
Abstract
Echolalia has been described as the repetition of words, phrases, songs or other more elaborate dialogues uttered by another person, which may be immediate or delayed (International Classification of Diseases, 11th Revision; Diagnostic and Statistical Manual of Mental Disorders, 5th ed.). Some classify echolalia as a communication impairment reflective of delay, while others consider it a restricted, repetitive pattern of behaviours, without meaningful communicative function. Little attention is given to the experiences of non-clinicians, such as parents or teachers who may hold valuable insights to further our understanding of this phenomenon. This study forms part of a larger programme of inquiry which interviewed parents (N = 133) about their experiences of their sons’ and daughters’ echolalia. Using hermeneutic phenomenological analysis in an abductive framework, we present a perspective of echolalia that has largely remained silent in literature: echolalia as an expression of neurodiversity. Participants push back against the status quo of intervention, reclaiming echolalia as being a part of their child’s identity. Participants want their children to not only enjoy their echolalia but to fully embrace it as being a part of their individual identity. We propose alternatives to a purely clinical perspective of echolalia; alternatives that may place the neurodiversity-affirmative perspectives of our participants in a co-existing tension with clinicians.
Lay abstract
Echolalia is a commonly found speech and language condition in autistic children. Children with echolalia repeat words and phrases they previously hear in place of proving a non-repetitive response. In research and when visiting speech and language services, one of the common goals is to modify these repetitions so that these children may, more socially, engage with their surrounding environment. In our research, we identified that not all parents want their children’s echolalia to be modified. Some parents want their child to be able to enjoy echolalia and others don’t want anyone to intervene because they see it as something that makes their child unique and being unique is something to be celebrated. We believe that there might be a way for speech and language services who want to modify echolalia and the parents in our study who do not want their child’s echolalia to be modified, to be able to exist side-by-side.
Keywords
Echolalia has long been a phenomenon of keen research and clinical interest, yet much uncertainty around the precise nature of this phenomenon remains. Echolalia is the common label ascribed for when a person repeats something that they previously heard (immediately following or in a delayed manner that can extend days, weeks and months later), as opposed to providing their own self-generated language (Cohn et al., 2022; Prizant, 1983; Prizant & Rydell, 1994; Schuler, 1979). Importantly, echolalia is not purely responsive in nature; rather, individuals may be able to mobilise their echolalia to initiate communicative exchanges. As such, they are not solely responsive but also sequence initiating (Sterponi & Shankey, 2014). This phenomenon has been frequently reported in a variety of populations, including autistic school-aged children (Fay, 1969; Schuler, 1979). Indeed, echolalia also forms an important part of the language acquisition and development in non-autistic populations (Bloom et al., 1974, 1976). However, when observed in autistic children, echolalia is often subjected to treatments with the aims of abatement, suppression or development towards self-generated speech.
Looking at echolalia within autism, there is a cascade of clinically situated literature designed to see echolalia modified or extinguished. Within this clinical literature, there are primarily two main paradigms that have sought to investigate echolalia, with each paradigm using their own methodologies, assessments and intervention approaches (Cohn et al., 2022; Schuler, 1979; Stiegler, 2015). One such paradigm is that of behavioural sciences, which has its roots in behavioural psychology. In the early work of Skinner (1953, 1957), who conceptualised language as a behaviour, it was offered that all language must serve the user a functional communication-based purpose. If the ‘behaviour’ did not serve a functional purpose, it was seen as not necessary. This epistemology was embraced by applied behaviour analysis (ABA) and the work of Lovaas (1966), who advanced the eradication of repetitious speech (Lovaas, 1977; Lovaas et al., 1974). Since this time, the behavioural sciences, which use the term ‘vocal stereotypy’ to label echolalia, have set about to see its abatement or suppression (Ahearn et al., 2007; Colon & Ahearn, 2019; Sloman et al., 2022). These professionals rationalise their behaviour modification therapy from the viewpoint that echolalia interferes with the learning environment, is not socially acceptable and it may hinder relationship formation (Haley et al., 2010; Healy et al., 2019; Liu-Gitz & Banda, 2009). Within literature from this platform, echolalia is often grouped together with other restrictive and repetitive behaviours (RRBs) such as hand flapping, spinning and flicking, among others (Rapp & Lanovaz, 2016; Rapp & Vollmer, 2005; Vollmer et al., 2014). It is important to note that within the behavioural sciences, while echolalia is seen as non-communicatively functional, some behaviour modification therapists highlight that it may serve other functions (Rapp & Lanovaz, 2016). Some of these functions include repetition for the purposes of self-soothing. Interestingly, while a functional purpose may have been acknowledged for echolalia by some behaviourists, modification therapies continue to suppress such repetitions and attempt to teach replacement behaviours that are seen as more socially acceptable and that serve the same function for the user, for example, Pivotal Response Training (Koegel et al., 1999; Koegel & Koegel, 2006).
In contrast to the behavioural paradigm is that of the developmental sciences. The developmental position asserts that echolalia should be modified but does not agree that this should be done through behavioural measures. Rather, this position sees echolalia as being a fundamental part in the language acquisition and development process (Prizant, 1982; Prizant & Duchan, 1981; Prizant & Rydell, 1984; Rydell & Mirenda, 1991; Stiegler, 2015). A significant difference distinguishing behavioural sciences from developmentalism is that the developmental paradigm advances that echolalia is inherently functional, with one of those functions being communication (Dyer & Hadden, 1981; Marom et al., 2018; Prizant & Duchan, 1981; Prizant & Rydell, 1984; Sterponi & Shankey, 2014). In addition to theorised communicative functions that echolalia may serve, other non-communicative functions have also been identified, including learning language and emotional self-regulation (Prizant, 2015). In this positioning, however, echolalia for non-communicative purposes is not to be modified.
