
Abstract
Caregivers can experience significant challenges following their child’s autism diagnosis and often seek informational, relational and emotional support. Post-diagnostic support for caregivers has received relatively little research attention and represents a significant gap in the international evidence base. We used an iterative codesign process to develop a manualised group-based post-diagnostic programme, Empower-Autism, with associated theory of change, to address the diverse needs of caregivers and improve caregiver mental health. Empower-Autism blended evidence-informed autism psychoeducation with psychotherapeutic components grounded in Acceptance and Commitment Therapy. Three feasibility groups (two in-person and one online) were delivered with 29 clinically referred, socioeconomically diverse caregivers. We evaluated feasibility and acceptability through quantitative attendance and satisfaction data, and thematic analysis of detailed interviews with 17 participants and 5 facilitators. Attendance was satisfactory (76% participants meeting prespecified criteria) and programme satisfaction was good. Qualitative analysis suggested the programme was acceptable and accessible, and highlighted the areas for improvement. Caregivers described perceived benefits from the programme, including improved wellbeing, social connection, autism positivity and more attuned parenting. Empower-Autism is being evaluated within a large randomised controlled trial and, if shown to be clinically and cost-effective, this programme will fill an identified evidence gap in the United Kingdom and global provision.
Lay Abstract
Parents and carers face many challenges following their child’s autism diagnosis. They often look for information, and social and emotional support. There has been relatively little research into how best to provide this support and this means that there is no evidence to guide the delivery of services. Studies have suggested that an approach called Acceptance and Commitment Therapy can help parents and carers with their adjustment and emotional wellbeing.
This article describes the development of a new group-based programme to address the diverse needs of caregivers after their child’s autism diagnosis. The new programme was developed with caregivers, autistic people and professionals. It was called Empower-Autism and contained lots of information about autism and strategies to support autistic children, alongside therapeutic aspects based on Acceptance and Commitment Therapy. The programme was delivered to 29 parents/carers in three groups. Attendance at the groups was satisfactory. Both parents/carers and facilitators liked and valued the programme and found it accessible. They made suggestions for improvements. After the programme, parents and carers described improved wellbeing. They felt more positive and more connected to other people. They also described parenting their child in a more informed and sensitive way.
The new programme is being tested within a large clinical trial. If there are positive results, the programme could be recommended for delivery and this would address an important gap in evidence-based practice.
Introduction
The period following a child’s autism diagnosis is a time of adjustment for families. Between 20% and 50% of caregivers show clinically significant levels of mental health difficulty in this period and on an ongoing basis (Casey et al., 2012; Lai et al., 2015; Salomone et al., 2018). Good caregiver mental health is vital in its own right but also because it is intricately linked to child’s wellbeing in autistic children (Yorke et al., 2018). A parent’s own sense of resolution around the diagnosis is linked to attunement in the parent–child relationship (Naicker et al., 2023), mediating the association between child’s behaviour and parent’s mental ill-health (Jones et al., 2018). Parental resolution and longer-term coping are important for effective uptake of parent-mediated interventions on which much service delivery relies (Jurek et al., 2023).
Caregiver mental health needs are unquestionably important but also diverse and often complex. A systematic review of caregiver experiences emphasised three distinct areas of post-diagnostic need: emotional, relational and informational (Legg & Tickle, 2019). Emotional needs include processing initial responses to the diagnosis which might not only involve relief and validation but also shock, anxiety and disorientation (Legg & Tickle, 2019). In the longer term, caregivers often need to develop stress management resources in the face of greater parenting complexities and the demands of navigating complex support systems and fighting for provision (Galpin et al., 2018). Relational needs concern social connection and validation and protecting against isolation, judgement and stigma (e.g. Kinnear et al., 2016). Many caregivers also have informational needs, wanting to understand better their child’s world, how to parent their child and know how to find appropriate information and support. Each of these areas can impact on short- and long-term caregiver mental health, and the promotion of mental health therefore requires a holistic and multifaceted approach, taking into account the multiple unmet needs and potential contributors to (poor) mental health to bring enduring benefits for caregivers, their autistic children and wider families.
The provision of evidence-based autism post-diagnostic support is a priority for the UK health system (NHS, 2019). Support to help caregivers better understand and support their autistic child is also a community priority for research and service provision (James Lind Alliance, 2016; Waddington et al., 2024). Current post-diagnostic provision is patchy (Rogers et al., 2016) and a source of dissatisfaction to both professionals and caregivers (Crane et al., 2016; Crane et al., 2018; Rogers et al., 2016). Caregiver psychoeducation is among the most commonly used autism intervention (Rogers et al., 2016) and is clinically intuitive. There are many local, national and international initiatives to develop and deliver generic psychoeducation packages, some of which have evidence of acceptability or observational evidence suggestive of positive outcomes (e.g. Dawson-Squibb et al., 2019; Salomone et al., 2022; Stuttard et al., 2016). Despite this, such interventions have received relatively little research attention and this remains a significant gap in the international literature. Moreover, while many psychoeducational packages aim to address informational and some relational aspects, caregiver’s emotional needs are often overlooked and therefore important determinants of mental health remain unaddressed.
Somewhat separate to the literature on post-diagnostic support, there is growing interest in the relevance of psychotherapeutic approaches to promote the mental health and wellbeing of caregivers of autistic children. Recent reviews (Bourke-Taylor et al., 2021; Lichtlé et al., 2020) concluded that cognitive–behavioural methods, mindfulness, and Acceptance and Commitment Therapy (ACT) can improve parenting stress, wellbeing and mental health. ACT is a relatively new acceptance and mindfulness-oriented ‘third wave’ cognitive–behavioural approach that aims to increase psychological flexibility (Hayes et al., 2012). Several clinical and research teams have recognised the utility of ACT to caregivers of autistic children in terms of adapting to new life circumstances, processing complex thoughts and emotions, and coping with long-term stress and uncertainty (Coyne et al., 2020). Recent small-scale trials have signalled positive effects on parental stress (Marino et al., 2021) and depression and family distress (Maughan et al., 2024). A recent systematic review by Juvin et al. (2022) concluded that the approach may be helpful to caregivers of autistic children but that larger rigorous tests of effectiveness were needed. To date, no such tests have been reported, although relevant trials are ongoing (Holmberg Bergman et al., 2023; Leadbitter et al., 2022; McLay et al., 2023; Whittingham et al., 2020).
This study is part of a larger programme of work (Leadbitter et al., 2022; ISRCTN: 45412843) aiming to address this key evidence gap by developing and robustly evaluating a novel manualised group-based programme, blending autism psychoeducation and psychotherapeutic support based on ACT, to address caregiver informational, relational and emotional needs and thereby improve their mental health. This article reports the first two of the four phases critical when developing and evaluating complex interventions (O’Cathain et al., 2019; Skivington et al., 2021): the development phase and feasibility phase. This study had two objectives:
To evaluate the feasibility and acceptability of the programme to participants and facilitators through the quantitative assessment of attendance levels and participant- and facilitator-rated post-session satisfaction ratings. Acceptable levels were pre-specified (https://www.isrctn.com/ISRCTNISRCTN45412843): acceptable attendance ⩾ 70% consented participants attending ⩾ 60% sessions; acceptable satisfaction ⩾ 70% sessions rated as ‘satisfied/very satisfied’.
To explore qualitatively: (a) the acceptability of the programme to facilitators and participants; (b) the accessibility of the programme to facilitators and participants and (c) whether there were perceived benefits to participants. These provider and caregiver perspectives were then used to inform protocol refinements.
Methods
Ethics
Ethical approval was granted by the UK Health Research Authority (ID: 268914).
