
Abstract
Most autistic adolescents experience anxiety. Interoception, defined as one’s ability to detect and interpret bodily signals, might contribute to this. The aim of this exploratory, qualitative study was to gain a better understanding of interoceptive experiences in autistic adolescents and how this relates to anxiety. Semi-structured 1:1 interviews were conducted with 13 UK-based, autistic adolescents, aged 14–17 years, who reported experiencing significant, day-to-day anxiety. Interviews were analysed using a reflexive thematic analysis approach. Interoception appeared relevant to experiences of anxiety in most participants, although this influence was exerted through various routes. While hypoawareness of interoceptive signals led to a reduced ability to detect and regulate anxiety, hyperawareness became overwhelming and anxiety-inducing. Overly negative evaluations of interoceptive signals, including catastrophising about the signals indicating danger, also triggered anxiety. Relationships between interoception and anxiety appeared bidirectional, with anxiety also affecting interoceptive awareness and evaluation. Interoceptive experiences were variable both across and within participants, with factors such as arousal and cognitive overload affecting experiences. Future research should focus on assessing the feasibility of interventions based on the mechanisms identified here.
Lay abstract
Anxiety is common in autistic adolescents. The detection and interpretation of signals coming from inside the body (e.g. heartbeat and hunger) is assumed to be related to both anxiety and autism. We interviewed 13 autistic 14- to 17-year-olds who reported experiencing significant anxiety, to explore the role that bodily signals played in their experiences of anxiety. Across most participants, there did appear to be a relationship, although the exact way it was related varied. When participants were very aware of bodily signals, they could become overwhelming, but if they were not aware at all, then it was difficult for them to notice themselves getting anxious until it was too late. If participants interpreted these signals negatively, for example, assuming the signals meant something was wrong with their body, they were also more likely to feel anxious. Whether participants were aware or negatively evaluated these signals was very variable and appeared to be context-dependent.
Introduction
Compared with their neurotypical counterparts, autistic adolescents face a higher risk of developing anxiety disorders, with research estimating that autistic children and adolescents are twice as likely as neurotypicals to have an anxiety disorder (Costello et al., 2005), and an estimated 40% of autistic youths experiencing one or more anxiety disorder (van Steensel et al., 2011). Autistic adolescents also have higher levels of trait anxiety (White et al., 2009). In general, adolescence is a pivotal time for the development of anxiety disorders and symptoms, potentially due to the increasingly complex social systems and physiological changes occurring (Pfeifer & Allen, 2021). Qualitative research has highlighted that in autistic populations specifically, these conventional triggers for anxiety exist alongside, and interact with, autism-specific anxiety triggers such as sensory hypersensitivity (Acker et al., 2018) and masking (Chapman et al., 2022). Concerningly, autistic youth appear to benefit less from conventional interventions for anxiety disorders than neurotypicals (van Steensel & Bögels, 2015), highlighting a need for a better understanding of the phenomenology of anxiety in autistic young people.
There are numerous routes by which autism may result in increased levels of anxiety (Rodgers & Ofield, 2018; Wood & Gadow, 2010), including interoception (Trevisan, Mehling, & McPartland, 2021). Interoception refers to the detection and interpretation of one’s internal, bodily signals, including signals within cardiac, respiratory and gastric domains (Craig, 2002). It encompasses various sub-dimensions including the accuracy of interoceptive perception (interoceptive accuracy), the amount of attention paid to interoceptive signals (interoceptive attention) and how positively or negatively interoceptive signals are evaluated and what they are interpreted to signal (interoceptive evaluation; Murphy et al., 2019; Suksasilp & Garfinkel, 2022).
Interoception has been theorised to be different in autistic compared with non-autistic individuals (Hatfield et al., 2019; Quattrocki & Friston, 2014), although research has produced mixed results, and some dimensions of interoception, such as evaluation, have not been researched at all (Williams et al., 2022). In terms of studies on autistic adolescents specifically, findings have been mixed, and there is a lack of consistency in the age groups defined, with many studies combining children and adolescents into one sample. When comparing autistic to neurotypical young people, poorer (Mash et al., 2017; Nicholson et al., 2019; Palser et al., 2018), greater (Schauder et al., 2015) and equal (Pickard et al., 2020) cardiac interoceptive accuracy and greater (Pickard et al., 2020) and equal (Butera et al., 2023; Palser et al., 2018) general interoceptive attention have been observed.
Interoception (especially within the cardiac domain) has also been suggested to be causal in anxiety, thus acting as a potential bridge between autism and anxiety. However, there is little consensus as to the exact mechanism by which interoception affects anxiety, for example, whether greater interoceptive accuracy results in an increased propensity to panic (Ehlers & Breuer, 1992), or whether anxiety is caused by a discrepancy between perceived versus actual interoceptive accuracy (Garfinkel et al., 2016). Mirroring this theoretical discrepancy, a recent meta-analysis found no overall relationship between anxiety and cardiac interoceptive accuracy in predominantly neurotypical samples with some autistic participants, but significant heterogeneity in findings (Adams et al., 2022). Within autistic populations specifically, findings of an association between interoception and anxiety are more consistent but limited in number. In autistic adults, the discrepancy between reduced interoceptive accuracy and higher interoceptive attention was predictive of state and trait anxiety (Garfinkel et al., 2016), and an intervention to improve cardiac interoceptive accuracy reduced anxiety (Quadt et al., 2021). In the single study involving adolescents, Palser and colleagues replicated Garfinkel’s findings in their sample of autistic 6- to 18-year-olds and found that interoceptive attention alone additionally predicted anxiety.
