
Abstract
Over the past few years, screen-based usage among children and youth has increased significantly, particularly among those with autism. Yet current screen time guidelines do not address the specific needs of autistic children and youth. Therefore, the objective of this study was to develop specific and clear guidelines and strategies that caregivers and expert clinicians agree upon to support the digital citizenship of children with autism. Using the Delphi method, 30 experts, including 20 clinicians and 10 caregivers, were invited to complete a series of three surveys. The experts had to rate their agreement levels on a series of statements that included possible guidelines and strategies. The final statements to be included in the guidelines were accepted by more than 75% of the panel. The final guidelines included six sections: (1) general principles, (2) considerations for timing and content of leisure screen time use, (3) strategies for caregivers and clinicians to monitor and regulate screen time use, (4) behaviors to monitor for screen time overuse, (5) additional guidelines for clinicians, and (6) resources. The agreed-upon guidelines developed in this study could be the stepping stones for clinical interventions targeting screen time overuse of children with autism, addressing the screen time challenges that many families are experiencing.
Lay Abstract
Children and youth with autism use screens in their daily lives and in their rehabilitation programs. Although parents and clinicians experience specific challenges when supporting positive screen time use of children and youth with autism, no detailed information for this group exists. Therefore, this study aimed to develop clear guidelines that are agreed by expert clinicians and parents of children and youth with autism. Using a method called Delphi, 30 experts—20 clinicians and 10 caregivers, who have experience working with or caring for children and youth with autism were invited to complete a series of three surveys. In each round, the experts had to rate their agreement with statements regarding screen time management. The agreement level was set to 75%. The final themes to be included in the guidelines were accepted by more than 75% of the panel. The final guidelines included six main sections: (1) general principles, (2) considerations for timing and content of leisure screen time use, (3) strategies for caregivers and clinicians to monitor and regulate screen time use, (4) behaviors to monitor for screen time overuse, (5) additional guidelines for clinicians, and (6) resources. The new guidelines developed in this study can provide potential guidance on how to further the development of digital citizenship for children and youth with autism and provide strategies to families to help manage screen time use.
Keywords
Over the past few years, there has been a significant increase in the use of screen-based technologies among children 1 and youth including the use of computers, television, tablets, video games, smartphones, and online social networking (Slobodin et al., 2019). Most children and youth, including those with autism, use these screen-based technologies as standard tools within educational, recreational, and social contexts (Good & Fang, 2015). Moreover, children’s recreational screen use has increased in recent years due to the COVID-19 pandemic (Aguilar-Farias et al., 2021; Eyimaya & Irmak, 2021). The ability to navigate through an ever-increasing digital world has become a modern-day skill necessary for this younger population to learn, a skill that is sometimes referred to as “digital citizenship.” Digital citizenship refers to ethical, safe, and responsible use of technology with capabilities related to Internet safety, online etiquette, the use of media, digital footprints, and rights and property (Lauricella et al., 2020).
While screen-based media use can support children and youth with autism to build cognitive, behavioral, and social competencies, concerns exist around the risks and harms associated with problematic screen time management (Must et al., 2014; Normand et al., 2021; Stiller & Mößle, 2018). Therefore, it is important to understand how to best support digital screen time use and digital citizenship among autistic 2 individuals and their families (Slobodin et al., 2019; Stiller & Mößle, 2018).
Normand et al. (2021) found that autistic children might be at higher risk of developing Problematic Internet Use (PIU) and Internet gaming disorder (IGD). Although IGD is not yet recognized as an official diagnosis within the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), the symptoms can cause significant difficulties and disruptions to an individual’s life (American Psychiatric Association, 2018). The relationship between problematic screen time use and autism could stem from autistic children’s increased need for solitary activities and sensory stimulation. The use of screen-based technologies may be able to fulfill both of these needs (Lane & Radesky, 2019). This makes screen-based media use a primary leisure activity for autistic children and youth (Lane & Radesky, 2019). In addition, difficulties in impulse control and response inhibition may contribute to excessive use of screen time in children and youth with autism (Slobodin et al., 2019). A recent systematic review demonstrated that these findings are in line with observations of many clinicians, that autistic children and youth are more susceptible to develop problematic behaviors associated with screen time (Normand et al., 2021). However, Normand et al. (2021) state that the main concern is not the amount of time spent with screens, but rather the consequent behaviors of excessive screen time use.
When thinking of screen use of children and youth with autism, parental attitudes and knowledge of screen time use play a major role in what manner and how often a child with autism is exposed to screen-based media (Laurie et al., 2019; Miguel-Berges et al., 2020). The role that caregivers play in influencing children’s exposure to screens includes effective parenting strategies for healthy behaviors, such as setting clear boundaries while still supporting the use of screens, allowing children to choose from educational options, and modeling healthy behaviors that will build the capacity for digital citizenship (Bowling et al., 2019).
Although the clinical field is in need of new adapted knowledge to support caregivers and clinicians in promoting healthy screen time use and digital citizenship among children and youth with autism, much of the current research focuses primarily on factors that contribute to problematic screen use. There is a substantial lack of knowledge regarding the strategies and guidelines that can limit risk factors while using technology that is beneficial, such as the use of Augmentative and Alternative Communication (AAC) (Donato et al., 2018). Apart from time restrictions, it is unclear which factors need to be considered when supporting caregivers and clinicians of children and youth with autism, and how this knowledge should be organized and provided.
Existing general screen time recommendations have been created by organizations, such as the World Health Organization (WHO), American Academy of Pediatrics (AAP), Canadian Pediatric Society (CPS), and the Canadian Society for Exercise Physiology (CSEP). However, no knowledge exists regarding screen time guidelines tailored to support the specific needs of children and youth with autism. The existing guidelines do not consider that screens may be more commonly used for educational and therapeutic purposes for this population, nor do they consider the unique challenges and risks screen use may pose (DiMartino & Schultz, 2020; Engelhard & Kollins, 2019; Goodwin et al., 2016). In addition, guidelines based on chronological age, such as the guidelines published by the WHO, AAP, CPS, and CSEP, may not be relevant for children and youth with autism as developmental regression is one of the characteristics of autism (and co-occurring intellectual disability is prevalent) (Zwaigenbaum et al., 2019). Finally, screen time guidelines for children and youth with autism should not only include recommendations about duration of use but also screen time management ideas and strategies to support caregivers and clinicians of children with autism (Mayer et al., submitted for publication).
The current study aims to contribute new knowledge regarding screen time guidelines tailored for autistic children and youth and their caregivers, and clinicians. To create and disseminate this new knowledge, we used the Knowledge to Action (KTA) model (Graham et al., 2006). The KTA model is a social constructivist model that suggests a planned action theory based on interactions and relationships with relevant stakeholders while considering specific local contexts (Graham et al., 2006; Straus et al., 2013). This framework presents a method that includes two interrelated processes: one is creating new adapted knowledge, and the other is taking action to implement the knowledge. At the core of the KTA stands knowledge creation (see Figure 1). In addition, the KTA acts as a cycle that includes the following steps: (a) identifying a specific problem and identifying the knowledge gap, (b) adapting the knowledge to the local setting, (c) identifying the barriers to, and the facilitators of, knowledge use, (d) planning and implementation, (e) monitoring knowledge use, (f) evaluating the outcomes of the implementation, and (g) developing strategies to sustain knowledge use. This framework supports planning and managing the creation and the implementation of new knowledge (Nilsen, 2020).
