
Abstract
Research has found that autistic women experience elevated rates of sexual and domestic violence and may benefit from accessing support to recover. This study aimed to explore the experiences of Australian practitioners and the approaches they use to support the recovery needs of autistic women who are survivors of sexual and domestic violence. Semi-structured interviews were conducted with 14 Australian practitioners to capture their experiences of supporting autistic women who are survivors of sexual and domestic violence. Data from these interviews were analysed using a reflexive thematic analysis, which generated four themes about participants’ experiences in supporting autistic survivors: (1) unburdening the processing load of understanding violence and trauma, (2) understanding support and recovery needs as interconnected, (3) lived experience as a therapeutic tool, and (4) the challenges of practicing within unaffirming and invalidating systems. The findings illustrate how Australian practitioners help autistic survivors by accommodating their recovery support needs, and the systematic and structural issues that create barriers to recovery for autistic survivors while putting additional strain on the practitioners who support them. The findings also highlight practice implications around how supporting autistic survivors with interoceptive awareness and understanding their needs within relationships is beneficial to their recovery.
Lay Abstract
Research has commonly found that autistic women are more likely than autistic men and non-autistic women to be harmed in their sexual and romantic relationships and may need support in healing from the impacts of these experiences. In this study, we wanted to find out more from the people who provide this support to autistic women. We asked 14 Australian practitioners about what they do to support autistic women who have experienced these types of harm in their relationships, and what makes this harder or easier for them to do. We then analysed the common patterns (themes) in what these practitioners said. From this we found that Australian practitioners often help autistic women to heal by providing a safe and supportive space to process their experiences and recover from what has happened to them. We also found that an important part of the support that practitioners provide autistic survivors is helping them to understand their experiences of violence and build awareness of feelings in their body (interoception). The practitioners in this study also talked about how the autistic women that they support often have bad experiences when getting help from support services and systems that commonly do not meet their needs. This often makes it harder for practitioners to help autistic women heal and a lot of them suggested that services could be made better by learning more about autistic people’s different support needs and how to accommodate these.
Autistic adults experience heightened levels of interpersonal violence and trauma, often marked by patterns of polyvictimisation (Gibbs et al., 2023, 2024; Pearson, Rees, & Forster, 2022; Trundle et al., 2023). These experiences of interpersonal violence and trauma commonly differ along gender-based lines as research has consistently found that autistic women experience elevated rates of sexual and domestic violence (SDV) compared to autistic men and non-autistic women (Cazalis et al., 2022; Cooke et al., 2024; Gibbs et al., 2022). Domestic violence (also known as intimate partner violence) includes acts of physical, sexual, financial, and/or emotional abuse occurring in intimate partner relationships, typically falling within a pattern of coercion and control by one partner over another (Shorey et al., 2023). SDV often occurs in unison and is underpinned by gender inequality, therefore falling under the umbrella of gendered violence (Sensenig, 2024).
A neurodiversity-informed approach involves examining the context of support around autistic/neurodivergent people, including the socio-cultural and structural factors that impact their rights and well-being, rather than focusing on impairment as the sole cause of the difficulties that they experience (Chapman, 2021; Rosqvist et al., 2022; Stenning & Rosqvist, 2021). The impacts of interpersonal trauma and post-traumatic stress across all populations commonly include a range of difficulties with interpersonal processes, emotional regulation, and increased occurrence of physical and mental health challenges (López-Martínez et al., 2018). Recovering from SDV and the impacts of interpersonal trauma is often a long and non-linear process for survivors (Carman & Kay-Lambkin, 2022); however, research suggests that access to both formal and informal supports can be highly beneficial (Melgar Alcantud et al., 2021). Autistic survivors commonly experience barriers in their recovery process due to support systems having a limited, and often deficit-based, understanding of their support needs (Ridout, 2022). In this study we employed a neurodiversity-informed approach to explore the systemic barriers that impact recovery for autistic survivors and how support practitioners navigate them (Chapman & Botha, 2022).
The impacts of SDV and interpersonal trauma are heightened for marginalised populations who are more likely to experience polyvictimisation, intersectional barriers to support, and have fewer resources to draw on in their recovery (Kulkarni, 2019). Intersectional feminist theory provides an analytical framework for understanding why women with overlapping marginalised identities experience multiplicative forms of inequality and oppression (Warrier, 2022). Autistic women are one such population as they experience high rates of interpersonal trauma and post-traumatic stress in relation to their experiences of SDV (Reuben et al., 2021; Schnabel & Bastow, 2023), while also encountering greater barriers to support services (Dubreucq & Dubreucq, 2021; Koffer-Miller et al., 2022; Seers & Hogg, 2022). We used an intersectional feminist approach throughout this study to examine the interpersonal violence that autistic women experience as a gendered and structural issue underpinned by intersectional disadvantage and marginalisation (Fox, 2025).