Given the multi-dimensionality of interoception and the heterogeneity of autism, a qualitative approach may be especially beneficial in understanding the relationships between autism, anxiety and interoception. It allows for a rich, bottom-up approach to theory generation, accounting for the fact that interoception may influence anxiety by multiple different, potentially bidirectional, routes.
Qualitative research focusing on experiences of anxiety in autistic individuals has not specifically focused on the role of interoception, although findings suggest it may be relevant. In a thematic analysis utilising focus group interviews with autistic adults, a ‘somatic’ theme emerged, where numerous participants reported feeling bodily symptoms of anxiety which triggered anxious thoughts (Halim et al., 2018), which was echoed in Spain and colleague’s (2020) interviews with six autistic men, and Trembath and colleagues’ (2012) study of 11 verbal autistic young adults and 10 caregivers and professionals. In adolescents specifically, Jackson and colleagues (2022) also found that somatic markers of anxiety (such as a rapid heartbeat and shortness of breath) were critical in the experiences of anxiety of six autistic girls.
Of the qualitative studies that specifically focus on interoception in autism, all participants were adults. One study used a content analysis approach on forum discussions of autistic adults describing interoceptive experiences (Trevisan, Parker, & McPartland, 2021). They reported a general hyposensitivity to internal signals such as thirst and hunger, but incidences of hyper-attention to anxiety-related bodily sensations, like one’s breathing rate or heartbeat. Another content analysis of autobiographical texts of 10 autistic individuals found that, while there were instances of both interoceptive hyper and hyposensitivity discussed, only persistent hyposensitivity was described (Elwin et al., 2012). The methodology of this study precluded the researchers from asking specific questions about the participants’ experiences, and the reliance on autobiographies resulted in the sample having strong verbal proficiency, limiting representativeness. Moreover, the use of content analysis in both studies means data is analysed in a more quantitative manner than with other qualitative methods, leaving scope for a more purely qualitative exploration of the topic.
To the best of our knowledge, ours is the first study to explore the role of interoception in autistic adolescents’ experiences of anxiety. The unique developmental characteristics of adolescence mean it is important to look at this age group specifically. Our aim was to both characterise interoceptive experiences within our sample and explore how this related to anxiety. This study addresses a pressing need for autism research that is constructed around the lived experiences of autistic individuals. Moreover, the use of qualitative methodology allows for a clearer understanding of the complexities of associations between autism, anxiety and interoception that quantitative research has not been able to capture.
Methods
Study design
We employed one-on-one interviews, analysed with a reflexive thematic approach (TA), to allow a view into the lived experiences of those interviewed, while acknowledging the role that the researcher plays in interpreting this. Please see the Supplementary Materials for our positioning statements. We pre-registered the study (https://osf.io/jgm98), which was approved by the Medical Sciences Division at the University of Oxford (reference: R85616/RE001) and carried out in accordance with the Declaration of Helsinki.
Participants and sampling
The eligibility criteria for this study were that all participants were between the ages of 14 and 17 years, spoke fluent English, had a diagnosis of autism and self-reported experiencing significant anxiety that impacted their day-to-day life. Prior to conducting the interviews, we estimated our sample size would be between 15 and 20 participants, basing this on previous interview studies with autistic adolescents (e.g. Acker et al., 2018), and the ‘information power’ approach (Malterud et al., 2016, see Supplementary Materials Table 1 for details).
Plans for the sample size were updated as we collected and analysed our data. We continued to conduct interviews until all authors felt ‘theoretical sufficiency’ (Low, 2019) had been reached. This resulted in a final sample of 13 participants.
Participants’ background characteristics are reported in Table 1.
Demographic Information.
