
Abstract
Effective support for autistic individuals is lacking in Brazil. Few centres offer services and those that do are limited in therapeutic options and geographical location. Paediatric Autism Communication Therapy is a low-intensity, evidence-based parent-mediated social-communication intervention that may be useful for this scenario. This implementation study aimed to assess the acceptability and feasibility of Paediatric Autism Communication Therapy for young autistic children (aged 2–10 years) in Brazil. Parents (n = 18) of 2- to 10-year-old autistic children and clinicians (n = 20) who work with autistic children in Brazil were interviewed and the data analysed using thematic analysis to explore their perceptions concerning the acceptability and feasibility of Paediatric Autism Communication Therapy. In addition, Paediatric Autism Communication Therapy was delivered to a case series of 15 further parent–child dyads; these parents were interviewed at the end of the therapy, and the data were analysed using thematic analysis. All parents and clinicians had favourable opinions about the acceptability, feasibility and perceived effectiveness of a parent-mediated intervention conducted mainly in the home. However, they also highlighted obstacles concerning the implementation of Paediatric Autism Communication Therapy in Brazil, especially related to engaging Brazilian parents in a parent-mediated model of therapy. Based on these data, minor adaptations were made to the original Paediatric Autism Communication Therapy protocol to facilitate the implementation of the intervention in Brazil.
Lay abstract
Parents of autistic children and health professionals who work with autistic children in Brazil had positive views about introducing Paediatric Autism Communication Therapy as a therapy for autistic children in Brazil. The parents and clinicians also mentioned some difficulties about using Paediatric Autism Communication Therapy in Brazil. We made adaptations to Paediatric Autism Communication Therapy to address these difficulties. Paediatric Autism Communication Therapy is a therapy to support the development of social and communication skills for autistic children aged 2–10 years. The therapy is conducted with the autistic child’s parent. Paediatric Autism Communication Therapy has not been used in Brazil before. There are few therapy options available for autistic children in Brazil and we believed that Paediatric Autism Communication Therapy may be useful. We asked three groups of people in Brazil about their views of Paediatric Autism Communication Therapy, after explaining how the therapy works. Group 1 included 18 parents of autistic children aged 2–10 years. Group 2 included 20 health professionals such as psychologists who work with autistic children. Group 3 included 15 parents of autistic children aged 2–7 years who received the Paediatric Autism Communication Therapy. We learned that parents and clinicians felt that Paediatric Autism Communication Therapy would be a beneficial therapy for autistic children in Brazil. We also found out about the challenges of using Paediatric Autism Communication Therapy in Brazil. We used these findings to make small cultural adaptations to Paediatric Autism Communication Therapy to make it more suitable for Brazil.
Introduction
Centres offering effective support and treatment for autistic individuals in Brazil are severely limited in number and geographical location, with only 650 centres nationwide (in a population of over 200 million) and 431 of those located in the south-eastern state of São Paulo (Portolese et al., 2017). Furthermore, the support and treatment options available are restricted mainly to psychoeducation and applied behaviour analysis (ABA) methods, and are not standardised across centres (Portolese et al., 2017). The Brazilian public health system (Sistema Único de Saúde, SUS) purportedly provides freely accessible mental health care for conditions such as autism via psychosocial care centres (Centro de Atenção Psicossocial, CAPS). However, CAPS centres for children are few in number and are unevenly distributed on a national scale; they also only offer non-standardised interdisciplinary group treatment for autistic children, which parents consider insufficient in terms of frequency and duration (Garcia et al., 2015; Lima et al., 2014). More accessible and acceptable therapeutic options for autistic children in Brazil are therefore crucially needed.
One intervention that may be particularly useful in the Brazilian context is Paediatric Autism Communication Therapy (PACT; Green et al., 2010). PACT is a parent-mediated therapy designed to improve social-communication development in young (2- to 10-year-old) autistic children of a wide ability range, including those with minimal language. The aim of PACT is to support child development via increasing parental sensitivity and responsivity to the autistic child’s communication and interaction as well as improving parental understanding of autistic and non-autistic social-communication development more broadly and their child’s social-communicative behaviour specifically. The intervention involves fortnightly sessions with the autistic child’s parent, during which a trained therapist supports the parent in learning how to increase their sensitivity to their child’s social-communication abilities and adapt their communication style to suit that of their child. To facilitate the parent’s learning, the therapist uses video feedback of play-based parent-child interactions. Parents also undertake 30 min of daily home practice of the PACT strategies with their child. See Aldred et al. (2018) and Green et al. (2010) for further details.
Randomised controlled trials (RCTs) of PACT in the United Kingdom highlighted its efficacy in increasing parental synchronous responses to child communication during parent–child interaction (Green et al., 2010; Green, Leadbitter, Ellis, et al., 2022). This altered parental synchrony resulted in increased child communication initiations with the parent, which in turn mediated enhancements in children’s independently evaluated social-communication skills and autism symptoms (Pickles et al., 2015). The treatment effect on autistic symptoms was sustained for several years post-treatment (Pickles et al., 2016). PACT also had positive effects on family well-being (Leadbitter et al., 2018). For these reasons, PACT is one of the social-communication interventions advocated by the UK NICE and by proposals for an evidence-based integrated care pathway for autism (Green, Leadbitter, Ainsworth, & Bucci, 2022). PACT has also been adapted, after an implementation study, for non-specialist delivery to parents of autistic children in South-Asian low- and middle-income countries (LMICs) (Divan et al., 2015, 2019). Data from RCTs showed that the PACT adaptation retained good fidelity to the original intervention model and was effective in improving parent-child communication compared to care-as-usual immediately post-intervention (Divan et al., 2019; Rahman et al., 2016).
Parent-mediated therapies such as PACT have been recommended as early interventions for autism because they are naturalistic (targeting everyday parent–child interactions) and may promote the generalisation of trained skills beyond specific tasks to the wider environment of the child, as well as stimulating family empowerment and resilience; these are important characteristics for long-term condition management (Green & Garg, 2018; Zwaigenbaum et al., 2015). While several other parent-mediated interventions for autistic children exist (recently reviewed in Crank et al., 2021; Sandbank et al., 2020), we selected PACT for implementation in Brazil for several reasons. First, PACT has a strong evidence base supporting its efficacy in improving various aspects of autistic children’s development and family functioning in both high-income countries (HICs) (Green et al., 2010; Green, Leadbitter, Ellis, et al., 2022) and LMICs (Divan et al., 2015, 2019; Rahman et al., 2016), as well as across delivery methods (online and in-person, parent-mediated and teaching assistant-mediated) (Green, Leadbitter, Ellis, et al., 2022). Indeed, an independently conducted meta-analysis of early autism interventions (Sandbank et al., 2020) highlighted the quality of the evidence for and methodology of PACT compared to other models.
Second, PACT has rigorous evidence for the mechanistic active ingredients for its positive effects on child outcomes. That is, improvements in the synchrony of parental (or teaching assistant) responses to the child in naturalistic interactions mediate improvements in child communication behaviour and autism symptoms (Green, Leadbitter, Ellis, et al., 2022; Pickles et al., 2015). This is an important consideration in cross-cultural adaptation because it allows for identification and testing of preserved key components of the intervention in new settings. The implementation of PACT in South-Asian LMICs demonstrated that this active ingredient was maintained in new settings (Divan et al., 2015, 2019).
Third, PACT is likely to be feasible for widespread use in an LMIC setting such as Brazil because it is low-intensity in terms of therapist time. This is important in any context but especially so in LMIC settings in which few resources are available in public health systems for neurodevelopmental interventions. Clearly, with reduced therapist involvement, the burden on families to provide therapy for their autistic child increases (Lord et al., 2022). This is a crucial consideration, especially for families in LMIC settings who may already be overburdened. To address this issue, PACT includes strategies to minimise parental burden (Aldred et al., 2018; Divan et al., 2015; Leadbitter et al., 2020).
