
Abstract
Children with autism spectrum disorder (ASD) are often placed in inclusive mainstream education (ME) or exclusive special education (SE) settings. While ME settings usually offer less-intensive and structured intervention programs than SE settings, they offer more exposure to typically developing peers. A total of 121 children (2–5 years old) with ASD, 85 in SE and 36 in ME, completed two Autism Diagnostic Observation Schedule, 2nd edition (ADOS-2) assessments. Repeated-measures analysis of covariance (ANCOVA) analyses were used to assess longitudinal changes in ADOS-2 calibrated severity scores (CSS) and language production (estimated from the ADOS-2), while accounting for baseline cognitive scores, age of diagnosis, and parent-reported intensity of intervention. Longitudinal changes in ADOS CSS did not differ significantly across educational settings but were strongly associated with the age of diagnosis, demonstrating that children diagnosed earlier improved more regardless of educational settings. These findings suggest that children with ASD placed in SE and ME exhibit similar longitudinal changes in core ASD symptoms. Further studies comparing additional outcome measures such as cognitive abilities and adaptive behaviors are highly warranted for establishing placement recommendations and public health policies.
Lay abstract
Today, children with autism spectrum disorder (ASD) are placed in mainstream or special education settings somewhat arbitrarily with no clear clinical recommendations. Here, we compared changes in core ASD symptoms, as measured by the Autism Diagnostic Observation Schedule, 2nd edition (ADOS-2) clinical assessment, across ASD preschool children placed in special or mainstream education. Longitudinal changes in ADOS-2 scores did not differ significantly across settings over a 1- to 2-year period. While some children improved in core ASD symptoms, others deteriorated in both settings. This highlights the need to identify specific criteria for establishing meaningful placement recommendations.
Keywords
Introduction
In most western countries, children with autism spectrum disorder (ASD) are placed in government-funded educational settings from an early age. These settings are heterogeneous and range from exclusive special education (SE) to inclusive mainstream education (ME) settings. In SE settings, small groups of children with ASD often receive intensive, structured, and specialized care from a relatively large staff of SE professionals and therapists. These children, however, are often excluded from interactions with typically developing peers since SE settings are often physically separated from ME settings. In contrast, children with ASD placed in inclusive ME receive considerably less specialized care but have the opportunity to learn social skills through daily interactions with their typically developing peers.
The potential benefits and morality of placing children with ASD in either educational settings is a topic of ongoing debate (Ravet, 2011). Some have argued that including children with ASD in ME and enabling them to interact with their typically developing peers is a basic human right (Allan, 2007; Pellicano et al., 2018). Others have posited that ME settings do not address the needs of children with ASD who may require specialized care to thrive (Mesibov & Shea, 1996; Waddington & Reed, 2017). To date, this debate has mostly been based on moral and theoretical arguments rather than empirical evidence regarding the outcome of children with ASD placed in either setting (Ravet, 2011).
Several previous studies have assessed longitudinal changes in the development of children with ASD in specific educational settings. Some have reported that children with ASD placed in SE settings exhibit significant improvement in cognitive and social abilities, as well as adaptive skills (Harris et al., 1991; Rogers & Vismara, 2008; Talbott et al., 2016; Zachor et al., 2007; Zachor & Itzchak, 2010). Others have reported that children placed in ME show significant improvements in adaptive behaviors, communication levels, and language and academic skills (Harrower & Dunlap, 2001; Little, 2017; Stahmer et al., 2011). However, these studies did not compare children across educational settings.
Only a handful of studies to date have directly compared the longitudinal development of children with ASD in special versus ME. One study of 97 children with ASD, 4–16 years old (mean age 8.5), reported that children in both educational settings improved similarly in overall adaptive behavior scores as assessed by the Vineland, while children in SE made greater improvements in conduct and socialization (Reed et al., 2012). Another study of 108 children with ASD, 5–18 years old (mean age 12.9), reported that children placed in SE settings performed better in academic language tests than those placed in ME (Waddington & Reed, 2017). In contrast, a third study with 98 young children (mean age 3.2 years old) reported that children placed in ME showed greater gains in cognitive scores than those placed in SE, particularly if they exhibited more severe initial social impairments (Nahmias et al., 2014). Finally, a recent randomized control trial (RCT) study that implemented the Early Start Denver Model (ESDM) intervention in inclusive and SE preschools, reported that children aged 15–32 months old in both settings showed similar improvement in language, social interaction, cognition, adaptive behaviors, and autism symptoms, irrespective of educational setting (Vivanti et al., 2019).
