
Abstract
Despite very high rates of suicidal thoughts and behaviors (STB) in autistic adults, the key psychosocial drivers of this phenomenon remain unknown. To investigate, we examined how lifetime stressor exposure and severity, which have been found to predict STB in non-autistic populations, related to STB in a multinational dataset of 226 autistic adults from the United Kingdom and Australia (67% female; Mage = 41.8, SD = 13.6, range = 19–73 years old). Results revealed that autistic men and women differ with respect to the count, severity, and type of stressors they experienced over the life course. Whereas autistic men were exposed to more numerous legal/crime-related stressors, autistic women experienced more stressors related to social relationships and chronic humiliation and typically experienced stressors as more severe. In addition, whereas chronic interpersonal loss was related to STB for men, acute stressors involving physical danger and lower exposure to chronic entrapment were related to STB in autistic women. These findings indicate that certain lifetime stressors may be differentially experienced, and relevant to STB, in autistic men versus women. They also suggest that screening for lifetime stressor exposure may help identify autistic individuals at greatest risk of suicide.
Lay abstract
When we encounter life events that we experience as stressful (“stressors”), it sets off a biological stress response that can impact mental health and contribute to suicidal thoughts and behaviors (STB). Although we know about specific stressors that are associated with STB in the general population, little is known about the kinds of stressors that increase the risk of STB in autistic people and whether these associations differ by gender. To examine this issue, we cataloged the life stressors that autistic men and women experienced over the entire life course and investigated how these stressors were related to STB. Data were derived from a multinational sample of 226 autistic adults from the United Kingdom and Australia who completed the Stress and Adversity Inventory for Adults. We found that autistic men and women differed in terms of both the lifetime stressors they experienced as well as their perceived severity. Whereas men experienced more legal/crime-related stressors, women experienced more stressors related to relationships with other people and more long-lasting stressors associated with humiliation. Autistic women often perceived life stressors as more severe than men, which is important given that it is the perceived severity of stressors that most strongly affects our health. We also found that different stressors may predict STB in autistic men versus women. Whereas loss of loved ones was most strongly associated with STB for men, for women, physically dangerous stressors were most relevant. In addition, women with fewer lifetime stressors involving entrapment had higher lifetime STB. These results suggest that lifetime stressor exposure may be important to assess to understand suicide risk in autistic people. Additional research is needed to confirm these associations and to examine possible mechanisms linking stress and STB.
Lifetime stress features prominently in neurobiological and psychological models of STB (Mann & Rizk, 2020; D. B. O’Connor et al., 2020; Stewart et al., 2019). Suicide is both a longitudinal correlate of childhood adversity (Sachs-Ericsson et al., 2016; Thompson et al., 2019) and an acute sequelae to adverse life events, which interact with distal adversity to elevate suicide risk (Liu & Miller, 2014; McFeeters et al., 2015). The impact of distal and proximal adverse events may be mediated by psychopathology (Howarth et al., 2020; Zhang et al., 2020): subjective perception and experience of life events (stressors) as “stressful” evokes a psychological and neurobiological response that, over time, degrades mental (and physical) health, particularly when stressors are chronic, interpersonal in nature, and/or occurring early in life (Johnson et al., 2020; McEwen, 2005; Shields et al., 2017; Slavich, 2020; Van Bodegom et al., 2017). However, many proximal stressors linked to suicide—such as bullying, sexual victimization, social exclusion, financial distress, and interpersonal loss (Fjeldsted et al., 2017; Liu & Miller, 2014; Massing-Schaffer et al., 2019; McFeeters et al., 2015; Paul, 2018; Stewart et al., 2019)—may also engender cognitive-affective states associated with suicide ideation, such as hopelessness, thwarted belongingness, perceived burdensomeness, and entrapment (Daniel et al., 2017; R. C. O’Connor & Kirtley, 2018; Van Orden et al., 2010). Some kinds of stressors, such as physical violence, conceptualized as physically painful and/or emotionally provocative events (Bender et al., 2011; Bond et al., 2021), are also hypothesized to erode fear of death and increase capability for suicide, as suggested by direct relations between violent (but not non-violent) abuse and suicide attempts (Sachs-Ericsson et al., 2017). As such, distal and proximal exposure to lifetime stressors, along with the individual’s particular psychological response to these events, are central in the development of STB and important predictors of STB risk.
One group at particularly high risk of STB is autistic people, in whom suicide ideation and attempts are alarmingly common beginning in childhood (Brown et al., 2024; Hedley et al., 2022; Huntjens et al., 2023; Newell et al., 2023; O’Halloran et al., 2022). Autistic adults have an up to seven-fold increased risk of premature death by suicide compared to their neurotypical peers (Hirvikoski et al., 2020; Santomauro et al., 2024), with the highest risk for persons without intellectual disability (Casten et al., 2023; Hirvikoski et al., 2016, 2020). To understand this finding, research has focused on risk factors that might be associated with the autistic phenotype, such as cognitive rigidity, insistence on sameness, and emotion processing and regulation difficulties (Conner et al., 2020; Hedley et al., 2021; Moseley, Shalev et al., 2024), as well as correlates of STB that might be more or less prevalent within autistic populations (Brown et al., 2024; Hedley & Uljarević, 2018). Additional risk of STB in autistic people has been related to co-occurring attention deficit/hyperactivity disorder (ADHD) and psychiatric illnesses (Hirvikoski et al., 2020; Moseley, Gregory et al., 2024; Pelton et al., 2023); non-suicidal self-injury (NSSI) (Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; Moseley et al., 2022a); employment problems (Cassidy, Bradley, Shaw, & Baron-Cohen, 2018); loneliness and lack of social support (Hedley, Uljarević, Foley et al., 2018; Hedley, Uljarevic, Wilmot, Richdale and Dissanayake, 2018; Hedley, Uljarević, Wilmot, et al., 2017); and camouflaging (Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; South et al., 2020).
STB risk has also been linked to risk factors from psychological theory, such as thwarted belongingness (Pelton et al., 2020), perceived burdensomeness (Moseley et al., 2022b; Pelton et al., 2020), and reduced fear of death (Moseley et al., 2022b). Thus far, the application of a lifetime stressor exposure framework has been underutilized for understanding STB in autistic people, despite its successful application in the general population (Brodsky, 2016; McFeeters et al., 2015; Sachs-Ericsson et al., 2016; Stewart et al., 2019) and in several clinical and minority groups (Delfel et al., 2023; Gillespie et al., 2022; Parra et al., 2023; Wiebenga et al., 2022).
In fact, life stressors likely play an important role in STB in autistic people, given that this population has a higher incidence of adverse childhood experiences (Hoover & Kaufman, 2018; Kerns et al., 2017) and greater likelihood of victimization, exploitation, abuse, and assault in adulthood (Griffiths et al., 2019; Weiss & Fardella, 2018), along with chronic difficulties with employment, finances, and housing (Harmuth et al., 2018; Hedley, Uljarević, Cameron, et al., 2017). Although these are instances where activation of the stress response would be clearly expected, recent theoretical work also conceptualizes camouflaging as a chronic stressor that can contribute to allostatic load and subsequent burnout and psychopathology (Mahony & O’Ryan, 2022).
In addition, the impact of acute and chronic life stressors may be exacerbated for autistic people by heightened perception of stressors as stressful (Bishop-Fitzpatrick et al., 2017), by difficulties regulating emotions and accessing adaptive coping skills (Beck et al., 2020; Muniandy et al., 2022), and by social exclusion (Jones et al., 2022), factors known to exacerbate impacts of life stress in non-autistic people (Clay et al., 2023; Massing-Schaffer et al., 2019; Moriarity et al., 2023). There are indeed associations between STB in autistic people and generic measures of trauma (Pelton et al., 2020) and painful and provocative events (Moseley, Gregory et al., 2024). There is also evidence linking adverse childhood experiences and bullying to psychopathology and suicide in autistic people (Chou et al., 2020; Holden et al., 2020; Warrier & Baron-Cohen, 2021). Yet, associations between specific life stressors, stressor types, and STB have been relatively unexplored in autistic people.
