
Abstract
An earlier diagnosis of autism spectrum disorder might lead to an earlier intervention, yet knowledge and awareness of autism spectrum disorder in Latin America and Caribbean Countries are limited. A later autism spectrum disorder diagnosis has been associated with negative consequences, as it might imply later access to services. This study aims to identify factors associated with the age of autism spectrum disorder diagnosis as reported by 2520 caregivers of autistic children from six Latin America and Caribbean Countries. Results indicate that on average, caregivers were concerned about their child’s development by 22 months of age; however, the diagnosis was 24 months later. Current age of autistic individuals, better language abilities, and having public health coverage increased the age of diagnosis. On the contrary, the presence of medical comorbidities, severity level, and type of diagnosis decreased the age of diagnosis. The age of diagnosis of autistic individuals in Latin America and Caribbean Countries corresponded to the start of formal schooling despite a much earlier age of first noticed developmental concern, highlighting the need to reduce this age gap and increase children’s probability of benefiting from early intervention. Taken together, autism spectrum disorder personal/clinical characteristics and access to health service are the main determinants for the age of diagnosis.
Lay abstract
An earlier diagnosis of autism spectrum disorder might lead to earlier intervention. However, people living in Latin American and Caribbean countries do not have much knowledge about autism spectrum disorder symptoms. It has been suggested that the older a child is when diagnosed, the fewer opportunities he or she will have to receive services. We asked 2520 caregivers of autistic children in six different Latin America and Caribbean Countries, the child’s age when they noticed some developmental delays and their child’s age when they received their first autism spectrum disorder diagnosis. Results indicate that, on average, caregivers were concerned about their child’s development by 22 months of age; however, the diagnosis was received when the child was 46 months of age. In addition, older children with better language abilities and public health coverage (opposed to private health coverage) were diagnosed later. On the contrary, children with other medical problems and more severe behaviors received an earlier diagnosis. In our study, children were diagnosed around the time they entered formal schooling, delaying the access to early intervention programs. In summary, the characteristics of the autistic person and the type of health coverage influence the age of diagnosis in children living in Latin America and Caribbean Countries.
Keywords
An earlier diagnosis of autism spectrum disorder (ASD) might lead to earlier intervention. Availability and effectiveness of early intervention are considered channels for autistic children to exert their human rights to inclusion, education, and play (Divan et al., 2021; Hahler & Elsabbagh, 2015). A later ASD diagnosis has been associated with negative consequences as it might imply later access to services (Fein et al., 2017; Klin et al., 2015). A growing body of research supports that early intervention programs can improve communication and adaptive behaviors in autistic children while facilitating social interaction (Dawson et al., 2022). Furthermore, treatment quality can be impacted since a diagnosis delay and a long gap between first parental concerns and age of diagnosis may be associated with a decreased utilization of evidence-based treatments (Zuckerman et al., 2017).
ASD diagnosis relies on observations of behaviors. Generally, the first signs of ASD usually emerge in the first year of life; however, the diagnosis comes at a much older age (Guthrie et al., 2013; Tanner & Dounavi, 2021). Despite a lack of consensus, a series of systematic reviews and meta-analyses reported an average age of diagnosis ranging from 38 to 120 months (Daniels & Mandell, 2014; Loubersac et al., 2021; van’t Hof et al., 2021). Unfortunately, in Latin America and Caribbean Countries (LACC), ASD knowledge and awareness are limited (Elsabbagh et al., 2012; Paula et al., 2020), and the infrastructure for its identification and diagnosis is underdeveloped (Chiarotti & Venerosi, 2020). Since most autism research has taken place in high-income countries (Divan et al., 2021; Durkin et al., 2015; Elsabbagh et al., 2012), data on the age of diagnosis in regions outside the United States and Europe is scarce, representing a knowledge gap regarding factors influencing the age of ASD diagnosis among diverse populations.
Few studies have targeted ASD diagnosis across cultures. A study conducted in Venezuela found that parents were aware of developmental difficulties before the second year of life; however, their children were diagnosed 36 months later (Montiel-Nava et al., 2017). For this sample, the presence of non-ASD behaviors and cognitive impairment was related to a later age of diagnosis. In Brazil, mothers had their first concerns regarding ASD when children were 24 months old, but formal diagnosis occurred with a 3-year delay, with a mean age of diagnosis of 60 months. Moreover, participants reported negative experiences with health professionals during the diagnostic process (Ribeiro et al., 2017). In 2016, the Red Espectro Autista Latinoamerica (REAL) launched a multisite study to identify the main needs and challenges of autistic individuals living in LACC. Results from the survey found that across LACC included in the study, the main barriers were waiting lists, cost of services, and lack of specialized services (Paula et al., 2020). In said sample, the average age of diagnosis was 46.3 months, with preschool-aged children being diagnosed at an earlier age (32.8 months) than school-aged children (50.9 months) and school-aged children being diagnosed earlier than adolescents (73.1 months). However, previous analysis did not include any demographic or clinical predictors of age of diagnosis.
Socioeconomic factors such as parental education and race have been identified to impact age of ASD diagnosis (Brett et al., 2016; Fountain et al., 2011; Mandell et al., 2009; Rosenberg et al., 2011). Furthermore, male-sex, language and communication deficits, symptom severity, comorbid disorders, as well as the level of support needed by the child have also been associated with an earlier ASD diagnosis, with lower levels of impairment and severity yielding a delay in diagnosis (Baghdadli et al., 2003; Brett et al., 2016; Daniels & Mandell, 2014; Fernell et al., 2013; Mandell et al., 2005; Perryman et al., 2018; Rosenberg et al., 2011; Shattuck et al., 2009). The reported age of diagnosis in studies conducted in LACC fall within the reported range in other parts of the world. However, a lack of resources in some geographical areas, shortage of trained professionals, parents’ educational level, lack of autism cultural beliefs, and healthcare coverage, among others, might impact the rates of identification and diagnosis of low-resourced communities (Divan et al., 2021; Hahler & Elsabbagh, 2015; Zakirova-Engstrand et al., 2020).
