
Abstract
Controversies regarding the neurodiversity movement may be exacerbated by confusion over its meaning. For example, some suggest neurodiversity entails acceptance of the social model, whereas others describe it as more nuanced. We aimed to help resolve conflicting viewpoints by inviting insights from 504 autistic and autism community members (278 autistic, 226 non-autistic), including 100 researchers (41 autistic), 122 professionals (35 autistic) and 162 parents/caregivers (53 autistic). They rated the neurodiversity movement, social model, medical model and intervention goals, and answered open-ended questions regarding the meaning of neurodiversity, the neurodiversity movement and disability models. Neurodiversity movement support was associated with endorsing societal reform and making environments more supportive, and lower support for normalization and adaptive skill interventions, though teaching adaptive skills was widely supported overall. Although participants often suggested the social model attributes disability solely to society, this ‘strong’ view was not universal. ‘Strong’ social model supporters still endorsed some interventions targeting individuals’ characteristics (specifically, teaching adaptive skills, curing depression and epilepsy). Findings confirm that neurodiversity movement supporters denounce normalization, but are open to individualized supports. Findings highlight strong support for autistic leadership (especially among autistic people, including autistic parents) and for societal reform, and suggest that oversimplified rhetoric may cause confusion regarding advocates’ views.
Lay abstract
Introduction
The neurodiversity movement (NDM), and its impacts on supports for and research about neurodivergent people, is intensely controversial (Bailin, 2019; Baron-Cohen, 2019; Chellappa, 2024; Lerner et al., 2023). Many autistic (Robertson, 2010; Walker & Raymaker, 2020) and non-autistic people (Des Roches Rosa, 2019; Savarese et al., 2010) speak strongly in support of approaches inspired by the NDM, while other people (Costandi, 2019; Hiari, 2018; Lutz, 2015) strongly denounce them.
Unfortunately, the concept of neurodiversity can be ambiguous, complicating debates regarding the NDM. One meaning of ‘neurodiversity’ is purely descriptive – referring to the reality of human neurocognitive diversity (Singer, n.d.; Walker, 2021) – but some understand it to be prescriptive or ideological (Ne’eman & Pellicano, 2022). It is also the basis of neurodiversity approach(es) (Dwyer, 2022), alternately called a ‘perspective’ (Robertson, 2010), ‘paradigm’ (Walker, 2014, 2021) or ‘framework’ (Kapp, 2020), that are clearly prescriptive. 1 The NDM champions neurological diversity and the neurodiversity approaches. But what, precisely, does this mean? Not only is neurodiversity often simply misunderstood (den Houting, 2019), but various parties can hold different legitimate views of what neurodiversity means (Chapman, 2020a; Dwyer, 2022; Ne’eman & Pellicano, 2022), in part because the neurodiversity concept was not developed by any single person (Botha et al., 2024; Dekker, 2023). This confusion makes it harder to resolve debates regarding the appropriateness of neurodiversity-affirming approaches towards autistic and neurodivergent people, their needs and intervention/supports.
Disability, Neurodiversity and Intervention
One particularly important question is the status of disability in neurodiversity approaches. While numerous NDM supporters strenuously deny claims that the NDM rejects the reality of disability (Ballou, 2018; den Houting, 2019; Thinking Person’s Guide to Autism, n.d.), the ways in which neurodiversity approaches conceptualize disability remain somewhat contentious. Models of disability such as the medical model (MM) and social model (SM) predate the emergence of autistic/neurodiversity advocacy in the 1990s (Botha et al., 2024; Kapp, 2013; Pripas-Kapit, 2020). For much of the 20th century, researchers and clinicians have generally operated within the dominant MM of disability, which – at least in its conventional, ‘strong’ form – conceptualizes autism and other neurodevelopmental differences as disorders and deficits rooted in biological differences between people (Kapp, 2023). In the MM, these biological differences might be understood to have a genetic aetiology, environmental influences (e.g. exposure to substances in utero) might be recognized or a genetic-environmental interaction might be recognized, but either way, in the traditional MM, the internal biological differences directly lead to a person’s experience of disability-related challenges. Under this model, experts prescribed interventions to cure, prevent or suppress autism and autistic behaviours (Kapp, 2023). Admittedly, in practice, individuals and groups using pathologizing rhetoric consistent with the MM do often end up advocating for societal changes of one form or another (Baker, 2011), but these might raise rights and justice concerns (e.g. restraints and subminimum wage; National Council on Severe Autism, n.d.) and can be an adaptation to the infeasibility of curing or preventing many disabilities using currently available technologies (Lutz, 2024).
In contrast to the MM, some authoritative sources suggest that neurodiversity approaches are aligned with the SM of disability (Bölte et al., 2021; Labour Party Autism/Neurodiversity Manifesto Steering Group, 2018; Thinking Person’s Guide to Autism, n.d.), which – again at least in its conventional ‘strong’ form – attributes difficulties associated with disabilities solely to societal inequalities, including active discrimination against people with disabilities (Shakespeare, 2006; illustrated in Figure 1). In its traditional form, the SM separates disability from ‘impairments’, the actual biological differences between disabled and non-disabled people. 2 Instead of directly causing disability, a person’s biological differences would only give rise to disability if societal institutions, infrastructure and practices were exclusionary (Oliver, 1990, 2009). For example, some autistic people, in some contexts, can communicate and connect with other autistics as successfully as non-autistic people can with other non-autistics (Crompton, Ropar, et al., 2020; Crompton, Sharp, et al., 2020). This and other research examining the double empathy problem (Milton, 2012), suggests that autistic social disabilities are not, in fact, inherent deficits in autistic people and may often be caused by exclusionary behaviours from neurotypicals – just as the ‘strong’ SM claims.
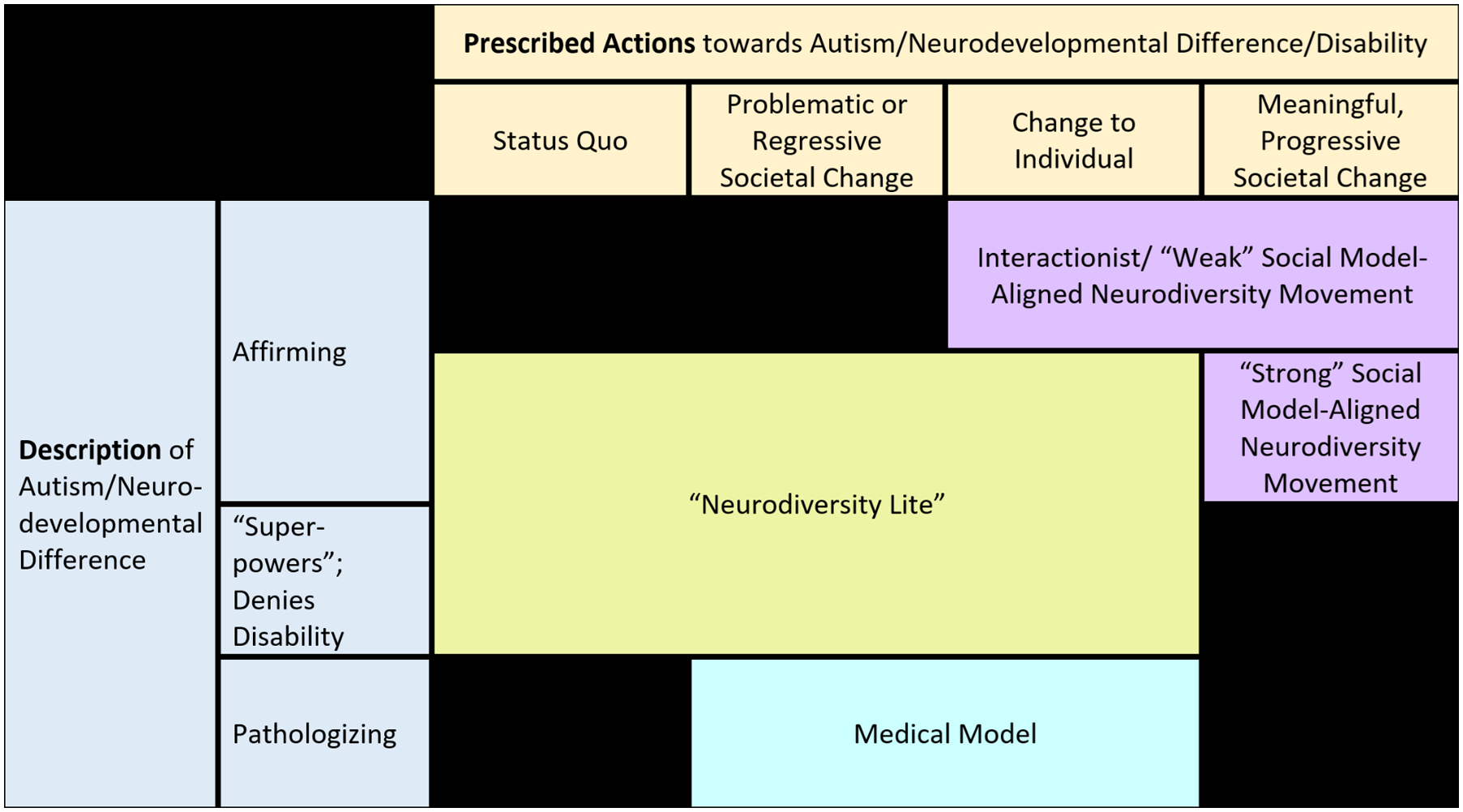
Illustration of how various models of and approaches towards autism/disability could characterize/understand autism and neurodevelopmental differences (in a pathologizing manner, an affirming manner or a manner that does not recognize challenges and focuses on ‘abilities’ and ‘superpowers’ only) and whether they prescribe changing the individual, society or both.
