
Abstract
This study sought to characterize caregiver concerns for autistic children receiving care in two public service systems—schools and mental health programs—and to identify child and family characteristics associated with these concerns. Caregivers of 353 school-age autistic children in mental health services (n = 192) or schools (n = 161) named, in their own words, the top three concerns for their child. A modified version of Weisz et al.’s Top Problem coding system was developed to expand beyond the original codes, capturing child emotional and behavioral problems, autism features, and adaptive behaviors. Most caregivers (61.8%) identified externalizing behaviors like aggression, as well as social differences (36.3%) and attention difficulties (35.4%) as top problems. Caregivers also mentioned autism-specific concerns related to social responsiveness (54.7%). Participant characteristics, including child age and caregiver race/ethnicity, were associated with concerns. Controlling for child age and caregiver ethnicity, concerns differed by setting; caregivers in mental health (vs. school) settings named more externalizing behaviors, while those in school settings named more restricted repetitive behaviors and social differences. Findings highlight the need to implement setting-specific interventions individualized to caregivers’ priorities and to ensure opportunities for cross-system coordination.
Lay abstract
This study explored what concerns caregivers have about their autistic children when receiving care from either mental health programs or schools. Caregivers shared, in their own words, the top three concerns they worry about most for their child. Caregivers had many different concerns, including worries about their child’s emotions and behaviors, autism-related traits, daily living skills, and ability to manage feelings and behavior. The study also found that caregivers’ concerns were linked to family characteristics like their child’s age, the caregiver’s race or ethnicity, and how many children live in the home. Caregivers’ concerns also differed based on where they were getting help. Caregivers in mental health programs were more likely to worry about challenging behaviors like aggression. Caregivers in school settings were more likely to be concerned about their child’s social skills and repetitive behaviors. These findings help us better understand what caregivers worry about when seeking support for their child. The findings also show why it is important to use the right strategies in each setting to meet the specific needs of caregivers and their children.
Autistic children receive care in multiple public service systems, including education and mental health, to address their diverse social, behavioral, academic, and mental health needs (Brookman-Frazee et al., 2018; Stadnick et al., 2020; Tamm et al., 2020). Caregivers play a pivotal role in initiating, sustaining, and mediating their child’s services (Pellicano et al., 2014). Integrating caregiver perspectives regarding their child’s service needs—widely considered a best practice in the education of autistic children—can increase caregiver engagement, strengthen provider−caregiver working alliances and family−school partnerships, and ensure that services align with the specific priorities of autistic children and their families (LaBarbera, 2017; Stadnick et al., 2013; Tschida et al., 2021). Indeed, this form of family-centered care is particularly critical to engage racially and ethnically diverse families of autistic children given existing disparities in service use (Smith et al., 2020). Hence, a growing body of literature has sought to examine caregiver concerns for autistic children within various service settings, including schools (e.g. Azad & Mandell, 2016; Hastings et al., 2022) and mental health settings (e.g. Brookman-Frazee et al., 2018). However, to date, no study has characterized caregiver emotional and behavioral concerns, as stated in their own words, across multiple service systems. This study investigates the concerns of caregivers of autistic children receiving care in two public service systems (mental health and schools).
Measuring caregiver concerns
Behavioral concerns for autistic children are predominantly evaluated through standardized caregiver self-report inventories (e.g. Achenbach et al., 2003; Constantino & Gruber, 2012; Goodman, 1997). While these standardized measurement approaches allow researchers and clinicians to gather norm-referenced data about their participants and clients, there is a growing appreciation for more individualized approaches which are client-centered, open-ended, and yield information unique to the individual and their experiences (Barlow & Nock, 2009). The Top Problems assessment is a client-centered approach that asks caregivers to name, rank, and rate the severity of the top three emotional or behavioral concerns they wish to prioritize in their child’s services, designed to complement standardized symptom measures and facilitate caregivers in sharing their primary concerns in their own words (Weisz et al., 2011). To date, few studies have used the Top Problems assessment to explore caregiver concerns for autistic children. Wood and colleagues (2022) used the Top Problems assessment to examine trajectories of caregivers’ autism-specific concerns in the context of clinical trial participation, finding the assessment to be a valid and reliable measure of autism features (Wood et al., 2022). Azad and Mandell (2016) applied this assessment approach to explore caregivers’ top school-related concerns (e.g. academics, communication) in public school settings, finding high concordance between caregiver and teacher concerns for school-age autistic students. To shed light on the concerns that bring autistic children into care across service settings, the current study applied the Top Problems assessment in schools and outpatient mental health clinic settings.
Caregiver concerns across service systems
Mental health services
Autistic children increasingly rely on publicly-funded mental health services, with common presenting problems being externalizing behaviors, followed by social differences, attention/regulation problems, and anxiety/fears (Brookman-Frazee et al., 2012). Co-occurring psychiatric disorders are also highly prevalent among autistic children in these settings. Indeed, in a diverse sample of autistic children receiving care in publicly funded mental health programs in Southern California, nearly all children met diagnostic criteria for at least one co-occurring psychiatric disorder—most commonly Attention-Deficit/Hyperactivity Disorder (ADHD), Oppositional Defiant Disorder (ODD), and Anxiety Disorders—with an average of more than two co-occurring diagnoses per child (Brookman-Frazee et al., 2018). Child factors associated with these diagnoses included gender (boys were more likely to have ADHD than girls), autism-related traits (associated with higher likelihood of meeting criteria for anxiety disorder), and externalizing behavior challenges (associated with higher likelihood of ADHD and ODD; Brookman-Frazee et al., 2018). A handful of additional studies have sought to characterize caregiver concerns for autistic children in publicly funded mental health settings via standardized psychiatric symptom measures (e.g. the Child Behavior Checklist (CBCL); Achenbach et al., 2003), finding affective, ADHD-related, and oppositional/conduct problems to be among the most commonly endorsed concerns (Boulton et al., 2023; Hutchison et al., 2024; Muratori et al., 2019).