In addition, a significant health determinant is socioeconomic status (SES; Fiscella et al., 2000) which has also been found to influence the age of diagnosis (Daniels & Mandell, 2014). Individuals with low SES are less likely to access primary-care services (DeVoe et al., 2008), which is especially problematic for the early detection of ASD. Interestingly, a study found that SES was a stronger predictor of age of diagnosis than symptom severity (Fountain et al., 2011). Likewise, access to health coverage is another vital healthcare use determinant (Emerson et al., 2016), with uninsured children being more likely to have unmet treatment and preventive care needs (Cummings et al., 2009). Nevertheless, some studies have found that access to health coverage does not necessarily translate to service utilization (Starfield & Shi, 2004) because the type of healthcare systems and the amount of financial and human resources available are also an important element in service accessibility (Paula et al., 2014; Sayal, 2006).
This study will present data from six countries: Argentina, Brazil, Chile, the Dominican Republic, Uruguay, and Venezuela. Although all six countries are considered upper-middle or high-income countries (The World Bank, 2022), their citizens experience health disparities, low mental-health expenditure, shortage of health professionals, and weak legal frameworks to protect autistic individuals (World Health Organization [WHO], 2018).
In addition to difficulties with ASD detection and diagnosis in LACC, treatment and access to services are also difficult to obtain (Kohn et al., 2018). The region counts with a treatment gap (difference between people needing care and those receiving it) for mental health disorders in children ranging from 64% to 86% (Kohn et al., 2018). A study by Montiel-Nava et al. (2020) reported that 19% of caregivers indicated their autistic children did not receive any services during their lifespan and that the use of services decreased with age (Montiel-Nava et al., 2020). The treatment gap can also be observed in health resource deficits; for instance, LACC has only 8.7 mental health practitioners for every 100,000 individuals (Kohn et al., 2018; WHO, 2018). Specialists are also scarce, which is why primary-care providers (PCPs) are the leading healthcare practioners whom families of autistic individuals encounter. Unfortunately, these providers are generally not adequately equipped to detect and assist families of children with mental health conditions such as ASD (Brookman-Frazee et al., 2012; Carbone, 2013; Espinola-Nadurille et al., 2010; Paula et al., 2020). In addition to the limited ASD-specific training, there is also limited collaboration among PCPs and specialists (Bordini et al., 2015; Durkin et al., 2015; Kohn et al., 2018; Montiel-Nava et al., 2017; Paula et al., 2012; Silva et al., 2018). This is problematic, given that when properly trained, PCPs are six times more likely to refer suspected ASD cases to the needed specialized treatment (Bordini et al., 2015). These barriers are even more taxing in hard-to-reach populations, such as those living in small towns and rural communities (Araripe et al., 2022; Kohn et al., 2018).
The early identification of ASD has been linked to a better outcome among autistic individuals (Dawson et al., 2010, 2012, 2022; Klin et al., 2015; Warren et al., 2011; Zwaigenbaum et al., 2013). Delays in diagnosis might pose a barrier to timely access to treatment. Divan et al. (2021) consider that only a small number of autistic children in low- and medium-income countries (LMICs) are identified due to certain barriers. Therefore, results about age of diagnosis in low-resource contexts in different countries need to be considered as underestimations of the age of diagnosis in the general population, considering that most families might have fewer resources and less access to diagnostic services. Thus, a better understanding of the demographic and clinical factors involved in the age of diagnosis in LMIC will provide a multidimensional framework to aid professionals and policymakers in developing culturally appropriate diagnostic initiatives to overcome barriers to accessing services. For this reason, the purpose of this study was to identify factors associated with the age of ASD diagnosis in LACC utilizing Andersen’s Behavioral Model framework (Andersen, 1995). The model proposes the existence of individual characteristics that affect access to services (predisposing factors), structural factors that enable or impede an individual’s use of service (enabling factors), and the need of individuals to utilize care (need factors). Those three factors work together to predict healthcare usage, such as diagnostic access or intervention enrollment. In specific, we explored how certain predisposing factors (i.e. gender, age of the autistic individual, and highest educational level of caregivers), enabling factors (i.e. country of residence, health coverage type, professional involved, and traveled distance to receive a diagnosis), and need factors (i.e. type of diagnosis, severity level, medical comorbidity, type of caregiver’s first concerns observed, and verbal ability of autistic individual) predicted age of diagnosis.
Method
Data and sample
This study focuses on the experience of 2520 caregivers from six LACC (Argentina, Brazil, Chile, Dominican Republic, Uruguay, and Venezuela) from the time they observed first developmental concern and the actual age of an ASD diagnosis. A total of 2965 caregivers of autistic individuals aged 2–17 years completed the online survey. Eleven cases (n = 11) were recorded by the system as a completed entry, but they only had information about the country where it was completed. A group of 108 participants reported a diagnosis under the “other” category (non-ASD diagnosis), while 29 left the diagnosis question blank. Caregivers of individuals older than 18 years were excluded from the analysis (n = 297), given the wide range of ages within this age group (18–63 years of age). The total number of excluded cases (n = 445) constituted 15% of the initial sample (Figure 1). Inclusion criteria consisted of (1) being the parent/caregiver 1 of an autistic individual, (2) a resident of one of the participating countries, and (3) being at least 18 years of age. No other exclusion criteria were established. Data were collected from December 2015 to April 2016.