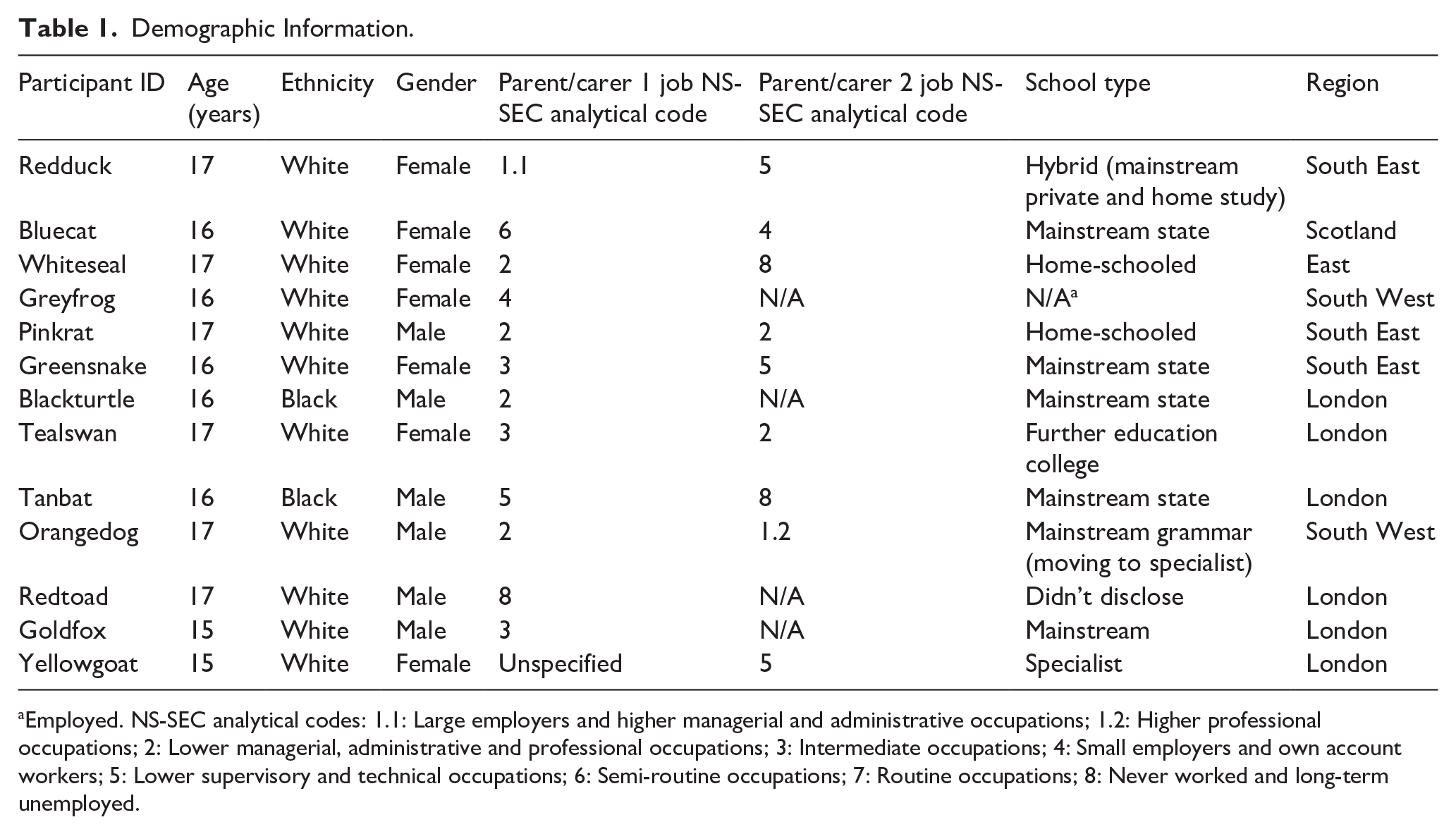
Employed. NS-SEC analytical codes: 1.1: Large employers and higher managerial and administrative occupations; 1.2: Higher professional occupations; 2: Lower managerial, administrative and professional occupations; 3: Intermediate occupations; 4: Small employers and own account workers; 5: Lower supervisory and technical occupations; 6: Semi-routine occupations; 7: Routine occupations; 8: Never worked and long-term unemployed.
Initially, any participant who indicated interest and fulfilled the eligibility criteria was interviewed. After eight interviews, we began to purposively sample using the demographic information from the screening questionnaires, selecting future participants on the grounds of ethnicity, gender, county and parental occupation, allowing for a diverse sample. Of particular importance was recruiting those from groups under-represented in autism research, such as non-male, non-white and participants from lower socioeconomic backgrounds. Our participants were selected from 19 who completed the screening questionnaire. Participants came from eight different counties within the United Kingdom.
Public and patient involvement
Initial public and patient involvement (PPI) work with two autistic adolescents and two parents of autistic adolescents (none of whom participated in the study) was conducted to inform the research design. See Supplementary Materials for demographics.
Feedback was given on the initial research design, our topic guide, how to make the interview setting more accessible and how to ensure a diverse sample was recruited. See the Supplementary Materials for examples of the changes made. The two autistic adolescents were included as co-authors and reviewed the analyses after themes were generated.
Topic guide
The topic guide (see Supplementary Materials) was developed by A.K., who amended it after discussion with co-authors and the PPI group. Broadly, the questions covered participants’ experiences of anxiety, their ability to detect emotions, how aware participants were of interoceptive signals, how signals were interpreted and how this related to their experiences of anxiety.
Procedure
Participants were recruited through adverts on social media. An information sheet was provided for parents, and an information PowerPoint for the adolescents, following which consent was gained. Participants then completed a short screening questionnaire (see Supplementary Materials), involving questions for both the adolescent and parent/guardian. This included demographic information to allow for purposive sampling and questions regarding the adolescent’s autism diagnosis (to ensure eligibility). Potential participants who completed the screening questionnaire were entered into a prize draw to win one of two £25 Amazon vouchers, regardless of whether they were selected for the interview.
The selected participants were informed by email and were able to choose whether they wanted to have their interview conducted remotely over Microsoft Teams, or in person. Four participants chose to do the interviews in person, and the rest chose to do it remotely. Eight participants chose to have an introductory call ahead of the meeting, to allow for rapport building, minimise anxiety and determine accessibility requirements (Robertson et al., 2018).