Finally, extensive implementation work has been conducted to evaluate the feasibility and efficacy of PACT in LMICs. Implementation work is crucial to ensure that interventions are acceptable and feasible and retain their efficacy in new cultural contexts (Peters et al., 2013). While other autism intervention models have undergone implementation for LMIC contexts (e.g. Sengupta et al., 2020, 2021), there are currently no data on the efficacy of those programmes in LMICs.
In summary, due to the highlighted characteristics of PACT, its successful prior implementation in LMICs and evidence of efficacy in both high-income and low-resource settings, we believed this intervention to present an important and viable therapeutic option for implementation and potential scale-up in Brazil. However, to date, there have been no studies of parent-mediated interventions for autism, including PACT, in Brazil. We, therefore, conducted this implementation study to investigate the acceptability and feasibility of PACT in the Brazilian context. Our specific aims were (1) to identify factors (e.g. parental attitudes to autism, child development and interventions; family structure and income) in Brazil that may affect the implementation of PACT in this setting and (2) to make any necessary cultural adaptations to the original PACT protocol and manual related to those factors.
Method
Methods overview
This study follows implementation science guidelines for the use of qualitative methods in adapting interventions to new contexts (De Silva et al., 2014; Peters et al., 2013). Specific methods were also based on a previous implementation study adapting PACT to South-Asian LMICs (Divan et al., 2015). The study was conducted in three stages. The first focused on understanding perceptions of PACT in Brazil among parents of autistic children (potential service users) and clinicians who work with autistic children (potential care providers) who had no previous experience with PACT. The second involved the delivery of PACT to a case series of primary caregivers of autistic children in Brazil and the qualitative exploration of their perceptions of PACT after completing the intervention. Stage 3 involved adaptations to the original PACT protocol in line with the findings from stages 1 and 2.
Study setting
The study took place in São Paulo, South-Eastern Brazil. São Paulo is one of the largest cities in the world with a population of 12.3 million. It is the richest city in Brazil but also has huge inequalities. Some regions are marked by higher average family income, greater availability of leisure and cultural activities and lower criminality rates, while others (favelas) are characterised by extreme poverty, overcrowding, lack of sanitisation and high rates of criminality and violence (Venceslau, 2021). São Paulo has the largest concentration of autism centres in Brazil and thus may be the best location to begin integration of new therapies into clinical settings.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of the Faculty of Medicine at the University of São Paulo (CAPPesq, ref: 20340819.7.0000.0068). All participants provided written informed consent before completing any study activity.
Translation of PACT intervention materials to Brazilian Portuguese
Three bilingual (Brazilian Portuguese/English) researchers in Brazil (MR, LS and FSPA for translation; LS, RGC and FSPA for back-translation) with expertise in autism and child development translated and back-translated the PACT manual and other materials from English to Brazilian Portuguese. The translated materials were evaluated by three accredited PACT therapists (PBGG, LRS and ES) working with autistic children in Brazil. Adaptations to the manual and protocol (described below) were made in Brazilian Portuguese before back-translation to English. The back-translation to English was evaluated by three native English-speaking researchers with expertise in autism and child development, two of whom are trained in PACT (ES, KL and HL).
Stage 1: qualitative exploration of acceptability and feasibility of PACT with potential service users and care providers in Brazil
Overview
Qualitative semi-structured interviews were conducted to explore the acceptability and feasibility of the original PACT protocol and identify potential barriers to implementation among parents of autistic children (potential service users) and clinicians (potential care providers) who work with autistic individuals in Brazil.
Participants
Parent sample
Eighteen parents of 2- to 10-year-old autistic children were recruited via word-of-mouth among health professionals at our publicly accessible autism clinic at the Department of Psychiatry, University of São Paulo, and from other local mental health clinics. Parents were first informed of the study by their health professional. If the parent indicated interest in participating, the professional passed the parent’s contact details to the research team (with parental consent). A member of the research team (PBGG) then invited the parent by telephone to participate in the study. All parents provided written informed consent to participate. They were mostly mothers (n = 15) aged 24–46 years living in different regions of the state of São Paulo, Brazil. Demographic characteristics (collected during the telephone interview) are presented in Table 1.
Demographic characteristics of the parents of autistic children who participated in interviews about the acceptability and applicability of PACT.
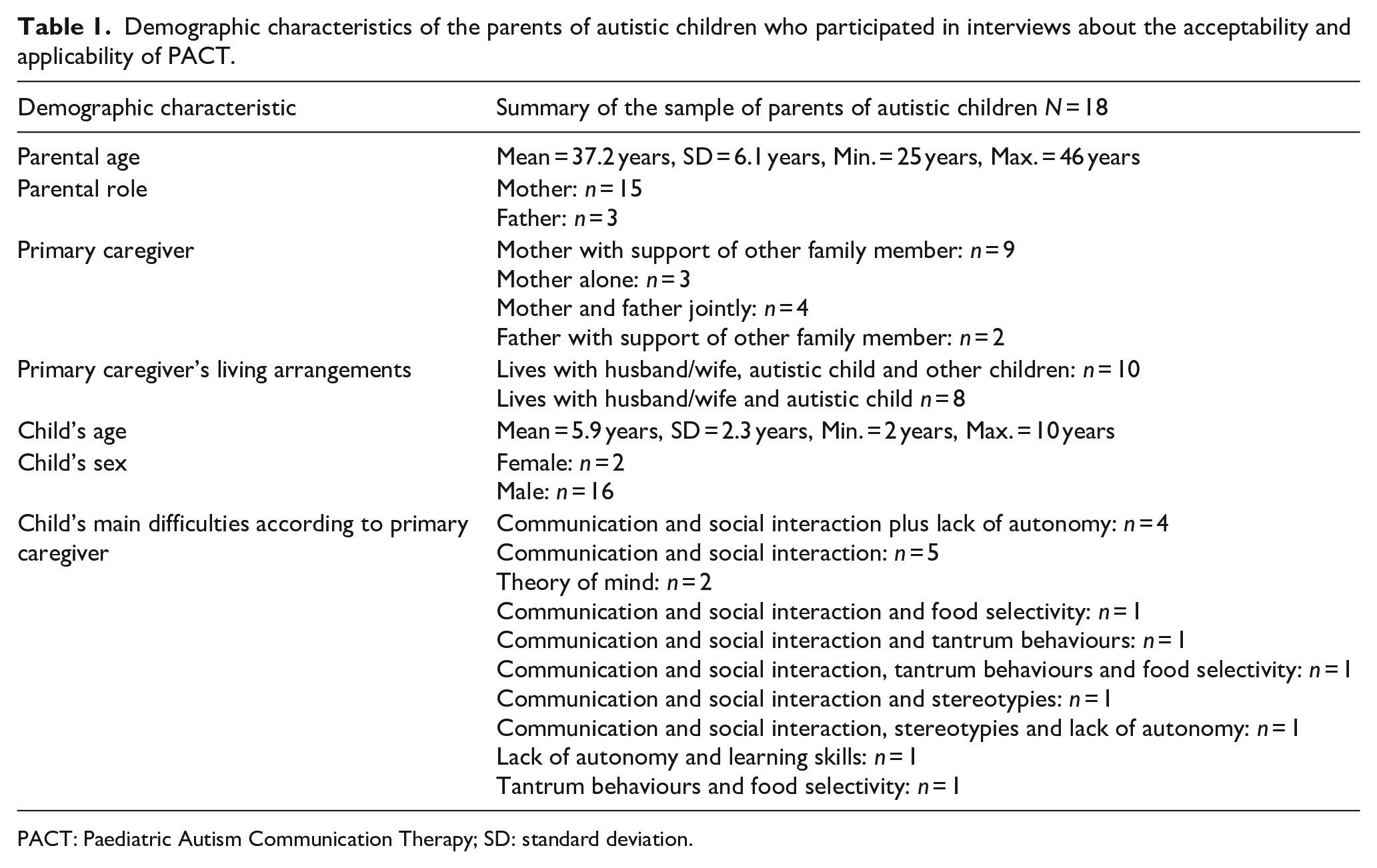
PACT: Paediatric Autism Communication Therapy; SD: standard deviation.