Lifetime stressor exposure might also be a useful explanatory framework for understanding individual differences in STB among the autistic population. In contrast to non-autistic populations, where suicide ideation is more prevalent in people assigned female at birth 1 and suicide deaths are more prevalent in those assigned male (Ilic & Ilic, 2022; Nock et al., 2008), population trends in autistic people suggest males and females are both at higher risk of experiencing suicidal ideation and dying by suicide (Kirby et al., 2024). However, although overall more autistic males than females die by suicide (Santomauro et al., 2024), autistic people assigned female at birth might be at greater risk of attempting suicide (Hirvikoski et al., 2020; Kolves et al., 2021; Santomauro et al., 2024), a finding at odds with non-autistic populations. Autistic females also have higher rates of self-injury that could be suicidal or non-suicidal (Lai et al., 2023; Martini et al., 2022), along with higher rates of psychopathology (Lai et al., 2023; Martini et al., 2022).
Through the lens of lifetime stress, it is notable that autistic people assigned female at birth, who may or may not identify as women, are more likely to be hospitalized, abused, and assaulted than autistic males (Gibbs et al., 2021; Schnabel & Bastow, 2023; Tint et al., 2023). They also tend to perceive stressors as more severe (McQuaid, Weiss, et al., 2022), as might be expected given greater emotion-regulation problems (Weiner et al., 2023). To some extent, some of these disadvantages mirror those seen in non-autistic populations, where female sex and gender are associated with greater risk of sexual victimization and harassment, abuse in intimate relationships, discrimination in the workplace and economic disadvantages, as well as greater burden of caregiving and household responsibilities (Helpman, 2023; World Health Organisation, 2021). Female sex is also associated with greater perceived severity of stressors, greater sensitivity to social stressors, and greater susceptibility to psychopathological consequences of the same (Bekhbat & Neigh, 2018; Helpman, 2023; Mengelkoch & Slavich, 2024; Rincón-Cortés et al., 2019; Slavich & Sacher, 2019). However, over and above biological and sociocultural effects associated with female sex and gender, autistic females identifying as women (i.e. those who are cisgender 2 ) may be additionally affected by poorer understanding and recognition of autism in individuals not assigned male at birth, and hence face additional barriers to healthcare and other forms of support (Gosling et al., 2023; Grove et al., 2023; Miller et al., 2022; Tint & Weiss, 2018). Differences in lifetime stressor exposure and stress perception may therefore help to explain the varied prevalence of psychopathology and STB in autistic males and females.
To explore this possibility, we took advantage of contemporary developments for high-precision mapping of relations between lifetime stressor exposure, stress perception, and STB. More specifically, we used the Stress and Adversity Inventory for Adults (STRAIN) (Slavich & Shields, 2018), which is an online stress assessment system that has been used to comprehensively assess the impact of a wide variety of life stressors on many different biopsychosocial and clinical outcomes (Clay et al., 2023; Ojha et al., 2022; Rolnik et al., 2019), including suicide (Stewart et al., 2019). Stewart et al. (2019), for example, found that stressors involving chronic interpersonal loss were strongly related to attempting suicide, and that stressors in general seemed to predict suicide ideation but only insofar as they predicted psychopathology, which is consistent with other findings of psychopathology as a key factor linking stressors and STB (Zhang et al., 2020).
We recently used the STRAIN to assess lifetime stressor exposure in autistic people (Moseley, Turner-Cobb, et al., 2021). In this context, we observed higher incidence of nearly every stressor type in addition to greater perceived stress, the latter which was related to current psychological distress in this sample. Certain stressor types appeared particularly impactful—namely, those involving interpersonal loss, entrapment, and role change/disruption—but STB was not explored as an outcome measure, and the relatively small sample size did not enable us to test for possible sex or gender differences.
Given the novelty of using the STRAIN in autistic populations and the present lack of research investigating associations between specific life stressors and suicide in autism, in this first-of-its-kind multinational study in Australia and the United Kingdom (U.K.), we leveraged two well-characterized STRAIN datasets to examine life stressors of greatest relevance for lifetime incidence of suicidal thoughts and behaviors (henceforth “lifetime STB”) in autistic individuals who identified as men and women. First, we examined gender differences in lifetime stressor exposure, stressor perception, psychological distress (indicative of psychopathology), and lifetime STB; next, we examined associations between lifetime stressor exposure, perception, and lifetime STB in men and women separately. Our hypothesis-driven approach focused on specific life stressor domains already linked to STB in autistic people, such as stressors relating to work and education (Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; Chou et al., 2020; Hedley and Uljarević, 2018; Holden et al., 2020) and stressors that have been related to major constructs from the field of suicidology, such as interpersonal loss (see the Method section; Stewart et al., 2019).
Based on the research summarized earlier, we hypothesized that autistic women would (a) have higher levels of psychological distress and, possibly, lifetime STB than autistic men; (b) report higher lifetime stressor counts (reflecting greater exposure to lifetime stressors) than autistic men, particularly for stressors involving victimization, help-seeking difficulties (e.g. treatment/health), and physical danger; and (c) perceive stressors as being more severe. We also hypothesized that, for both autistic women and men, (d) greater cumulative exposure to lifetime stressors relevant to STB in that group, as well as the perceived severity of the same, would be related to greater lifetime STB, even while controlling for current levels of psychological distress (Stewart et al., 2019; Zhang et al., 2020).
Method
Participants
This study was a secondary data analysis of pooled data from two research groups in Australia and the U.K. The U.K. sample (n = 127) was recruited between May and June 2018 through social media (Moseley, Turner-Cobb, et al., 2021). These participants had to be over the age of 18 years and formally diagnosed as autistic (with participants asked to report the year in which they were diagnosed). The Australian sample (n = 108) was recruited between October 2020 and June 2021. They had responded to an advertisement in an emailed newsletter sent to all participants from one of two Australian longitudinal studies on autism (Arnold et al., 2019; Richdale et al., 2022). Interested individuals first registered their interest in the study via REDCap (Harris et al., 2019; Harris et al., 2009) and were subsequently contacted by a member of the Australian research team to determine interest and eligibility.
For this analysis, we removed data from nine participants, including five U.K. participants who lived in Australia and four Australian participants who reported their gender as “other.” The analytic sample thus comprised 226 autistic adults (see Table 1). The majority were diagnosed as autistic in adulthood, with only 8% diagnosed before the age of 18 years, and 55.7% diagnosed between ages 18 and 45 years. Although neither study measured participant IQ, the recruitment approaches and experimental protocol of each study would have been inaccessible to individuals with more severe learning disabilities. Moreover, the Australian study required participants be verbally fluent, and both studies required a level of computer literacy which started from being able to read, comprehend, and respond meaningfully to the virtual advertisements and subsequent questions. To address ethics requirements, participants in the Australian study were asked if they had a current diagnosis of an intellectual disability and were excluded from the study if they did. All study procedures were pre-approved by the relevant university ethics committees (La Trobe University, HEC20235; Bournemouth University: 19040), and all participants provided informed consent.
Demographics for United Kingdom, Australia, and final combined sample.