School services
The number of children with an educational classification of autism in U.S. public schools has increased by nearly 500% over the past two decades (Cardinal et al., 2021). While schools are mandated to involve caregivers in the development of children’s Individualized Education Program (IEP), limited attention has been devoted to understanding what caregivers’ primary concerns are (Reiman et al., 2010; Rossetti et al., 2021). Azad and Mandell (2016) assessed caregiver and teacher concerns via the Top Problems assessment, finding that the most common caregiver concerns pertained to social interaction, followed by externalizing behavior, academics, and communication. Notably, this study did not examine demographic correlates of these concerns. International studies in school settings have largely examined caregiver concerns using standardized norm-referenced inventories (e.g. Ashburner et al., 2010; Ding et al., 2010; Hastings et al., 2022). For example, Hastings and colleagues (2022) assessed caregiver-reported emotional and behavioral problems among autistic U.K. public school students via the Strengths and Difficulties Questionnaire. Not surprisingly, caregivers of autistic children reported higher levels of emotional differences, conduct problems, hyperactivity, and peer interaction challenges relative to national norms. Boys exhibited greater hyperactivity than girls, autism features were associated with emotional symptoms, and socioeconomic disadvantage was associated with emotional, conduct, and peer interaction problems.
Given the growing number of autistic children relying on public sector services, characterizing caregivers’ primary concerns is critical for practice and policy. For providers, understanding these concerns may improve awareness of the diverse emotional and behavioral profiles of autistic clients, an increasingly recognized need expressed by autistic self-advocates, caregivers, and providers within the autism community across multiple service settings (Brede et al., 2022; Williams & Haranin, 2016). At a systems level, understanding the prevalence of these concerns, how they relate to family characteristics, and how they vary across service settings may inform more strategic selection of evidence-based intervention protocols for implementation within each setting, enhancing individualization of services and improving child outcomes.
The current study
Despite the growing number of autistic children receiving public services, no study has comprehensively evaluated caregiver priorities, as stated in their own words, across multiple service systems. In addition, there is limited research on how child and family characteristics relate to caregiver concerns, which is crucial for individualized and culturally responsive care. The current study had three aims: (1) to understand the primary concerns that are motivating service engagement among caregivers of autistic children in publicly funded educational and mental health settings, as described on their own terms; (2) to examine how child and family characteristics may relate to these caregiver concerns; and (3) to assess whether the caregiver concerns motivating service engagement differ depending on where families present for care. Given the dearth of prior research examining caregiver concerns across multiple service systems in this population, the current study is exploratory, and we did not assert a priori hypotheses.
Method
Baseline data for the current study were extracted from the Translating Evidence-Based Interventions for ASD: Multi-level Implementation Strategy (TEAMS) project (Brookman-Frazee & Stahmer, 2018; Brookman-Frazee et al., 2025). TEAMS includes two linked, cluster randomized hybrid type 3 implementation trials conducted in California testing implementation strategies for two autism evidence-based interventions—An Individualized Mental Health Intervention for Autism (AIM HI; Brookman-Frazee et al., 2016) in mental health programs (Study 1) and Classroom Pivotal Response Teaching (CPRT; Suhrheinrich et al., 2011)—in schools (Study 2). Child and caregiver participants were drawn from the caseloads or classrooms of providers participating in the TEAMS project.
Participants
Participants in this study were caregivers of the 353 autistic children (Mage = 7.89 years, SDage = 2.92, rangeage: 3−13, 80.2% male, 46.4% Hispanic/Latinx) enrolled in the combined TEAMS Project. Study 1 (Mental Health) participants included caregivers of 192 children (Mage = 9.71 years, SD = 2.92, range: 4−13, 77.4% male, 59.6% Hispanic/Latinx). To be eligible, children had to be between 5 and 13 years old with an existing autism diagnosis on record with both the parent and child speaking English or Spanish as their primary language. Study 2 (School) participants included caregivers of 161 children (Mage = 6.25 years, SD = 2.39, range: 3−11, 82.8% male, 35.0% Hispanic/Latinx). To be eligible, children had to be between 3 and 10 years of age with a primary educational classification of autism with both the parent and child speaking English or Spanish as their primary language. See Table 1 for a summary of participant characteristics as reported by caregivers by study.
Participant characteristics.