These limited and ambiguous findings demonstrate the scarcity of empirical data regarding outcome of children with ASD placed in different educational settings. Note that data are particularly lacking for preschool children and that none of the studies listed above examined longitudinal changes in core ASD symptoms using standardized assessments.
Here, we examined longitudinal changes in core ASD symptoms of 16- to 59-month-old children with ASD, initially placed in either special or ME. The severity of ASD symptoms was assessed with the Autism Diagnostic Observation Schedule, 2nd edition (ADOS-2) using the calibrated severity scores (CSS) at diagnosis, and again 12–24 months later. The ADOS-2 CSS are specifically designed to enable assessment of longitudinal changes regardless of the changing age and language abilities of the children across timepoints.
Methods
Participants and procedure
This study examined longitudinal data collected at the Azrieli National Center for Autism and Neurodevelopment Research (ANCAN) in Israel. ANCAN is located inside Soroka University Medical Center (SUMC) where approximately 150 children are diagnosed with ASD annually. SUMC is the only clinical center where children insured by the Clalit HMO (who cover 70% of the population in southern Israel) can receive an ASD diagnosis, thereby yielding a representative community sample of this geographical area (Dinstein et al., 2020; Meiri et al., 2017). We extracted a convenience sample of 121 children (91 boys) from the ANCAN database that included all children who were diagnosed with ASD between 2015 and 2019, were younger than 5 years old at the time of diagnosis, and completed an ADOS-2 assessment (Lord et al., 2012) at diagnosis (Time 1) and again 12–24 months later (Time 2). All participating children were diagnosed with ASD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria by a developmental psychologist and either a child psychiatrist or pediatric neurologist. In addition, 112 of the children (92.5%) completed cognitive assessments at diagnosis (Table 1). The remaining 9 children did not complete cognitive testing because they were not cooperative. Finally, parents of all children completed a follow-up questionnaire regarding educational placement and the quantity of occupational therapy, speech therapy, physiotherapy, and emotional treatments that the child had received since diagnosis. Of this sample, 36 children were placed in inclusive education settings and 85 children were placed in SE settings. Parents of all children signed an informed consent form, and the study was approved by the local Helsinki committee. There was no community involvement in the study.
Characteristics of children in the entire sample, separated according to their placement in ME or SE settings.
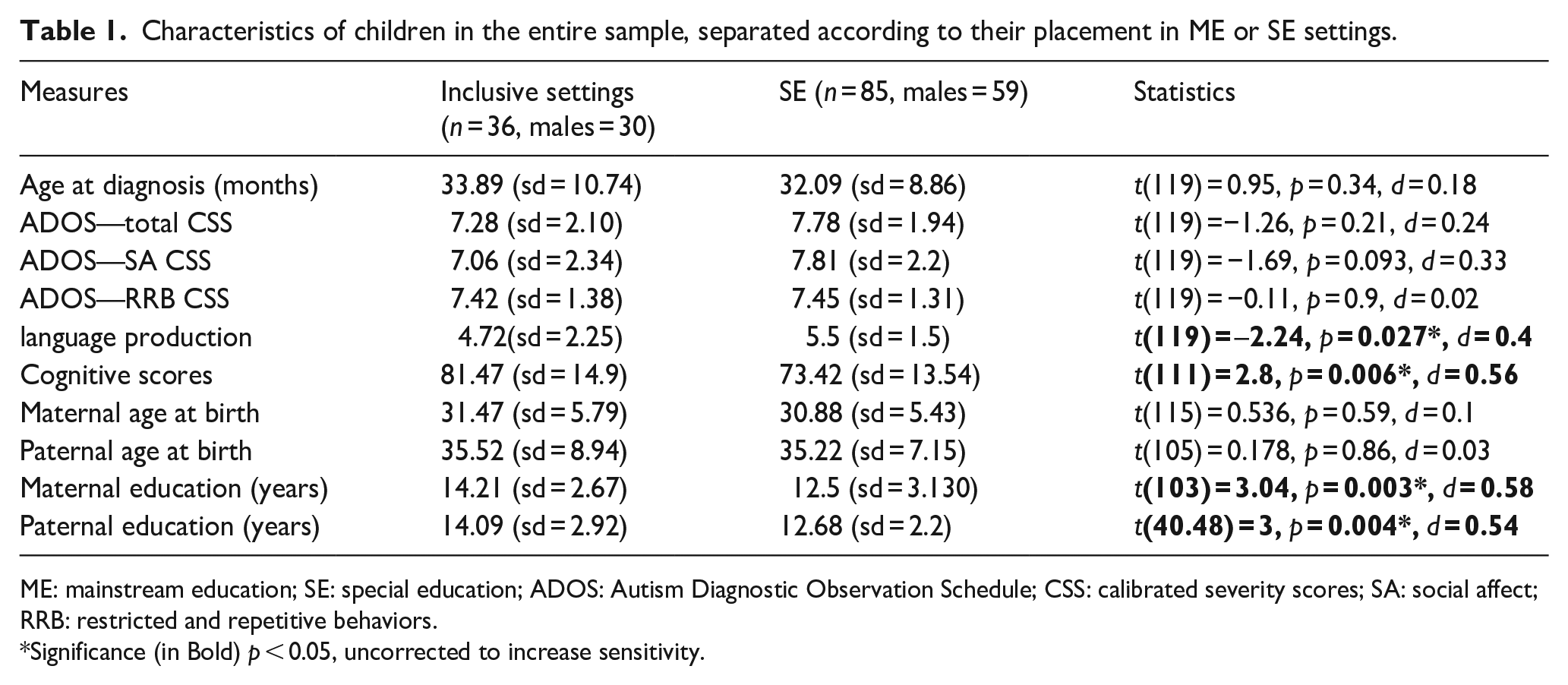
ME: mainstream education; SE: special education; ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity scores; SA: social affect; RRB: restricted and repetitive behaviors.