Participants were given the option to have a supportive individual with them during the interview, but none chose to do this. Participants were also encouraged to express their views through writing or drawing (via Miro if online) if they felt more comfortable but no participants did. Stim/sensory toys and tissues were placed on the table and participants were told they could use them at any time. Participants were told they could take breaks at any time, come back to questions later or avoid questions completely, and that they could do anything that made them comfortable, including avoiding eye contact.
Interviews were completed between May to October 2023. Interviews took 45 min to an hour and a half, and participants who were interviewed were compensated £20 in Amazon vouchers. All interviews were voice recorded.
The topic guide was used as a flexible basis for the interview, but the question wording and order were contextual. At the end, participants were asked if there was anything else they would like to add. If something was brought up and suggested to be important in one interview, the interviewer adapted the interview schedule for the next interviews, ensuring that the topics of research were guided by those with lived experiences of autism.
Transcription was conducted immediately following the interview and in line with the guidance given by Braun and Clarke (2013). Transcription was performed manually, as part of data familiarisation. Participants were sent the transcripts as part of the validation process. They were given 2 weeks to make any minor changes. Two participants added further information that was included in the final transcripts and indicated by italicised font. The full, anonymised transcripts can be accessed on OSF (https://osf.io/jgm98) to facilitate open science.
Analysis
A bottom-up, inductive approach was taken given that there is no singular theory guiding research. Analysis was conducted using the following six steps as guidance (adapted from Braun & Clarke, 2013): data familiarisation, line-by-line analysis and preliminary code generation, grouping of codes into initial themes, theme assessment and construction of theme map, defining and naming themes and writing and finalising analysis. Analysis was performed in a flexible and iterative manner during data collection, moving back and forth between the different stages. All coding was done in NVivo 14 (Lumivero, 2023).
Assuring validity
A.K. kept a research journal throughout the process, facilitating reflection on her role in the construction of themes and conclusions. This included field notes and analytical insights.
Most of the analysis and development of the thematic structure was conducted by A.K., in collaboration with W.P. Participants were active collaborators in the research process. Between stages 3 and 4 of the analysis, the codes and themes identified were sent to participants and the autistic co-authors/PPI contributors, and they could provide further feedback. Two participants gave suggested amendments, which were integrated into the themes.
Community engagement
Authors S.J. and B.M., who participated in PPI, were involved in the analysis and gave feedback on the write-up, are both autistic. The research design was informed by both their feedback, as well as the feedback of two parents of autistic adolescents, during PPI.
Results
Quotations are verbatim, with ellipses used to indicate some speech has been cut for brevity.
We constructed three main themes: interoceptive awareness, interoceptive evaluation and situational interoception. There were a further 10 subthemes, as illustrated in Figure 1.
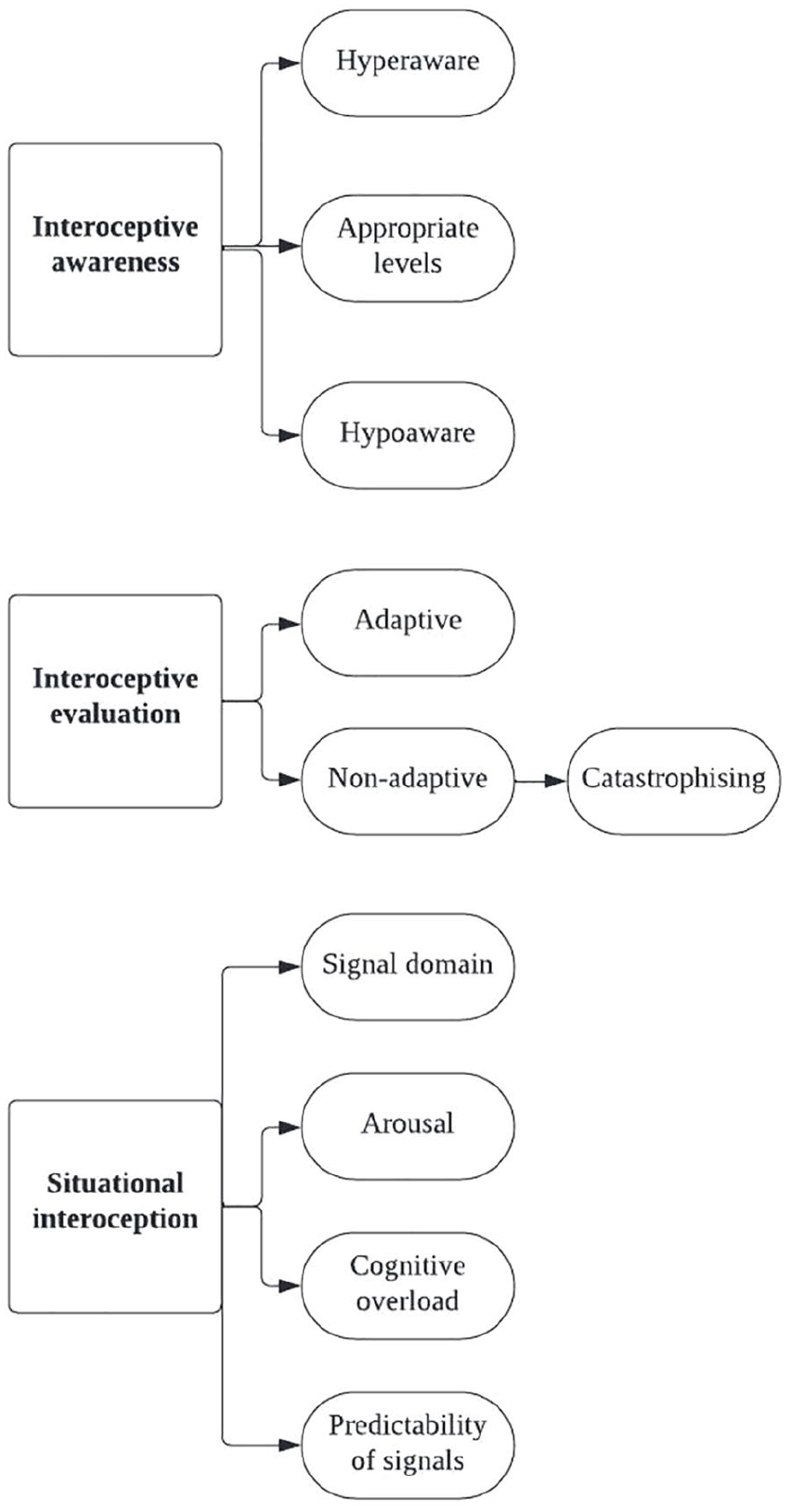
Themes and subthemes.