Community involvement
Community members, including caregivers of autistic children and autistic adults, were involved throughout the development phase (reported below). An advisory group of caregivers (including autistic caregivers) and a steering committee involving two caregiver representatives influenced decision-making across the wider project.
Development of programme theory and protocol
The programme was a priori designed to be deliverable and cost-effective within a publicly funded health system. It therefore needed to be (a) group-based and of relatively low intensity; (b) deliverable by facilitators from the range of professional backgrounds typically employed within autism services (e.g. speech and language therapy, psychology, paediatrics, social work, occupational therapy); (c) suitable for, and relevant to, all caregivers of children and young people aged 2–15 years with diverse autism presentations. In response to the COVID-19 pandemic, an additional specification was added, ensuring the programme’s feasibility for both face-to-face and remote delivery via videoconferencing.
Guided by established principles for developing complex interventions (O’Cathain et al., 2019; Skivington et al., 2021), we adopted Theory of Change (De Silva et al., 2014) as a framework to identify and articulate the background context and assumptions, interventional components, and theoretical mechanisms of change and short- and long-term outcomes. A multi-stage development process was undertaken, as shown in Figure 1. A Theory of Change diagram and the prototypes of intervention guidelines, slides and resources were developed and refined throughout this process.
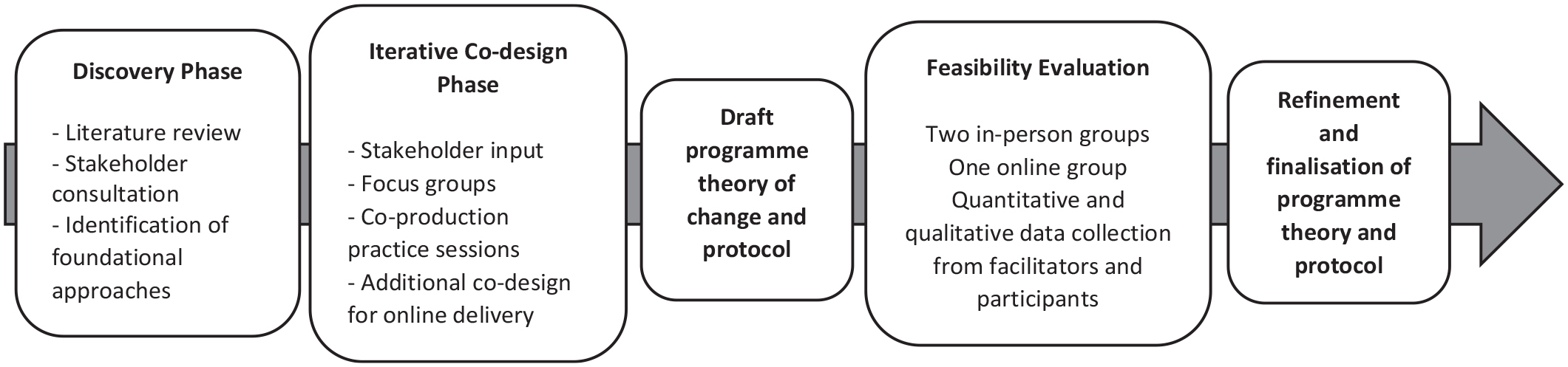
Process of the development of the theory of change and programme protocol.
Discovery phase
Literature review: This examined articles that documented parental experiences of autism diagnosis for their child or that assessed the acceptability or effectiveness of psychoeducational and psychotherapeutic approaches for caregivers of autistic children.
Stakeholder consultation: Initial consultation was undertaken with 28 caregivers of autistic children and an advisory group of three parent representatives. Perspectives were sought on different types of post-diagnostic support and their views and concerns around blending psychoeducation and psychotherapeutic support within one programme. We also consulted with a range of professionals working within autism teams about current practice and priorities.
Identification of foundational approaches: The literature review and stakeholder consultation enabled us to identify two antecedent approaches to act as a foundation and guide further development:
The Manchester Autism Post-Diagnostic Workshop, developed and delivered within a multi-agency autism diagnostic team over 10 years and modified iteratively in response to participant and professional feedback. Published evaluations reported high attendance and excellent feasibility and acceptability (Flynn et al., 2010; Mockett et al., 2011).
A brief manualised ACT programme, developed by clinical researchers at the University of Queensland and delivered with caregivers of children diagnosed with cerebral palsy and brain injury with good promise (Brown et al., 2015; Whittingham et al., 2016), and with caregivers of autistic children with good acceptability (K. Sofronoff, personal communication, November 24, 2017). We selected ACT as an approach because of its growing evidence base for effectiveness in adult mental health (e.g. A-tjak et al., 2015) and its particular relevance to the psychological and emotional task faced by caregivers of children newly diagnosed as autistic due to its focus on: psychological acceptance – validating emotions and cognitions rather than seeking to change them – important when adjusting to a new life circumstance; mindfulness techniques, known to be successful in managing day-to-day stressors and reducing caregiver mental health difficulties (Conner & White, 2014); and a ‘core values’ focus that may help re-assert parenting values unsettled by realisation of the child’s neurodivergence and the associated contextual challenges.
Iterative codesign phase
A detailed and iterative codesign process was undertaken, drawing on the principles and processes of experience-based codesign (Donetto et al., 2015) to further develop the approaches and integrate them into one coherent programme. Key components of this phase were as follows.
Stakeholder input: Input from a range of stakeholder representatives: caregivers of autistic children, autistic adults, ACT experts, a range of health, education and third sector professionals, including those who had delivered the foundational approaches and other similar interventions.
Focus groups: Four focus groups were held involving 20 people with personal, family or professional expertise recruited via social media and local networks.
Co-production practice sessions: Team members ran ‘mock’ sessions with four parent volunteers (three non-autistic and one autistic) to pilot session content and activities and modify according to feedback.
These codesign activities centred on a range of topics, most notably as follows:
The diversity of caregivers; the many factors contributing to poor mental health in caregivers; related potential pathways to improved mental health and how to provide ‘something for everyone’. This enabled specification of (a) seven change mechanisms which we theorised would lead to improved mental health across a diversity of caregivers and (b) programme components that would impact on these mechanisms (see Figure 2). For example, we identified that an autism/neurodiversity-positive approach could lead to increased acceptance and hope, so embedded this within the manualised ethos. We also recognised that insight and empathy with one’s autistic child were key change mechanisms and therefore ensured content engendered not just knowledge and skills but also the ability for parents to experience the world from their child’s point of view.
The diversity of children’s presentations and how to provide ‘something for everyone’. This led to (a) manualised decision points allowing facilitators to tailor content to the needs of their particular group; (b) time and space to apply learning to one’s own child; (c) content offered with a ‘take it or leave it’ approach, recognising that not everything would be relevant to everyone.
Refining the content and timing of all components. For example, discussion informed the decision to run five 3-h sessions as, while a range of opinions were expressed, this was the option preferred by a majority; the decision to have the ACT-specific workshop in Session 4, once the group had formed and established.
Exploring options for extended learning and peer support, and anticipating potential barriers to access. From this, we decided to include between-session activities which promoted reflection and trying out new ideas within daily life, but not to expect between-session reading or more formal ‘homework’.