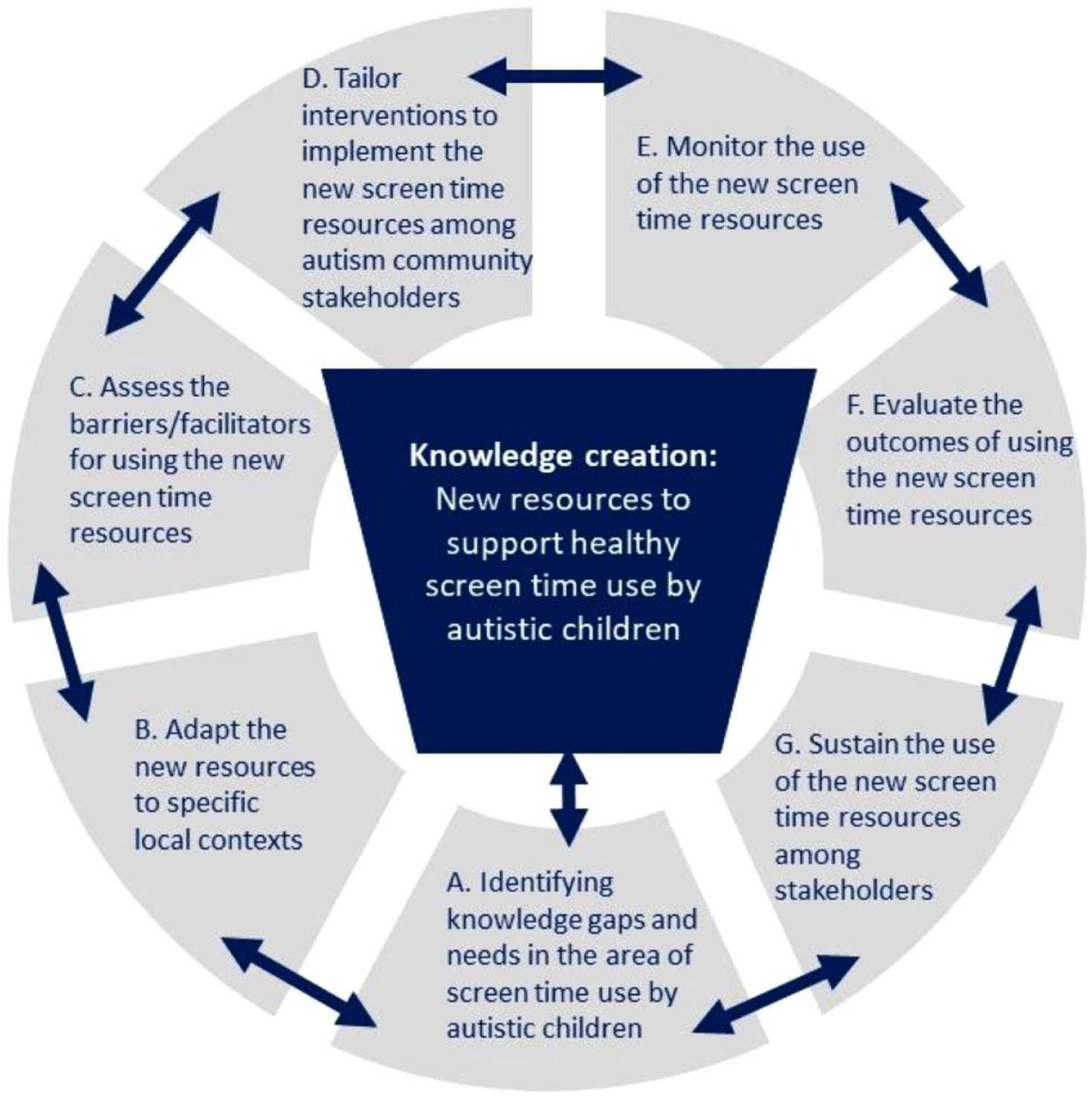
The KTA framework for creating new knowledge to support healthy screen time use by children with autism (the model is based on Graham et al., 2006).
In the former stage of this project (Mayer et al., submitted for publication), knowledge gaps in screen time management of children and youth with autism were identified (Steps A and C in the KTA model, see Figure 1). Guided by the KTA model, the former stage mapped the knowledge gaps and barriers for screen time management knowledge for children with autism. The conclusion of the former study was that there is an urgent need for accessible and useful resources that will inform screen time management for children with autism. This article describes the following stage of the study, focusing on knowledge creation phase of the framework and the creation of such needed resources (see Figure 1, core process).
This study aimed to fill the knowledge gap addressing screen time use strategies and guidelines for caregivers and clinicians of children with autism by collaborating and co-creating guidelines with knowledge users and stakeholders. Knowledge creation within the KTA model allows for the tailoring of activities to the needs of potential users (Graham et al., 2006). It is important to collaborate with knowledge users and stakeholders at this point of knowledge synthesis as it ensures usability and uptake of the knowledge by stakeholders (Graham et al., 2006).
Methods
Study design
The Delphi method, a structured iterative online survey process that is combined with controlled feedback, was employed for the purpose of this study. In addition, the Delphi method is well suited for consensus building among a diverse group of experts (Ghanouni et al., 2019; Hsu & Sandford, 2007; Powell, 2003). This methodology was ideal for this study as it allowed autism community members to contribute their opinions and prevent any one individual from dominating the consensus process (Keeney et al., 2006). It also allowed the iterative process of co-creating knowledge with community members and knowledge users (Ghanouni et al., 2019). Finally, the administration of the Delphi surveys online increased accessibility of the surveys by allowing experts in different geographical locations to participate (Ghanouni et al., 2019).
Participants
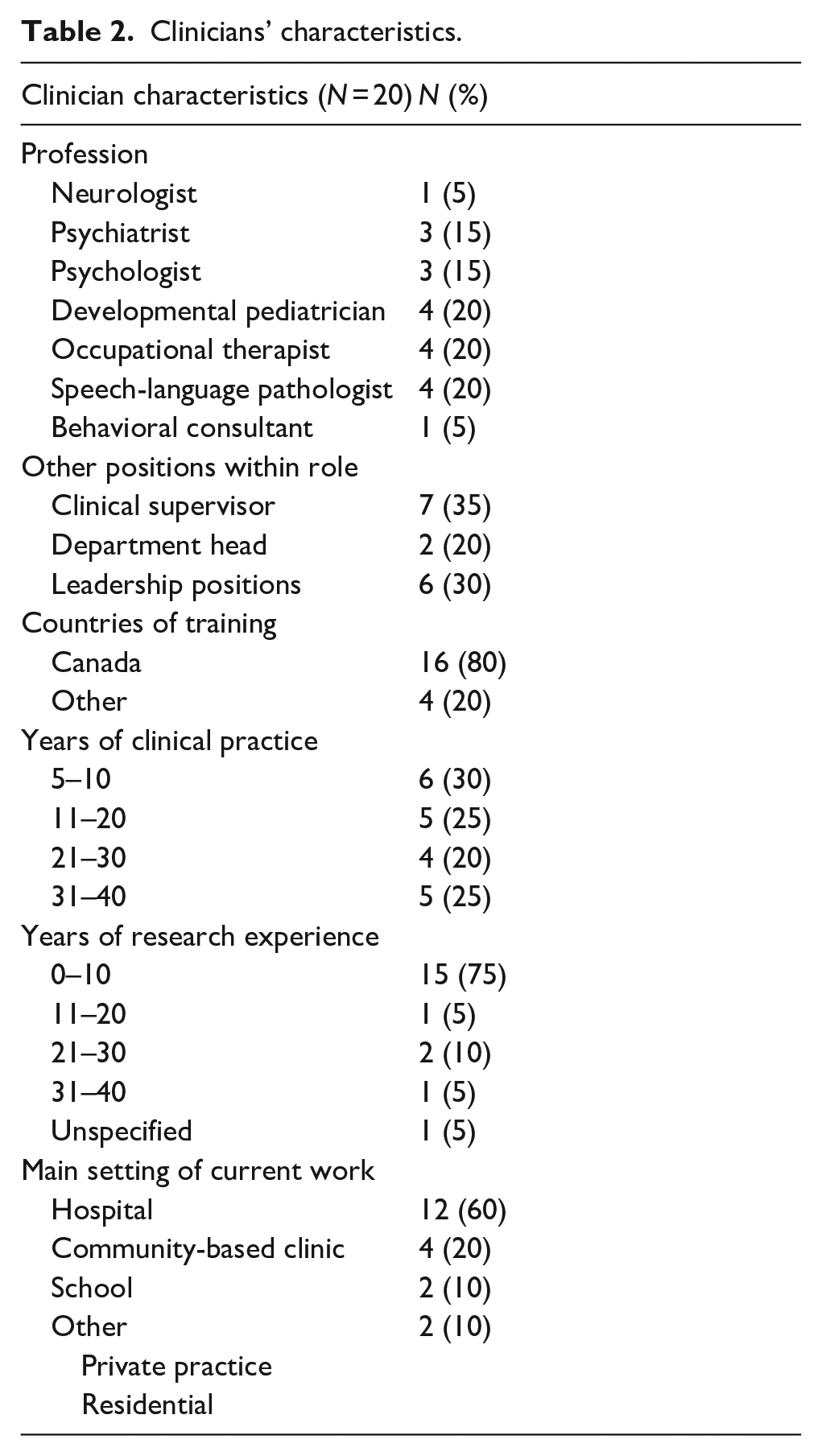
The expert panel included 20 clinicians and 10 caregivers who are caring for children and youth with autism. A larger expert clinician group allowed for the representation of different pediatric professions and as many professional perspectives as possible. The clinician group included representatives of each profession that families may meet with when asking for advice about screen time use by their children with autism (i.e. pediatricians, psychiatrists, psychologists, and occupational therapists). Two of the participants were both clinicians and caregivers and are referred to as clinicians in the calculations as they were recruited as such. Two families had three children with autism, two families had two children with autism, and eight families had one child with autism. The recruitment was purposive and expert panel members were recruited through direct contact, either by phone or by email, by the study’s primary investigators and two co-investigators. Inclusion criteria specific to clinicians included a minimum of 5 years of experience working with children or youth with autism aged 3–18 years and being known by their colleagues as expert clinicians in the field of autism. The clinicians chosen for the study were the ones who (a) are providing services for autistic children, (b) holding leadership and teaching positions within the children’s hospital, which is an academically affiliated hospital (e.g. Psychiatry Department head, Head of the Psychology Department), and (c) some are published authors in the field of autism. The study was conducted in collaboration with one of the largest developmental care centers in Canada, which allowed access to a large network of autism experts across the country. Inclusion criteria specific to caregivers included having at least one child and youth diagnosed with autism. Caregivers included in this study were known as advocates in the area of autism through their active engagement in community work and advocacy activities including participation in previous autism-related research. Ethical approval was obtained from a Behavioral Research Ethics Board from the University of British Columbia. Informed consent was obtained from the participants prior to administering the surveys. Tables 1 to 3 present the participants’ demographics.
Participants’ demographics.
