
Abstract
Anxiety has been associated with social communication and interaction differences among autistic children. We sought to clarify the direction of these associations longitudinally, and test executive function as a moderator. Participants were autistic children (N = 157; 15% female, 85% male) engaged in a longitudinal study. Analyses focused on two timepoints during preadolescence (M ages 9.7 and 10.7 years). A cross-lagged panel model tested whether parent-reported anxiety at age 9 years predicted teacher-reported social communication and interaction differences at age 10 years, and vice versa. Next, multigroup analyses tested for similarity in cross-lagged pathways at different levels of teacher-reported metacognition and behavioural regulation (two facets of executive function). At each time point, respectively, 22% and 21% of children had anxiety exceeding a suggested clinical threshold. Longitudinal associations between parent-reported anxiety and teacher-reported social communication and interaction differences were not significant in the full sample. However, multigroup analyses found lower levels of parent-reported anxiety at age 9 years predicted greater teacher-reported social communication and interaction differences at age 10 years among participants with clinically elevated behavioural dysregulation. Findings indicate low levels of anxiety, coupled with behavioural dysregulation, may signify potential for increasing social communication and interaction differences observed by teachers among autistic children entering adolescence.
Lay abstract
Anxiety is a mental health concern affecting many autistic children, and has been linked to greater differences in social communication and interaction style. Executive functioning (i.e. the ability to direct and regulate attention and behaviour) plays an important role in autistic children’s social–emotional development. We tested whether anxiety (reported by parents) predicts social communication and interaction differences (reported by teachers) over time or vice versa among autistic preadolescents. We also investigated whether the link between anxiety and social communication and interaction differed depending on children’s EF abilities (reported by teachers). We found less parent-reported anxiety predicted more teacher-reported social communication and interaction differences a year later – but only for children who had heightened behavioural dysregulation (an aspect of executive functioning that includes impulse and emotion control). Our work suggests autistic preadolescents with behavioural dysregulation and limited anxiety may be at greater risk for social difficulties, and may need more support in this area. Executive functioning may be a useful mechanism to target in treatment for this group of children.
Autism is a heterogeneous neurodevelopmental condition characterised by differences in social communication and patterns of restricted and repetitive behaviours. Anxiety is a major mental health issue affecting 42%–79% of autistic children (Kent & Simonoff, 2017), with broad, adverse functional impacts, including interference in peer interactions, participation at school and overall family well-being (Adams & Emerson, 2021). Investigating how and why anxiety develops and relates to important domains within autism (i.e. social and cognitive functioning) may uncover predictors and mechanisms that hold implications for assessment and treatment.
Anxiety and social communication and interaction
Social communication and interaction (SCI) encompasses verbal and nonverbal behaviours used in reciprocal social interaction, typically judged according to neurotypical expectations. Early emergent differences in SCI styles between autistic and non-autistic people may result in persistent misunderstandings between groups (as detailed in the double empathy problem theory; Milton, 2012). It has been proposed that for autistic people, being misperceived by the neurotypical majority can lead to negative developmental and mental health consequences (Mitchell et al., 2021). Cross-sectional research has highlighted positive associations between anxiety and SCI differences in autistic youth (e.g. Chang et al., 2012; Swain et al., 2015). However, longitudinal studies yield conflicting findings. In a population-based sample of children not ascertained for autism (N = 9491), Pickard et al. (2017) found parent-reported SCI differences at ages 7 and 10 years predicted increased parent-reported social anxiety 3 years later, but not the reverse, supporting the hypothesis that SCI differences provoke experiences of social exclusion and anxiety (Wood & Gadow, 2010). In contrast, in a sample of 2- to 10-year-old autistic children (N = 130) referred to mental health services, Duvekot et al. (2018) found parent-reported anxiety predicted parent-reported SCI differences 2 years later but not the reverse, supporting the hypothesis that anxiety-related avoidance and/or rigidity may impede opportunities to learn and practice social skills (S. W. White et al., 2014). Elsewhere, in a non-referred sample of 5- to 17-year-old autistic youth with diverse cognitive abilities (N = 54), Teh et al. (2017) found no significant associations between anxiety and SCI differences (both parent-reported) over a 10–19 month period.
The discrepancy between these findings is perhaps unsurprising given methodological differences and the possibility that SCI differences in non-autistic versus autistic samples reflect different underlying mechanisms (Lord & Bishop, 2021). Pickard et al.’s (2017) findings within a general population sample may not hold among autistic children. Duvekot et al.’s (2018) findings may apply primarily to autistic youth with elevated mental health symptoms. Moreover, wide age ranges within Teh et al. and Duvekot et al.’s samples could obscure developmental variations in anxiety trajectories. Notably, the transition to adolescence is a developmental period characterised by dramatic shifts in identity, self-awareness and cognitive control, alongside increasing reliance on peer relations (Blakemore, 2008). This period is also associated with increasing anxiety symptoms in autistic children (Vasa et al., 2013), for whom SCI differences, when coupled with increasing social demands, may confer anxiety disorder risk.