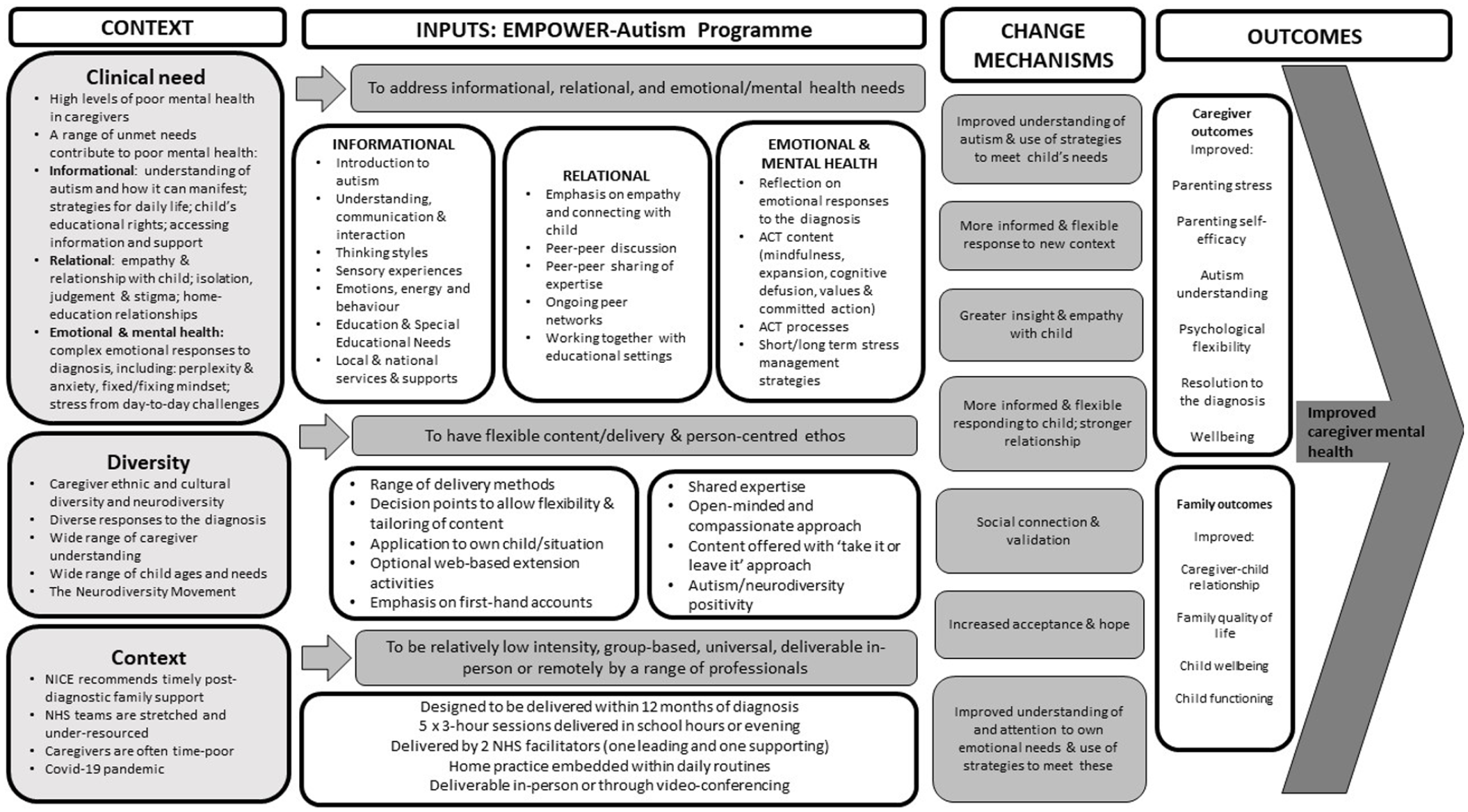
Theory of change of Empower-Autism programme.
Additional codesign in move to online delivery
In response to the COVID-19 pandemic, further codesign explored online delivery through videoconferencing. This included reviewing the literature around best practice for online delivery and discussion with team members, an ACT consultant, colleagues already running online groups and the advisory group. Careful consideration was given to the number and length of sessions; competencies and confidence of facilitators; practicalities of online delivery; supporting peer relationships and responding to strong emotions over videoconferencing. Guidelines were produced for participants. An additional practice run was conducted with three new parent volunteers (all non-autistic) to test online delivery of programme. Feedback was collected and contributed to protocols for online delivery.
Draft programme theory of change and programme protocol
These were then produced. It is important to note that these were further refined and finalised after the feasibility evaluation phase. The theory of change is provided in Figure 2. A detailed overview of the content of the Empower-Autism programme and proposed change mechanisms is provided in the supplementary materials (Parts 1–4). In brief, the programme consisted of 15-h group-based contact time (5 3-h sessions when delivered in-person; 10 1.5-h sessions when online, corresponding to each of the in-person sessions divided into two), with manualised autism psychoeducation and ACT content: Session 1 offered an introduction to autism and ACT; Session 2 centred on thinking styles in autism, the education system, and managing stress; the third session addressed communication; Session 4 was an ACT-focussed session and Session 5 covered sensory, emotional and behavioural regulation. Delivery methods and ethos were also manualised.
Quantitative data collection (addressing objective 1)
Sample – participants
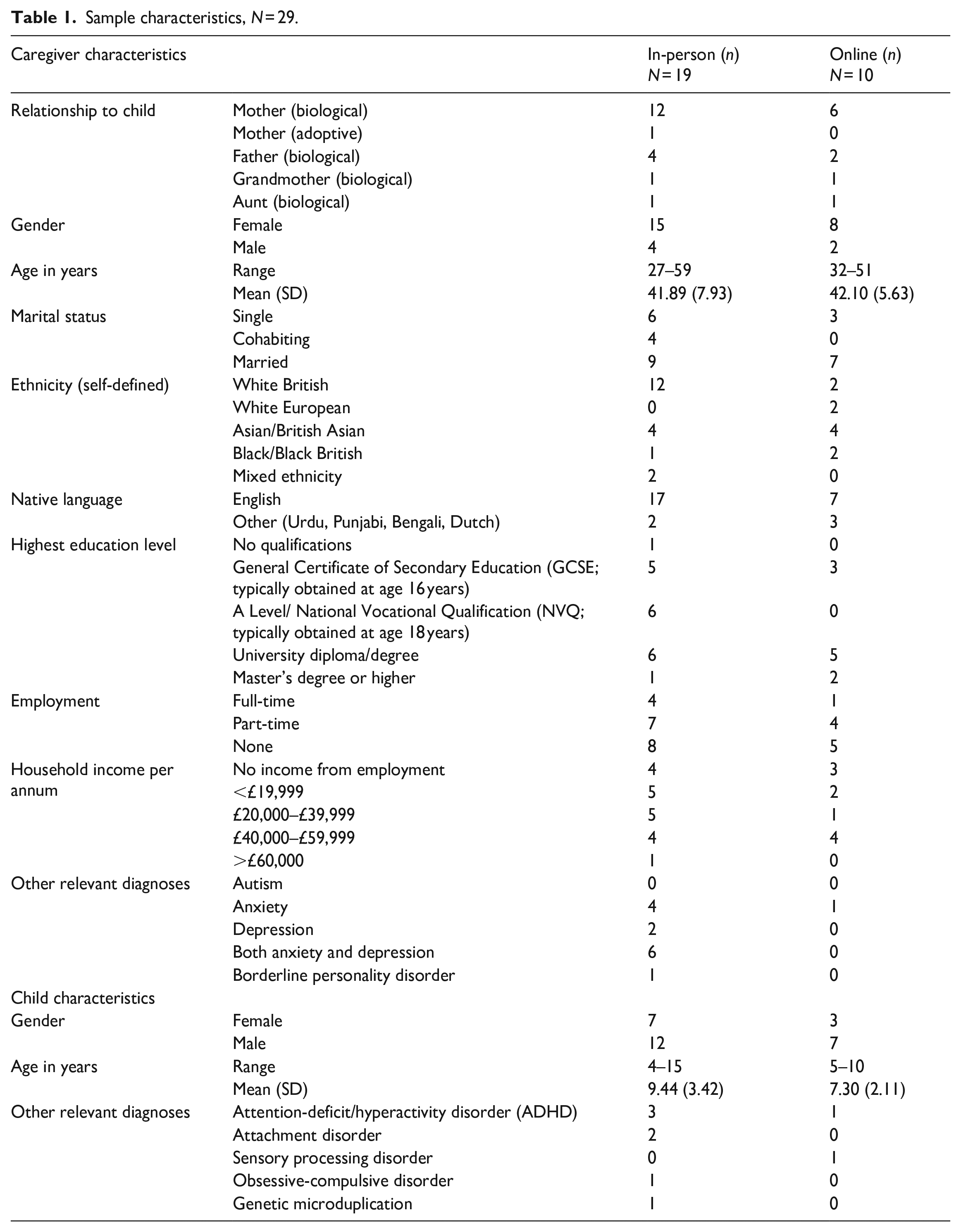
Participants were referred from an autism assessment team in the north of England and met the following eligibility criteria: (a) child aged 2–15 years diagnosed with autism within the past 12 months; (b) one index adult per family, aged above 18 years, with a parenting role for the child (one additional adult per family could attend sessions but were not considered research participants); (c) able to access the programme in English; (d) caregiver without significant learning disability, hearing or visual impairment or severe psychiatric condition which would preclude participation; (e) no significant current safeguarding concerns within the family unit. Overall, 37 referrals were made and 29 caregivers gave informed consent (19 for in-person groups and 10 for the online group). Table 1 shows sample characteristics.