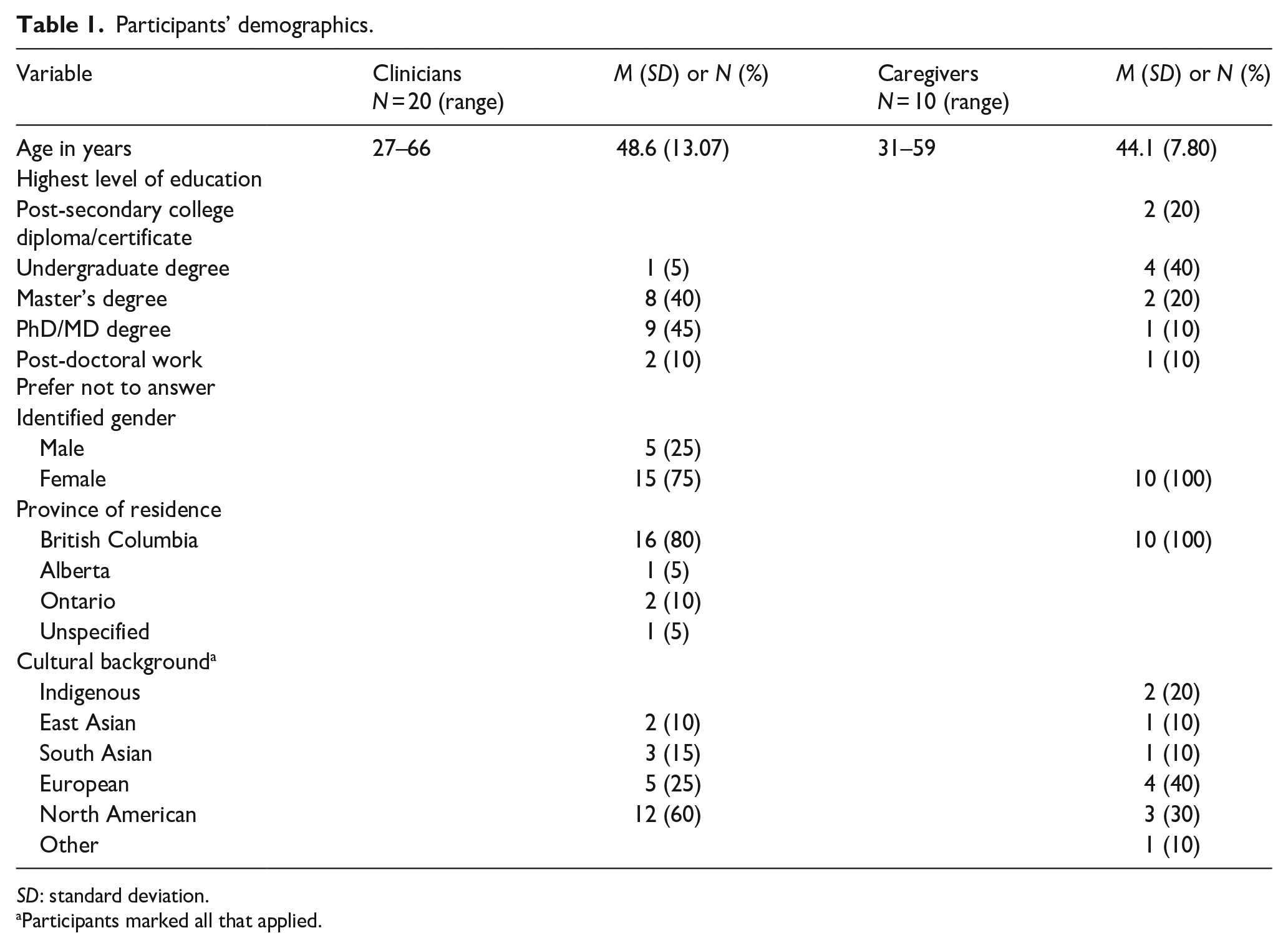
SD: standard deviation.
Participants marked all that applied.
Clinicians’ characteristics.
Parent and child characteristics.
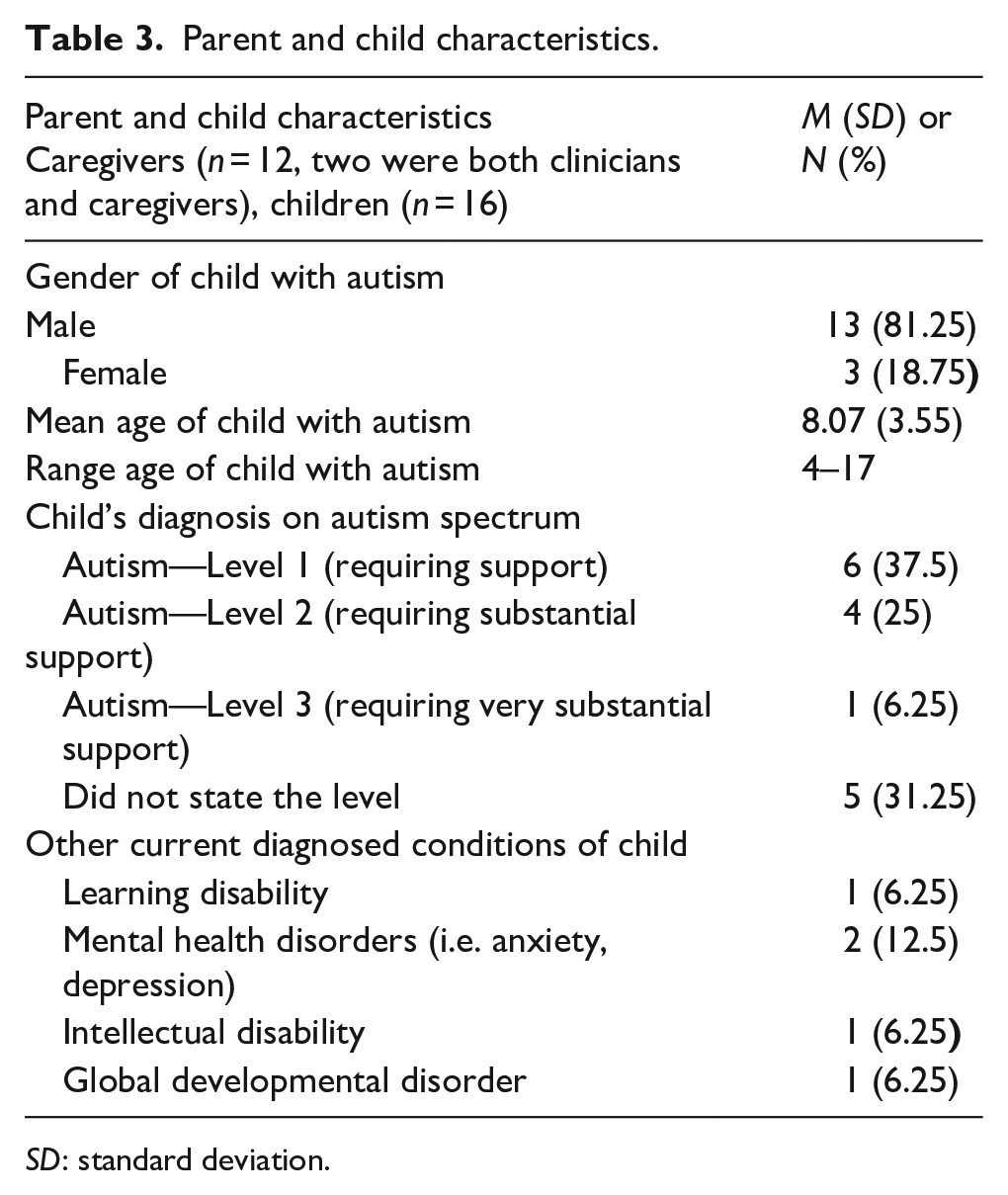
SD: standard deviation.
Procedure
The guidelines
The guidelines were developed using the following steps. First, an extensive literature search was conducted, exploring existing information about screen time management guidelines and strategies for children and youth with autism. The search was performed across five electronic databases: PsycINFO, PubMed, MEDLINE, ERIC, and CINAHL. Literature search keywords included “screen time,” “autism,” “autistic,” “autism spectrum disorder,” “guidelines,” “recommendations,” “strategies,” “children,” and “youth.” Based on the literature review, 96 guideline statements were collected. All statements were reviewed for content validity and clinical relevance by the team that included an experienced developmental pediatrician (head of the autism network in one of the largest developmental centers in Canada), a developmental pediatrician fellow, a child clinical psychologist experienced with autism, an occupational therapist professor, two Masters of Occupational Therapy students, and two caregivers of children with autism. The team screened all the guidelines and strategies to ensure that they were appropriate, respectful, relevant, and clear. The team also divided the guidelines into three sections: (a) Timing and Content of Leisure Screen Time Use (e.g.: the content of screen time should be individualized for children with autism, keeping in mind the child’s interest), (b) Strategies for Caregivers and Clinicians to Monitor and Regulate Screen Time Use (e.g. screen time management strategies should include being consistent, setting rules, using time monitoring apps, schedules, and timers), and (c) Best Ways for Implementing the Guidelines (e.g. families with children/youth with autism should be given choices when provided with screen time use recommendations). Four guideline statements were excluded as they were repetitive or unclear.