Moving beyond clinical perspectives
Literature has siloed its views of echolalia generally through a clinical lens, with various modification procedures available: some to develop echolalia, others to see it abated or suppressed. There are inherent limitations when viewing echolalia solely from a clinical perspective. First, the clinical literature is generally dichotomous, with each of behaviourism and developmentalism seeking to advance their own field’s agenda. Second, the clinical lens necessarily focuses on issues and goals for therapeutic intervention, where there is an a-priori assumption that something needs to change (e.g. the suppression or development of echolalia). Third, the clinical perspective privileges the views and values of clinicians and falls short of acknowledging alternative perspectives. Consequently, echolalia is presented as an ‘all-or-nothing’ phenomenon in the context of clinical assessment and diagnosis. Finally, there is a growing movement in the literature and society to empower the voices of those who are seeking to reclaim the narrative around how previously pathologised autistic characteristics (such as repetitive behaviours, including echolalia) are conceptualised and characterised as an expression of human diversity (Nolan & McBride, 2015; Rodas, 2018; Walker, 2021). When viewing echolalia solely from a clinical perspective, neurodiversity-affirming voices are silenced and our understanding of the phenomena of echolalia is arguably the poorer. The assumptions around echolalia are naturally being re-examined as the autistic community and their allies continue to challenge long-held clinical perspectives; the clinical sphere leaves little to no room for voices, regardless of their lived experience, to broaden the narrative around conceptualisations and characterisations of autistic characteristics. Of this changing conceptualisation, recent work by Cohn et al. (2023) found that not all parents of children with echolalia agree with clinically oriented definitions, rather, they have their own formulations of a definition and description of echolalia. Specifically, the definition proposed by Cohn et al. (2023), informed by parents, moves away from historical clinical definitions which previously included specific components of function, linguistic features, and how echolalia is manifest. While the new definition includes these components, it assumes an individualistic stance by suggesting that echolalia may assume a variety of different functions, linguistic features and manifestations, among other components, and that these are largely different for each person with echolalia (Cohn et al., 2023).
Within literature, there is limited work that has taken alternative perspectives of echolalia. Some examples of alternative perspectives of echolalia can be found in works by De Jaegher (2013), Gernsbacher et al. (2016), Sterponi and de Kirby (2016) and Sterponi and Fasulo (2010). It should be noted that, while presenting echolalia in a new light, scholarship which presents alternate perspectives of echolalia is still in its infancy.
Since the conceptualisation of neurodiversity by Singer (1998), the popularity with which this perspective has been embraced by the autistic community has forced researchers, policy makers and clinicians to reconsider how best to support those who are autistic. Reframing autism as neurological differences rather than deficits, neurodiversity is a fundamental paradigm shift that positions conditions such as autism through a cultural lens. Moving away from medical and psychological paradigms has resulted in new understandings of autistic empathy, communication and social norms. Traditional therapies such as social skills interventions are no longer seen by many autists as being necessary and are often perceived as being damaging (Milton, 2018). Of this, many in the neurodiversity movement argue that individual agency (the control over one’s life) should indeed remain with the individual themselves; others, such as interventionists, or well-meaning concerned others, should not be the determiners of what behaviours a person should and should not have. Of note, the United Nations Conventions of the Rights of Persons with Disabilities supports the ideology that agency and decision making over one’s life should remain with the person themselves (United Nations, 2006).
Neurodiversity-affirming communities seek to shift the conversation towards acceptance, inclusivity of individual identity (including identifying terminology), among other endeavours (den Houting, 2019; Kapp et al., 2019; Monk et al., 2022; Pellicano & den Houting, 2022; Shaw et al., 2022).
Within the context of this lived experience revolution, a purely clinical perspective of echolalia provides little room to develop an understanding of the multiplicity of perspectives of echolalia as an experienced phenomenon, and an expression of diversity. Furthermore, a clinical perspective curtails the experiences of nearby others who have exposure to echolalia frequently but are not deemed as ‘clinically qualified’ to speak about their experiences and understandings.
This study provides insight into a perspective of echolalia that has been seldom explored in literature: echolalia as an expression of a person’s individuality, not as a speech and language condition per se. We step outside the clinical dichotomy, seeking to examine an alternative perspective of echolalia. In this study, we attend to the voices of one group who have been marginalised in this discussion, namely parents. Simply stated, the study presented in this article examines an important and previously neglected perspective of echolalia: the views of parents of autistic children who have echolalia.
Methodology
This study represents a sub-study situated within a larger programme of research (presented elsewhere) which sought to examine the experiences of one group of people who encounter echolalia frequently but who have been left on the periphery of echolalia research, namely parents. In that larger programme, 133 parents were interviewed about their experiences of echolalia through their children. The entire multifaceted parent experience in its full complexity is beyond the scope of this article; rather, presented here are the perspectives of 8 parents (from the entire 133) who share a counter-narrative to the prevailing clinically oriented assumptions of echolalia.
Research team positionality
The research team comprised of (1) a special education teacher and doctoral candidate (E.G.C.); (2) a special education teacher, academic and lecturer in special and inclusive education (M.J.H.); and (3) a clinical psychologist, academic and lecturer in disability and inclusion studies (K.R.M.).
Research design
The larger programme of research, in which this study is encapsulated, adopted a phenomenological design. Phenomenology, as a research methodology, is concerned with examining how people understand, interact with and make sense of phenomena as they are lived and brought into consciousness (Moustakas, 1994). The larger programme of inquiry is informed by Heideggerian hermeneutic phenomenology. Hermeneutic phenomenology is grounded in the philosophy of interpretations (Healy, 2011; Heidegger, 1927/2010; Smith, 2017). That is, hermeneutic phenomenology is concerned with the interpretation of phenomenon in what is known as a ‘double hermeneutic’ (Smith et al., 2009). Essentially, the participant is trying to make sense of the phenomena, and the researcher is trying to make sense of the participant who is at the same time trying to make sense for themselves (Smith, 2004). In hermeneutic phenomenology, the researchers own professional experience and connectedness to the process of inquiry are invited to contribute towards the interpretation of the participants’ own lived experience sense-making (Aijawi & Higgs, 2007; Fleming et al., 2003; Frechette & Carnevale, 2019; Reiners, 2012).