Methodological limitations also warrant consideration. Prior studies have relied upon anxiety subscales from broadband measures of psychopathology rather than a more comprehensive anxiety-specific measure. Reliance on a single-informant (parent) in these studies also leaves open the possibility that positive associations between anxiety and SCI were influenced by single-informant bias (Podsakoff et al., 2003). Using a multi-informant approach could reduce this possibility and shed light on children’s social–emotional functioning across contexts (De Los Reyes et al., 2015). Assessing how parent-reported anxiety relates to teacher-reported SCI behaviours may be especially valuable given that autistic children experience the symptoms and impact of anxiety across home and school (Adams & Emerson, 2021; Adams et al., 2019; Ambrose et al., 2021), and given teachers’ particular ability to observe SCI with varied peers throughout the day.
The role of executive functions
Executive function (EF) encompasses a set of cognitive processes that enable planning, forethought and goal-directed behaviour (Diamond, 2013; Miyake et al., 2000). Theoretical models divide EF into core processes of working memory, inhibition and cognitive flexibility (e.g. Miyake et al., 2000). The Behaviour Rating Inventory of Executive Functioning (BRIEF; Gioia et al., 2000) is a widely used measure of EF behaviours as they manifest in daily life, and assesses EF behaviours within two empirically derived indices: metacognition (an awareness of one’s own thought processes involving planning, organisation and working memory) and behavioural regulation (involving impulse control, cognitive flexibility and emotion regulation).
EF difficulties across the lifespan are common, but not universal among autistic people (e.g. Demetriou et al., 2018), and may account for some heterogeneity in functional outcomes. Although most studies examining EF behaviours in autistic children have relied upon parents’ perspectives, those employing both parent and teacher-report suggest EF challenges at home and school (Gentil-Gutiérrez et al., 2022; Tschida & Yerys, 2022). Cross-sectional research suggests informant-reported metacognitive abilities are related to academic performance, adaptive functioning, functional communication and social skills (Gardiner & Iarocci, 2018; Hutchison et al., 2020; Pugliese et al., 2015), while behavioural regulation difficulties covary with greater anxiety, depression, verbal communication challenges and SCI differences (Gardiner & Iarocci, 2018; Hollocks et al., 2014; Hutchison et al., 2020; Jones et al., 2018; Lawson et al., 2015; Leung et al., 2016). Longitudinal research among autistic children has also highlighted associations between earlier EF and later social communication abilities (Pellicano, 2013), play skills (Faja et al., 2016) and theory of mind (Kouklari et al., 2019).
Recent longitudinal research from the Pathways in Autism Spectrum Disorder study (Pathways; www.asdpathways.ca) has also examined the mechanistic role EF may play (i.e. as a mediator or moderator) in shaping mental health outcomes among autistic youth. Ameis et al. (2022) found that middle childhood EF difficulties measured via the BRIEF (specifically poorer behavioural regulation, but not metacognition) mediated the pathway from early childhood autism characteristics to adolescent externalising behaviours, while Carter Leno et al. (2022) found that EF abilities (also measured via the BRIEF) moderated the link between stressful life events and internalising symptoms: stressful life events were more strongly associated with later internalising difficulties among children with clinically elevated shifting difficulties compared with those with typical shifting abilities.
These findings suggest strong cross-sectional links between EF and both anxiety and SCI behaviours among autistic children. Longitudinal evidence suggests that EF may predict variability in SCI, and indicates the potential for EF to moderate outcomes in autistic youth’s social–emotional development. Similarly, EF may influence the developmental interplay between anxiety and SCI differences. For example, although SCI differences may provoke experiences of social rejection or victimisation (Pickard et al., 2018), cognitive flexibility and inhibitory/emotional control may facilitate self-acceptance or adaptation to one’s social environment, buffering against the development of anxiety. Alternatively, though anxiety can lead to behavioural rigidity and social withdrawal (S. W. White et al., 2014), stronger EF abilities may enable autistic children to cope with fears and worries more flexibly, reducing social withdrawal and subsequent loss of opportunities to develop social skills. Examining these possibilities may highlight cognitive mechanisms that could be targeted in early support programmes (e.g. Kenworthy et al., 2014).
The current study
Longitudinal investigations regarding the relationship between anxiety and SCI in autistic children are few, have produced mixed results and have relied upon samples with wide age ranges. Moreover, existing research has not examined EF as a moderator or focused on SCI in school settings, an important social context in preadolescence. We examined (1) whether parent-reported anxiety and teacher-reported SCI differences are associated over time in a community sample of autistic preadolescents, and (2) whether teacher-reported EF behaviours moderate these associations. We predicted anxiety and SCI differences would be positively associated (with no specific hypotheses about temporal directionality), with stronger associations in children with elevated EF challenges.
Method
Participants
Participants engaged in the Pathways in Autism Spectrum Disorder study (Pathways; www.asdpathways.ca), a prospective cohort study examining autistic children’s development beginning in 2005. Initially, 421 children were recruited to Phase 1 from five Canadian autism centres (Halifax, Montreal, Hamilton, Edmonton and Vancouver). Children met inclusion criteria if they (1) were between ages 2 and 5 years at enrolment, and (2) had a recent (within 4 months) diagnosis of autism based on Diagnostic and Statistical Manual of Mental Disorders (4th ed. text rev., DSM-IV-TR) criteria. Diagnoses were confirmed via the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2002) and Autism Diagnostic Inventory-Revised (ADI-R; Rutter et al., 2003). Children with diagnoses of cerebral palsy, neuromotor disorders, genetic or chromosomal abnormalities, and significant vision or hearing impairments were excluded, and only one child per family could participate. Caregivers were required to be verbally proficient in English or French. A total of 314 families entered Phase 2, when assessments occurred at 4 yearly time points from ages 7.7 to 10.7 (T5-T8). The current study analysed data collected during preadolescence: T7 (M age = 9.71 years, SD = 2.59 months) and T8 (M age = 10.76 years, SD = 2.93 months).