The Delphi survey
First, the research team contacted participants identified as suitable for the study individually (by email). If they agreed to participate, they were sent a link with the consent form and the research questionnaire. The expert panel responded to three rounds of surveys administered online. The first round included 92 items and had six sections: (a) general knowledge and attitudes, (b) “Red Flags” for screen time overuse, (c) screen time timing and content, (d) monitoring screen time, (e) guidelines for clinicians (adapting screen time guidelines to the family’s needs), and (f) best ways to provide the guidelines. The second survey included 19 items divided into two sections. The first included items from the first survey that were close to being agreeable, or that in which expert panel’s comments indicated if items were reworded, they were acceptable. Subsequently, wording was changed based on the expert panel’s comments and suggestions. The second section included new items that the expert panel suggested in the open comment sections of the first survey. In addition, the second round asked about inclusion of an appendix including (a) behaviors to monitor, (b) guidelines’ principles, and (c) additional resources that were developed based on feedback in the first round of surveys. The third round included seven items and addressed (a) the level of agreement on the final guidelines and (b) questions about dissemination strategies (i.e. the use of an online versus printed platform, accessibility, organization and structure, clarity, relevance, knowledge, and delivery).
In each of the Delphi surveys, the expert panel participants were asked to rate their level of agreement on the inclusion of the different items in the guidelines, using a four-point Likert-type rating scale (1—strongly disagree, 2—disagree, 3—agree, and 4—strongly agree). The expert panel also had the opportunity to explain their level of agreement or disagreement through an open-ended comments section. The Likert-type scale did not include a neutral option because it would impede the goal of reaching an agreement and make it difficult to calculate agreement or disagreement based on the total sample size (Ghanouni et al., 2019). From the time the surveys were emailed, the experts were given 4 weeks to complete the first survey and 3 weeks to complete the second and third surveys. The expert panel received email reminders to complete the survey 1 week prior to the deadline. Each survey ended only when all the 30 experts answered the survey. All the experts were rewarded with a US$450 honorarium. Furthermore, the experts were offered the opportunity to be recognized by name when publishing the results or remain anonymous. Those who asked to be acknowledged provided their names, titles and affiliation, and provided a written consent to include their information in the knowledge products. Those who asked to publish their names are acknowledged in this article and the website that includes the study results (https://asdtechnology.osot.ubc.ca.octosa.ca/section2-acknowledgements.html).
Data analysis
Surveys were analyzed both quantitatively and qualitatively. The quantitative data were analyzed using the Statistical Package for Social Sciences (SPSS). Qualitatively, written comments were analyzed using thematic analysis (Nowell et al., 2017). During data analysis, the options strongly agree and agree were considered as agreement and the options strongly disagree or disagree were considered as disagreement. The percentage of agreement was calculated by adding up the sum of the number of expert panel participants who selected agreement levels (i.e. agree and strongly agree) for an item divided by the total number of participants. To allow equal impact of caregivers and clinicians, the consensus level was calculated for each group separately and an average score of both agreement levels was calculated. Consensus was determined by 75% agreement criteria in the total score (Powell, 2003). Items that reached lower than 50% agreement were removed completely after each round of surveys. Items that reached agreement of between > 50% and < 75% or reached consensus only in one of the groups (clinicians or caregivers) were rephrased based on qualitative comments made by the experts and included in the next round (see Appendix 2; Ghanouni et al., 2019). Finally, in the final guidelines, items were combined if the expert panel indicated that they contained similar content (Berglund et al., 2017; Ghanouni et al., 2019).
Community involvement statement
All the authors are clinicians—three are occupational therapists, one is a child clinical psychologist with a specialty in working with children with autism, and two are developmental pediatricians based in a large children’s hospital specializing in diagnosing and providing care for children with autism and associated neurodevelopmental diagnoses.
Results
Survey 1
General knowledge and attitudes toward autism and screen time
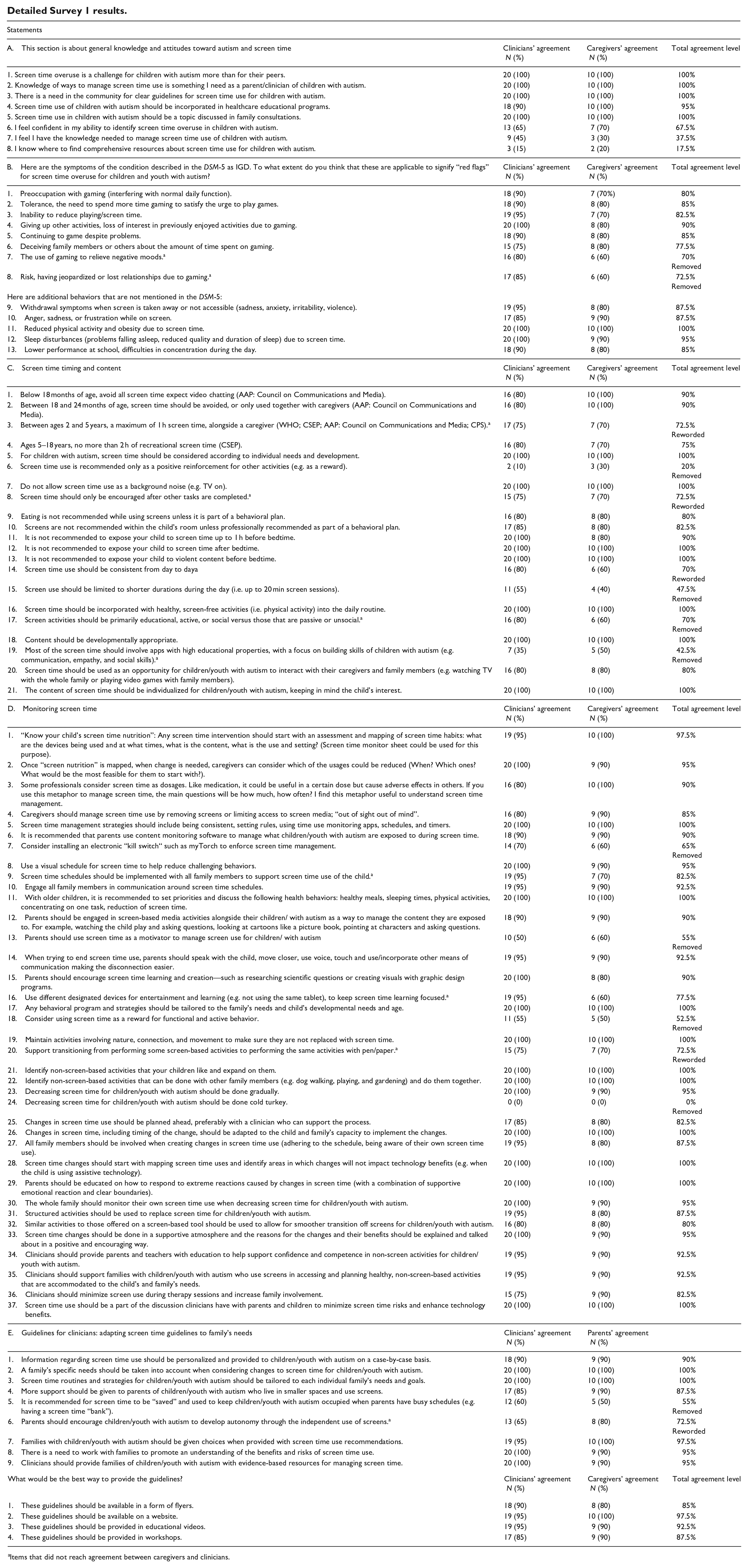
The first section included items regarding general knowledge and attitudes toward autism and screen time management (see Appendix 1). The data indicated that 100% of the panel agreed that screen time overuse represented a notable challenge with autistic children and youth in comparison to their neurotypical peers, and that knowledge about screen time management among this population is highly important yet still scarce. Only a few experts indicated that they were aware of relevant resources and most of the experts (N = 25, 83.3%) indicated that they were not familiar with resources specific to screen time management for children and youth with autism.
Consensus levels and inclusion or removing items
Overall, 92 items were included in the first survey: 8 of them addressed general knowledge and attitudes toward screen time use of children with autism, and 4 of them addressed the best ways to disseminate the new knowledge. However, 76 items in the first survey reached consensus; 75% agreement across the panel was reached regarding 64 guideline-specific statements from these items (see Table 4). See Appendix 2 for details on all guidelines and their respective agreement level for Survey 1.
Total number of statements that reached agreement (Survey 1).