Data collection
A semi-structured online interview approach was adopted to understand how parents, legal guardians and other caregivers experience echolalia. The semi-structured interviews were conducted through online video conferencing software. Interviews were up to 40 min in duration and took place between November 2021 and March 2022. In total, there were 48 h of interview recording, the mean interview time was 21.48 min and the standard deviation was 9.90 min.
The interview protocol had a set of standard topic–related questions for demographic purposes. Aside from these questions, a discussion style interview was encouraged. Sample questions asked participants to consider the circumstances of their child and included questions such as (a) please describe a recent situation in which you experienced echolalia; (b) how do you experience echolalia; and (c) what is it like to experience echolalia through your child? We asked the questions, what does echolalia mean to parents with respect to their child, and what might be the implications for them? It is important to note that the interview facilitator did not use, or make reference to, a neurodiversity-affirmative perspective; the responses by parent participants are organic and presented ‘in their own words’.
Participant sampling
We sent out a ‘call for participants’ advertisement to several speech, language, behavioural intervention, disability and communication organisations. The aim of our study was to examine non-clinical perspectives of echolalia and as such, we specifically targeted parents, legal guardians and caregivers. We did not place any age range inclusionary criteria, nor did we limit the inclusion of people with echolalia to a specific diagnosis. If a participant was interested in participating in the research, they were required to provide written consent; the same participant was again asked to provide final verbal consent prior to the commencement of the interview.
Participant demographics
Here, this study focuses on the experiences of eight parents who present a counter-narrative to prevailing clinical assumptions of echolalia. That is to say, our larger programme of inquiry interviewed 133 parents; this study focuses on the voices of 8 of those participants. Table 1 presents a summary of the participant demographics.
Summary of neurodiversity-affirming participant demographics.
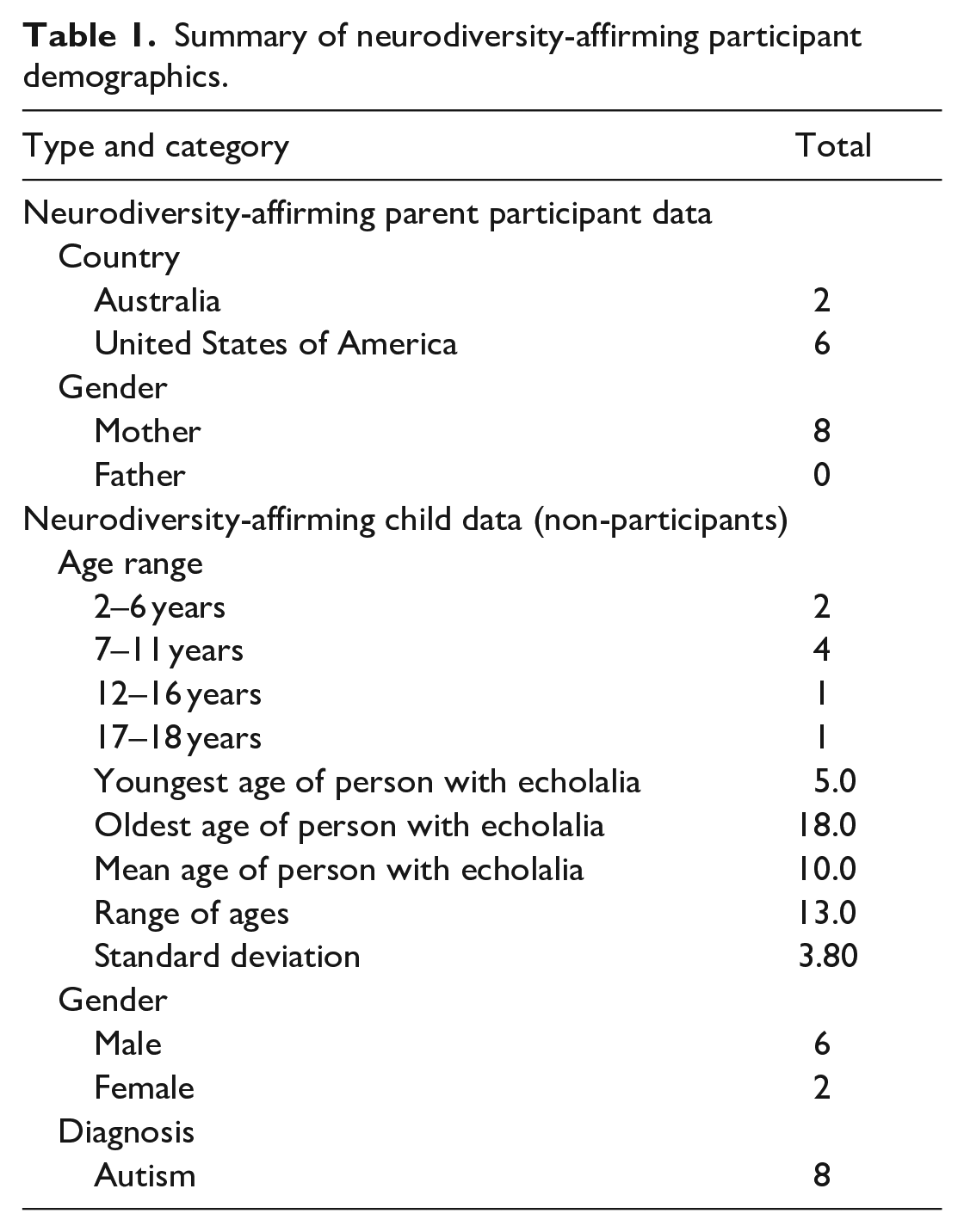
The participant profile made up of the majority of participants in each category for parents is mothers (8 of 8), who are residents of the United States of America (6 of 8). The profile of the children (non-participants) of which these parents spoke of were males (6 of 8), between the ages of 7 and 11 years (4 of 8) (Mage = 10, SD = 3.80, range = 13.0), residents of the United States of America (6 of 8), and who had a diagnosis of autism (8 of 8).