Sample characteristics, N = 29.
Sample – facilitators
Six facilitators delivered the sessions in total, with two delivering each session. Three were project team members and three worked for a local clinical service. Their professional backgrounds were clinical psychology (n = 2), speech and language therapy (n = 1), nursing (n = 2) and social work (n = 1). All were female, White British and aged between 30 and 55 years. They all had prior professional experience of autism assessment and running intervention groups, but not of delivering Empower-Autism groups.
Procedure
Participants were invited to attend one of the three feasibility groups. Two in-person programmes ran in January–February 2020 (n = 10 and n = 9), taking place in a charity-owned conference room close to the local children’s hospital and consisting of five 3-h sessions over consecutive weeks. The online group took place via videoconferencing (Zoom) in September–October 2020 and participants (n = 10) joined from their home or place of work. The online programme consisted of 10 1.5-h sessions running twice-weekly over five consecutive weeks. Attendance data were collected for each session. At the end of each session, participants were invited to complete an anonymous feedback form consisting of quantitative and qualitative items (see Supplementary Materials Part 5). For in-person groups, this was completed on a paper form and posted into a box. For online groups, this was completed using online software (SelectSurvey). The form asked a general satisfaction question ‘How satisfied were you with today’s session?’ with four response options (very satisfied, satisfied, unsatisfied, very unsatisfied), more detailed satisfaction questions with the same response options (see Table 3) and open-ended questions about their feelings about the session. Facilitators were asked to complete a non-anonymous post-session feedback form consisting of quantitative and qualitative items (see Supplementary Materials Part 6), which included one item asking about overall satisfaction, with four response options (very satisfied, satisfied, unsatisfied, very unsatisfied).
Qualitative data collection (addressing objective 2)
Sample – participants
Two weeks following the last session, 24 caregivers were sampled purposively by group and attendance rate from the pool of caregivers in the sample for quantitative data collection (see above) and invited to take part in a semi-structured interview about their experiences of and engagement with the programme. Three did not respond and four declined (three citing reasons associated with family illness/ overwhelm/ childcare issues; one gave no reason). 17 participants opted in: 4 low/non-attenders (i.e. attended < 60% sessions; 3 from in-person groups; 1 from online group) and 13 satisfactory/good attenders (8 in-person; 5 online). The sample comprised 10 mothers, 4 fathers, 1 grandmother and 2 aunts (Mage = 42.94 years; SD = 7.00); 8 were White British and 9 reported other ethnicities; 7 had a university diploma/degree or higher qualification; 3 were in full-time and 9 in part-time employment. None were diagnosed as autistic although three self-identified as autistic in interviews. Full sample characteristics are provided in the Supplementary Materials Part 8.
Sample – facilitators
After delivery of their last session, all six facilitators were invited to attend a focus group or individual interview with two team members to discuss their views on the programme. Five facilitators agreed (three project team members and two members of local clinical services); one was not available (member of local clinical service with a nursing background).
Procedure
The topic guide for participants was informed by quantitative and qualitative responses to session-specific feedback forms, the research questions and theory of change. Interviews were conducted by one of two team members, familiar with the programme and underpinning theory, but not involved in session delivery and previously unknown to participants. Participants were informed that the programme was still under development and therefore their honest feedback was welcome. Full interviews took place with the satisfactory/good attenders, lasting 30–54 min (M = 43.96 mins; SD = 8.06). Briefer interviews (< 16 min) took place with the low/non-attenders which explored reasons for low/non-attendance and questions from the topic guide where appropriate. Interviews were conducted by telephone or videoconferencing, according to participant preference. Topic guides for facilitators were informed by facilitator session-specific feedback forms, the research questions and theory of change. One focus group (1 h 51 min) was attended by three facilitators and two facilitators joined individual interviews (40 and 44 min).
Data analysis
The interviews and focus group were audio-recorded and transcribed verbatim. Data were analysed using reflexive thematic analysis (Braun & Clarke, 2022). A deductive and inductive approach was used: domains were pre-specified for higher-level theme development to ensure detailed understanding of acceptability, accessibility and perceived outcomes, which were of practical importance to the development of the programme; this was coupled with inductive development of subthemes to allow for data-driven and unanticipated findings. A realist epistemological stance was adopted with meaning explored at a semantic level, with the assumption that facilitator and participant reports would broadly reflect their realities of the programme. Transcripts were coded by two researchers who contributed to programme development, but not delivery. Coders met regularly throughout the analysis period to compare and sense-check interpretations, develop the coding framework and synthesise theme generation. Supervision and further sense-checking were provided by an experienced qualitative researcher not part of the programme development or delivery team.
Results
Quantitative results
Participant attendance: A satisfactory attendance rate was observed for both groups. For in-person programmes (n = 19), 14 participants (74%) attended ⩾ 3/5 sessions of which 58% attended all 5 sessions. Three participants (16%) attended no sessions. For the online programme (n = 10), 8 participants (80%) attended ⩾ 6/10 sessions with 3 (30%) attending all 10 sessions. One participant attended no sessions. The demographic characteristics of the seven low/non-attenders (i.e. those who attended < 60% sessions) were five female, two male; four White British, two Asian/British Asian, one Black/Black British and three with no relevant diagnosis, two with anxiety and two with both depression and anxiety.
Participant satisfaction: Overall, 68 post-session feedback forms (100% return rate) were returned for the in-person programmes and 64 (86% return rate) for the online programme. Satisfaction was high, with 74% of sessions rated as ‘very satisfied’ and 26% as ‘satisfied’ for the in-person sessions and 66% rated as ‘very satisfied’ and 34% as ‘satisfied’ for the online sessions. A breakdown of ratings by session is provided in Table 2.
Overall participant satisfaction ratings in-person and online groups by session (session titles in table footnote; split sessions combined for online groups to render them comparable to in-person groups).