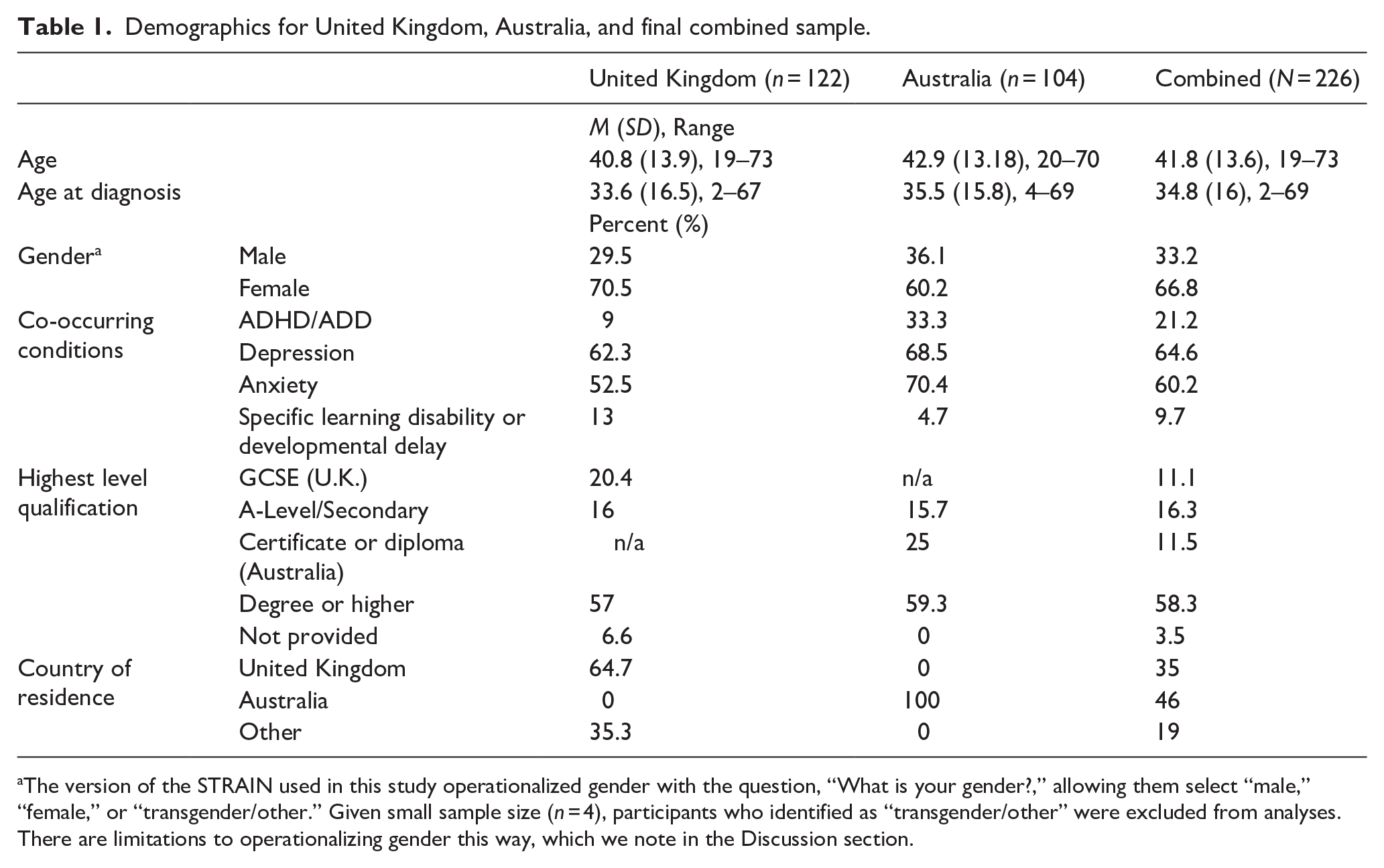
The version of the STRAIN used in this study operationalized gender with the question, “What is your gender?,” allowing them select “male,” “female,” or “transgender/other.” Given small sample size (n = 4), participants who identified as “transgender/other” were excluded from analyses. There are limitations to operationalizing gender this way, which we note in the Discussion section.
Procedure
For the U.K. dataset, the STRAIN (see below) was conducted in the course of an online survey on stress and health, which included tasks reported elsewhere (Moseley, Gregory, Smith, & Sui, 2022); scores in these other tasks, which required clear evidence of engagement, were used to verify that responses were valid. Participants completed a variety of scales online in a self-paced manner, with remote (email) support provided by author RLM if required. The Australian sample initially completed online consent, demographics, and self-report instruments on REDCap and then completed the STRAIN virtually via Zoom interview with author DH or a research assistant. 3 Identified suicidal risk was managed according to a risk-management protocol (see Byrne et al., 2022; Hedley et al., 2021). Both U.K. and Australian participants received monetary compensation for their time.
Measures
The Stress and Adversity Inventory for Adults (STRAIN)
The STRAIN (Slavich & Shields, 2018) is an National Institute of Mental Health/Research Domain Criteria (NIMH/RDoC)-recommended instrument that provides high-resolution data on cumulative exposure to life stressors—including their perceived severity, frequency, exposure timing, and duration. The STRAIN differentiates between stressors occurring in childhood versus adulthood, as well as those that are acute versus chronic (e.g. being assaulted vs prolonged financial problems), and also identifies their primary life domain (e.g. work, housing, marital relationship) and core social-psychological characteristic (e.g. interpersonal loss, humiliation; see https://www.strainsetup.com). The STRAIN has strong concurrent, discriminant, and criterion validity, correlating strongly with cortisol levels, and also predicts a variety of behavioral, biological, and clinical outcomes (Cazassa et al., 2020; Lam et al., 2019; Smith et al., 2020; Stewart et al., 2019; Sturmbauer et al., 2019). Moreover, these psychometric properties are invariant to the mode of administration (i.e. self- vs interviewer-administered). For the present analysis, we focused on participants’ total counts of eight different types of lifetime stressors and eight variables reflecting the perceived severity of these stressors rated on a scale of 1–5, with higher scores reflecting greater severity. We also examined counts and perceived severity of the same stressors when grouped by their social-psychological characteristics and their acute or chronic nature (18 variables as described below). Because the STRAIN does not measure any latent constructs, internal consistency is not relevant.
The Suicide Behaviors Questionnaire-Revised (SBQ-R)
We used the four-item SBQ-R (Osman et al., 2001), which assesses lifetime suicide ideation and suicide attempts, recent suicide ideations in the last 12 months, expression of suicidal intent to others, and perceived likelihood of future suicide attempts. We used its total score, the sum of all four items, as an index of lifetime suicidal behavior (i.e. “lifetime STB,” defined herein as past STB, as well as present judgments of future risk). Recommended cutoff scores of 7–8 indicate suicide risk in non-autistic populations. The SBQ-R has adequate psychometric properties in the general population (Batterham et al., 2015; Cassidy, Bradley, Bowen, et al., 2018) and showed adequate internal consistency in the present study (UK sample α = 0.81; AU sample α = 0.72).
Data analysis and covariates
Two male participants neglected to enter their age and so were dropped from analyses using this covariate. Otherwise, there were no missing data and no extreme datapoints. We used the Kessler 6-item Psychological Distress Inventory (K6) (Kessler et al., 2003), initially as a dependent variable for comparison between groups, and then as a covariate in regression to adjust for the possible influence of current psychological distress indicative of psychopathology. For the K6, higher scores indicate increased psychological distress (Furukawa et al., 2003; Kessler et al., 2003). Cutoff scores of 8–12 indicate mild-to-moderate mental illness, whereas scores of 13 and above indicate more severe mental illness.
Comparisons between men and women
To test our a priori hypotheses regarding greater psychological distress, STB, lifetime stressor count, and perceived stressor severity in autistic women than in men, we compared the two groups in four univariate and multivariate analyses of variance (MANOVAs; alpha levels corrected to p = 0.0125), while controlling for the age difference between men (M = 45.9, SD = 14.5 years) and women (M = 39.8, SD = 12.64 years), t(222) = 3.18, p = 0.002, d = 0.45, 95% CI [0.17, 0.74] and for potential variance associated with study site. 4
To test whether autistic women had higher scores in psychological distress and STB than autistic men (Hypothesis 1), we performed two univariate ANOVAs to compare their K6 scores and SBQ-R scores, respectively. Subsequently, to examine whether women were exposed to more numerous life stressors and experienced them as more stressful (Hypotheses 2 and 3), we compared autistic men and women with respect to lifetime stressor count and perceived stressor severity. The STRAIN categorizes stressors by life domains, and of these, stressors from eight domains 5 were previously associated with STB in autistic people (Black et al., 2022; Chou et al., 2020; Cooper et al., 2022; Doherty et al., 2022; Hedley and Uljarević, 2018; Holden et al., 2020; Pearson et al., 2023; Weir et al., 2022; Yew et al., 2021). Therefore, this MANOVA included count and perceived severity of stressors related to Work (e.g. being fired or made redundant, struggling to gain employment); Housing (e.g. moving frequently, living in unsafe or poor conditions); Financial (e.g. difficulty covering rent and basic needs); Education (e.g. dropping out, failing exams); Treatment and Health (e.g. being hospitalized, seeking or receiving treatment); Legal/Crime (e.g. being the victim of a crime, being arrested); Marital/Romantic Relationships (e.g. having major fights or chronic conflict); and Other Relationships (e.g. being discriminated against or excluded, losing friendships).