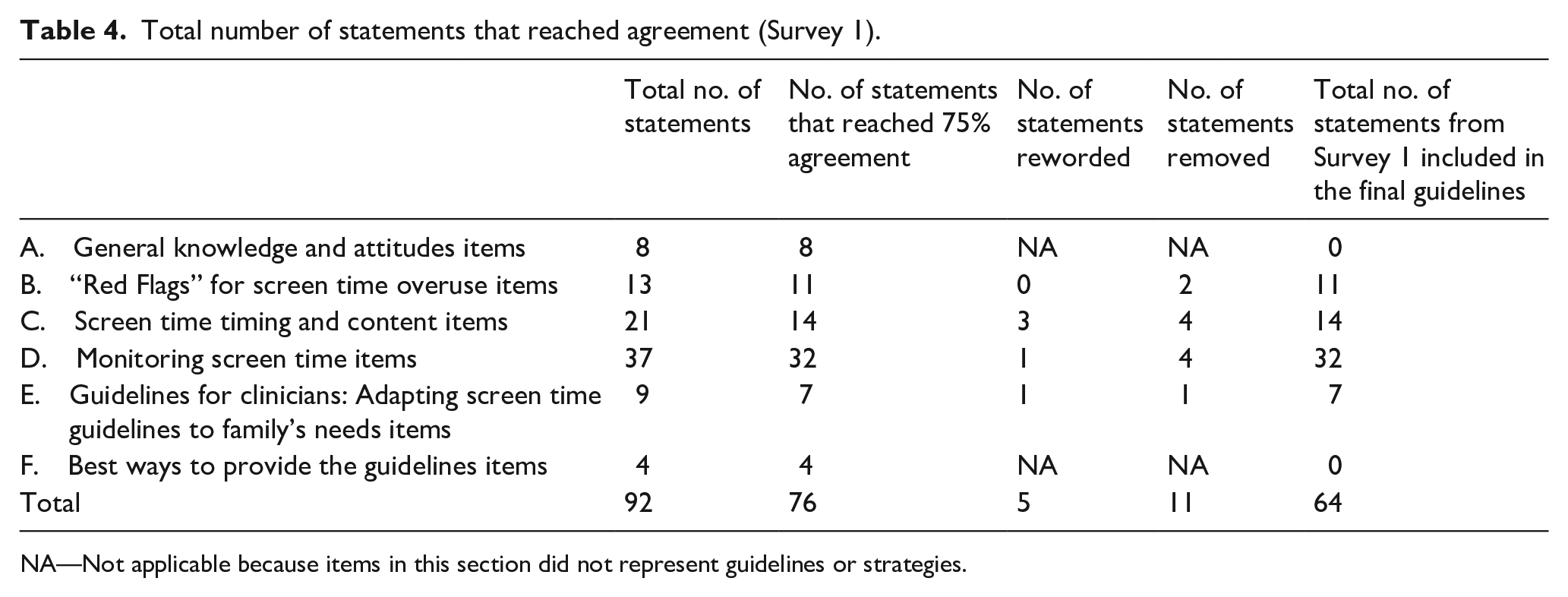
NA—Not applicable because items in this section did not represent guidelines or strategies.
Clinicians and caregivers had different agreement levels on 11 statements (all items are marked with a star in Appendix 1). For example, while clinicians as a group reached the 75% agreement criteria on the statement “screen time use should be consistent from day to day,” only 60% agreement was reached among caregivers. Comments from caregivers reflected a need for the guidelines to be flexible and individualized according to the needs of the family. Caregivers also commented that there was limited consistency with their family routines due to the nature of having a child with autism. However, 95% of clinicians agreed on the following statement: “use different designated devices for entertainment and learning to keep screen time learning focused.” However, this statement only reached 60% agreement among caregivers. Caregivers commented on possible financial limitations as a barrier for families to own multiple devices; therefore, the words “if feasible” were added. In addition, caregivers reached a 90% agreement level on the statement “clinicians should minimize screen use during therapy sessions and increase family involvement” while clinicians only reached 75% agreement level. This statement was included because it reached the total agreement level needed. Statements that elicited disagreement among one group but not the other were reworded and presented to the experts in the next rounds.
Developing a new section based on experts’ feedback
Based on experts’ feedback, it was apparent that there was a need to develop a new section that included overarching principles related to considerations in the use of technology. These statements were developed based on a thematic analysis of the rich and detailed feedback from the expert panel (Nowell et al., 2017). These principles were (a) the ubiquitous nature of technology and screens in modern day society, (b) digital citizenship as a necessary everyday skill for all children, (c) the importance of individual values, meanings, and needs of families, (d) the need for a respectful and collaborative approach to screen time monitoring, (e) the agency and ownership of children over their screen time decisions, and (f) the developmental and dynamic nature of screen time use. These principles were presented in the second survey to evaluate the panel’s level of agreement in relation to this new addition.
Survey 2 results
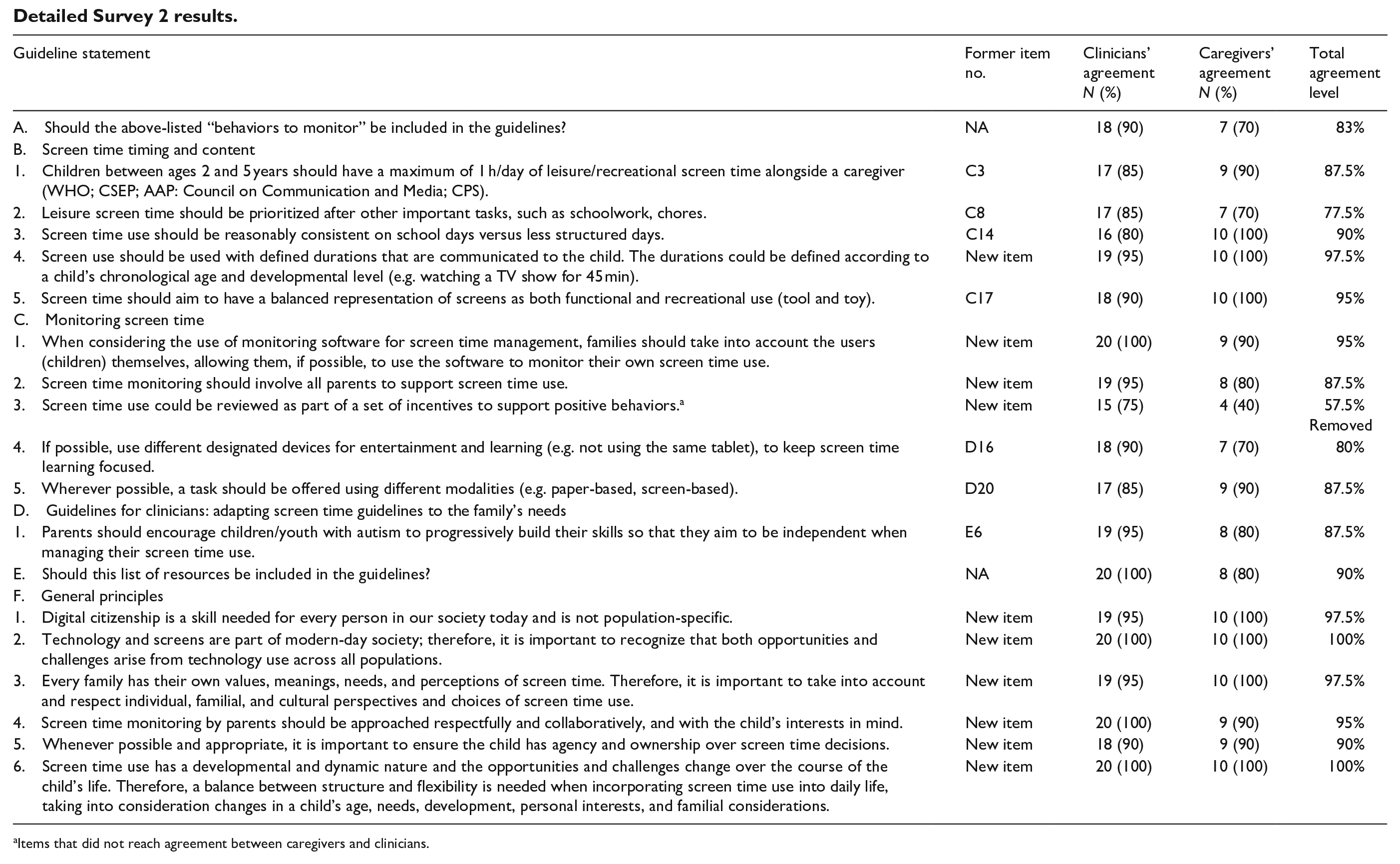
The second survey included 19 items: 10 items were newly based on the comments from the first survey and 9 items were reworded statements from the first survey (see Table 5 and Appendix 3). One item, screen time as incentive, did not reach agreement and was removed from the guidelines. Consensus was reached among experts to include a list of behaviors to monitor for screen time overuse (83% consensus) and 13 screen time resources (90% consensus) in the final set of guidelines. Agreement above 75% was also reached on the six additional statements related to special considerations and principles, created based on the panel’s feedback within comments highlighting the importance of considering values when addressing screen time management of children with autism.
Total number of statements that reached agreement (Survey 2).