An inclusion/exclusion flowchart for the current study is presented in the Supplement (S1). In all, 157 participants (15% female; 85% male) were included in the analysis for Aim 1 (investigating associations between anxiety and SCI). To be included, participants needed to have (1) anxiety data at T7 and/or T8, (2) SCI data at T7 and/or T8 and (3) no more than mild impairments in intellectual ability or communicative functioning, as the validity of some anxiety measures has been questioned in children with notable cognitive or communicative difficulties (Kerns et al., 2021). This criterion was indexed by either a Full Scale IQ (FSIQ) score ⩾ 50 on the Wechsler Intelligence Scales for Children, 4th Edition (WISC-IV), or a Communication Domain standard score ⩾ 50 on the Vineland Adaptive Behaviour Scales, Second Edition (VABS-II). Eight participants had a VABS-II Communication standard score < 50 and did not complete the WISC, while 42 did not complete the VABS-II or the WISC; these 50 individuals were excluded from the sample.
To be included in analyses for Aim 2 (investigating EF as a moderator), participants needed to have EF data at T7 or T8, resulting in 149 participants included in analyses examining behavioural regulation as a moderator, and 148 included in analyses examining metacognition as a moderator (see below).
Ethical considerations
All participating families provided written informed consent. The study was approved by the University of Hamilton Integrated Research Ethics Board (REB; Project No. 04-353) and each participating site’s REB.
Measures
Cognitive ability and adaptive functioning
Demographic information was drawn from a study-specific parent questionnaire administered at T7 (or T8, if T7 data were missing). Overall intellectual ability and communicative functioning were measured at T6 using the WISC-IV (Wechsler, 2003) and the Communication Domain standard score of the parent-reported VABS-II (Sparrow et al., 2005).
Anxiety
Anxiety was measured at T7 and T8 via the parent-report Spence Children’s Anxiety Scale (SCAS; Spence, 1999). A parent-report measure was selected, as teachers may be more likely to underreport anxiety symptoms (Llanes et al., 2020). The SCAS is a 38-item measure including a total anxiety score and six subscales – Panic/Agoraphobia, Physical Injury fears, Separation Anxiety, Social Phobia, Obsessive-Compulsive Disorder and Generalised Anxiety. We used the total anxiety score, which demonstrated internal consistency at T7 (α = 0.91) and T8 (α = 0.89). Raw total scores ⩾ 24 are one standard deviation above the mean in a community sample (Nauta et al., 2004), and have been used as a cut-off for clinically elevated anxiety in prior autism research (Rodgers et al., 2012).
SCI
SCI behaviours were measured at T7 and T8 via the teacher-report Social Responsiveness Scale (SRS; Constantino & Gruber, 2005). Teacher-report was selected to capture SCI in school settings, where teachers can observe a child’s SCI behaviours among peers. The SRS is a 65-item questionnaire assessing autistic characteristics with demonstrated convergent validity with the ADOS and ADI-R (Charman et al., 2007) and discriminant validity against ratings of anxiety in autistic children (Renno & Wood, 2013). The second version of the SRS (SRS-2; Constantino & Gruber, 2012) uses the same 65 items, and derives two domain scores compatible with Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5) criteria for autism: SCI and Restricted Interests and Repetitive Behaviour. We computed an SCI domain score compatible with SRS-2, that had high internal consistency (T7 α = 0.93; T8 α = 0.94).
EF
EF was measured at T7 and T8 via the teacher-report BRIEF, an 86-item questionnaire that measures EF behaviours in real-world settings. Items map onto eight clinical scales comprising two broader indices: Behavioural Regulation Index (BRI; comprising Inhibit, Shift and Emotional Control scales) and Metacognitive Index (MI; comprising Initiate, Working Memory, Planning, Task Monitor and Organisation scales). Teacher-report was selected over parent-report as school may be more structured and less accommodating to cognitive challenges than home, and thus more likely to capture a child’s EF difficulties (Mares et al., 2007). Analyses were conducted using the BRI and MI to measure these aspects of EF separately. Internal consistency was high at both time points (BRI: T7 α = 0.92, T8 α = 0.94; MI: T7 α = 0.95, T8: α = 0.96).
Covariates
Recruitment site, sex assigned at birth, FSIQ and adaptive communication were included as covariates in all models, regressed on anxiety and SCI variables at T7 and T8. Research suggests sex differences in SCI (Constantino & Gruber, 2012) and anxiety (Gotham et al., 2015), and enhanced detection of some anxiety symptoms in autistic children with stronger cognitive or communicative abilities (Gotham et al., 2015; Kerns et al., 2021).
