation relative to being a sport avoider. Socio-economic position and living with both biological parents were strongly associated with higher participation in all sporting trajectories, whereas speaking a language other than English at home was linked to lower participation in team or mixed-sport trajectories (but not individual sport). Neighbourhood advantage was associated with higher likelihood of being a team sportsperson or mixed sportsperson. Attendance at parks/pools (at age 6–7 years) was associated with increased likelihood of being a mixed sportsperson and individual sportsperson, but not a team sportsperson.
Additional exploratory analyses were conducted to investigate potential moderation of the effect of autism by covariates. Specifically, we tested a series of models with two-way interactions of autism and each covariate and compared each model to the model presented in Table 3 using likelihood ratio tests. This analysis (Appendix Table 5) found no support for moderation by any covariate, suggesting that risk factors for sport participation trajectories are largely similar among autistic and non-autistic children.
Discussion
Supporting sport participation in autistic children has the potential to enhance sustained PA participation into adulthood, thus resulting in positive health and wellbeing outcomes. As such, in line with the socio-ecological model this study aimed to explore the trajectory of sport participation of autistic children, as well as the potential impact of intrapersonal, interpersonal (family) and community factors on patterns of sport participation over time. Our findings show that there exist distinct patterns of consistent non-participation, sustained participation (particularly in team sports) or declining participation in team or individual sports. When addressing Research Question 1, for both individual and team sports autistic children showed declining likelihood of participation on average as they aged. For the trajectory groups specifically, autistic children were substantially more likely to belong to the ‘sport avoider’ group – with consistently low participation in both team and individual sport – and correspondingly less likely to exhibit patterns of either continued participation in (team) sport or desistance from participation. This indicates that autistic children’s sport participation is already low at an age when non-autistic children are still participating in sport at much higher rates, suggesting that intervention earlier in childhood is important to reduce gaps in participation between autistic and non-autistic children. Notably, there was no difference between autistic and non-autistic children in the likelihood of belonging to the ‘individual sportsperson’ group, which may indicate that there are opportunities for individual sport to provide an alternate route for autistic children’s participation. Interestingly, while no previous literature existed specific to sport participation for autistic children, several studies have demonstrated declining rates of PA participation from childhood to adulthood for the general population (Corder et al., 2019; Dumith et al., 2011). These findings highlight the importance of research continuing to focus on improving the sustained sport participation of children and youth, more broadly, while acknowledging that autistic children may require different supports to do so.
When addressing the second research question exploring potential intrapersonal, interpersonal, and community factors that may predict trajectories of sport participation for autistic children, several factors were identified. In relation to intrapersonal factors, autism was associated with reduced sport participation. This was particularly so for team sports with autistic children participating in significantly less team sports when compared with their non-autistic peers. Autism is characterised by several core characteristics including differences in social communication, sensory processing and sensory-motor behaviours (American Psychological Association, 2022), all of which can be significantly impacted by typical sporting environments (specifically team sport environments). For example, a mismatch in social communication preferences between autistic children and their teammates and coaches has been identified as a major barrier to sport participation for many autistic children (Blagrave & Colombo-Dougovito, 2019; Lamb et al., 2016; Ryan et al., 2018; Salters et al., 2022). Many autistic people, for example, do not recognise social hierarchies or methods of communication such as the use of gesture, eye-contact and eye-gaze, abstract language and use of vocal tone to express meaning (Dunn et al., 2023). Furthermore, autistic individuals process auditory information differently to non-autistic people and as such require additional time to process verbal instructions (Dunn et al., 2023). This can result in many autistic people appearing to not be interested in others and not follow rules, instructions or routines. For autistic children with sensory processing differences, sport often occurs in overstimulating environments such as stadiums, gyms and arenas. With many autistic children experiencing hypersensitivity to noise (e.g. sounds of crowds, cheering, sirens), touch (other players, sweat, dirt) and visual stimulation (e.g. lights), as well as difficulties regulating temperature the unpredictable sensory environment of sporting activities can often present a barrier to participation (Blagrave, 2017; Healy et al., 2013; Lamb et al., 2016; May et al., 2018).
Many autistic individuals also have differences in motor skill development which has been found to negatively influence their sport participation (Rios & Benson, 2020). Interestingly, the highest participation within team sports appeared to occur between the ages of 8 and 11 years before rapidly declining. While self-awareness, self-evaluation and self-efficacy start to develop in early childhood, children between the ages of 6 and 12 begin to have greater contact with society, and as such begin to compare their own efforts and skills to others. Lack of self-efficacy and feelings of incompetence and not belonging have been identified as a barrier to sport participation for many autistic children and youth (Okkenhaug et al., 2024). Due to the difficulties autistic children can experience with motor skills, coupled with their increasing level of self-awareness, this may contribute to the reduced team sport participation rates for autistic children after the age of 11. To confirm this hypothesis, further research is required to explore reasons why children choose to withdraw from team sports.