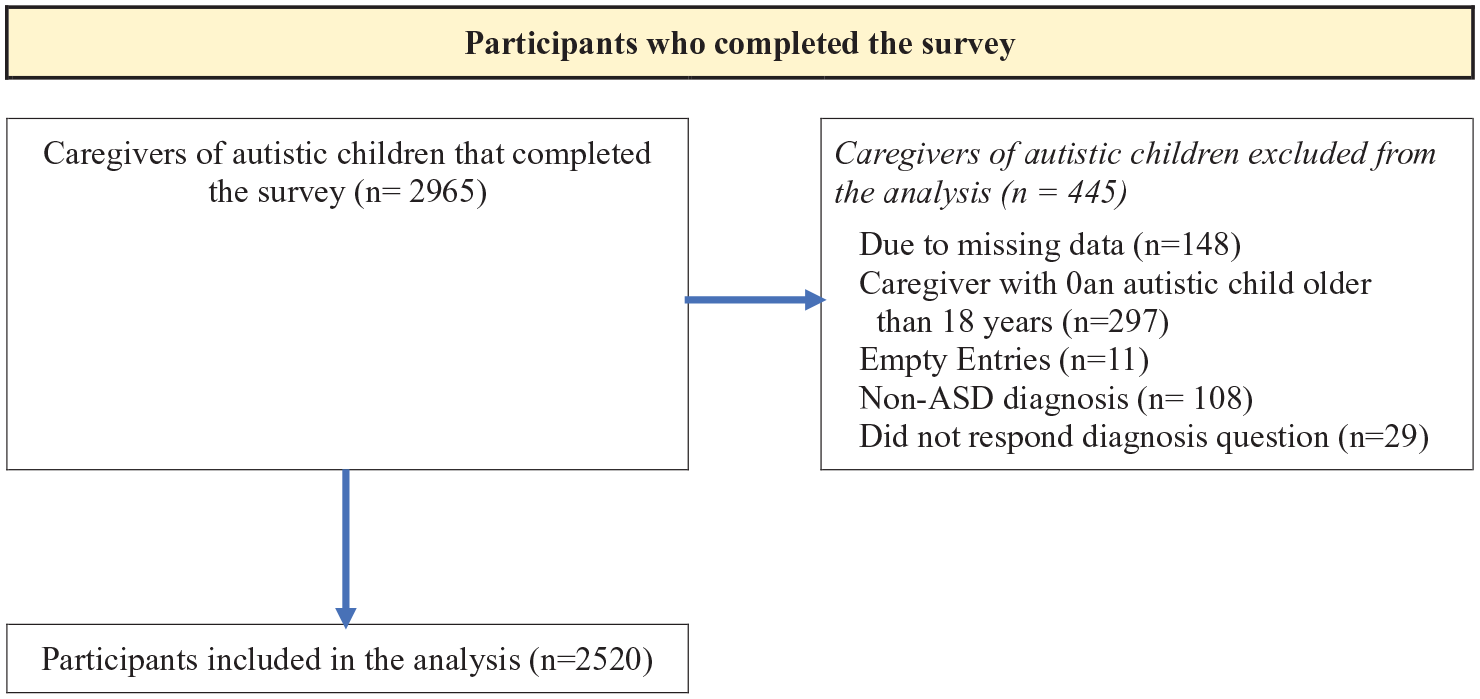
Sample diagram.
Instrument
Caregivers responded to the Caregivers Needs Survey (Daniels et al., 2017) adapted from English to Spanish and Portuguese. The adaptation process involved translating the survey from English (original language) to Spanish and Portuguese and then back-translating it to English by an external translator. After the translation and back-translation process, a regional modification took place to adjust the content and language to each country’s reality and customs. For example, educational modalities and levels, types of health coverage, and informed consent wording varied across countries. In the end, most changes were language adjustments to the local Spanish. Once each country had a final version, the survey was uploaded into a server, and piloted with 10 families per country to obtain feedback about length, language used, lay readability, and website accessibility. No further modifications were required at this stage.
The survey took approximately 30 minutes to complete and contained four sections: family demographics, individual characteristics, service encounters, and parent/caregiver perceptions. The sociodemographic section included sex of ASD individual, health coverage (private, public, or both), and country. Clinical variables included diagnosis of the affected individual (autism/autistic disorder, Asperger’s disorder, PDD, PDD-NOS, ASD, among others) and the presence of medical comorbidities at the time of the study. The survey contained diagnosis options based on the Diagnostic and Statistical Manual of Mental Disorders: Fourth edition (DSM-IV-TR; American Psychiatric Association [APA], 2000) and the DSM-5 (APA, 2013), and the caregiver could only select one diagnosis. The survey used different questions to inquire about the child’s language and symptom severity. Complete information on the development and properties of the survey is given in the works of Torres et al. (2021), Paula et al. (2020), and Montiel-Nava et al. (2020).
Procedure
Recruitment information was advertised via social media, parent associations, and non-profit agencies. To complete the survey, caregivers accessed the website by clicking on a link provided in the recruitment materials. Once they entered the project’s website, they needed to select their country of residence to obtain the informed consent form for that country, which included information of that particular country’s study coordinator. After caregivers provided their initials as signature, a random computer-generated identification (ID) number was provided. This ID allowed caregivers to complete the survey at a different time without losing entered data. No personal information (e.g. name, phone number, or email address) was collected, giving participants anonymity. In addition, there was no monetary compensation for completing the survey. Ethics approval was granted by the ethics board of the different agencies to which the national coordinators were affiliated.
Data analysis
We computed descriptive statistical and multiple regression analyses to identify age of first concerns observed by caregivers and age ASD diagnosis. Both age of first concerns and age of diagnosis were continuous variables, as caregivers entered the requested age in a field box (open-ended question). We then explored the direct relationship between enabling, predisposing, and need factors (explanatory variables) and age of diagnosis in months (continuous and dependent variable). The significance of analysis was at 0.05 to reduce type I error. See Table 1 for a description of the different variables, questions used to retrieve caregivers’ responses, type of variables, and answer options.
Variables.