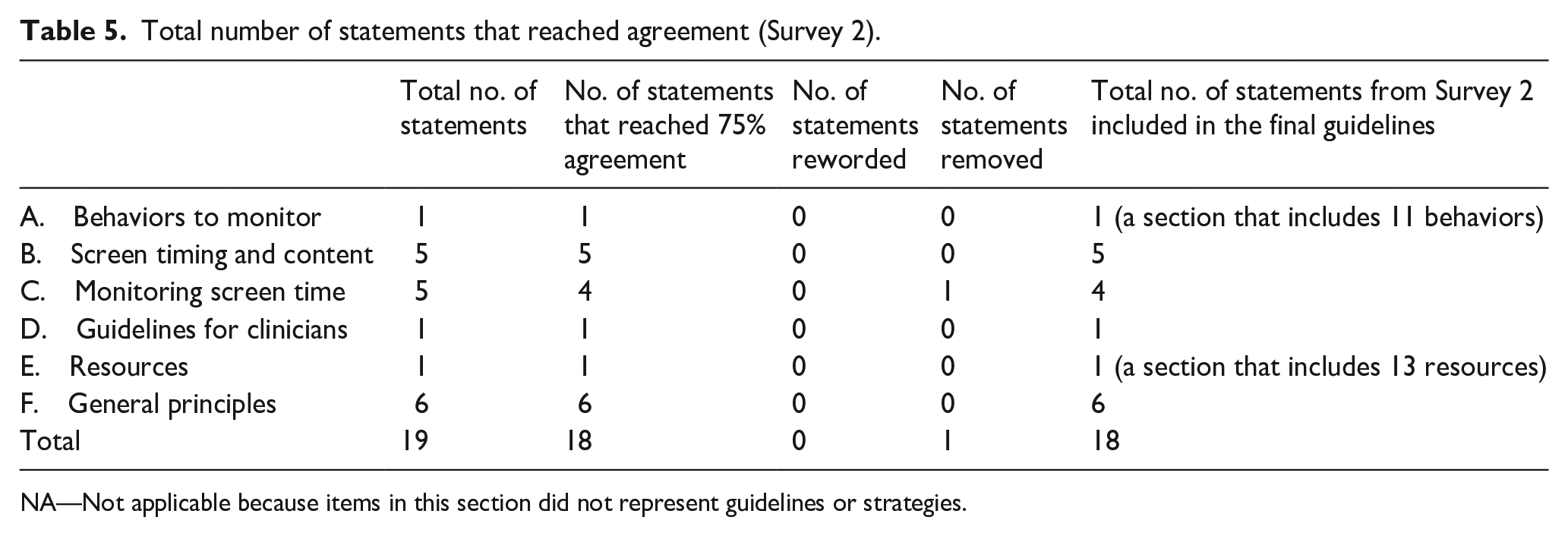
NA—Not applicable because items in this section did not represent guidelines or strategies.
Survey 3 results
In the third survey, experts were asked about the final list of guidelines. Overall, 100% of the experts agreed with the final guidelines. However, 25 (83.3%) of the experts agreed that a booklet (online or printed) would be a “good way” to share the guidelines. Experts also reached above 95% agreement that accessibility, organization and structure, clarity, relevance, knowledge and delivery are important aspects to consider within the knowledge translation product for the next phase of this project. Survey 3 also provided an opportunity for experts to offer final comments. In the comments, many experts stated they agreed with the content in the guidelines and made suggestions relating to the organization of the statements. The experts suggested highlighting the main portion of the guidelines focused on timing, content, and strategies and to leave the other parts, such as resources, as additional sections not included in the main guidelines. The experts also suggested reorganizing the list of resources by topic. These comments were taken into account and the final guidelines document was reorganized accordingly (see Appendix 3). The guidelines were also made available to the public at this link: https://asdtechnology.osot.ubc.ca/screen-time-use-guidelines/
Discussion
The purpose of this study was to fill the knowledge gap of screen time recommendations and to promote digital citizenship of autistic children and youth by collaborating and co-creating new guidelines with knowledge users and stakeholders. Some might question why guidelines and strategies for screen time use should be tailored specifically for autistic children. One of the reasons is that children and youth with autism use technology in their rehabilitation, learning, and leisure more than their neurotypical peers (Gwynette et al., 2018; Slobodin et al., 2019; Stiller & Mößle, 2018). The common screen time use guidelines that solely address the duration of use are not applicable or useful, and may cause shame and guilt among caregivers and clinicians. In addition, because of the unique characteristics of children with autism, screen time management may pose unique challenges and require adapted strategies, as indicated by the experts in the first survey.
Previous studies primarily examine screen time habits as well as benefits and risks of screen time use for autistic children and youth (Gwynette et al., 2018; Slobodin et al., 2019; Stiller & Mößle, 2018). While past literature presents valuable but generalized and non-specific information regarding screen time use in the lives of children and youth with autism, this study outlines specific ways in which caregivers and clinicians can best support the use of screen time among this population. Our work adds to the existing literature by demonstrating the importance of engaging clinicians and caregivers as knowledge users in the development of new resources. We found that while there was abundant agreement among both caregivers and clinicians that screen time for autistic children and youth needed to be managed, there was also an acknowledgment of the benefits of screen-based technology within their daily lives. These findings reinforce existing literature that support the healthy use of screen-based media (Reid Chassiakos et al., 2016).
The KTA model was a sound methodological framework that guided the steps necessary to develop such knowledge (Graham et al., 2006). The importance of engaging communities and knowledge users in developing knowledge was well demonstrated in this study—guidelines that did not reach an agreement were removed. Other guidelines were developed based on the feedback and knowledge produced by the panel of experts. The panel added an important section that included general principles. This section adds to the humanistic spirit of the guidelines and the child- and family-centered approach that guided this study. This humanistic approach in digital citizenship education is fundamental because this topic could easily cause shame and guilt among caregivers of children with autism (Mayer et al., submitted for publication). Therefore, it is imperative to create knowledge and develop supportive, respectful, and feasible interventions that do not in any way enhance the emotional burden of caregivers raising children with autism.
The guidelines that were developed in this study are based on the understanding that most families and children have a relationship with technology within the household and family structure. The use of technology and digital citizenship is a critical skill in our modern age. The guidelines aim to address the importance of digital citizenship and acknowledge how to best support the needs of children and youth with autism in promoting their well-being and inclusion in society. The newly developed guidelines are extensively different from the existing ones. The existing guidelines contain durations only, do not include any practical strategies to implement changes, and are not specific for children with autism. The final new guidelines focused on two main themes: (1) managing the amount of time of screen use and (2) managing the content of screen use. The first theme addressed included considerations, such as how daily screen time use should be organized for children or youth with autism, how changes to timing this use should be implemented and maintained, and the applicability of existing screen time use guidelines. The content section included preferred content types for children and youth with autism, strategies to manage screen time content, and recommendations on how autistic children and youth should be engaged in non-screen activities to reduce screen time and enhance other healthy activities. These two sections provide tangible and practical strategies and suggestions for managing screen time. In addition, the experts raised an important new section that should be included in the guidelines: the principles and values that should guide screen time management. These principles may serve as a compass when educating clinicians and caregivers regarding digital citizenship of children and youth with autism.
This work is one of the first studies that engages knowledge users and stakeholders in the creation of a screen time resource for autistic children and youth. While we did not examine how these guidelines may apply to neurotypical children, we can assume that many of the guidelines apply to other groups of children. Nevertheless, some of the guidelines take into consideration the unique needs of autistic children. For example, when considering implementing changes, many suggested strategies would be important in supporting the transition challenge for autistic children and their families. The guidelines are worded to support the family as a whole, assuming that changes should be useful and feasible. “Family-friendly” interventions are essential for children with autism, so caregivers can quickly implement and easily maintain these strategies in their natural environments and during ongoing daily activities (Schreibman et al., 2015).
The participation of both clinicians and caregivers was essential. The unique background of each clinician contributed to the development of new themes in the guidelines and the inclusion of both caregivers and clinicians brought different perspectives together. One of the implications of this model is the importance of analyzing group differences and not treating the panel as one homogeneous group. Differences in agreement levels between caregivers and clinicians revealed interesting gaps in perspectives. For example, 95% of clinicians agreed with the following statement: “Use different designated devices for entertainment and learning to keep screen time learning focused.” However, this statement only reached 60% agreement among caregivers. Within the comments, caregivers raised financial issues as a possible barrier to implementing such a strategy. This is an interesting finding that calls out clinicians to be aware of socio-economic issues and the financial burden that families raising children with autism may face and consider that when creating treatment plans and intervention programs.
The co-creation of knowledge also has the potential to increase the speed of which new knowledge can be converted into practice (Pearce et al., 2020). The next step in applying this knowledge to practice will be to monitor use of the website, the knowledge translation strategy that has been developed, and evaluate the outcomes to measure if the translation of knowledge is yielding the desired outcome (Graham et al., 2006).
Limitations
The findings from the study may be limited for several reasons. First, the study was conducted mainly in Canada—more global, diverse perspectives could be included in the future to better validate the guidelines. Second, the purposeful sampling method and lack of randomization of experts may affect the perspectives shared by the panel. At the same time, some voices are not heard and included in the new guidelines. This is also related to the Delphi method which, by its nature, consists of a limited sample of experts. To address this limitation, future studies will share the new guidelines with a more extensive and randomized sample of stakeholders to receive feedback, include more voices, and adapt the guidelines accordingly. Challenges may exist in the implementation of screen time guidelines, and gaps exist between the existence of knowledge and the implementation of such knowledge. It was difficult to encompass the large diversity among families and children within the guidelines but we addressed this by creating guidelines that incorporated inclusive language.
Implications and future directions
Going forward, the guidelines will need to be examined and tested for their applicability and agreement among diverse family and clinician populations. The guidelines and strategies can be used as an educational tool in the area of screen time use with autistic children and youth, provide guidance for caregivers and clinicians on the best ways to use screen time, and highlight strategies on how to mediate screen time conflicts. These guidelines are the stepping stones for clinical interventions for screen time use of children and youth with autism. Clinicians can use this resource for their professional education and as a tool to provide caregivers and families with information that can be used to plan screen time changes. The urgency for screen use guidelines specific to children and youth with autism is evident in experts requesting to begin implementation of the guidelines as soon as possible, highlighting a valuable connection between research and its use in the greater community. The KTA framework will also be used in future steps of the project to understand the experiences of using the new knowledge (Ramos-Morcillo et al., 2020) and to continue developing the suggested guidelines.
