
Abstract
Increased reactivity to daily stressors is associated with mental health difficulties, which are common in autistic individuals. We investigated affective reactivity to daily-life stress, cognitive emotion regulation, and their link with co-occurring mental health symptoms in adolescents and young adults with autism. A 6-day ecological momentary assessment protocol was used to assess perceived daily-life stress (event-related, activity-related, and social stress) as well as negative affects in autistic (n = 39, age = 18.4) and non-autistic (n = 55, age = 18.1) participants. Co-occurring mental health difficulties, social functioning, and cognitive emotion regulation were assessed with questionnaires and clinical evaluations. Youth with autism showed higher levels of perceived stress related to their daily social context and activities, as well as an increased affective reactivity to activity-related stressors compared with non-autistic youth. Moreover, they reported using less adaptive and more non-adaptive emotion regulation, the latter increasing their affective response to daily stressors and possibly contributing to the severity of co-occurring mental health symptoms. Our findings demonstrate high perceived daily-life stress in autistic adolescents and young adults. To minimize the negative effects of stress and the development of mental health symptoms, interventions could focus on effective stress management and strategies that autistic young people use to manage their emotions.
Lay abstract
Previous research has shown that autistic individuals report high levels of perceived stress and have an increased likelihood of developing mental health difficulties. Increase in individuals’ negative emotions in relation to perceived stress (i.e. affective reactivity to stress) is a known risk factor for mental health difficulties. In this study, we investigated perceived daily stress and affective reactivity to stress in autistic (n = 39, age = 18.4) and non-autistic (n = 55, age = 18.1) adolescents and young adults. We used the ecological momentary assessment, a technique that allows to assess individuals repeatedly in their daily life using their smartphone. Moreover, participants filled a questionnaire to evaluate the strategies they use to regulate emotions when faced with difficulties. Finally, a clinical interview and a parent-report questionnaire were used to assess mental health symptoms. Autistic youth reported higher levels of perceived daily stress compared with non-autistic peers. Moreover, they showed increased affective reactivity to stress related to their daily activities. Autistic participants reported more emotion regulation difficulties (e.g. more repetitive thinking of difficulties) compared with non-autistic participants. Difficulties in emotion regulation increased negative emotions in relation to stress and might contribute to the severity of mental health symptoms. We conclude that adolescents and young adults with autism report high perceived stress in their daily lives. To minimize the negative impact of stress and the development of mental health symptoms, people supporting autistic young people could focus on stress management skills and the strategies that the youth use to manage emotions.
Keywords
Introduction
Some studies show that autistic individuals report higher levels of perceived stress compared with non-autistic individuals (Bishop-Fitzpatrick et al., 2017; Hirvikoski & Blomqvist, 2015; McGillivray & Evert, 2018; van der Linden et al., 2021), and it is increasingly shown that they may be more likely to be exposed to adverse experiences, including traumatic and stressful life events, such as bullying (Haruvi-Lamdan et al., 2018; Hoover & Kaufman, 2018). Sources of stress that are not generally considered traumatic/stressful in the general population (e.g. changes in routine or loud sounds) may also affect autistic individuals strongly (Kerns et al., 2015). Previous research (Storch et al., 2012; Taylor & Gotham, 2016) has shown that exposure to past adversities may contribute to the high rates of co-occurring psychiatric conditions, such as (social) anxiety and mood disorders, reported in autistic individuals (Kirsch et al., 2020; Lai et al., 2019). Social anxiety and difficulties in social skills may increase their vulnerability to interpersonal stressors (Haruvi-Lamdan et al., 2020), which could contribute to increase in subsequent social difficulties. Indeed, negative social experiences may lead autistic individuals to avoid social interactions, resulting in social isolation and feelings of loneliness (Umagami et al., 2022). Adolescents and young adults with autism might be particularly prone to negative social experiences, as this age is associated with increasing complexity in social relationships (Picci & Scherf, 2015).
A mechanism linking past exposure to external stressors to the development of co-occurring clinical conditions may be an increase in individuals’ response to subsequent stress, that is, increased stress reactivity. The concept of stress sensitization states that previous exposure to external stress can sensitize an individual to daily stressors, through an increase in the intensity of physiological and subjective stress responses, and heighten the risk of developing mental health difficulties (Collip et al., 2008). A particularly suitable technique for assessing how individuals react to context-spesific daily stress is the ecological momentary assessment (EMA), a structured diary technique that allows repeated assessments and captures contextual nuances in the flow of daily life (Myin-Germeys et al., 2018). EMA has been used and proven to be feasible with adolescents and adults with autism (e.g. Chen et al., 2014; Dallman et al., 2022; Kovac et al., 2016), but limited research has focused on stress (van der Linden et al., 2021). Previous EMA studies have validated measures of stress, conceptualized as a subjective appraisal of stressfulness of events or small disturbances in the flow of daily life (Vaessen et al., 2015). Furthermore, the increase in negative affects (NA) related to daily stressors has been conceptualized as affective reactivity to stress in previous work (Myin-Germeys et al., 2001). Earlier studies have shown that exposure to stress, including bullying, could increase individuals’ affective reactivity to stressors, especially in vulnerable individuals (Rauschenberg et al., 2017; Rauschenberg et al., 2021). Affective reactivity to daily stress is important to investigate in autistic individuals, as it is considered a vulnerability factor for mental health difficulties (Myin-Germeys et al., 2003; Myin-Germeys et al., 2001).
However, to date, there is a paucity of studies on affective reactivity to stress in autism. A recent EMA study showed that the association between unpleasant daily events and activities with NA was stronger in autistic adults than in non-autistic adults, indicating heightened affective reactivity to event- and activity-related stress (van der Linden et al., 2021). Moreover, findings from studies examining physiological markers of stress may indirectly indicate alterations in stress sensitivity; in individuals with autism, some alterations have been observed in the functioning of two main stress response pathways: the hypothalamic–pituitary–adrenaline (HPA) axis and the autonomic nervous system (ANS), even though results are mixed (Cheng et al., 2020; Taylor & Corbett, 2014). In some studies, HPA and/or ANS markers have been associated with higher levels of anxiety and depressive symptoms in autistic children (Guy et al., 2014; Hollocks et al., 2014; Hollocks et al., 2016; Sharpley et al., 2016). However, the relationship between affective reactivity to stress and clinical manifestations, such as co-occurring mental health symptoms or social withdrawal, has not yet been investigated in autistic adolescents.