Data analysis
Preliminary analyses (examining normality of outcome variables, selective attrition, missing data and potential outliers) are presented in the Supplemental material (S2-S5). Participants who were included (N = 157) versus excluded (N = 157) among the 314 families entering Phase 2 were compared across demographic (site, sex, household income) and analysis variables (anxiety, SCI, EF) available at the beginning of Phase 2 (T5). The proportion of included versus excluded participants differed across study sites. No other differences were found on demographic or analysis variables.
Cross-lagged models
Analyses were conducted using the Lavaan package in R (Rosseel, 2012) and used a cross-lagged, structural equation modelling design, following previous longitudinal studies of anxiety and SCI (Duvekot et al., 2018; Pickard et al., 2017). Continuous variables (WISC, VABS-II, SRS and SCAS scores) were mean-centred. Full information maximum likelihood was used to account for missing data. Maximum likelihood with robust estimation of standard errors was used to account for non-normal distribution of T7 and T8 anxiety scores.
Whole sample analysis
To assess longitudinal associations between anxiety and SCI differences in the full sample, a saturated model was run, allowing all variables to freely covary within time points.
Multigroup moderation analyses
Multigroup models testing EF as a moderator were based on BRIEF scores at T7 (BRI: n = 113; MI: n = 109), or T8 if T7 data were missing (BRI: n = 36; MI: n = 39). Participants missing BRIEF data at T7 and T8 (BRI: n = 8; MI: n = 9) could not be classified and were excluded from this set of analyses. Correlations between T7 and T8 scores were moderate to large (BRI: r = 0.62, p < 0.001; MI: r = 0.42, p < 0.001), so T8 scores were considered an acceptable substitution for missing T7 scores. As MI correlations were moderate, we ran the MI model without substitutions (n = 118) as a sensitivity test; the pattern and significance of the findings remained the same. Individuals with T-scores ⩾ 70 on the BRI/MI, indicating clinically elevated difficulties (Gioia et al., 2000), formed the Clinical BRI (n = 80) and Clinical MI (n = 70) groups. Those scoring < 70 formed the Non-Clinical BRI (n = 69) Non-Clinical MI (n = 78) groups. There was considerable, but not complete, overlap between BRI and MI groups: 51 participants were in both the Clinical BRI and Clinical MI groups, while 50 participants were in both the Non-Clinical BRI and Non-Clinical MI groups. BRIEF clinical cutoffs were based on normative data from a general population sample not ascertained for neurodevelopmental conditions (Gioia et al., 2000), and therefore children in the Clinical BRI/MI groups were considered to demonstrate elevated EF difficulties relative to neurotypical children.
To investigate whether EF moderated associations between anxiety and SCI differences, the saturated model was first run in the two BRI groups. In a second model, equality constraints were applied to the cross-lagged path estimate for T7 anxiety predicting T8 SCI differences. In a third model, equality constraints were applied to the cross-lagged path estimate for T7 SCI differences predicting T8 anxiety. Relative model fit in the saturated versus each of the constrained models was compared, using the Satorra–Bentler scaled chi-square difference statistic (Satorra & Bentler, 2001), with significant differences indicating a moderating effect of behavioural regulation on the relevant cross-lagged pathway. The multigroup analysis was then repeated in the two MI groups to examine metacognition as a moderator.
Model fit statistics and adjusting for multiple comparisons
Fit for constrained multigroup models was indicated by the comparative fit index (CFI), root mean square error of approximation (RMSEA) and standardised root mean residual (SRMR). A Bonferroni correction was applied to the path coefficients within each saturated model (six coefficients per model; significance set at p < 0.008). To account for multiple comparisons between models in the moderation analyses (4 sets of models compared), statistical significance was set at p < 0.013.
Community involvement
In 2005, parents, advocates, researchers and practitioners met to establish the aims of the Pathways study. Community members continue to engage in aspects of Pathways, including providing feedback on study protocols and research aims, and informing the design of Phase 2. Community members were not directly involved in shaping the research questions, analytic approach and interpretation of results for the current study.
Results
Descriptive analyses
Table 1 presents demographic information and summary statistics for analysed variables. At T7 and T8, 22% and 21% of children respectively exceeded the suggested clinical cut-off for SCAS total anxiety score. Participants in the Clinical BRI and MI groups had significantly higher SCI differences per the SRS than those in the Non-Clinical groups (S4). Across the whole sample, anxiety and SCI differences significantly decreased from T7 to T8; however, the decrease in anxiety was significant only in the Clinical BRI group, while the decrease in SCI differences was significant only in the Clinical BRI and MI groups (S5).
Demographic characteristics and key variables.

WISC-FSIQ: Wechsler Intelligence Scale for Children-Full Scale IQ (standard score); VABS-Communication: Vineland Adaptive Behaviour Scales-Communication Domain (standard score); SCAS Total: Spence Children’s Anxiety Scale-Total (raw score); SRS SCI: Social Responsiveness Scale-Social Communication Index (raw score); BRIEF BRI: Behaviour Inventory Rating of Executive Function-Behavioural Regulation Index (t-score); BRIEF MI: Behaviour Inventory Rating of Executive Function-Metacognitive Index (t-score).