Footnotes
Appendix 1
Detailed Survey 1 results.
| Statements | |||
| A. This section is about general knowledge and attitudes toward autism and screen time | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
| 1. Screen time overuse is a challenge for children with autism more than for their peers. | 20 (100) | 10 (100) | 100% |
| 2. Knowledge of ways to manage screen time use is something I need as a parent/clinician of children with autism. | 20 (100) | 10 (100) | 100% |
| 3. There is a need in the community for clear guidelines for screen time use for children with autism. | 20 (100) | 10 (100) | 100% |
| 4. Screen time use of children with autism should be incorporated in healthcare educational programs. | 18 (90) | 10 (100) | 95% |
| 5. Screen time use in children with autism should be a topic discussed in family consultations. | 20 (100) | 10 (100) | 100% |
| 6. I feel confident in my ability to identify screen time overuse in children with autism. | 13 (65) | 7 (70) | 67.5% |
| 7. I feel I have the knowledge needed to manage screen time use of children with autism. | 9 (45) | 3 (30) | 37.5% |
| 8. I know where to find comprehensive resources about screen time use for children with autism. | 3 (15) | 2 (20) | 17.5% |
| B. Here are the symptoms of the condition described in the DSM-5 as IGD. To what extent do you think that these are applicable to signify “red flags” for screen time overuse for children and youth with autism? | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
| 1. Preoccupation with gaming (interfering with normal daily function). | 18 (90) | 7 (70%) | 80% |
| 2. Tolerance, the need to spend more time gaming to satisfy the urge to play games. | 18 (90) | 8 (80) | 85% |
| 3. Inability to reduce playing/screen time. | 19 (95) | 7 (70) | 82.5% |
| 4. Giving up other activities, loss of interest in previously enjoyed activities due to gaming. | 20 (100) | 8 (80) | 90% |
| 5. Continuing to game despite problems. | 18 (90) | 8 (80) | 85% |
| 6. Deceiving family members or others about the amount of time spent on gaming. | 15 (75) | 8 (80) | 77.5% |
| 7. The use of gaming to relieve negative moods. a | 16 (80) | 6 (60) | 70% |
| 8. Risk, having jeopardized or lost relationships due to gaming. a | 17 (85) | 6 (60) | 72.5% |
| Here are additional behaviors that are not mentioned in the DSM-5: | |||
| 9. Withdrawal symptoms when screen is taken away or not accessible (sadness, anxiety, irritability, violence). | 19 (95) | 8 (80) | 87.5% |
| 10. Anger, sadness, or frustration while on screen. | 17 (85) | 9 (90) | 87.5% |
| 11. Reduced physical activity and obesity due to screen time. | 20 (100) | 10 (100) | 100% |
| 12. Sleep disturbances (problems falling asleep, reduced quality and duration of sleep) due to screen time. | 20 (100) | 9 (90) | 95% |
| 13. Lower performance at school, difficulties in concentration during the day. | 18 (90) | 8 (80) | 85% |
| C. Screen time timing and content | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
| 1. Below 18 months of age, avoid all screen time expect video chatting (AAP: Council on Communications and Media). | 16 (80) | 10 (100) | 90% |
| 2. Between 18 and 24 months of age, screen time should be avoided, or only used together with caregivers (AAP: Council on Communications and Media). | 16 (80) | 10 (100) | 90% |
| 3. Between ages 2 and 5 years, a maximum of 1 h screen time, alongside a caregiver (WHO; CSEP; AAP: Council on Communications and Media; CPS). a | 17 (75) | 7 (70) | 72.5% |
| 4. Ages 5–18 years, no more than 2 h of recreational screen time (CSEP). | 16 (80) | 7 (70) | 75% |
| 5. For children with autism, screen time should be considered according to individual needs and development. | 20 (100) | 10 (100) | 100% |
| 6. Screen time use is recommended only as a positive reinforcement for other activities (e.g. as a reward). | 2 (10) | 3 (30) | 20% |
| 7. Do not allow screen time use as a background noise (e.g. TV on). | 20 (100) | 10 (100) | 100% |
| 8. Screen time should only be encouraged after other tasks are completed. a | 15 (75) | 7 (70) | 72.5% |
| 9. Eating is not recommended while using screens unless it is part of a behavioral plan. | 16 (80) | 8 (80) | 80% |
| 10. Screens are not recommended within the child’s room unless professionally recommended as part of a behavioral plan. | 17 (85) | 8 (80) | 82.5% |
| 11. It is not recommended to expose your child to screen time up to 1 h before bedtime. | 20 (100) | 8 (80) | 90% |
| 12. It is not recommended to expose your child to screen time after bedtime. | 20 (100) | 10 (100) | 100% |
| 13. It is not recommended to expose your child to violent content before bedtime. | 20 (100) | 10 (100) | 100% |
| 14. Screen time use should be consistent from day to daya | 16 (80) | 6 (60) | 70% |
| 15. Screen use should be limited to shorter durations during the day (i.e. up to 20 min screen sessions). | 11 (55) | 4 (40) | 47.5% |
| 16. Screen time should be incorporated with healthy, screen-free activities (i.e. physical activity) into the daily routine. | 20 (100) | 10 (100) | 100% |
| 17. Screen activities should be primarily educational, active, or social versus those that are passive or unsocial. a | 16 (80) | 6 (60) | 70% |
| 18. Content should be developmentally appropriate. | 20 (100) | 10 (100) | 100% |
| 19. Most of the screen time should involve apps with high educational properties, with a focus on building skills of children with autism (e.g. communication, empathy, and social skills). a | 7 (35) | 5 (50) | 42.5% |
| 20. Screen time should be used as an opportunity for children/youth with autism to interact with their caregivers and family members (e.g. watching TV with the whole family or playing video games with family members). | 16 (80) | 8 (80) | 80% |
| 21. The content of screen time should be individualized for children/youth with autism, keeping in mind the child’s interest. | 20 (100) | 10 (100) | 100% |
| D. Monitoring screen time | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
| 1. “Know your child’s screen time nutrition”: Any screen time intervention should start with an assessment and mapping of screen time habits: what are the devices being used and at what times, what is the content, what is the use and setting? (Screen time monitor sheet could be used for this purpose). | 19 (95) | 10 (100) | 97.5% |
| 2. Once “screen nutrition” is mapped, when change is needed, caregivers can consider which of the usages could be reduced (When? Which ones? What would be the most feasible for them to start with?). | 20 (100) | 9 (90) | 95% |
| 3. Some professionals consider screen time as dosages. Like medication, it could be useful in a certain dose but cause adverse effects in others. If you use this metaphor to manage screen time, the main questions will be how much, how often? I find this metaphor useful to understand screen time management. | 16 (80) | 10 (100) | 90% |
| 4. Caregivers should manage screen time use by removing screens or limiting access to screen media; “out of sight out of mind”. | 16 (80) | 9 (90) | 85% |
| 5. Screen time management strategies should include being consistent, setting rules, using time use monitoring apps, schedules, and timers. | 20 (100) | 10 (100) | 100% |
| 6. It is recommended that parents use content monitoring software to manage what children/youth with autism are exposed to during screen time. | 18 (90) | 9 (90) | 90% |
| 7. Consider installing an electronic “kill switch“ such as myTorch to enforce screen time management. | 14 (70) | 6 (60) | 65% |
| 8. Use a visual schedule for screen time to help reduce challenging behaviors. | 20 (100) | 9 (90) | 95% |
| 9. Screen time schedules should be implemented with all family members to support screen time use of the child. a | 19 (95) | 7 (70) | 82.5% |
| 10. Engage all family members in communication around screen time schedules. | 19 (95) | 9 (90) | 92.5% |
| 11. With older children, it is recommended to set priorities and discuss the following health behaviors: healthy meals, sleeping times, physical activities, concentrating on one task, reduction of screen time. | 20 (100) | 10 (100) | 100% |
| 12. Parents should be engaged in screen-based media activities alongside their children/ with autism as a way to manage the content they are exposed to. For example, watching the child play and asking questions, looking at cartoons like a picture book, pointing at characters and asking questions. | 18 (90) | 9 (90) | 90% |
| 13. Parents should use screen time as a motivator to manage screen use for children/ with autism | 10 (50) | 6 (60) | 55% |
| 14. When trying to end screen time use, parents should speak with the child, move closer, use voice, touch and use/incorporate other means of communication making the disconnection easier. | 19 (95) | 9 (90) | 92.5% |
| 15. Parents should encourage screen time learning and creation—such as researching scientific questions or creating visuals with graphic design programs. | 20 (100) | 8 (80) | 90% |
| 16. Use different designated devices for entertainment and learning (e.g. not using the same tablet), to keep screen time learning focused. a | 19 (95) | 6 (60) | 77.5% |
| 17. Any behavioral program and strategies should be tailored to the family’s needs and child’s developmental needs and age. | 20 (100) | 10 (100) | 100% |
| 18. Consider using screen time as a reward for functional and active behavior. | 11 (55) | 5 (50) | 52.5% |
| 19. Maintain activities involving nature, connection, and movement to make sure they are not replaced with screen time. | 20 (100) | 10 (100) | 100% |
| 20. Support transitioning from performing some screen-based activities to performing the same activities with pen/paper. a | 15 (75) | 7 (70) | 72.5% |
| 21. Identify non-screen-based activities that your children like and expand on them. | 20 (100) | 10 (100) | 100% |