Clinician sample
Twenty clinicians and educators working with autistic children in Brazil were recruited by word-of-mouth from various states of Brazil, though principally São Paulo. We aimed to recruit professionals from both the public health system and private practice to understand the potential feasibility and acceptability of PACT in both healthcare settings. The majority (n = 15) of clinicians were working in private practices; the remaining five worked in the public health system, either exclusively (n = 2) or combined with private work (n = 3). Demographic characteristics (collected during the telephone interview) are presented in Table 2.
Demographic characteristics of the clinicians who participated in in-depth interviews about the acceptability and applicability of PACT.
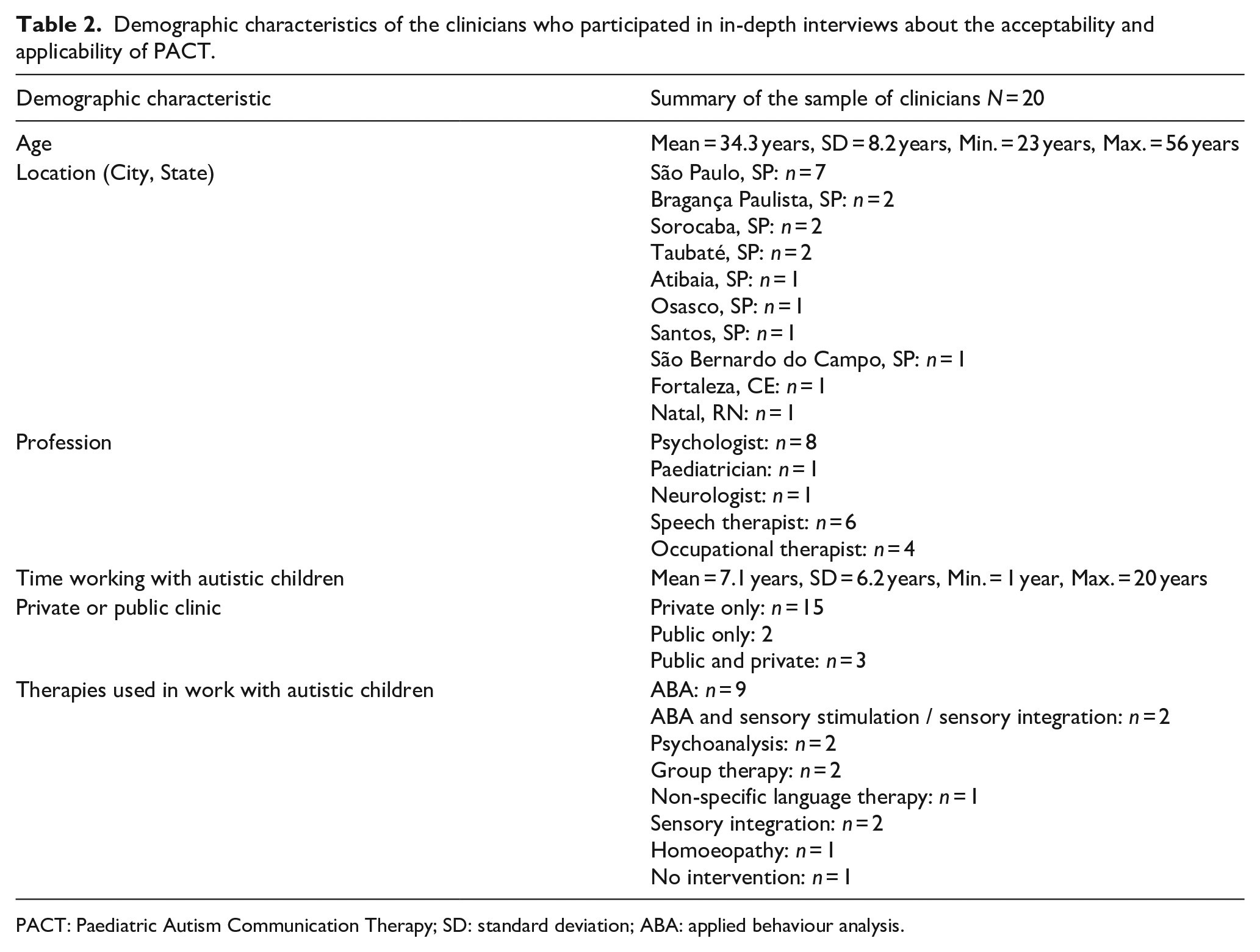
PACT: Paediatric Autism Communication Therapy; SD: standard deviation; ABA: applied behaviour analysis.
Data collection
In both parent and clinician samples, interview schedules were developed to cover the following key topics specifically related to the PACT intervention: opinions about parent-mediated reflective approaches to intervention, use of video feedback, duration of intervention, home visits, and factors (e.g. cost, childcare) affecting participation in intervention. The interview schedules (see eAppendix 1–2 in the Supplementary material) were based on a schedule successfully used in a previous adaptation study of PACT to South-Asian LMICs (Divan et al., 2015). The interview schedule of Divan et al. (2015) was reviewed by two key members of the Brazilian research team (PBGG, ES) to determine whether the content was appropriate for the research aims of the current study and subsequently translated to Brazilian Portuguese by PBGG (native Brazilian Portuguese speaker and fluent in English). No changes were made to the interview schedules once data collection had begun.
All interviews were carried out in Brazilian Portuguese, via telephone (necessitated by the COVID-19 pandemic during 2020), in one sitting of 27–52 min (mean 40 min) for the parents and 23–67 min (mean 40 min) for the clinicians. Interviews were audio-recorded with consent and conducted by a native Brazilian psychologist with experience in neurodevelopmental conditions and trained in PACT (PBGG), who had no prior contact with the clinicians and parents. Before beginning the interview questions, the researcher explained the purpose and methods of the implementation study and the PACT intervention. Previous studies have indicated that telephone interviews can provide sufficient data to understand multiple perspectives from individuals when needed (Lechuga, 2012). Data collection began with the sample of parents (date of first parental interview: 24 January 2020, date of last parental interview: 28 April 2020). Data collection from the sample of clinicians was conducted shortly after completion of parental data collection (date of first clinician interview: 08 May 2020; date of last clinician interview: 26 August 2020). The end of data collection was determined by a combination of COVID-19 pandemic restrictions, the need to conduct the case series and implement changes to the PACT protocol, and the finding that no new information emerged from analyses of collected interview data. These interviews were conducted during the first months of the COVID-19 pandemic; therefore, the intervention was presented to parents and clinicians as an intervention that could be delivered flexibly in clinic, in the family’s home or online, rather than in online-only format, which is how the parents in the case-series received the intervention in Stage 2.
Analysis
All analyses were conducted by one main researcher, PBGG, who is a native Brazilian psychologist, neuropsychologist and accredited PACT therapist and is fluent in English. Parental and clinicians’ interviews were transcribed verbatim by PBGG in Brazilian Portuguese. Interview data were then analysed by PBGG using thematic analysis following the six phases outlined by Braun and Clarke (2006); Clarke and Braun (2013). A senior researcher with expertise in qualitative analysis methods (LM) supervised the analysis.