Whole sample analysis
Autoregressive paths for anxiety (B = 0.764, 95% CI = [0.640, 0.889], β = 0.875, p < 0.001) and SCI differences (B = 0.489, 95% CI = [0.298, 0.680], β = 0.491, p < 0.001) were significant. Covariances between anxiety and SCI differences were non-significant at T7 (B = 38.435, 95% CI = [−11.608, 88.478], β = 0.151, p = 0.132) and T8 (B = 15.267, 95% CI = [−7.126, 37.660], β = 0.158, p = 0.181). The cross-lagged pathway from T7 SCI differences to T8 anxiety was non-significant (B = 0.006, 95% CI = [−0.045, .056], β = 0.012, p = 0.830), as was the cross-lagged pathway from T7 anxiety to T8 SCI differences (B = −0.225, 95% CI = [−0.507 0.057], β = −0.117, p = 0.118).
Moderation analyses
Behavioural regulation
When the sample was split into BRI groups (Figure 1 and Supplemental Figure S6), the pathway from T7 SCI to T8 anxiety was non-significant in both groups. The pathway from T7 anxiety to T8 SCI differences was non-significant in the Non-Clinical BRI group, but significant and negative in the Clinical BRI group (B = −0.500, 95% CI = [−0.853, −0.147], β = −0.288, p = 0.005), such that higher T7 anxiety was associated with lower T8 SCI differences for participants with clinically elevated BRI difficulties. Fit for the model with constrained T7 SCI to T8 anxiety paths was excellent (CFI = 1.000, RMSEA = 0.000, SRMR = 0.001), and did not differ significantly from the saturated model (Δχ2(1) = 0.023, p = 0.879). Fit for the model with constrained T7 anxiety to T8 SCI paths was poor based on RMSEA as an indicator (CFI = 0.989, RMSEA = 0.233, SRMR = 0.015). Relative fit for this model was significantly poorer than for the saturated model (Δχ2(1) = 10.466, p = 0.001), indicating a moderating effect of BRI grouping on this lagged pathway (see Figure 2).

Associations between parent-reported anxiety and teacher-reported SCI differences by teacher-reported behavioural regulation ability.
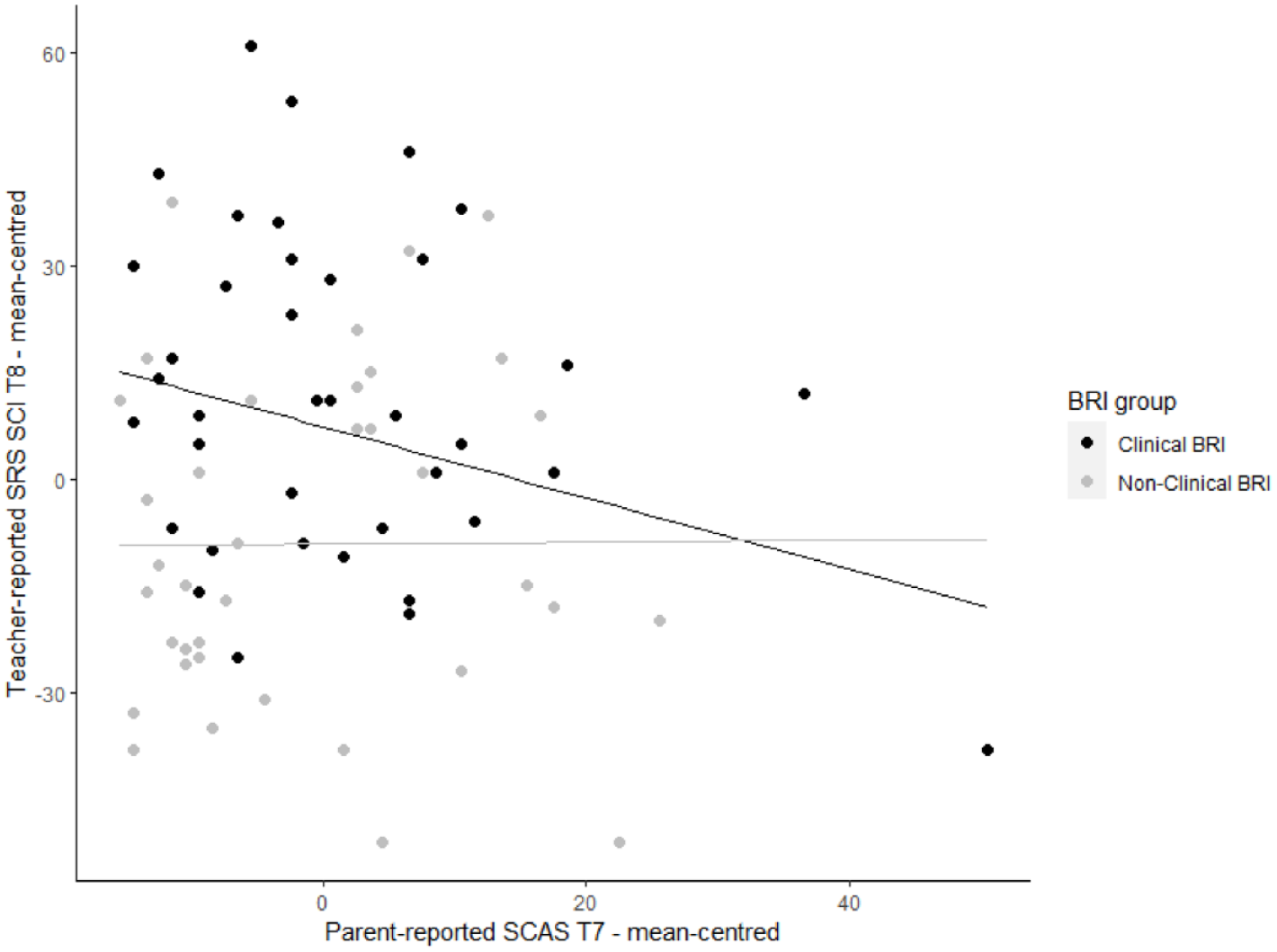
Model-predicted relationship between T7 parent-reported anxiety and T8 teacher-reported SCI difficulties, in the clinical and non-clinical BRI groups.