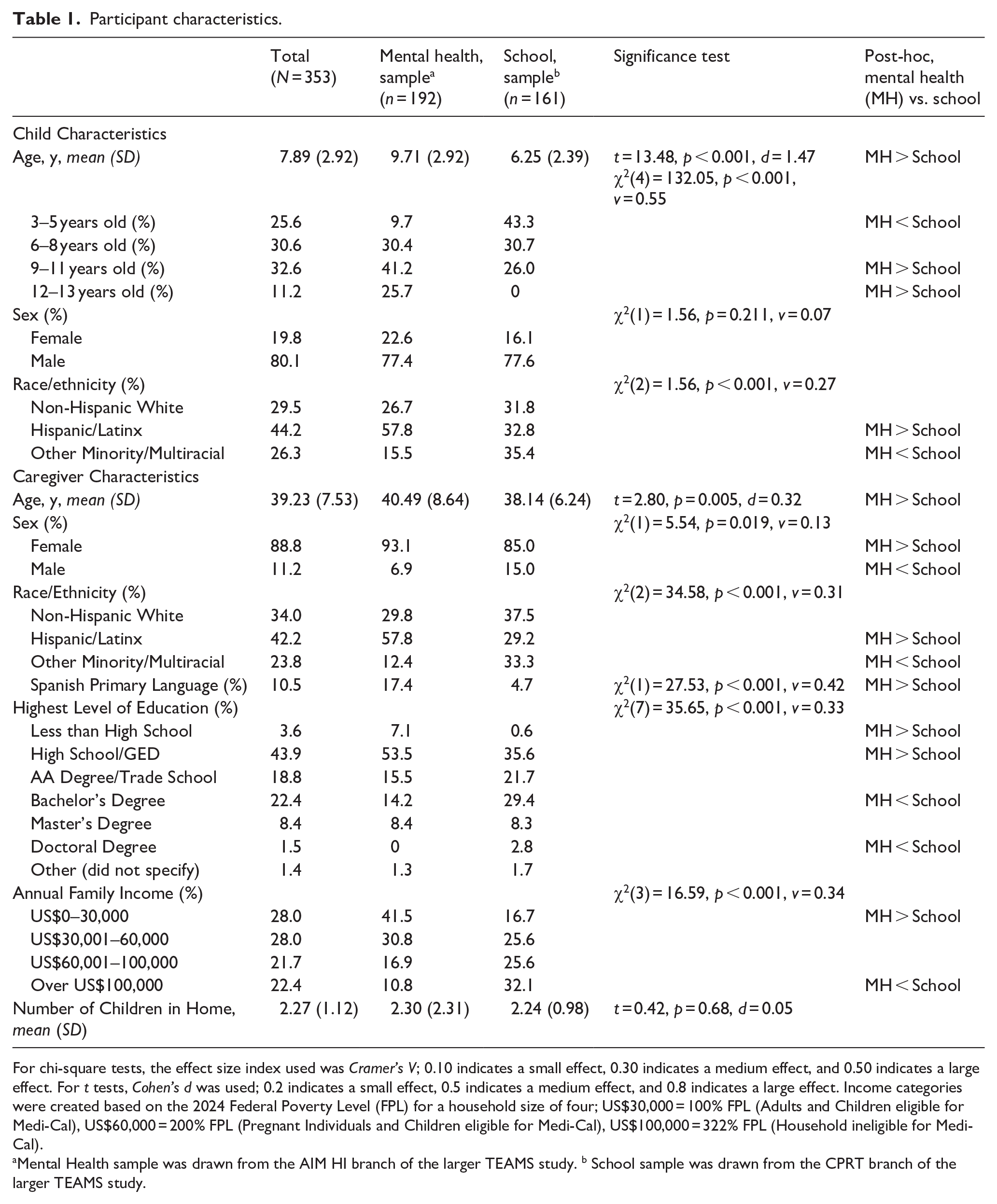
For chi-square tests, the effect size index used was Cramer’s V; 0.10 indicates a small effect, 0.30 indicates a medium effect, and 0.50 indicates a large effect. For t tests, Cohen’s d was used; 0.2 indicates a small effect, 0.5 indicates a medium effect, and 0.8 indicates a large effect. Income categories were created based on the 2024 Federal Poverty Level (FPL) for a household size of four; US$30,000 = 100% FPL (Adults and Children eligible for Medi-Cal), US$60,000 = 200% FPL (Pregnant Individuals and Children eligible for Medi-Cal), US$100,000 = 322% FPL (Household ineligible for Medi-Cal).
Mental Health sample was drawn from the AIM HI branch of the larger TEAMS study. b School sample was drawn from the CPRT branch of the larger TEAMS study.
Procedure
Informed written consent was obtained from all caregivers. At study baseline, caregivers completed the Top Problems Assessment (Weisz et al., 2011), a demographics questionnaire, and additional survey measures to assess caregiver perceptions of child behaviors. All procedures were approved by the University of California, San Diego Institutional Review Board.
Measures
Child and caregiver characteristics
Caregivers reported demographic information, including age, gender, race/ethnicity, income, education, and preferred languages through a demographic interview with study personnel administered at baseline.
Top problems assessment
Caregivers completed Weisz and colleagues’ (2011) Top Problems assessment via interview with postbaccalaureate and doctoral-level study personnel. Study personnel were trained to administer the Top Problems assessment interview by doctoral-level clinicians. Training involved review of the Top Problems administration protocol (Weisz et al., 2011), participation in mock interviews with trainers, and conducting a Top Problems assessment with live supervision. Trained study personnel contacted caregiver participants via a scheduled phone call, which generally lasted between 20 and 30 min. Study personnel did not have any relationship with the study participants prior to this call; participants who agreed to receive further information about the study were informed via email that they would be contacted by a member of the research team to review the consent form and complete a brief prestudy interview. Immediately following review of the caregiver consent form, caregivers were asked to report and rank the top three problems (e.g. emotional or behavioral challenges, challenges related to autism features, challenges with social communication or daily living skills) they were most concerned about, using prewritten prompts and probes. Following indication of top problems, caregivers rated the severity of each problem from 0 (not a problem at all) to 10 (very much a problem). Study personnel wrote down caregivers’ top problems verbatim and their corresponding rank and severity level, which were later coded by a separate coding team; interviews were not recorded. The Top Problems assessment has been used to measure emotional and behavioral concerns among non-autistic youth in community-based outpatient treatment, demonstrating strong test–retest reliability, sensitivity to treatment, and strong convergent validity with established measures of youth psychopathology (Weisz et al., 2011). The Top Problems assessment has also been used to measure caregiver and teacher academic concerns, demonstrating high concordance between caregiver and teacher concerns for school-age autistic students (Azad & Mandell, 2016), as well as autism-related traits among autistic youth in the context of clinical trial participation, demonstrating short-term test–retest reliability, sensitivity to treatment, and strong convergent validity with established measures of autism-related traits (Wood et al., 2022).