Data coding and theme development were approached at the semantic level and primarily using top-down deductive coding due to our aim of addressing the specific research questions (understanding the acceptability and feasibility of PACT and specific barriers to its implementation in Brazil). However, data-driven inductive coding was also included whenever important information that was not directly related to the research questions was present. A critical realist epistemological standpoint was taken since we wanted to understand the experiences of the participants in relation to autism interventions and PACT specifically, and we assumed they would report those experiences in a way that more or less reflected their realities.
Interview transcripts were first read repeatedly to become immersed and intimately familiar with the data and make notes of early impressions (Phase 1: Familiarisation). Next, initial codes were generated from important features of the data considered relevant to answering the research questions, that is potential benefits and obstacles related to PACT, impressions about the PACT protocol and methods (Phase 2: Coding). Data were coded using MAXQDA 2020 software (VERBI GmbH, Berlin, Germany). A slight departure from Braun and Clarke’s (2006, 2013) method was taken in that a second bilingual researcher (ES) with expertise in autism and PACT conducted familiarisation and coding phases independently on a proportion of the interviews (approximately 5%) to aid in the process of data familiarisation. Since the results of this study will be used for very practical purposes, that is the adaptation of an intervention for vulnerable young children in a new cultural and socioeconomic setting, and the results will potentially have important implications for this population, we wanted to ensure that the main analyst could discuss any doubts about their understanding of the parental and clinician’s responses and coding with another researcher who was also intimately familiar with the interview data. The main analyst’s coding was used for the remaining stages of the analysis (Phases 3–5: Theme development, refinement and naming). In these phases, all initial codes were organised into preliminary themes by PBGG. Specifically, using data from all parents and clinicians, PBGG grouped codes into potential themes and sub-themes according to their semantic associations and relation to the topics of the interview schedule, which in turn mapped on to the research questions of the study. The data in each candidate theme were then translated to English by PBGG; translations were checked by a native English speaker also proficient in Brazilian Portuguese (ES) in preparation for Phase 6 (Writing). The themes were then discussed by PBGG and at least one other senior researcher (ES and/or LM). Finally, themes were reorganised, refined and named and quotes from each participant were selected for illustration.
Stage 2: case-series to assess the feasibility of delivering PACT in Brazil
Overview
Three psychologists (PBGG, LRS and ES) resident in São Paulo were trained in PACT by the developers of the intervention in Manchester, UK. Training included a half-day online e-learning component and a 2-day in-person course with classroom-based learning, video review, role-play and session observation as well as post-course supervision. These same psychologists administered PACT to a case series of 15 dyads of primary caregivers and their autistic children aged 2–10 years, with online supervision from the UK PACT team. At the end of the intervention, each parent was interviewed to explore their perceptions and experiences of receiving PACT.
Participants
The parent–child dyads were receiving care from child psychiatrists at two publicly accessible clinics in São Paulo (one at the Department of Psychiatry, University of São Paulo; one CAPS centre). Eligible caregivers (defined as those who had a child aged 2–10 years with an existing clinical diagnosis of autism) were initially approached by their child psychiatrist and informed about the study. Caregivers who expressed interest in receiving PACT as part of the case study were then referred to the research team. A member of the research team (PBGG) contacted the caregiver by telephone to explain the study in full and confirm whether they would like to participate. All caregivers provided written informed consent prior to participating.
The dyads were mostly from different regions of São Paulo and all primary caregivers were mothers. In one case, in addition to the mother, an adult older brother who took care of the child most days participated in the intervention. Demographic characteristics are presented in Table 3. Of the 15 dyads who consented to participate, 11 received all 12 sessions of the intervention. Of the four who did not complete the 12 sessions, two discontinued after session 9 and two withdrew after the initial (see ‘Results’ section for further details).
Demographic characteristics of the parent–child dyads participating in the case-series and post-PACT interview.
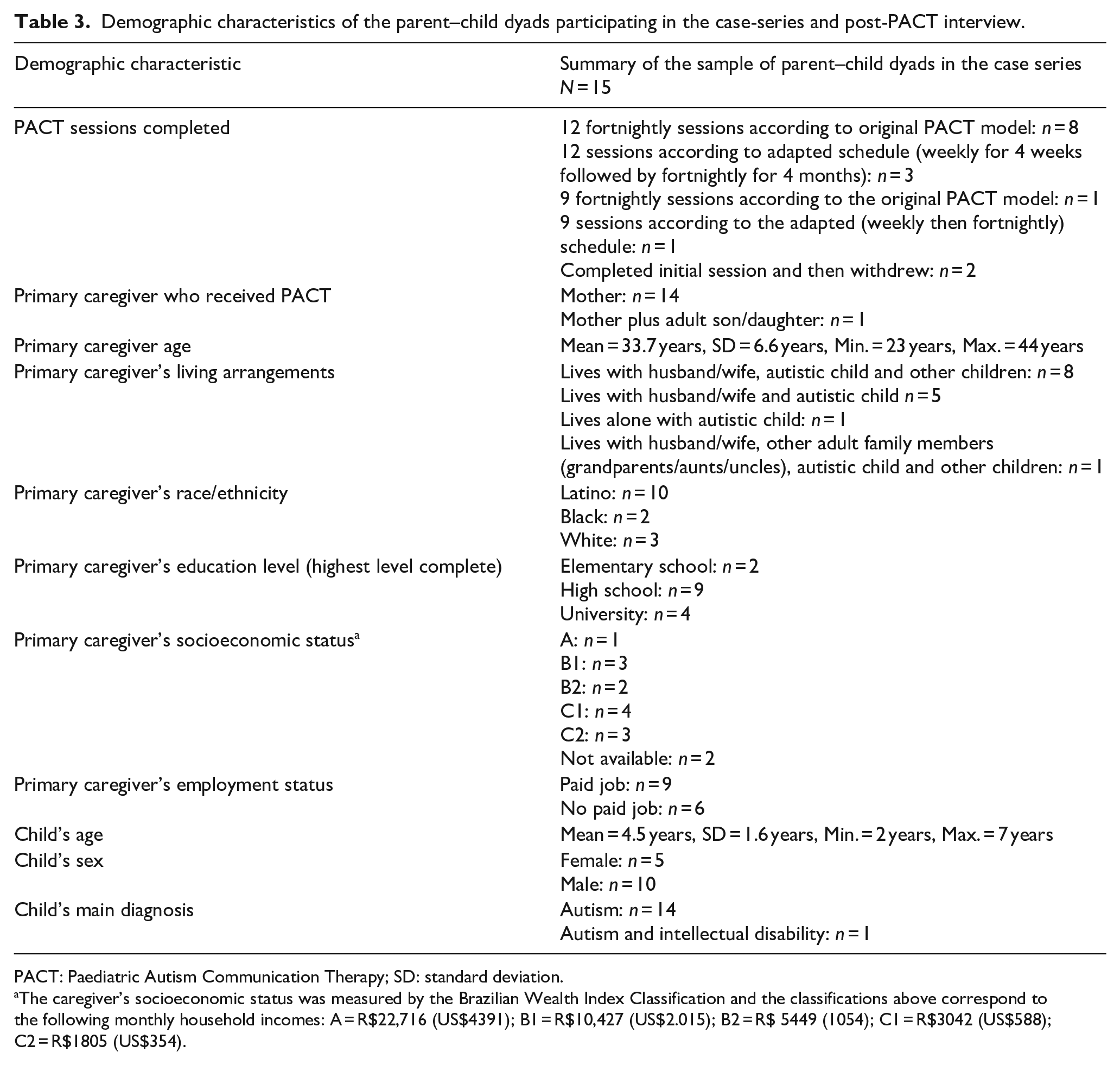
PACT: Paediatric Autism Communication Therapy; SD: standard deviation.