However, some NDM and/or disability 3 advocates, including the first author, reject the ‘strong’ form of the SM (Ballou, 2018; Kapp, 2013; Shakespeare, 2014) and support various interactionist or social-relational models of disability (Autistictic, 2020; Chapman, 2021; Dwyer, 2022; Kapp, 2013; Shakespeare, 2014) generally conceptualizing disability as the product of poor person–environment fit: a mismatch between the person and their environment disables them. Neither the person nor the environment is necessarily always the sole culprit. As such, in different contexts, intervention might appropriately focus on either changing the person, changing their environment or both (see Figure 1). While the NDM clearly suggests that intervening to cure autism would always be inappropriate, some advocates suggest that interventions could still teach useful adaptive skills (Autistic Self Advocacy Network, 2021; Dwyer, 2022; Kapp et al., 2013; Sinclair, 1992), seemingly in alignment with these interactionist views.
In addition, not everyone endorsing ‘the social model’ supports a ‘strong’ SM. While some ‘strong’ SM supporters reject any possibility of common ground with the MM (Cameron, 2024), for decades, others have called for the SM to expand beyond its societal focus to acknowledge biological differences as important in themselves (Crow, 1996; B. Hughes & Paterson, 1997), creating what might be called a ‘weak’ SM (see Figure 1). Even Mike Oliver, a leading ‘strong’ SM champion, readily acknowledged that its dismissal of biological differences made it only a politically useful tool, not a complete theory (Oliver, 2009, 2013). Thus, contrary to some assertions (J. A. Hughes, 2021), some SM-endorsing neurodiversity advocates might support some individual-focused interventions. Because autism interventions have generally focused on changing autistic people rather than society (Bottema-Beutel et al., 2018; Broderick & Roscigno, 2021; Scott et al., 2019), advocates might simply see the SM as a tool for shifting towards greater balance between these objectives, and modifying intervention goals and practices accordingly. Notably, neurodiversity advocates often acknowledge that some co-occurring conditions – for example, clinical anxiety, depression, epilepsy – should be medically cured if possible (Autistic Self Advocacy Network, 2022; Chapman, 2019; Kapp, 2020; Love, 2022; Thinking Person’s Guide to Autism, n.d.), though opinions vary (e.g. see Armstrong, 2010, a non-autistic writer). This leads to an important question – do autistic and autism community members who claim to support the SM endorse a ‘strong’ SM?
Further complicating the situation, not only is the NDM sometimes mischaracterized as less capable of recognizing and supporting personal difficulties than it often is (Bailin, 2019; Ballou, 2018), NDM supporters have expressed concern over ‘neurodiversity lite’ views: adoption of neurodiversity rhetoric and slogans without a full understanding of the NDM or commitment to its goals, and perhaps even to oppose the NDM’s goals or seek personal profit (Chapman, 2023; den Houting, 2019; Neumeier, 2018; Roberts, 2021). For example, ‘neurodiversity lite’ could involve performatively speaking about celebrating neurocognitive differences while simultaneously promoting masking/camouflaging and reinforcing neurotypical social norms, and/or stereotyping neurodivergent people as having marketable ‘super powers’ that can be exploited to increase productivity.
Thus, in summary, perspectives regarding the nature of disability among NDM advocates remain ambiguous, though many NDM advocates appear to have more nuanced perspectives than implied by a ‘strong’ SM.
This study
This study used a mixed-methods approach to explore perspectives regarding these issues in the autistic and autism communities. Importantly, we do not aim to suggest that particular views should be adopted merely because they are more or less popular, but to illuminate common understandings of the NDM and their implications for interventions and supports, so that discussions and debates can proceed with greater clarity and fewer misunderstandings. We were especially curious about – and sceptical of – whether neurodiversity advocates commonly endorse views consistent with a ‘strong’ SM: in particular, focusing solely on changing society and rejecting all efforts to change autistic people.
Through social media and requests for autism organizations to distribute recruitment information, participants who were autistic, or had a connection to autism in other ways (such as being a family member of an autistic person, or having a professional/research role related to autism) were recruited and asked to quantitatively rate their support for the NDM, models of disability and intervention goals. Furthermore, to contextualize these data, participants were also asked to qualitatively define neurodiversity, the NDM and models of disability. We hypothesized that:
Support for the NDM would be associated with reduced endorsement of normalization/behaviour reduction goals, but not with altered endorsement of adaptive skill or well-being/mental health goals, in alignment with findings from a study examining attitudes towards neurodiversity and interventions in the autism community around a decade ago (Kapp et al., 2013).
Autistic neurodiversity proponents would show a greater focus on environmental and societal barriers, and support for interventions capable of changing these than non-autistic neurodiversity proponents, as they would be less susceptible to ‘neurodiversity lite’ than non-autistic neurodiversity proponents.
Many participants who report supporting the SM would endorse supports that aim to change the autistic person through teaching of adaptive skills, not just reforms to environments and society, inconsistent with the tenets of the ‘strong’ SM.
As such, this mixed-methods study relates to a number of domains of inquiry. It is inextricably concerned with disability studies and theory, while findings regarding the perceived desirability of specific intervention goals to participants and subsets of participants also have implications for practice. Parts of the article relate to philosophy, logical consistency and ontology. The study is empirical and an exercise in scientific hypothesis-testing, but findings also have political implications.
Methods
Participants
This study’s sample is also described in the study by Hersh et al. (2024). Participants were recruited from social media and through contacting autism organizations in multiple countries; to be eligible, they were required to be adults with a connection to autism, such as being autistic, being family members of an autistic person and/or autism professional/research roles. After removal of putatively invalid/bot/fake data and incomplete responses whose validity could not be evaluated (see Supplemental Appendix A; see also Goodrich et al., 2023; Pellicano et al., 2023), 504 responses (278 autistic, 226 non-autistic) remained (see Table 1). Most participants came from Canada (n = 55), the United Kingdom (n = 60) or the United States (n = 337).
Sample demographics.