The access barriers to support that autistic populations experience include inflexibility and a lack of universal design with services (O’Connor et al., 2023), un-accommodating service delivery environments and communication practices (Doherty et al., 2022), and providers having a limited knowledge around working with autistic adults (Maddox et al., 2020). These access barriers are compounded for autistic women who face intersectional disadvantage in relation to gender inequality (Fox, 2024) and the under-recognition of autism in women and girls (McCrossin, 2022). In addition, autistic women report adversity in engaging with support services due to practitioners having a limited understanding of the gender-based issues that they experience (Murphy et al., 2022), often underpinned by a gender bias in how they respond to autistic women (Tint et al., 2017; Tint & Weiss, 2018).
When considering the high rates of interpersonal violence that they experience, preliminary studies have highlighted the importance of understanding trauma recovery needs as a factor in how practitioners support autistic people (Pearson, Rose, & Rees, 2022). Previous research has provided insights into autistic survivors’ experiences of SDV (Douglas & Sedgewick, 2024; Ridout, 2020) and their recovery needs in relation to this (Pearson et al., 2024). However, there is limited research on practitioners’ perspectives and how they can better support autistic survivors’ recovery. This study aimed to address this knowledge gap by capturing practitioner’s experiences and insights around supporting autistic survivors. In this study we investigated the experiences of Australian practitioners in supporting autistic survivors using the following research questions: (1) What approaches do Australian practitioners use to support autistic survivors of SDV? (2) What challenges do they face in providing this support?
Methods
Participants and procedure
We obtained ethical approval for this study from the Queensland University of Technology’s Human Research Ethics Committee (UHREC). The inclusion criteria for this study were practitioners located in Australia who have experience working with autistic women who are survivors of SDV. We compiled an email list of potential participants using an Internet search (with Australia as the geolocation) of key words based on these inclusion criteria (e.g. ‘therapy’, ‘autistic’, ‘women’ and ‘trauma’). We added practitioners with a range of professional backgrounds, skills and approaches to this list as recruitment focused on inviting all potential participants with experience in supporting autistic survivors of SDV. We then sent a total of 126 invitations to participate out to this email list of potential participants. We also advertised this study as being an autistic-led project. We also used a snowball sampling method where interested participants forwarded the invitations onto their networks.
Recipients responded to these invitations via an online form hosted through Qualtrics. This online form involved answering screening questions about the context(s) of their practice experience along with demographic data (see Table 1). Specific data on participant’s socioeconomic status and race/ethnicity were not recorded as these data were not deemed relevant to this study sample. In addition, demographic data were captured, that is, socio-cultural groupings such as generation and gender identity but has not been included in this article to protect the identity of participants. Of the 20 respondents who completed the form, 16 responded to follow-up emails and scheduled their interview. Two of the 16 participants withdrew from the study prior to their interview.