Some adverse experiences for autistic people operate across multiple life domains and may do so in an enduring manner (e.g. rejection and bullying may occur for autistic people in relation to Education, Work, Other Relationships, Marital/Romantic Relationships; Jones et al., 2022). In this context, the shared social-psychological characteristics of apparently diverse stressors may be particularly meaningful, as might their nature as acute or chronic (Stewart et al., 2019). As such, our second analysis categorized lifetime stressors by their core social-psychological nature and their duration as acute (lasting no more than a few days) or chronic (lasting at least 1 month). In this MANOVA, we compared autistic men and women in the count and perceived severity of acute and chronic instances of interpersonal loss (e.g. separation from a partner, bereavement); acute and chronic instances of humiliation (e.g. being fired, bullying); acute and chronic instances of physical danger (e.g. assault, living in unsafe environments); chronic instances of entrapment, which by nature is only chronic (e.g. caregiving responsibilities or financial insecurity); and acute and chronic instances of role change/disruption (e.g. being temporarily disabled by illness, caring for elderly parents).
Associations between stressor exposure, stress perception, and STB
As a preliminary analytic step, we plotted correlations between all STRAIN variables, K6 scores, and SBQ-R scores for all participants combined (see Supplemental Table S1 and Supplemental Table S2). Subsequently, to test our prediction that cumulative lifetime stressor exposure and perceived severity would be related to psychological distress and lifetime STB (Hypothesis 4), we performed four planned hierarchical regressions (Enter method), with alpha levels corrected to p = 0.0125 to account for multiple comparisons. Prior to performing these analyses, we mean-centered all variables, confirmed homoscedasticity and normal distributions of residuals, and ensured independence and the absence of multicollinearity between STRAIN variables. To increase robustness of our findings, we used bootstrapping with 5,000 resamples in each regression (providing bias-corrected confidence intervals; BCa 95% CI).
In the first regression, we modeled site of data collection in Block 1, lifetime stressor count for eight key life domains (Work, Housing, Financial, Education, Treatment/Health, Legal/Crime, Marital/Romantic Relationships, Other Relationships) in Block 2, and current psychological distress (K6 scores) in Block 3. While keeping Block 1 and Block 3 constant, in the second regression, we replaced Block 2 variables with lifetime stressor counts for acute and chronic instances of interpersonal loss, humiliation, physical danger, entrapment, and role change/disruption. In the third regression, we replaced Block 2 variables with perceived severity of stressors categorized by the eight life domains above, while keeping Blocks 1 and 3 constant. In the fourth regression, we similarly retained Block 1 and 3 variables but modeled perceived severity of acute and chronic stressors categorized by social-psychological type. In each instance, SBQ-R scores were modeled as the dependent variable. With regressions stratified by gender, we compared the models using Fisher’s z; we additionally report Cohen’s q with 95% CI.
Community involvement
The research team includes neurotypical and neurodivergent people. The U.K. study was led by an autistic researcher who designed and implemented the study. The Australian study partnered with local autism associations, peak organizations, and included an autistic advisory group who were consulted and advised on the design of the study, ensuring that it was acceptable to participants, used respectful language throughout, and included appropriate safeguarding measures.
Results
Psychological distress (K6) and STB (SBQ-R)
Levels of psychological distress (K6 scores) were indicative of greater-than-average psychological distress in the sample, indicative of elevated psychopathology (M = 18.5, SD = 6, range = 6–30). Similarly, the present sample exhibited high levels of STB, with average SBQ-R total scores of 9.8 (SD = 3.9, range = 3–18).
Gender differences in psychological distress, STB, and lifetime stress
Between-group comparisons on study variables are provided in Table 2. Autistic women and men did not differ significantly on psychological distress (p = 0.074) or lifetime STB (p = 0.158). In relation to lifetime stressor count, with stressors categorized by life domain (Figure 1, part a), we found that autistic men experienced more Legal/Crime-related stressors and that autistic women experienced more Other Relationships stressors. Moreover, women tended to perceive Treatment/Health-related stressors and Other Relationship stressors as being more severe (see Figure 1, part A, and Table 2, row 1). With acute and chronic stressors categorized by core social-psychological characteristics (Table 2, row 2), autistic women experienced significantly more chronic humiliation stressors than autistic men and perceived these stressors as being more severe. Autistic women also perceived chronic entrapment stressors as being more severe, although they did not experience more of them (Figure 1, part b).
Between-group comparisons of psychological distress, lifetime suicidal thoughts and behaviors, lifetime stressor count and perception in autistic men and women.

Asterisks and bold text highlight comparisons significant at an adjusted threshold of p < 0.0125.
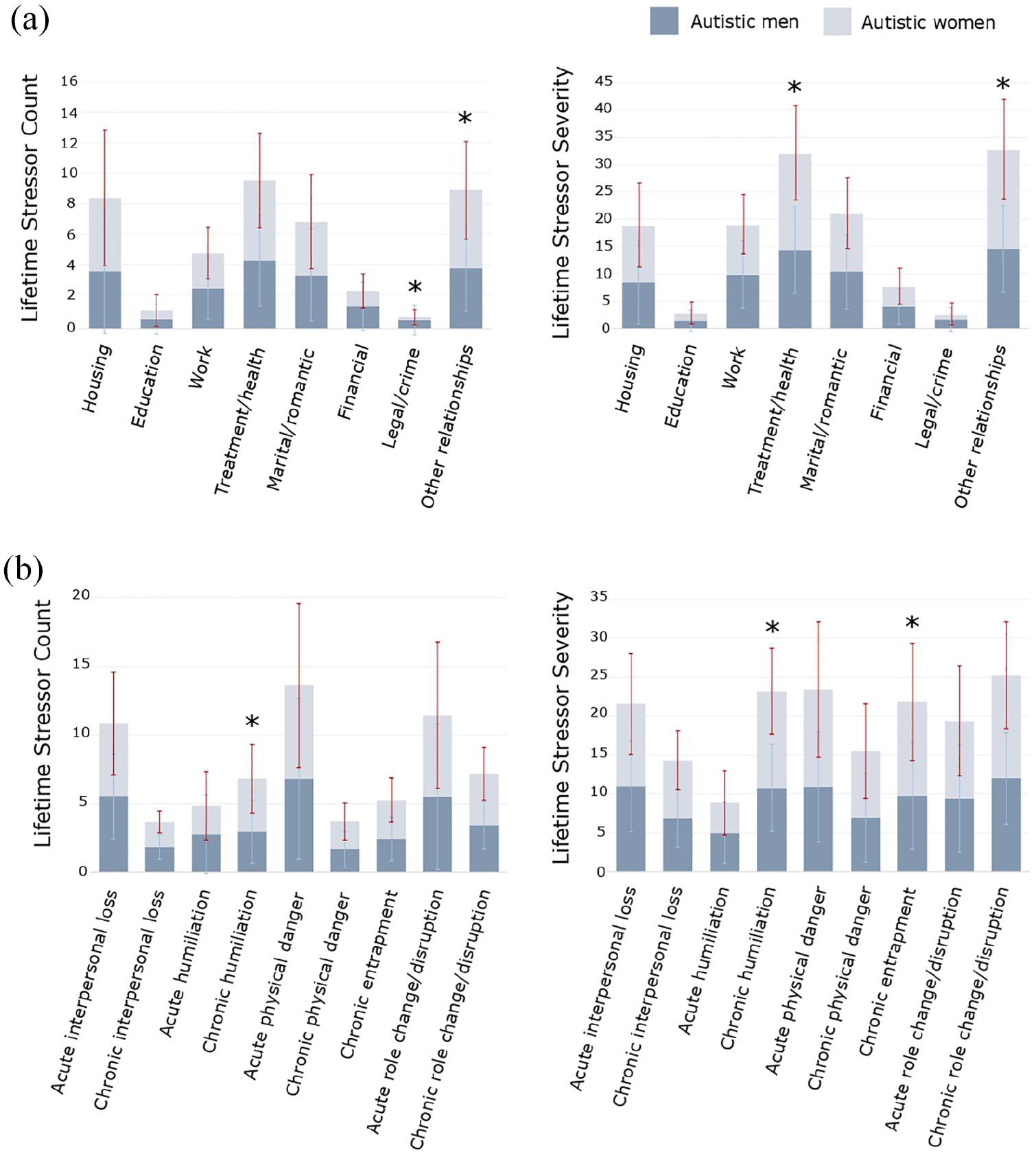
Lifetime stressor exposure in autistic men and women. Lifetime stressor count and perceived severity categorized by (a) primary life domain and (b) core social-psychological characteristic. Error bars reflect standard deviations, and significant differences between autistic men (dark gray) and autistic women (light gray) are marked with asterisks (*).