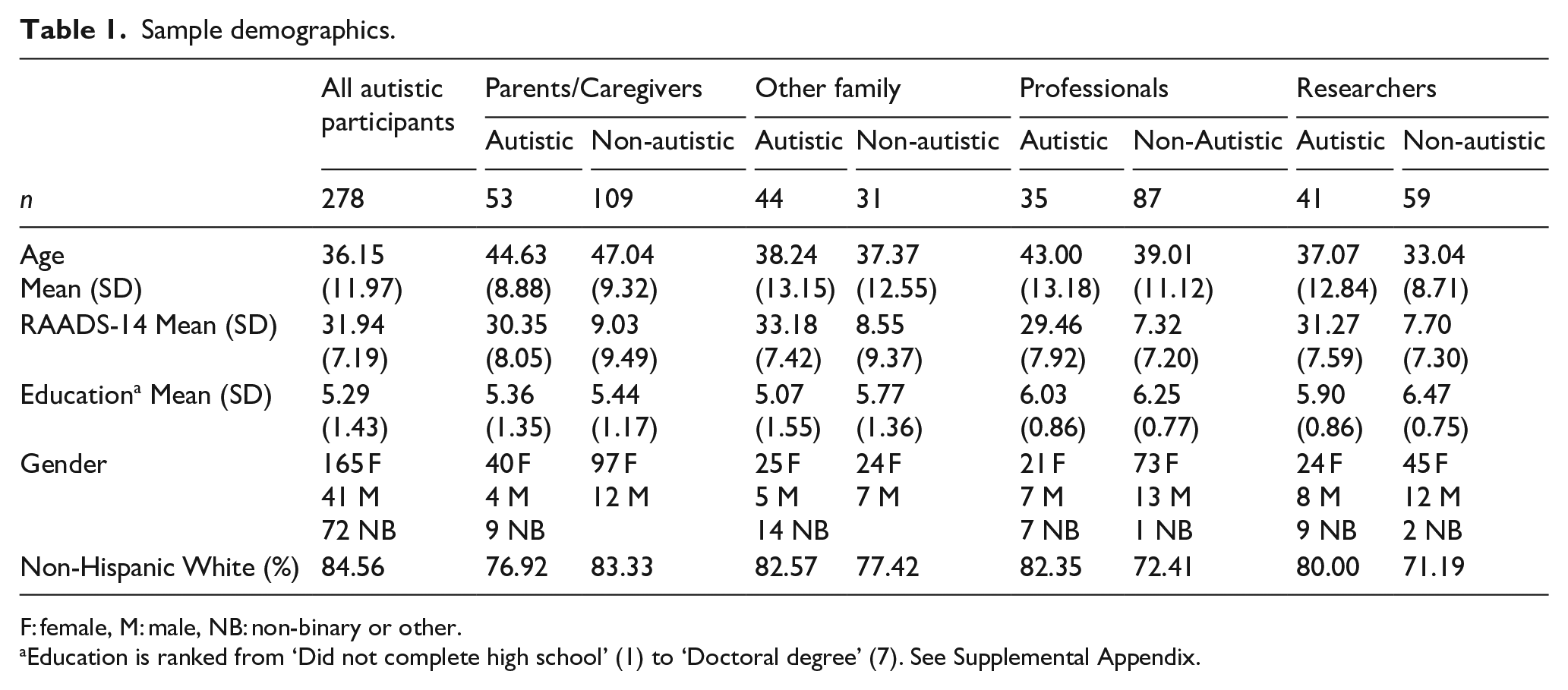
F: female, M: male, NB: non-binary or other.
Education is ranked from ‘Did not complete high school’ (1) to ‘Doctoral degree’ (7). See Supplemental Appendix.
Measures
NDM support/identification
Participants were asked whether they had heard of neurodiversity. If yes, NDM support/identification was measured on a 5-item, 7-point Likert-type scale adapted from the study by Nario-Redmond et al. (2013; see Supplemental Appendix B). Participants were also asked open-ended questions: ‘What do you think “neurodiversity” means?’ and ‘What do you think “the neurodiversity movement” means?’
Models of disability
If participants had heard of the SM or MM of disability (respectively), participants expressed support/opposition for them using single items (6-point Likert-type, Supplemental Appendix B). They were asked to define each model, and to comment on similarities and differences between each model and the NDM (open-ended, see Supplemental Appendix B).
Intervention views
Participants completed the Autism Intervention Attitudes Scale-General (AIAS-G) measuring support for different intervention goals using six Likert-type-scale response options (Baiden et al., 2024). The AIAS-G version administered in this study was adapted and edited to focus on a wide variety of autism intervention goals. In the same sample included in this study, Hersh et al. (2024) previously explored the dimensional structure of 35 AIAS-G items using exploratory graph analysis (Golino & Epskamp, 2017), finding five subscales: normalization (nine items), adaptive skill (eight items), well-being (six items), societal reform (five items) and supportive environment (five items) goals; two items were discarded. Item-level descriptive statistics and comparisons of autistic and non-autistic participants are presented in Supplementary Table C.3.
In addition, participants answered single-item questions about who should choose intervention goals (autistic people who can communicate, professionals, parents, autistic adult consultants) and whether spoken communication should be prioritized over other forms. Their views on curing, teaching useful skills to and making the world more supportive for people with anxiety, depression and epilepsy were solicited; they were also asked whether no intervention was needed for those conditions, and whether the appropriate approach varied between challenges (details in Supplemental Appendix B).
Qualitative content analysis
Data from open-ended questions were analysed using content analysis (Hsieh & Shannon, 2005; Kondracki et al., 2002). In general, our approach was inductive, though we endeavoured to make coding schemes comparable across questions where possible. However, related to our investigation of Hypothesis 3 regarding the ‘strong’ SM, some codes were formulated deductively, in order to explore the following:
1.Who defines an SM of disability in a ‘strong’ way, by focusing only on the role of society in disabling people, excluding individual contributions to disability?
(a) Which participants only support interventions and supports that aim at changing society and not interventions focusing on the individual?
2.Which people believe the NDM entails an SM of disability?
(a) And which people believe that it entails a ‘strong’ SM, one that excludes: individual contributions to disability and/or interventions focusing on the individual?
Questions regarding definitions of neurodiversity and the NDM, SM and MM were coded by P.D. and S.K.K. and those regarding similarities and differences between the NDM and the SMs and MMs were coded by A.N.G. and E.K. Each pair drafted coding schemes, which were circulated to all authors for edits, after which pair members separately coded 20% of the responses for each question; inter-rater agreement of 80% or higher was required for each code. Coders were blinded to participants’ autism status and other characteristics (unless these were disclosed in responses to the open-ended questions being coded). After reliability was attained, the remaining responses were coded by a single coder.
Quantitative analyses
Because of the non-normal and skewed distributions of many variables (e.g. see Figures 2 and 3, Supplementary Figures C.1–C.6), we used ordinal statistics.