Participant demographics and practice experience (N = 14).
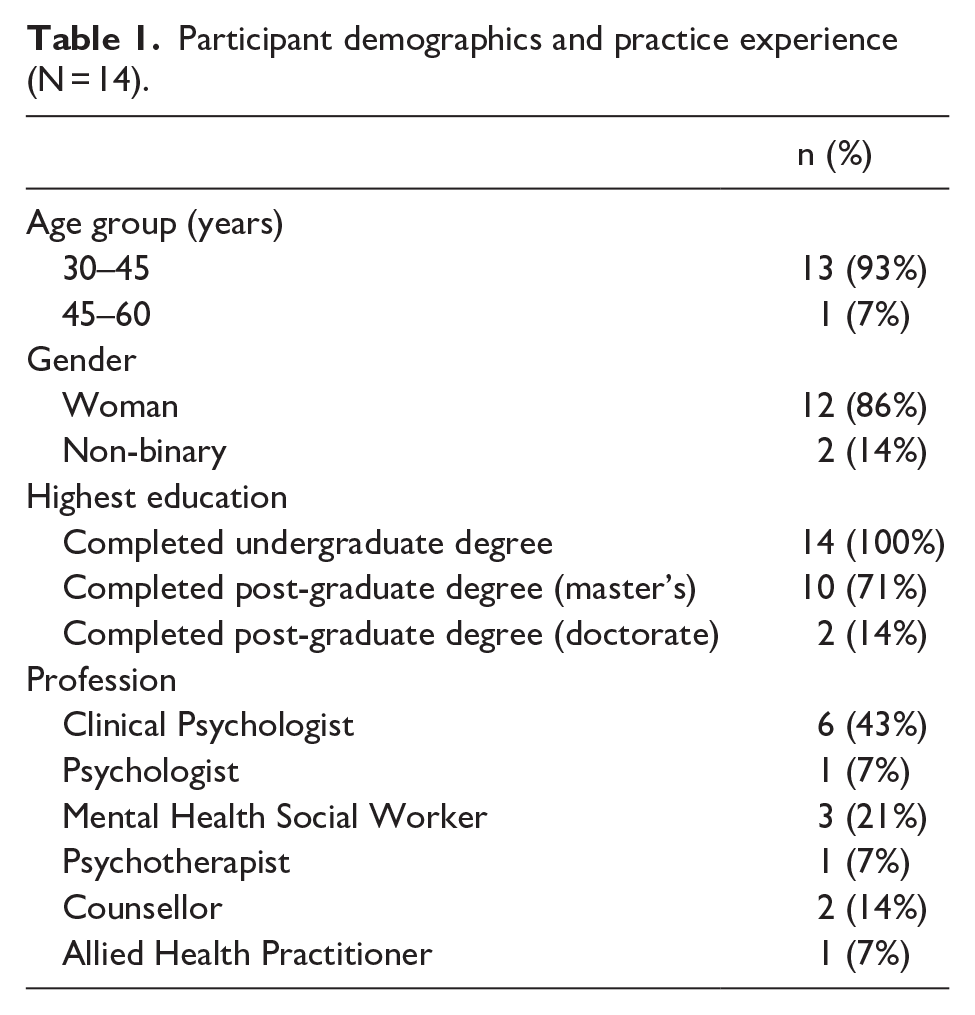
We asked participants about their practice background and experience working with autistic women who are survivors of SDV. The majority of participants were private practitioners; however, several had previously worked within SDV services prior to this. One participant worked with autistic survivors as a both a clinical psychologist and sexual assault counsellor. Many of the participants specialised in working with autistic adults, with several being leaders in their respective fields in terms of training, supervision and resource development. The majority of participants (64%, n = 9) identified as being autistic.
Methodological approach
Interviews
We developed the interview schedule used in this study (see supplementary material) based on analysis of the existing research literature and consultation with an autistic survivor of SDV who provided feedback on the questions. Examples of the interview questions include the following:
What is your approach to supporting the autistic women you work with who have experienced violence?
What factors do you think might make autistic women more vulnerable to victimisation?
What do you think is important for practitioners to consider when working with autistic women who have experienced violence?
J.F conducted semi-structured interviews with 14 participants between March and June 2024. Interviews were between 30 and 60 min in length (mean = 45 min). J.F conducted two interviews over the phone and 12 over video conferencing (Zoom). We sent a copy of the interview questions to participants prior to their interview to allow for additional processing and preparation. We transcribed audio data using AI transcription software. We also gave participants the option of reviewing their interview transcript. Two requested this but did not elect for any changes to be made.
Analysis
We used a hybrid inductive/deductive reflexive thematic analysis approach to analyse the data (Braun & Clarke, 2006; Clarke & Braun, 2017). J.F completed all coding using NVivo software. We used a deductive coding approach for the initial coding phase underpinned by a neurodiversity-informed, intersectional feminist framework. This initial coding process was followed by an inductive coding phase that also built on the deductive codes. We used a combination of semantic and latent approaches throughout the coding and theme development process. J.F completed a coding journal throughout the process to ensure reflexivity around her positionality as an autistic survivor of interpersonal violence. J.F developed the codes into initial themes and sent them to J.A.C. and J.D. who then contributed further analysis and review.
Community involvement statement
The research team for this project comprised one autistic researcher and two non-autistic academics. An autistic survivor of SDV also contributed to this study as a project consultant.
Results
We generated four main themes from the data (see Figure 1) using inductive and deductive codes.