Metacognition
When the sample was split into MI groups (Figure 3 and Supplemental Figure S6), the pathway from T7 SCI differences to T8 anxiety was non-significant in both groups, as was the pathway from T7 anxiety to T8 SCI differences. Fit for the model with constrained T7 SCI to T8 anxiety pathways was excellent (CFI = 1.000, RMSEA = 0.000, SRMR = 0.002), and did not differ significantly from the saturated model (Δχ2(1) = 0.048, p = 0.827). Similarly, fit for the model with constrained T7 anxiety to T8 SCI pathways was excellent (CFI = 1.000, RMSEA = 0.000, SRMR = 0.001) and did not differ significantly from the saturated model (Δχ2(1) = 0.110, p = 0.740), indicating that MI grouping did not moderate either pathway.

Associations between parent-reported anxiety and teacher-reported SCI differences by teacher-reported metacognitive ability.
Post hoc analyses
Post hoc analyses were conducted using specific BRI subdomains as moderators (S7). Inhibition and Emotion Control, but not Shifting abilities, moderated the negative association between T7 anxiety and T8 SCI differences. In addition, to test the specificity of associations between anxiety and SCI differences (as opposed to behavioural differences more broadly), analyses were run, replacing the SRS’s SCI index score with the Restricted and Repetitive Behaviours (RRB) index score (S8). T7 anxiety did not significantly predict T8 RRBs in the full sample or in any of the EF groups, suggesting a specific association between T7 anxiety and T8 SCI differences among children with behavioural regulation challenges.
Discussion
This study aimed to clarify how parent-reported anxiety and teacher-reported SCI differences are related over time for autistic preadolescents, and whether these relationships are contingent upon a child’s teacher-reported EF behaviours. Contrary to our first hypothesis, in the full sample, higher levels of parent-reported anxiety did not predict greater teacher-reported SCI differences 1 year later, or vice versa. This contrasts with findings reported by Duvekot et al. (2018) – who found anxiety predicted greater SCI differences over time – as well as meta-analytic findings of a negative association between anxiety and social competence (Adams et al., 2023). Below, we propose several possible explanations.
This study’s participants were drawn from a prospective cohort of autistic children diagnosed before age 5 years, not ascertained for mental health concerns and with a likely broader spectrum of anxiety severity (just over one-fifth with clinically elevated anxiety problems) relative to Duvekot et al.’s clinically referred sample. Our findings align more with Teh et al. (2017), who did not find longitudinal associations between parent-reported SCI and anxiety in a community sample of autistic youth – suggesting relationships between anxiety and SCI may depend on anxiety levels within study samples. Furthermore, our use of multiple informants likely reduced measurement error via shared-method variance (Podsakoff et al., 2003). At the same time, discrepancies between our cross-informant model and prior single-informant findings may reflect true situational variations in children’s behaviour. Research indicates low parent-teacher agreement in reporting autistic children’s anxiety (Adams et al., 2018; Llanes et al., 2020), which may reflect differences in children’s experiences and expressions of anxiety across settings (De Los Reyes et al., 2015). Different associations might be observed if teacher-reported anxiety or parent-report SCI were used, and this should be investigated in future work. Third, we focused on preadolescence, and evidence suggests that the association between anxiety and SCI weakens with age – perhaps due to changes in the phenomenology and outcomes of anxiety as children enter adolescence (Adams et al., 2023). It is possible that social anxiety, which becomes more prominent during preadolescence, relates to SCI in a different manner compared with forms of anxiety more common in younger children (e.g. separation anxiety, phobias). Specifically, social anxiety may link to greater SCI differences for some (e.g. SCI differences precede negative social experiences, and subsequent social fear and withdrawal), but fewer SCI differences for others (e.g. camouflaging, which may result from and exacerbate social anxiety, could lead to decreasing SCI differences; Perry et al., 2022). When combined, these distinct pathways could weaken the overall relationship between anxiety and SCI during this developmental period (Adams et al., 2023), a hypothesis that also requires further study.