Significance (in Bold) p < 0.05, uncorrected to increase sensitivity.
Measures
ADOS-2
The ADOS-2 is a semi-structured evaluation of core ASD symptoms (Lord et al., 2012). Children completed the toddler module or modules 1–3 of the ADOS-2, according to their age and language abilities. The evaluation was performed by a research-reliable clinician with over 5 years of experience in ASD diagnosis. The ADOS-2 scoring system enables transformation of raw scores into CSS, which allows comparison of ASD severity across children of different ages and language capabilities and across timepoints (Esler et al., 2015; Gotham et al., 2009). ADOS-2 CSS were computed separately for each of the two core ASD symptom domains; social affect (SA), and restricted and repetitive behaviors (RRBs) (Esler et al., 2015; Hus et al., 2014).
Cognitive assessments
Younger children completed the Bayley Scales of Infant and Toddler Development, third edition (Bayley, 2006), suitable for children ages 1–42 months old. Older children completed the Wechsler Preschool and Primary Scale of Intelligence, third edition (WPPSI; Wechsler, 2002), suitable for children ages 2.6–7.3 years old. Since Bayley cognitive scores exhibit strong correlations with general intelligence WPPSI scores (Bayley, 2006; Bode et al., 2014) and both tests yield equivalent standardized scores with a mean of 100 and a standard deviation of 15, we combined scores from the two assessments in all analyses.
Language production
Spoken language ability was evaluated using ADOS item A1, which is not incorporated into the ADOS CSS scores. The A1 item evaluates the spoken language abilities of the child using a scale that differs across ADOS modules. In module 1 and the toddler module, this item scores language abilities from no spoken language to using pairs of words, in module 2 from single words to combinations of three or more words, and in module 3 from combinations of 2–3 words to complex sentences. We used the coding system developed by Visser et al. (2017) to create a common 8-point scale across modules with the following criteria:
0: Children used sentences in a largely correct fashion (complex utterances with >2 clauses)
1: Children exhibited relatively complex speech (occasional utterances with >2 clauses) with recurrent grammatical errors.
2: Children exhibited non-echoed speech with utterances of >3 words.
3: Children mainly used individual 2- to 3-word phrases, with or without minimal grammar.
4: Children mainly used individual words with occasional simple phrases.
5: Children only used individual words (minimum of 5 different words).
6: Children only used echoed speech (<5 words).
7: No language production at all.
Follow-up questionnaire
Parents completed a follow-up questionnaire that included questions about the type and number of treatments that their child received since the time of diagnosis, and their child’s educational setting.