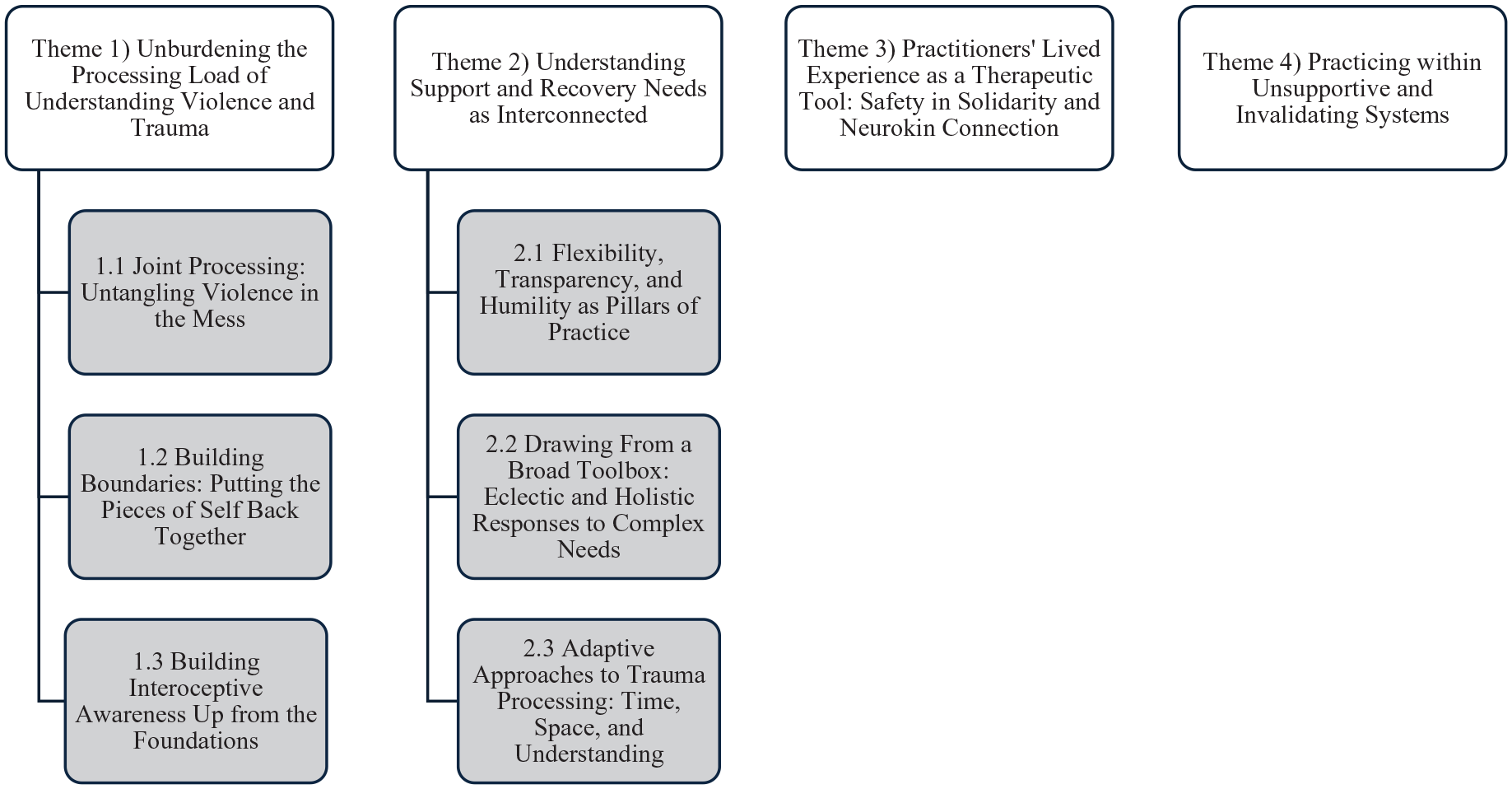
Themes and subthemes.
Theme 1: unburdening the processing load of understanding violence and trauma
Many participants reported that autistic survivors often need support to understand their experiences of SDV and trauma as many are initially confused about what has happened to them and the impacts of this. Support with processing, especially at the intrapersonal and somatic levels, was a key theme in participants’ responses.
Subtheme 1.1: joint processing: untangling violence in the mess
Participants noted that a key element of their approach to supporting autistic survivors involves helping them to process and understand their experiences of SDV. Participants described how this often required explaining what abusive and coercive behaviour is and contextualising this to their client’s situations as autistic survivors may have difficulty understanding this: ‘When they are recognising their experiences of violence, there’s a discrepancy between that sort of contextual and lived experience. So, there’s a lot of work and processing around helping people understand that’ (P7, Counsellor).