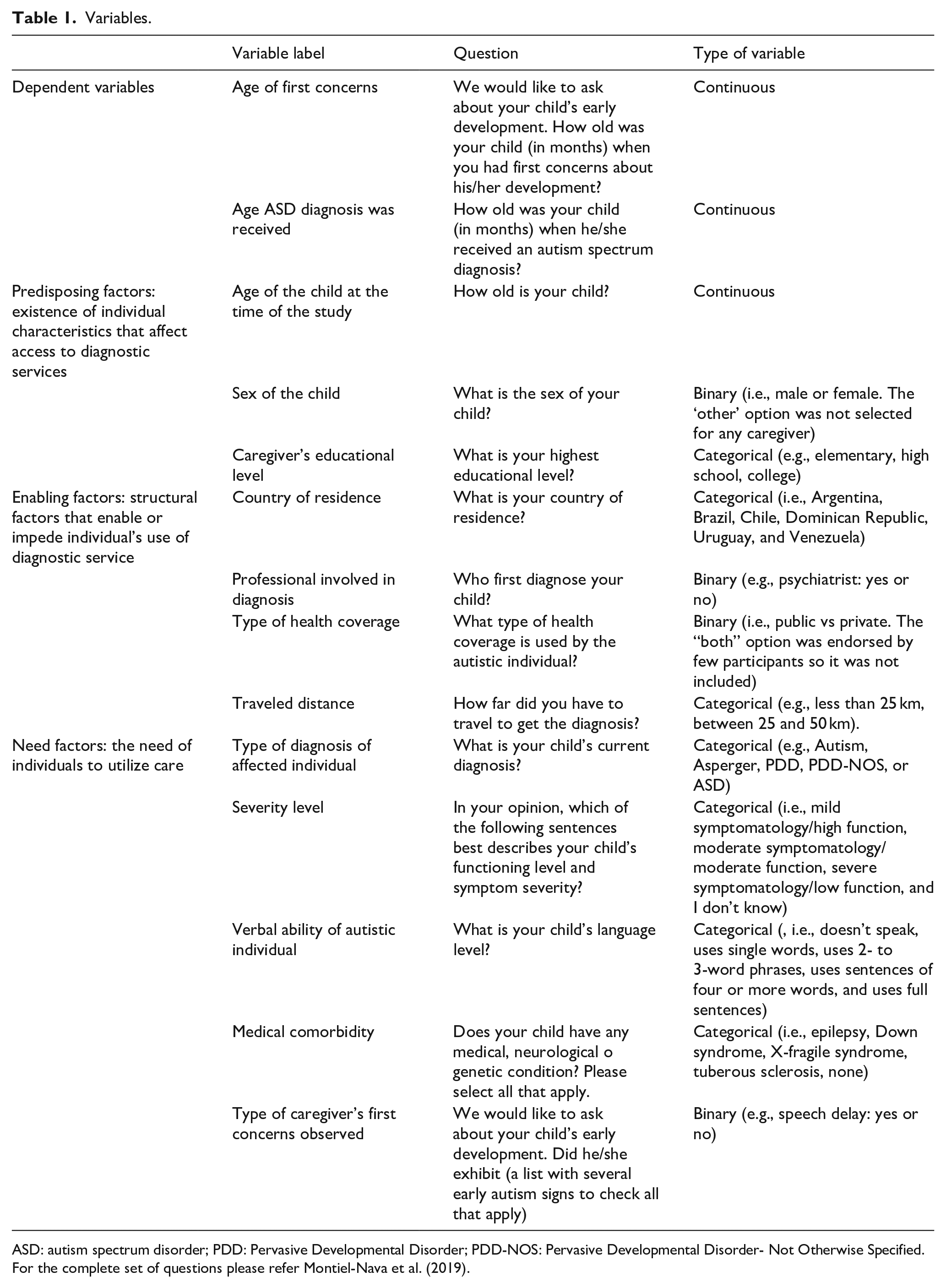
ASD: autism spectrum disorder; PDD: Pervasive Developmental Disorder; PDD-NOS: Pervasive Developmental Disorder- Not Otherwise Specified.
For the complete set of questions please refer Montiel-Nava et al. (2019).
Explanatory variables
Predisposing factors
Variables included in this domain consisted of gender, age of autistic individual when the survey was completed and highest level of education of caregivers. The age of the child consisted of a continuous variable, while sex of the child was considered binary. The original item included the option for “female,” “male,” and “other,” yet no caregiver indicated “other.” The analysis was thus conducted considering sex a dichotomous variable. Level of education consisted of a categorical variable with a range of options from primary schooling to no schooling completed.
Enabling factors
Country of residence was categorical, while type of health coverage and professional involved in diagnosis were treated as binary variables (e.g. private vs public, psychiatrist: yes or no). Traveled distance was treated as a categorical variable (e.g. less than 25 km, between 25 and 50 km).
Need factors
This domain included type of diagnosis (categorical variable; e.g. Autism, Asperger, PDD, PDD-NOS, or ASD) of the affected individual, severity level (categorical, e.g. mild symptomatology/high function, moderate symptomatology/moderate function, severe symptomatology/low function, and I don’t know), medical comorbidity (categorical, e.g. epilepsy, Down syndrome, X-fragile syndrome, tuberous sclerosis, none, and other), type of caregiver’s first concerns observed (binary; yes or no, see Table 3), and verbal ability of autistic individual (categorical; e.g. doesn’t speak, uses single words, uses 2- or 3-word phrases, uses sentences of four or more words, and uses full sentences). The severity level and verbal ability of autistic individuals allowed caregivers to respond about symptom severity with the added insight into language capacity.
Community Involvement: As mentioned before, the survey was translated from English to Spanish and Portuguese. After the final versions were established, each country team ran a pilot, with 10 caregivers of autistic individuals per country. This pilot aimed to explore caregivers’ impressions of the instrument in terms of length, the language used, appropriateness and lay readability, and the website’s accessibility before its wide implementation. Caregivers also advised the best ways to advertise the research study among the general community.
Results
Age of diagnosis and demographic characteristics
Despite participants from all countries being included in the different analyses, most caregivers were Brazilian (39.7%) and Argentinian (28.1%), mothers (88.5%) of a male child (84.2%) with an ASD or autism diagnosis (63.3%), moderate symptom severity (43.2%), speaking in sentences (38.1%), and had a neurologist involved in first diagnosis (42.8%). For the most part, caregivers had an undergraduate or graduate degree (55.8%) and private health coverage (74.2%) and reported traveling less than 50 kms to obtain a diagnosis (68.9%). The mean age of diagnosis in our sample was 46.3 months (SD = 29.9), whereas mean age of first concern was 22.4 months (SD = 15.6), exhibiting a difference of 23.9 months between the two (Table 2). At the time of the study, the mean age of the child was 7.2 years (SD = 3.60).
Demographic characteristics.