In the larger programme of inquiry, we did not place any inclusionary or exclusionary criteria based on diagnosis, and it was found that the majority of people with echolalia had received a diagnosis of autism. Specifically, of the 134 people with echolalia, 127 (95%) were reported as being autistic. The parents of the remaining seven people with echolalia (5%) did not disclose a diagnosis. In addition to autism, parents reported other co-occurring conditions such as attention-deficit hyperactivity disorder (ADHD), asthma and depression. None of the remaining co-occurring conditions, however, have been implicated as being causative, or additive, of echolalia (Ganos et al., 2012).
Community involvement
It is important to note here that this study, and the wider research inquiry, did not have any direct autistic community involvement. Importantly, this was not done by design; indeed, we want to hear the experiences and perspectives of all people outside the clinical dichotomy, regardless of whether they identified as autistic or not. Rather, parent participants did not report if they themselves identified as autistic. We acknowledge that should parent participants be autistic themselves, and potentially steeped in a neurodiversity-affirming paradigm, this might shape how they interpret their child’s echolalia. Indeed, interactions between autistic parents and their autistic children with echolalia could form part of future work.
Data analysis
Consistent with the overarching phenomenological research design, data analysis was informed by, but did not explicitly follow, the data analysis steps of interpretative phenomenological analysis (IPA) by Smith et al. (2009). The unearthing of themes and sub-themes in the analysis was conducted in an abductive framework approach, which was informed by multiple works, such as Thompson (2022) and Vila-Henninger et al. (2022). That is to say, we approached the data using a-priori reasoning in the first data pass, which was then followed by a second data pass using a-posteriori logic. A full articulation of the steps in the data analysis can be found in Supplemental Material 1.
Results and findings
Following data analysis, we found that alongside current clinical perspectives, parents also have their own formulations of how echolalia is experienced. Here, we present an emergent perspective uncovered during our analysis. It is important here to note that this study focuses on one new emergent parent perspective. We believe that this new way of seeing echolalia should be cast into its own individual examination because it presents an entirely new perspective of echolalia; a perspective which is not grounded in the prevailing clinical ways of thinking. We are presenting a new viewpoint here that warrants further research as opposed to making an overreached claim based on limited data. Simply, we invite here the consideration of non-clinical perspectives of echolalia and, more specifically, one which affirms neurodiversity.
A neurodiversity-affirmative framing of echolalia
We present here the perspectives of eight parents (6% of the total data set) that offer a counter-narrative to the prevailing clinical sphere of echolalia. This counter-narrative represents a neurodiversity-affirmative understanding of echolalia, and one which considers echolalia not as a pathology or state of development, but rather an expression of who their child is as a person.
There were eight participants who shared a neurodiversity-affirmative perspective of echolalia. Specifically, the overarching theme, termed ‘neurodiversity-affirmative perspective’, is characterised by parents who see their child’s echolalia as being enjoyed by their child and is something that rejects current social pressures with respect to what might constitute socially acceptable, neurotypical behaviour. Figure 1 presents a thematic map of the emergent theme, and sub-themes, unearthed during analysis.
Thematic map of the neurodiversity-affirmative perspective of echolalia unearthed in this study.
First, the sub-theme of enjoyment focuses on the child themselves, and echolalia offers this child an internal satisfaction which is additionally enjoyed externally by other communication partners. Next, parents aligning with the second sub-theme, rejection of social pressures, look outside the familial environment seeking to push back against the status quo ultimately reclaiming echolalia as being something that should be celebrated as another part of diversity in humans.
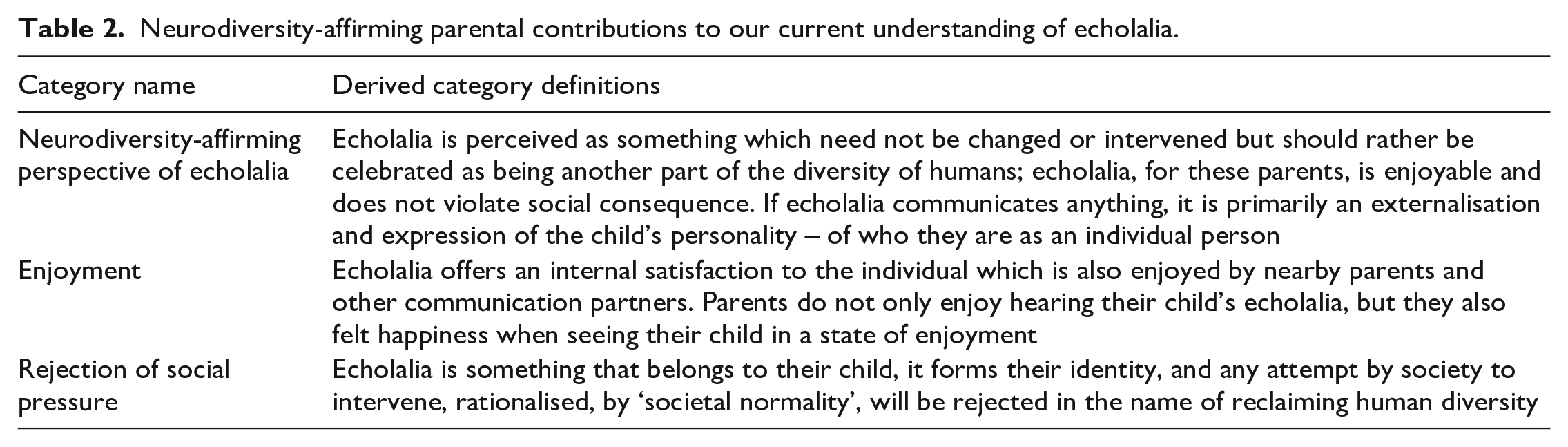
Table 2 presents the proposed new category names and derived definitions for a neurodiversity-affirming framing of echolalia.