Coding manual
The current study used Weisz et al.’s (2011) coding procedure, which uses a directed deductive content analysis approach to classify top problems according to items on the CBCL (Achenbach et al., 2003). As the current sample included children aged 3 through 13, the coding scheme included codes that aligned with the preschool (1.5−5 years) and school-age (6−18 years) editions, for a total of 166 unique items. Coding procedures developed by Wood et al. (2022) were also employed to classify top problems aligned with the 65 items on the Social Responsiveness Scale–Second Edition (SRS-2; Constantino & Gruber, 2012). In addition, we expanded the Top Problems classifications to include concerns that related to adaptive behavior that were not covered by the codes described above. Drawing upon definitions and subscales from the Vineland Adaptive Behavior Scale−Third Edition (VABS-3; Sparrow et al., 2016), we developed three Communication Skills codes (i.e. Receptive Language, Expressive Language, and Written Language) and three Daily Living Skills codes (i.e. Personal, Domestic, and Community Living Skills). Finally, many caregivers described their child’s Top Problem as “emotion regulation” or “self-regulation” without further specifying behaviors; hence, we incorporated a General Regulation Difficulties category to capture these comments. The full coding manual is available upon email request to the first author.
Coding training and procedure
A doctoral-level clinical psychology student (L.R.B.) and two undergraduate research assistants majoring in psychology coded the Top Problems interview. Coders were trained through manual review and group didactic training. Coders were permitted to code independently once they reached a Cohen’s (1960) kappa of 0.65 (p < 0.05) indicating good agreement with master coder classifications on a set of criterion or “gold standard” comments for training purposes (Cohen, 1960). Coders determined the occurrence (1) or non-occurrence (0) of each of 238 top problem codes (166 CBCL items; 65 SRS-2 items; six VABS-3 items; one Emotion Regulation item) for each caregiver-reported top problem. They could assign multiple codes if indicated. If coders were unable to assign a code to a caregiver-reported problem, these problems were examined by two doctoral-level clinical psychology students, who independently coded these descriptions and then met to achieve consensus. Top problems falling outside the scope of the coding scheme (e.g. “parents’ divorce”) and those deemed too vague or brief (e.g. “coping skills” or “emotions”) were not coded; these represented less than 1% of responses. Monthly booster sessions were held with coders to prevent coder drift.
Reliability
Twenty-five percent of the caregiver-reported top problems were double-coded to assess interrater agreement, which was, on average, kappa = 0.78 (SD = 0.32), indicating substantial agreement (Cohen, 1960; McHugh, 2012).
Scoring
Each item on the Top Problems coding scheme corresponded to one or more of the following scales or subscales. Primary Top Problem scales included CBCL Externalizing Problems (including Aggression and Rule-Breaking Behavior subscale items) and Internalizing Problems (including Anxiety, Withdrawn/Depressed, Emotional Reactivity, and Somatic Problems subscale items), SRS-2 Social Communication and Interaction and Restricted Repetitive Behaviors scales, VABS-3 Communication Skills scale and Daily Living Skills scales, and the General Regulation Difficulties single-item scale. Other Top Problems subscales included the following CBCL subscales: Aggression, Rule-Breaking Behavior, Anxiety, Withdrawn/Depressed, Emotional Reactivity, Somatic Problems, Attention Problems, Sleep Problems, Social Problems, Thought Problems, and Other Problems. A dichotomous presence variable was created for each scale/subscale represented on the Top Problems coding scheme, with a “1” indicating that a participant named a problem that was coded within a given scale/subscale in at least one of their top three problems, and a “0” indicating that they did not name a problem coded under the scale/subscale within their top problems. Scoring syntax is available upon request.
Community involvement statement
The TEAMS project included work with community members with lived experience, including families, providers, leaders, and community advisory boards, in all phases in an advisory capacity (Brookman-Frazee et al., 2020; Stahmer et al., 2012; Suhrheinrich et al., 2020).
Data analysis
Descriptive statistics for participant characteristics were computed using SPSS Version 28. Chi-square tests, independent-samples t tests, and multiple regression analyses were run to identify group differences between the mental health and school samples. To characterize caregiver concerns (Aim 1), frequencies for each Top Problem subscale were computed for the combined sample and the mental health and school samples. To determine whether child and family characteristics were associated with caregiver concerns (Aim 2), bivariate correlations were run between participant characteristics and the seven primary Top Problem scales (i.e. CBCL Externalizing Problems, CBCL Internalizing Problems, SRS-2 Social Communication and Interaction, SRS-2 Restricted Repetitive Behaviors, VABS-3 Communication Skills, VABS-3 Daily Living Skills, and the General Regulation Difficulties single-item). For continuous variables, Pearson point-biserial correlations were used (coefficient r); for binary variables, phi (φ) coefficients were used. To determine whether caregiver concerns differed by service setting over and above child and family characteristics (Aim 3), a multivariable logistic regression analysis was run with setting (mental health vs school) as the binary outcome variable and the primary Top Problem scales as independent variables. Child age and caregiver ethnicity (Hispanic vs non-Hispanic) were included as covariates in this model as they were associated with at least one Top Problem scale (p < 0.05) and significantly differed by setting. To further explore the specific factors associated with setting differences on the primary Top Problem scales, we conducted a post hoc sensitivity analysis with setting (mental health vs school) as the binary outcome variable and the CBCL subscales as independent variables in a multivariable logistic regression, controlling for child age and caregiver ethnicity.
Results
Descriptive statistics and participant demographics
Table 1 summarizes participant characteristics. Mental health and school participants significantly differed on child age, child race/ethnicity, caregiver age, caregiver sex, caregiver race/ethnicity, caregiver education, household income, and caregiver primary language.