The caregiver’s socioeconomic status was measured by the Brazilian Wealth Index Classification and the classifications above correspond to the following monthly household incomes: A = R$22,716 (US$4391); B1 = R$10,427 (US$2.015); B2 = R$ 5449 (1054); C1 = R$3042 (US$588); C2 = R$1805 (US$354).
The case series included two subgroups of participants. The first included 11 parent–child dyads who were recruited to receive 12 fortnightly sessions of PACT delivered over 6 months according to the original protocol. The second included four parent–child dyads who were recruited to receive an adapted schedule delivered over 5 months, consisting of 4 weekly sessions followed by eight fortnightly sessions. This adaptation was made in response to themes developed in analysis of the interview data from parents and clinicians (described below).
Data collection and analysis
All PACT sessions were delivered online, via Skype or Zoom, due to the COVID-19 pandemic preventing in-person sessions during 2020. Modifications required to the PACT protocol to enable families to participate and retention rates were documented throughout the case series and are described below. At the end of the case series, interviews were conducted with each participating mother to evaluate parental opinions and experiences of receiving the intervention. Caregivers who did not complete all 12 PACT sessions were also contacted and invited to participate in the post-intervention interview. The interviews were conducted in Brazilian Portuguese, via telephone, within 1 week after the end of the intervention, in one sitting of 14–40 min (mean 22 min) and by the same PACT-trained Brazilian psychologist who conducted the parental and clinicians’ interviews (PBGG). Since the interviewer had also delivered the intervention to some of the families, parents were reassured that they should respond honestly about their opinions because their responses would be used to determine the acceptability and feasibility of PACT for Brazil and identify any changes needed. Responses of the families who received the intervention by PBGG were compared to those of parents who received PACT by the other therapists and no differences were detected in the themes reported. The interview schedule (available in eAppendix 3, Supplementary materials) covered the following key topics related to the research questions of the study: general impressions about having received PACT (benefits, harms and challenges), opinions about the video-feedback and the parent-mediated format, feasibility, benefits and challenges of the home setting configuration and the home practice between sessions, impressions about the frequency and duration of the intervention, and changes in the dyad’s interaction behaviour.
Post-intervention interviews were processed and analysed using the same methods as for the parental and clinicians’ interviews described above for Stage 1. We chose to analyse the datasets from Stage 1 and Stage 2 separately because it is a very different experience to hear about an intervention, in the case of the first sample of parents and clinicians, than to receive an intervention, in the case of the parents in the case series.
Stage 3: adjustments to the PACT protocol to suit the Brazilian context
Potential adaptations to the original PACT protocol and manual were identified by PBGG and ES following analysis of the interviews with parents and clinicians and during and after the case series. Potential changes were discussed in depth with members of the PACT consortium (KL, JG) and researchers who conducted the implementation and adaptation of PACT to South-Asian LMICs (GD, KL, JG). Adjustments were accepted if there was consensus among all researchers (PBGG, ES, KL, GD, JG) that they were necessary. The adjustments (reported in the ‘Results’ section) were made in Brazilian Portuguese and included in the translated manual and the back-translation to English.
Results
Stage 1: findings from the qualitative interviews from parents and clinicians about the acceptability and feasibility of PACT
Three themes concerning the acceptability and feasibility of PACT were developed from parental and clinicians’ interviews (Figure 1).
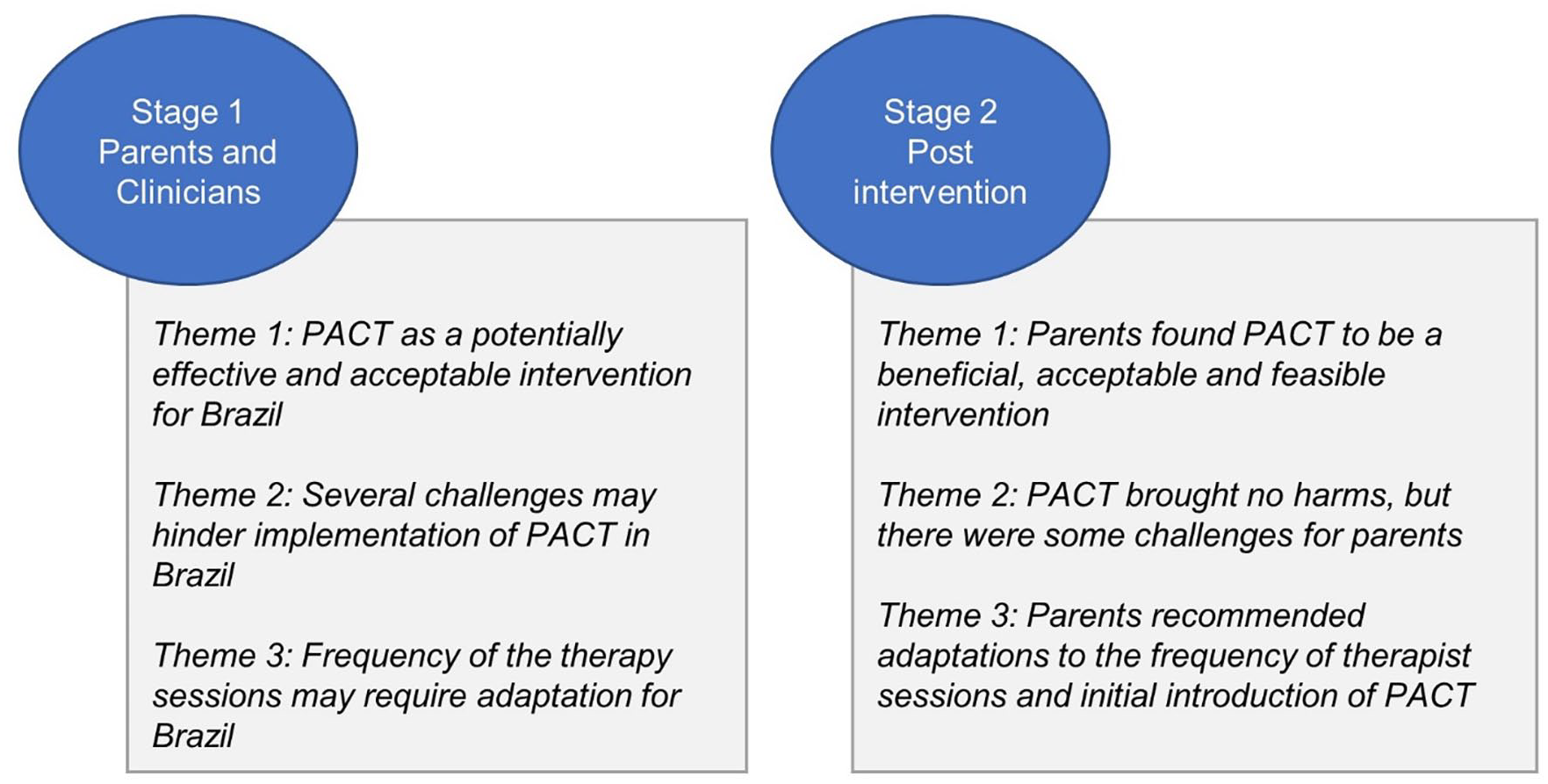
Summary of themes developed in the parental, clinician and post-PACT interviews.