Neurodiversity-affirming parental contributions to our current understanding of echolalia.
Enjoyment
PRNT003, a mother of a 13-year-old boy, highlighted that her son seems to enjoy repeating things. She rationalised her position as he is seemingly not hurting anyone or not repeating rude words that might overtly offend others. This parent questions the need to stop her son from echoing if it is something that he enjoys doing:
His repeating speech is something that he enjoys doing, it’s something that he likes to do, it must seem nice to him. If he is feeling good about it and it is not hurting anyone, I mean, he isn’t violent and doesn’t say rude things, if it isn’t hurting anything then why would I stop him from being himself? (PRNT003)
PRNT027 saw her son’s echolalia as something he enjoys doing. This parent held the view that stopping her son from doing something he enjoys (i.e. his echolalia) would be a ‘mean’ thing to do:
People come in all shapes and sizes; everyone is different. I see echolalia as something that my son enjoys, it makes him feel good, I can tell because he smiles, laughs, and gets excited. His echolalia is not communication but why would I want to, or want anyone else to, stop his echolalia if he likes it? That would be mean. (PRNT027)
PRNT044 also saw her son’s echolalia as being something that he does for enjoyment. This parent did not see her son’s echolalia as behavioural or communicative in nature:
Echolalia is just something that my son does, he loves the feeling of the sounds, and he gets very excited when he does it. It’s not a behaviour, but it’s also not necessarily communication, it’s something that he enjoys and if he enjoys it then I just let him do it. (PRNT044)
Similarly, PRNT020 noted that her daughter’s echolalia doesn’t need intervention – of either the developmental or behavioural kind – rather it was just her daughter being herself. This parent said, ‘I don’t see it as being anything that I need to change, either through developing it, or through removing it. I see it as just my daughter and her own unique way of enjoying herself’ (PRNT020). This parent championed her daughter’s enjoyment of echolalia and the diversity that it means for her.
In another example of a parent who saw her son’s echolalia as something he enjoys doing, PRNT067 highlighted that she also enjoys when her son repeats things because of the melodic contours he uses in his voice:
The way that my son does it is just lovely to hear, he sort of sings and goes up and down with his voice. I don’t necessarily see it as communication and I don’t think it is behavioural . . . I think that it is just him, it makes him happy and I love hearing him do it. (PRNT067)
The parents in our study, who perceived their child’s echolalia as offering enjoyment, did not interfere with their child when they hear them echoing; rather, these parents themselves gained enjoyment from hearing their children seemingly enjoying one of their autistic characteristics: echolalia.
Rejection of social pressure
Another parent, PRNT030, advocated for a neurodiversity-affirmative perspective when viewing echolalia. This parent highlighted that because echolalia might seem unconventional to some people, there is this inherent need to want to employ intervention early and consistently to echolalia so that it might be shaped to fit within societal (neurotypical) expectations:
I have always seen echolalia as something that is just to be thought of as another part of diversity in humans. I know other parents and other groups that are very concerned with saying it is one or the other, I don’t think like that. Why can’t people come to understand that maybe it just is different. But I think that because it is different it makes people uncomfortable and then they want to put it in the behavioural box or put it in the communication orientated box. It’s just human difference, its beautiful when I hear it. (PRNT030)
Another parent similarly highlighted that she enjoys hearing her son’s echolalia but also calls into question the need to change it if it brings enjoyment to him. This parent compared her son’s echolalia to the enjoyment actions that she herself does and notes that it is because echolalia is heard by others, and is noticeable in various environments, that the need to intervene (by clinicians) is brought about:
Let me tell you, I see echolalia as being a part of my sons’ identity. There have been people who say he needs intervention . . . what exactly are we intervening? And why do we need to interfere with everything? He likes it, it brings him enjoyment in a similar way that I do things for enjoyment. It’s just that because it is language it is heard by others, if he did things for enjoyment that people didn’t hear, I doubt anyone would have a problem with it. (PRNT078)
A mother of a 7-year-old boy held strong views about how she views society as seeking to interfere with everyone, almost in attempts to see people shaped into one specific way:
Why the need to change people and the things they do all the time? So what, he repeats quotes from movies sometimes, where is the harm to others in that? Not everyone needs to be modified to fit into this perfect image that society wants. Echolalia, to me, is my son, and how he exists in this world. (PRNT019)
Parents who aligned with the neurodiversity-affirmative perspective did not consider echolalia as being developmental or behavioural, nor did they see the need to interfere with it in any way. These parents highlighted that their children just have a unique way of existing in the world with their echolalia highlighting individual human difference and diversity. Any communicative or non-communicative functions that echolalia might have are not taken into consideration or even acknowledged by these parents. If echolalia communicates anything, it is primarily an externalisation and expression of the child’s unique identity – of who they are as an individual person.
Discussion
In this study, we sort to step outside the clinical dichotomy that has traditionally defined echolalia in terms of either a behavioural pathology or developmental trait. As part of a larger programme of research investigating the phenomena of echolalia from different perspectives, we attended to the experience of a sub-set of parents whose voice has not been represented in the literature, and who speak of echolalia as an important aspect of their child’s autistic identity.