Data analysis and statistics
All analyses were performed using IBM SPSS (version 23). Independent sample t-tests and paired sample t-tests were used to compare continuous variables (e.g. age at diagnosis) across children in ME and SE settings. Mann–Whitney U-tests were used to compare categorical variables across groups. Chi-square tests were performed to compare the distribution of nominal variables across timepoints, and Pearson’s correlations were used to assess the relationship between age at diagnosis and changes in ADOS CSS over time. A repeated-measures analysis of covariance (ANCOVA) was preformed to compare longitudinal changes across educational settings. This analysis was carried out with ADOS CSS and language production scores as dependent variables. Age at diagnosis, cognitive scores at diagnosis, number of treatment hours per week, and the length of interval between diagnosis and follow-up were included as covariates. In all cases, alpha was set to 0.05. All analyses were performed twice, once with the entire sample and again with matched sub-groups (see Results).
Matched sub-groups
To further enable a fair comparison of longitudinal changes across educational settings, we also performed several of the analyses with a sub-sample of 27 pairs of children (i.e. 27 children from each educational setting) who were tightly matched for age at diagnosis (±4 months), initial cognitive scores (±5 points and within the same cognitive category), initial ADOS CSS (same module and ±1 CSS points), and initial language production score (±1 point).
Results
In line with national reports from the Israeli Ministry of Education regarding placement of children with ASD (Weisbly, 2015), approximately one-third of the children in our sample were placed in ME and two-thirds were placed in SE (Table 1). Parental reports revealed that children in SE received, on average, twice as many personal (one-on-one) hours of intervention per week (M = 4.22, SD = 2.55) in comparison to children in ME (M = 2.2, SD = 1.35). This difference was highly significant with a large effect size (t(119) = –5.6, p < 0.0001, d = 0.98).
Sample characteristics at diagnosis
Most characteristics of children with ASD who were placed in SE did not differ significantly from those of children placed in ME (Table 1). This was true for the age at diagnosis (t(119) = 0.955, p = 0.34), total ADOS CSS (t(119) = −1.26, p = 0.21), ADOS SA CSS (t(119) = −1.7, p = 0.09), and ADOS RRB CSS (t(119) = −0.1, p = 0.9). Hyper-activity (U(120) = 1279.5, p = 0.16), disruptive behavior (U(120) = 1438, p = 0.54), and anxiety (U(120) = 1362, p = 0.11) as measured by specific ADOS-2 items (see Methods) also did not differ significantly across groups. However, children placed in ME exhibited significantly higher initial cognitive (t(111) = 2.8, p = 0.006, d = 0.56) and spoken language (t(119) = –2.24, p = 0.027, d = 0.4) abilities.
Parental age at the time of the child’s birth did not differ across groups for mothers (t(115) = 0.54, p = 0.59) or fathers (t(105) = 0.18, p = 0.86), but parents of children placed in ME had significantly more years of education as reported by mothers (t(103) = 3, p = 0.003, d = 0.58) and fathers (t(40.48) = 3.03, p = 0.004, d = 0.54).
To ensure that our longitudinal comparisons were not biased by initial differences across educational settings, we also performed several analyses with a sub-sample of 27 pairs of children, one from each group, who were matched for age at diagnosis, initial cognitive scores, initial ADOS CSS, and initial spoken language abilities (see Methods). These matched sub-groups did not differ significantly on any of the examined variables (Table 2).
Characteristics of children in the matched sub-groups.