Participants also outlined how another important component of this joint processing was de-normalising their client’s experiences of interpersonal violence as it is often frequent and pervasive within their lives. Participants also discussed how the ‘mess’ of violence and abuse can therefore be difficult to delineate and understand within the greater context of interpersonal adversity that autistic people experience and the heightened processing load that this creates. Therefore, participants felt that helping autistic survivors to make sense of their experiences of violence was an essential part of the processing support that they provide:
A lot of the time when someone’s talking about their own trauma, sometimes they just need to dump it all out in this horrible mess, and then you’re going to try and pick it out and represent it to them in a way that they can understand. (P5, Allied Health Practitioner)
Subtheme 1.2: building boundaries by putting the pieces of self back together
An additional part of the support that practitioners provide was around helping autistic survivors to understand their needs and sense of self as part of building boundaries:
I do a tonne of education around boundaries and healthy relationships and what these look like. I try to make it really explicit with clear examples of what red and green flags are. And then figuring out how to support them to be able to advocate – okay, what do we say when people say this? What do we do when people do that? (P4, Mental Health Social Worker)
Participants also noted that a key aspect of helping autistic survivors to identify their needs in relation to their sense of self (and by extension boundaries) centres around undoing a lifetime of having their needs and sense of self-invalidated:
I help them with exploring their sense of self and developing personal boundaries off this. We talk about the concept of needs within that umbrella of personal boundaries, because our needs are so frequently shut down in society. So, encouraging them to think about what their needs are from a relationship. (P7, Counsellor)
Subtheme 1.3: building interoceptive awareness up from the foundations
Differences in interoception (the process by which the nervous system integrates and responds to information about the body’s internal state), possibly in relation to the compounded impacts of trauma and alexithymia (sub-clinical condition associated with difficulties in recognising and describing emotions), were also noted as a barrier that autistic survivors needed support around in terms of processing their experiences: ‘So very much dealing with learning to identify internal states, what are they related to, whether that’s alexithymia, or even dissociation from the trauma that’s created that. And then building awareness of their needs and how to meet these’ (P3, Clinical Psychologist). Participants also talked about supporting autistic survivors to build this awareness in ways that are accessible to them, including guidance in helping them to connect emotional states to experiences in the body:
I think they just need a bit of prompting and maybe a bit of guidance like ‘you say you’ve got butterflies in your stomach, that makes me think of anxiety, do you think it’s anxiety?’ So, in that sense, it’s about making it accessible by giving them a bit more support with it. (P14, Clinical Psychologist)
Theme 2: understanding support and recovery needs as interconnected
The majority of participants espoused a neurodiversity-informed approach as central within their practice. Many participants identified that this approach involves identifying support needs and recovery needs as separate but interconnected, also noting the need for neurodiversity-affirming approaches to trauma. However, several participants also emphasised the importance of understanding the differences and overlapping aspects of a neurodiversity-affirming approach to trauma:
I think one of the big things is to stop confusing trauma with being autistic in terms of how it presents, because it’s both. There are so many myths that it’s all just trauma. So have some humility in the learning process because it’s both and we need to make these accommodations. (P13, Psychologist)
Participants also discussed their experiences of identifying the differences between post-traumatic stress and autistic traits in terms of how it informed their approach to working with autistic survivors: ‘The way I work is treating the symptoms of trauma but affirming the discovery of neurodiversity. And they’re quite different because one can change, and the other doesn’t. So, separating them out is a starting point for me’ (P2, Clinical Psychologist).
Subtheme 2.1: flexibility, transparency and humility as pillars of practice
Participants reported using a range of different psychotherapeutic modalities; however, their approaches were grounded in common principles that helped them centre their clients’ needs. Flexibility in adapting practice to meet people’s support needs was a central component of participants’ approach:
I think being adaptable and flexible. Like my very generous woman who informs me that it’s important for her to infodump
1
, so we spend half an hour infodumping because that gives her spoons. We’ve actually put her sessions longer so that there’s space for that. (P2, Clinical Psychologist)
Flexibility was also essential in validating and affirming their clients’ experiences of the world, particularly in relation to the use of psychoeducation, which participants often spoke about adapting to include information about the intersections of trauma and neurodivergence more broadly.
Direct and explicit communication was also key in fostering transparency as part of this approach: ‘More than anything, being very, very transparent, and open. And just cutting the crap’ (P6, Counsellor). This was also relevant to accommodating different ways of understanding and ensuring communication is accessible to autistic clients: ‘This is this is how I adapt therapy in general, but it’s making the implicit explicit’ (P13, Psychologist). The importance of humility and reflecting on neuronormative assumptions was also an aspect of creating a flexible and transparent approach to practice: ‘You need to consider what neuronormative assumptions you might be making and how this will be invalidating for autistic clients’ (P12, Clinical Psychologist). Neurotypical practitioners noted that this required reflection on how their neurotype position might inform deficit-based assumptions about their autistic clients. Autistic practitioners, on the other hand, discussed how for them this involved understanding that their autistic clients might experience the world in similar but different ways to them.