Drawing on these experiences of the parents who embrace echolalia as a component of neurodiversity allows for a reconsideration of long-held and dominant views in clinical thinking. Revisiting the literature through the lens of these data raises four key questions that speak to the tensions in how society best supports the person with echolalia, with important ramifications for anyone working with these individuals, be they speech pathologists, psychologists, teachers or classroom assistants. These four specific questions emerged from discussions between the research team in debating as to why these parents held different perspectives from other perspectives in the larger programme of research. By answering these questions, the research team felt they could then hypothesise as to why this small sub-set of the broader participant pool held distinct views.
Why do many in the autistic community and their allies want to move beyond a clinical understanding?
All eight participants highlighted in the findings argued for a position of non-intervention for the person with echolalia. For example, PRNT078 brought to attention the inseparable link between the manifestation of echolalia and who their child is, as an autonomous individual. Likewise, PRNT019 rejects any need for change as an act of cultural homogenisation. These intimate, deeply personal perspectives are not discussing hypothetical individuals, but rather someone they presumably have a close bond with and with whom they share a life – their daughter or son. They recognise these people in all their complexities. Autistic authors such as Bascom (2011), Kapp (2020), Milton (2022), Milton et al. (2020), Pripas-Kapit (2020), Singer (1998, 1999) and Yergeau (2019) bring this lived experience perspective to the academic literature, recognising that the differences manifesting from autism are an intrinsic part of autistic identity. Both by inference and in some cases explicitly, the participants highlight that historical clinical paradigms provide the warrant for the erasure of autistic identity.
This sense of threat is expressed on several levels by the participants in this study, reflecting the emergence of critical voices from the social sciences that challenge the need for intervention. While the behavioural paradigm is seen as the most overtly objectionable, the developmental position still presents challenges for those who seek acceptance because it still signals pathology (e.g. delayed typical development) and the person with echolalia need to change. It is true that developmental paradigm is not grounded in a deficit framing of autism, yet it still seeks to use the differences of autism as a vehicle to change the individual to better meet the expectations of the neurotypical majority. This notion of intervening is explicitly challenged by PRNT078, who questions the continued desire to intervene with echolalia as opposed to leaving it be.
It is only when we consider the value of lived experience as qualification to decide under what condition intervention is required, in competition with traditional notions of qualification, that we can begin to understand why a growing number of autistic individuals seek to challenge the dominant clinical narratives.
What are the implications for clinicians in recognising echolalia as part of autistic identity?
There is no doubt that this shift in thinking presents several critical implications for clinicians, many of whom have dedicated their careers to attempting to ensure that their patients enjoy a high quality of life. Questioning their expertise will naturally be confronting for many, challenging the inherent values of the professions who have traditionally held the power in making these decisions. For example, PRNT030 questions a common practice of clinicians, in the way that ‘autistic behaviours’ are segmented into one view or the other. The implication here for clinicians is the viewing of the person as an autonomous individual first before segmenting their behaviour for therapy. Such a perspective aligns with the public facing shift towards recognising the importance of person-centred practice (Magowan & McGowan, 2021; Murphy & Joseph, 2019).
Systematic commercial drivers require clinicians to be positioned as interventionists, with systems such as the National Disability Insurance Scheme in Australia requiring that clinicians ‘do something’ to be compensated for their time (Dickinson et al., 2022). For example, the setup of funding models in some countries may require that parents take their children to interventionists for an extended period of time; parents in our study, who reject social pressures, would be less likely to employ interventionists over extended periods – this could have financial ramifications for both well-meaning service providers and larger disability organisations.
A preference for intervention may also be shaped by a collective sense of professional pride and a fear of redundancy, with professional associations serving to lobby policy makers to ensure their members remain the determiners of intervention. While commercial interests would foreseeably have some role in these organisations arguing for the status quo, we also recognise that clinicians are also a product of systematic social reproduction having been trained to carry forward the entrenched ableist norms of our broader society. It will undoubtedly challenge the professional identity of individual clinicians to recognise that they have been serving as a mechanism of ableism.
However, what has been presented here for consideration is very consistent with an emerging trend towards neurodiversity-affirmative practice in both speech–language therapy, where Yu and Sterponi (2023) call for ‘. . . increasing understanding of diverse ways of expressing and relating, honouring and bridging differences, and making social participation more accessible’ for autistic people (p. 28), and in psychology where there has been a call for cultural competence (in addition to clinical competence) when working with autistic people (Bulluss, 2021). Such cultural competencies enable practitioners to recognise autistic people as ‘different communicators’ rather than poor or dysfunctional communicators (Jellett & Flower, 2023). Such cultural competencies are asserted to better enable practitioners to recognise the spectrum of neurodiversity (including autism, ADHD, Tourette’s syndrome, dyslexia, dysgraphia, dyspraxia and others) are not conditions to be diagnosed with the view to simply cure. Rather, they are individual neurotypes with unique strengths, needs and challenges for the person, and the goal, if any, of ‘therapy’ is to affirm the person in their own identity, and to support the person to construct strategies that both enable them to live in a neurotypically dominated world while advocating for the acceptance and inclusion that is their right as a human being.
What might be the unintended consequences for the autistic community of moving away from a clinical understanding of autism?