When looking at intrapersonal factors that potentially supported sustained sport participation, socio-emotional and learning development were associated with higher likelihood of belonging to trajectory groups characterised by sustained participation in sport (particularly the ‘team sportsperson’ and ‘mixed sportsperson’ groups). While limited research is available evaluating the impact of these two factors specifically on sport participation for autistic children, social understanding, self-regulation, problem-solving skills and ability to understand and follow rules and routines have been identified as both barriers and facilitators to sport participation for autistic children (Okkenhaug et al., 2024). However, due to the social and cognitive benefits that can be achieved through sport participation, further research is required to determine whether these results were due to these participants having higher levels of social-emotional and cognitive functioning to begin with, or whether this level of functioning had been achieved due to their sustained sport participation. Overall, our results suggest that the impacts of socio-emotional and learning on sport participation may be similar for autistic and non-autistic children, suggesting that these factors are important considerations for efforts to increase sport participation generally as well as programmes specific to autistic children.
In relation to interpersonal factors, children were more likely to belong to trajectories of sustained sport participation if they resided with both biological parents. Although this specific finding is novel to this study, past literature has highlighted the importance of parent support to sustained sport participation for autistic children (Okkenhaug et al., 2024). As being raised within a single-parent household can impact time and financial resources (Bahri et al., 2023), this could result in a reduction in the parent’s capacity to provide the support necessary for successful, long-term sport participation. Considering that autistic children are at greater risk of experiencing parental separation (Bahri et al., 2023), further exploration into this finding is crucial to ensure that sport and PA opportunities are not only inclusive and accessible to the autistic child, but also to their families. Interestingly, children were also more likely to have sustained sport participation if English was their first language. This finding is unique to this study, and therefore further research is required to explore why this might be the case. While overall associations of language with sport participation did not differ between autistic and non-autistic children, programmes supporting autistic children should nonetheless consider what potential language barriers might impact families of autistic children and ensure that supports are appropriately tailored. Gender also appeared to influence sport participation as females were less likely to participate in trajectories including sport participation than males, indicating that girls are much more likely to belong to the ‘sport avoider’ trajectory characterised by consistent non-participation. This is consistent with the general population as males have been found to have increased levels of sport and PA participation (Australian Bureau of Statistics, 2015).
In relation to community factors, living in higher socio-economic locations appeared supportive of children sustaining participation in sport over time, with particularly strong positive associations with membership in the ‘team sportsperson’, ‘mixed sportsperson’ and ‘individual sportsperson’ groups relative to the ‘sports avoider’ group. Furthermore, for children aged 6 to 7 years, having access to active environments such as parks and pools was found to be associated with sustained individual sport participation. For autistic children, an additional challenge to sport participation recognised within the literature (Okkenhaug et al., 2024) has been a lack of inclusive environments and opportunities, with many autistic children only having access to expensive programmes, with long waitlists. As such, future research should explore ways in which autistic children can be better supported to participate in sport and PA within their own communities, rather than needing to rely on autism-specific programmes.
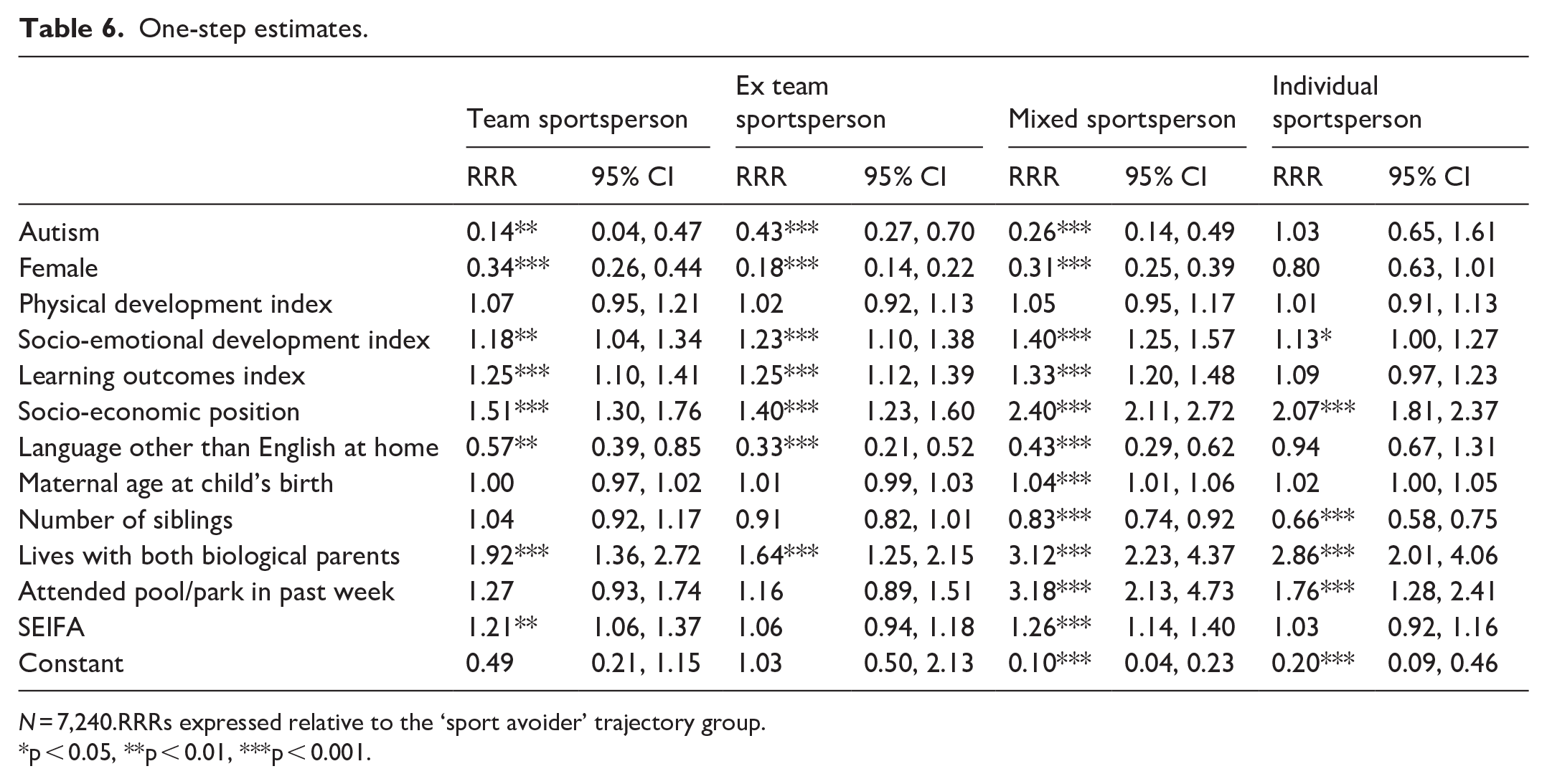
