
Abstract
There is a significant variability in the prevalence of psychotropic medication use among young autistic persons worldwide and this is under-studied in Australia. Apart from risperidone, approved by the Therapeutic Goods Administration to manage challenging behaviour, the appropriateness of other psychotropic medications prescribed to young autistic persons warrants scrutiny. This retrospective study aims to gain initial insight into the magnitude, types and indications of psychotropic medication use in autistic children and adolescents in Western Australia. We analysed de-identified data from 239 autistic children and adolescents (⩽21 years) who participated in the Western Australian Autism Biological Registry between 2011 and 2015 and who completed a questionnaire regarding medication use. One-quarter (n = 66, 28%) of young autistic people reported using a total of 137 medications. Most (n = 46, 70%) of those medicated were under 12 years of age; half (n = 33) were 6–12 years and a fifth (n = 13) were under 6 years. The most used medications were stimulants (n = 35, 53.0%), followed by antidepressants (n = 24, 36.4%), antiepileptics (n = 21, 31.8%), sedatives (n = 15, 22.7%) and antipsychotics (n = 14, 21.2%). These medications were mainly to manage attention deficit hyperactivity disorder, challenging behaviours, seizures, insomnia, undefined anxiety, depression and mood instability. While most autistic young people in the Western Australian Autism Biological Registry did not report using psychotropic medication, over a quarter were prescribed medications, primarily stimulants, to manage symptoms of attention deficit hyperactivity disorder. Various medications, including risperidone, were used to help manage challenging behaviours. Medication use should be studied more comprehensively in a larger cohort of autistic persons to confirm our current preliminary observations. Further, future studies should monitor the effectiveness and safety outcomes of such medications due to a limited understanding of their effectiveness in managing the atypical presentation of co-occurring disorders in young autistic persons.
Lay abstract
Prescriptions and use of medications to treat mental health conditions in young autistic populations are inconsistent worldwide. This makes it hard to compare findings from international studies to the Australian autistic population, where there are limited relevant studies. Apart from risperidone, there are no other medications specified for direct use in autistic persons. This study aims to gain initial broad understanding of the use of medications, commonly prescribed for mental health conditions, specifically by autistics under the age of 21 years. We analysed data that were previously collected as part of the Western Australian Autism Biological Registry between 2011 and 2015 which amounted to 239 surveys completed on young persons with diagnosed autism. The questionnaires included information on co-occurring conditions, current or previous use of medications and reasons for use of the medications. Only one-quarter of the participants in this study reported using at least one mental health–related medication in their lifetime. The most reported medications were stimulants, antidepressants and antiepileptics. The reasons for using medication included managing attention deficit hyperactivity disorder, challenging behaviours, seizures, sleep difficulties and symptoms of anxiety and depression. The number of individuals reporting medication use in this study was lower compared to other developed countries. Nevertheless, these medications should be monitored due to limited understanding of their use to manage co-occurring symptoms in young autistic persons. The findings highlight the importance of ongoing research to better understand mental health–related medications and inform best practice.
Keywords
Introduction
Autism spectrum disorders (ASDs) are lifelong neurodevelopmental conditions typically detected during early childhood. Core autistic traits may result in differences in how young autistic persons communicate, self-regulate, socially interact and develop relationships (American Psychiatric Association, 2013). As many as 70% of young autistic persons have co-occurring mental health disorders, including anxiety, depression and attention deficit hyperactivity disorder (ADHD) (Lawrence et al., 2015; Leyfer et al., 2006; Simonoff et al., 2008; Whiteford et al., 2014). This prevalence appears to significantly differ in non-autistic populations, where the prevalence of mental health disorders is markedly lower, approximately ~7% (American Psychiatric Association, 2013; Lawrence et al., 2015; Simonoff et al., 2008). The core symptoms of ASDs and co-occurring mental health disorders negatively impact the wellbeing and quality of life of autistic children and adolescents due to their early onset and lifelong persistence (Bijl & Ravelli, 2000; Davis et al., 2010; Hess et al., 2010; Joshi et al., 2010; Lai et al., 2019; Lawrence et al., 2015; Leyfer et al., 2006; Rai et al., 2018; Simonoff et al., 2008; Strang et al., 2012; Volirath & Angst, 1989; Whiteford et al., 2014; Whitehouse et al., 2009).
Psychotropic medications are widely used in autistic children despite limited evidence from randomised controlled trials supporting their use and an absence of formalised clinical guidelines (Fergusson et al., 2005; Food and Drug Administration (FDA), 2003; Hammad et al., 2006; Nickels et al., 2008; Posey et al., 2008; Reddihough et al., 2019; Williams et al., 2013). Atypical antipsychotics, risperidone and aripiprazole are the only medications approved by the US FDA to explicitly manage irritability and maladaptive behaviours in autistic children and adolescents (Findling et al., 2014; FDA, 2006; Owen et al., 2009). In Australia, risperidone is the only pharmacological agent approved by the Therapeutic Goods Administration (TGA) and subsidised by the Australian government under the Pharmaceutical Benefits Scheme (PBS) for use in autism (The TGA, 1993). Risperidone is indicated for severe behavioural disturbances defined as aggression and injuries to self or others, where nonpharmacological methods alone have been unsuccessful in autistic children and adolescents (The TGA, 1993). The continued use of psychotropic medications is despite limited information on the safety and efficacy of psychotropic medication use in young autistic people (Jobski et al., 2017; Park et al., 2016; Siegel & Beaulieu, 2012; Solmi et al., 2020; Williams et al., 2013). Furthermore, the justification for prescribing psychotropic medications to autistic children is controversial because most evidence for psychotropic medication use has been from trials conducted in non-autistic populations (Brown et al., 2017; Chugani et al., 1999; Cipriani et al., 2018; Hahamy et al., 2015; Linke et al., 2017; Supekar et al., 2013; Wagner et al., 2003). Therefore, research findings from a non-autistic population may not be generalisable to neurodiverse individuals, since possible differences in neurology, brain and/or wiring have been reported (Brown et al., 2017; Chugani et al., 1999; Courchesne et al., 2001; Hahamy et al., 2015; Linke et al., 2017; Supekar et al., 2013).