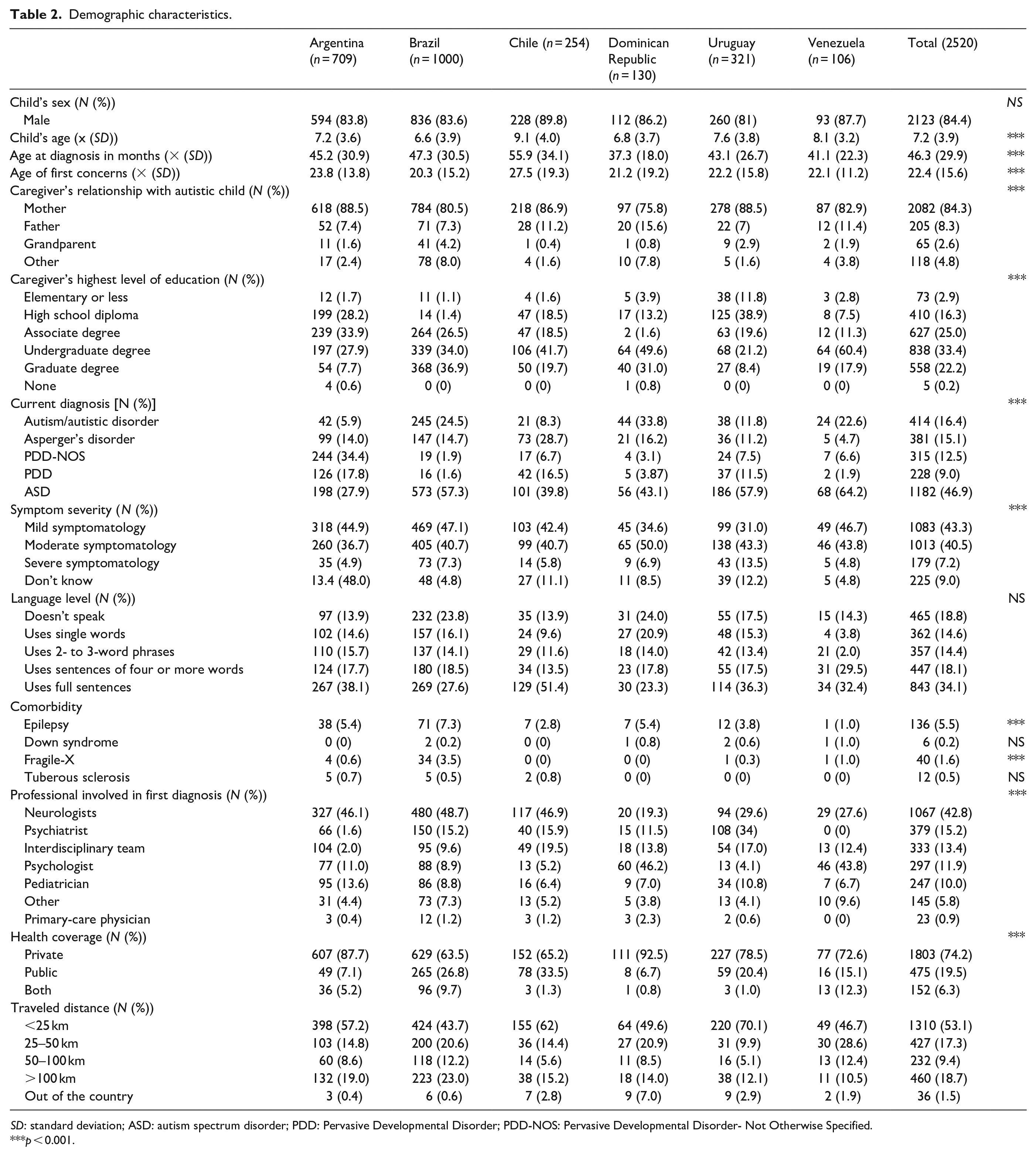
SD: standard deviation; ASD: autism spectrum disorder; PDD: Pervasive Developmental Disorder; PDD-NOS: Pervasive Developmental Disorder- Not Otherwise Specified.
p < 0.001.
Predictors of the age of ASD diagnosis
The multiple regression results indicated that the overall model explained 25.6% of observed variance and a significant collective effect between predisposing, enabling, and need factors F (10, 24) = 85.04, p < 0.001. Within the predisposing factors, current age of the individual with ASD was the only factor that significantly predicted age of diagnosis. Enabling and need factors that significantly predicted the age of diagnosis were health coverage type, country of residence, type of diagnosis child received, comorbidity with another medical, neurological or genetic issue, and language level of child (Table 3). When observing these factors closer, age of autistic child (predisposing factor) increased age of diagnosis by 19.61 months. Within the enabling factors, significant predictors of age of diagnosis were type of health coverage, with public health coverage increasing age of diagnosis by 3.22 months, country of residence decreased age of diagnosis by 1.38 with Chile having the oldest mean age of diagnosis (M = 55.98, SD = 34.09) and Dominican Republic the youngest mean age of diagnosis in months (M = 37.34, SD = 18.04). For need factors, the presence of comorbidity such as medical, neurological, and genetic conditions decreased age of diagnosis by 8.86 months, severity level decreased it by 3.27 months, whereas type of diagnosis decreased it by 1.89 months. Finally, language level of child with ASD increased age of diagnosis by 7.92, with those children exhibiting better language abilities being diagnosed later.