It should be emphasized that not all individuals exposed to adverse (social) experiences will develop mental health difficulties or withdraw from the social world. Difficulties in regulating emotions when faced with negative experiences can increase vulnerability to negative outcomes of stress (Nolen-Hoeksema & Watkins, 2011). Emotion regulation (ER) can be defined as the evaluation and modification of one’s emotional reactions in order to achieve one’s goals (Thompson, 1994). Cognitive ER strategies (thinking) include cognitive processes that individuals use to regulate emotions, and are proposed to be distinct from behavioral ER (acting) (Garnefski et al., 2001). Certain cognitive processes, such as cognitive reappraisal (i.e. reinterpreting the meaning of the event) have been shown to reduce NA (Ray et al., 2010) and be associated with less mental health symptoms (Aldao et al., 2010). Such strategies associated with adaptive emotional outcomes are considered as “adaptive” strategies to cope with stressful events. On the contrary, some strategies are defined as “non-adaptive” in regulating emotions, notably rumination (i.e. repetitive thinking of the negative event or negative feelings caused by the event), which could be associated with more intense stress responses (Krkovic et al., 2018) and poor clinical outcomes, including depression and other psychiatric conditions (Aldao et al., 2010). Mazefsky and White (2014) proposed that several characteristics experienced by some autistic people, such as alexithymia (i.e. difficulty to identify, differentiate, and express one’s emotions), cognitive rigidity, or difficulty in perceiving social cues, may increase the likelihood of using non-adaptive ER. Indeed, earlier studies have reported ER difficulties in autistic individuals from childhood to adulthood (Jahromi et al., 2012; Samson et al., 2015; Samson et al., 2012), which could contribute to negative clinical evolution, including co-occurring mental health symptoms and social difficulties (Cai et al., 2019; Goldsmith & Kelley, 2018; Patel et al., 2017). Therefore, identifying ER strategies used by autistic youth and examining their role in modulating the affective responses to daily stressors is important.
The current study aimed to investigate affective reactivity to daily stress, cognitive ER, and their relationship with mental health difficulties in autistic adolescents and young adults. EMA was used to allow an ecological approach to investigate perceived stress in relation to individuals’ daily-life context, which is important to study because several environmental factors (e.g. aversive sensory stimuli, unpleasant events, or social demands) might represent a great source of stress for some individuals with autism (Kerns et al., 2015), possibly increasing NA. The first aim was to investigate affective reactivity to different types of stress: event-related stress (i.e. stress related to daily hassles), activity-related stress (i.e. stress related to activities that individuals are involved in), and social stress (i.e. stress related to current social context), as well as the associations with clinical symptoms. We hypothesized that autistic youth would show higher levels of perceived stress and increased affective reactivity to daily stressors compared with non-autistic youth. Moreover, we expected increased affective reactivity to stress to be associated with higher levels of co-occurring mental health symptoms and social isolation in youth with autism. The second aim was to investigate cognitive ER and its impact on affective reactivity to stress. We hypothesized that autistic participants would use less adaptive and more non-adaptive ER strategies than non-autistic participants, and that non-adaptive ER would be associated with clinical symptoms. Finally, we expected that the use of adaptive/non-adaptive ER would moderate the stress–NA association in daily life.
Method
Sample
A total of 43 participants diagnosed with autism spectrum disorder (ASD), aged 12–29 years, and 57 non-autistic participants, aged 12–26 years, participated in the current study. Data were collected between October 2018 and March 2022. Autistic participants were recruited through clinical centers in Geneva and France, through a network of medical professionals and through announcements to family associations in Switzerland and France. Non-autistic participants were recruited through the Geneva local community as well as through an ongoing longitudinal cohort involving typically developing participants and youth with a neurogenetic condition (see Sandini et al., 2020). Sample characteristics are shown in Table 1 and in Supplementary Table 1. Participants had to be verbally fluent and have a parent/caregiver available to participate in the study. All participants had reading comprehension skills at least equal to the level of 11–12-year-old children (6th grade in France), as assessed by their parents using the Vineland-II scale (Sparrow et al., 2005). Autistic participants were assessed with the Autism Diagnostic Observation Schedule, second version (ADOS-2) (Lord et al., 2012) and their caregivers completed the Autism Diagnostic Interview-Revised (ADI-R) (Rutter, Le Couteur, & Lord, 2003) or the Social Communication Questionnaire (SCQ) (Rutter, Bailey, & Lord, 2003). Non-autistic group was screened using the SCQ, with a mean score of 2.8 and none of the participants scoring above the clinical cutoff (15). The exclusion criteria for individuals without autism were premature birth, first-degree relative with neurodevelopmental disorder (with the exception of a de novo neurogenetic condition), or lifetime presence of psychiatric disorders, neurological issues, or neurodevelopmental disorders. Part of the non-autistic sample (n = 47) overlapped with the sample of our previous study (Ilen et al., 2023). All participants and caretakers gave their written consent. Participants received a financial compensation of 100 CHF for participating in a larger study including additional measures. The study was approved by the Cantonal Research Ethics Committee of Geneva (CCER) (2018-01117). Autistic community members were not involved in the design of this study.
Group comparisons of demographic characteristics and variables of interest.
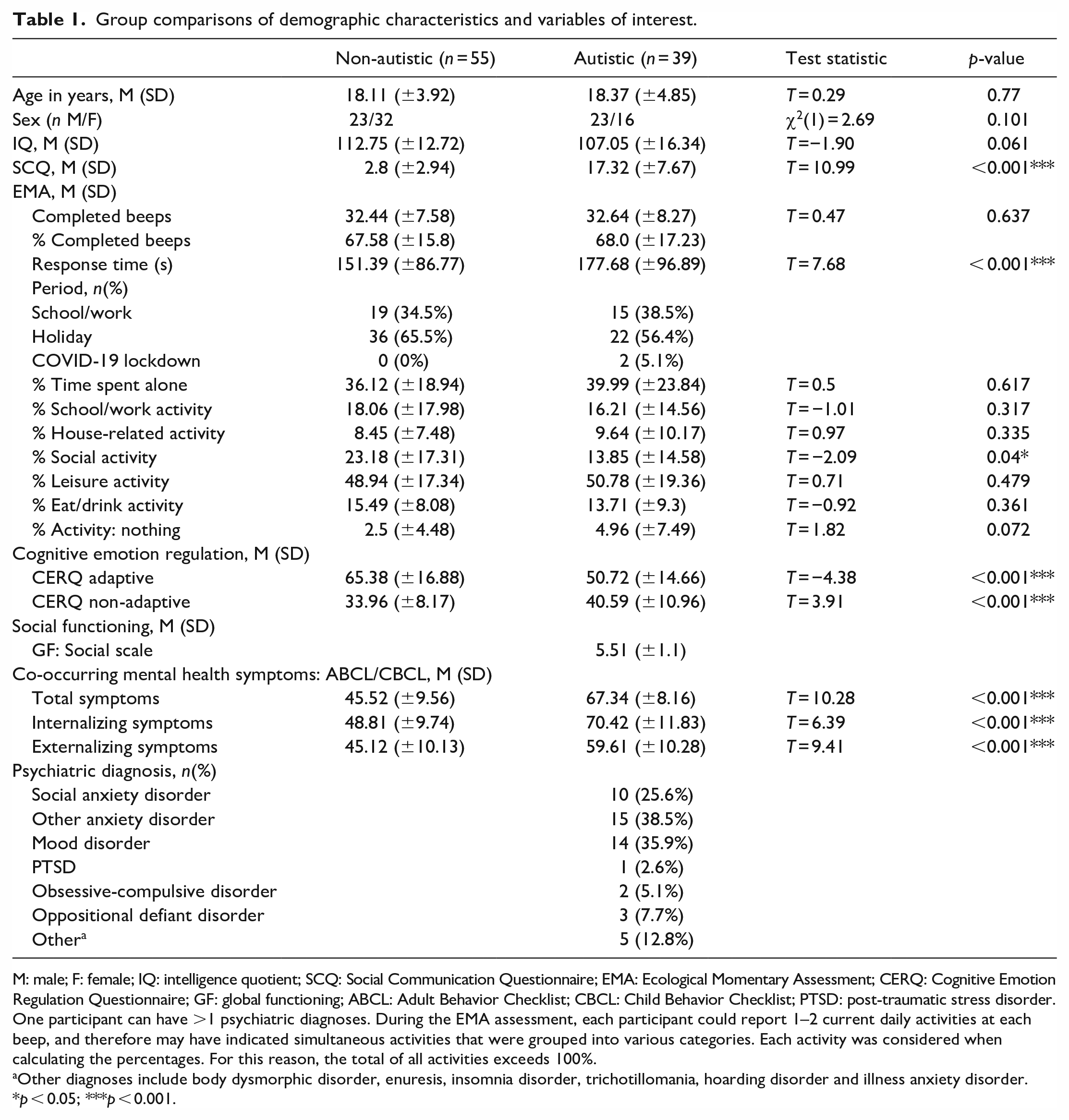
M: male; F: female; IQ: intelligence quotient; SCQ: Social Communication Questionnaire; EMA: Ecological Momentary Assessment; CERQ: Cognitive Emotion Regulation Questionnaire; GF: global functioning; ABCL: Adult Behavior Checklist; CBCL: Child Behavior Checklist; PTSD: post-traumatic stress disorder.
