
Abstract
The aim of this study was to evaluate the efficacy of the youth version of the program Parents Taking Action in Bogota, Colombia, using a quasi-experimental design. We hypothesized that parents in the treatment groups would improve in levels of knowledge, empowerment, self-efficacy, and use of strategies related to topics of adolescence and sexuality compared to the control group. We recruited 25 Colombian parents of pre/adolescent youth with autism spectrum disorder between the ages of 10 and 17 in Bogota. The intervention included four weekly sessions in which the new content about sexuality and adolescence was delivered. Twelve parents were in the intervention group and 13 were in the control group. Intervention participants significantly improved in Knowledge (t = 4.37 p < 0.001), Self-Efficacy (t = 7.15, p < 0.001), Use of Strategies (t = 4.29, p < 0.001), and Family Empowerment (t = 3.82, p < 0.005) between baseline and follow-up. The control group did not improve on any of the outcome measures, and the mean differences between baseline and follow-up scores were significant between intervention and control groups. The program has potential for high impact as information is scarce and parents do not have resources related to pre/adolescence. The program shows promise as an efficacious tool for community organizations and health providers to support families.
Lay abstract
We evaluated the efficacy of the youth version of the program Parents Taking Action in Bogota, Colombia. This program aims to provide information, resources, and strategies about topics of puberty, sexuality, and adolescence for parents of preadolescents with autism spectrum disorder. We examined whether parents in the treatment groups would improve in levels of knowledge, empowerment, self-efficacy, and use of strategies compared to the control group. We recruited two groups of Colombian parents of pre/adolescent with autism spectrum disorder between the ages of 10 and 17 in the city of Bogota, Colombia, through a community-based organization. One of the groups received the intervention and the other served as a control group. Parents in the control group received the intervention after the 4-month follow-up. The intervention included four 3-h weekly sessions in which the curriculum with nine topic areas was delivered providing parents with a space to practice strategies, learn from others, and set goals. Parents in the intervention group reported significantly greater knowledge, self-efficacy, use of strategies, and empowerment compared to the control/waitlist group. Parents were also highly satisfied with the content, materials, and peer connections that the program offered. The program has potential for high impact as information is scarce and parents do not have resources related to the complicated developmental stages of pre/adolescence. The program shows promise as an efficacious tool for community organizations and health providers to provide extra support to families of youth with autism spectrum disorder.
Keywords
Background
The prevalence of autism spectrum disorder (ASD) has increased in recent decades around the world. In the United States, 1 in 44 children is diagnosed with ASD (Centers for Disease Control and Prevention, 2022), while the World Health Organization (2022) estimates that worldwide 1 every 100 children has ASD. In Colombia, there are no statistics about ASD, and the lack of research and information about supports for children and youth with ASD and their families in Colombia limits the services and supports available for this population. In addition, disability in Colombia is still considered a taboo, and it has a strong stigma that prevents people with disabilities from fully participating in the community (Hernandez Buitrago & Miranda Molano, 2019).
Worldwide, there is a particular need for services that focus on youth and topics such as puberty, sexuality, and adolescence development (André et al., 2020; Matson et al., 2009). Sexuality includes a variety of aspects such as body changes, hygiene, self-image, interaction with others, consent, sexual orientation, and relationships among many other. However, for people with ASD, there are some difficulties when approaching them such as lack of social skills in relationships, public masturbation, process of emotions, establishment of personal boundaries isolation, risk of abuse, and understanding the complexities of sexuality (Nichols & Blakeley-Smith, 2009; Parchomiuk, 2019). Evidence shows that parents and professionals present negative attitudes toward sexuality as well as a lack of knowledge of how to address the topic using useful strategies. For example, Latino caregivers might conceptualize sexuality only as physical changes in the body, and the available programs are more about accepting the topics instead of addressing them with specific strategies (Campos Guzmán et al., 2022). Other studies in Latin countries explore the perception of parents and professionals about sexuality, and they showed that conservative attitudes toward the topic and stereotypes become an obstacle to guide adolescents with ASD through this stage (Manzone et al., 2022). However, there is limited evidence about specific training programs for Latino parents that address sexuality and ASD using specific strategies. Most research focus on perceptions, and how sexuality happens in people with ASD. In fact, most evidence suggests the need to develop this type of educational programs. To the best of our knowledge, there is no evidence in the literature of these programs in Colombia or other Latino countries.