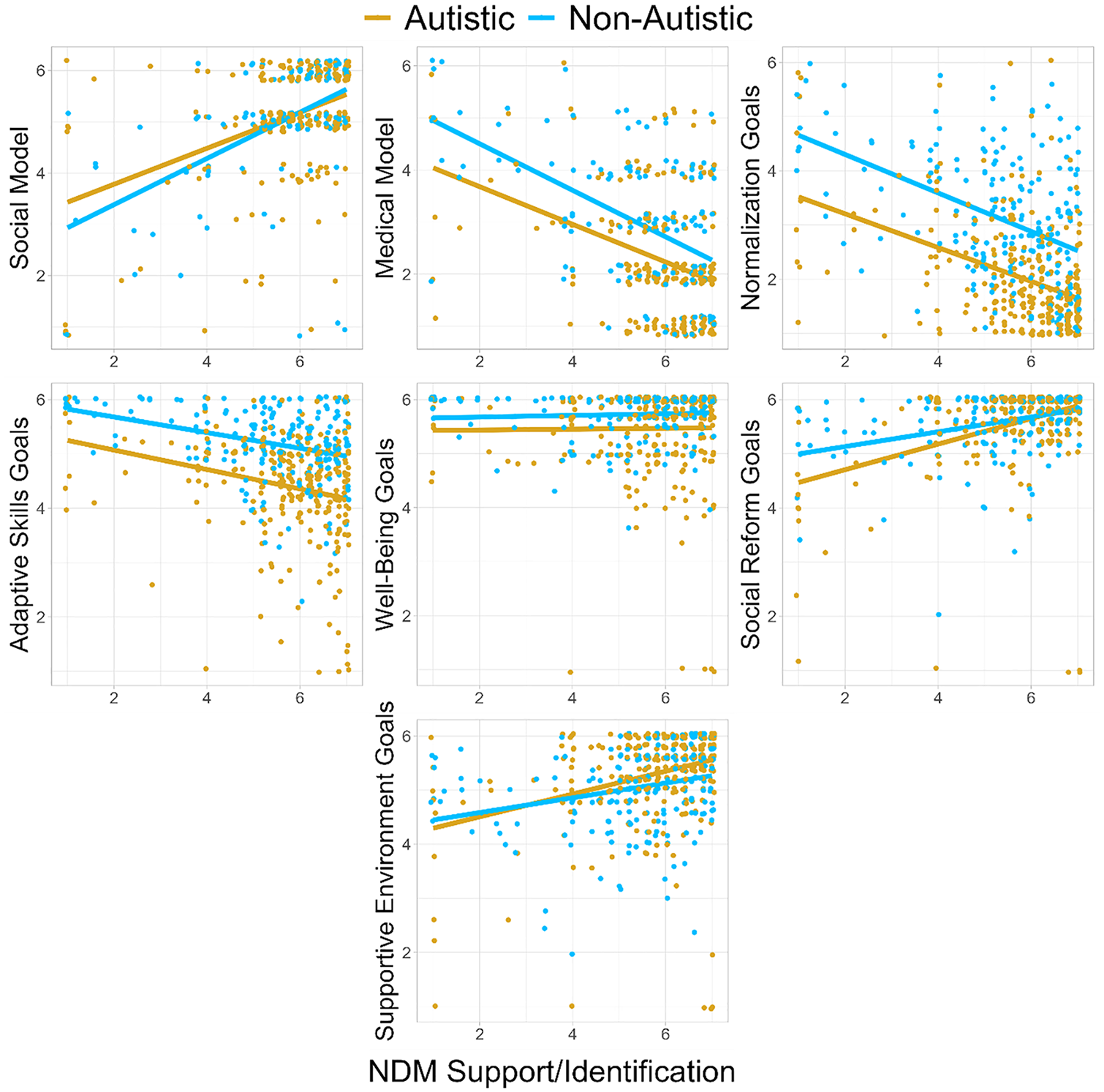
Linear slopes representing associations between NDM support/identification and support for the SM, the MM and AIAS intervention goal types, separately for autistic and non-autistic participants.
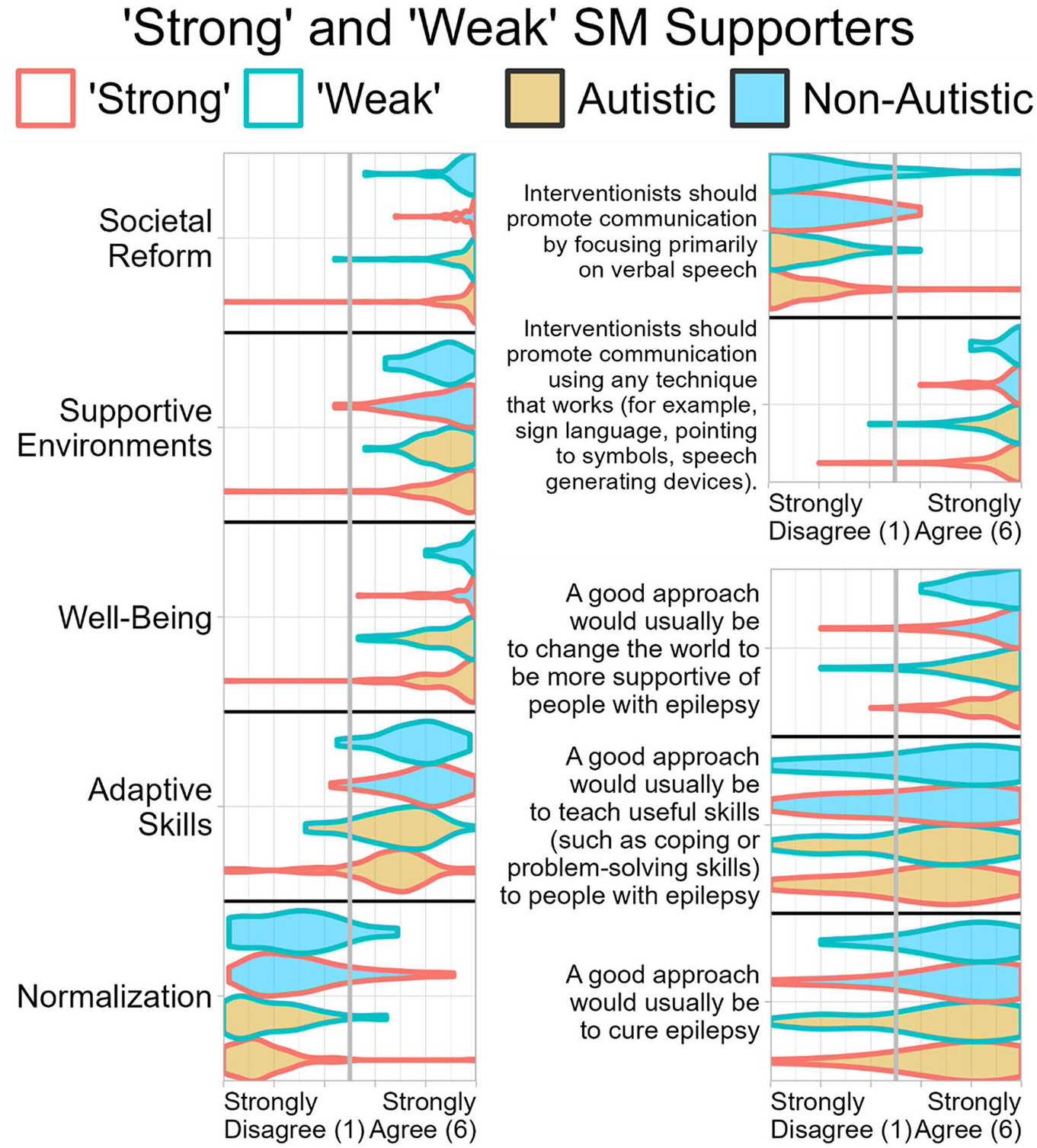
Violin plots depicting ratings of intervention goal types from the AIAS (left), approaches towards promoting communication (top right) and, as an example, co-occurring condition of interventions for people with epilepsy (bottom right), as a function of whether participants identified as autistic and whether their open-ended descriptions of the SM followed ‘strong’ understandings, in which society alone constructs disability (n = 159) or ‘weak’ understandings, with interacting societal and individual contributions creating disability (n = 71).
Direct comparisons of participants from two groups (e.g. autistic and non-autistic participants) used Wilcoxon–Mann–Whitney tests with Cliff’s delta (Cliff, 1993; Torchiano, 2022) as an effect size. Comparisons of one group’s responses to ‘neutral’ responses (i.e. scores reflecting neither agreement nor disagreement) used one-sample Wilcoxon tests. False discovery corrections (Benjamini & Hochberg, 1995) were applied to each table of comparisons.