Lifetime stressor exposure predicted STB
As hypothesized, experiencing more Treatment/Health-related stressors over the life course was related to greater STB for both autistic men and women (see Table 3). For autistic women, lifetime Treatment/Health-related stressor count remained a significant predictor of STB even while controlling for current psychological distress. Categorizing acute and chronic stressors by their core social-psychological characteristic revealed that different stressors were most strongly related to STB for autistic men versus women. Specifically, whereas experiencing more lifetime chronic interpersonal loss stressors predicted STB in men, experiencing more lifetime acute danger stressors predicted STB for women. Moreover, in contrast to the hypothesized direction of associations between stressors and STB, experiencing fewer chronic entrapment stressors over the life course predicted STB in autistic women.
Lifetime stressor counts as predictors of lifetime suicidal thoughts and behaviors: regression models for autistic men and women.
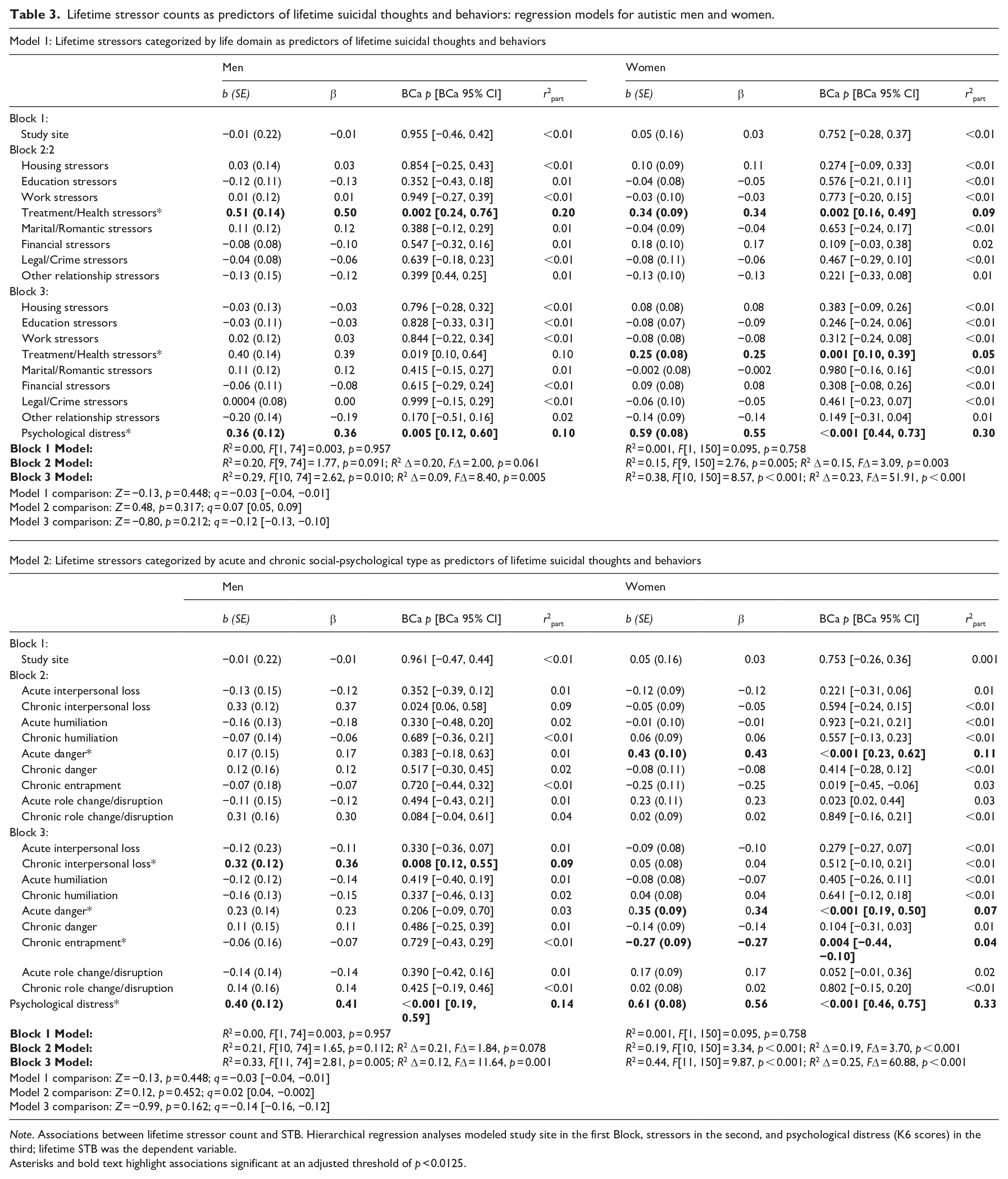
Note. Associations between lifetime stressor count and STB. Hierarchical regression analyses modeled study site in the first Block, stressors in the second, and psychological distress (K6 scores) in the third; lifetime STB was the dependent variable.
Asterisks and bold text highlight associations significant at an adjusted threshold of p < 0.0125.
Lifetime perceived stressor severity predicted STB
Focusing on perceived stressor severity, as hypothesized, greater lifetime perceived severity of Treatment/Health-related stressors was related to more STB for both autistic men and women (Table 4). Having lower lifetime perceived severity of Other Relationship (e.g. friendship) stressors was associated with more STB in autistic women, but not independent of current psychological distress. Finally, we found that greater lifetime perceived severity of acute dangerous stressors was associated with greater STB for autistic women.
Lifetime perceived stressor severity as predictive of lifetime suicidal thoughts and behaviors: regression models for autistic men and women.