Building on a parent educational intervention implemented in Colombia with parents of young children, Parents Taking Action (PTA) (Magaña et al., 2021), we developed content that incorporated new topics and provided information, resources, and supports for Colombian parents of youth (including preadolescents and adolescents). We retained some of the original content from PTA and added new content. This new content was informed by available research on topics such as sexuality, parents’ perceptions about sex and transition in adolescents with ASD, and sexual education (Mackin et al., 2016; Nichols & Blakeley-Smith, 2009). The original PTA program implemented in Colombia was delivered by student and parent mentors. For the current study, it was delivered by a graduate student and not by parents. The aim of this study was to evaluate the efficacy of the adapted youth version of PTA in Bogota, Colombia, using a treatment and control group. Our primary research question was as follows: (1) Did parents in the treatment group improve between pre- and post-test in levels of knowledge, empowerment, self-efficacy, and use of strategies compared to the control groups? We hypothesized that parents in the treatment group would significantly improve in these outcomes and the control group would not. (2) Were the differences between pre- and post-tests within each group significant across groups? We hypothesized that the differences found in research question 1 would be significant across the two groups, demonstrating the efficacy of the intervention. (3) Were parents satisfied with the content, materials, and peer connections provided by the program?
Method
Participants
We recruited 25 Colombian parents of preadolescent and adolescent youth with ASD in the city of Bogota, Colombia, through a community-based organization. The intervention group had 12 participants while the control/wait list group included 13 participants. The inclusion criteria were Colombian parents/caregivers of children between 10 and 16 years old with a confirmed diagnosis of ASD. As shown in Table 1, most participants were female, had low incomes, and were unemployed. Their children’s average age was 13 (ranging from 10 to 17) years, most of them were male, verbal, and had a diagnosis of ASD. All parents finished the intervention.
Sample demographics by group.
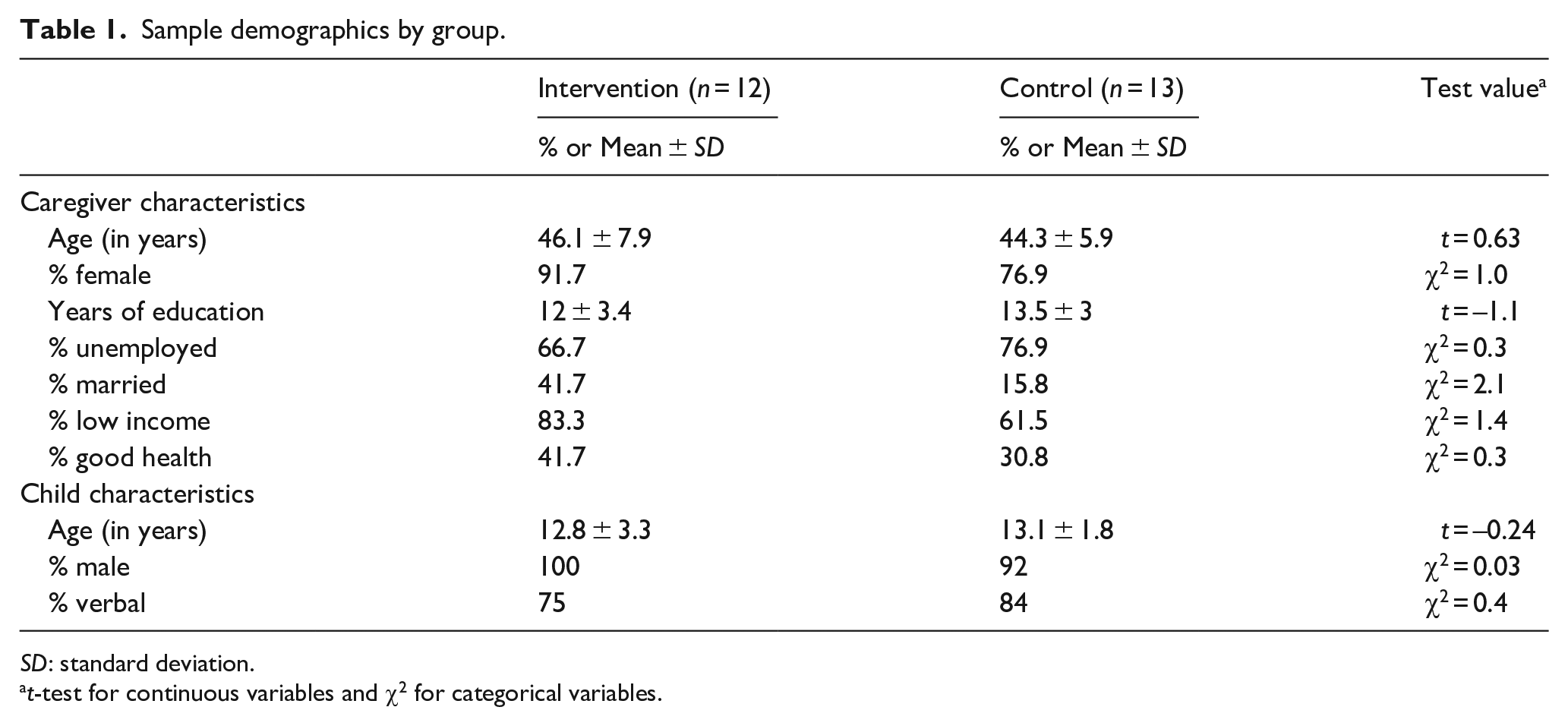
SD: standard deviation.
t-test for continuous variables and χ2 for categorical variables.
Intervention protocol and curriculum