Theme 1: interoceptive awareness
Theme 1 reflects the degree to which participants reported being aware of interoceptive signals, which appeared to influence anxiety. Interoceptive awareness encompassed whether they felt they could accurately detect internal signals (interoceptive accuracy) and the proportion of time they felt aware of these signals (interoceptive attention), which participants did not distinguish between. Interoceptive awareness also encompassed the degree to which interoceptive signals took priority over other signals for attentional resources. It varied significantly across participants, spanning from constant hyperawareness, to ‘typical’ awareness, to constant hypoawareness. It also varied within participants, with some participants experiencing both at different times.
Theme 1, sub-theme 1: hyperaware
I am almost constantly aware of my heartrate. (Tealswan)
Participants who experienced hyperawareness of interoceptive signals described not being able to tune out from them. These participants were commonly hypersensitive to a range of sensory signals (e.g. bright lights and food smells), not just interoceptive signals. For them, awareness of interoceptive signals was frequent, largely involuntary and problematic. Interoceptive signals were too frequently the object of consciousness, resulting in other information being drowned out.
I could be having a really nice quiet walk which to a lot of people would be super peaceful but because I’m hyperaware of how my heart is beating or how fast I’m breathing or you know every tiny bit of movement I get incredibly over-stimulated. (Tealswan)
These participants described how interoceptive signals could become overwhelming and they felt unable to cope and anxious. This was especially challenging if there were other stressors present. One participant describes it as:
just another thing to keep track of when things are getting too much. (Pinkrat)
Whereas another described:
it feels like you are going to pop you’re going to explode. (Orangedog, referring to the rare occasions he experienced interoceptive hyperawareness)
The overwhelming nature of some of these signals also resulted in both shutdowns and meltdowns in several participants.
Like normally the path will be I’ll get anxious about something and then um (.) . . . I’ll go to break and it will be really noisy and that leads to me getting overwhelmed and then I’ll go to another lesson and that’s noisy and that escalates and it’s just like too much and then I become more aware of everything like my heart my breathing and then I’ll like shut down. (Greensnake)
Shutdowns and meltdowns are behavioural responses characterised by a loss of control. While a shutdown results in internal behaviours, like withdrawal and halted communication, a meltdown results in a more external response, including aggression and screaming. Interoception was identified as both a cause and a consequence of shutdowns and meltdowns, allowing for it to act as a maintenance factor in a vicious cycle. The consequences are discussed in more detail in Theme 3.
Theme 1, sub-theme 2: appropriate levels
A smaller group of participants had levels of interoceptive awareness that were deemed appropriate, as their awareness allowed them to enact behaviours to maintain allostasis, while not inducing anxiety. These participants were able to tune in and consciously access information about internal signals if they focused on it, or if the signal was especially strong, but were not overly focused in a way that negatively impacted their day-to-day life.
I wouldn’t have noticed that if we haven’t been talking about it obviously because now I’m focusing [I can]. (Yellowgoat, referring to her heart rate)
Theme 1, sub-theme 3: hypoaware
When participants experienced hypoawareness of interoceptive signals, they were unable to detect internal signals, even if they tried, meaning that they struggled to meet their body’s homeostatic needs. Frequently discussed examples were not knowing when to eat until they felt faint, or not being aware of the need to use the bathroom until it was almost too late.
I just cannot tell when I’m thirsty or not I have no idea. (Goldfox) I can go the whole day without eating anything at all and I’m feeling fine. (Tanbat)
This difficulty recognising one’s needs led to a general sense of physical discomfort, as well as causing participants to worry that it affected their behaviour in a way that would lead to negative appraisal from others (e.g. needing to run to use the bathroom at the last moment). In the case of interoceptive signals that indicate anxiety, such as heart rate, it led to participants not being able to recognise low-level anxiety and remove themselves from such situations, thus allowing anxiety to increase.