One participant can have >1 psychiatric diagnoses. During the EMA assessment, each participant could report 1–2 current daily activities at each beep, and therefore may have indicated simultaneous activities that were grouped into various categories. Each activity was considered when calculating the percentages. For this reason, the total of all activities exceeds 100%.
Other diagnoses include body dysmorphic disorder, enuresis, insomnia disorder, trichotillomania, hoarding disorder and illness anxiety disorder.
p < 0.05; ***p < 0.001.
Measurement
EMA
Smart-phone based EMA was used to evaluate participants’ NA and perceived stress in daily life. The RealLife Exp application (associated to the Lifedatacorp platform) was installed on the smartphone of each participant. We used a semi-random signal-contingent sampling scheme with eight notifications per day for six consecutive days between 07:30 am and 22:30 pm, resulting in a maximum of 48 beeps per person. Participants had 15 min to complete each questionnaire. In line with previous studies (e.g. Myin-Germeys et al., 2001), only participants who completed a full questionnaire for at least one-third of the beeps were included in the analyses. The period during which each participant took part in the EMA assessment was noted (either: school/work, holidays, or lockdown due to COVID-19).
NA were assessed using the mean score of the following items: I feel alone, I feel anxious, I feel irritated/angry, I feel sad, each measured on a scale from 1 (not at all) to 7 (extremely). To assess perceived stress, a similar approach to that used in various EMA studies was applied (Myin-Germeys et al., 2001; Schneider et al., 2020; van der Linden et al., 2021). All items included in the stress variables were measured on a scale from 1 (not at all) to 7 (extremely). To assess event-related stress, participants were asked to think about the most important event that happened since the last beep and evaluate how enjoyable this event was. Participants were also asked whether they were in the company of others during this event (yes/no). To assess activity-related stress, participants evaluated their current activity with the following items: This activity is difficult, and I enjoy doing this activity, (reversed score for analyses). Finally, at each beep, participants were asked whether they were alone (yes/no). Social stress was assessed during the beeps when participants reported being in the company of others using the following items: I would prefer to be alone, This company is pleasant, (reversed score for analyses), I feel judged by this/these person(s), I feel nervous in the presence of this/these person(s). The percentage of beeps during which each participant reported being alone during the EMA assessment was calculated as a measure of social isolation in daily life. More detailed information about the EMA protocol and the psychometric properties of the EMA measures are provided in the Supplementary Material.
Questionnaires
Cognitive ER was assessed with the French version (d’Acremont & Van der Linden, 2007) of The Cognitive Emotion Regulation Questionnaire (CERQ) (Garnefski et al., 2001), a self-report questionnaire that assesses the use of different strategies to regulate emotions in response to negative events; 36 items examine the use of adaptive and non-adaptive ER strategies on a 5-point Likert-type-scale (1 = almost never, 5 = almost always). Adaptive subscale consists of five strategies: acceptance, positive refocusing, refocus on planning, positive reappraisal, and putting into perspective, whereas non-adaptive subscale includes strategies of self-blame, rumination, catastrophizing, and blaming others. In the original article, Cronbach’s alpha for the CERQ subscales ranged from 0.68 to 0.83 (Garnefski et al., 2001), and in the French version, from 0.62 to 0.82 (d’Acremont & Van der Linden, 2007). To our knowledge, reliability scores have not been published for individuals with autism. However, the CERQ has previously been used with autistic adults (Bruggink et al., 2016) and an adapted version was used with autistic children (Rieffe et al., 2011).
Co-occurring mental health symptoms were measured through a parent-report questionnaire: the Child Behavior Checklist (CBCL) (Achenbach & Rescorla, 2001) or the Adult Behavior Checklist (ABCL) (Achenbach & Rescorla, 2003). The age-normalized T-scores of total mental health symptoms as well as of the externalizing and internalizing subscales were used in the analyses. The test–retest reliabilities for these three subscales range from 0.80 to 0.94, and Cronbach’s alpha coefficients from 0.90 to 0.97 (Achenbach & Rescorla, 2001, 2003).
Clinical assessment
A comprehensive clinical assessment was conducted with autistic participants to examine the presence of Diagnostic and Statistical Manual of Mental Disorders (5th ed; DSM-5) diagnoses (see Supplementary Material). The sum of current psychiatric diagnoses was used as a measure of co-occurring psychiatric conditions, in line with earlier studies (Sandini et al., 2020).
To assess social functioning (with a special focus on social withdrawal), the Global Functioning (GF) Social scale (Cornblatt et al., 2007) was used. The interview-based scale assesses the quantity and quality of peer relationships, peer conflicts, intimate relationships appropriate to age, and involvement with family members. The score ranges from 1 = extreme dysfunction to 10 = superior functioning.
Cognitive assessment
Intellectual functioning was assessed with Weschler Intelligence Scale for Children (Wechsler, 2014) or Adults (Wechsler, 2008).
Statistical analyses
The analyses were conducted using STATA 16 (StataCorp, 2019) and R version 4.2.1 (R Core Team, 2020) using the esmpack (Viechtbauer & Constantin, 2021) and nlme packages (Pinheiro et al., 2022). As the EMA data have a two-level structure, with repeated measurements (Level 1) nested within individuals (Level 2), multilevel regression models were used. The models were corrected for autocorrelation between residuals using an AR(1) autocorrelation structure. Multiple comparisons were corrected with Benjamini–Hochberg (B-H) correction (Thissen et al., 2002).
Group comparisons for non-EMA variables were done using linear regression models and the chi square test. For time-invariant EMA variables (% time spent alone, % different activities), multiple linear regression models were used for group comparisons. For time-varying EMA variables (NA, stress), group comparisons were examined using multilevel regression models with random intercepts. For the analyses conducted on the EMA variables, age, gender, intelligence quotient (IQ) and EMA period (0 = school/work, 1 = holidays or 2 = lockdown due to COVID-19) were included as covariates.