Characterizing caregiver concerns (Aim 1)
Caregiver Top Problem frequencies for the total sample and within each sample are presented in Table 2. In the total sample, 99.2% of caregivers reported at least one CBCL item as a Top Problem; 61.8% reported at least one CBCL Externalizing top problem, and 54.7% reported at least one CBCL Internalizing top problem. The most common CBCL subscales reflected in the sample were Aggression (61.8% of caregivers), Social Problems (36.3%), Attention Problems (35.4%), and Withdrawn/Depressed (34.8%). In the total sample, 54.7% of caregivers named at least one SRS-2 item as a Top Problem; 45.9% reported an item on the Social Communication/Interaction subscale; and 18.1% reported an item on the Restricted Repetitive Behavior subscale. About 15.3% of caregivers named at least one VABS-3 Communication Skills−related top problem, and 10.5% named at least one VABS-3 Daily Living Skills−related top problem. About 9.1% of the total sample reported General Regulation Problems as a Top Problem. A sample of caregiver-reported top problems and their corresponding codes is presented in Table 3.
Caregiver-reported “top problems” by service setting.
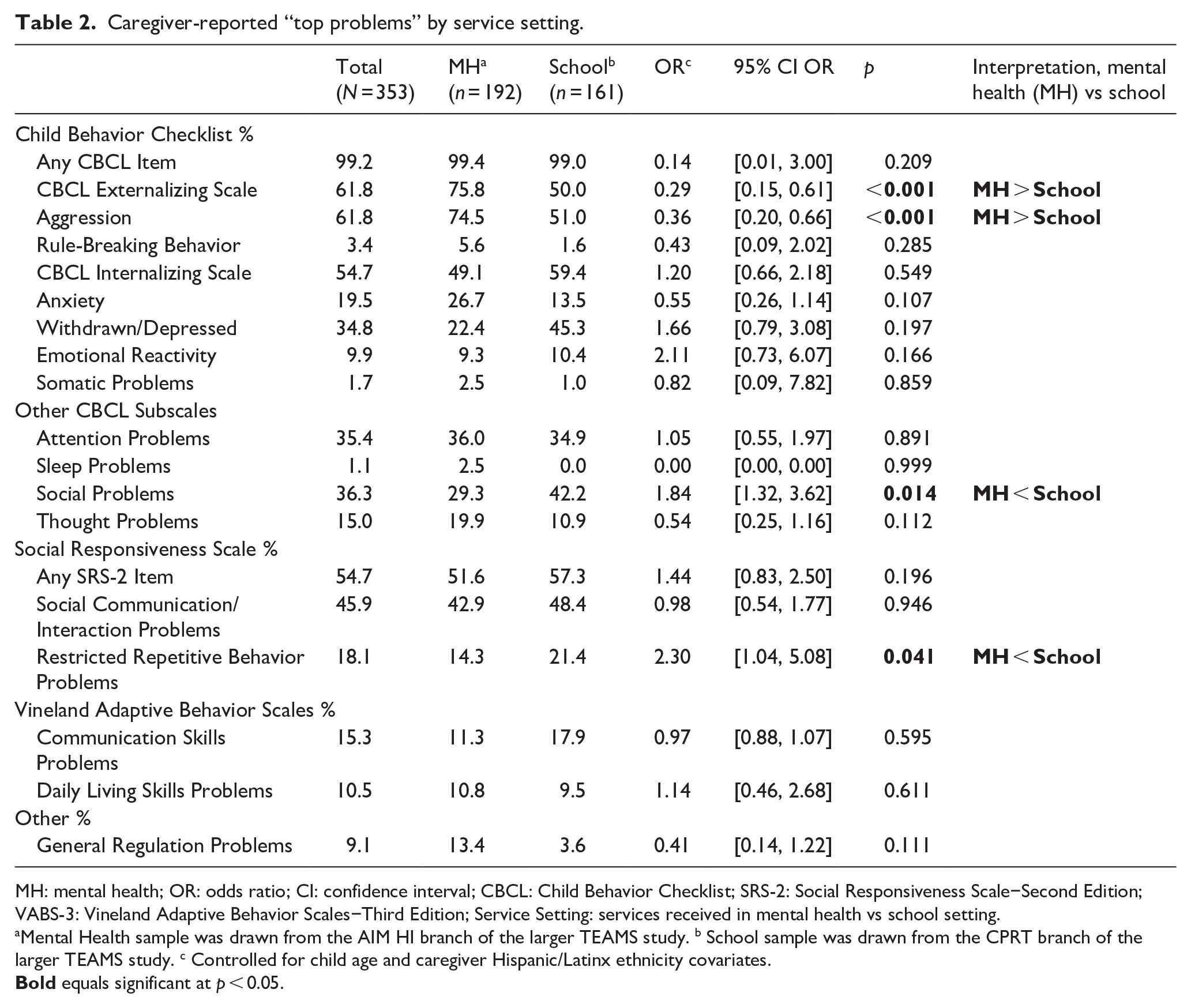
MH: mental health; OR: odds ratio; CI: confidence interval; CBCL: Child Behavior Checklist; SRS-2: Social Responsiveness Scale−Second Edition; VABS-3: Vineland Adaptive Behavior Scales−Third Edition; Service Setting: services received in mental health vs school setting.
Mental Health sample was drawn from the AIM HI branch of the larger TEAMS study. b School sample was drawn from the CPRT branch of the larger TEAMS study. c Controlled for child age and caregiver Hispanic/Latinx ethnicity covariates.
Sample top problems and corresponding codes.