The intervention curriculum was delivered through four weekly 3-h group sessions and included nine modules with information, resources, strategies, and supports about the stage of adolescence, in-session activities, and discussions. The topics include puberty, body changes, and public–private spaces (modules 2–3); emotions, strangers, and mental health (modules 4–6); and relationships, Internet, and steps for the future (modules 7–9). Content of the first module was an adaptation from the original PTA (Magaña et al., 2017) and included an overview of the diagnosis of ASD, evidence-based strategies associated with ASD, and identifying needs of each family. In each session, parents had the opportunity to practice some of the evidence-based strategies recommended, including ABA strategies (token economy, positive reinforcement, modeling, etc.), creating social narratives, and role-playing. Parents in the control group received the intervention after the intervention group. To learn more about the adaptation of the intervention, see Magaña et al. (2021). The first author who is a psychologist delivered the intervention entirely in Spanish.
Study design
We used a quasi-experimental design that included an intervention and control/waiting-list group with evaluations at baseline and follow-up (post intervention or 4 weeks after baseline). The first group was offered the intervention immediately after baseline, and the second group was offered the intervention after the follow-up evaluation of the first group was completed.
Instruments
Knowledge questionnaire
This instrument was developed by the lead author and contains 20 items on the topics covered in the curriculum, and it aimed to evaluate the level of new content that parents acquire in relation to sexuality, autism, strategies related to adolescence, and so on. The Cronbach’s alpha was 0.9 (pre), 0.842 (post), which indicates a high level of internal consistency in both the pre and post assessments.
Self-efficacy questionnaire
This instrument was adapted from the original version of the PTA (Magaña et al., 2021) and includes an 11-item Likert-type scale. This questionnaire measures the level of competency of parents in applying the knowledge and strategies learned during the program. Responses were added for a total self-efficacy score. Cronbach’s alpha was 0.86 (pre) and 0.781 (post) indicating high internal consistency.
Utilization of strategies
This instrument is a 14-item Likert-type scale ranging from never (1) to always (4) that measures the frequency in the use of the strategies. This was also adapted from the original version of PTA (Magaña, 2021). Responses were summed for a total use of strategies score. Cronbach’s alpha was 0.75 (pre) and 0.83 (post), indicating a high level of internal consistency in both pre- and post-tests.
Family empowerment scale
The Family empowerment scale (FES) instrument measures attitudes, behaviors, and knowledge at the family level (Koren et al., 1992). For this study, this instrument includes only the family subscale, which contains a 12-item Likert-type scale, and measures empowerment at the family level and parent empowerment. Responses were summed for a total empowerment score. This instrument has a high level of internal consistency with a Cronbach’s alpha of 0.88 (pre) and 0.85 (post).