Psychotropic medications are commonly prescribed to autistic children to manage symptoms characteristic of mental health disorders occurring in non-autistic individuals (Jobski et al., 2017; Langworthy-Lam et al., 2002). However, it is unclear whether prescribing on this basis is appropriate due to the atypical presentation of symptoms in autistic people (Cath et al., 2008; Coury et al., 2012; Kerns et al., 2014; Rosenberg et al., 2010; Russell & Sofronoff, 2005; Williams et al., 2013). For example, anxiety in autistic individuals may present typically and fulfil the criteria in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V) or may be related to autism traits, such as worry about disruption to routines, coping with change, confusion about social situations and sensory over-sensitivity or overstimulation (Kerns & Kendall, 2012; Ozsivadjian et al., 2012). Furthermore, anxiety-related symptoms such as repetitive behaviours and restricted interests may be associated with comfort, relief and enjoyment rather than distress in autistic individuals (Bearss et al., 2015; Cath et al., 2008; Kerns et al., 2014; Russell & Sofronoff, 2005). Therefore, with limited placebo-controlled trials examining psychotropic medication use in autistic children compared to non-autistic children, there is insufficient clinical evidence to justify such medication use in the autistic population (Sturman et al., 2017; Williams et al., 2013).
Most studies examining psychotropic medication use have been conducted in North America with limited research regarding the prevalence of psychotropic medication use in autistic children and adolescents in Australia. Studies have reported varying rates (2.7%–80%) in prescribing psychotropic medication to autistic children and adolescents (Jobski et al., 2017) which is in part due to the variability in study design. This variability makes it difficult to make meaningful comparisons between different studies and populations. Further, while international studies provide helpful insights into medication usage in the young autistic population, they may not be generalisable to the Australian context (Aman et al., 2005; Mandell et al., 2008; Spencer et al., 2013). Marked differences in psychotropic medication use reported in autistic populations from different countries may be due to variable prescribing practices and geographical or cultural factors.
While a few studies have explored pharmacological interventions in the Australian autistic population, the findings from these studies do not provide a clear understanding of medication use due to the heterogeneity between the study methodologies. Rasmussen et al. (2019) comprehensively reported on psychotropic medication use on data collected in 2014 from 7005 participants of the Longitudinal Study of Australian Children (LSAC) linked with dispensing claims from the PBS (Australian Government). The LSAC participants were recruited in 2004 from two age groups, 4 years apart, i.e. 0–1 and 4–5 years old, and then further examined the data from the recruited individuals when aged between 10 and 11 years and 14 and 15 years, which they termed children and adolescents, respectively. Of these autistic children and adolescents, Rasmussen reported that one-third were supplied with psychotropic medication in 2014. Although Rasmussen et al. (2019) provided some preliminary understanding of psychotropic medication use in Australian children, they only examined the use of medications by children in the age ranges 10–11 and 14–15 years (Rasmussen et al., 2019). Solely relying on data from these specific age groups might not provide a comprehensive understanding of how medication is utilised across the other ages in autistic children and adolescents. In 2018, Birch et al. (2018) reported findings from the Bettering the Evaluation and Care of Health programmes (BEACH), which examined the clinical encounters of Australian general practitioners (GPs) with the Australian paediatric population (autistic and non-autistic) under 25 years between 2000 and 2014. Although this study provides information on medication prescribed to autistic and non-autistic individuals, the categorisation of medication was not according to the conventional respective therapeutic use for medication in Australia or internationally, which limits a clear understanding of the prevalence of psychotropic medication use reported. They reported that the overall rate of prescribed medications per 100 encounters was similar for autistic and non-autistic individuals; however, the medication types differed significantly. Psychological medications were prescribed notably more in ‘ASD’ encounters than in ‘non-ASD’ encounters. The most prescribed medication subtypes varied between ‘ASD’ and ‘non-ASD’ encounters, with antipsychotics and antidepressants being prominent in ‘ASD’ encounters and antibiotics in ‘non-ASD’ encounters. Despite psychotropic medication use in young autistic people, it remains unclear whether these medications are as effective and safe in neurodiverse as they are in neurotypical people.
The variability of information from international studies and the scarcity of research on the Australian population highlight the need for additional studies to understand the current prescribing patterns of psychotropic medication in autistic children and adolescents in Australia. Based on this need, this study used retrospective data from the Western Australian Autism Biological Registry (WAABR) to gain insight into the use of psychotropic medications in autistic children and adolescents in Western Australia. The main objectives are to report descriptive statistics of types of psychotropic medications prescribed and their indications for use in a cohort 21 years and younger.
Methods
Ethical approval
The study was approved by the Curtin University Human Research Ethics Committee (HRE2018-0098) on 13 March 2019.
Data source
Individuals included in this study were enrolled in the WAABR which is an ongoing study of autistic children and their families in Western Australia by the Telethon Kids Institute (TKI). Participants were recruited via flyers distributed to local service providers and clinicians. This study examines data from 247 autistic people (2–39 years) registered in the database between 2011 and 2015.
Diagnosis in Western Australia mandates a consensus diagnosis following a multidisciplinary assessment by a paediatrician, clinical psychologist and speech–language pathologist (or by a psychiatrist and speech therapist). To confirm the clinical diagnosis, a multidisciplinary assessment team administered the ADOS-G (Autism Diagnostic Observation Schedule – Generic) to participants with parent or caregiver consent (Lord et al., 2000). The ADOS-G screens for deficits in social communications and interactions similar to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) and International Classification of Diseases, Tenth Revision (ICD-10). According to the DSM-V, individuals meeting the criteria for DSM-IV diagnosis are classified as meeting the diagnosis for ASDs (Lord et al., 2000).