To examine associations between perceived stress and NA, separate multilevel regression models with random intercepts and random slopes were estimated using the MIXED command, with each stress variable, group and their interaction as independent variables and NA as a dependent variable, controlling for age, gender, IQ and EMA period. To model participants’ individual level of affective reactivity to stress, a “stress reactivity variable” was created calculating a momentary-level within-person beta coefficient of the association between perceived stress and NA for each participant and for each context of stress (three beta coefficients per participant) (see Kramer et al., 2014). Social stress reactivity variable could not be calculated for three participants (n = 2 autistic) due to collinearity issues as well as for two participants (n = 1 autistic) who reported being in a company of others during less than four beeps. To examine associations between affective reactivity to stress and clinical symptoms, several multiple linear regression models (for total, internalizing and externalizing symptoms, % time spent alone in EMA) and ordinal logistic regression models (for co-occurring psychiatric conditions, score of GF social scale) were used. In the models, each stress reactivity variable was added separately as an independent variable and each mental health or social functioning variable as a dependent variable, controlling for age, gender, IQ, and EMA period.
Group differences in cognitive ER were conducted using multiple linear regression models, controlling for age, sex, and IQ. To examine whether ER was associated with clinical symptoms, several multiple linear/ordinal logistic regression models were conducted using the CERQ adaptive/non-adaptive subscale as an independent variable and each mental health and social functioning variable as a dependent variable, controlling for age, gender, and IQ (and EMA period for % alone). Finally, to examine whether ER moderated the effect of perceived daily stress on NA, separate multilevel regression models with random intercepts and random slopes were estimated, with each stress variable, ER and their interaction as independent variables and NA as a dependent variable, controlling for age, gender, IQ and EMA period. The analyses were conducted first in the entire sample, and then in the two groups separately.
The current study was co-registered during data collection (https://doi.org/10.17605/OSF.IO/KQM3A). Of note, we conducted few additional analyses which were observational and not registered (see Supplementary Material). The data set is publicly available through the YARETA data preservation system. (https://doi.org/10.26037/yareta:ldxhgkxj6ngavohnc7k7l3uumy).
Results
Sample characteristics and EMA compliance
Of the total of 100 participants assessed, five participants (n = 3 autistic, n = 2 non-autistic) were excluded from the study as they provided less than 16 valid responses (<33.3% of total number of beeps) during the EMA protocol. Moreover, one participant with autism was excluded due to a possible careless responding (fast responses with a specific pattern). 27 beeps (n = 11 in autistic group and n = 16 in non-autistic group) were excluded due to a too long response time (>15 min). The final sample consisted of 39 autistic participants with 1273 valid responses and 55 non-autistic participants with 1784 valid responses. Detailed information about compliance of participants is shown in Table 1. The groups did not differ in terms of EMA compliance, but participants with autism had a longer average response time than non-autistic participants. Age, sex and IQ did not significantly differ between the groups.
Group comparisons for EMA variables
A multilevel analysis showed that autistic participants reported higher levels of NA in their daily lives than non-autistic participants (Table 2). Moreover, they reported significantly higher levels of perceived social and activity-related stress, but no event-related stress, compared with the group without autism. A post hoc analysis was conducted to examine whether the social context of daily events modulated perceived stress in the autistic group. Youth with autism evaluated daily social events (i.e. events in the flow of daily life during which they were in company of other people) as significantly less pleasant than events when they were alone (b = −0.449 (95% confidence interval (CI) −0.66 to −0.24), p < 0.001). Of note, 56% of the events reported by autistic participants and 62.5% of events reported by non-autistic participants were social events.
Descriptive statistics and group comparisons of EMA measures.
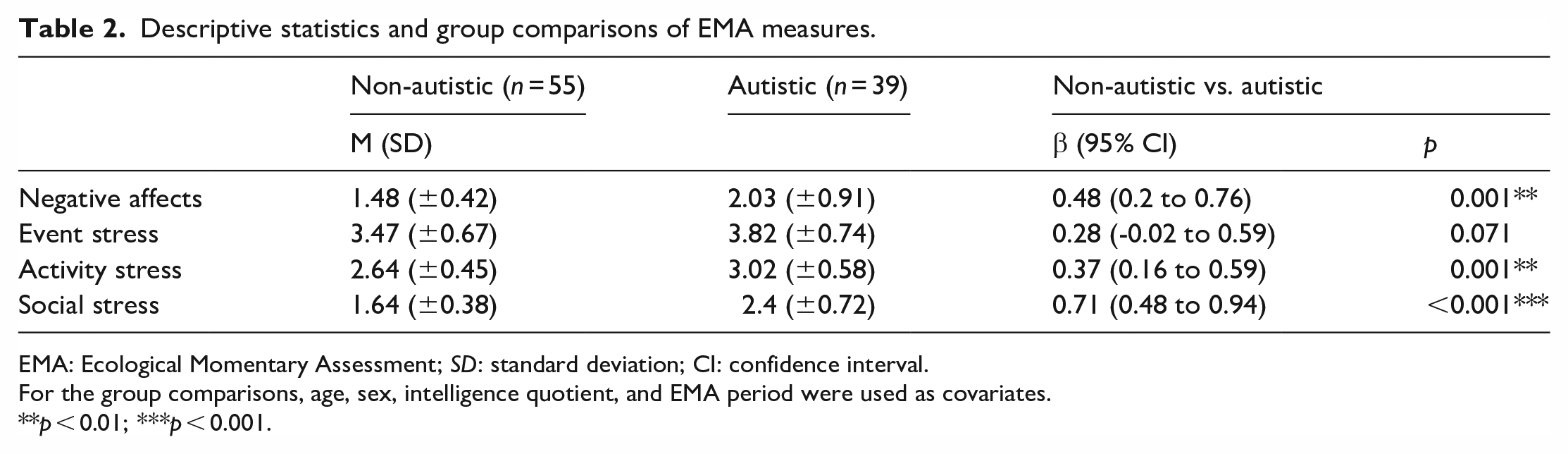
EMA: Ecological Momentary Assessment; SD: standard deviation; CI: confidence interval.
For the group comparisons, age, sex, intelligence quotient, and EMA period were used as covariates.
p < 0.01; ***p < 0.001.
Moreover, multiple linear regressions showed that the percentage of time spent alone during the week did not differ between the groups but youth with autism reported being less often engaged in activities related to social contact than the non-autistic group (Table 1).
Affective reactivity to stress
As shown in Figure 1, multilevel regression models showed that perceived stress in all three contexts was significantly associated with increased NA (Table 3). However, the stress × group interaction was only significant for activity stress, indicating that, compared with the non-autistic group, participants with autism showed increased affective reactivity to activity-related stressors, but similar reactivity to social- and event-related stressors. In participants with autism, a post hoc analysis showed increased affective reactivity to daily social events compared with nonsocial events (b = −0.069 (95% CI = −0.13 to −0.01), p = 0.017). Interestingly, affective reactivity to activity-related stress (t(38) = 3.25, p = 0.002) and event-related stress (t(37) = 2.84, p = 0.007) was higher in autistic females than in males. Age was not associated with affective reactivity to stress (data not shown). Finally, likelihood ratio tests showed that allowing intercept and slope variances to differ across groups improved the model fit, indicating greater between-person variability within autistic group compared with the non-autistic group in affective response to perceived event-related stress (standard deviation (SD) for non-autistic = 0.623, SD for autistic = 0.889, χ2(3) = 28.31, p < 0.001), activity stress (SD for non-autistic = 0.629, SD for autistic = 0.857, χ2(3) = 22.05, p < 0.001), and social stress (SD for non-autistic = 0.554, SD for autistic = 0.806, χ2(3) = 9.67, p = 0.0215).