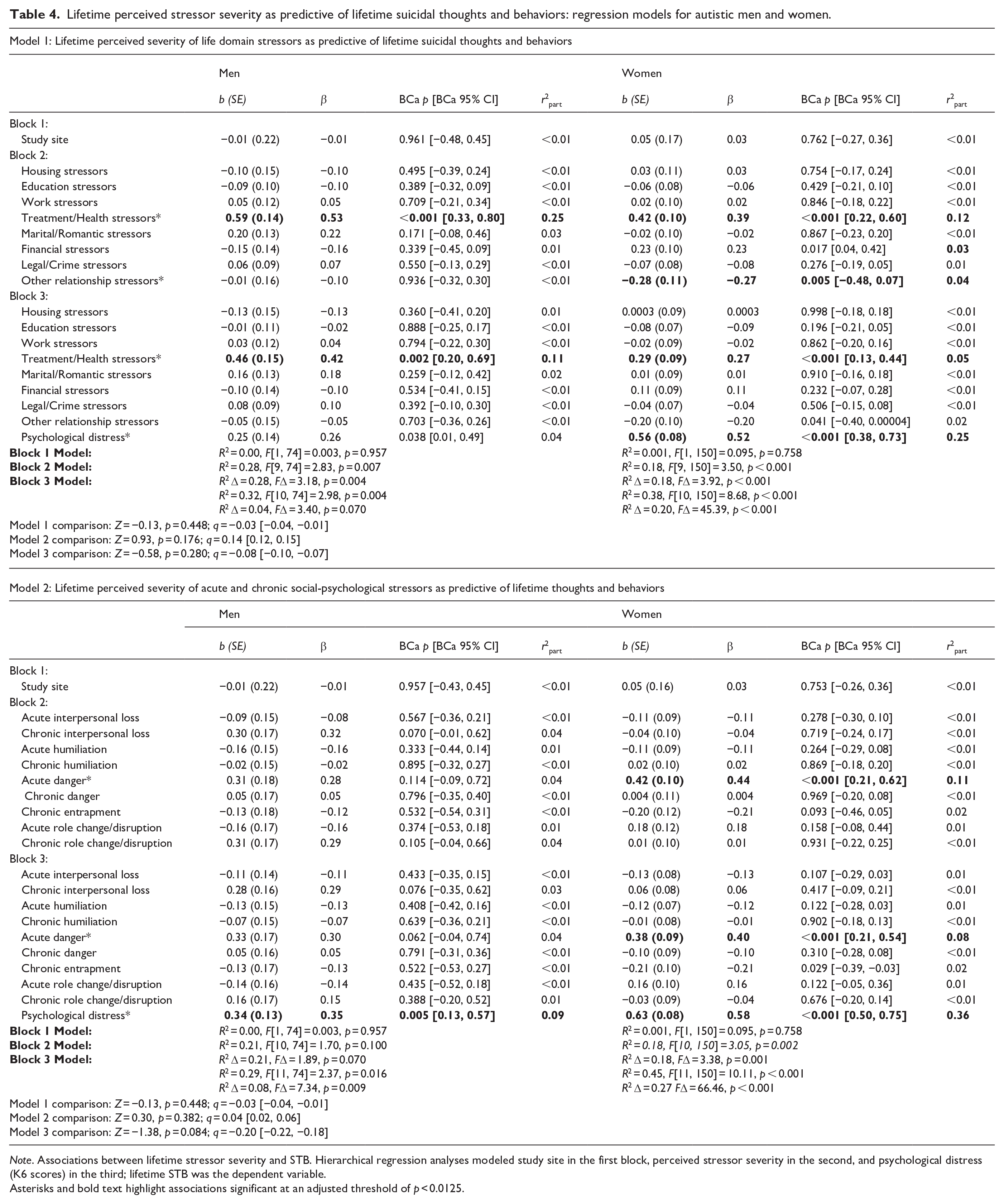
Note. Associations between lifetime stressor severity and STB. Hierarchical regression analyses modeled study site in the first block, perceived stressor severity in the second, and psychological distress (K6 scores) in the third; lifetime STB was the dependent variable.
Asterisks and bold text highlight associations significant at an adjusted threshold of p < 0.0125.
Discussion
In this first multinational study of lifetime stressor exposure and STB in autistic people, we investigated how a variety of different stressors occurring across the entire life course were related to STB in autistic participants and whether any stressor-STB associations differed by gender. Consistent with our primary hypothesis, autistic men and women differed significantly in their exposure to and perceived severity of life stressors. Specifically, whereas treatment and health-related stressors were associated with STB for both autistic men and women, there were gender differences in the relevance of other specific life stressors for STB. Although these associations require replication with larger samples in longitudinal designs, our data suggest that different lifetime stressors may predict STB for autistic men versus women.
Stressor exposure and perception differs in autistic men and women
Prior research using the STRAIN has revealed greater lifetime exposure to (and perceived severity of) almost every kind of stressor in autistic compared to non-autistic participants (Moseley, Turner-Cobb, et al., 2021). The present findings build on this research by identifying gender differences in autistic participants that mirror those seen in the general population (Cazassa et al., 2020; Slavich et al., 2019; Slavich & Shields, 2018; Sturmbauer et al., 2019)––namely, like their neurotypical counterparts, autistic men experienced more legal/crime-related stressors over the life course, whereas women experienced more friend/family relationship stressors over the life course. We found that autistic women experienced more chronic humiliation than did autistic men, although this gender difference in humiliation is less reliably observed in non-autistic women (Cazassa et al., 2020; Slavich & Shields, 2018). Interestingly, we did not find evidence that autistic women experienced more entrapment or interpersonal loss stressors than autistic men, which has been found in non-autistic samples (Cazassa et al., 2020; Slavich & Shields, 2018; Sturmbauer et al., 2019). Since stressor exposure in non-autistic women has been linked to social inequities (Helpman, 2023), the marginalization of autistic people broadly (Jones et al., 2022), in addition to their greater lifetime stressor burden (Mahony & O’Ryan, 2022; Moseley, Turner-Cobb, et al., 2021), may be why some gender differences are less apparent, even while others emerge.
In both autistic and non-autistic samples, experiencing stressors as more stressful has been found to mediate the impact of lifetime stressor exposure on mental health (Moseley, Turner-Cobb, et al., 2021; Shields et al., 2023). The present data, in corroboration with other reports (McQuaid, Weiss, et al., 2022), suggests that autistic women may be more likely to perceive, and experience, life stressors as more stressful than autistic men. Because greater stressor exposure typically increases the perception of stressors as being stressful (Slavich, 2020), and also increases their impact on health (Slavich & Cole, 2013; Slavich, Mengelkoch, & Cole, 2023), some instances of higher perceived stressor severity in autistic women could reflect their greater lifetime exposure to that stressor—as in our data, for instance, where autistic women had higher stressor count and perceived stressor severity related to other relationships and chronic humiliation. At the same time, there were also some stressors, namely those related to chronic entrapment and treatment/health, which, with higher perceived severity, appeared to affect autistic women more severely than autistic men, despite women not having experienced more of them. Regardless of whether autistic women actually experience more major stressors across the life course, the fact that they perceive some stressors as more severe would have highly significant implications for their health and wellbeing given evidence showing that it is the perception of stressor severity that matters most for health (Slavich, 2020, 2022; Slavich, Roos, et al., 2023).
Intraindividual differences in stressor perception can be traced back to a variety of factors that influence psychosocial vulnerability and resilience (Lebois et al., 2016; Shields et al., 2023; Slavich et al., 2022). Vulnerability factors for autistic women could originate from the social environment, such as greater pressure to perform femininity in occupational and familial spheres (Gore et al., 2023; Grove et al., 2023) and, perhaps relatedly, greater burden of camouflaging (McQuaid, Lee, & Wallace, 2022; Wood-Downie et al., 2021). Some vulnerability factors, such as existing psychopathology and greater difficulty with emotion regulation (Weiner et al., 2023), could be related to longer duration of undiagnosed autism in some people assigned female at birth (Mandy et al., 2022). Vulnerability can also be conferred by the relative absence of protective factors such as social support, given the difficulties autistic women often face in establishing and maintaining relationships (Black et al., 2022; Gosling et al., 2023; Sedgewick, Crane et al., 2019; Sedgewick, Hill, & Pellicano, 2019). Autistic women also have reduced access to a range of professional support, most notably in healthcare settings (Miller et al., 2022; Tint et al., 2023; Tint & Weiss, 2018), where they often experience misdiagnoses, invalidation, and gaslighting (Fusar-Poli et al., 2022; Gosling et al., 2023; Grove et al., 2023; Tint & Weiss, 2018). This fact may be why, even while our hypothesis of more numerous healthcare/treatment-related stressors in women was not supported, these stressors were perceived as more severe.