Procedures
Parents and/or caregivers were specifically asked to complete the case history questionnaire that sought information on family sociodemographics, early child development and biological parents’ health. In a section of the case history questionnaire related to medication use, parents were also asked, ‘Please provide details of any prescribed medications your child has taken’. In addition, they were asked to list the name of the medication, the reason for use and whether it has led to improvement in symptoms.
Study population/inclusion and exclusion criteria
This study is a retrospective analysis of a subset of the WAABR data. The inclusion criteria were children and adolescents 21 years of age or younger on the day of completing the questionnaire between 2011 and 2015. The age range classification described by the American Academy of Pediatrics was employed to separate children and adolescents into developmental age ranges (Hardin & Hackell, 2017). Those between 0 and 5 years were classified as children, those between 6 and 12 years as middle childhood and those between 13 and 21 years as late adolescents. Demographic characteristics are presented in Table 1. After the database population was classified, individuals not reporting the use or previous use of psychotropic medications were excluded from the analysis (Figure 1). Figure 2 is a graphical representation of the medicated population (n=66) based on their sex and age.
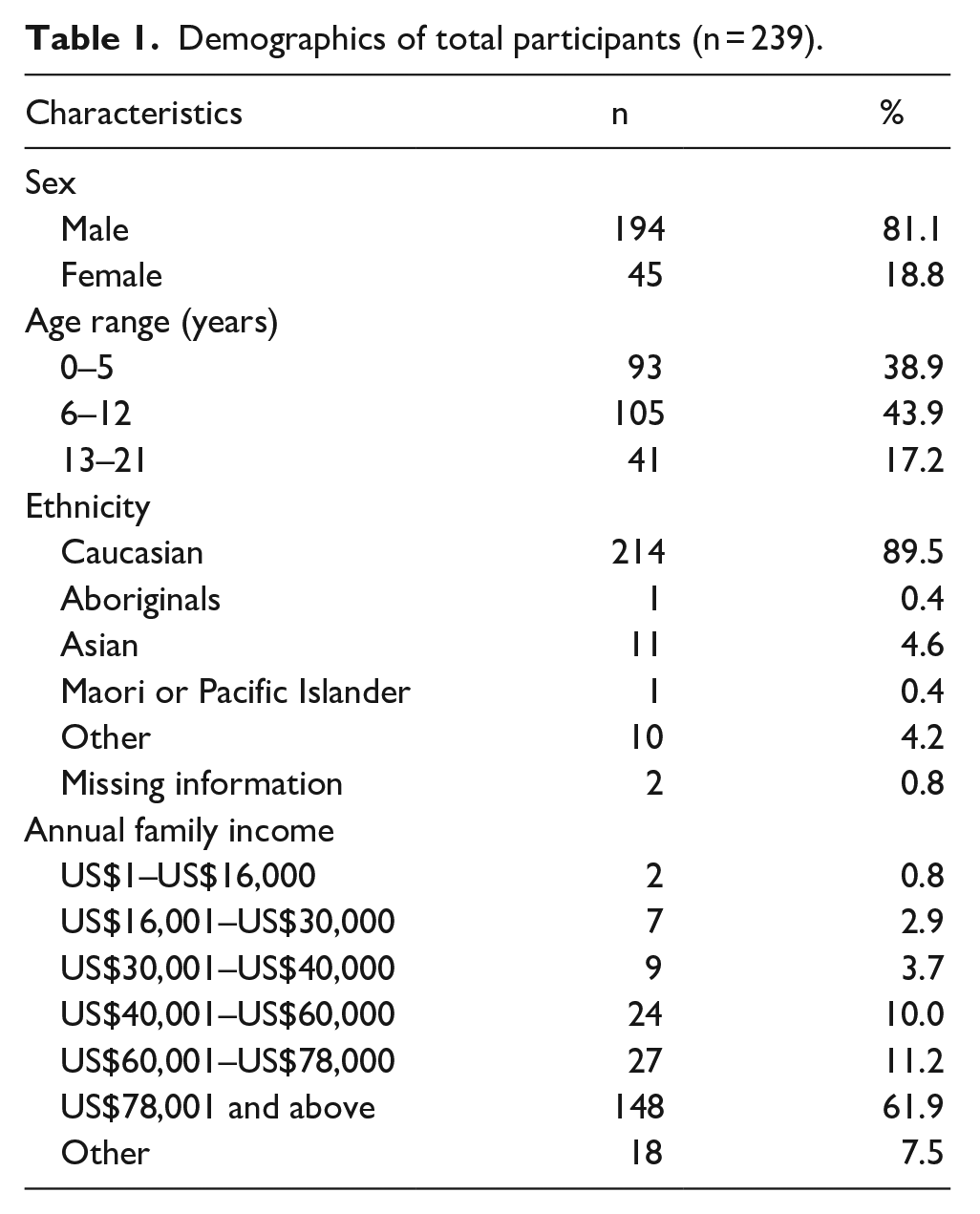
Demographics of total participants (n = 239).