Overall satisfaction
This questionnaire included 10 questions in a Likert-type scale. This questionnaire was created by the author, and it targeted satisfaction with the content, material and resources, and peer connection.
Analysis
For the data analysis, we used a paired-sample t-test to compare the pre–post data within each group, and an independent t-test of within-group mean differences between baseline and follow-up to determine the efficacy of the intervention group compared to the control. We also used Cohen’s d to report effect sizes of each outcome.
Finally, we also measured level of satisfaction with the intervention at the end of the four sessions.
Community involvement
An autistic self-advocate, community organizations, and family members of autistic youth were involved in helping to ensure the content was culturally appropriate and useful for the community before implementation. One community organization in Colombia helped to recruit family members and hosted the program.
Results
First, we examined whether the two groups differed in demographic variables at baseline. Table 1 shows that both groups were similar with respect to socio-economic status (level of education and income), gender, health care status, and child characteristics. There were no significant differences between the two groups in any of the demographic variables.
Pre-test, post-test differences for intervention and control group
Table 2 shows the means, standard deviation, and t scores for the outcomes of knowledge, self-efficacy, use of strategies, and empowerment for both intervention and control group. In addition, for the intervention group, effect size is also reported using Cohen’s d. In these results, we found that all the outcomes increased significantly for the intervention group compared to the control group. The significance level of all outcomes and the large effect size suggests that after receiving the intervention, parents increased their knowledge about topics, resources, and supports of the stage of adolescences and sexuality, the frequency of the use of the strategies to support their children in these areas, and a higher sense of self-efficacy and empowerment. The control group did not improve on any of the outcome measures as shown in Table 2.
Comparison of pre-test and post-test for the intervention groups and the two pre-tests for the control group using paired t-test.
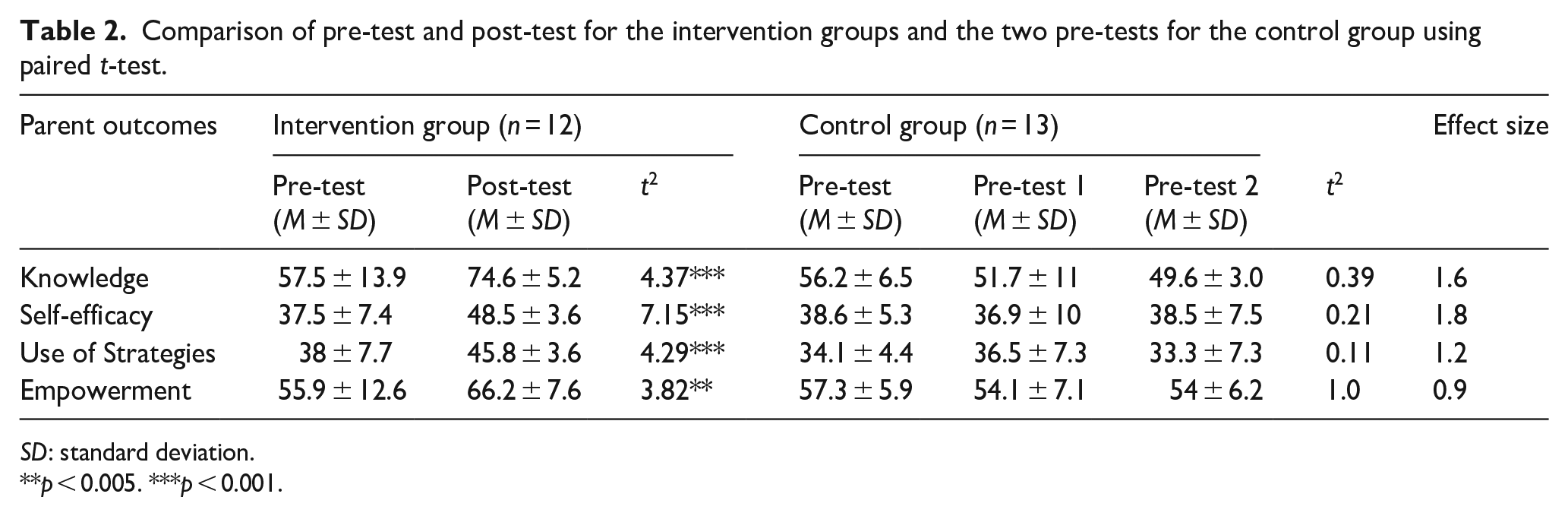
SD: standard deviation.
p < 0.005. ***p < 0.001.