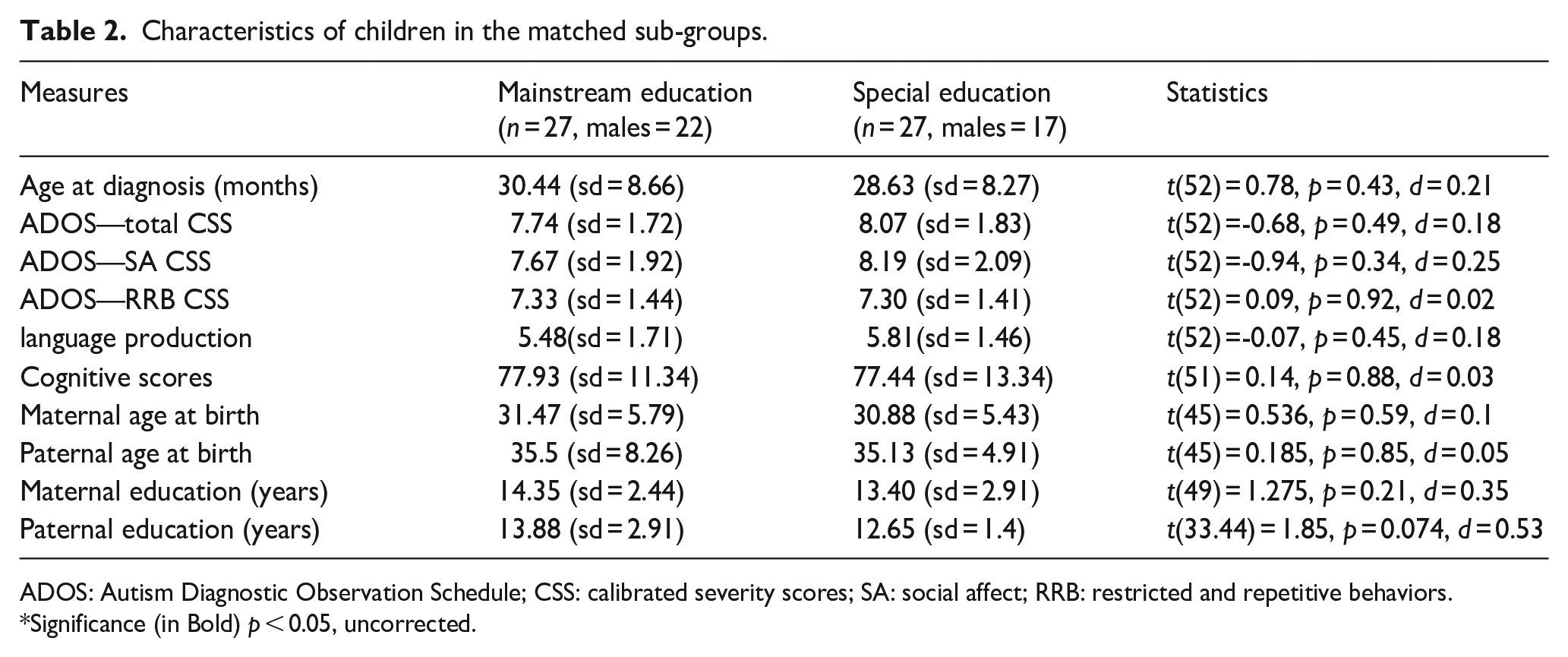
ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity scores; SA: social affect; RRB: restricted and repetitive behaviors.
Significance (in Bold) p < 0.05, uncorrected.
Longitudinal changes in ASD symptom severity
We first quantified the proportion of children in each educational setting who exhibited changes in ASD symptom severity that were larger than one ADOS-2 CSS point. This corresponds to half a standard deviation in our sample (Table 1), a threshold commonly considered to represent significant change (Norman et al., 2003). Similar proportions of children exhibited improvements in their ADOS CSS in both educational settings. Approximately 61% of children placed in ME and 52% of children placed in SE showed a decrease that was larger than one ADOS-2 CSS point (χ2 (121) = 0.683, p = 0.41).
Assessing the overall magnitude of change over time revealed that the children improved (i.e. decreased) in their ADOS-2 CSS scores in both ME (t(35) = 3.071, p = 0.004) and SE (t(84) = 3.398, p = 0.001) settings (Figure 1). These improvements were driven by improvements in the ADOS-2 SA CSS in both ME (t(35) = 3.851, p < 0.001) and ME (t(84) = 4.138, p < 0.001) settings. ADOS-2 RRBs CSS did not change significantly in either ME (t(35) = 0.621, p = 0.54) or SE (t(84) = -0.978, p = 0.33) settings.