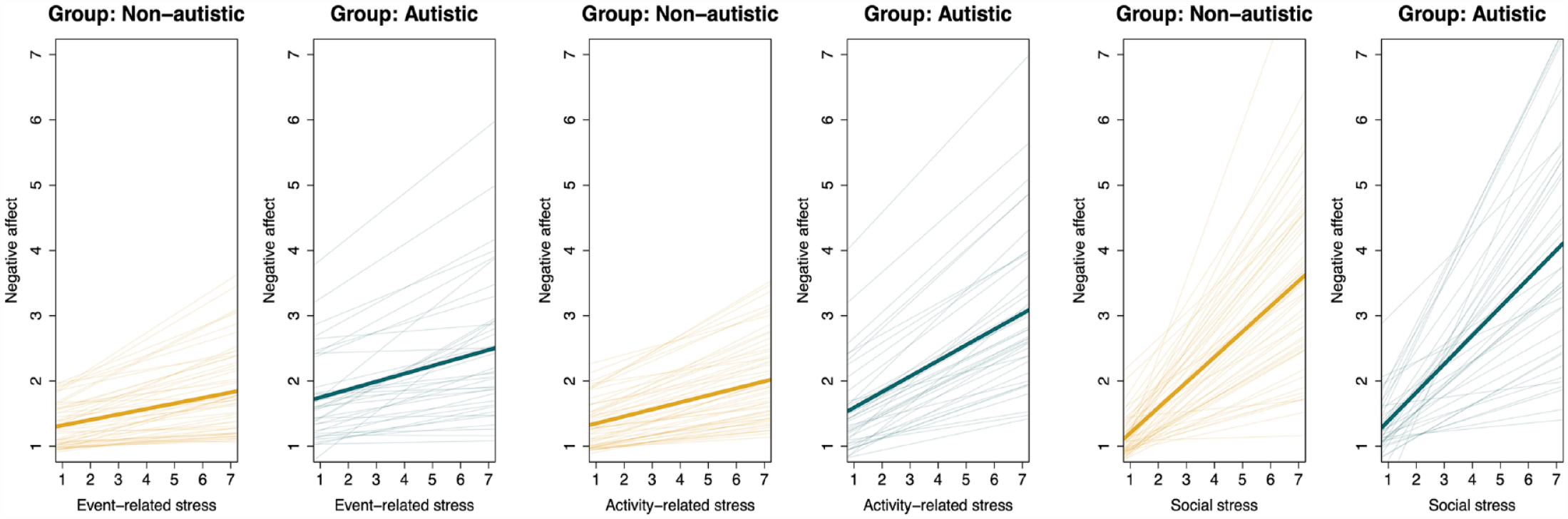
Estimated regression lines modeling the relationship between stress in different contexts and negative affect for non-autistic and autistic participants.
Associations of perceived stress and stress × group a interaction with negative affects, controlling for age, sex, intelligence quotient, and EMA period.
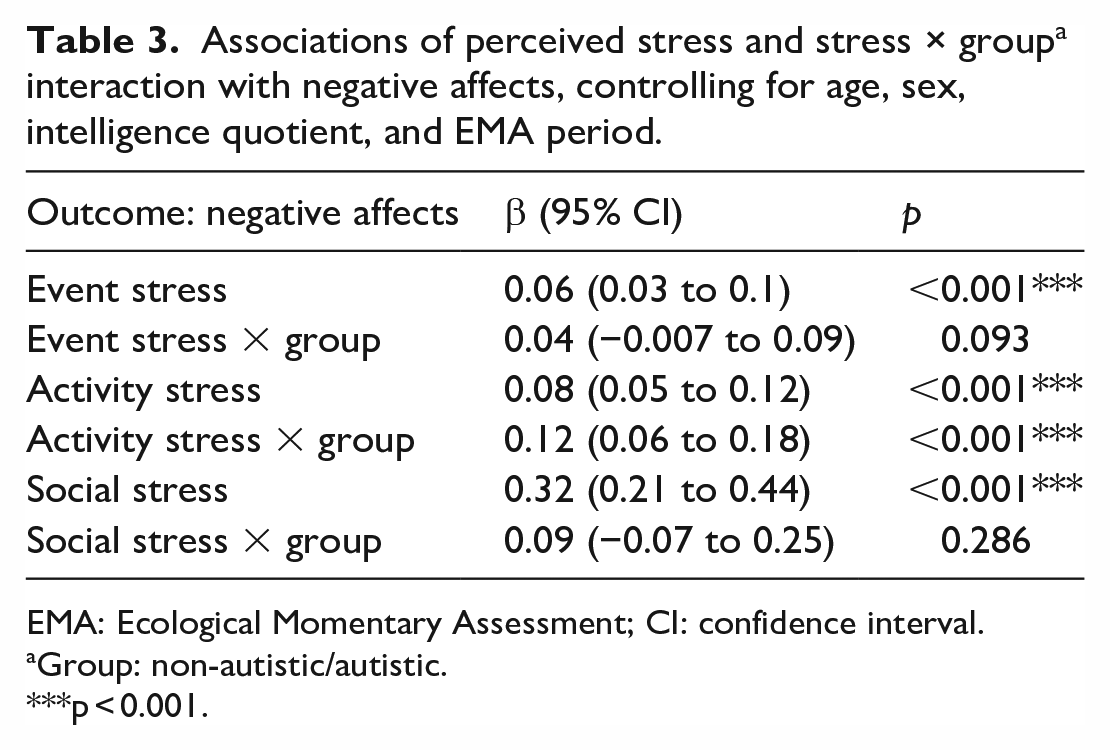
EMA: Ecological Momentary Assessment; CI: confidence interval.
Group: non-autistic/autistic.
p < 0.001.
In autistic participants, multiple linear regressions showed that affective reactivity to event-related (t(36) = 2.41, p = 0.022) and activity-related (t(37) = 2.43, p = 0.021) stressors were associated with higher internalizing mental health symptoms. However, the associations did not remain statistically significant after correcting for multiple comparisons (respective B-H thresholds were 0.0083 and 0.0042). Externalizing symptoms or the number of co-occurring psychiatric conditions were not associated with affective reactivity to stress (see Supplementary Material). Regarding social functioning, the percentage of time spent alone was not significantly associated with any stress reactivity variable, but a logistic regression analysis showed that individuals with higher event stress reactivity (OR 0.001; 95% CI = 0.000009 to 0.2, p = 0.01) and social stress reactivity (OR 0.14; 95% CI = 0.02 to 0.9, p = 0.038) tended to have a lower social functioning. However, these associations did not survive the multiple comparison correction (B-H threshold = 0.0042). Supplementary analyses were conducted to investigate whether similar associations between affective reactivity to stress and mental health would be found in non-autistic youth, but no significant associations were observed (see Supplementary Material).