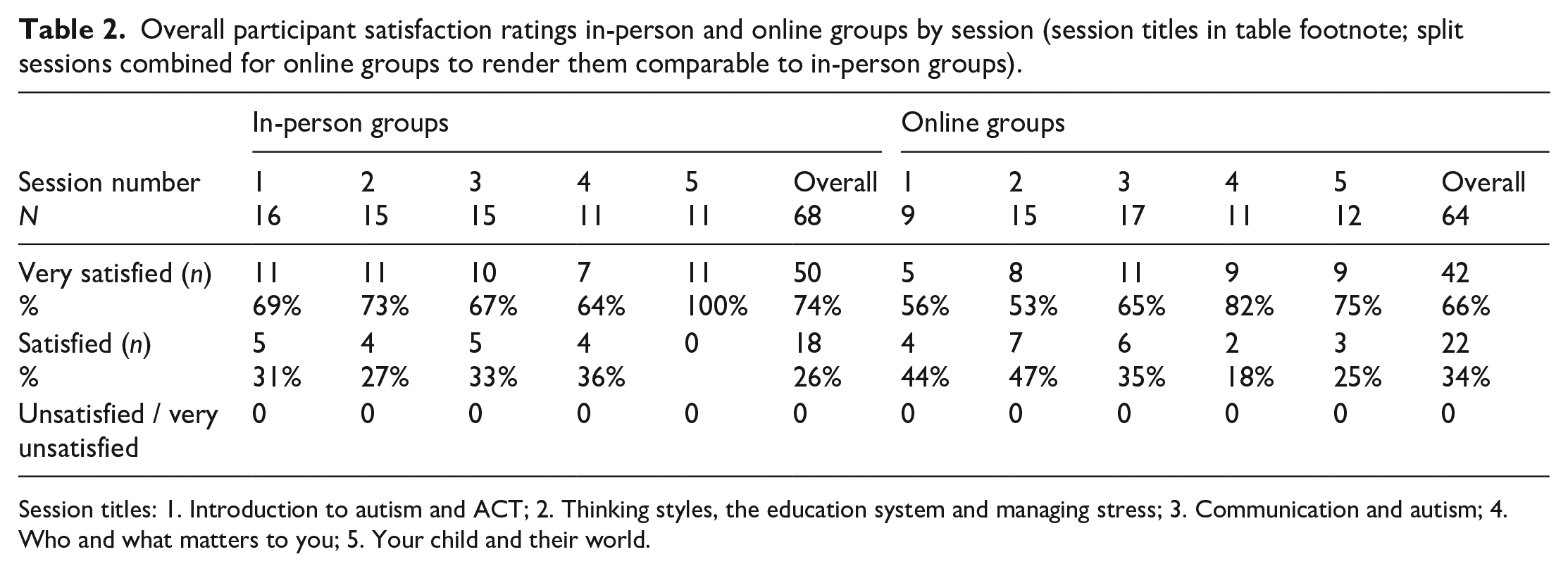
Session titles: 1. Introduction to autism and ACT; 2. Thinking styles, the education system and managing stress; 3. Communication and autism; 4. Who and what matters to you; 5. Your child and their world.
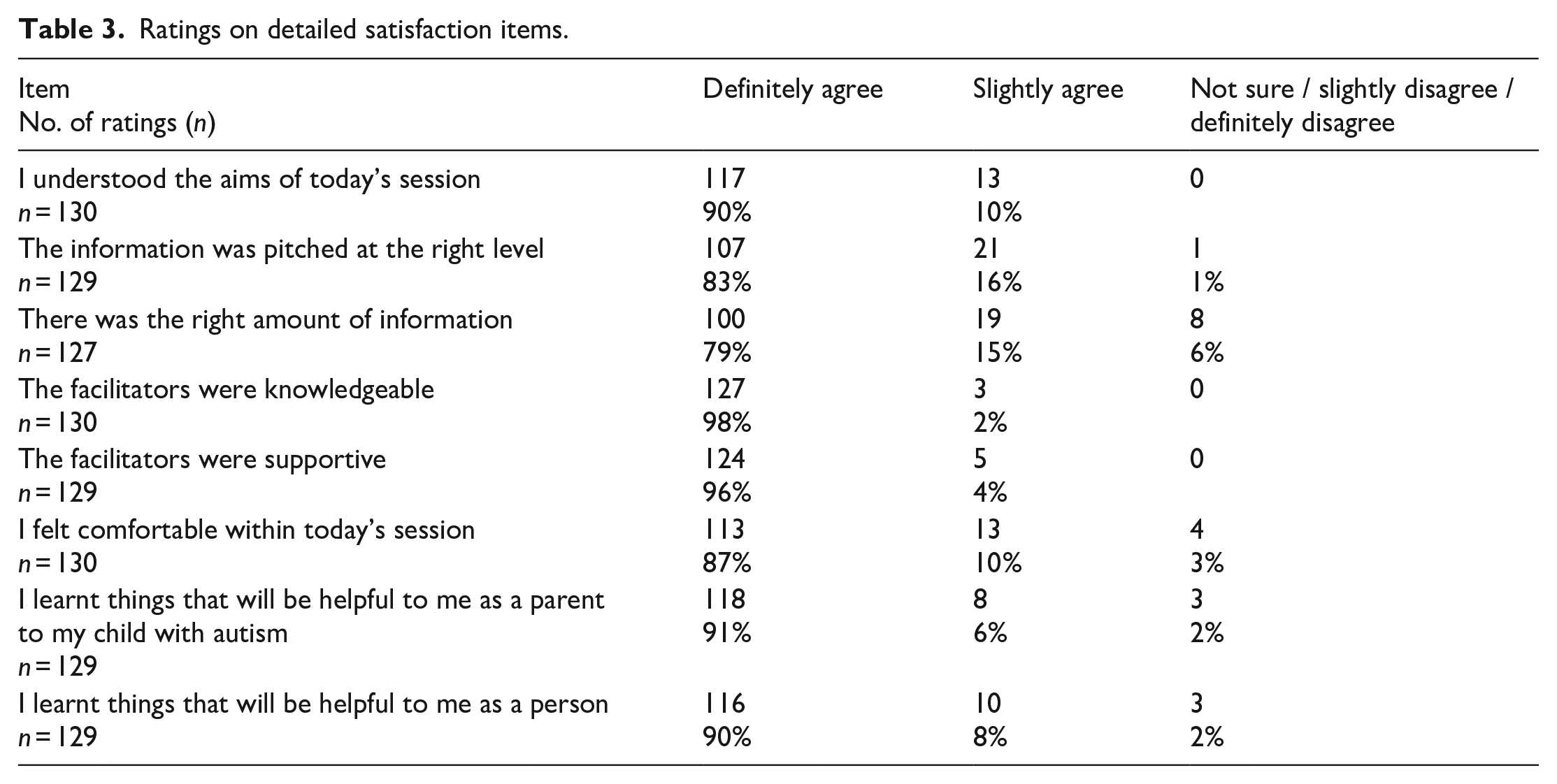
Responses to the detailed satisfaction items are shown in Table 3; in-person and online sessions were rated similarly and data are therefore collapsed. A full breakdown is provided in the Supplementary Materials Part 7.
Ratings on detailed satisfaction items.
Facilitator satisfaction: 10 post-session feedback forms (100% return rate) were returned for the in-person programmes and 10 (100%) for the online programme. 30% sessions were rated as ‘very satisfied’, 65% ‘satisfied’ and 1 session (5%) as ‘unsatisfied’.