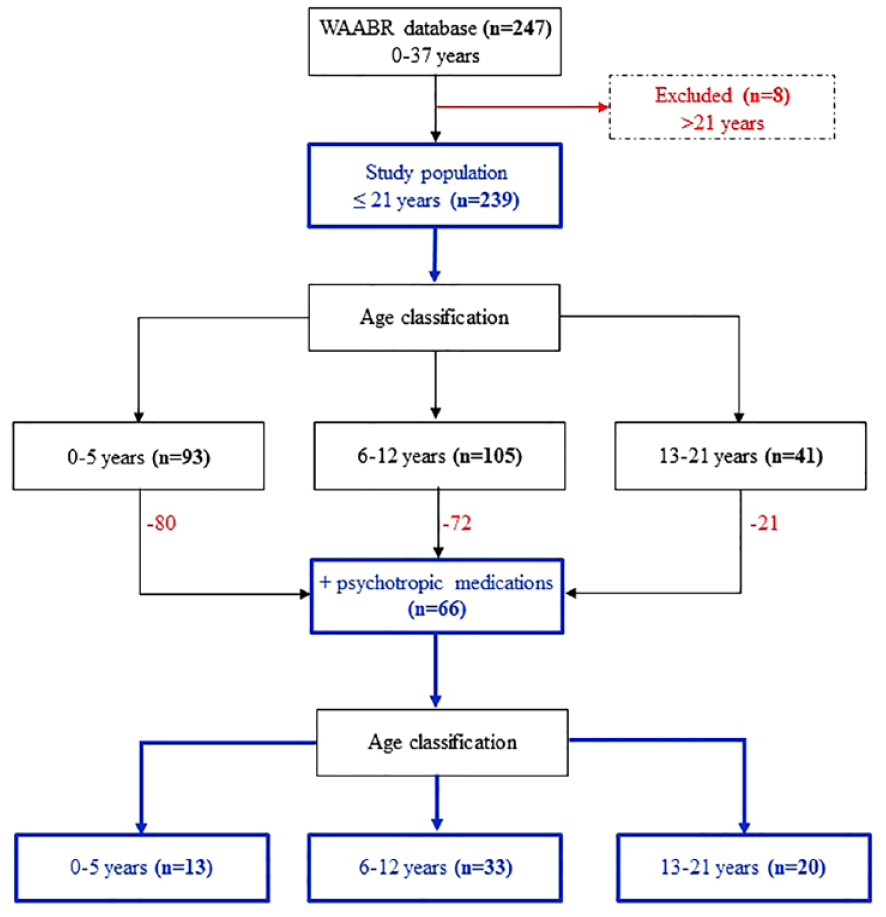
Flow diagram depicting manner of selection of study participants.
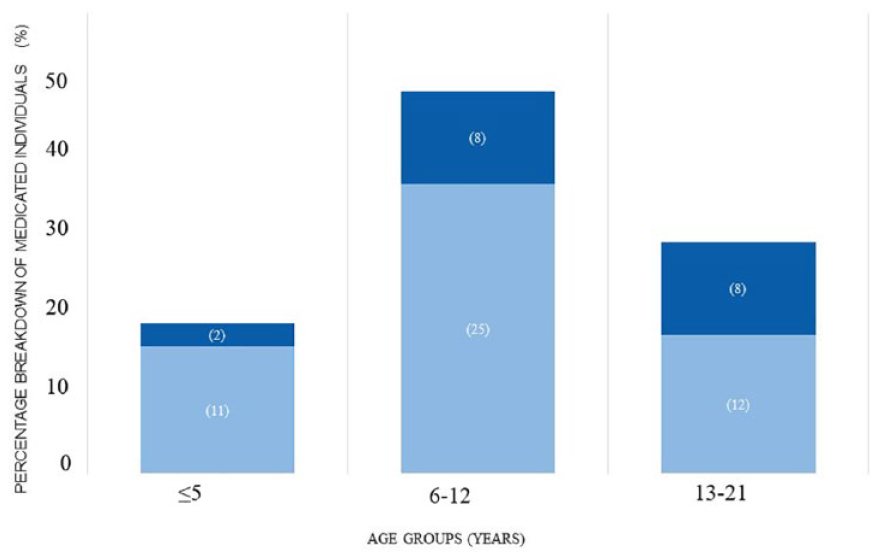
Psychotropic medication use by age group and sex.
Outcome measures
The Anatomical Therapeutic Chemical (ATC) classification system by the World Health Organisation (WHO) and the Australian Medicines Handbook (AMH, 2020; WHO Collaborating Centre for Drug Statistics Methodology, 2018) were used to code and classify psychotropic medications. These classes included stimulants, antiepileptics, antidepressants, antipsychotics, hypnotics–sedatives and non-stimulant ADHD medications. Only one record of each psychotropic medication class was recorded for each participant. Each medication class was further broken down to itemise individual medications used. To provide an example of the categorisation system, if a parent reported that their child used fluoxetine (Prozac®), it was categorised as an ‘antidepressant’ and a more specific subcategory based on its drug class, ‘Selective Serotonin Reuptake Inhibitor (SSRI)’. For everyone who reported psychotropic medication use, the indications for medication use and whether there was an improvement in symptoms were also recorded.
Data analysis
The dataset was analysed using the IBM SPSS Statistical Software Package (IBM Statistics for Windows, Version 5) and Statistical Analysis Software Version 9.4 (SAS Institute Inc, 2016). The sample was dichotomised into psychotropic or non-psychotropic medication users based on caregiver reports of psychotropic medication use. Before analysis, psychotropic medications and indications were categorised within Excel, coded into SAS variables and then imported into IBM SPSS 24.0. Descriptive statistical analyses were used to present the data, using counts and percentages. Percentages of any psychotropic medication use and indications for use were calculated within the predefined age groups. In addition, we described the medications used within the defined medication classes (according to the AMH) and itemised the medications used for specific reported indications.
Community involvement section
A family member, community provider and policy and agency leader are authors who were involved in the design, development, implementation and interpretation of the study and findings.
Results
Study population
A total of 239 children and adolescents, 21 years and younger, participated in the WAABR between 2011 and 2015. The population predominantly comprised males (n = 194, 81.1%), and most (n = 214, 89.5%) were of Caucasian ethnicity. The mean age was 7.8 years, with most participants being children aged 6–12 years (n = 105, 43.9%). The general demographic characteristics of the study population are provided in Table 1. The population is weighted towards a high-income level.