Predictive factors for age of diagnosis.
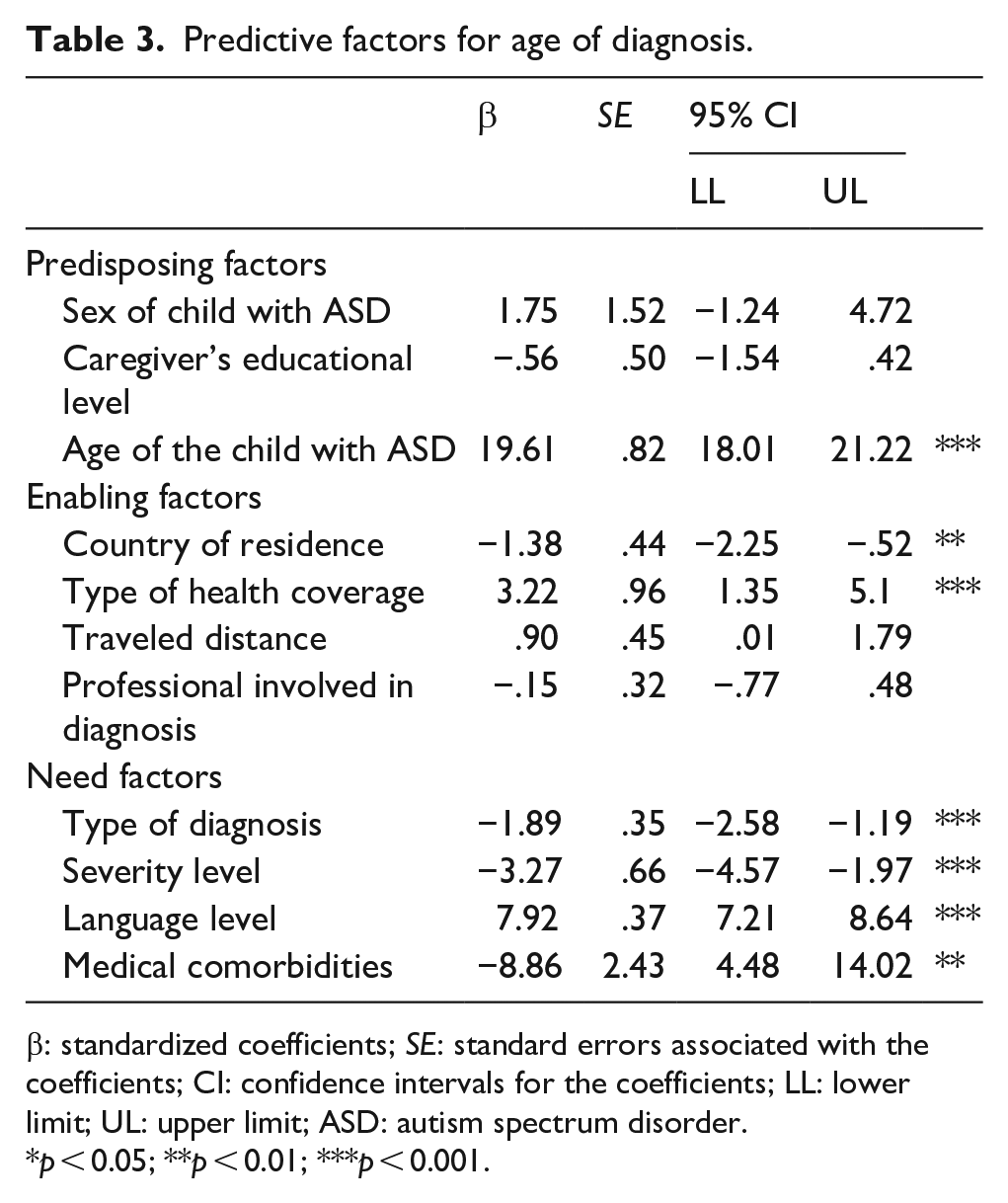
β: standardized coefficients; SE: standard errors associated with the coefficients; CI: confidence intervals for the coefficients; LL: lower limit; UL: upper limit; ASD: autism spectrum disorder.
p < 0.05; **p < 0.01; ***p < 0.001.
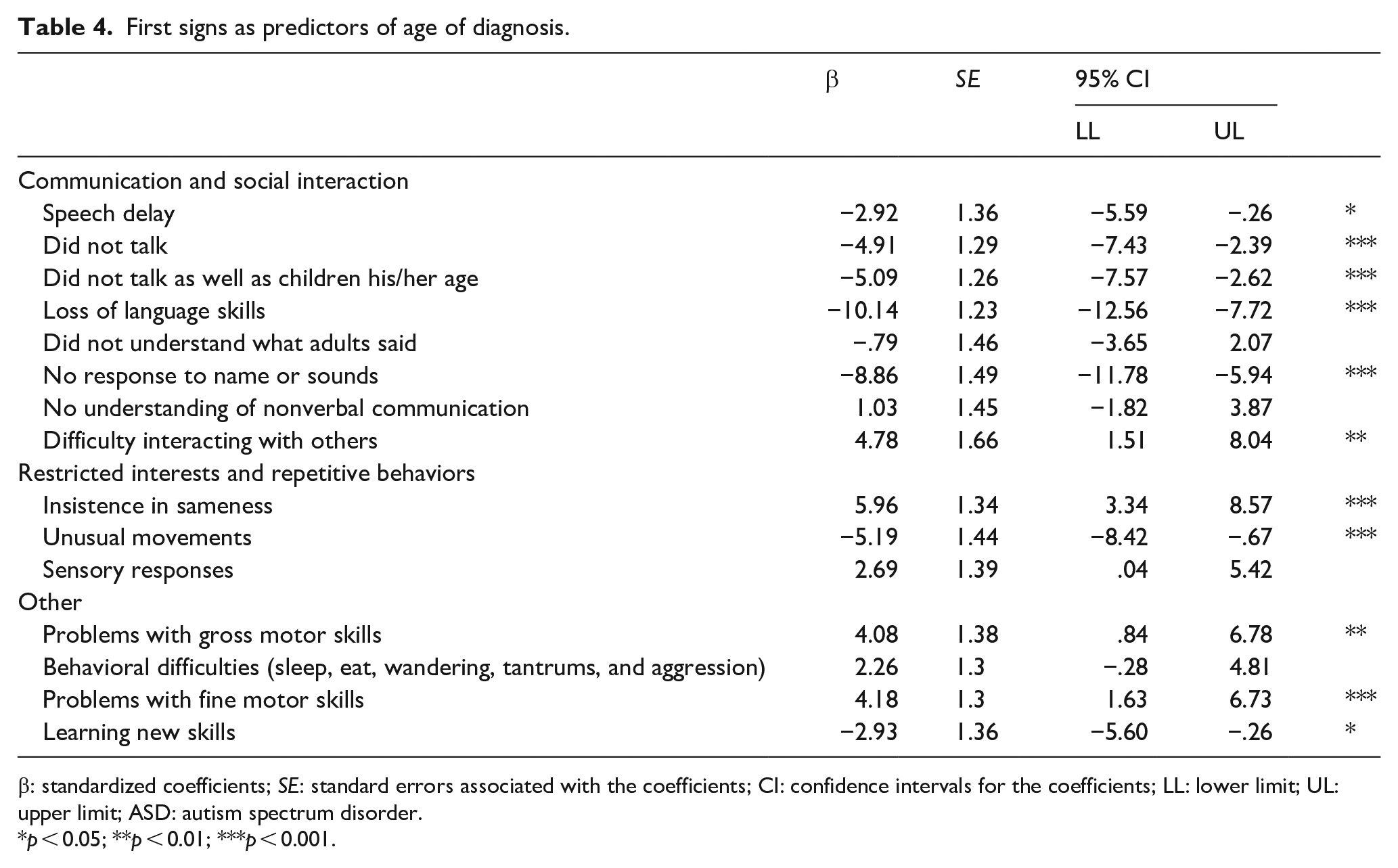
Among the need factors, we were particularly interested in understanding the role of the caregiver’s first concerns (Table 4). These predictors, grouped to match DSM-5 domains for diagnostic criteria (APA, 2013), consisted of a Communication and Social Interaction domain, which included child not responding to name or to sounds (β = –8.86, p < 0.001), speaking delay (β = –2.92, p < 0.05), not talking (β = –4.91, p < 0.001), not speaking as well as other children their age (β = –5.09, p < 0.001), and loss of language skills (β = –10.14, p < 0.001). Within the Restricted Interests and Repetitive Behaviors domain, insisting on sameness (β = 5.96, p < 0.001) and having unusual movements such as flapping (β = –5.19, p < 0.001) were significant predictors. Finally, other concerns reported by caregivers that predicted age of diagnosis consisted of problems with gross motor skills (β = 4.08, p < 0.05), problems with fine motor skills (β = 4.18, p < 0.01), and difficulty learning new skills such as getting dressed (β = –2.0, p < 0.05).