Stressors relevant for STB across both groups
The extent to which gender differences in lifetime stressor exposure and perception are relevant for health rests on their deleterious sequalae (Alley et al., 2025; Mengelkoch & Slavich, 2024; Slavich & Sacher, 2019). Here, we examined associations between lifetime stressor exposure, stressor perception, and STB as dependent or independent of psychological distress given the role that psychopathology plays in mediating the impact of stressor exposure on suicide (Hockey et al., 2022; Stewart et al., 2019; Zhang et al., 2020) and the fact that psychopathology can explain the elevated rates of suicide death seen in autistic versus non-autistic women (Lai et al., 2023). Some lifetime stressors were associated with STB in autistic men and women, while some were associated with STB in men or women alone. While cross-sectional research precludes conclusions of directionality between stressors and STB, these findings may provide important priorities for further investigation.
Regarding associations that were significant for both autistic men and women, we found that greater exposure to and perceived severity of treatment/health-related stressors was associated with greater STB in men and women. The prominence of these stressors is perhaps foreseeable given the poorer physical and mental health of autistic adults (Lai, 2023; Ward et al., 2023), who will necessarily encounter these stressors more frequently than non-autistic counterparts (Moseley, Turner-Cobb, et al., 2021). Although relations between treatment/health-related stressors and STB could reflect the well-established association between physical/psychiatric morbidity and STB (Fu et al., 2023; Onyeka et al., 2020), they could also be related to dissatisfactory or even traumatic healthcare encounters among autistic people (Brede et al., 2022; Doherty et al., 2022; Marsden et al., 2024).
Although we cannot confirm either interpretation, particularly in this time-insensitive design, both are easily conceptualized within theoretical frameworks for suicide. Indeed, chronic illness is frequently associated with feelings of hopelessness, entrapment, psychological pain, perceived burdensomeness, and social disconnection from others (Rogers et al., 2020; Shim et al., 2023). These feelings are also apparent in autistic accounts of facing barriers to healthcare (“I just felt like a burden” (Crane et al., 2019); “I’m alone almost all the time . . . I wonder what the point of me being here is . . . I have no life and no purpose” (Camm-Crosbie et al., 2019)). Although greater lifetime perceived severity of treatment/health-related stressors was related to STB for both autistic men and women in this sample, the fact that autistic women tended to perceive these stressors as more severe suggests that this association might be relevant to their higher levels of suicidal behavior (Hirvikoski et al., 2020; Kolves et al., 2021; Santomauro et al., 2024).
Stressors differentially relevant for STB in autistic men and women
Several stressor types emerged as differentially related to STB for autistic men and women in the present data. For autistic men, exposure to chronic interpersonal loss across the life course was associated with STB. A profound human need for connection lies at the heart of prominent approaches to suicide (Klonsky & May, 2015; Van Orden et al., 2010), stress, and health (Allen et al., 2021; Slavich, 2020, 2022; Slavich, Roos, et al., 2023; Slavich & Sacher, 2019). With reference to dominant theories of suicide, interpersonal loss may contribute to thwarted belongingness (Van Orden et al., 2010), the loss of social connectedness which might anchor an individual to living (Klonsky & May, 2015), and the absence of a social safety net (Zhang, 2019); it is, moreover, one of several core social threats capable of invoking a neurobiological stress response and subsequently damaging mental and physical health (Slavich, 2020; Slavich & Sacher, 2019). Among other social stressors, Stewart et al. (2019) found that instances of acute interpersonal loss uniquely precipitated suicide attempts in neurotypical adolescents. Given our older autistic sample, the relevance of chronic interpersonal loss to STB may be more akin to the role of loneliness in autistic psychopathology and suicide (Grace et al., 2022; Hedley, Uljarević, Foley, Richdale and Trollor, 2018; Levi et al., 2023), where individuals may have fewer social connections which dwindle over time.
Interestingly, a similar interpretation as for social connectedness might pertain to the emergence of chronic entrapment as a predictor of STB in autistic women. Although STB are typically associated with greater feelings of entrapment (Li et al., 2018; R. C. O’Connor & Kirtley, 2018), we found that autistic women with lower lifetime exposure to and perceived severity of entrapment stressors reported greater STB. Chronic by nature, entrapment stressors include such experiences as being a caregiver, 6 experiencing overwhelming demands in social, educational, or occupational spheres, and being trapped in unsafe/dissatisfying living circumstances. Although not universally true, it is conceivable that some entrapment stressors are a form of connectedness (Klonsky & May, 2015), either to other people or to a meaningful project, job, or role. As per this theory, such connections may keep individuals invested in living when their strength equates or surpasses that of psychological pain and hopelessness.
This interpretation is intriguing in relation to our prior study, where examining the U.K. sample alone revealed that greater entrapment was associated with greater psychological distress (Moseley, Turner-Cobb, et al., 2021). The precise nature of entrapment stressors experienced by our sample is unknown to us, but it is conceivable that some might have deleterious effects on mental health while still functioning as a source of connection. As a putative example, unemployment is linked to STB in autistic and non-autistic people alike (Kolves et al., 2021). However, workplace relationships and insufficiently adapted environments also cause considerable stress in autistic people (Bury et al., 2021; Hayward et al., 2020; Tomczak & Kulikowski, 2023), which could explain why employment may not protect autistic people against depression and STB in the same way as it does non-autistic people (Hedley et al., 2019; Kolves et al., 2021; Schwartzman & Corbett, 2022). Employment could therefore be conceived of as an entrapment stressor which, although providing a sense of purpose and/or relationships with other people, also incurs stress and subsequent health impacts.
A similar explanation might account for why lower perceived severity of other relationship stressors was associated with greater STB in autistic women (albeit not independently of psychological distress). Autistic women tended to experience more such stressors and to perceive these stressors as being more severe than did autistic men, and finding relationships stressful could incur allostatic load, or biological “wear and tear” on the body. However, it is possible that perceiving these stressors as less stressful is indicative of having fewer such relationships, which even if stressful, provide connection, meaning, and purpose. Although this interpretation requires further investigation, it would appear consistent with the proposed centrality of social connection and belongingness in STB (Mournet et al., 2023), and the challenges associated with social relationships in autistic men and women (Grove et al., 2023; Jones et al., 2022; Moseley, Shalev et al., 2024; Schnabel & Bastow, 2023).
Finally, for autistic women, lifetime exposure to and perceived severity of acute physically dangerous stressors was relevant to STB over and above psychological distress. Across different frameworks, suicide capability is proposed as a mechanism through which physically painful and/or dangerous experiences can erode evolutionary instincts for self-preservation (Klonsky & May, 2015; O’Connor & Kirtley, 2018; Van Orden et al., 2010). This mechanism was supported in autistic people (Moseley, Gregory, Smith, Allison, Cassidy and Baron-Cohen, 2022a; Moseley, Gregory et al., 2024) but only partially explains the relation reported elsewhere between traumatic events and STB (Pelton et al., 2020; Warrier & Baron-Cohen, 2021). It is possible that post-traumatic sequalae of dangerous stressors might additionally explain this association. Future research should, however, elucidate the timeframe between such events and STB and the mechanisms which might, for some individuals, link the two.
Strengths and Limitations
Several strengths of this study should be noted. Most notably, this is the first multinational study of how lifetime stressor exposure and perception relate to STB in autistic adults. STB is a critical issue in autistic populations, and although stressor exposure is a well-recognized risk factor in many other contexts (Dedoncker et al., 2021; Gilgoff et al., 2024; Seiler et al., 2020, 2024), it is not yet widely regarded as a critical risk factor in autistic populations. Moreover, using a statistically robust, hypothesis-driven study design, we provide evidence of how lifetime stressor exposure and perceived severity are patterned by gender and, in addition, differently related to STB for autistic men versus women.
Several limitations also bear remembering. Foremost, the cross-sectional design precludes drawing conclusions about the direction of associations between stressor exposure, stress perception, psychological distress, and STB––particularly since STB can exacerbate or generate psychopathology and interpersonal stress (S. S. O’Connor et al., 2021; Tong et al., 2021). STB are dynamic and fluctuate nonlinearly over time (Bryan et al., 2020) and so are best studied over multiple timepoints. Second, we did not have a non-autistic comparison group. Third, autistic adults with intellectual disabilities were excluded, and the sample is thus not representative of the full autism spectrum. Indeed, given the majority of the autistic sample were diagnosed in adulthood, they may be less representative of those diagnosed in childhood and more representative of an autistic sub-demographic often represented in studies recruiting online, who tend to be more highly qualified and employed than the autistic population broadly (Rødgaard et al., 2022). Generalization of the findings to autistic men may be particularly tentative given the comparably smaller size of this group in our study.