Cognitive ER
Multiple linear regression models showed that participants with autism reported using significantly less adaptive and more non-adaptive cognitive ER strategies than the non-autistic group (Table 1). More specifically, they reported a less frequent use of the following strategies: positive refocusing (t(93) = −3.61, p = 0.001), refocus on planning (t(93) = −2.83, p = 0.006), positive reappraisal (t(93) = −5.27, p < 0.001), and putting into perspective (t(93) = −3.86, p < 0.001). Moreover, autistic participants reported using more often the following non-adaptive strategies: rumination (t(93) = 2.89, p = 0.005), catastrophizing (t(93) = 2.77, p = 0.007), and self-blame (t(93) = 2.46, p = 0.016).
In participants with autism, multiple linear regressions showed that more frequent use of non-adaptive cognitive ER was associated with higher levels of total (t(37) = 2.34, p = 0.025, B-H threshold = 0.0042) and internalizing mental health symptoms (t(37) = 2.22, p = 0.033, B-H threshold = 0.0083), but not with externalizing symptoms (t(37) = 1.41, p = 0.168). However, the associations did not remain significant after correcting for multiple comparisons. On the contrary, adaptive ER was not associated with co-occurring mental health symptoms. Moreover, the use of adaptive/non-adaptive ER strategies was not associated with social functioning (see Supplementary Material). A supplementary analysis did not reveal similar associations between non-adaptive ER and mental health in non-autistic individuals, but interestingly, a negative association between adaptive ER and mental health symptoms was observed (see Supplementary Material).
Finally, in the entire sample, a multilevel analysis showed that more frequent use of non-adaptive ER moderated the association between perceived stress in all the contexts and NA (Table 4). These results appeared to be driven by the group of participants with autism. Indeed, when investigating the groups separately, similar findings were observed in autistic participants, but not in the non-autistic group, except in the context of activity-related stress. In contrast, the use of adaptive ER only significantly moderated the association between event-related stress and NA in participants without autism.
The effect of cognitive ER on the stress-NA association in the entire sample and in the two groups separately.
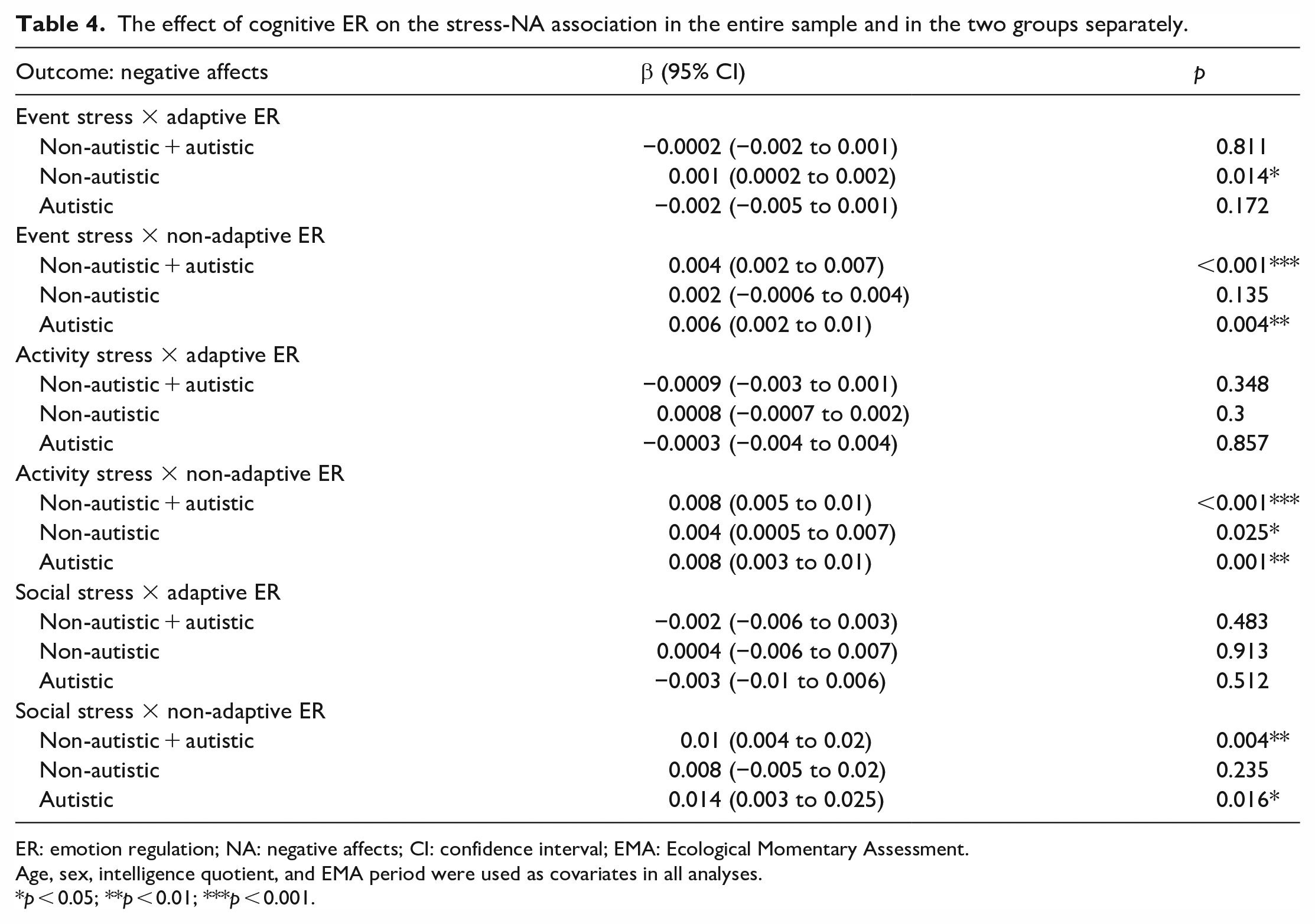
ER: emotion regulation; NA: negative affects; CI: confidence interval; EMA: Ecological Momentary Assessment.
Age, sex, intelligence quotient, and EMA period were used as covariates in all analyses.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
Our results indicate that autistic adolescents and young adults in this sample report increased levels of perceived stress related to their daily social context and activities. They also showed a heightened affective reactivity to activity-related stressors compared with their non-autistic peers. By contrast, affective reactivity to social or event-related stressors did not differ between the groups, but individuals with autism showed higher reactivity to daily social events than to nonsocial events. It should be noted that the autistic group was characterized by greater inter-individual variability in terms of affective reactivity to stress. Finally, autistic youth reported using less adaptive and more non-adaptive cognitive ER strategies than non-autistic youth, which could increase the negative impact of perceived stress; we observed that more frequent use of non-adaptive ER moderated the stress–NA association and might contribute to the severity of co-occurring mental health symptoms.