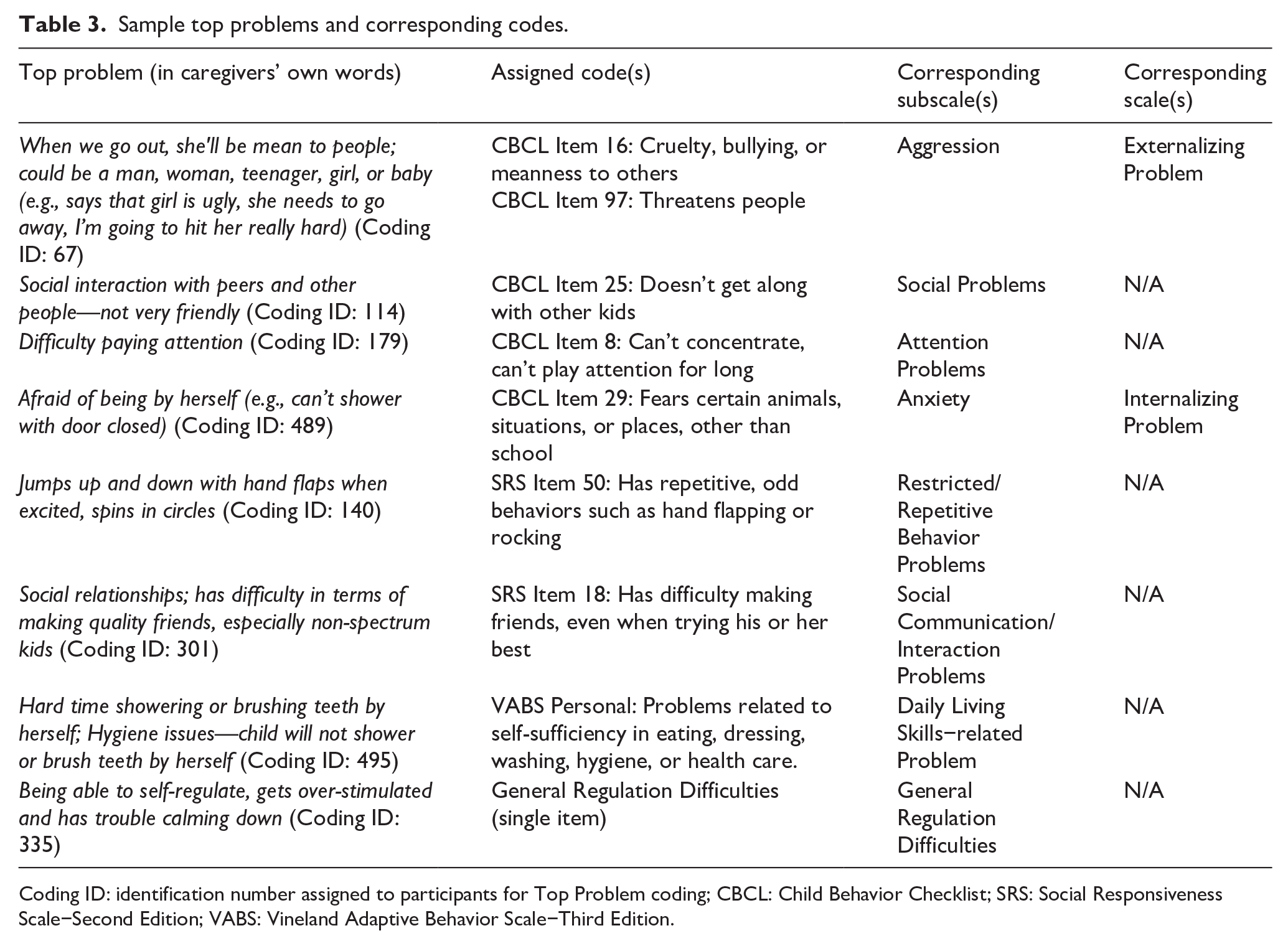
Coding ID: identification number assigned to participants for Top Problem coding; CBCL: Child Behavior Checklist; SRS: Social Responsiveness Scale−Second Edition; VABS: Vineland Adaptive Behavior Scale−Third Edition.
Associations between child and family characteristics and caregiver concerns (Aim 2)
Associations between child and family characteristics and caregiver concerns are displayed in Table 4. Child age was negatively associated with CBCL Internalizing Top Problems (r = −0.11, p = 0.039) and VABS-3 Communication Skill Top Problems (r = −0.18, p < 0.001), and positively associated with VABS-3 Daily Living Skill Top Problems (r = 0.12, p = 0.035). Caregiver race/ethnicity was associated with CBCL Externalizing Top Problems, such that other Minority/Multiracial individuals (vs Latinx/Hispanic individuals) were more likely to report a CBCL Top Externalizing Problem (φ = 0.16, p = 0.010). Number of children in the home was positively associated with VABS-3 Communication Skills Top Problems (r = 0.12, p = 0.023). Child sex, child race/ethnicity, caregiver preferred language, and caregiver education were not significantly associated with any primary Top Problem scales, ps > 0.05.
Bivariate associations between child and family characteristics and top problems.