We expect a strong rebuttal from clinicians who see their interventionist role as empowering rather than disenfranchising their clients with echolalia. If deferred happiness or temporary discomfort leads to ultimately achieving a more fulfilling life, then the extinction of echolalia is surely a small price to pay? Crooke and Winner (2021), for example, argue that it is vital that autistic children learn to adhere to the established social norms so that they can make friends, gain employment and be in relationships. These are worthwhile goals for anyone should they choose them, but the prescribed pathway to social nirvana is grounded by a requirement for social homogenisation. It is difficult to imagine echolalia having any place in Crooke and Winner’s previous descriptions of ideal social interactions. Arguments for sacrificing the here and now for suggested future benefits are made in relation to everything from eating vegetables to exercising regularly, but this does not align with the evidence of what we now know about echolalia. Critically, this ignores the role described by PRNT044 in these behaviours serving an important self-regulatory function. Rather than merely prioritising immediate joy to fit in with social norms, the findings of this study confirm that for some children these behaviours can be a mechanism for regulating their emotional state and an indicator for others that are in a heightened emotional state.
Stepping back from trying to locate the purpose and function of echolalia for autistic individuals, it is also important to consider where the agency should lie in determining whether a behaviour has value. Who should have agency in determining which behaviours have value for an individual? If we return to the Convention on the Rights of People with Disability (United Nations, 2006), it is clear that the central decision should be with the individual. Singer (1998) highlights a moral imperative of more than consultation, with the agency of the autistic individual to determine the conditions in which intervention is in their best interest being an unwavering human right. This is likely to be a confronting notion for parents.
To what degree should neurodiverse voices be privileged above those with clinical expertise?
Locating the position of those with lived experience in the intervention hierarchy is at the very centre of the debate between acceptance and change. In her thesis that informed much of the modern conceptual and philosophical arguments for neurodiversity, Singer (1998) called for reconsidering disability as a label ascribed to the autistic community. Complex interactions with community identity, disability rights legislation and social support funding has resulted in not everyone in the autistic community enthusiastically embracing this line of argument. Critics of those espousing support instead of intervention point to this as elitism by those with low support needs, ignoring the needs of individuals with co-occurring intellectual disabilities. This is a tension that is unlikely to resolve anytime soon. For example, a division of needs within the unified spectrum was recently observed by Lord et al. (2022), with these authors calling for a sub-classification of ‘profound autism’. For many autistic individuals, who see themselves through Singer’s autoethnographic research, this latest attempt to divide the spectrum was seen as another neurotypical warrant for the erasure of their existence.
Reviewing this debate in the context of the data analysed in this study, it is reasonable to question how representative are these eight neurodiversity positive responses of autistic individuals with high support needs? Are these the responses of carers of individuals with a range of functional needs, or do the small number of neurodiversity-positive parents suggest that this is an elite minority ignoring the plight of those with more complex needs? Alternatively, are the limited percentage of respondents espousing neurodiversity-affirmative perspectives on echolalia simply a product of historical marginalisation, and are critiques using those who have higher support needs as a shield against the valid criticisms of the recently emboldened neurodiversity movement? These questions are complex to answer but nevertheless are important to explore through future studies that give a voice to all sections of the autistic community.
One certainty that emerges from the data is the need to ensure that a range of perspectives are included in all clinical training and that the diversity of voices within the autistic community are embedded throughout teaching and learning for clinicians. While sharing research such as the present study can be a starting point, we argue that the only way for future clinicians to fully comprehend the depths of these debates is to actively learn alongside those with lived experience from the very outset of their professional education. Every clinical training programme should require the inclusion of perspectives and teaching staff with lived experiences to humanise the ‘other’ in the decision whether to embrace neurodiversity in all its facets, including echolalia or vocal stimming, or to go down the pathway of intervention.
This is especially true of the larger fields of behavioural psychology together with speech, language and communication in which echolalia has historically remained siloed. Because echolalia has historically been conceptualised as a speech, language or behavioural disorder, previous research has left little room for those with alternative arguments. This, then, raises the question: are the perspectives of our parents, who see echolalia as bringing enjoyment and rejecting social norms, strong and loud enough to privilege themselves over predominant lines of thinking? Or, has the preponderance of intervention centric, and clinical dominated literature, perhaps tunnelled our vision so that we are immune to other perspectives sitting on the periphery?
In asking these questions and considering possible answers, we hope to prompt new thinking of the complexities in deciding when, and under what conditions, accommodations are arguably more important and if acceptance is preferable to intervention.
Limitations of this study
It should be noted that there were a few limitations to the current study. We invited parents, legal guardians and other caregivers to participate but only parents responded. As a result, the experiences of others, such as teachers, classroom assistants and disability support workers, who may experience echolalia in additional contexts beyond that of parents, remain a target population for future work. Next, while our data confirm that echolalia is highly prevalent in autistic populations, future work could examine the occurrence of echolalia in those other than members of the autistic community. Finally, clinically oriented researchers may question the small number of participants on which we base a new emergent conceptualisation of neurodiversity-affirming echolalia. However, we propose this perspective as a counter-narrative pushing back against clinical perspectives that have saturated literature for decades, and in so doing seek to lay the basis for a future and more substantive programme of research, inclusive of autistic people themselves.
Contribution to science and society
Our work offers an original contribution by adding insights and nuances in difference to those that neurodiversity scholarship and autistic advocates have already offered. That is, trailblazers in the field such as Bascom (2011) and Higashida (2007, 2017), Kapp (2020), Milton (2022), Milton et al. (2020), Nolan and McBride (2015), Rodas (2018), Walker (2013, 2021) and Yergeau (2019) have created a path in the academic literature by unearthing their own lived experiences and offering advocacy. Work by Yu and Sterponi (2023), while not sharing their own lived experiences, suggests that a linguistic research method, Conversation Analysis, might be able to, when configured by academicians, offer insights into neurodiversity. However, our research, while still offering and advocating for a neurodiversity-affirmative perspective of echolalia, is of a different kind to that of these authors. Specifically, our study shares the experiences of parents of autistic children with echolalia. On that point, parents in our study are sharing their perspectives on the echolalia of their children and not themselves. It is not the parents’ own echolalia; it is the echolalia of their autistic children. That is to say, our parents might not be self-advocates, or they may not have echolalia themselves. They are sharing their experiences of echolalia through that of their children while also advocating for their autistic children. That is the first point of difference between our work and that of previous scholarship in the field.