Perceived stress in daily life
Adolescents and young adults with autism reported increased levels of perceived stress related to their daily social context and activities. These results were expected, as elevated stress has already been reported in autistic adults using EMA (van der Linden et al., 2021), as well as in children and adults using self- or parent-reported questionnaires (Bishop-Fitzpatrick et al., 2017; Corbett et al., 2016; Hirvikoski & Blomqvist, 2015; McGillivray & Evert, 2018). In adolescence and emerging adulthood, puberty-related changes and the growing complexity of social relationships may increase stress levels in autistic individuals (Picci & Scherf, 2015), who might be particularly vulnerable to social stressors (Haruvi-Lamdan et al., 2020). Although significant group differences were not observed in perceived stress related to daily events, we showed that youth with autism evaluated daily social events (i.e. events during which they were in company of other people) as significantly less pleasant than nonsocial events. The heightened vulnerability to social stressors could be linked with the increased prevalence of social anxiety (Simonoff et al., 2008), as well as difficulties in social cognition and social competences (Fakhoury, 2015) associated with autism, which may lead to a more negative appraisal of social interactions. As stress and social functioning likely have a bidirectional relationship, it is also possible that repeated (chronic) stress could contribute to alterations in social behavior, such as social withdrawal (Sandi & Haller, 2015). In autistic adults, few studies have observed a link between increased stress and poorer social functioning (Bishop-Fitzpatrick et al., 2015, 2017; Haruvi-Lamdan et al., 2020). On the contrary, for some autistic people, social withdrawal might be a helpful strategy to manage stress and “autistic burnout” (see Raymaker et al., 2020), as it can reduce social load and masking of autistic traits. Indeed, for certain individuals, autism masking can be an important stressor contributing to autistic burnout and internalizing symptoms (Arnold et al., 2023; Ross et al., 2023). However, more research on the long-term impact of social withdrawal is needed. In the current study, youth with autism spent less time than the non-autistic group doing activities related to social contacts, which may suggest that they withdraw from stressful social interactions. However, they did not spend less time overall in the company of other people than non-autistic youth, potentially suggesting that their interactions are less frequently “chosen,” but occur more frequently in the family or school/work environment, without a specific purpose of interaction (Feller et al., 2023). Qualitative identification of the type of daily-life social interactions, events, and activities that are perceived as stressful by autistic youth could help us target interventions to reduce stress and the negative effects of stress, including social withdrawal. This would be particularly important because some authors have suggested that individuals with autism may experience different sources of stress than the general population (Haruvi-Lamdan et al., 2018).
Affective reactivity to stress and mental health
Although autistic individuals reported generally perceiving more stress than their non-autistic peers, not all responded to stress in the same way. In the current study, autistic youth showed increased affective reactivity to activity-related stress, in line with earlier findings in adults (van der Linden et al., 2021). This indicates that unpleasant and difficult daily-life activities might specifically impact youth with autism by increasing their NA more than their non-autistic peers. It is possible that executive functioning difficulties (Kenworthy et al., 2008) or cognitive rigidity (Leung & Zakzanis, 2014), associated with autism, could interfere with effective problem-solving and coping with perceived stress related to daily-life activities. Feelings of difficulty with daily tasks may also be related to low self-esteem, which is reported in some individuals with autism (Cooper et al., 2017), and has been linked with heightened stress reactivity (Jongeneel et al., 2018). Moreover, poor person–environment fit might further explain the fact that activity-related stressors particularly seem to impact autistic youth (e.g. Lai et al., 2020). It is possible that some of the daily-life environments, such as school and work, lack support or are not adapted to specific needs of autistic individuals, for example, in terms of sensory stimuli, which might increase NA related to daily activities. By contrast, affective reactivity to social or event-related stressors did not differ between the two groups. Regarding event-related stressors, the results are surprising as they are in contradiction with what has been previously shown in adults (van der Linden et al., 2021). The findings could possibly be explained by the type of events experienced by our sample; we observed that autistic youth reported higher NA in response to social events compared with nonsocial events, which suggests a higher affective reactivity to interpersonal stress. To our knowledge, earlier studies have not examined the quality of events nor the affective reactivity to social and nonsocial events separately.
There appeared to be quite high inter-individual differences in affective reactivity to stress within the autistic group, which is consistent with previous results regarding physiological reactivity to stress, showing a great heterogeneity in individuals with autism (for a review, see Cheng et al., 2020; Taylor & Corbett, 2014). The results could possibly be explained by heterogeneity in terms of environmental factors and/or individual characteristics. Indeed, certain environmental factors, such as high social support, could work as a protective factor against the negative effects of stress (Cohen & Wills, 1985). Another important factor explaining differences in affective reactivity to stress may be previous exposure to stressful/traumatic life events. Autistic individuals may more likely to be exposed to stressful, traumatic (early) life events than their non-autistic peers (Berg et al., 2016; Hoover & Kaufman, 2018). In particular, prior exposure to negative interpersonal events and notably bullying, which is more common in children and adolescents with autism than without autism (Maïano et al., 2016), may be related to increased reactivity to stress (Cristóbal-Narváez et al., 2016). On the contrary, several characteristics of autistic individuals could also impact their reactivity to stress. Interestingly, we observed that female autistic participants showed increased affective reactivity to activity- and event-related stressors compared with males, as previously reported in individuals with a psychotic disorder (Myin-Germeys et al., 2004). A potential explanation may be that females with autism might be more prone than males to report stressful and traumatic events, especially social ones (Haruvi-Lamdan et al., 2020; McGillivray & Evert, 2018). Heightened affective reactivity to stress in autistic females may increase their vulnerability to mental health difficulties. Moreover, individual puberty-related changes, not investigated in the current study, could have an impact on stress reactivity (van den Bos et al., 2014). It should also be noted that, even though we observed a strong positive association between perceived stress and NA, they were measured separately (i.e. current affects and appraisal of current event/activity/social context in the moment in daily life). It is therefore possible that some of the inter-individual variability could be explained by the fact that the increase in NA may not be only related to the specific stressor, but also to other factors, such as other life events, environmental demands, or personality, which were not evaluated. Future studies should further investigate the impact of these individual factors, as well as the person–environment fit, to further tackle the important question of inter-individual variability.
Autistic youth with increased sensitivity to daily stressors may be more prone to have associated mental health difficulties. We observed a positive association between increased affective reactivity to activity- and event-related stressors and internalizing mental health symptoms (e.g. anxio-depressive symptoms and withdrawal). Similarly, increased social- and event-related stress reactivity were associated with difficulties in global social functioning (i.e. social isolation). The results are consistent with some previous evidence showing a link between physiological reactivity to stress and co-occurring mental health symptoms in children with autism (Guy et al., 2014; Hollocks et al., 2014; Hollocks et al., 2016), although the topic has not been examined a lot. However, the associations of the current study should be interpreted with caution because they did not survive multiple comparison correction, possibly due to lack of power in the analyses. For future research, a larger sample size should be used to replicate the results. Moreover, another instrument to examine social isolation could be used, as the current ordered scale did not differentiate individuals very well. Moreover, the fact that we did not find an association between affective reactivity to stress and daily-life social isolation may indicate that the percentage that participants reported being alone in their daily lives is not a pure measure of social isolation. Indeed, participants may have had different opportunities to spend time with others during the EMA period; for example, participation during the COVID-19 pandemic may have resulted in limited social contact. Nonetheless, our preliminary results are important, as they support the proposition of increased affective reactivity to stress as a mechanism associated with the development of co-occurring mental health symptoms in autistic youth, as previously observed in other clinical populations (Myin-Germeys et al., 2001, 2003). As the likelihood of developing co-occurring mental health difficulties during the lifespan is increased in autistic individuals (Lai et al., 2019), possible risk and protective factors are important to define. The current study suggests that effective stress management may be a crucial target in preventing mental health symptoms. Moreover, making environmental adjustments to improve person–environment fit (Lai et al., 2020) seems important to reduce some environmental stressors, such as noise and other sensory stimuli or unpredictability of the environment, as well as negative reactions to these stressors.