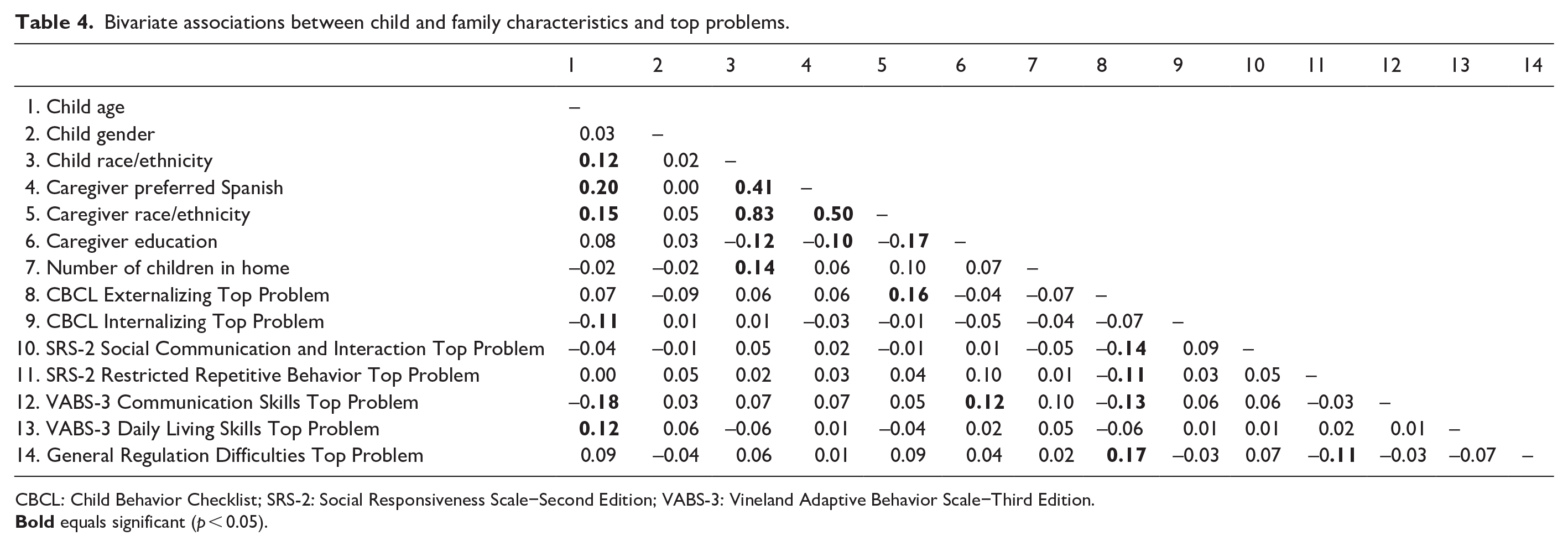
CBCL: Child Behavior Checklist; SRS-2: Social Responsiveness Scale−Second Edition; VABS-3: Vineland Adaptive Behavior Scale−Third Edition.
Comparing concerns between mental health and school service settings (Aim 3)
Multiple logistic regression analysis (Table 2), controlling for child age and caregiver ethnicity covariates, found that caregiver concerns significantly differed by service setting, χ2(9) = 181.88, p < 0.001, Nagelkerke’s R2 = 0.559. Specifically, those from school (vs mental health) settings were less likely to report a CBCL Externalizing Top Problem (odds ratio (OR) = 0.29, p < 0.001) but more likely to report an SRS-2 Restricted Repetitive Behavior Problem (OR = 2.30, p = 0.041). Post hoc sensitivity analyses, controlling for child age and caregiver ethnicity, found that caregiver concerns on the CBCL subscales also significantly differed by setting, χ2(12) = 188.93, p < 0.001, Nagelkerke’s R2 = 0.575. Specifically, those from school (vs mental health) settings were less likely to report a top problem on the CBCL Aggression subscale (OR = 0.32, p < 0.001) but more likely to report a top problem on the CBCL Social Problems subscale (OR = 1.84, p = 0.014). No other CBCL subscales differed by service setting, ps > 0.05.
Discussion
This study investigated the primary concerns of caregivers of autistic children receiving care in two public service systems (mental health and schools). Almost all caregivers named at least one concern that corresponded to an item on the CBCL, with most reporting externalizing problems like aggression, as well as attention and social problems. Caregivers also frequently named autism-specific concerns corresponding to items on the SRS-2, particularly those related to social communication. Family characteristics including child age, caregiver race/ethnicity, and number of children in the home were associated with caregiver concerns. Caregiver concerns significantly differed by service setting, controlling for child age and caregiver ethnicity. Caregivers from mental health (vs school) settings were more likely to report CBCL Externalizing problems, particularly those on the CBCL Aggression narrowband subscale. Those from school (vs mental health) settings were more likely to report concerns on the SRS-2 Restricted Repetitive Behavior subscale and the CBCL Social Problems subscale.
Although all of the children in the sample were autistic, the majority of caregivers reported concerns related to behaviors that were not autism-specific, but rather reflected a range of mental health−related challenges. Most caregivers reported externalizing behavioral concerns, which is consistent with prior research on the top reasons for referral to mental health services among autistic children (Brookman-Frazee et al., 2012). Our findings expand on previous work by elucidating the specific mental health concerns reported by caregivers, including aggression, attention problems, social problems, depressive symptoms, and anxiety, which align with prevalence data on co-occurring psychiatric conditions in autistic children receiving publicly funded mental health services (Brookman-Frazee et al., 2018). These findings help enhance the field’s general awareness of prevalent mental health concerns among autistic children, which is an increasingly recognized training need for providers. Indeed, in a study of mental health clinicians working in publicly funded mental health agencies in Southern California, nearly half of providers reported that they did not feel comfortable diagnosing mental health needs in autistic children, most reported low confidence in providing mental health interventions to autistic children, and nearly one third felt that the mental health system was not an appropriate place for their autistic client (Williams & Haranin, 2016). Similarly, in a survey of 300 educators in California, training in mental health and behavioral interventions was identified as a primary need for teachers of autistic children (Schetter & England, 2015). Increasing providers’ awareness of the diverse mental health needs faced by autistic clients has the potential to reduce diagnostic overshadowing and increase provider confidence and training efforts. These findings suggest that greater clinical attention to the mental health needs of autistic children is imperative.
This study also identified several child and family characteristics associated with caregiver concerns. As child age increased, caregivers were less likely to report communication skill-related concerns and more likely to report daily living skill−related concerns. These differences may reflect a shift in focus from communication to daily living skills as children grow older and as communication skills improve through maturation, with exposure to schooling or other supportive services. Surprisingly, the likelihood of caregivers reporting internalizing concerns decreased with child age, contrary to expectations given that internalizing problems typically increase with age in this population (Vaillancourt et al., 2017). This unexpected finding may be partly due to double-coding of caregiver statements onto both the CBCL internalizing and SRS-2 Social Communication subscales, which both showed a similar negative association with child age. For example, the top problem “doesn’t verbally communicate feelings” could be coded onto the CBCL Withdrawn/Depressed subscale item “refuses to talk” and the SRS-2 Social Communication subscale item “isn’t able to communicate his or her feelings to others,” per Weisz et al.’s (2011) and Wood et al.’s (2022) original Top Problem coding manuals. Hence, while several problems mapped onto CBCL internalizing items, some may be better captured by autism features, particularly within the social communication domain.