We used scaled, ranked regression to examine whether NDM support/identification scores (on the measure adapted from Nario-Redmond et al. (2013)) predicted SM, MM and AIAS intervention goal endorsement. This was analogous to using Spearman’s correlations, but allowed us to include autistic/non-autistic group (entered into analysis as sum-coded contrast factor) and its interaction with NDM support/identification, to control for group differences, and to determine whether group differences could be accounted for by NDM/support identification. We also used scaled, ranked regression when examining effects of multiple categorical variables simultaneously. False discovery corrections were applied to each table of comparisons.
Supplementary, exploratory comparisons of code endorsement frequencies across autistic and non-autistic participants are reported with both logistic regression and Fisher’s exact tests. No multiple comparison correction was applied to these exploratory analyses.
Community involvement
This study team was highly neurodiverse. All authors primarily responsible for coding qualitative data presented in this article (i.e. P.D., E.K., S.K.K. and A.N.G.) are autistic. Several other authors identify as non-autistic, albeit often with close family and other personal ties to autism. This project did not involve any participatory research methodology (e.g. community-based participatory research) with non-academic community members.
Results
Almost all participants had heard of neurodiversity (98.92% autistic, 95.58% non-autistic), and most had heard of the SM (79.86% autistic, 53.54% non-autistic) and MM (78.42% autistic, 65.02% non-autistic). Autistic people were more likely to have heard of each, p ⩽ 0.03 (see Supplementary Table C.1).
Autism identification in relation to views on neurodiversity, disability models and intervention
Hersh et al. (2024) previously examined whether being autistic versus non-autistic predicted NDM, SM, MM and intervention goal support in this dataset (see also Supplementary Table C.2; single items in Supplementary Table C.3). 4 Here, we further examine this question in subgroups: among parents/caregivers, other family, professionals and researchers (see Supplementary Tables C.4–C.7), finding results generally similar to those in the full sample (see Supplementary Table C.2). However, differences in viewpoints based on autism identification were most apparent among parents/caregivers. For example, autistic parents/caregivers endorsed the SM more than non-autistic parents/caregivers, but differences in SM support between autistic and non-autistic participants were not apparent among other family members, professionals, or researchers. Similarly, only autistic parents/caregivers rated well-being goals significantly lower than non-autistic parents/caregivers (likely reflecting concerns about how those goals would be pursued 5 ); differential ratings of well-being goals for autistic participants were not observed for other subgroups.
Means and group comparisons from additional single-item questions are presented in Supplementary Tables C.8–C.12. Interestingly, autistic participants – including autistic parents/caregivers and professionals, respectively – much less often endorsed parents and trained professionals having leading roles in setting intervention goals, and more often supported involvement of autistic consultants in developing goals for young children. Autistic participants also less often supported promoting communication primarily through verbal speech.
Views on intervention objectives for co-occurring conditions (anxiety, depression and epilepsy) were overall similar across groups, but autistic participants sometimes favoured efforts to make a supportive world more than non-autistics, and were sometimes more sceptical of cure- or skill-building-oriented interventions (see Supplementary Tables C.13–C.17).
Correlates of NDM support
To examine our first hypothesis – that neurodiversity support would be associated with decreased endorsement of normalization/behaviour reduction intervention goals, but not with altered endorsement of adaptive skill and well-being goals – we used scaled, ranked regression to investigate associations between NDM support/identification and AIAS subscale scores.
NDM support/identification predicted greater support for the SM and for societal reform and supportive environment intervention goals, corrected p < 0.0001 (see Figure 2; Supplementary Table C.18). It also ordinally predicted greater support for well-being intervention goals, p = 0.004. NDM support/identification predicted reduced endorsement of the MM and normalization and adaptive skills intervention goals, p < 0.0001.
In relation to the second hypothesis (that autistic neurodiversity supporters would be less susceptible to ‘neurodiversity lite’ rhetoric and therefore would be more enthusiastic about societal reform than non-autistic neurodiversity supporters), autistic and non-autistic people did not statistically differ in endorsement of societal reform and supportive environments when accounting for NDM support (see Supplementary Table C.18). However, autistic participants continued to endorse the MM and normalization, adaptive skill, and well-being intervention goals less than non-autistics in models that included NDM support, p ⩽ 0.0001 (see Supplementary Table C.18): thus, autistic people tended to like these goals less even when compared to non-autistics who considered themselves equally NDM-supportive. Autism status and NDM support/identification did not interact significantly, uncorrected p ⩾ 0.13 (see Supplementary Table C.18).
NDM support/identification was related to greater endorsement of autistic people playing a leading role in setting intervention goals, and involving autistic consultants when interventions are for young children, as well as of promoting communication using any technique. NDM support/identification was associated with reduced support for parents and professionals playing leading roles and for focusing primarily on verbal speech (see Supplementary Table C.19, Supplementary Figure C.3). Neurodiversity support/identification predicted robustly greater enthusiasm for making the world more supportive for people with anxiety, depression and epilepsy, and modestly reduced support for curing those conditions (Supplementary Table C.20, Supplementary Figures C.4–C.6). Interestingly, NDM supporters – at least among autistic participants – were slightly less likely to state people with anxiety did not face challenges or need support, although few participants expressed that opinion.
Open-ended responses
Open-ended responses are summarized in greater detail in Supplemental Appendix E, which presents coding schemes, frequencies of code endorsement and illustrative quotations (see Supplementary Tables E.1–E.8). A subset of codes is briefly narratively summarized below.
Definitions of neurodiversity
‘Neurodiversity’ was typically understood as a descriptive term (81.06%), referring to neurocognitive diversity in everyone (54.38%) or neurodivergent people (25.46%; see Supplementary Table E.1). However, some definitions implied neurodiversity is an inherently value-laden and prescriptive term (29.33%) and, in that vein, many responses suggested it values diversity (30.75%). Most respondents referred to biology/neurobiology (63.34%) and many alluded to cognition/perception (31.57%); behaviour was seldom mentioned (9.57%).
Definitions of the NDM
The NDM was almost universally understood as prescriptive (96.10%), though exploratory comparisons suggested autistics (66.18%) were more likely than non-autistics (55.81%) to suggest it advocates for neurodivergent people (vs autistic people or all humans), uncorrected p = 0.02 (see Supplementary Table E.2). More non-autistic (65.12%) than autistic (51.84%) participants talked about the NDM accepting/valuing differences, p = 0.003, whereas more autistic (60.66%) than non-autistic (48.84%) participants, p = 0.009, discussed the NDM changing society – notably, through seeking rights (15.81% autistic, 6.51% non-autistic, p = 0.002) and opposing stigma/discrimination (11.76% autistic, 4.65% non-autistic, p = 0.007). Furthermore, autistic people (22.79%) more often than non-autistics (14.42%), p = 0.02, suggested that the NDM promotes the thriving of neurodivergent people. Across neurotypes, around a quarter of participants suggested the NDM opposes pathologization (27.10%).
Definitions of the SM
Participants overwhelmingly agreed the SM postulates society is involved in causing disability (84.71%; see Supplementary Table E.3). Most participants provided ‘strong’ definitions of the SM, indicating society constructs disability (60.29%), but some suggested society causes most issues (11.47%) or exacerbates issues (6.47%), or that person–environment misfit causes disability (4.41%). Participants frequently mentioned the SM’s focus on structural/systemic issues, such as barriers, inaccessibility, lack of supports and social norms (68.53%), and some respondents discussed oppression faced by disabled people (19.71%). Many suggested the SM rejects medicalization/pathologization (34.41%).
Definitions of the MM
Most participants indicated the MM postulates that individuals’ own characteristics contribute to disability (58.68%); indeed, ‘weak’ forms of the MM, with societal factors also contributing, were rarely described (2.48%; see Supplementary Table E.4). Disability in the MM was often described as rooted in biology (24.52%). Participants described the MM as a pathology-based viewpoint (68.60%), suggesting it argues intervention should change individuals (49.04%), including through cure/normalization (43.53%).