Regarding our second aim, higher levels of parent-reported anxiety were associated with fewer teacher-reported SCI differences over time, but only among children with clinically elevated behavioural dysregulation relative to general population norms. By contrast, metacognition was not a significant moderator, suggesting the specificity of behavioural regulation as a moderator of behavioural outcomes, consistent with prior research (Ameis et al., 2022). One possible explanation for our findings is that, in line with evolutionary theories (Bateson et al., 2011), anxiety may dovetail with increased behavioural inhibition. Although anxiety is linked to self-regulation difficulties among non-autistic children (Eysenck et al., 2007), evidence also suggests stronger inhibitory control predicts greater anxiety among behaviourally inhibited children (L. K. White et al., 2011). Moreover, children with attention-deficit/hyperactivity disorder (ADHD) and co-occurring anxiety disorders have been found to perform better on inhibitory control tasks compared with those with ADHD alone (Menghini et al., 2018; Yurtbaşı et al., 2018). Similarly, among children with elevated familial likelihood for autism, anxiety has been associated with stronger inhibitory control (Godoy et al., 2021). It is possible that for autistic children with significant behavioural dysregulation, very limited anxiety could go hand-in-hand with social disinhibition, leading to more obvious SCI differences and subsequent social challenges as children approach adolescence. Among these children, some anxiety may accompany or enable greater self-regulation. Congruently, post hoc analyses demonstrated that inhibitory and emotional control (as opposed to shifting) moderated the relationship between anxiety and SCI differences, lending some support to this proposed mechanism.
Within this explanation, anxiety could signal heightened awareness and observation of neurotypical social norms and expectations. Indeed, research has found that autistic youth with elevated social anxiety tend to demonstrate greater empathy and social understanding compared with their less socially anxious peers (e.g. Hunsche et al., 2022; Niditch et al., 2012). Our use of a broadband measure of anxiety precludes evaluating this interpretation; however, future research using social anxiety measures may delineate mechanisms by which social awareness and/or anxiety may relate to fewer SCI differences for autistic children. Although fewer SCI differences were not associated with increasing anxiety in this study, extending this research to adolescence will be a critical next step. It is possible that as social demands intensify during adolescence, even subtle SCI differences may lead to negative social experiences (e.g. misunderstandings between peers, exclusion), and increased anxiety or depression – akin to findings reported by Pickard et al. (2017), who studied youth into their teenage years. Moreover, for some, pressure to suppress one’s SCI style over time could further increase anxiety, despite apparent decreases in SCI differences (Livingston et al., 2019). Future work should move beyond parent- or teacher-observed SCI behaviours only, to incorporate self-report and consider how SCI differences may shape mental health outcomes via one’s social experiences. Importantly, this work should entertain the potential for both positive (e.g. increasing connection; Livingston & Happé, 2017) and detrimental outcomes (e.g. camouflaging that compromises sense of self, victimisation, social confusion, and loneliness; Beck et al., 2020; Kerns et al., 2015, 2022; Schiltz et al., 2021).
An alternative explanation is that anxiety may not contribute directly to decreasing SCI differences, but instead correlate with additional (unmeasured) mechanisms. Developmental maturation processes involving diverse neural, behavioural and environmental elements (Soto-Icaza et al., 2015) may bring about increasing awareness of, and adaptation to, one’s environment, which could result in the emergence of anxiety and subsequent development of social skills. Notably, children with ADHD have been found to demonstrate delayed cortical growth trajectories, achieving peak cortical thickness in preadolescence (Shaw et al., 2007). For participants with significant behavioural regulation difficulties (who likely had elevated ADHD symptoms, although this was not assessed), delayed cortical maturation could lead to the emergence of greater attentional capabilities, vigilance to one’s surroundings and developing social skills during preadolescence. Indeed, preliminary analyses revealed that the Clinical BRI group demonstrated greater development in SCI from ages 9 to 10 years. Although regression to the mean could partially account for this change, the whole sample showed changing SCI scores, suggesting this period may be important for social development and growth. Investigating neurocognitive development, and whether its timing explains the emergence of anxiety and SCI skills, are needed to support this interpretation.
Limitations and future directions
The Pathways study included early-diagnosed children with autism without co-occurring sensory, neurological or genetic conditions. As such, our findings may not generalise to autistic children with these conditions (which may influence clinical presentation; Ziats et al., 2021) or those later-diagnosed. Relatedly, our sample included youth with no more than mild cognitive or communicative impairments, and findings may not apply to those with moderate to severe intellectual disability, who represent a considerable minority of autistic children yet are often underrepresented in research (Russell et al., 2019). Our sample also included relatively few individuals assigned female at birth, and we could not quantify sex or gender diversity given that only male/female options were queried at time of data collection. Finally, most caregivers in our sample were white. Future research should address these limitations by examining these questions in samples with greater racial and ethnic diversity, intellectual disability (using appropriate measures), and quantifiable sex and gender diversity. This is particularly important given developmental and gender differences in the presentation of anxiety and SCI differences (Kerns et al., 2021; Sedgewick et al., 2020), as well as recent calls to investigate the health needs of gender diverse autistic people (Mittertreiner et al., 2024) and for research to better reflect the diversity of youth in need of clinical care.