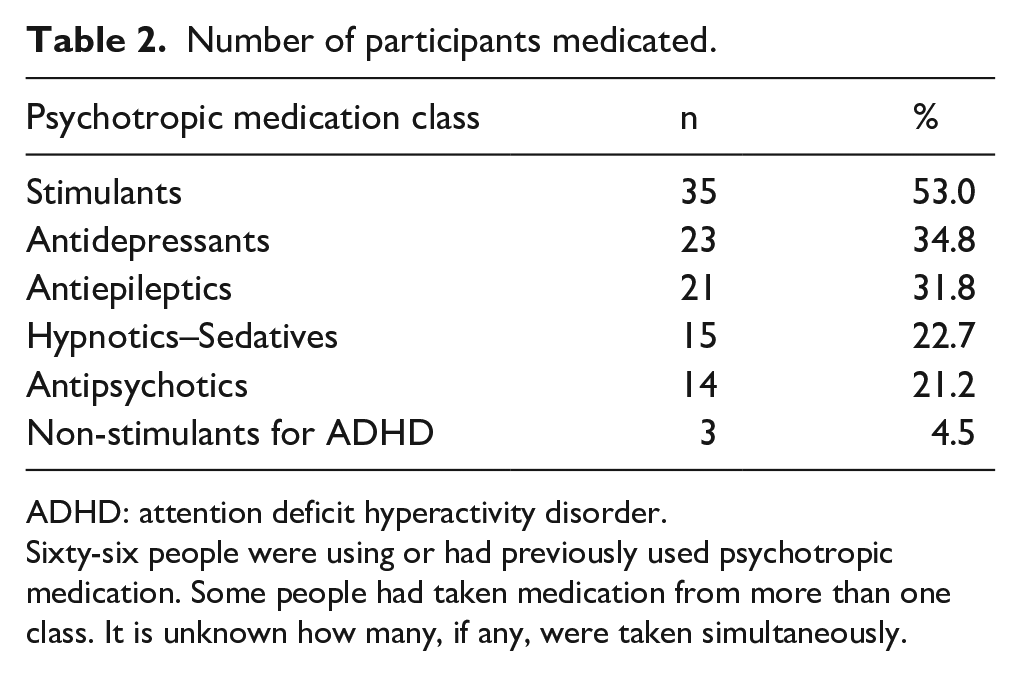
Of the 239 children and adolescents, n = 66 (27.6%) were either currently or previously prescribed one psychotropic medication, and n = 35 (53.0%) had received more than one type of medication on enrolment into the study. However, it is unclear from the dataset whether medications were used simultaneously, separately, consecutively or within the timeframe. Most individuals used stimulants (n = 35, 53.0%) (Table 2), with more stimulant users taking methylphenidate than dexamphetamine (Table 3). Antidepressants were the second most prevalent class of medications (n = 24, 36.4%), with fluoxetine or sertraline being the predominantly prescribed drugs. Valproate was the most frequently prescribed antiepileptic. However, it should be noted that both antiepileptics and benzodiazepines can have multiple indications and may not have been prescribed solely for their antiseizure properties (Table 5). Therefore, it is likely that medications were prescribed for dual therapeutic effects. For example, clobazam may be chosen for its beneficial side effects profile to manage challenging behaviours when utilised for seizures. Melatonin was the only medication used as a sedative/hypnotic in this population.
Number of participants medicated.
ADHD: attention deficit hyperactivity disorder.