Fourth, we combined data from two studies with different sampling methods and modes of STRAIN administration. The STRAIN is robust to differences in administration (i.e. self- vs interviewer-administered), and we also controlled for study site in our analyses. Nevertheless, sampling and administration differences should be avoided where possible. As the STRAIN assesses lifetime exposure to and perception of specific kinds of stressors, rather than current stress, we similarly believe that the different times when the data was collected (the U.K. data before the COVID-19 pandemic, the Australian data during it) did not notably impact STRAIN variables; however, this could potentially have affected participants’ K6 and SBQ-R scores. Again, controlling for differences in study site would have minimized this issue, but caution is still warranted when interpreting the results.
Fifth, our measurement tools were not specifically designed by or for autistic people. Namely, neither the K6 nor STRAIN have been validated in autistic people, and the latter, particularly, may neglect life experiences that are especially relevant for, or perceived as severe in, autistic populations. Likewise, classifying lifetime stressors into social-psychological categories like entrapment and humiliation may not be the most appropriate classification for autistic people. The SBQ-R has since been found to operate slightly differently in autistic people (Cassidy et al., 2020), leading to the development of a revised version (Cassidy et al., 2021), which was not available at the time our studies were completed.
Sixth, we used SBQ-R total score as a dependent variable, which reflects a broad index encapsulating multiple facets of STB (i.e. lifetime STB), including proclivity to communicate suicidal thoughts to others and perceived likelihood of future suicide attempts. This approach was deemed appropriate given the time-insensitive cross-sectional design, but as there are gender differences in these different facets of STB in the general population (Schrijvers et al., 2012), there may also be differences in autistic adults (Kirby et al., 2024; Newell et al., 2023; Santomauro et al., 2024) which are important to consider. In particular, since the prevalence of suicide ideation may be equally prevalent across autistic people (Santomauro et al., 2024), and since we do not know whether there are differences in disclosure behavior in autistic adults, the use of total SBQ-R scores may be the reason our analyses did not reflect apparently higher risk rates of suicide attempts and deaths in autistic women (Santomauro et al., 2024). Unrepresented in SBQ-R scores, of course, are those whose suicide attempts led to death by suicide.
Seventh and relatedly, our exploration of gender was limited by (a) our assessment of this variable, (b) insufficient representation of minorities, and (c) a lack of direct statistical comparisons between groups, since we lacked sufficient power to model gender as a moderator. In this version of the STRAIN, gender was operationalized by a single question with response options “female,” “male,” or “transgender/other.” However, our use of language was limited, since some transgender women and men may have responded as “female” or “male,” respectively, thus neglecting an important distinction given the additional inequalities and adversity faced by transgender men and women (Murchison et al., 2023; Strang et al., 2021). The exclusion of a few participants who did not identify as either male or female also meant that those who identify outside of the gender binary were excluded, although their higher rates of STB and life adversity suggest the relevance of a stress framework to this group (Gosling et al., 2022). In examining associations between life stressors and STB, moderating effects of a more expansive gender concept, as well as sex assigned at birth, would be an important goal to identify stressors of differential relevance to STB in people of different sexes and genders.
Finally, we note other clinically relevant factors to stress and suicide in autistic people that were not assessed here due to insufficient variance in the dataset. These factors include race and ethnicity (Ames et al., 2022); age at diagnosis (Mandy et al., 2022; Newell et al., 2023), particularly given its relationship with sex and gender (Lai et al., 2022); and age at study participation, given differential importance of life experiences to suicide at varied points of the lifespan (Stewart et al., 2019). Indeed, the autistic community are often perceived monolithically as regards their challenges and related suicide risk, but life stages may be highly influential (Moseley, Druce, et al., 2021). Although we used a hypothesis-driven approach with an existing, empirically supported tool, more exploratory approaches toward developing a taxonomy of life events that autistic people of different ages experience as stressful and understanding their relation not only to self-reported outcomes but also to physiological indices of stress linked to STB would be a worthy goal. Given the present scarcity of research focusing on protective factors in relation to STB in autism (c.f., Hedley et al., 2024), we also highlight factors that might mitigate the impacts of life stressors as an important target for further study.
Conclusion
Notwithstanding these limitations, this is the first multinational study to investigate how lifetime stressor exposure and severity relates to STB in autistic adults and whether these effects differ between men and women. We found that autistic men and women had different patterns of lifetime stressor count and perceived severity and, in addition, that the effects of these stressors on STB differed across these groups. The direction of these associations must be further investigated, but in the meantime, the data highlight the potential utility of screening for lifetime stressor exposure when predicting suicide risk in autistic individuals and may also help refine thinking and research on this topic, particularly with respect to understanding key drivers of health disparities in the autistic population.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241299872 – Supplemental material for Lifetime stressor exposure is related to suicidality in autistic adults: A multinational study
Supplemental material, sj-docx-1-aut-10.1177_13623613241299872 for Lifetime stressor exposure is related to suicidality in autistic adults: A multinational study by Rachel L Moseley, Darren Hedley, Julie M Gamble-Turner, Mirko Uljarević, Simon M Bury, Grant S Shields, Julian N Trollor, Mark A Stokes and George M Slavich in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613241299872 – Supplemental material for Lifetime stressor exposure is related to suicidality in autistic adults: A multinational study
Supplemental material, sj-docx-2-aut-10.1177_13623613241299872 for Lifetime stressor exposure is related to suicidality in autistic adults: A multinational study by Rachel L Moseley, Darren Hedley, Julie M Gamble-Turner, Mirko Uljarević, Simon M Bury, Grant S Shields, Julian N Trollor, Mark A Stokes and George M Slavich in Autism
Footnotes
Acknowledgements
The authors sincerely thank the individuals who took part in the U.K. and Australian studies, as well as the members of the Australian autistic advisory group. The authors acknowledge, for the Australian study, the financial support of the Suicide Prevention Australia National Suicide Prevention Research Fund and Untapped Holdings; data for this study were collected and managed using REDCap electronic data capture tools hosted at La Trobe University (Harris et al., 2009, ![]() ). For the U.K. study, the authors thank their institution for the internal funding which made this study possible and the moderators of Facebook groups where they recruited the participants.
). For the U.K. study, the authors thank their institution for the internal funding which made this study possible and the moderators of Facebook groups where they recruited the participants.
Author contributions
Data availability
Requests for access to the Australian sample data should be directed to Darren Hedley, PhD, School of Psychology and Public Health, La Trobe University, Melbourne 3086, VIC, Australia; email: d.hedley@latrobe.edu.au. Requests for access to the U.K. sample data should be addressed to Rachel Moseley, PhD, Department of Psychology, Bournemouth University, UK; email: rmoseley@bournemouth.ac.uk. The corresponding author had full access to all of the study data and had final responsibility for the decision to submit the report for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DH was supported by a Suicide Prevention Australia National Suicide Prevention Research fellowship. MU was supported by a Discovery Early Career Researcher Award from the Australian Research Council (DE180100632). JNT was supported by NHMRC Investigator Grant GNT2009771. GMS was supported by the grant #OPR21101 from the California Governor’s Office of Planning and Research/California Initiative to Advance Precision Medicine. The findings and conclusions in this article are those of the authors and do not necessarily represent the views or opinions of these organizations, which had no role in designing or planning this study; in collecting, analyzing, or interpreting the data; in writing the article; or in deciding to submit this article for publication.
Ethical approval
The Australian research was approved by La Trobe University Human Research Ethics Committee HEC20235, and the U.K. study was approved by the Ethics Panel of the Faculty of Science and Technology, Bournemouth University (ID: 19040). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from participants after the nature of the study was explained.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.