Subtheme 2.2: drawing from a broad toolbox: eclectic and holistic responses to complex needs
Participants were asked about the ways in which they feel existing approaches and modalities might need to be adapted to meet the needs of autistic survivors. Many participants noted not only that person-centred accommodations were often key in tailoring different modalities to support their clients, but also that drawing on a range of approaches was necessary in meeting the complexity of autistic survivors’ needs. In turn, many participants used an eclectic practice approach which often involved a combination of evidence-based psychotherapy modalities, person-in-environment accommodations and practical support to meet the broad scope of needs that autistic survivors commonly present with:
It’s hard to say what I actually do because I draw from so many different theories and models all together. But I’m drawing from lots of different things to increase regulation and increase understanding of what happened, to then be able to move towards some form of trauma processing. (P13, Psychologist)
A person-in-environment approach to creating a neurosafe space was an important component underpinning participants’ practice:
Just being really mindful of the space and what might be needed in terms of sensory accommodations, having different things available like fidget toys and just kind of chatting with people about what their needs are. And just being mindful of that so that creates more of a safe space. (P11, Mental Health Social Worker)
In line with a neurodiversity-affirming approach, this involves a focus on adapting the environment to the person’s needs, rather constructing their needs as the problem. Participants also noted that practical support, such as helping with social scripting, filling out forms and supporting people with phone calls, was also an essential component of accommodating their client’s needs: ‘Having someone help you fill out the forms or apply to get NDIS 2 support or apply to get a victims recognition payment is going to be so much helpful than just sitting and talking about it sometimes’ (P9, Psychotherapist).
Subtheme 2.3: adaptive approaches to trauma processing: time, space, and understanding
Eye Movement Desensitization and Reprocessing (EMDR) (psychotherapy that uses bilateral stimulation to reduce trauma-related distress) was the most commonly reported modality used by participants. However, several participants spoke about the need to adapt their approach across neurodivergent differences, especially in relation to the integration of information and sensory (including interoception) dimensions of processing:
You need to assess the person’s sensory needs and their sensitivities and make sure you’re taking that into account in therapy with them. Because if the person is in constant sensory overload, they can’t process trauma, like their whole nervous system shuts down. (P10, Mental Health Social Worker)
Another essential consideration is around the time that autistic survivors often need to process trauma and how their recovery journey may take longer because of this:
Often trauma therapy takes a lot longer with autistic clients with complex trauma, and dissociation. Because of the amount of complex trauma, but also it takes longer, and people need more integration time and information processing time. And to rush that you would actually do more harm than good. (P1, Clinical Psychologist)
Theme 3: practitioners’ lived experience as a therapeutic tool: safety in solidarity and neurokin connection
The majority of autistic practitioners drew from both professional and lived experience in supporting autistic survivors. Many of the autistic practitioners were also survivors of SDV, which added an additional layer of lived experience, which participants felt was highly beneficial to their approach:
I personally would not feel comfortable working in a client group that I did not have lived experience in. That might not be the same for every clinician, but I found it’s been invaluable and I don’t think I would be as good a clinician without those lived experiences. (P1, Clinical Psychologist)
In this sense, the therapeutic use of self was an important tool in breaking down barriers within normative practice conventions, bridging divides in understanding, facilitating self-acceptance and building safety within the working relationship.
Participants also discussed how the therapeutic use of self also went beyond just being beneficial from a clinical perspective as they felt that it was essential in establishing a sense of solidarity and community connection with autistic survivors. A key aspect of this solidarity and community connection was facilitating safety through non-judgemental practice and reducing the inherent power differentials that exist within therapeutic relationships. This approach often involved forming a unique therapeutic relationship that transcends the service provider and client dynamic by cultivating a neurosafe space:
I think that by being autistic, it just creates an autistic space where we can be tangential and laugh and be intense and not know the answers. And I think it can be really helpful. I think it just levels the playing field to be honest. (P14, Clinical Psychologist)
Participants who were autistic survivors also expressed how cultivating a neurosafe space through solidarity and neurokin connection was powerful in fostering an overarching sense of healing for their clients, not just from SDV-related trauma, but also from a lifetime of trying to survive in a neuronormative world:
This woman is in her 60s and she just cried, and cried in the counselling room where it was just that real, beautiful sense of everything kind of all coming together. And this person really feeling like this is safe, I’m understood, and the connection was just there straight away. I feel like there’s so much within the work that we do where all we kind of need is the space and the safety. (P6, Counsellor)
Theme 4: practicing within unsupportive and invalidating systems
The majority of participants felt that the systems and structures that exist around their practice created significant challenges rather than the clients themselves. Participants felt that the work they do in fostering a supportive and safe space for autistic survivors to recover was commonly undermined by their clients’ experiences of engaging with other service delivery environments and the inadequacy of Australia’s social support systems.