I sometimes only realise I’m getting overwhelmed when it gets quite extreme . . . that can lead to . . . a bigger meltdown than I would have had if I’d spotted it earlier. (Greensnake)
Theme 2: interoceptive evaluation
The second theme of interoceptive evaluation, which refers to the interpretation of the interoceptive signals that participants were aware of, also varied across participants and appeared to exist along a spectrum.
Theme 2, sub-theme 1: adaptive
Some participants could be described as having ‘adaptive’ interoceptive evaluation, meaning that certain signals were suitably aversive to allow them to fulfil their role as motivational states (for example, feeling hungry would motivate them to eat), but the degree to which they found these signals aversive did not negatively impact their day-to-day life or cause undue anxiety. These participants could recognise the diagnostic values of the signals.
Uh neutral or positive . . . they don’t really uh fall on the negative side. (Blackturtle)
One participant recognised that interoceptive signals can be evaluated as a positive rather than a negative in certain situations and that this can directly reduce anxiety. This suggests that sometimes these signals can be reassuring or a distraction.
sometimes these signals will . . . be the cause of anxiety or even help stimulate it. But there’s other times where it will in fact be the thing that stops the anxiety or calms it. (Redtoad)
Theme 2, sub-theme 2: non-adaptive
Although theoretically, non-adaptive evaluations could encompass both those that were overly negative or positive, the latter was not identified from these interviews. Many participants described how they had overly negative evaluations of interoceptive signals, which impacted their everyday life and went beyond what could be seen as adaptive or proportional.
I absolutely detest feeling full up. Hate it hate it hate it. (Orangedog) I can’t see a positive of feeling every time my heart beats to me all that’s doing is making me more stressed out and over-stimulated. (Tealswan)
Some participants directly linked this to their anxiety.
I’ll find that the increase in heartbeat . . . definitely creates a feedback loop of anxiety. (Redtoad)
Theme 2, sub-theme 3: catastrophising
One subset of an overly negative, non-adaptive interoceptive evaluation was catastrophising, which several participants described. This is where one noticed a change in bodily signals that could indicate anxiety (e.g. an increase in heart rate) and assumed this was a sign that something was wrong. This would further cause them to panic, resulting in a positive feedback loop which further increased their heart rate and thus anxiety. For some, the interoceptive signals were interpreted as a sign of ill health, or something being wrong with their body.
The physical response is exceptionally scary . . . It feels like you’re dying. (Orangedog) You just find your heart like beating so fast you’re (.) it makes me sometimes afraid like am I am I going to have like a heart attack. (Tanbat)
One participant highlighted how a focus on these internal signals made her aware of how little control she had over her body. Lack of control was highlighted earlier in the interview as a key trigger for her anxiety.
When I get overwhelmed by the internal processes I get overwhelmed by the sense I have no control. (Redduck)
A need for control is something often linked to the autistic experience (Kinnaird et al., 2019). It is interesting to note here how it interacts with interoceptive experience in a complex way, resulting in an interpretation of interoceptive signals that may be unique to autism.
Theme 3: situational interoception
Theme 3 illustrates how both interoceptive awareness and evaluation were variable within as well as across participants.
It depends on the situation. (Blackturtle, referring to feeling his heart beating)
Theme 3, sub-theme 1: signal domain
Signal domain refers to the type of interoceptive signal, for example whether it is cardiac, respiratory or gastric. In the case of interoceptive awareness (Theme 1), some participants were hyperaware of certain signals, but hypoaware of others. In particular, the cardiac signal consistently appeared to be the most difficult to detect in day-to-day life, with few participants able to feel their heartbeat at rest.
Different interoceptive signals also seemed differentially aversive. While signals typically associated with the symptoms of anxiety, such as elevated heart rate and faster breathing, were more commonly cited as anxiety-inducing, interoceptive signals relating to more general bodily needs (such as thirst or needing the bathroom) were more commonly seen as neutral. Interestingly, signals relating to appetite existed between these, with a minority of participants finding these intensely aversive, but the majority finding them neutral.
Theme 3, sub-theme 2: arousal
Almost unanimously, participants reported being more aware of their heartbeat when it was raised due to anxiety or exercise.
After exercising is probably when it feels the most or when you know I’m stressed for whatever reason. (Pinkrat) When I do feel really anxious or have really high emotions I can feel it really really strongly. (Greyfrog)
In some cases, this heightened awareness with anxiety was general to all interoceptive signals, not just heartbeat.
In the potent situations I can feel absolutely everything in my body all at once. (Orangedog)
This highlights a bidirectional link between anxiety and interoception, thus allowing for the positive feedback loops mentioned in the previous section.
Some expressed the idea that it was the change in state that triggered their awareness, rather than simply higher than normal levels.
I can kind of feel when it changes. (Goldfox, referring to heart rate)
Even within participants, there were differences in how interoceptive awareness manifested when anxious. One participant (Tealswan) linked this to either shutdowns or meltdowns, both of which she experienced, although she was unsure about whether there were different triggers to these two scenarios.
I’m either super super present where like everything is a million degrees . . . or the like input that I’m being given is just nothing at all. Or like I’m completely dissociated I cannot really feel anything. (Tealswan)
For some participants, shutdowns led to feeling completely detached from interoceptive signals, as though they could feel nothing at all.