Similarities of NDM and SM
Many participants suggested the NDM and SM share common goals and attitudes (52.44%), such as promoting accessibility (27.44%) and inclusion and acceptance (38.11%; see Supplementary Table E.5). Some responses indicated that NDM and SM share a ‘strong’ view that disability is socially constructed (19.21%). The models were described as agreeing that disability is neutral (12.80%)/not negative (11.59%). Some responses suggested that NDM emerged from the SM (15.55%).
Differences between the NDM and SM
Some participants simply denied the existence of differences between the NDM and SM (18.94%; see Supplementary Table E.6). Others suggested they have different goals and attitudes (15.28%): for example, the SM advocates more for accommodations (3.67%), or the NDM advocates more for acceptance/inclusion (6.98%). The SM was noted to apply to more disabilities/diagnoses (13.00%). Certain responses suggested that NDM is practical/applied and the SM philosophical/theoretical (8.97%). Notably, some participants suggested the models have different views on the origin of disability (19.27%), with the NDM recognizing medical needs that cannot be addressed through societal reform (12.96%) or accepting both individual and societal contributions to disability (9.30%), in contrast to an SM in which disability is socially constructed (8.97%).
Similarities between the NDM and MM
Numerous responses asserted the NDM and MM are not similar (46.89%; see Supplementary Table E.7). However, some suggested they have common goals and attitudes (33.62%): for example, recognizing the reality of differences, disability and challenges (14.41%), advocating for supports/intervention (9.04%), ascribing biological origins to disability (7.91%), and acknowledging medical needs (4.24%). A few responses commented on their shared propensity for dividing the world into typical/divergent binaries (4.24%).
Differences between the NDM and MM
Most respondents felt that goals and attitudes of the NDM and MM were dissimilar (56.82%) in terms of their acceptance of diversity (12.50%), endorsement of societal reform (23.01%) and desire to change individuals (38.07%; see Supplementary Table E.8). Regarding the latter, responses suggested cure/prevention is promoted by the MM (20.17%) and opposed by the NDM (10.80%), and that treatment/intervention is promoted by the MM (22.44%) and opposed by the NDM (5.11%). Participants also commented on the models’ different views of deficits/strengths differences (43.75%), with many indicating the MM pathologizes differences (28.98%) but that the NDM does not (30.68%). Some described disability arising in the individual in the MM (7.10%) but being socially constructed in the NDM (7.39%). Certain respondents simply suggested that NDM and MM are completely different (13.07%).
Qualitative–quantitative triangulation
To examine our third hypothesis –that many participants claiming to support the ‘strong’ SM would express views that seem inconsistent with it, potentially confusing debates regarding neurodiversity and making it more difficult to resolve disagreements – we defined ‘strong’ SM supporters as the subset of participants (108 autistic, 51 non-autistic) who quantitatively supported the SM and described it in ‘strong’ terms, with societal and not individual characteristics constructing disability (see Supplemental Appendix D for details). One-sample Wilcoxon tests examined whether their support for AIAS intervention goals differed from neutrality (scores of 3.5: between ‘Slightly Disagree’ and ‘Slightly Agree’); this was also done for single items regarding conventional, speech-oriented versus atypical/augmentative/alternative approaches to promoting communication and single items regarding person- versus societal-oriented interventions for anxiety, depression and epilepsy (see Figure 3).
Overall, ‘strong’ SM-supporting participants had more-negative-than-neutral views of AIAS normalization intervention goals and of focusing primarily on verbal speech over other forms of communication, p < 0.0001 (see Figure 3, Supplementary Tables D.1, D.4). However, they had more-positive-than-neutral opinions towards AIAS adaptive skills intervention goals; curing depression and epilepsy; and teaching useful skills to people with anxiety, depression and epilepsy, p ⩽ 0.002, even though these involve changing the individual, seemingly contrary to the ‘strong’ SM’s sole focus on society. ‘Strong’ SM-supporting participants also enthusiastically supported AIAS well-being, societal reform, supportive environment goals and changing the world to be more supportive of people with anxiety, depression and epilepsy, p < 0.0001. Similar results held among autistic and non-autistic participants separately (see Supplementary Tables D.2, D.3, D.5 and D.6), although non-autistic ‘strong’ SM supporters’ views on curing depression did not significantly depart from neutrality. Identical patterns of statistical significance were obtained when analyses incorporated information from responses to ND/NDM questions to better classify participants as having ‘strong’ (84 autistic, 39 non-autistic) views or not (see Supplementary Tables D.7–D.12).
We also used scaled, ranked regression (controlling for differences between autistic and non-autistic participants) to compare ‘strong’ SM supporters to participants who supported a ‘weak’ SM (44 autistic, 27 non-autistic). We found no statistical differences between ‘strong’ and ‘weak’ supporters in their views on AIAS intervention goals, spoken versus any communication items and person- versus societal-focused intervention items for epilepsy, anxiety and depression, corrected p ⩾ 0.17 (see Supplementary Tables D.1, D.6), though before correction there was a tendency for ‘strong’ supporters to be more enthusiastic about supportive environment goals, uncorrected p = 0.03. Similar results were obtained when ND/NDM questions were used to better classify participants as having ‘strong’ or ‘weak’ views (see Supplementary Tables D.7–D.12).
Discussion
This study used mixed methods to richly characterize understandings of neurodiversity and models of disability in a large sample of autism community members. As previously reported by Hersh et al. (2024), participants generally supported the NDM and SM of disability, while opposing the MM. Participants were also highly aware of neurodiversity, and high awareness of neurodiversity has previously been linked to support for NDM-aligned views (Kapp et al., 2013).
Social construction of disability
One of the key topics investigated here is autism community members’ views on the social construction of disability. Many critiques of the NDM connect it to the SM, arguing that the ‘strong’ SM’s denial of individual characteristics’ disabling effects is inappropriate for some or all autistic people (J. A. Hughes, 2021; Nelson, 2021).
Some of this study’s participants were not familiar with the SM, but among those who were, the SM was generally seen as similar to the NDM. Moreover, most supported the SM and provided ‘strong’ definitions of it, noting society’s construction of disability without recognizing an influence of individual characteristics. While a considerable minority put forward ‘weak’ definitions, remaining open to the possibility individuals’ characteristics might have disabling effects independent of society, one might be tempted to conclude from solely quantitative data that NDM critics’ concerns are justified.
However, when open-ended responses about neurodiversity/the NDM were considered (not just those about the SM itself), the number of responses expressing ‘strong’ and ‘weak’ views became roughly even. Even more crucially, as per our third hypothesis, ‘strong’ SM supporters were generally comfortable with interventions aiming to change people by teaching adaptive skills. Furthermore, most ‘strong’ SM supporters endorsed curing depression and epilepsy. At first glance, it might seem contradictory for people who deny individual characteristics a role in disability to then support interventions to change these characteristics. Several interpretations seem possible.
First, although ultimately viewing society as responsible, and desiring a societal solution, ‘strong’ SM advocates might be open to individual-focused interventions, at least in some contexts, due to the difficulty of reforming society.
Second, participants might support ‘strong’ SM views only in relation to particular disabilities or characteristics (Ne’eman & Pellicano, 2022), with adaptive skills, depression and epilepsy falling (wholly or partly) outside the scope they perceive for the SM, or perhaps outside the scope of the traits/conditions coming to mind as disability-relevant.
Third, not all people who use and endorse the ‘strong’ SM may understand theoretical distinctions between the ‘strong’ and ‘weak’ SM, or these distinctions may seem academic and unimportant in their daily lives. They may be advocating for societal reforms without intending to deny the importance of biological and cognitive differences between people. If so, ‘strong’ SM rhetoric could risk misrepresenting its adherents’ actual views on concrete issues.