Sixty-six people were using or had previously used psychotropic medication. Some people had taken medication from more than one class. It is unknown how many, if any, were taken simultaneously.
Number of participants reported to have taken an individual psychotropic medication within each class at some stage in their life.
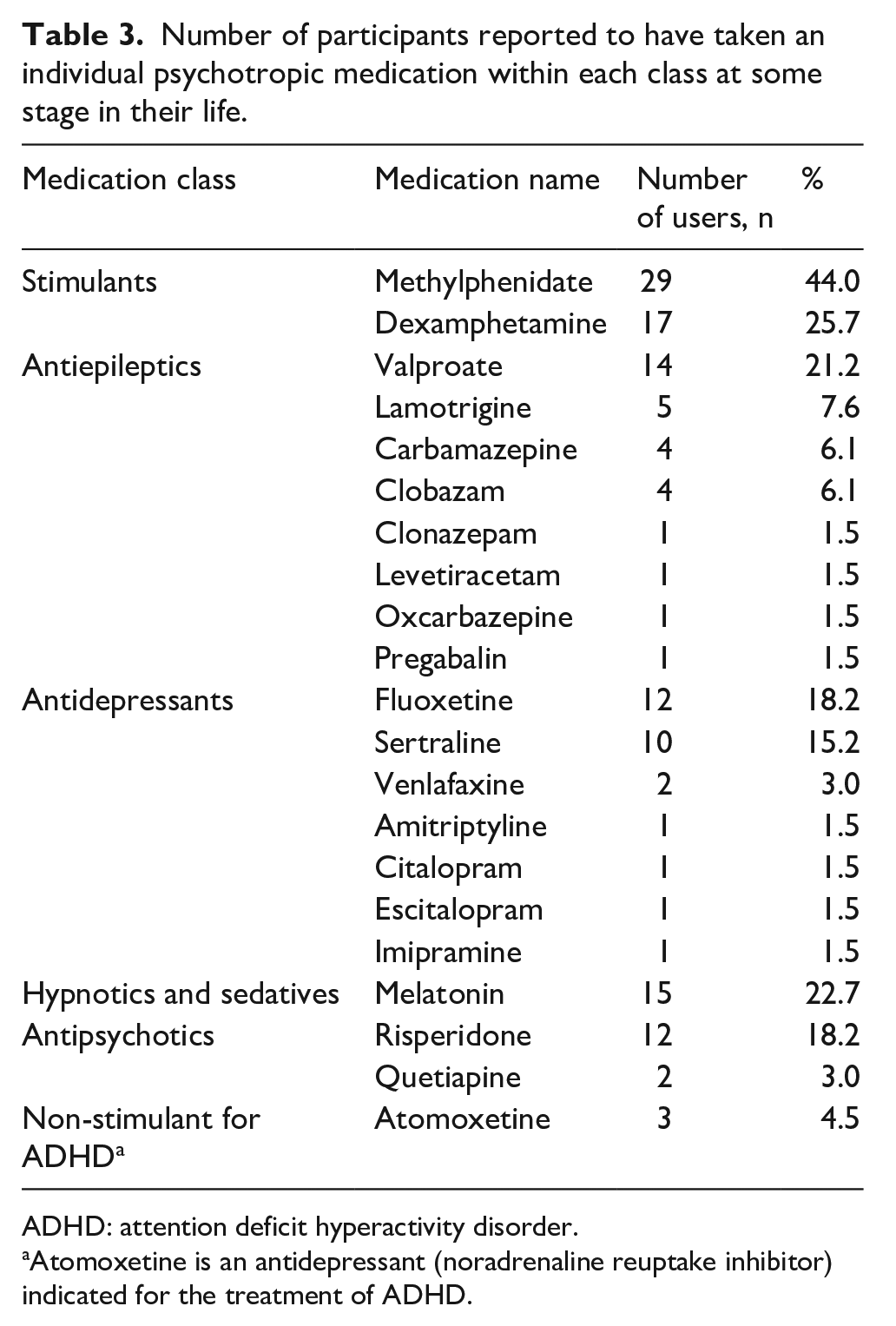
ADHD: attention deficit hyperactivity disorder.
Atomoxetine is an antidepressant (noradrenaline reuptake inhibitor) indicated for the treatment of ADHD.
Indications for psychotropic medication used
The indications for psychotropic medication use are summarised in Table 4. All individuals using psychotropic medication indicated that medications were used for managing symptoms of co-occurring mental health and behavioural disorders, including attention deficit, challenging behaviours, seizures, insomnia, anxiety, depression and mood stability. Challenging behaviours and attention deficit symptoms were the most common indication for psychotropic medication use, particularly among children between 6 and 12 years old.
Prescription indications/presentations, based on reports from the 66 individuals taking psychotropic medications.
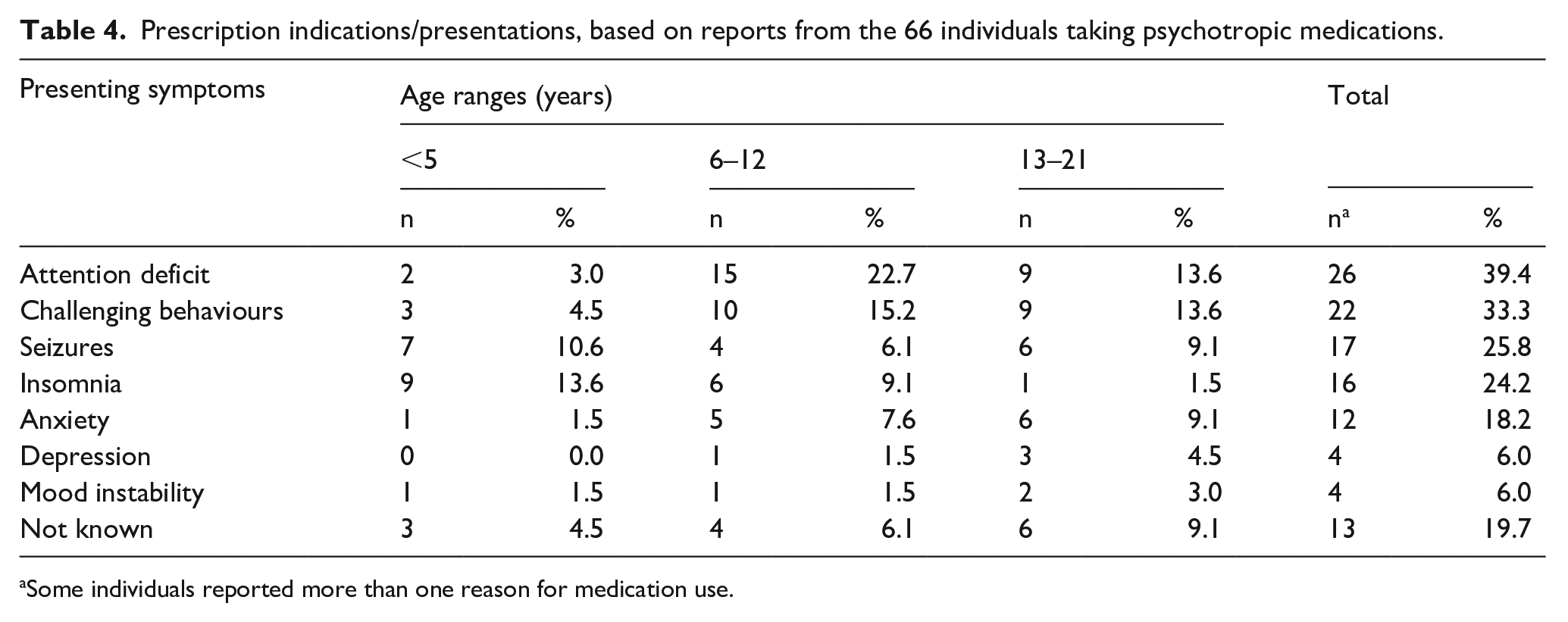
Some individuals reported more than one reason for medication use.