Efficacy of the youth version of PTA
To examine efficacy, we conducted an independent t-test to compare the mean difference between baseline and follow-up for both intervention and control groups for all four outcomes. The results indicate that parents who received the intervention reported a higher score (M = 17.08, SD = 13.5) in knowledge when compared to the control group (M = –2.16, SD = 8.4); t(25) = 4.17, p < 0.001. Self-efficacy for the intervention group (M = 11.08, SD = 5.36) also increased compared to the control group (M = 1.58, SD = 2.16); t(25) = 4.86, p < 0.001. Parents who received the intervention reported an increase in the use of strategies (M = 7.75, SD = 6.2) when compared to the control group (M = 6.51, SD = 4.22); t(25) 4.22, p < 0.001. Finally, parents felt more empowerment after receiving the intervention (M = 10.03, SD = 9.3) than parents who did not receive the intervention (M = 0, SD = 5.13); t(25) = 3.35; p < 0.005.
Overall satisfaction
Results showed that parents were highly satisfied with the material and resources (M = 4.0), content of the program (M = 3.99), and peer connections (M = 3.95). In addition, we report a high retention rate as all 12 intervention participants attended all four sessions.
Discussion
In this study, we evaluated the efficacy of the youth version of PTA for Colombian parents of preadolescent and adolescent youth with ASD using a quasi-experimental design. Large effect sizes for all the outcomes suggest that parents of youth with ASD in the intervention group increased their knowledge, use of strategies, self-efficacy, and empowerment with respect to the topics related to puberty, adolescence, and sexuality compared to the control group.
In terms of the curriculum, parents were highly satisfied with the program. They reported that program content, materials, and peer connection were appropriate and that it was what they needed to support their children. Since previous research suggested the need for these programs for Latino caregivers (Campos Guzmán et al., 2022), these results add to the literature on training program with specific strategies for caregivers of youth with ASD. In addition, this is the first time this type of curriculum was created for a Colombian population. Results also suggest that parents were able to apply the skills at home and felt more comfortable leading difficult conversations. Results in regard to their sense of self-efficacy and empowerment indicate that parents felt equipped to apply what they learned and find the balance between family demands and adjustment to a new routine after the program.
These findings are also consistent with those of similar studies which demonstrated this type of parent education as an appropriate resource for parents of preadolescents (André et al., 2020; Ballan & Freyer, 2017; Mackin et al., 2016; Nichols & Blakeley-Smith, 2009).
Results not only suggest that the program has efficacy, but it is also appropriate for the culture and the needs of Colombian parents as indicated by the high satisfaction and retention rates. These findings add to previous research that attempted to develop educational programs for parents in different contexts and cultures (Klein et al., 2005). Adolescence and sexual development are topics that happen across cultures and countries, but it is important to address these differences, so families become knowledgeable about how to provide support to their children.
A limitation of the study was the sample size (n = 25), which can limit the detection of more significant findings. However, despite the small sample, we were able to determine significant findings across all outcomes. The fact that this was limited to Colombians in a large city does not allow us to generalize the findings across all Colombian settings. Also, participants were not randomly assigned to the two groups, which limits the attribution of causality to the intervention. Finally, data were self-reported, and this can add some potential biases to some of the responses. For example, there was not an objective measure for the use of strategies, and it was solely based on parent’s report.
Overall, the PTA program has potential for high impact as information is scarce, and parents do not have resources related to the complicated developmental stages of pre/adolescence. Future research can explore a train the trainer model for community organizations and health providers to deliver this program as extra support for families of youth with ASD.
Footnotes
Acknowledgements
The authors thank Fundación Avante and Liga Colombiana de Autismo in Bogota, Colombia, for their support during the implementation of the program. They also thank the autistic self-advocate and family members who support them reviewing the content of the program before its implementation.
Ethical approval
All participants of this study signed an informed consent as this study was approved by the University of Illinois at Chicago IRB.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.