| 22. Identify non-screen-based activities that can be done with other family members (e.g. dog walking, playing, and gardening) and do them together. | 20 (100) | 10 (100) | 100% |
| 23. Decreasing screen time for children/youth with autism should be done gradually. | 20 (100) | 9 (90) | 95% |
| 24. Decreasing screen time for children/youth with autism should be done cold turkey. | 0 (0) | 0 (0) | 0% |
| 25. Changes in screen time use should be planned ahead, preferably with a clinician who can support the process. | 17 (85) | 8 (80) | 82.5% |
| 26. Changes in screen time, including timing of the change, should be adapted to the child and family’s capacity to implement the changes. | 20 (100) | 10 (100) | 100% |
| 27. All family members should be involved when creating changes in screen time use (adhering to the schedule, being aware of their own screen time use). | 19 (95) | 8 (80) | 87.5% |
| 28. Screen time changes should start with mapping screen time uses and identify areas in which changes will not impact technology benefits (e.g. when the child is using assistive technology). | 20 (100) | 10 (100) | 100% |
| 29. Parents should be educated on how to respond to extreme reactions caused by changes in screen time (with a combination of supportive emotional reaction and clear boundaries). | 20 (100) | 10 (100) | 100% |
| 30. The whole family should monitor their own screen time use when decreasing screen time for children/youth with autism. | 20 (100) | 9 (90) | 95% |
| 31. Structured activities should be used to replace screen time for children/youth with autism. | 19 (95) | 8 (80) | 87.5% |
| 32. Similar activities to those offered on a screen-based tool should be used to allow for smoother transition off screens for children/youth with autism. | 16 (80) | 8 (80) | 80% |
| 33. Screen time changes should be done in a supportive atmosphere and the reasons for the changes and their benefits should be explained and talked about in a positive and encouraging way. | 20 (100) | 9 (90) | 95% |
| 34. Clinicians should provide parents and teachers with education to help support confidence and competence in non-screen activities for children/youth with autism. | 19 (95) | 9 (90) | 92.5% |
| 35. Clinicians should support families with children/youth with autism who use screens in accessing and planning healthy, non-screen-based activities that are accommodated to the child’s and family’s needs. | 19 (95) | 9 (90) | 92.5% |
| 36. Clinicians should minimize screen use during therapy sessions and increase family involvement. | 15 (75) | 9 (90) | 82.5% |
| 37. Screen time use should be a part of the discussion clinicians have with parents and children to minimize screen time risks and enhance technology benefits. | 20 (100) | 10 (100) | 100% |
| E. Guidelines for clinicians: adapting screen time guidelines to family’s needs | Clinicians’ agreement |
Parents’ agreement |
|
| 1. Information regarding screen time use should be personalized and provided to children/youth with autism on a case-by-case basis. | 18 (90) | 9 (90) | 90% |
| 2. A family’s specific needs should be taken into account when considering changes to screen time for children/youth with autism. | 20 (100) | 10 (100) | 100% |
| 3. Screen time routines and strategies for children/youth with autism should be tailored to each individual family’s needs and goals. | 20 (100) | 10 (100) | 100% |
| 4. More support should be given to parents of children/youth with autism who live in smaller spaces and use screens. | 17 (85) | 9 (90) | 87.5% |
| 5. It is recommended for screen time to be “saved” and used to keep children/youth with autism occupied when parents have busy schedules (e.g. having a screen time “bank”). | 12 (60) | 5 (50) | 55% |
| 6. Parents should encourage children/youth with autism to develop autonomy through the independent use of screens. a | 13 (65) | 8 (80) | 72.5% |
| 7. Families with children/youth with autism should be given choices when provided with screen time use recommendations. | 19 (95) | 10 (100) | 97.5% |
| 8. There is a need to work with families to promote an understanding of the benefits and risks of screen time use. | 20 (100) | 9 (90) | 95% |
| 9. Clinicians should provide families of children/youth with autism with evidence-based resources for managing screen time. | 20 (100) | 9 (90) | 95% |
| What would be the best way to provide the guidelines? | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
| 1. These guidelines should be available in a form of flyers. | 18 (90) | 8 (80) | 85% |
| 2. These guidelines should be available on a website. | 19 (95) | 10 (100) | 97.5% |
| 3. These guidelines should be provided in educational videos. | 19 (95) | 9 (90) | 92.5% |
| 4. These guidelines should be provided in workshops. | 17 (85) | 9 (90) | 87.5% |
Items that did not reach agreement between caregivers and clinicians.
Appendix 2
Detailed Survey 2 results.
| Guideline statement | Former item no. | Clinicians’ agreement |
Caregivers’ agreement |
Total agreement level |
|---|---|---|---|---|
| A. Should the above-listed “behaviors to monitor” be included in the guidelines? | NA | 18 (90) | 7 (70) | 83% |
| B. Screen time timing and content | ||||
| 1. Children between ages 2 and 5 years should have a maximum of 1 h/day of leisure/recreational screen time alongside a caregiver (WHO; CSEP; AAP: Council on Communication and Media; CPS). | C3 | 17 (85) | 9 (90) | 87.5% |
| 2. Leisure screen time should be prioritized after other important tasks, such as schoolwork, chores. | C8 | 17 (85) | 7 (70) | 77.5% |
| 3. Screen time use should be reasonably consistent on school days versus less structured days. | C14 | 16 (80) | 10 (100) | 90% |
| 4. Screen use should be used with defined durations that are communicated to the child. The durations could be defined according to a child’s chronological age and developmental level (e.g. watching a TV show for 45 min). | New item | 19 (95) | 10 (100) | 97.5% |
| 5. Screen time should aim to have a balanced representation of screens as both functional and recreational use (tool and toy). | C17 | 18 (90) | 10 (100) | 95% |
| C. Monitoring screen time | ||||
| 1. When considering the use of monitoring software for screen time management, families should take into account the users (children) themselves, allowing them, if possible, to use the software to monitor their own screen time use. | New item | 20 (100) | 9 (90) | 95% |
| 2. Screen time monitoring should involve all parents to support screen time use. | New item | 19 (95) | 8 (80) | 87.5% |
| 3. Screen time use could be reviewed as part of a set of incentives to support positive behaviors. a | New item | 15 (75) | 4 (40) | 57.5% Removed |
| 4. If possible, use different designated devices for entertainment and learning (e.g. not using the same tablet), to keep screen time learning focused. | D16 | 18 (90) | 7 (70) | 80% |
| 5. Wherever possible, a task should be offered using different modalities (e.g. paper-based, screen-based). | D20 | 17 (85) | 9 (90) | 87.5% |
| D. Guidelines for clinicians: adapting screen time guidelines to the family’s needs | ||||
| 1. Parents should encourage children/youth with autism to progressively build their skills so that they aim to be independent when managing their screen time use. | E6 | 19 (95) | 8 (80) | 87.5% |
| E. Should this list of resources be included in the guidelines? | NA | 20 (100) | 8 (80) | 90% |
| F. General principles | ||||
| 1. Digital citizenship is a skill needed for every person in our society today and is not population-specific. | New item | 19 (95) | 10 (100) | 97.5% |
| 2. Technology and screens are part of modern-day society; therefore, it is important to recognize that both opportunities and challenges arise from technology use across all populations. | New item | 20 (100) | 10 (100) | 100% |
| 3. Every family has their own values, meanings, needs, and perceptions of screen time. Therefore, it is important to take into account and respect individual, familial, and cultural perspectives and choices of screen time use. | New item | 19 (95) | 10 (100) | 97.5% |
| 4. Screen time monitoring by parents should be approached respectfully and collaboratively, and with the child’s interests in mind. | New item | 20 (100) | 9 (90) | 95% |
| 5. Whenever possible and appropriate, it is important to ensure the child has agency and ownership over screen time decisions. | New item | 18 (90) | 9 (90) | 90% |
| 6. Screen time use has a developmental and dynamic nature and the opportunities and challenges change over the course of the child’s life. Therefore, a balance between structure and flexibility is needed when incorporating screen time use into daily life, taking into consideration changes in a child’s age, needs, development, personal interests, and familial considerations. | New item | 20 (100) | 10 (100) | 100% |
Items that did not reach agreement between caregivers and clinicians.
Appendix 3
Acknowledgements
The authors thank the Michael Smith Health Research Foundation for supporting this study. They thank Aliza Weiss for her help. They also thank the parents, clinicians, researchers, and stakeholders who contributed to the development of the guidelines, some are listed here and others chose to stay anonymous: Alexandra Samuel, Bruce Pipher, Camille Bailey, Cris Rowan, Ivonne Montgomery, Katie Allen, Kenneth D. Cole, Lucy Ruthven, Marilyn Noort, Melanie Penner, Mohammad Zubairi, Molly Flindall-Hanna, Rashmeen Nirmal, Sara Dick, Tammy Innes, Vikram Dua; their roles and credentials are listed in this webpage: ![]()
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding for the research from the Michael Smith Health Research BC C2 Program and from the University of Haifa for the open-access publication.