Future multi-informant work should seek to disentangle the effects of informant perspectives and contextual variation of behaviour, in order to establish whether and how associations among anxiety, SCI, and EF vary across different settings. Relatedly, parents’ anxiety may have influenced their reporting of their child’s anxiety (Burrows et al., 2018). Multiple factors (including shared environment and genetic susceptibility) likely contribute to the relationship between parents’ and children’s mental health (e.g. Baker et al., 2021; Woodman et al., 2015), and future research, ideally incorporating parent- and self-reports, could investigate this. Anxiety was highly stable, particularly in the non-clinical EF groups, which may have suppressed some cross-lagged effects. Our findings may apply to standard expressions of anxiety measured by the SCAS – which was developed for non-autistic children – but not distinct expressions of anxiety (e.g. fears related to social confusion or minor change) that commonly present in autistic youth (Kerns et al., 2014, 2021). SRS scores likely capture not only SCI differences, but also aspects of broader externalising behaviours (Hus et al., 2013). This may be particularly relevant to the classroom, where teachers are more likely to detect and report overt (e.g. intrusive) as opposed to subtle (e.g. withdrawn) behaviours. Although sensitivity analyses indicate specific links between anxiety and SCI behaviours (as opposed to broader behavioural differences), measuring SCI with more specific measures (e.g. the ADI-R, ADOS) could provide greater nuance and precision. Relatedly, although using the BRIEF, which measures children’s application of EF skills across everyday contexts, increased our study’s accessibility and clinical utility, objective measures may better disentangle specific cognitive components of EF (McAuley et al., 2010; Toplak et al., 2013) from other factors (e.g. ADHD symptomatology, emotion dysregulation, motivation). In future research, comprehensive assessment of EF that incorporates informant-report and objective measures could further illuminate our findings (Isquith et al., 2013). Moreover, the number of children classified as having clinically elevated EF difficulties was based on a general population normative sample. Developing and also considering norms based on autistic populations in future research could offer important nuance regarding EF differences within autistic children and the extent to which use of general population norms may overestimate or oversimplify difficulties experienced.
Our findings captured a brief snapshot of a likely complex and ongoing developmental picture. Modelling joint trajectories of anxiety, SCI and EF may build upon this study by elucidating whether these constructs develop in tandem, or whether patterns of development in one predict outcomes in another. Finally, future research should consider other potential mechanisms (e.g. language skills) in this unfolding association – although we accounted for parent-reported adaptive communication abilities, including objectively assessed language abilities could provide greater insight into the potential role of language: one possibility is that children with greater verbal abilities more readily communicate their anxiety (leading to higher anxiety scores), and adapt to their social environment (leading to decreasing SCI differences).
Clinical implications and conclusions
In this community sample of autistic preadolescents, less anxiety was associated with more SCI differences one year later, but only among those with clinically elevated behavioural dysregulation. Our work highlights the importance of investigating the full spectrum of anxiety – as an important human emotion that can also have detrimental mental health impacts – and how its interactions with neurocognitive characteristics may shape autistic children’s social development. For autistic children with elevated behavioural dysregulation, minimal parent-reported anxiety may signal a need for increasing SCI support at school, which could foster social connectedness during the transition to adolescence. Conversely, among this group of children, the presence of some anxiety may indicate a developing awareness of neurotypical social expectations and/or an emerging ability to self-regulate; however, the potential masking of one’s SCI style, and associated costs to self-esteem and mental health, should be considered. Developing a more precise mechanistic understanding of how this association unfolds may be relevant for enhancing support of anxiety and social connectedness. For example, it may be important for anxiety interventions to help autistic youth (particularly those presenting with behavioural dysregulation) to recognise and reconcile both adaptive and maladaptive aspects of anxiety. This may enable autistic children to harness anxiety’s guiding function (e.g. noticing and responding to others’ emotions), while also detecting when it becomes impairing (e.g. diminishing self-esteem). Incorporating evidence-based interventions for EF and emotion regulation skills may also be worthwhile (e.g. Weiss et al., 2018) to support autistic children in developing coping strategies that draw upon self-regulation rather than fear. In sum, research examining how different forms of anxiety relate to SCI across contexts, and over adolescence, may enhance clinical care for autistic individuals by providing more individualised approaches to support both social and emotional well-being.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241296589 – Supplemental material for Longitudinal associations between autistic children’s anxiety and social communication differences
Supplemental material, sj-docx-1-aut-10.1177_13623613241296589 for Longitudinal associations between autistic children’s anxiety and social communication differences by Elise Ng-Cordell, Hannah Pickard, Rachael Bedford, Annie Richard, Anat Zaidman-Zait, Lonnie Zwaigenbaum, Eric Duku, Teresa Bennett, Stelios Georgiades, Isabel M Smith, Tracy Vaillancourt, Peter Szatmari, Mayada Elsabbagh and Connor M Kerns in Autism
Footnotes
Acknowledgements
The authors thank all the children and families who participated in the Pathways in ASD Study. They also acknowledge the Pathways in ASD Study Team (research staff members and trainees) who contributed to this study.
Correction (December 2024):
Article has been updated to correct minor formatting errors in Table 1 and captions of Figures 2 and 3.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Pathways in ASD Study was supported by the Canadian Institutes for Health Research (grant nos HDF-70333 and FDN 93621), Kids Brain Health Network (formerly NeuroDevNet), Autism Speaks, the Government of British Columbia, Alberta Innovates Health Solutions and the Sinneave Family Foundation. E.N.C. was supported by a Cordula and Gunther Paetzold Fellowship and a Killam Doctoral Scholarship from the University of British Columbia. C.M.K. was supported by a Michael Smith Foundation Scholars Award.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.