I feel completely. . . not in my body. (Whiteseal)
By contrast, for those who experienced meltdowns, interoceptive signals (in much the same manner as other sensory signals) became increasingly more intense and unbearable.
I feel too much going on inside my body. (Greensnake, when asked how meltdowns feel)
This further underscores the immense complexity of experiences of interoception in relation to anxiety.
Arousal was also likely to influence one’s interoceptive evaluation (Theme 2). If participants were already feeling overwhelmed, they were more likely to interpret interoceptive signals in a negative way.
It depends on what environment I’m in because there’s not really anything else that’s overwhelming me at the moment I don’t mind but if I was in somewhere where there was someone talking to me someone else having a conversation next to me um some background noise and then I started feeling my heartbeat as well I think that’s too many things for me to focus and process . . . that would cause me more anxiety. (Greensnake)
One participant avoided exercise because any feeling of her heart increasing at all made her panic, even if she knew there was a non-threatening explanation for it. This highlights an indiscriminate negative evaluation of interoceptive signals, regardless of the situation.
Like I don’t really like running and stuff because like when I run . . . my heart beats fast and that like reminds me of being anxious. (Bluecat)
Theme 3, sub-theme 3: cognitive overload
Some participants found it harder to notice interoceptive sensations (Theme 1) when focusing on numerous other things already.
I think it’s also like based on how overwhelmed I feel sometimes cause like if I feel really overwhelmed then I just won’t feel like eating. (Bluecat, when talking about her appetite)
Masking (defined as the automatic or voluntary suppression of natural autistic responses; Pearson & Rose, 2021) was another factor that affected some participants’ ability to detect internal signals. They felt more detached from themselves and less attuned to internal sensations when masking, as their attention was directed outwards rather than inwards. Relatedly, focusing on observing and imitating the behaviour of others was cognitively demanding and left little room to focus on interoceptive signals.
My ability to read myself lessens quite a bit because I’m so focused on other people and their actions and their experiences and I think that’s why I ended up having so many um shutdowns in school . . . I wasn’t reading the signs that I was getting overwhelmed. (Greensnake)
One participant describes how they only began to experience hunger properly when they were home-schooled and could begin to focus on themselves rather than masking to fit into their external environment.
When I was masking at school like I wouldn’t really feel hungry or thirsty and stuff and like I often wouldn’t even go to . . . the toilet until I literally got home got through the front door and then like kind of unmasked more. (Whiteseal) I noticed since I started homeschooling . . . I’m doing my own thing that then I seem to kind of realise oh I need to go to the toilet I need to drink because I’m thirsty. (Whiteseal)
For other participants who masked, masking resulted in a hyperawareness of certain, anxiety-related interoceptive signals due to the stress of vigilantly monitoring their behaviour.
heartbeat and breathing . . . might be heightened . . . in times where I’m like in social situations or masking because (.) I would be (.) like (.) using my body would kind of be using that as an indicator. (Redtoad)
As well as masking, some participants experienced a kind of cognitive overload that came with extreme emotions that made it difficult to focus on bodily signals.
Trying to listen to your body sometimes does become very difficult if you are feeling very strong emotions. (Greyfrog)
Theme 3, sub-theme 4: predictability of signals
For one participant, the ability to detect signals (Theme 1) and how anxiety inducing they were (Theme 2) depended on their predictability.
Because hunger and thirst or needing the toilet do not have a set order or schedule I often misread them . . . But because heart rate and breathing are consistently there when I do tune into them it is not confusing for me to interpret. (Redduck)
Discussion
We found that in our sample of 13 autistic adolescents who experience significant anxiety, interoception played a role in the majority’s experiences of anxiety, although the route by which interoception affected, or was affected by, anxiety varied both within and between participants. One route by which interoception resulted in anxiety was when participants felt hypoaware of certain signals, meaning that they missed signs that they were becoming anxious and therefore missed opportunities to engage in positive emotion regulation strategies at lower levels of distress. Hypoawareness would also result in participants not attending to their bodily needs sufficiently, which could result in general discomfort and fatigue that might further exacerbate anxiety. Another route was by interoceptive hyperawareness, which led to interoceptive signals becoming overwhelming. When participants were aware of signals, there was also the possibility for overly negative interpretations of these signals to result in anxiety, especially when participants catastrophised about these signals and perceived them as a sign they were in danger. A key theme across these routes was the variability of interoceptive experiences, both within and between participants. Indeed, the context one was in (including factors such as cognitive overload, masking and arousal) and the specific signals in question played a huge role in how one experienced interoceptive signals and thus the potential for it to cause anxiety.
In terms of how our findings relate to the extant literature, our overall finding of an association between anxiety and interoception echoes the suggestion made by Spain and colleagues (2020) when looking specifically at social anxiety in autistic adults. However, it is important to note that this association was not endorsed by all of our participants, with a minority expressing that interoception played no role in their experiences of anxiety.
Our finding that hyperawareness can cause anxiety is consistent with models proposed within the context of more general sensory sensitivity in autism (Green & Ben-Sasson, 2010; Hazen et al., 2014), as illustrated in Acker and colleagues’ (2018) interpretative phenomenological analysis of interviews with 13 male autistic adolescents. Our findings are consistent with evidence that sensory sensitivities for both internal and external information can occur in a similar manner in autism, leading to similar relationships with anxiety.