Qualitative results
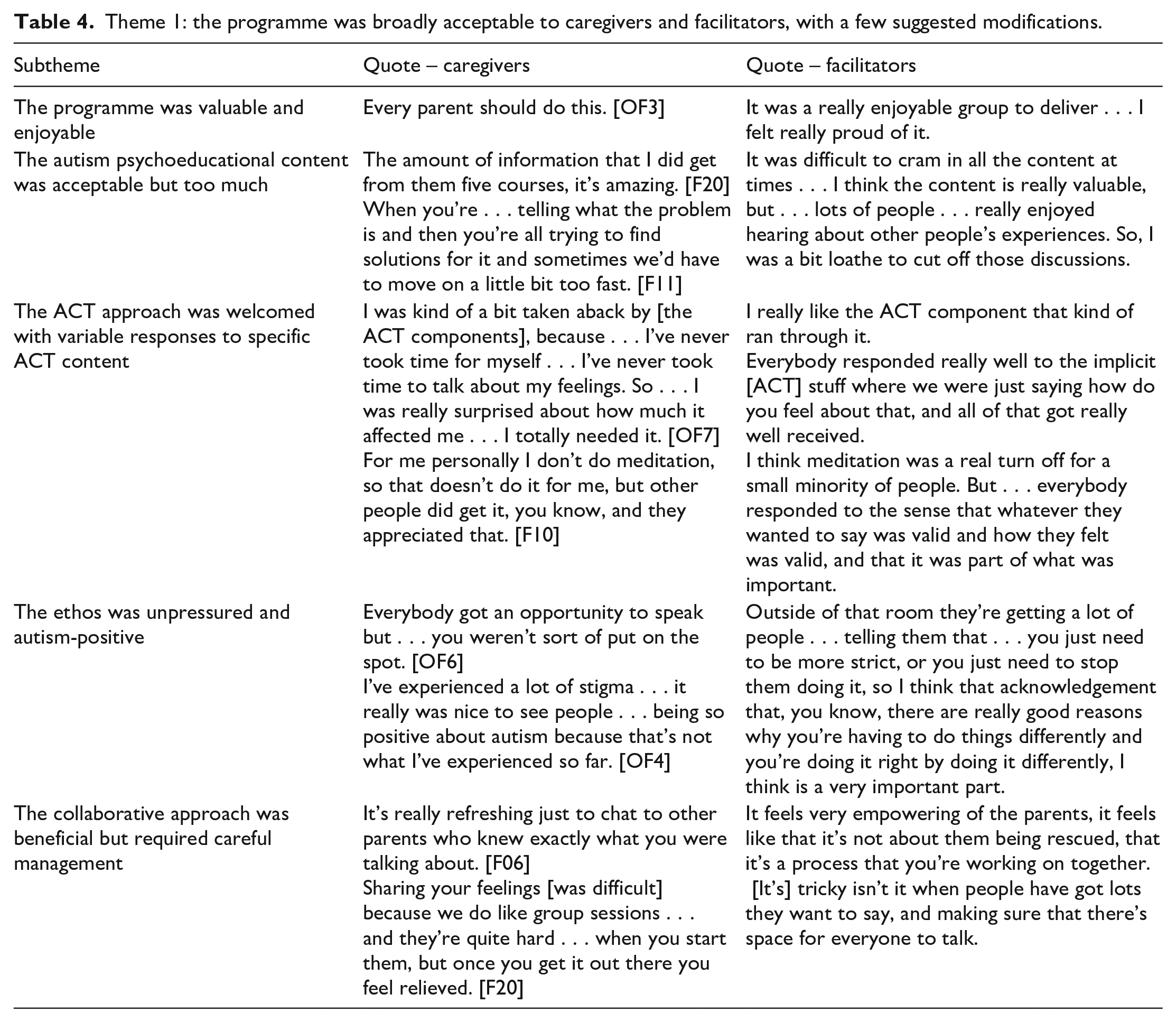
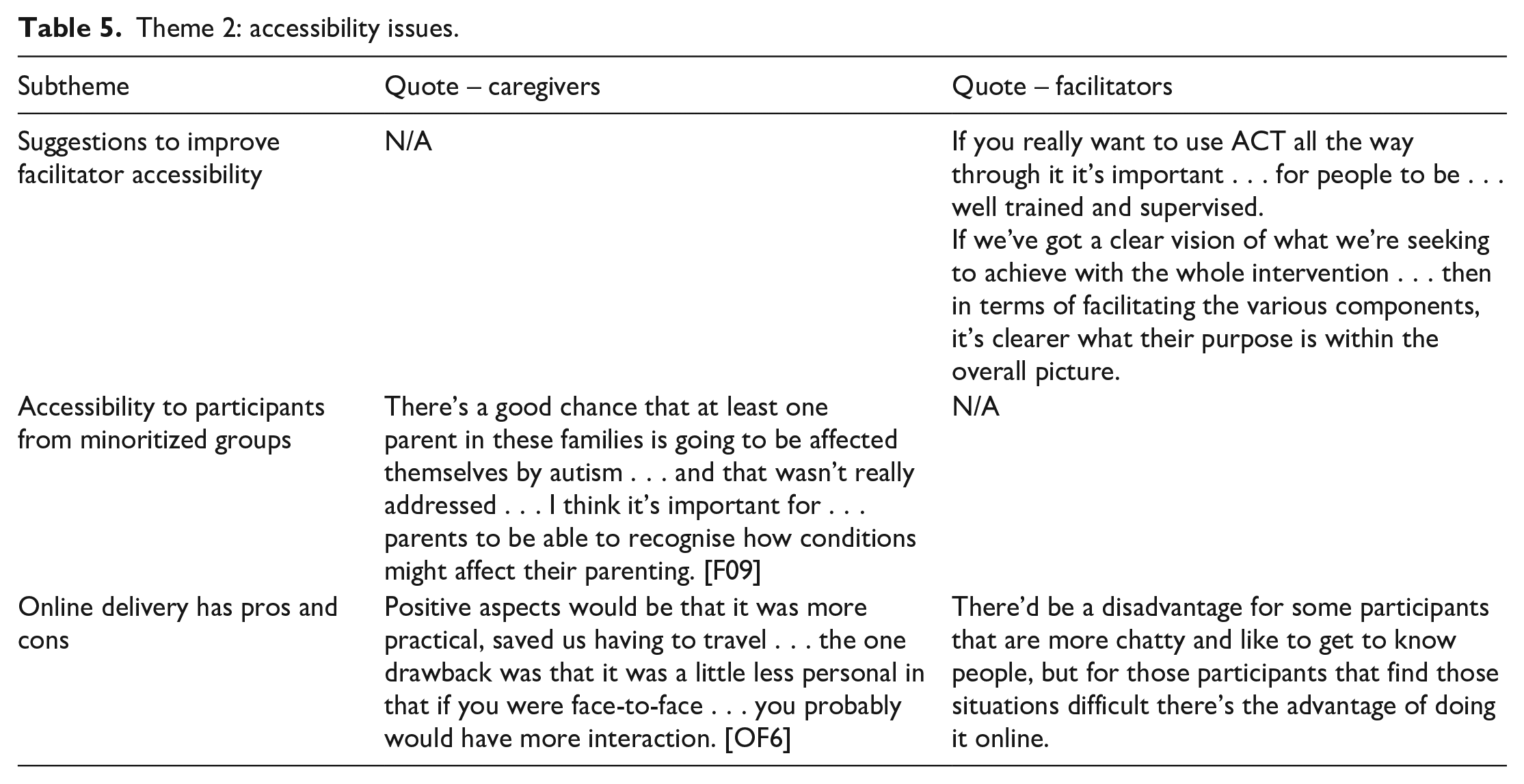
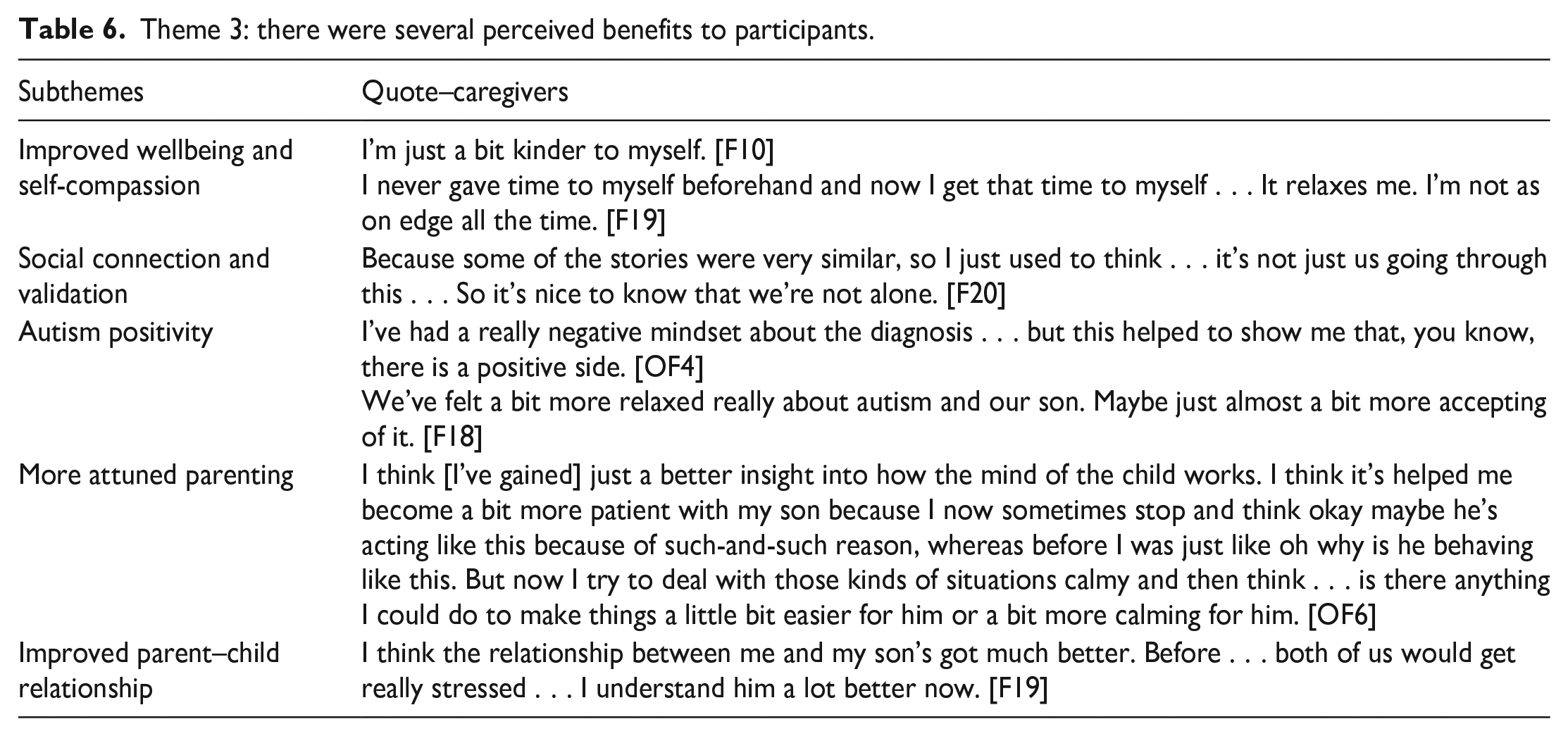
Themes, subthemes and supporting quotes are shown in Tables 4 to 6. Participant IDs are shown alongside their quotes (F = in-person participant; OF = online participant). A narrative summary is provided below, with themes and subthemes.
Theme 1: the programme was broadly acceptable to caregivers and facilitators, with a few suggested modifications.
Theme 2: accessibility issues.
Theme 3: there were several perceived benefits to participants.
The programme was broadly acceptable, with a few suggested modifications
Facilitators and participants described that the programme was valuable and enjoyable. Facilitators felt proud of the programme. Participants would recommend the programme to others. Reported reasons for low/non-attendance were associated with life circumstances rather than the programme itself. The autism psychoeducational content was acceptable but too much. Participants stated that they received a lot of information and learnt a lot. Some participants stated that the information was too basic, but they tended to qualify this saying it was helpful for knowledge assimilation and reassurance. Both facilitators and participants felt that there was too much content for the time available. This meant that, sometimes, the delivery was rushed and beneficial conversations had to be closed down. The ACT approach was welcomed, with variable responses to specific ACT content. Facilitators spoke explicitly about liking the ACT therapeutic approach and feeling it held relevance to participants’ situations. Some participants described that the ACT content and the emphasis on self-care was a revelation and they had not realised how much they needed it. Others found that specific ACT activities were not a good fit for them, although often adding that they could see that other members valued them. This variability was also reported by facilitators who also noted that discussion about which exercises did and did not work was itself valuable. Participants described that the ethos was supportive and autism-positive and this was refreshing and empowering. They welcomed the ‘upbeat feel’, where they could discuss the positives about their children and autism, and the affirmative ethos which focussed on adapting the environment around the child, rather than trying to change the child themselves. Facilitators described that the collaborative approach was beneficial but required careful management. This approach embraced the lived experience brought by caregivers and empowered them to share expertise with each other. Participants also described the beneficial effects of sharing feelings and experience, and practical strategies ‘tried and tested’ by other parents. Both caregivers and facilitators reflected on the challenges of a collaborative approach and the need for careful and sensitive management to ensure that everyone felt comfortable and able to contribute.
Accessibility issues