Theme 1: PACT is a potentially effective and acceptable intervention for Brazil
Parents and clinicians had favourable opinions about the feasibility and perceived effectiveness of a parent-mediated intervention that would be conducted mainly in the home. This included viewing PACT as an intervention that could help parents with how to interact better with the child and provide them with the skills to support their child’s social-communication development: I really liked it [PACT] because, in fact . . . we go to the speech therapist and the psychologist once a week, but I think we really need to be prepared, whoever is with him at home, in his daily life, needs to know how to help him develop better, because it is not with a once-a-week therapy that he will be able to learn what he needs to learn . . . (Parent, ID 9) It brings advantages because you will teach the family how to interact better with the child and this will improve the parents’ and the child’s social communication skills. This will bring benefits to the child’s own interaction with the family in their daily life, so the family will see that when they communicate differently with the child, it improves their communicative skills. And the child’s improvement can be a reinforcement for the family to continue engaging in behaviors that will benefit the child’s communication skills, as a circle of reinforcement. (Clinician, ID 20)
Clinicians additionally highlighted that PACT would have broader benefits, including positive effects on parents’ mental health and its feasibility, as a low-cost intervention, for use in the Brazilian public health system: I think [focusing on parent-child interaction and social communication skills] is the key to improving parents’ quality of life, many parents report not interacting with their children because they do not know what to do, so I think it is very important . . . (Clinician, ID 1) I think it’s super feasible for Brazil. Exactly because it contributes to the reduction of hours of therapies, which implies better cost, which is very important . . . the other thing is the child’s development, because of the greater involvement of the family in the intervention . . . when the family is involved it helps a lot. Especially for our reality, thinking about the public health issues, this is extremely important. (Clinician, ID 14)
In addition to the benefits of PACT, both parents and clinicians considered practical aspects of the therapy to be acceptable and feasible for the Brazilian context. For example, several parents said they would manage to integrate the home-practice in their daily lives: ‘I think it is possible to manage the house routine so that you have 30 minutes to pay attention to your child, to play with him’. (Parent, ID 3). Most parents and clinicians seemed to particularly like the video-feedback aspect of PACT and considered this to be an effective tool for intervention: With the video we can have a different point of view because when you are there, inside the play situation, you can behave wrongly, but after watching the video you can see what you could have done . . . this will help the therapist to explain to the parents what was happening in the play situation and how to do it better . . . I think it’s positive. (Parent, ID 2) The use of video also seems to be very effective . . . When parents observe themselves in the video, they are also able to pay attention to various aspects of their own behavior that they did not see before while they were involved in the situation. I think it is really good. (Clinician, ID 17)
Theme 2: several challenges may hinder implementation of PACT in Brazil
Parents and clinicians noted several potential barriers to the successful use of PACT in Brazil. These included cramped and noisy home environments, which could complicate parents’ implementation of the intervention strategies: Particularly in my case it would be an obstacle . . . because I live in small place with 5 more houses, there are a lot of people there, so this is already an obstacle. So, having a quiet place is difficult. (Parent, ID 15) I think social and economic issues may be obstacles. Many families would easily have adequate space and time [to practice], but many families do not . . . people who live with the rest of the family in the house, share rooms with other people or parents who have many children, I do not know if they would have the entire 30 minutes uninterrupted in an adequate place. (Clinician, ID 8)
Several parents also highlighted that it would be challenging for many parents to find time in their busy day-to-day lives for the intervention: ‘I think [PACT] is important, but you have to consider that some parents work and don’t have so much free time and this type of therapy could end up psychologically overloading them’. (Parent, ID 4).
Both parents and clinicians raised the issue of cultural beliefs surrounding treatment for children in Brazil. They noted that it may be difficult to engage parents in PACT due to perceptions that a professional should be responsible for treating the child, not the parent: I think the biggest obstacle is going to be explaining why the therapist cannot apply the therapy themselves, why it has to be the parents, because there are parents who think they put the child in a clinic for therapy, so they don’t need to do anything else. (Parent, ID 17) While you were explaining [PACT] I was thinking about some patients for whom I have the impression that some families would be resistant because of the fact that they have to do it themselves at home. We have this culture here [in Brazil] that you take the child to a clinic and the professionals there are responsible for the child’s development . . . some parents think it’s the professional who has to do everything, that they just have to pay and the professional is the one who has to work with the child and give the developed child back. (Clinician, ID 15)
An additional concern raised by some clinicians was that parents may not understand the PACT strategies and may do something ‘wrong’ with the child: One possible risk is the parent does not do things properly at home, for example if you go to the gym and do not do the right exercise you can do harm instead of improving, but if it is done properly, ok. So, the risk is the parent looks like they learn properly but does different things at home. (Clinician, ID 12).
Theme 3: frequency of the therapy sessions may require adaptation for Brazil
Particularly relevant to the implementation of PACT in Brazil, parents and clinicians felt that weekly sessions with the PACT therapist (in contrast to the fortnightly sessions in the original PACT protocol) would be important in promoting parental engagement and understanding:
‘I think it’s good [the fortnightly sessions], but maybe there are families that will need to see the therapist every week in the beginning, to adjust their dynamics, so the family can understand better how it [PACT] works’. (Parent, ID 5).
I am wondering if fortnightly meetings wouldn’t be too infrequent. I think there is the risk of the intervention not being effective because the parents couldn’t practice 30 minutes every day during those 15 days between sessions. I think that maybe more frequent meetings in the beginning may help the therapist to feel the family’s rhythm and engagement. I think the family would not have the necessary engagement with fortnightly meetings. (Clinician, ID 13)
Stage 2: findings from the case series on the feasibility of PACT
Of the 15 families recruited to participate in the case series, two discontinued after the initial session (one due to unstable Internet preventing participation in the online sessions, one for unknown reasons); both families were assigned to receive the 12 PACT sessions over 6 months according to the original protocol. A further two families (one from each of the PACT delivery schedules) withdrew after the ninth session due to time-management difficulties, but both took part in the interview at the end of the sessions. Thus, post-intervention interviews were conducted with 13 parents. Thematic analysis of the interviews generated three themes (Figure 1).
Theme 1: parents found PACT to be a beneficial, acceptable and feasible intervention
All parents reported benefits of PACT for their child and for themselves. These included improvements in the child’s initiation of communication and increased parental understanding of the child: I thought he would never be able to initiate communication and I ended up discovering that he is able, I just needed to give him some space to feel comfortable starting some actions, but I couldn’t see it before. I also realized that he is able to interact with other children . . . I would say that before [PACT], he used to avoid contact with other children, but when I started to let him initiate interactions with me and gave him more space to do some things, he started to loosen up, not only at home with me, he started to approach other children, now I see him calling other children to play when we go out . . . (Case-series parent, ID 11)
Parents noted that receiving the intervention at home made the child feel more comfortable and saved on transportation costs and time: I thought it was great, I thought it was an excellent idea because it became part of his daily life, with own his toys, his own places, so I think it’s a great idea to do [PACT] at home. It also made my life easier because we didn’t have to leave the house, my son could explore his own things and I think I could learn better at home, I also saved more time. (Case-series parent, ID 2)
Parents considered the video-feedback strategy to be very useful: In our daily interaction I couldn’t notice some details that I could see clearly in the video. I could pay better attention to what he was looking at, if he was interested in something, if he wanted to talk, so this was very good for us, I thought the videos were great. (Case-series parent, ID 9)
Finally, most parents said that they could manage the home practice most days: I did it every day, sometimes I didn’t do it at the same time but every day we sat with him, we did some things, some activities, so it happened every day . . . sometimes it wasn’t a very structured play, but there was always this time in which we used the techniques in an interaction with him. (Case-series parent, ID 3)
Theme 2: PACT brought no harms, but there were some challenges for parents
Despite the positive experiences of receiving PACT, parents highlighted difficulties in adapting to the parent-mediated design and the home-setting. For instance, several parents experienced difficulty in managing the therapy sessions and 30 min daily practice alongside their other daily-life demands, especially for parents in employment and with other children: ‘I think the only obstacle was to manage my other children’ (Case-series parent, ID 4). These difficulties were particularly marked in the two families who discontinued PACT after the ninth session: I couldn’t manage it [the home-practice] every day because of the daily rush, but I think it’s very important if parents could do it every day. My obstacles were the housework, things I had to do outside the house, appointments, things like that. . . I could practice 3-4 times a week with her, but I know we would have even better results if I had practiced every day. (Case-series parent, ID 12, discontinued after session 9)
Another challenge for several parents was feeling unsure at the beginning about what PACT would involve and insecure about their capabilities to implement the intervention with their child: I think the biggest challenge was at the beginning to understand how the intervention would be, I was wondering if I was going to learn, I was nervous at first about how to decrease my anxiety when interacting with him, but then I saw that I was capable. (Case-series parent, ID 2)
One parent also reported challenges in finding an appropriate place in the home to conduct the therapy: My biggest difficulty was to find the best place in the house, for example, we started doing it in a large and open room, but then we discussed with the therapist and found out that it would be better to do it in a smaller room, with more restricted space with the door closed without much external sound from the house because I couldn’t keep his attention in a larger environment with other people and noises. (Case-series parent, ID 10).