Moreover, the importance of overly negative interoceptive evaluation in triggering anxiety identified here aligns with initial quantitative findings in neurotypical adults (Paulus, 2013; Taylor et al., 1991), as well as qualitative reports from autistic adults (Halim et al., 2018; Trembath et al., 2012) and autistic adolescent girls (Jackson et al., 2022). Trevisan, Parker and McPartland (2019) directly explored interoception in their content analysis of forum posts by autistic adults. In the current study, they found that some participants discussed being constantly worried due to an inability to distinguish benign bodily sensations from serious health issues.
The variability and situational nature of interoception are consistent with Trevisan, Parker and McPartland’ (2021) finding of both hypo- and hypersensitivity specifically to interoceptive signals in autistic adults. Although hyposensitivity was more common, hypersensitivity was mentioned by participants in the context of anxiety-related interoceptive signals such as heart rate and breathing. While we also found that our sample of autistic adolescents responded differently to anxiety and non-anxiety-related interoceptive signals, the way this linked to either hypo- or hypersensitivity was not as clear as in Trevisan’s study. This could be due to differences in the age groups involved in the studies.
The finding that masking can affect interoception is consistent with previous qualitative work which suggests that sensory suppression is a key part of masking in autistic adults (Miller et al., 2021). This pathway from masking to either hypo or hyperawareness and therefore anxiety may be one of many potential reasons that masking is associated with poorer mental health (Cook et al., 2021).
Our findings could be understood with reference to monotropism (Murray et al., 2005). Monotropism describes a claimed autistic tendency towards intense and targeted attention ( ‘hyperfocus’). Such hyperfocus may explain hyperawareness of interoceptive information in instances where interoceptive signals are the focus of attention, and hypoawareness when they are not.
The findings of this study have a variety of wider applications. First, it highlights the importance of further research into interoceptive evaluation, which has been under-researched and typically measured using non-specific and unvalidated questionnaires. Given the importance of interoceptive evaluation in our study, better measures should be developed that would allow larger-scale quantitative investigations to be triangulated against qualitative findings. There is also potential for interventions for interoceptive evaluation, perhaps by using cognitive restructuring to encourage patients to focus on interpreting bodily signals neutrally and teaching about alternative, non-anxiety-related explanations for changes in certain signals such as heart rate and breathing. This is currently a key part of Cognitive Therapy, which has been found to be efficacious in neurotypical adolescents with social anxiety (Leigh & Clark, 2023), but has not yet been evaluated within autistic populations.
Our findings also suggest that existing technologies could be used by autistic adolescents with anxiety to help manage their symptoms. Smartwatches that detect bodily signals may be useful for those experiencing interoceptive hypoawareness who find recognising anxiety difficult. However, this could be anxiogenic for those who are hyperaware of interoceptive signals and liable to overly negative evaluation. A co-design approach should be a priority for researchers looking to develop interoception-based interventions, given the nuances of the relationship between anxiety and interoception.
Our study is the first study to focus on how interoceptive experiences in autistic adolescents relate to anxiety. Autistic young people were included in the design of the study and analysis, and our qualitative data allowed for a rich exploration into the lived experiences of our participants. Interpretation was also influenced by both A.K.’s lived experiences of an anxiety disorder, as well as W.P.’s experience as a clinical psychologist, both of which allowed for an understanding and rapport to be built in interviews that facilitated a more open discussion with participants. Despite these strengths, there are some limitations to address. Despite efforts to sample purposively, some groups (those of Asian heritage, non-binary participants and those with severe intellectual disability) remained unrepresented due to time constraints. However, we did manage to include several often under-represented groups. Over half of our participants were autistic girls, we had two Black participants and participants of a range of socioeconomic statuses (parental occupation) and regions of the United Kingdom. Several participants were either home-schooled or in specialist schooling, and one participant experienced selective mutism.
The results of this qualitative study present a more complex picture than that typically explored in quantitative research of interoception, which may explain the inconsistency in quantitative findings of studies exploring the associations between interoception and anxiety and autism (Adams et al., 2022; Williams et al., 2022). Given that autistic participants may be hyper-, hypo-, or typically aware of interoceptive signals, and that this can vary within individuals according to contextual factors, the likelihood of either null or conflicting findings due to different experimental settings and sampling variance is high. Despite the variation in the possible routes, we found overall that interoception related to experiences of anxiety in many of our participants, highlighting a potential route for intervention. It would be beneficial to triangulate these findings with future large-scale questionnaire studies, allowing us to better ascertain the generalisability of these results.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251314595 – Supplemental material for Experiences of interoception and anxiety in autistic adolescents: A reflexive thematic analysis
Supplemental material, sj-docx-1-aut-10.1177_13623613251314595 for Experiences of interoception and anxiety in autistic adolescents: A reflexive thematic analysis by Adams Kiera, Smith Jonahs, Brown Mary, Bird Geoffrey and Waite Polly in Autism
Footnotes
Author contributions
Data availability statement
Transcripts and coding books are available on the Oxford University Research Archive.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KLA is funded by the University of Oxford Medical Sciences Graduate School Studentship (Clarendon Fund in partnership with the University College Award and the Experimental Psychology Studentship, SFF2122_CB2_MSD_1303888).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.