Supporting the third interpretation, ‘strong’ SM supporters were, after correction, statistically indistinguishable from ‘weak’ supporters when compared on various items and subscales indexing support for individually versus societally oriented interventions, perhaps implying that their ‘strong’ SM rhetoric masks ‘weak’ SM views. Due to the small number of ‘weak’ supporters, this result should be treated with caution – but these results do at least seem to suggest that any possible difference in views would be of modest magnitude. Thus, it seems clear that ‘strong’ SM rhetoric is something of a distraction, and that in practice, most of its adherents in the autism community remain open to individually focused interventions and supports, used appropriately and judiciously.
That said, one should not conclude this means the SM is irrelevant/facile. Efforts to develop and study autism interventions have overwhelmingly focused on changing autistic individuals, rather than society (Bottema-Beutel et al., 2018; Broderick & Roscigno, 2021; Scott et al., 2019), and currently, autism is diagnosed within a framework that assumes disability/impairment is rooted in the person, largely ignoring context (American Psychiatric Association, 2013); the SM is well-positioned to critique these realities. Moreover, SM supporters staunchly opposed normalization goals from our adapted AAIS. Thus, even a ‘weak’ SM can be transformational.
Understandings of neurodiversity and the NDM
This study also explored qualitative views of neurodiversity/the NDM and quantitative correlates of NDM support/identification. As we predicted in our first hypothesis, NDM support was associated with greater opposition to normalization intervention goals, but not endorsement of well-being intervention goals. However, contrary to our hypothesis, greater NDM identification was related to decreased support for adaptive skill intervention goals (we had expected no relationship). However, NDM supporters in this study generally reported some support for these adaptive skill goals, arguably in keeping with our hypothesis’ spirit. Participants simply became less enthusiastic about them as their support for the NDM increased. As several adaptive skill scale items concerned social/interpersonal challenges, this might relate to insightful neurodiversity-aligned critiques of social skills training (Autistic Self Advocacy Network, 2021; Bottema-Beutel et al., 2016, 2018).
NDM support was positively associated with support for societal reform and building supportive environments. It was also associated with support for making the world better for people with anxiety, depression and epilepsy – yet only slightly associated with scepticism towards efforts to cure these conditions – emphasizing that pursuit of cure and pursuit of societal reform can, if appropriate, be pursued simultaneously (see Baker, 2011). NDM support was associated with enthusiasm for promoting communication through any effective method rather than prioritizing verbal speech (consistent with Schuck et al., 2022) and with support for autistic leadership and consultancy in intervention decision-making, and reduced support for leadership from parents and professionals.
Few quantitative studies compare experiences of autistic and non-autistic parents, and to our knowledge, this is the first to directly compare views on important political questions such as acceptability of intervention goals and views on who should make decisions in interventions. Autistic parents/caregivers were considerably less supportive of parent leadership in intervention development than non-autistic parents/caregivers. This may reflect advocacy-oriented approaches to parenting among autistic parents/caregivers, as they were also more supportive of the SM and the NDM than their non-autistic counterparts. Autistic parents’ support for child autonomy over parent leadership may also help address concerns that autistic/neurodiversity advocacy leads to ‘parent-blaming’ (Lutz, 2020; Mitchell, 2019). While ‘autism parents’ often do face immense stress and make sacrifices (Hayes & Watson, 2013; Hellman, 2022; Naughton, 2021), these data suggest neurodiversity advocates’ concerns about child autonomy and parents’ power are shared by autistic people who are autism parents themselves (see Crane et al., 2021; Dugdale et al., 2021; Hwang & Heslop, 2023). (Predominantly non-autistic) family/carer perspectives and agency have generally been dominant over autistic people’s in-media portrayals (Holton, 2013; Karaminis et al., 2023; Lewin & Akhtar, 2021); there remains room to address this neglect without dismissing caregivers’ perspectives.
Open-ended questions provided intriguing information regarding conceptualizations of neurodiversity and the NDM. Although most participants’ definitions of ‘neurodiversity’ framed it as a descriptive term referring to the neurocognitive diversity of humanity, value-laden/prescriptive understandings were also common, as suggested by Ne’eman and Pellicano (2022). This is consistent with the term’s history of being used to suggest that neurological diversity can be neutral or positive (Blume, 1998; Langdon, in Dekker, 2023; Singer, 2016).
Participants usually understood neurodiversity as neurological/biological, similarly to prior research on understandings of autism’s origins (Gillespie-Lynch et al., 2017; Kapp et al., 2013). This may seem consistent with assumptions by some MM adherents that autism has knowable biological markers (Parellada et al., 2023; Shen et al., 2019). However, the high levels of SM and NDM support observed in this study highlight how biological views of the origin (‘etiology’) of human neurocognitive diversity need not prevent people from recognizing societal factors that can contribute to challenges neurodivergent people face. Moreover, in a new measure of neurodiversity beliefs, items about autism’s permanence and neurobiological ‘hard-wiring’ converge with an item rejecting the possibility of curing autism (VanDaalen et al., 2024): apparently, some essentialist biological understandings of neurocognitive differences can motivate rejection of the traditional MM’s cure/prevention agenda (see also Ellis, 2023). However, autism is biologically and causally (‘etiologically’) heterogeneous (Havdahl et al., 2021; Myers et al., 2020). Thus, some NDM leaders and scholars reject biological essentialism and emphasize the social construction of many neurotype categories, including autism (e.g. see Chapman, 2020b; Milton in Milton & Timimi, 2016).
Many autistic/autism community participants’ definitions of neurodiversity referred to cognitive/perceptual aspects, which may help to avoid this tension within biological focuses. Indeed, an interest in cognition has helped autistic people develop descriptive cognitive frameworks to help make sense of their experiences (see, e.g. Buckle et al., 2021; Dekker, 1999; Milton & Timimi, 2016; Murray et al., 2005).
In contrast to this emphasis on biology and cognition, participants’ answers seldom mentioned behaviour, though it is used to diagnose autism, attention-deficit hyperactivity disorder (ADHD), and other neurodivergent categories (American Psychiatric Association, 2013). This is consistent with autistic people’s tendency to define autism in an internal way (Gillespie-Lynch et al., 2017).
Autistic and non-autistic people and ‘neurodiversity lite’
In our second hypothesis, we predicted that autistic neurodiversity proponents would focus more on environmental and societal barriers, and support for interventions capable of changing them, than non-autistic neurodiversity proponents. Admittedly, when prompted, autistic and non-autistic participants both endorsed societal reform and supportive environment-building intervention goals; their quantitative ratings did not differ. Yet in exploratory comparisons of autistic and non-autistic participants’ free-text descriptions of the NDM, autistic participants spontaneously mentioned efforts to reform society and promote neurodivergent thriving more often, while non-autistic participants spontaneously appeared more focused on the NDM’s celebration of diversity. This is consistent with concerns that some non-autistic people are (perhaps unknowingly) co-opting the NDM by advancing ‘neurodiversity lite’ ideas (Neumeier, 2018).
Also consistent with that concern are findings suggesting that non-autistic people were – even after accounting for neurodiversity support – less sceptical of various intervention goals, including normalization- and adaptive skill-oriented interventions. Thus, some non-autistic neurodiversity proponents may not have fully appreciated concerns about the harms arising from efforts to suppress autistic traits (see, e.g. Anderson, 2023; McGill & Robinson, 2021).
At the same time, these differences should not be overemphasized. Overall, our data revealed remarkable consensus among participants in this sample, and the overlap between autistic and non-autistic participants was extensive. Even if some degree of co-option of neurodiversity ideas could be reflected in our data, our data overall clearly depict meaningful agreement and allyship between autistic and non-autistic advocates.
Limitations
Although this mixed-methods study offers a rich and nuanced examination of key issues in autistic and autism communities, it is not without limitations. The study describes views and conceptualizations of neurodiversity and models of disability in a predominantly White, well-educated sample of autism community members, mostly from wealthy Anglophone countries. Different ideas are being developed in other cultural contexts (Cheng et al., 2023; Kapp, 2011; Ngwagwa, 2022) and more intersectional and cross-cultural analysis of the NDM is greatly needed. Moreover, language is not static, and NDM advocates – especially neurodivergent advocates – will continue to advance new ideas. Thus, these results are not a definitive idea of what the NDM is or could be.