Theme 3: parents recommended adaptations to the frequency of therapist sessions and initial introduction of PACT
Most parents considered fortnightly meetings with the therapist to be feasible and they noted changes in their child’s behaviour between sessions of this frequency. However, some parents believed that weekly sessions would make them more engaged and more likely to complete the daily practice: When you have this 15-day break you end up getting lost in the organization because you have a lot of time to practice. . .sometimes I realized it was almost close to the next session and I hadn’t practiced with him . . . I noticed that I dedicated myself more when the next session was close. So weekly sessions may give the impression that you don’t have much time to lose, it would probably make me dedicate myself more. (Case-series parent, ID 4)
All parents who received the adapted schedule (4 weekly sessions followed by 8 fortnightly sessions) expressed satisfaction with this frequency, with no suggestions about the schedule, and reported believing that this was more effective than if they had received fortnightly sessions only.
Four parents suggested that an extra initial module with psychoeducational information about communication development and clearer expectations of what would be required of the parent during the intervention would make them feel less anxious at the beginning of the intervention: I think it would be good to have some initial material that explains a little more about the intervention, with some videos for parents to understand or see examples of how it works, it can make a difference, it can be important because sometimes parents have no idea, they don’t know where to start. . . (Case-series parent, ID 4)
Stage 3: adaptations to the original PACT protocol
Most Brazilian parents highlighted that they may be too busy with daily-life duties to act as their child’s therapist and are more familiar with therapist-led interventions. Parents and clinicians were concerned about parental engagement and dedication to the intervention. These concerns were partially borne out in the case series of 15 families who received PACT. Four of these families did not complete the full 12 sessions of the intervention. Further, in post-intervention interviews, some of the parents who did complete the 12 sessions reported difficulties in being disciplined to complete the daily practice between sessions and others reported that they would find it easier to take their child to a therapist. Thus, we considered it necessary to make changes to the original PACT protocol to increase parental engagement in the Brazilian context.
Expanded psychoeducational module
We followed parents’ suggestions of including a more extensive psychoeducational module at the beginning of PACT. We considered that increasing parental knowledge about and confidence in the intervention methodology would help improve engagement. An extended psychoeducational module was included in the South-Asian adaptation of PACT to train the non-specialists who delivered the intervention (Divan et al., 2015). This module from South Asia was used as the basis of the expanded psychoeducational module for Brazil. With this module, Brazilian families could learn why and how a parent-mediated intervention focused on communication skills could be effective and how they could adapt their routine and daily life duties to include practice with their child. They could also learn more about autism and communication development, since some parents also reported lack of understanding about that in themselves and even more so in other family members. The expanded psychoeducational module covered the following themes: (1) what communication is, (2) how communication skills develop, (3) communication difficulties in autistic children, (4) what PACT is and what it is not, (5) how PACT may improve the child’s communication skills and enhance parent-child communication synchrony, (6) the structure and methodology of PACT, including the frequency of the sessions, session and intervention duration, what happens in the sessions, and a discussion about how 30 min daily practice could be integrated in the family’s routine.
Altered frequency of PACT sessions
To promote parental engagement, we adapted the schedule of therapist sessions from 12 fortnightly meetings to four weekly sessions followed by eight fortnightly sessions. This decision was based on two factors. First, parents and clinicians had opposing opinions about the fortnightly sessions in all three groups interviewed. They considered that weekly sessions would facilitate engagement, but fortnightly sessions could be less overwhelming and allow the caregiver enough time to practice and see results in the next session. Second, caregivers who received the intervention reported that they felt more engaged when they saw that they were learning and their child’s play behaviour and communication skills were changing. Therefore, we considered that the first 4 weekly sessions could establish a stronger initial engagement with the caregiver and the last eight fortnightly sessions would give more time for the parent to practice each goal and see results. As reported above, this schedule showed good acceptability in the subsample of families who received it.
Real-life examples of PACT strategies
Real-life examples were included in the manual to illustrate the use of PACT strategies. Many Brazilian families reported that they often use a directive style of teaching the child, which incorporates explicit stimulation and reinforcement and frequent questions directed to the child. Parents, therefore, had difficulty in adapting their communication style to be non-directive. To help families with this, we added concrete, real-life examples (see eAppendix 4 of the Supplementary materials) of the PACT strategies in each section of the manual which the therapist can use to explain PACT strategies to parents. The examples were developed partially based on the examples used to explain the strategies to the families in the case series and partially based on examples that had been added to the protocol for the South-Asian adaptation of PACT (Divan et al., 2015).
Addressing challenges in the home environment
Many Brazilian parents reported difficulty in finding an adequate place in their home to conduct the therapy and in managing the presence of other people in the house during the sessions and practice. However, most parents were able to find an appropriate place and to implement strategies for managing household distractions via discussion and suggestions from the therapist. To ensure the therapist is aware of the need to address these issues, we highlighted in the manual that the therapist should ask about the family’s home environment in the initial session and discuss any potential difficulties in conducting the sessions and practice in the home. Some parents also reported that they could not manage the 30 min daily practice because of their busy and stressful lives. To address this difficulty, we included reminder notes in the practice programme documentation for the therapist to reinforce the idea that parents do not need to set aside 30 min of structured play to practice each day. They can instead use the intervention techniques in everyday care of the child, such as at bath-time or mealtimes.
Audio-recorded feedback and summary
While not raised by parents or clinicians, the Brazilian members of the research team highlighted that a considerable proportion of adults are illiterate in Brazil (6.6%/~11 million, Pesquisa Nacional por Amostra Domicílios, 2019). These adults would have difficulty with the written feedback and summary of practice goals that is provided to parents at the end of each therapy session. We, therefore, included optional instructions in the manual for the feedback and practice programme to be audio-recorded rather than written.
Expanded toy suggestions
All parents who received PACT highlighted the importance of being able to use their children’s own toys in their home environment. To maintain this naturalistic approach and suit the vast socioeconomic variability of Brazilian families, in the manual, we included a wider range of toy suggestions for the therapist sessions and home practice, and the possibility of using toys created by the family from household objects.
Discussion
PACT differs from other therapeutic interventions for autistic children in Brazil in that it is parent-mediated. Our qualitative findings indicated that both parents and clinicians, including parents who received PACT, considered the intervention to be acceptable, feasible and potentially beneficial in the Brazilian context, but to also present contextual challenges for implementation. Challenges mainly concerned parental engagement and understanding and integrating the intervention within parents’ busy lives and home environments. In-depth discussions of these challenges between the Brazilian researchers, members of the UK PACT consortium and researchers who implemented PACT in South-Asian LMICs resulted in a series of minor adaptations to the original PACT protocol to address the challenges. Importantly, the adaptations involved only a minor change to the frequency of PACT sessions and the expansion of information already present in the PACT protocol to pre-emptively address parental concerns. As such, we are confident that these adaptations did not affect the core principles or practices of PACT and that the model will be preserved in this new LMIC context.