A lot of external factors being very distressing for the client makes my job harder as a psychologist to be able to a have the client stable enough to do trauma processing. And I think just so many systemic issues and a lack of support for autistic women in general then leaves them in really difficult situations. (P1, Clinical Psychologist)
Participants reported that the recovery process for autistic survivors was often disrupted by cycles of retraumatisation, whereby sessions needed to be spent addressing adverse experiences of help-seeking within neuronormative systems. Many of their clients’ adverse experiences were related to the attitudes and practices that they encountered within these systems, which participants described as being un-affirming and invalidating, as well as underpinned by ableist and neuronormative assumptions:
I get so frustrated when I refer people to services, and they couldn’t get in the door, because someone had been ableist, or made a really invalidating comment. And then I need to try and repair that and then refer again, and now I’ve missed three sessions to be able to process the trauma with a client. So, the opportunity to actually help the person gets impacted by all of this other stuff. (P13, Psychologist)
Participants also touched on how socioeconomic disadvantage and financial hardship/poverty contribute to the vulnerability and distress that autistic survivors experience, which often cannot be addressed through therapeutic practice alone.
Definitely the most enduring challenges, the things that get in the way of the work, are structural. The clients have to work way beyond their capacity to survive, or they’re stuck at home when they really don’t want to be there, or they’re dependent on people in a way they don’t want to be. So, it’s the lack of access to housing, the below the poverty level rate of welfare support payments. And also, just how not autism friendly the world is. (P14, Clinical Psychologist)
These socioeconomic factors also made the trauma recovery process more difficult for autistic survivors due to the lack of stability in their lives, also creating challenges for the practitioners to support their recovery. In addition, these structural disadvantages often increased the risk of autistic survivors being revictimised by entering, or staying in, unsafe situations due to a lack of adequate support.
Discussion
This study explored the experiences of Australian practitioners in supporting autistic women who are survivors of domestic and/or sexual violence (SDV), capturing their insights around the approaches they use, the practice challenges they encounter and their suggestions for improving support services/systems. The findings underline the importance of providing a safe, neurodiversity-affirming, trauma-informed space for autistic survivors to process their experiences and develop an understanding of their support and recovery needs. Here, these findings are discussed in terms of their implications and relevance to existing literature.
This study found that guidance with understanding and processing their experiences of violence and building boundaries for self-protection are key components of supporting autistic women who are survivors of SDV. An essential aspect of this noted by the participants in this study is around the importance of understanding these experiences through the lens of being autistic and the layers of processing involved in this. These findings echo previous qualitative research about the experiences of autistic women who only started to recognise their experiences of violence in retrospect after realising that they are autistic (Bargiela et al., 2016). These findings also highlight the importance of fostering hermeneutic justice for autistic people who are survivors of interpersonal violence in developing a language to understand their experiences and the impact this has on their recovery (Pearson, Rose, & Rees, 2022).
Interoception was also an essential aspect for consideration in supporting autistic survivors of SDV as participants touched on the importance of understanding how neurodivergent differences in interoception may affect trauma processing. Alexithymia was also mentioned as a factor in trauma processing difficulties as autistic people often need more tailored support to identify their emotions and how these are experienced in the body. The link between alexithymia and difficulties with interoception within autistic populations has been well described within previous research (Hatfield et al., 2019; Williams et al., 2023). Additionally, preliminary research with a small sample suggests that specialised interventions aimed at teaching interoceptive awareness to autistic children may hold promise for reducing the interoception difficulties that they experience (Hample et al., 2020). However, this study is the first to explore findings about interoception and alexithymia within the context of interpersonal violence and trauma. The findings of this study suggest that therapeutic and other practice approaches need to assess and consider how difficulties with interoception and alexithymia may create trauma processing barriers for autistic survivors.
Another finding from this study was around the use of a combined neurodiversity-affirming and trauma-informed approach. This combined approach involves fostering an understanding about the complexity in how autistic survivors might experience trauma, including the differences, and overlap, between recovery needs and support needs. Flexibility, transparency and humility were also found to be foundational components of this approach. These findings align with research outlining how humility in reflecting on neuronormative assumptions and flexibility in meeting people’s individual needs are key principles of neurodiversity-affirming practice (Chapman & Botha, 2022). This study expands this to include transparency as another dimension of this approach relevant to trauma-informed practice principles (Pemberton & Loeb, 2020). The importance of flexibility, humility and flexibility in creating safety, both within the service delivery environment and in the working relationship, was also highlighted by this study, which aligns with the insights of Australian autistic service users captured by O’Brien et al. (2024).