This study’s autistic sample included few individuals with higher support needs: for example, only seven autistic people with intellectual disabilities and five nonspeaking autistic people. Ironically for a study about the NDM and SM, our efforts to collect highly rich, nuanced data reduced the accessibility of the study. Obtaining perspectives from across the diversity of autism is a crucial direction for further research.
Finally, although we attempted to direct recruitment invitations to organizations and communities from across the spectrum of ‘autism politics’ opinion, neurodiversity proponents appeared more likely to participate. Thus, while the data depict consensus in favour of the NDM and societal reform, and strong opposition to normalization and the MM (which could reflect growing awareness of the NDM: see Kapp et al., 2013), this may not be representative of the autism community overall.
Future directions
To address these limitations, one direction for future research could be to examine whether this study’s results hold true in samples recruited using other approaches: for example, sampling online databases such as Prolific, recruiting in-person in local communities, engaging marginalized populations within wealthy Anglophone countries (e.g. indigenous nations, socioeconomically deprived locales) or focusing recruitment on other countries. New studies would also allow our interpretations of this study data to be turned into explicit propositions, so that one could investigate the degree to which community members agree with the interpretations put forth in this article.
Another important direction for future research will be clarifying the acceptability of specific discourses and practices. For example, given the large number of socially relevant items on the adaptive skills scale, these findings suggest ‘teaching adaptive skills’ such as social-communication skills may be acceptable in principle, especially when done mutually with interaction partners (Milton, 2012). Yet our results and prior investigations of the acceptability of social skills training (Bottema-Beutel et al., 2016) and Pivotal Response Treatment (Schuck et al., 2022) show that this by no means guarantees that key practices will be endorsed by community members (e.g. concerns about normalization and lack of child autonomy; Autistic Self Advocacy Network, 2021). Experiences of misunderstanding, stigma and bias from professionals and educators (e.g. see Brownlow et al., 2021; Darazsdi & Bialka, 2023; McGill & Robinson, 2021) could also adversely affect the actual acceptability of supports. Furthermore, because of the paramount importance of customizing supports to the needs and perspectives of individuals (and, as appropriate, their supporters), tools should be developed to help individuals (and, as appropriate, representatives such as family members) make meaningful choices about supports, goals and practices in their own contexts.
Conclusion
Notwithstanding limitations and associated calls for follow-up research, we believe our results provide some of the most comprehensive available evidence today regarding what neurodiversity, the NDM, and the SM of disability mean to supporters in the autistic and autism communities. Those with concerns about the NDM or SM should read these results carefully and ensure that any critiques they offer describe NDM and SM advocates’ views accurately. If debates remain free of mischaracterizations or false stereotypes, it will be easier for NDM supporters and their critics to make progress in discussions about genuine disagreements. In particular, this study suggests that SM rhetoric masks the more nuanced views most of its adherents have on concrete questions regarding intervention goal appropriateness. It indicates that neurodiversity supporters denounce normalization, and can be open to curing co-occurring conditions and teaching adaptive skills; future research and debate could continue to explore how the latter could be pursued in neurodiversity-affirmative and socially valid ways.
Furthermore, although our study was not designed to determine how common neurodiversity-affirming views are within the autistic and autism communities, participants’ clear enthusiasm for the NDM does suggest that improving access to neurodiversity-affirmative supports is necessary to serve increasing numbers of neurodiversity-supporting community members. In addition to confirming that self-identified neurodiversity supporters are generally opposed to interventions aiming to suppress and normalize autistic traits and behaviours, this study directs attention towards the importance of power dynamics, with neurodiversity supporters desiring additional prioritization of autistic leadership and involvement. Thus, interventions and supports reflecting these preferences must be made available to neurodiversity-supporting individuals and families. Moreover, though there were some differences between autistic and non-autistic respondents (including autistic and non-autistic parents), there were relatively few/modest differences overall: all groups expressed strong, striking desires for societal reform and efforts to make the world more inclusive of autistic and neurodivergent people.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241273029 – Supplemental material for Community views of neurodiversity, models of disability and autism intervention: Mixed methods reveal shared goals and key tensions
Supplemental material, sj-docx-1-aut-10.1177_13623613241273029 for Community views of neurodiversity, models of disability and autism intervention: Mixed methods reveal shared goals and key tensions by Patrick Dwyer, Ava N Gurba, Steven K Kapp, Elizabeth Kilgallon, Lynnette H Hersh, David S Chang, Susan M Rivera and Kristen Gillespie-Lynch in Autism
Footnotes
Acknowledgements
We warmly thank our participants for taking the time to take part in this study. We also thank Emily J. Goldknopf for helpful advice regarding visualization of theoretical models.
Author Contributions
P.D., S.K.K., K.G.-L. and S.M.R. designed this study. Recruitment was conducted by S.K.K., P.D. and K.G.-L. P.D. and D.S.C. coded and removed invalid data. P.D., A.N.G., E.K. and S.K.K. coded data from the open-ended questions presented in this report. Quantitative analysis was conducted by P.D., with contributions from L.H.H. This article was drafted by P.D. and edited and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the UC Davis MIND Institute. P.D.’s time was partially supported by an Autism Speaks / Royal Arch Masons CAPD Fellowship. L.H.H.’s time was partially supported by a UC Davis Dean Keith Simonton research award.
Positionality Statement
The authors identify as supporters or allies of the neurodiversity movement.
P. D. is a White Canadian autistic autism researcher, a neurodiversity advocate, and a supporter of social-ecological/interactionist models of disability. P.D.’s main research focus is neurodivergent sensory experience, his background is in developmental and cognitive science, and he is broadly interested in many factors relevant to neurodivergent people’s well-being.
ANG is a White, cisgender neurodivergent and disabled woman from the United States, a disability and neurodiversity advocate and autistic autism researcher. She also has cerebral palsy and mental health disabilities, which she also sees as important identities within the neurodiversity movement. She has a Master’s degree in neuroscience but is currently working in many areas of autism research, including neurodiversity-affirming interventions and supports, mental health in autistic people and autistic identity. Finally, she recognizes that her position is not reflective of all forms of oppression and experience, especially those faced by racial and ethnic minorities, those with LGBTQ+ identities, and those with disabilities that extend beyond her own experience.
S. K.K. is a White cisgender man, American and permanent UK resident, disability rights and neurodiversity activist, developmental psychologist and autistic autism researcher. S.K.K.’s research broadly considers the nature or meaning of autism and neurodiversity as well as means of supporting autistic and other neurodivergent people.
E. K. is a White, autistic autism researcher from the United States who supports the neurodiversity movement. She advocates for neurodiversity-affirming practices in interventions, education and research. Her autistic identity gives her some level of understanding of oppression (e.g. ableism), but recognizes that being a part of the dominant racial group, her privilege is a large part of her positionality. She tries to learn and listen to the BIPOC autistic community and is on a continuous journey of allyship and cultural humility.
D. S.C. is a Taiwanese-American educator from the United States with a background in autism research. D.S.C.’s work with children of diverse backgrounds within various educational contexts has guided his interest in researching the experience of neurodivergent individuals. He works to continue building a perspective of allyship and cultural responsiveness in both research and education.
SMR is a White, LatinX researcher from the United States. Her research investigates questions about how underlying brain activity and behaviour supports the development of skills (e.g. attention, visual perception, sensory processing and emotion regulation) necessary for adaptive cognition and social-emotional well-being. In addition to this scientific work, she is also committed to championing the tenets of neurodiversity and advocacy to the public and the academic community.
K. G.-L. is a White, bisexual woman from the United States. She was very briefly in special education in kindergarten, purportedly due to skipping in an unusual way, before being moved into a gifted group. She experiences some executive functioning and social differences but has not been diagnosed with a disability. She has many neurodivergent family members and close friends.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.