In addition, the number of children in the home was positively associated with communication skill-related concerns, possibly due to a greater necessity to communicate one’s own needs or increased social comparison across siblings, highlighting social communication difficulties. Although recent research suggests that having siblings may, in fact, improve social interaction for autistic children (Ben-Itzchak et al., 2019), social communication may be highlighted as a difference. There were also differences in caregiver concerns by race/ethnicity. Hispanic/Latinx caregivers were less likely to report externalizing behavioral concerns than other racial/ethnic minorities, aligning with literature suggesting that Hispanic/Latinx caregivers of autistic children are less likely to perceive or report their child’s behaviors as burdensome (Rivera-Figueroa et al., 2022; Sanner et al., 2023). Taken together, these findings offer preliminary insight into demographic factors that may influence caregivers’ primary concerns for autistic children across school and mental health service settings. Such findings may be of particular utility to providers, who may leverage clients’ background information to further individualize care.
Finally, the current study is the first to illuminate differences in caregiver concerns between mental health and school settings. Controlling for differences in child age and caregiver ethnicity, caregivers in the mental health (vs school) sample were more likely to report externalizing behavioral concerns, particularly aggression. These findings align with prior data on the prevalence of ODD in this population (Brookman-Frazee et al., 2018), and reflect the focus of mental health systems on addressing externalizing behaviors (Brookman-Frazee et al., 2012). The high prevalence of externalizing behavioral concerns in this sample signals a high clinical need, suggesting that providers—particularly those within publicly-funded mental health settings—should be prepared to address co-occurring externalizing behaviors among their autistic clients. At a systems level, the findings signal a need to implement interventions that specifically target externalizing symptoms, especially in publicly funded mental health contexts.
Controlling for differences in child age and caregiver ethnicity, caregivers in the school (vs mental health) sample were more likely to report social differences as a primary concern, consistent with prior findings on school-based concerns (Azad & Mandell, 2016; Hastings et al., 2022). This is unsurprising, as the school setting inherently involves more peer interactions, which may make goals in supporting social engagement more salient. Caregivers also reported restricted and repetitive behaviors as a primary concern more frequently in school (vs mental health) settings, which contrasts with previous work (e.g. Azad & Mandell, 2016), but remains plausible. The structured demands of school environments, including following routines and engaging in peer interactions, may trigger or highlight these behaviors. While restricted and repetitive behaviors are likely adaptive for autistic children, they can also be seen by teachers as impeding educational and social participation, making them a greater concern for caregivers in school settings. Conversely, restricted and repetitive behaviors are less prioritized in mental health settings, where the focus is more often on helping caregivers manage externalizing behaviors, attentional difficulties, and internalizing symptoms as they present in the home. The high prevalence of social communication concerns named by caregivers in school settings highlights the need to implement interventions that specifically address social communication in classroom settings, corroborating previously identified training needs for teachers (Schetter & England, 2015).
This study had a number of limitations. First, this study exclusively relied on caregiver-reported concerns for autistic children, potentially overrepresenting observable (e.g. externalizing) behaviors and underrepresenting internalizing symptoms that may be more accurately reported by the children themselves. Future research should investigate the self-reported concerns of autistic children. The limited clinical information about the children in this sample is another limitation. While in earlier studies from our group samples did significantly differ on IQ score by setting (Brookman-Frazee et al., 2019; Stahmer et al., 2023), we were unable to confirm nor control for these differences in our study. We also note that data were not collected on participants’ multisystem involvement; participants may have accessed services from more than one system, which was not accounted for in the current study analyses. Finally, we recognize the potential effects of selection bias in our sample; caregivers in the school sample, who enrolled in our study through a teacher receiving training a school-based intervention, may have been more likely to report school-related concerns given the study context. Similarly, caregivers in the mental health sample, who enrolled in the study as a dyad with a therapist receiving training in a mental health intervention, may have been more likely to report mental health−related primary concerns. As such, these findings may not generalize to all autistic children in these settings.
To summarize, these findings highlight the wide range of concerns—spanning mental health, autism, adaptive behavior, and self-regulation domains—named by caregivers of autistic children across two public service systems (school and mental health) as well as several demographic factors associated with these concerns. Study findings emphasize the need for the implementation of targeted mental health interventions in systems of care serving autistic populations, particularly prioritizing evidence-based interventions targeting externalizing behaviors for children receiving publicly-funded mental health services and social difficulties for children in school settings, respectively. It is also important to note that, controlling for child age and caregiver ethnicity covariates, several caregiver concerns did not differ between school and mental health settings (e.g. anxiety, attention problems, social communication/interaction-related problems). Indeed, providers in both school and mental health settings may be faced with overlapping presenting concerns and cross-system coordination of care may be beneficial. Future research will leverage data from this study to examine the effects of AIM HI and CPRT—two evidence-based interventions aimed at addressing behaviors in mental health settings and enhancing communication skills in school settings, respectively—on caregiver primary concerns.
Footnotes
Author contributions
Data availability
Data, code books, and syntax related to this study are available from the corresponding author, L.R.B., upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by the National Science Foundation Graduate Research Fellowship under Grant No. DGE-2038238. Research reported in this publication was also supported by grants R01MH111950 and R01MH111981 from the National Institute of Mental Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Science Foundation or National Institutes of Health.