For each indication, Table 5 shows the psychotropic medication reported for managing the presenting symptom. Stimulants methylphenidate and dexamphetamine were primarily linked to ADHD. Challenging behaviours appear to be addressed by administration of methylphenidate/dexamphetamine and risperidone. Seizures appear to be mainly managed by valproate and insomnia by melatonin. Anxiety and depression appear less of an issue in this population, commonly managed by an SSRI.
The distribution of medications used to address diagnostic challenges/symptoms (n = 66).
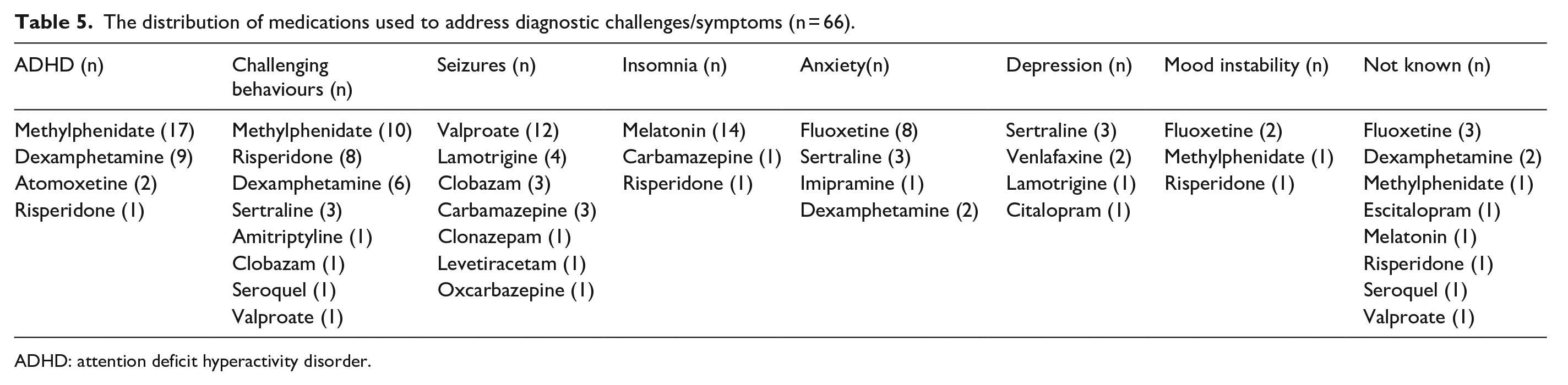
ADHD: attention deficit hyperactivity disorder.
The n = 66 people who reported current or previous use of psychotropic medications were using or had previously used n = 137 medications. Of these medications, n = 82 (59.9%) were reported to have helped alleviate the indicated symptoms or conditions. For the remaining medications, n = 37 (27.0%) did not improve symptoms, and n = 18 (13.1%) had no information on whether they improved symptoms. For participants with more than one medication, the data did not define whether participants switched between medications at different time points due to side effects or lack of effectiveness.
Discussion
Three-quarters of the children and adolescents in the WAABR database were not using psychotropic medications. In addition, over one-quarter of children in the WAABR reported having used or previously used a psychotropic medication, with over half of those prescribed pharmacotherapy having tried up to seven medications. It was unclear whether medications were used concurrently or sequentially. The most used classes were stimulants and antidepressants. The most reported reasons for these prescriptions were ADHD, challenging behaviours, anxiety and depression.
There appears to be large variability (3%–80%) in the prevalence of use of psychotropic medications across the literature among autistic young people, potentially due to differences in population demographics, socioeconomic aspects, methodological variations between studies as well as cultural and prescribing differences between countries (Akins et al., 2014; Esbensen et al., 2009; House et al., 2016; Madden et al., 2017; Mandell et al., 2008; Mire et al., 2014; Murray et al., 2014; Oswald & Sonenklar, 2007; Rosenberg et al., 2010; Witwer & Lecavalier, 2005). In Australia, there is limited access to linkage data from large databases as what is often used in international cohorts. Nonetheless, our findings provide preliminary insights into the patterns of psychotropic medication use in young autistic individuals in WA, albeit reporting on a subset of data from a biobank registry (WAABR), which represent individuals from a higher socioeconomic group.
In our dataset from the WAABR database, the prevalence of autistic children and adolescents using psychotropic medication appears within the low range of medication use (~28%) compared to previous studies (>40%) within a similar timeframe (Coury et al., 2012; House et al., 2016; Lake et al., 2012; Logan et al., 2012; Madden et al., 2017; Mire et al., 2014). However, it is important to note that our lower numbers of medicated children and young adults may be in part an artefact of the larger population (n = 93; 39%) of very young children (0–5 years) in our study that may not be included/of significance in other studies (i.e. considering the 6- to 21-year age group, medication use = 36%, Figure 1). Other reasons contributing to the differences could include variations in data sources, methodological approaches or definition/categorisation of medications (Aman et al., 2003; Birch et al., 2018; Logan et al., 2012; Mandell et al., 2008; Rasmussen et al., 2019; Schubart et al., 2013).
Further, we speculate that participating in a study like the WAABR population, run by a team of researchers and clinicians who may advocate and provide families with access to support services (e.g. speech pathology, occupational therapy and behavioural interventions), would expose carers to a greater variety of interventions. Therefore, the WAABR participants may have been exposed to greater access to nonpharmacological interventions, which may also lead to a lower reliance on medications (Horlin et al., 2014; Irvin et al., 2012; Thomas et al., 2007). We also speculate that our findings may be, at least in part, related to the sociodemographic status of the guardians of our participants (Table 1) (Australian Bureau of Statistics, 2013). Considering factors such as income, education and access to healthcare resources can reveal how socioeconomic disparities may influence medication prescribing. Recent reports in the literature indicate that parents of autistic children with higher income levels are more likely to use and enrol their children in nonpharmacological interventions such as private speech pathology and Applied Behaviour Analysis (ABA) interventions than families with lower household incomes (Irvin et al., 2012; Thomas et al., 2007). Future studies should focus on including participants of broader demographic characteristics to gain a more comprehensive and nuanced understanding of medication prescribing practices. This approach not only provides a clearer overview of prescription trends but also helps identify potential disparities and factors influencing medication use. Moreover, it enables researchers to better compare prescribing patterns in young Australian autistic populations to international cohorts, contributing to a more robust and informative body of research.