The study had important strengths, including notably the use of a representative cohort of children and the use of a sophisticated longitudinal approach to identify patterns of change and stability in sport participation over time. The analysis also illustrates the importance of distinguishing between team and individual sport for autistic children given the distinct barriers that are likely to be present in team sport environments. There are also important limitations which may be addressed in future research. First, although the sample prevalence of autism is broadly similar to recent population estimates for children of similar age, autism is parent reported, and the sample characteristics may, therefore, differ from studies with clinically confirmed diagnosis. Second, the LSAC data do not permit detailed analysis of the intensity of sport participation or the experiences of autistic children within sport. More detailed evidence on these issues is likely to be crucial to understanding the impacts of sport on health and social relationships for autistic children and overcoming barriers to participation. Third, inconsistencies in the measurement of sport participation over time, while not under our control, may have affected our results. Fourth, misclassification of children to trajectory groups may bias associations between covariates and group membership. To address this issue, we refit our model using an alternative ‘one-step’ approach where covariate effects are estimated simultaneously with group membership. This analysis (Appendix 1, Figure 3 and Table 6) results in a highly similar set of trajectory groups. Estimated associations of group membership with autism and other covariates are generally slightly stronger than reported in the main analysis but lead to identical substantive conclusions.
This study resulted in key findings which will assist to guide future research. First, it was found that autistic children have a consistently low rate of sport participation when compared with their non-autistic peers, with numbers continuing to decrease as they age. Due to the research showing the association between individuals who successfully participated in sport as children becoming physically active adults (Telama et al., 2014), further research is required to explore methods to support the sustained sport participation for autistic children and youth. Second, participation rates were particularly low for autistic children engaging in team sports. Among the general population, while both individual and team sports have been found to have benefits for health and wellbeing, team sports have been shown to have a particularly positive influence on mental health outcomes including creating a sense of belonging, increasing self-esteem and improving social interactions (Andersen et al., 2019; Eime et al., 2013). For autistic children, however, recent evidence suggests that team sport may not have the same benefits, and may in fact contribute to poorer mental health in some instances (O’Flaherty et al., 2025). Due to the complexity of many team sport environments in relation to the social, sensory and physical demands, further research should be conducted to explore ways in which these activities might be adapted to be more inclusive of autistic children (Hill et al., 2024). Examples of such strategies might include environmental modification or coach training allowing them to better understand and respond to the needs of their autistic athletes. Individual sport may offer a more welcoming environment for autistic children due to reduced social or sensory barriers and greater potential scope for coaches to tailor activities to the needs of a specific child (Hill et al., 2024; O’Flaherty et al., 2025). Individual sport may, therefore, offer an important alternative context for promoting participation for autistic children, although we stress that this should not be understood as a rationale to avoid working to make team sport environments more inclusive. Finally, children showed greater sustained sport participation if they lived in a two-parent household and had easy access to community activities. As such, supports and strategies developed to enhance the sport participation of autistic children should also ensure that they are considerate of their whole family and can be implemented at a low cost, within their own community.