Perhaps sharing some similarities to that of Yu and Sterponi (2023), our work adds to the neurodiversity-affirmative perspective of echolalia by using research methods, methodologies and approaches that may not necessarily be common place in the neurodiversity field. Specifically, the neurodiversity literature can be broadly stated to use autoethnographic and autobiographical methodologies that share firsthand lived experiences. We use here a phenomenological methodological approach that employs semi-structured interviewing as the data generation instrument. On that point, we did not have pre-formulated questions that sought to unearth the neurodiversity-affirmative perspective from the onset; rather, our questions asked the participants broadly what it was like for them to experience echolalia through their children. From these initial broad questions, parents were then able to share their experiences however they came to be experienced, with such experiences of parents in this study of autistic children with echolalia being that of a neurodiversity-affirmative perspective.
An additional contribution offered by our work, given that the demographics of the children in our sample are primarily those of school-age, also has implications for the intersectionality of the familial experience and the practice of educators at schools that these children might attend. Specifically, important but challenging questions can be raised from our work in relation to schools, for example: for parents who do not wish for their child’s echolalia to be intervened, how is the parental wish for the rejection of intervention to be communicated to schools? Furthermore, how can educators support their students multifaceted development (i.e. social, learning and emotional, among others), while also following the wishes of their parents? In practice, as echolalia has been observed by parents in this study, as repeating what others have just said and repeating television show lines often in a loud voice and at seemingly spontaneous times, how might educators then provide a learning environment for these children to continue to repeat (in the name of enjoyment and rejecting social pressure) while also catering for other students in the same classroom, or indeed in the ambient environment, who might have auditory sensitivities or might find echolalia disrupting? These are important and challenging questions that could be raised by our study, in which parents share their experiences on the echolalia of their autistic children, which may not have been addressed in the work of others. This is the next point of difference between our work and that of previous scholarship. The answering of these challenging questions is not the focus of this study but rather in surfacing these questions we aim to highlight how our work differs from that of others who have sought to re-frame certain speech types (including that of echolalia) in light of neurodiversity. While similar questions, answers and ideas might be raised in work in the context of a neurodiversity-affirmative perspective of autism (Bascom, 2011; Cohen et al., 2022; Crooke & Winner, 2021 Higashida, 2007, 2017; Milton, 2022; Rodas, 2018; Walker, 2021; Yergeau, 2019), there is little-to-no work, aside from the current study, that addresses echolalia specifically from within the parent experience. This is an important distinction as recent work by Cohn et al. (2023) unearthed that echolalia is defined, conceptualised and experienced differently, within the parent experience.
Conclusion and next steps
Unlike clinicians who, by virtue of their qualifications and training, seek to govern the debates and research agenda surrounding echolalia, parents in our study challenge the status quo, advocate for their children and share their perspectives from within the parental domain – something which is seldom experienced in clinical literature. Parents in our study highlight that a solely clinical perspective of echolalia is inherently limited because it does not consider the multiplicity of views of parents who experience their child’s echolalia in a firsthand manner across a far greater variety of environments and contexts – both of which are key in understanding echolalia. A clinician’s view attempts to change the person and their behaviours so that they can ‘fit’ within societal norms. Parents in our study, however, highlight that a person and their behaviours are inseparable and that any attempts to modify the latter would significantly alter the former. Simply stated, the person plus any of their associated behaviours fundamentally create that person’s identity.
We suspect that perhaps there might be a way in which neurodivergent and clinical perspectives can co-exist as a productive tension. Future work continuing with our line of thinking might seek to explore if clinical perspectives can incorporate such neurodiversity-affirmative perspectives, and if so, how this might be achieved. If harmony cannot be achieved, might more radical changes be required? Specifically, might there be an alternative means for social inclusion that supports the person with echolalia but within a new paradigm that excludes clinical intervention? Can we, as Nirje (1985) proposed, seek a world where people are free to be themselves among others?
In conclusion, we hope that this neurodiversity-affirmative perspective will serve as a catalyst for change in moving towards an understanding that echolalia can no longer be considered as a ‘condition’ of primarily clinical relevance. Rather, echolalia is a phenomenon of multiple facets and intricacies, all of which are experienced by parents. It is perhaps the work by Thoreau (1854/2004) that best summarises the sentiment of this neurodiversity-affirmative perspective of echolalia shared by parents in this study ‘if a [hu]man does not keep pace with this companions, perhaps it is because [they] hear a different drummer; let [them] step to the music which [they] hear, however measured or far away’ (Thoreau, 1854/2004, p. 281).
To that end, when one delves beneath the surface structure, it is clear that there is more to echolalia than meets the ear and that parents may have ‘specially tuned ears’ that understand echolalia in a different way and can offer considerable insight that furthers our understanding of this phenomena (Cohn et al., 2022, 2023).
Supplemental Material
10.1177_13623613231195795 – Supplemental material for ‘Let me tell you, I see echolalia as being a part of my son’s identity’: Exploring echolalia as an expression of neurodiversity from a parental perspective
Supplemental material, 10.1177_13623613231195795 for ‘Let me tell you, I see echolalia as being a part of my son’s identity’: Exploring echolalia as an expression of neurodiversity from a parental perspective by Eli G Cohn, Matthew J Harrison and Keith R McVilly in Autism
Footnotes
Authors’ note
All enquiries regarding supplemental material should be directed to the corresponding author, Eli G Cohn.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The interview protocol was reviewed and approved by the University Human Research Ethics Committee from The University of Melbourne, Australia; Approval Number 2021-22230-23628-5.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The first author, Eli G Cohn, is the recipient of the Australian Government Research Training Program Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.