Our study identified age as a particularly influential factor that could account for the observed results. Unlike previous studies, our study reports higher likelihood of medication use among children (<12 years) compared with their older adolescent counterparts (13–21 years) but this needs further investigation since it could be related to age of autism diagnosis (Coury et al., 2012; Memari et al., 2012; Rasmussen et al., 2019). Further research evidence is required to provide stronger support for use of psychotropic medications in young autistic persons, especially considering that the symptoms they are prescribed for are not yet fully understood.
Although our current study suggests that autistic children and adolescents are receiving medication for managing co-occurring mental health conditions, it is important to note that some indications for the use of particular medications were unclear. This lack of clarity may be attributed to many aspects including the inherent complexity of the symptoms for which these medications are employed, as their interpretation can vary significantly, making it challenging to ascertain the precision of reported indications. For instance, when individuals reported using medications to manage challenging behaviours, variations in what each considered a ‘challenging’ behaviour could have occurred. Observable and disruptive symptoms such as tantrums (associated with ADHD) or hand flapping (as a result of anxiety) may be perceived as challenging behaviours (Teagle, 2002). The medication used for symptoms reported as ‘challenging behaviours’ in the WAABR cohort may have depended on the clinician’s interpretation of the symptoms; however, this is unclear from the dataset (Cervantes et al., 2013). The subjectivity of understanding symptom interpretation may result from the unavailability of objective measures of what constitutes challenging behaviour, especially how behaviours perceived as challenging may be related to co-occurring conditions. The variation in the report for the indication, such as challenging behaviour, may have been affected by the data collection period of the study, which occurred when a dual diagnosis of ADHD and ASD was not permitted under the DSM-IV criteria for ASD diagnosis. Therefore, it is possible that some reports of ‘challenging behaviours’ were related to ADHD, which may further explain the frequent report of stimulant medication in the WAABR cohort. Although risperidone has been approved by the TGA for managing severe behavioural disturbances, there was more frequent use of antidepressants reported in the WAABR cohort. However, challenging behaviours are not an indication for antidepressants in Australia. Nonetheless, the use of antidepressants may have been prescribed to deliver some benefits related to reduced repetitive behaviours that can be associated with anxiety and obsessive–compulsive disorders in autistic individuals with less severe side effects (Blankenship et al., 2010; Cervantes et al., 2013; De Hert et al., 2011; Hollander et al., 2004; Kent et al., 2013; Owley et al., 2005; Ozsivadjian et al., 2012). More research is needed to establish a more consistent interpretation model and objective measures for defining symptoms such as challenging behaviours to help standardise when medication should be considered.
Some limitations arise in this study since this study is an analysis of data collected to gain a preliminary understanding of current medication use and identify areas to further employ in a research environment. This study could not consider polypharmacy as the WAABR questionnaire did not enable the determination of when psychotropic medications were used and for which indications. As a result, we could not investigate whether individuals sequentially trialled multiple medications due to a lack of efficacy or side effects experienced. In addition, due to the retrospective nature of this study, it is essential to approach the reported effectiveness of psychotropic medication with caution. The data are solely derived from a single time point, preventing meaningful baseline comparisons. As a result, drawing definitive conclusions about the long-term efficacy of these medications in the studied population is limited. Finally, potential participant bias in the WAABR cohort and the small sample size of this study reduces the generalisability of the results. Selection bias can potentially create a non-representative sample, undermining the study’s capacity to draw conclusions that apply to the autistic population. Therefore, findings may not accurately represent the entire population, potentially underrepresenting individuals not seeking medical care from specific locations. In particular, our study had a relatively lower percentage of individuals with intellectual disability compared to larger autistic samples. This may have implications on the prevalence of the medications observed. Future research should implement more rigorous sampling techniques, such as random or stratified sampling, to mitigate the sample bias. Nevertheless, the findings from this study contribute to the growing understanding of psychotropic medication use in autistic children and adolescents in Australia and confirm many of the findings of the previous Australian study by Rasmussen et al. (2019).
Although this study is limited by the narrow population studied and biased towards participants from higher socioeconomic backgrounds, it extends the existing literature about the associations between medication use, indications and family sociodemographic characteristics. Further research using larger representative samples, prescription patterns, medication types, indications, effectiveness and side effects will assist in developing evidence-based clinical guidelines.
Conclusion
This study highlights the multifaceted nature of psychotropic medication usage in young autistic people. Particularly, within a population from a high socioeconomic background, primarily consisting of younger autistic children, the findings of our study suggest that psychotropic medication use may not be frequently sought. Those individuals who reported using psychotropic medication received them to manage co-occurring symptoms and conditions; however, the appropriateness of this usage remains uncertain, especially given the complex nature of co-occurring symptoms in young autistic individuals. Therefore, larger studies that enable deeper understanding of the effectiveness and safety of psychotropic medication use in the context of symptom presentation remain crucial.
Footnotes
Acknowledgements
The authors greatly acknowledge the families who participated in the Western Australian Autism Biological Registry (WAABR) database, without whom this research would not be possible.
Author contributions
All authors helped in research concept and design, critical revision of the article and the final approval of the article. AW helped in collection and/or assembly of data. RB and RP helped in statistical analysis. RB, KW, RP, BS and RC helped in data analysis and interpretation. RB helped in drafting the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.