Facilitators shared suggestions to improve facilitator accessibility. They emphasised the therapeutic skill required to deliver the sessions and the need for ongoing ACT supervision. They requested more streamlined notes, a more explicit framework and a clearer understanding of the flow of ACT content through the programme. They also suggested that increased flexibility for different age groups and group dynamics and a wider range of ACT tools would increase accessibility and individual goodness-of-fit for participants. Participants did not report issues with accessibility to participants from minoritized groups. Self-identified autistic participants described that they could tell that consideration had been given to autistic attendees. They suggested that facilitators could be upfront about the potential for autistic participants within the group to make this easier to be openly discussed. They also wanted further reflection on how participants’ own autistic traits might impact on their parenting. Online delivery has pros and cons. There were practical benefits to online delivery, including no travel time and ease of fitting around work and childcare commitments. There were reported challenges too. It could be difficult to manage distractions when joining from work or home and to share personal information with colleagues or family within earshot. Some participants were initially worried about the technology, but all participants ultimately were able to use it without major problems. Facilitators and most participants felt that social connections did happen within the online programme, but sometimes this took longer. They noted that reduced opportunity for informal social chat could be an advantage to some, and disadvantage to others.
Perceived outcomes for participants
Participants described several perceived outcomes in response to the programme. Some caregivers described improved wellbeing and self-compassion. Participants gave examples of increased self-care and taking moments in their day-to-day life to use strategies learnt in the programme, such as grounding exercises or connecting with values, with positive impact on their wellbeing. Many participants reported that the programme gave them a sense of social connection and validation of their feelings and situation. Some caregivers remained in touch after the programme and continued to offer mutual support. Some participants reported that they completed the programme with increased autism positivity, feeling less anxious and afraid and more accepting of autism. In addition, participants described more attuned parenting through a greater understanding of their child, more patience and a greater insight of their child’s behaviour, allowing them to respond in more informed way. Furthermore, some described that these changes resulted in an improved parent–child relationship.
Final modifications
Themes and subthemes were discussed within the trial team and advisory group. This discussion led to decision-making by consensus around the final refinements to the theory of change and programme protocol. These refinements included: making more time for discussion by stripping out content that received less favourable feedback, was less important to the theory of change and overall programme coherence or was disproportionately time-consuming to deliver well; ensuring robust ongoing ACT supervision; adding further flexibility for different age groups and group dynamics; including a wider range of ACT activities/tools and a clearer overarching framework; and facilitators being more upfront about the potential for autistic participants within the group.