Remaining physically active across one’s life has many health and wellbeing benefits. This study found that autistic children have low rates of sport participation which continue to decrease as they age. To better support autistic children to become more physically active adults, further research is required to implement supports and strategies to ensure that autistic children and their families have access to inclusive sporting opportunities within their own communities.
Footnotes
Appendix 1
One-step estimates.
| Team sportsperson | Ex team sportsperson | Mixed sportsperson | Individual sportsperson | |||||
|---|---|---|---|---|---|---|---|---|
| RRR | 95% CI | RRR | 95% CI | RRR | 95% CI | RRR | 95% CI | |
| Autism | 0.14** | 0.04, 0.47 | 0.43*** | 0.27, 0.70 | 0.26*** | 0.14, 0.49 | 1.03 | 0.65, 1.61 |
| Female | 0.34*** | 0.26, 0.44 | 0.18*** | 0.14, 0.22 | 0.31*** | 0.25, 0.39 | 0.80 | 0.63, 1.01 |
| Physical development index | 1.07 | 0.95, 1.21 | 1.02 | 0.92, 1.13 | 1.05 | 0.95, 1.17 | 1.01 | 0.91, 1.13 |
| Socio-emotional development index | 1.18** | 1.04, 1.34 | 1.23*** | 1.10, 1.38 | 1.40*** | 1.25, 1.57 | 1.13* | 1.00, 1.27 |
| Learning outcomes index | 1.25*** | 1.10, 1.41 | 1.25*** | 1.12, 1.39 | 1.33*** | 1.20, 1.48 | 1.09 | 0.97, 1.23 |
| Socio-economic position | 1.51*** | 1.30, 1.76 | 1.40*** | 1.23, 1.60 | 2.40*** | 2.11, 2.72 | 2.07*** | 1.81, 2.37 |
| Language other than English at home | 0.57** | 0.39, 0.85 | 0.33*** | 0.21, 0.52 | 0.43*** | 0.29, 0.62 | 0.94 | 0.67, 1.31 |
| Maternal age at child’s birth | 1.00 | 0.97, 1.02 | 1.01 | 0.99, 1.03 | 1.04*** | 1.01, 1.06 | 1.02 | 1.00, 1.05 |
| Number of siblings | 1.04 | 0.92, 1.17 | 0.91 | 0.82, 1.01 | 0.83*** | 0.74, 0.92 | 0.66*** | 0.58, 0.75 |
| Lives with both biological parents | 1.92*** | 1.36, 2.72 | 1.64*** | 1.25, 2.15 | 3.12*** | 2.23, 4.37 | 2.86*** | 2.01, 4.06 |
| Attended pool/park in past week | 1.27 | 0.93, 1.74 | 1.16 | 0.89, 1.51 | 3.18*** | 2.13, 4.73 | 1.76*** | 1.28, 2.41 |
| SEIFA | 1.21** | 1.06, 1.37 | 1.06 | 0.94, 1.18 | 1.26*** | 1.14, 1.40 | 1.03 | 0.92, 1.16 |
| Constant | 0.49 | 0.21, 1.15 | 1.03 | 0.50, 2.13 | 0.10*** | 0.04, 0.23 | 0.20*** | 0.09, 0.46 |
N = 7,240.RRRs expressed relative to the ‘sport avoider’ trajectory group.
p < 0.05, **p < 0.01, ***p < 0.001.
Acknowledgements
MO and MB are supported by The University of Queensland Strategic Funding for the 360-Kids Community Network Health Research Accelerator (HERA) programme. SRG is partly funded by the Health and Wellbeing Centre for Research Innovation, a jointly funded research centre by The University of Queensland and Health and Wellbeing Queensland.
Author Contributions
Data availability
Researchers may apply for access to the LSAC data through the Australian Data Archive.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The LSAC study received ethics approval from the Australian Institute of Family Studies Human Ethics Review Board. Parents or guardians provided informed consent for themselves and their child. The current study was deemed exempt from ethics review by The University of Queensland Human Research Ethics Committee.