Autistic participants in this study who were survivors of SDV also noted that the combination of lived and professional experience was a powerful tool in facilitating safety and connection within the working relationship. Existing research has highlighted the important contribution of autistic researchers and academics in the development of autism knowledge (Botha, 2021; Jones, 2021). Emerging insights have also been explored within the literature about the potential strengths of autistic healthcare professionals in relation to their understanding of autism (Woods, 2024) and the health inequalities and access barriers that autistic populations experience (Doherty et al., 2023). This study provides greater insights around how autistic practitioners can draw on their various lived experiences to facilitate better service delivery outcomes for autistic populations. These findings are also relevant to the emerging understanding of the proposed triple empathy problem which is characterised by difficulties in understanding that arise from the combination of cross-neurotype differences in communication and practitioner–client differences (Shaw et al., 2024). Autistic practitioners therefore have the potential to bridge both of these divides in understanding as they occupy a unique position at the intersection of these experiences.
The primary challenges for Australian practitioners who support autistic survivors arise from the structural disadvantage and levels of retraumatisation and invalidation that autistic survivors often experience when engaging with services. The adversity that autistic women experience in accessing services, particularly in relation to invalidation, has been captured in previous research (Koffer-Miller et al., 2022; Tint & Weiss, 2018); however, this study adds a new dimension of understanding around how this also interacts with the impact of retraumatisation for autistic women who are survivors of SDV. Systemic issues around inadequate levels of support being available to autistic survivors was also a key challenge reported by practitioners in this study. These findings were similar to the challenges reported by Australian practitioners in navigating similar systemic challenges in working with disabled survivors of SDV and how they foster barriers for both service providers and users (Cullen et al., 2022). This study, however, adds to this by elucidating how these challenges, and the barriers associated with them, are experienced by autistic survivors and the practitioners who support them.
Limitations and future directions
This study captured the experiences of practitioners who work with autistic survivors who have the capacity to access and engage with this support. The findings of this study are therefore limited in terms of their applicability to the experiences of autistic survivors who have not engaged with therapeutic support or SDV services. Moreover, this research only captured the experiences of practitioners in terms of their perceptions of the working relationship. The findings of this study should therefore only be considered in terms of the insights that can be gained by practitioners looking to expand their approach to supporting autistic survivors rather than as a reflection of autistic survivors’ experiences. Furthermore, this study was conducted within an Australian context and the findings therefore pertain to Australian support systems. While these insights may also translate across international contexts, particularly those with similar public system models such as the United Kingdom, the findings and implications of this study should primarily be understood within an Australian context.
While this study was underpinned by an intersectional framework, the findings only reflect the broader axes of gender (specifically women) and neurodivergence. Future research into this area should explore how autistic survivors with multiple marginalised identities may experience compounded forms of adversity and disadvantage. This is particularly pertinent to autistic people from marginalised groups who experience interpersonal violence at heightened rates such as gender-diverse people (Cooke et al., 2024), individuals for whom English is a second language (culturally and linguistically diverse groups) (Afrouz & Robinson, 2023; Khawaja & Hebbani, 2024) and people with co-occurring disabilities including learning and intellectual disabilities (Kildahl & Helverschou, 2023). Framing this within an Australian context, future research should also endeavour to capture the dimensions of supporting Indigenous autistic survivors as Indigenous women in Australia experience significantly heightened rates of SDV (Guggisberg, 2019). Further investigation into the experiences of autistic survivors who have not accessed support, and the factors that underpin this, is also needed to capture a more holistic understanding of access barriers.
Conclusion
This study sought to investigate the experiences of Australian practitioners in relation to the approaches that they use to support autistic survivors of SDV, illuminating the factors that create challenges for them and recovery barriers for the women that they support. The findings highlight how supporting autistic survivors with processing and understanding their experiences are key recovery support needs. Practitioners also emphasised the importance of responding to autistic survivors in ways that affirm their support needs while also validating their recovery needs. The main challenges reported by Australian practitioners were related to the structural disadvantage that autistic survivors face, the invalidation and retraumatisation that they experience when accessing support services, and the ways in which these foster additional recovery barriers. Addressing these barriers is essential to alleviating these practice challenges and improving the support available to Australian autistic survivors.
Footnotes
Acknowledgements
We wish to acknowledge Ranae Zollner for their contribution as a project consultant. We also wish to acknowledge all of the participants who gave up their time to be part of this project.
Author Contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
Ethical approval for this study was obtained from the Queensland University of Technology’s Human Research Ethics Committee (UHREC). Approval number: LR 2023-7365-1582.
Consent to participate
Informed consent to participate in this study was obtained both in writing and verbally during participant’s interviews. Participants were distributed an expression of interest form via a Qualtrics link which contained all required information about the study, including the potential risks of harm associated with participation, and option to give informed consent through a digital signature.
Consent for publication
Informed consent for publication was provided verbally by participants during their interviews.
Data availability statement
Data is not publicly available for this project due to the sensitive nature of the topic and potential risk of participants being identified based on their data.