Discussion
This study aimed to develop and assess the feasibility and acceptability of a novel manualised group-based programme – Empower-Autism. This programme blends autism psychoeducation and psychotherapeutic support based on ACT to address the informational, relational and emotional needs of caregivers of children and young people recently diagnosed with autism. The detailed, iterative development phase involved a wide range of stakeholders and resulted in a novel manualised relatively low-intensity intervention underpinned by a theory of change. It met prespecified criteria demonstrating feasibility (attendance and satisfaction) within a socioeconomically diverse, clinically referred sample. The qualitative analysis provided more detailed information about the acceptability and accessibility of the programme. Suggested improvements were incorporated within the final stage. Perceived proximal outcomes were consistent with the change mechanisms proposed in the programme theory of change, including increased self-care, enhanced autism acceptance and positivity, a more attuned parenting of their autistic child, and a mitigation of stigma and isolation experienced within the community. These perceived benefits could potentially strengthen caregiver resilience in the face of ongoing stress caused by systemic or individual factors and thereby result in improved mental health and wellbeing. This programme was deliverable by trained staff typical of those working within UK autism clinical pathways, with potential scalability to service provision more widely. The programme took skilled therapeutic delivery and facilitators emphasised that this requires specific competencies, careful training and ongoing supervision.
There are important points to note when considering the programme’s feasibility and acceptability. First, the study and its intervention groups included caregivers of recently diagnosed autistic children of a wide age range (4–15 years). This age range is reflective of the UK diagnostic service from which we recruited participants and is broadly consistent with previous research reporting on current diagnostic practices in the United Kingdom (Male et al., 2023; O’Nions et al., 2023) and therefore the suitability of this programme for this full age group is a strength. However, flexible delivery of content and careful management of interpersonal dynamics were vital to ensure relevance and sensitivity to caregivers of children of all ages. Future clinical delivery could consider grouping caregivers more narrowly by child age and further research could assess the acceptability of the programme to caregivers of very young children (e.g. 18–48 months). Second, an important finding of this study was that four of the seven low or non-attenders had a diagnosis of anxiety. Representatives of this group did not state that their anxiety affected their attendance and six other caregivers with anxiety did attend well but, nonetheless, we cannot rule out that anxiety played a role in limiting attendance for some individuals. Further research could explore the relationship between caregiver anxiety and the feasibility and acceptability of group-based, psychotherapeutic programmes, and whether alternative provision may sometimes be more accessible. A third issue for reflection concerns the session length of our programmes. The in-person programmes consisted of five 3-h sessions and the online programme of 10 90-min sessions (each full session divided into two). Session length and number were discussed in detail with stakeholders during both the in-person and online codesign phases, and a range of preferences were expressed, with a slightly stronger inclination towards fewer longer sessions for in-person groups and more shorter sessions for online groups. We did not find evidence from the qualitative feedback that either format was a barrier to attendance or engagement generally, rather that preferences related to individual circumstances and that the ideal scenario, if possible, is to offer flexibility and choice to maximise accessibility to caregivers in diverse circumstances.
This study contributes to the growing literature suggesting that ACT is a promising approach to provide emotional support to caregivers of autistic children (e.g. Juvin et al., 2022). This study adds to existing knowledge by evidencing how ACT is perceived and responded to by caregivers of autistic children in the post-diagnostic period and provides examples of how it can be embedded positively within their daily lives. The Empower-Autism programme is novel in its integration of ACT with autism psychoeducation within one programme. A systematic review of parental experiences of parent-mediated interventions for autistic children emphasised the need for mental health and wellbeing support to be delivered along child-focussed interventional strategies (Jurek et al., 2023). This study provides new evidence of how ACT and autism psychoeducation can work successfully together within one programme to efficiently meet diverse and multifaceted needs. This complements the work of other international teams who are developing and evaluating programmes that incorporate mental health and wellbeing support for caregivers with broader child-focussed interventional approaches (e.g. McLay et al., 2023; Salomone et al., 2022). A shift towards a more neurodiversity-affirmative framework that emphasises acceptance and environmental goodness-of-fit is occurring in contemporary autism research and practice (Leadbitter et al., 2021). Our findings suggest that this programme is broadly consistent with this approach and that it holds potential to improve the goodness-of-fit of children’s social, emotional and physical environments.
The COVID-19 pandemic necessitated a move to online delivery. This provided a ‘natural experiment’ to pilot online alongside in-person delivery. The quantitative data suggest similar levels of acceptability of these two delivery modes. The qualitative analysis found that participants acknowledged both advantages and disadvantages to online delivery. There were no major practical problems with this delivery mode and it was possible to deliver the programme ethos and facilitate social relationships. These findings are largely consistent with those of Hermaszewska and Sin (2021) who also reported that parents of autistic children were largely open to online delivery of intervention groups and those of Lau et al. (2022) who found that both online and in-person modes were feasible and acceptable, and both brought advantages and disadvantages. However, it is important to bear in mind that our sample size was small and, due to the pandemic context, participants were evaluating online delivery as the only option available at that time, so different results may have been found in a non-pandemic context.
One limitation of this study was that the qualitative data collection and analysis were carried out by team members involved in the development of the programme which could bring about potential for bias. We tried to counteract this by emphasising to participants that the programme was still in development and therefore improvements could be made. Interviewers had not personally delivered or supervised delivery of the sessions. In addition, we employed reflexivity within our analysis and sense-checking activities, and reflected that the two analysts who had developed the programme were naturally invested in its success, but also that, at this project stage, any necessary changes to optimise the programme could be made to maximise its acceptability and effectiveness at the next stage and therefore we were open to constructive criticism. A further limitation was that, as facilitators were new to the programme, fidelity of delivery was not objectively measured. This will be an important priority for the next project phases.
The Empower-Autism programme is now being evaluated in a large randomised controlled trial to ascertain its effectiveness and cost-effectiveness (Leadbitter et al., 2022; ISRCTN: 45412843). A qualitative nested process evaluation within this trial will further elucidate the acceptability and implementation factors associated with the programme. If shown to be clinically and cost-effective, this programme would address a community priority for research and service provision (James Lind Alliance, 2016; Waddington et al., 2024) and fill an identified evidence gap within current provision in the United Kingdom and internationally.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241274566 – Supplemental material for The development, feasibility and acceptability of Empower-Autism: A new psychoeducational and psychotherapeutic programme for caregivers of children recently diagnosed with autism
Supplemental material, sj-docx-1-aut-10.1177_13623613241274566 for The development, feasibility and acceptability of Empower-Autism: A new psychoeducational and psychotherapeutic programme for caregivers of children recently diagnosed with autism by Kathy Leadbitter, Louisa Harrison, Sophie Langhorne, Ceri Ellis, Richard Smallman, Amelia Pearson, Latha Hackett, Leo Kroll, Alison Dunkerley, Hilary Beach, June Gilbert, Amy van Gils, Tessa Hutton, Jonathan Green and Penny Bee, and the REACH-ASD Team in Autism
Footnotes
Acknowledgements
The authors thank: the wider REACH-ASD Team, including Henna Ahmed, Petrina Chu, Richard Emsley and Kirsty James; the experts-by-experience who provided helpful guidance, feedback and got involved in co-production, including the autism@manchester Expert by Experience Group; and the contribution of many colleagues within Manchester University NHS Foundation Trust who inputted into the programme development and who referred participants to the study, including Katy Baldwin, Emily Birch, Jo Bromley, Alison Hunter, Rachel Lancaster, Rachel Samuels, Sam Todd and Lisa Walker. They also thank: Katy Roe from Mindscape Psychology, Abigail Sterne from One Education and Debbie Waters from the National Autistic Society; Kate Sofronoff and Koa Whittingham from the University of Queensland for the generous sharing of their ACT manual and other works. Finally, they thank all the participants for their valuable insights.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UK National Institute of Health and Social Care Health Technology Assessment (HTA Project: 17/80/09). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.