Cognitive ER
One way to prevent mental health difficulties could be to work on ER. In the current study, youth with autism showed a reduced use of adaptive cognitive ER strategies (positive refocusing, refocus on planning, positive reappraisal, putting into perspective) and increased use of non-adaptive cognitive ER (rumination, catastrophizing, self-blame), in line with earlier results (Samson et al., 2015; Samson et al., 2012). As previously proposed (see Mazefsky & White, 2014), less efficient ER may be a characteristic of autism, explained by several autism-related symptoms, such as cognitive rigidity (Leung & Zakzanis, 2014), sensory sensibilities (Watling et al., 2001), or alexithymia (Kinnaird et al., 2019). Indeed, it has been shown that not only identifying one’s own emotional states (Barrett et al., 2001) but also predicting one’s emotions during future events (Werner & Gross, 2010) appears to be important for effective regulation of emotions. Difficulties in episodic future thinking, associated with reduced anticipatory pleasure, have been reported in some adolescents and young adults with autism (Feller et al., 2021). On the contrary, as the current study only examined cognitive ER, it is likely that youth also used other types of adaptive or non-adaptive strategies to (directly or indirectly) regulate their emotions, which were not captured. These might include, among others, interpersonal ER (Dixon-Gordon et al., 2015) or various behavioral strategies, such as stimming (Kapp et al., 2019), engaging in physical activity (Tse, 2020) or special interests (Patten Koenig & Hough Williams, 2017), sleeping (Palmer & Alfano, 2017), or self-injuring (Andover & Morris, 2014).
Difficulties in ER skills demonstrated by autistic youth may also be related to the high levels of co-occurring internalizing symptoms (Mazefsky et al., 2013). The current results potentially suggest that frequent use of non-adaptive cognitive ER strategies in response to daily stressors might be related to internalizing symptoms in some autistic youth through an increase in their NA, such as anxiety and sadness. Indeed, we observed that a more frequent use of non-adaptive cognitive ER increased the affective response to perceived daily-life stress, and that the effect appeared to be relatively specific to the youth with autism. The results indicate that reducing non-adaptive cognitive ER, such as rumination and catastrophizing, may be an effective strategy to prevent stress-related negative affective states and the emergence of mental health difficulties. Interventions using mindfulness techniques may be helpful, as they aim to increase appreciation of the present moment without focusing on thoughts about the past or future (Beck et al., 2021; Werner & Gross, 2010). These techniques can include, for example, Mindfulness-based Stress Reduction (Kabat-Zinn, 2003) or Mindfulness-based Cognitive Therapy (Segal et al., 2018), which have shown some effectiveness in autistic adults (Kiep et al., 2015; Sizoo & Kuiper, 2017). In contrast, adaptive ER did not have a moderating effect on the stress–NA association in the autistic group, which might be explained by the fact that other than cognitive strategies were not evaluated. It is important to further assess other types of ER strategies that may be helpful in decreasing NA in autistic youth. One important approach could be to engage with autistic young people and their families to explore their views and understading of the use of different strategies.
Limitations and future directions
We showed that the EMA can be used to study affective reactivity to stress in verbally fluent adolescents and young adults with autism. However, some methodological limitations should be considered. First, the EMA consists of subjective assessments, which means that interpretation of items may differ between individuals. To minimize this issue, all the items were reviewed with participants during installation. Moreover, most of the items required assessing internal states or personal appraisals of daily-life situations, which can be limited in some autistic individuals (Hill et al., 2004). Considering the relationship between emotion identification and ER (Barrett et al., 2001), poor identification may also result in difficulty in evaluate one’s ER strategies. It should also be noted that the CERQ questionnaire has not yet, to our knowledge, been validated for an autistic population, even though the questionnaire has previously been used in autism research (Bruggink et al., 2016; Rieffe et al., 2011). However, our results are in line with earlier findings about perceived stress and ER in individuals with autism. To limit the issue of subjective assessment, future studies could combine EMA evaluations with objective measures, such as heart rate variability or cortisol, or clinical observations. The use of more objective techniques would also allow the inclusion of a wider range of youth with autism in the studies. Indeed, our participants were verbally fluent and had mostly (above) average intellectual functioning, so the current results cannot be generalized to all youth on the autism spectrum.
Furthermore, the internal consistency of some EMA stress measures was quite low. However, a previous study has shown the validity of similar stress measures (Vaessen et al., 2015). In line with earlier research, event-related stress was measured as a subjective evaluation of unpleasantness of daily events (e.g. Myin-Germeys et al., 2001). It should be noted that this kind of approach does not consider “positive” stressors, that is, events that participants may experience as stressful but still pleasant. Indeed, although stress was conceptualized as a negative state in the current study, it is important to emphasize that stress responses are not inherently negative, but an adaptive mechanism that enhances survival (McEwen & Akil, 2020). In addition, in the current study, the compliance related to study days or measurement occasions was not investigated, and the impact of elapsed time was not considered. As we used a cross-sectional study design, we cannot do any causal interpretations about the stress–NA association, which could be examined in the future using time-lagged measures (e.g. Klippel et al., 2018). Moreover, using a longitudinal study design would allow to examine the causal relationship between affective reactivity to stress, ER, and the development of mental health difficulties.
Finally, a recent study showed that individuals’ daily use of ER strategies does not always correlate with the global self-report measures of ER (Koval et al., 2023). Therefore, investigating the use of ER strategies at the momentary level using EMA, may give us important information about specific strategies that youth tend to use in different situations, as well as their relationship with affects. This could help individualize interventions that aim to improve ER.
To conclude, the current results support earlier findings of high perceived stress and vulnerability to interpersonal stressors in adolescents and young adults with autism. Our findings also show increased affective reactivity to activity-related stressors in autistic youth. Autistic individuals with increased affective reactivity to stress may be more prone to have associated mental health symptoms, and girls and women may be more vulnerable than boys and men. To prevent stress-related NA and mental health difficulties, people working with and/or supporting autistic young people could focus on effective stress management and strategies that the youth use to manage their emotions.
Supplemental Material
sj-docx-1-aut-10.1177_13623613231204829 – Supplemental material for Cognitive emotion regulation difficulties increase affective reactivity to daily-life stress in autistic adolescents and young adults
Supplemental material, sj-docx-1-aut-10.1177_13623613231204829 for Cognitive emotion regulation difficulties increase affective reactivity to daily-life stress in autistic adolescents and young adults by Laura Ilen and Maude Schneider in Autism
Footnotes
Acknowledgements
The authors warmly thank all the participants and their families for their commitment. They also thank all the professionals and institutions with whom they collaborated for the recruitment. Finally, they thank Charlotte Dubois for her help in data collection, as well as their colleagues from the Developmental Imaging and Psychopathology Lab Research Unit (University of Geneva, PI Prof. Stephan Eliez) who participated in the recruitment and evaluation of non-autistic participants.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Ambizione grant from the Swiss National Science Foundation to M.S. (PZ00P1_174206). Open access funding was provided by the University of Geneva.
Ethical approval
The study was approved by the Cantonal Research Ethics Committee of Geneva (CCER) (2018-01117). Autistic community members were not involved in the design of this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.