First signs as predictors of age of diagnosis.
β: standardized coefficients; SE: standard errors associated with the coefficients; CI: confidence intervals for the coefficients; LL: lower limit; UL: upper limit; ASD: autism spectrum disorder.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
The first signs of autism are recognizable in the first years of life, and with the growing evidence of the benefits of early intervention programs (Dawson et al., 2022; Devescovi et al., 2016; Zwaigenbaum et al., 2015), the importance of having an early autism diagnosis is more evident and pressing. A later diagnosis is considered a factor influencing the developmental trajectory of autistic children (Loubersac et al., 2021). Our study’s first objective was to assess differences between age of first concern observed by caregivers and age of diagnosis received. In our sample, and consistent with other studies conducted in South America (Montiel-Nava et al., 2017; Ribeiro et al., 2017) and other regions of the world (Karst & Van Hecke, 2012), caregivers indicated first concerns of their child’s development by 22 months of age; however, according to our sample, the diagnosis did not come until 21 months later. Nonetheless, our sample was highly educated, and the survey required parents to have Internet access and a computer, posing a sampling bias. Such bias implies that our results underestimate the age of diagnosis of the general population that has lower education and limited access to the Internet. Also, in our sample, we collected information from a group of caregivers with better access to healthcare services than the regular citizen, as evidenced by the high percentage of caregivers with private insurance. This is a significant finding since all participating countries have universal health coverage. Our results depict the health disparities characteristics of LACC countries.
The age of diagnosis in our study corresponds to the start of formal schooling in most of the countries included, which could be too late for the access to early intervention programs since many of these programs are provided for children under the age of 3 (Lopez, 2014; Shrestha et al., 2019). This is unfortunate when one considers some autistic individuals who access earlier intervention are more likely to no longer meet ASD diagnostic criteria and need less services and support (Orinstein et al., 2014).
Despite previous studies exploring factors influencing later age of diagnosis (Mandell et al., 2005; Zuckerman et al., 2017), our research is the first to explore multiple predictors of the age of diagnosis in LACC. Through our second objective, to explore predisposing, enabling, and need factors and their influence on delayed diagnosis, we can better understand risk factors for delayed diagnosis despite caregivers noticing early concerns. The type of diagnosis child received, comorbidity with another medical, neurological, or genetic issue, and language level of child (need factors), current age of the individual with ASD (predisposing) and health coverage type and country of residence (enabling factor) are the drivers for the age of ASD diagnosis identified in our sample.
One of the significant factors affecting a delayed diagnosis was the actual age of individuals with ASD when the study was being conducted. Older individuals had a later diagnosis than younger ones. These results indicate that in Latin America and Caribbean, age of diagnosis has been decreasing throughout the years. A meta-analysis by van’t Hof et al. (2021) showed a similar worldwide tendency toward a reduced age of diagnosis in recent years. This trend could be explained by important changes that have occurred throughout the years, such as more inclusive and encompassing diagnostic criteria, more specialized diagnostic tools, and improved symptom recognition in society at large (National Academies of Sciences, Engineering, and Medicine, 2015). Yet, it is important to note that despite an earlier age of diagnosis among younger individuals, there was still a large gap between age of first concern observed by caregivers and diagnosis received.
Our findings suggested that predisposing factors such as sex of the autistic individual and caregivers’ level of education were not predictors of age of diagnosis (see Table 4). Even those finding are not consensual in the literature, our results are similar to the ones obtained by Rosenberg et al. (2011), for which sex of child and education of caregivers were not significant predictors for later diagnosis. In this study, possible confounding variables could have affected a delayed diagnosis such as females with Asperger showing less stereotypical ASD symptoms and exhibiting more developed language skills (Rosenberg et al., 2011). In our sample, more than 80% were males, possibly accounting for the lesser effect of sex imbalances in delayed diagnosis. In terms of caregiver’s education effect on age of diagnosis, results are mixed. Previous studies indicate that lower education is associated with a later age of diagnosis (Fountain et al., 2011). In contrast, other research indicates that when controlling for confounding variables, such as health coverage, caregivers’ education ceased to be statistically significant (Shattuck et al., 2009). Rosenberg et al. (2011) posit a plausible explanation for this last scenario, in which caregivers willing to participate in research studies are highly motivated. When this is the case, educational level ceases to be a significant predictor of age of diagnosis.
In our sample, type of health coverage predicted age of diagnosis with public health coverage delaying diagnosis by several months. Public health coverage does not warrant access to diagnostic services in many participant countries, and the cost of diagnostic services is not affordable for most parents. This result should reflect service access differences between high and low SES families, even among those from LMICs, as the cost of a diagnostic evaluation is a barrier to accessing care. Policymakers must be alert to these results and attempt to eliminate diagnosis and treatment disparities. Especially when considering the large economic impact associated with ASD and the high out-of-pocket costs (Zavaleta-Ramírez et al., 2020). For example, a study by Horlin et al. (2014) indicated high costs associated with needed services and the loss of income due to increased time needed to care for the autistic individual. Horlin et al. (2014) further reports of the increased cost for every added symptom.
Country of residence also influenced later diagnosis, with autistic individuals in Chile being diagnosed later compared to other countries at almost 60 months (Table 1). These differences could be partially explained by caregivers reports of first observed concerns being highly shaped by environmental factors and cultural norms (Amiet et al., 2014; Mandell et al., 2009; Norbury & Sparks, 2013; Nowell et al., 2015). Another plausible explanation could be variability in terms of countries policies and laws that protect vulnerable populations (Montiel-Nava et al., 2020) and limited implementation of these. For example, a recent study by Sakellariou et al. (2020) examined legislations and decrees aimed at protecting the population at large in several Latin American countries including Argentina, Brazil, and Chile. Results indicated that even when legislations were passed, these rarely included the protection of disabled individuals. Moreover, in those instances in which legislations included special provisions to protect disabled individuals, these rarely had a protocol in place to ensure their implementation. These issues, despite being more salient in Chile, indicate a generalized fragmented and oftentimes non-existence inclusive legislation where those most vulnerable are not being properly safeguarded (Sakellariou et al., 2020). Contrary to what was expected, traveled distance was not a predictor of age of diagnosis. Our participants were residents of capital or big cities, partially explaining these results. Although traveled distance was not identified as a barrier for our participants, not needing to travel does not represent a better access to services, since in LACC the few available services are usually overbooked and with few trained specialists (de Almeida, 2005; Kohn et al., 2018).