Indeed, our findings from the qualitative post-PACT interviews with mothers who received the intervention indicated that the parent–child dyads experienced improvements in social-communication and interaction synchrony, as have been reported in qualitative studies investigating parental experiences of receiving PACT in the United Kingdom (Leadbitter et al., 2020) and South Asia (Divan et al., 2015). Furthermore, the challenges raised by parents and clinicians in Brazil and the subsequent adaptations to the PACT protocol mirrored those in the South-Asian LMIC setting (Divan et al., 2015). For instance, like the Brazilian mothers who received PACT, parents in South-Asian LMICs described not knowing what to expect from the intervention and being sceptical about its utility (Divan et al., 2015). This prompted the expansion of the initial psychoeducational module in South Asia (Divan et al., 2015), which we have also implemented for Brazil. Other challenges that were reported in Brazil were also identified in the United Kingdom (Leadbitter et al., 2020) and South Asia (Divan et al., 2015), such as the challenge of engaging and/or finding time to complete the home practice and feeling uncertain or self-conscious in the first video-feedback sessions.
Concerning the difficulties parents reported in engaging in the home practice, the South-Asian implementation study of PACT suggested that parents became more able and willing to find time to complete the practice as the intervention progressed and they began to see changes in their child and their interactions with the child. Enhancing parental engagement and motivation may therefore be key to resolving difficulties with completing home-practice. In the Brazilian context, we hope that the adapted frequency of the therapist sessions will promote parental engagement, and consequently they may feel more motivated and able to incorporate the home-practice in their busy lives. Greater support by the therapist in helping parents integrate practice of the strategies during normal, everyday activities with the child rather than in structured play situations is also likely to help, since it may reduce the pressure on parents to carve out time to practice. Finally, recent qualitative work in Brazil suggests that some parents may be uncertain about the role of parent–child play in their child’s development and the type of play that is appropriate (Yakuwa et al., 2022). We believe that the expanded psychoeducational module at the beginning of PACT, which explains in more detail the objective and importance of the daily home-practice during playful interactions, may also help parents understand and engage with this aspect of the intervention.
In summary, the current findings indicate that the adapted PACT protocol for Brazil maintains the theoretical construct of the original intervention model, utilising a naturalistic approach to support and promote the development of communication and social interaction skills in young autistic children. We believe that these findings emphasise the utility of PACT across multiple cultural contexts. Furthermore, this intervention represents an important new therapeutic option for autistic children in Brazil.
Several limitations to this study should be noted. The study was conducted entirely online and by telephone during the COVID-19 pandemic. This brought challenges but also some benefits. For instance, it is possible that the families would have had fewer difficulties in understanding the intervention and the non-directive approach if they had met in person with the therapist. There were also practical challenges. For example, during the online PACT sessions, the parent was requested to properly position the computer or cell phone camera to obtain a clear view of the parent and child. The therapist then recorded the parent–child play interaction via the video call programme that was used to deliver the session. Next, the therapist shared her screen with the parent via the video call programme and they watched the video of the interaction together. This was followed by the feedback procedure, as in face-to-face delivery of the intervention. Although the video-feedback process occurred in a similar way to face-to-face intervention, it seemed to be more difficult in the online procedure to prevent interruptions and distractions the video-feedback. In some moments, it seemed to be challenging or stressful for the parent to maintain full attention to the video-feedback while taking care of the child’s needs in the home. This in turn could have affected the way the parent received and responded to the therapist’s non-directive comments and the acceptability of the intervention. Green, Leadbitter, Ellis, et al. (2022) also reported challenges in delivering PACT online, with possible effects on the intervention outcomes. On the other hand, online delivery made it easier for parents to fit the intervention into their daily schedule and enabled families who live outside São Paulo to receive the intervention, although Internet issues prevented the participation of some families who live in more extreme socioeconomic vulnerability. Since the study was conducted during the COVID-19 pandemic, participating families were likely experiencing elevated stress and anxiety levels. The fact that many parents were working from the home may have helped or hindered their motivation and capacity to engage with the intervention. We believe that online delivery of PACT is viable for Brazil, but that in-person delivery of the intervention should also be tested as a next step to determine the utility of the intervention for families who cannot participate online. We note, however, that online delivery of PACT has been achieved in very low-income settings in New Delhi in an ongoing RCT of the adapted intervention model for South Asia (https://doi.org/10.1186/ISRCTN21454676).
A related issue is that the qualitative interviews with parents and clinicians concerning the feasibility and acceptability of PACT were conducted immediately prior to and during the first few months of the pandemic (January–August 2020). At that time, the move to telehealth was underway but not well-established and many people held the view that ‘things would return to normal’ in a matter of months, including in-person treatments. Therefore, the intervention was not presented to these participants as being delivered only in an online format, as it was delivered to the case series. This difference in how PACT was presented to the first sample of parents and clinicians versus the experience of the case-series parents in receiving the intervention may have influenced perceptions of the feasibility and acceptability of PACT. While the case-series parents reported very similar perceptions of PACT to the parents and clinicians despite receiving it online, this aspect of the study should be considered while interpreting the findings.
The study was conducted largely in the state of São Paulo, the main economic and industrial centre of Brazil. São Paulo was selected partly for practical reasons since this is where the research team is based, and also because it is the most populous state in Brazil which receives the largest number of people arriving to work and live from other states in the country. While São Paulo varies widely in socioeconomic conditions and cultural diversity, it does not represent all of the cultural diversity in Brazil, a country of continental size. Families living in rural areas of the country undoubtedly have different life experiences, beliefs and needs to those in São Paulo. Future research should include families from other regions of Brazil. It should also be noted that the families participating in the case series were of mid-to-high socioeconomic status. PACT should be tested in a broader sociodemographic in Brazil.
Conclusion
This implementation study demonstrated the acceptability of a culturally-adapted version of the parent-mediated PACT intervention for use with autistic children in Brazil. The main adaptations addressed Brazilian families’ unfamiliarity with parent-mediated rather than therapist-led interventions, difficulties related to busy and cramped or noisy home environments, and challenges in understanding non-directive social communication, all of which were reported to reduce parental engagement and/or comprehension of the intervention. In view of the potential benefits of PACT for the Brazilian public health system, our next efforts involve testing the efficacy of the adapted intervention in a large-scale RCT and assessing its effectiveness in a real-life clinical setting, specifically in our publicly accessible psychiatric institute in São Paulo. This study also highlights the importance of conducting implementation research before using an autism or child development intervention in a new country or context.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221144501 – Supplemental material for Acceptability and feasibility of a parent-mediated social-communication therapy for young autistic children in Brazil: A qualitative implementation study of Paediatric Autism Communication Therapy
Supplemental material, sj-docx-1-aut-10.1177_13623613221144501 for Acceptability and feasibility of a parent-mediated social-communication therapy for young autistic children in Brazil: A qualitative implementation study of Paediatric Autism Communication Therapy by Priscilla Brandi Gomes Godoy, Lorna McWilliams, Leticia Rodrigues da Silveira, Mirian de Cesaro Revers Biasão, Fernanda Speggiorin Pereira Alarcão, Leonardo Seda, Renata Generoso Campoli, Holan Liang, Gauri Divan, Kathy Leadbitter, Jonathan Green and Elizabeth Shephard in Autism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E.S. was supported by a Young Investigator award from the São Paulo Research Foundation (FAPESP, grant number 2020/05964-1)
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.