Child characteristics, symptom severity, and language ability also significantly affected age of diagnosis. Those with more severe symptomatology were diagnosed earlier as observed before. For example, autistic children without cognitive impairment are diagnosed later than those with more noticeable symptomatology (Maenner et al., 2020, van’t Hof et al., 2021). Language could also, partially, explain differences in age of diagnosis with less verbal types of ASD being diagnosed earlier as observed in our sample. Previous research has shown how individuals with Asperger’s, who exhibit overly precision in language are diagnosed later (de Giambattista et al., 2019). And thus, a call is made for clinicians and service providers to increase awareness, particularly among mild and verbal autistic children.
This study identified that children with medical comorbidities were also diagnosed earlier. Research on the topic shows that depending on type of comorbidity, age of diagnosis can be impacted. For example, those with epilepsy show greater impairment in areas of social awareness and communication which could predispose them to an earlier diagnosis (Ko et al., 2016). Other studies show a different picture when other comorbidities are present. For example, a systematic review by Sainsbury et al. (2022) showed that those with a comorbidity such as attention-deficit hyperactivity disorder were diagnosed later with an ASD diagnosis. In other words, because of the diagnosis of the comorbid condition, ASD was not being recognized. For caregivers, this is problematic. Stevens et al. (2016) indicated that caregivers of children with ASD and other comorbidities were diagnosed with ASD almost 4 years later. Furthermore, the misdiagnosis or missed diagnosis prevented caregivers from having the whole picture of what was happening to their child and distracted specialists and educators from considering an ASD diagnosis (Stevens et al., 2016). And thus, a key component of an ASD diagnosis is having a comprehensive view of the child’s symptomatology to ensure ASD is not misdiagnosed or underdiagnosed. One way to achieve this is paying close attention to caregivers, who are experts when it comes to understanding their child’s symptomatology (Bangerter et al., 2019). However, some specialists in Latin-American countries might perceive lower-income patients as not possessing the requisite rationality and understanding to cope with a diagnosis (Cooper, 2015). In this aspect, lower-income families would be in a disadvantages position when trying to access diagnostic services.
When contemplating first concerns observed by caregivers, not only did caregivers in our sample indicate an earlier age of concerns than the time of the actual diagnosis was provided, but the most endorsed first concerns aligned with ASD diagnostic criteria as per the DSM-5 (APA, 2013). For example, difficulties maintaining eye contact, communication, and interacting with others allude to persistent social difficulties that are a hallmark of ASD. Similarly, concerns regarding insistence on sameness, unusual movements, and sensorial responses may indicate a pattern of restrictive and repetitive behaviors/interests which also characterize ASD. Despite similarities in terms of first concerns observed by caregivers and DSM-5 diagnostic criteria, it is important to note that comparable to those participating in the Autism and Developmental Disabilities Monitoring Network in 2006, where Latino children in the United States exhibited fewer behaviors from the repetitive/restricted domain (Maenner et al., 2013), in our sample, these behaviors were also among the least frequent categories reported by parents. And thus, it is imperative for practitioners to be aware of these least-reported concerns to ensure Latinos in general do not continue to be misdiagnosed or underdiagnosed due to caregivers feeling they are being ignored and not listened to (Chlebowski et al., 2018).
Autism research suffers from incomplete and biased knowledge since it usually takes place in North America and western Europe and mostly focuses on White individuals (Cascio et al., 2021; Durkin et al., 2015). As Cascio et al. (2021) so eloquently puts it “The exclusion of marginalized subgroups of people with autism is a major ethical concern.” (p. 22). And thus, by focusing on the lived experiences of caregivers of individuals with ASD living in LACC, this study is consistent with recent calls within the autism community to expand research horizons by becoming more inclusive of those usually underrepresented and unsupported (Cascio et al., 2021; Durkin et al., 2015).
Our study had limitations such as diagnosis not being confirmed by a healthcare provider or specialist. Moreover, a biased sample might have been yielded due to the sampling process and families coming from higher educational backgrounds, having a computer and access to the Internet, thus skewing our sample toward a population of caregivers with higher financial means. Consequently, our findings might underestimate age of diagnosis of those with lower educational background and without Internet. Despite multiple countries being included, interpreting results was challenging due to different policies and practices. In addition, sample size was not homogeneous across countries, representing another facet of sampling bias. Future studies would benefit from doing a more in-depth analysis on how regional policies and practices affect age of diagnosis. As a cross-sectional survey study, results have limitations in terms of inferential or predictive results. In that regard, data were collected retrospectively and with caregivers of children with a wide age range, which poses a risk for recall bias in the participants. Finally, it is important to mention that this survey was originally developed in English, and the majority of questions were adaptations of instruments developed for a population with different cultural and ethnic background. Hence, it is likely that the responses elicited from the survey did not capture the diverse cultural subtleties and caregivers needs in the participating countries (Paula et al., 2020).
Despite these limitations, this study not only assessed age of diagnosis and first concern of caregivers in a multisite sample of caregivers but also described multiple factors impacting the age of diagnosis of autistic individuals living in six LACC. The analysis of a multinational caregiver’s survey provided us with information usually not presented in research (Baxter et al., 2015; Elsabbagh et al., 2012). In addition, an important contribution provided by this study is the better understanding of caregivers’ concerns within specific ASD symptom areas which has important implications for screening ASD within different cultural groups (Rato et al., 2016). Knowing which early signs are reported and at what rates could further help clinicians and researchers be better equipped at listening and identifying caregivers’ concerns as signs for possible ASD diagnostic criteria. In addition, this study can serve policymakers and community advocates from Latin America, the Caribbean, and other less-favored regions to design and implement public policies and community outreach endeavors that will better help treat and diagnose autistic individuals.