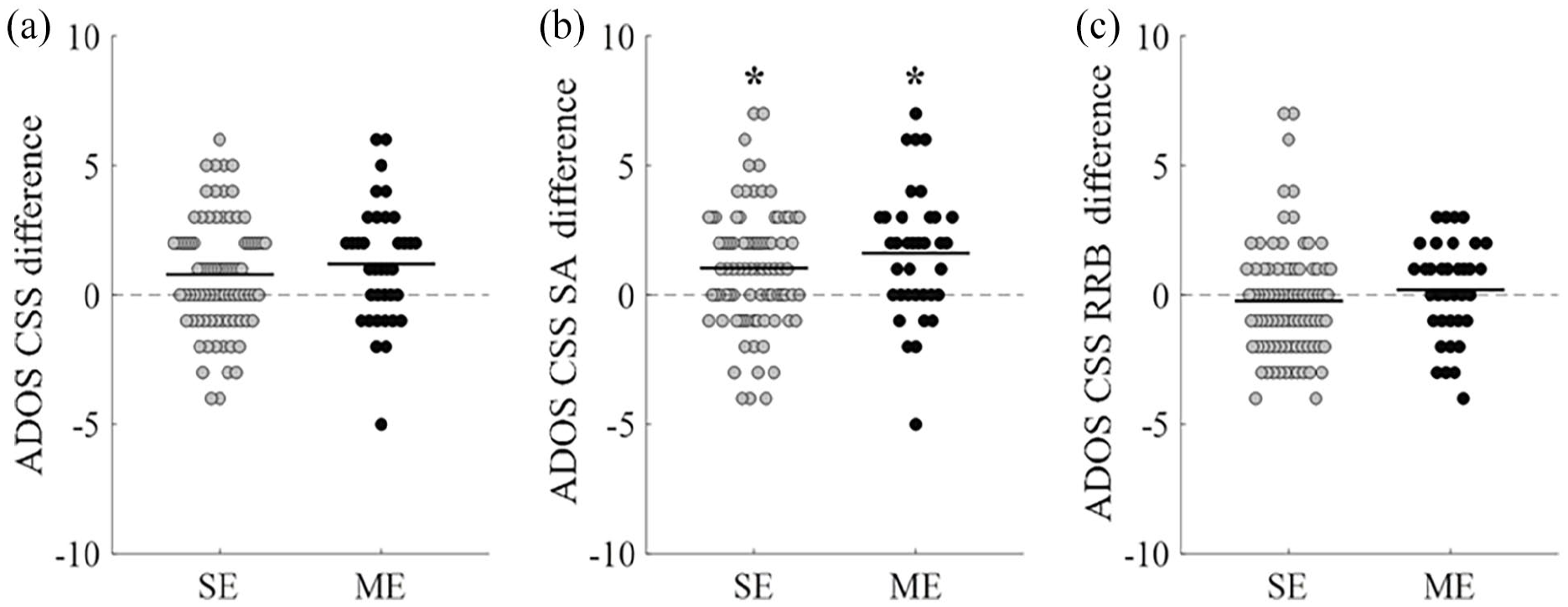
Longitudinal changes in ASD symptoms severity. Bee swarm plots of longitudinal changes in ADOS CSS in children with ASD placed in SE (gray) or ME (black) settings. (a) Change in ADOS CSS (Time1—Time2). Note that positive change values indicate improvements (i.e. reduction in ADOS scores) over time. (b) Change in ADOS SA CSS. (c) Change in ADOS RRB CSS. Each point represents a single child. Horizontal lines represent the group mean.
Similar findings were also apparent when examining the matched sub-sample. A significant decrease in ADOS-2 CSS scores was apparent in both ME (t(26) = 4.075, p < 0.001) and SE (t(26) = 2.691, p = 0.012) settings. Here, too, improvements were driven by a decrease in the ADOS-2 SA CSS in both ME (t(26) = 4.786, p < 0.001) and SE (t(26) = 2.691, p = 0.012) settings. In the matched sample, however, children in SE exhibited a significant increase (deterioration) in the severity of RRB symptoms (t(26) = -2.185, p = 0.038) while children in ME did not (t(26) = 0.108, p = 0.915) .
We performed a repeated-measure ANCOVA to compare longitudinal changes across the two educational settings, while accounting for several potentially confounding variables (see Methods). This analysis revealed that changes in ADOS-2 CSS did not differ significantly across educational settings (f(107,1) = 0.88, p = 0.35). Potential confounding variables including initial cognitive scores, the time interval between diagnosis and follow-up, and the amount of treatment that the children received were not significantly associated with longitudinal changes in ADOS-2 CSS (Table 3). However, a highly significant interaction was found between the age at diagnosis and the magnitude of longitudinal change in ADOS-2 CSS (f(107,1) = 15.9, p < 0.0001), demonstrating that children who were diagnosed earlier exhibited larger improvements in ADOS-2 CSS over time regardless of educational setting.
Longitudinal changes in ADOS-2 across children placed in ME and SE settings.
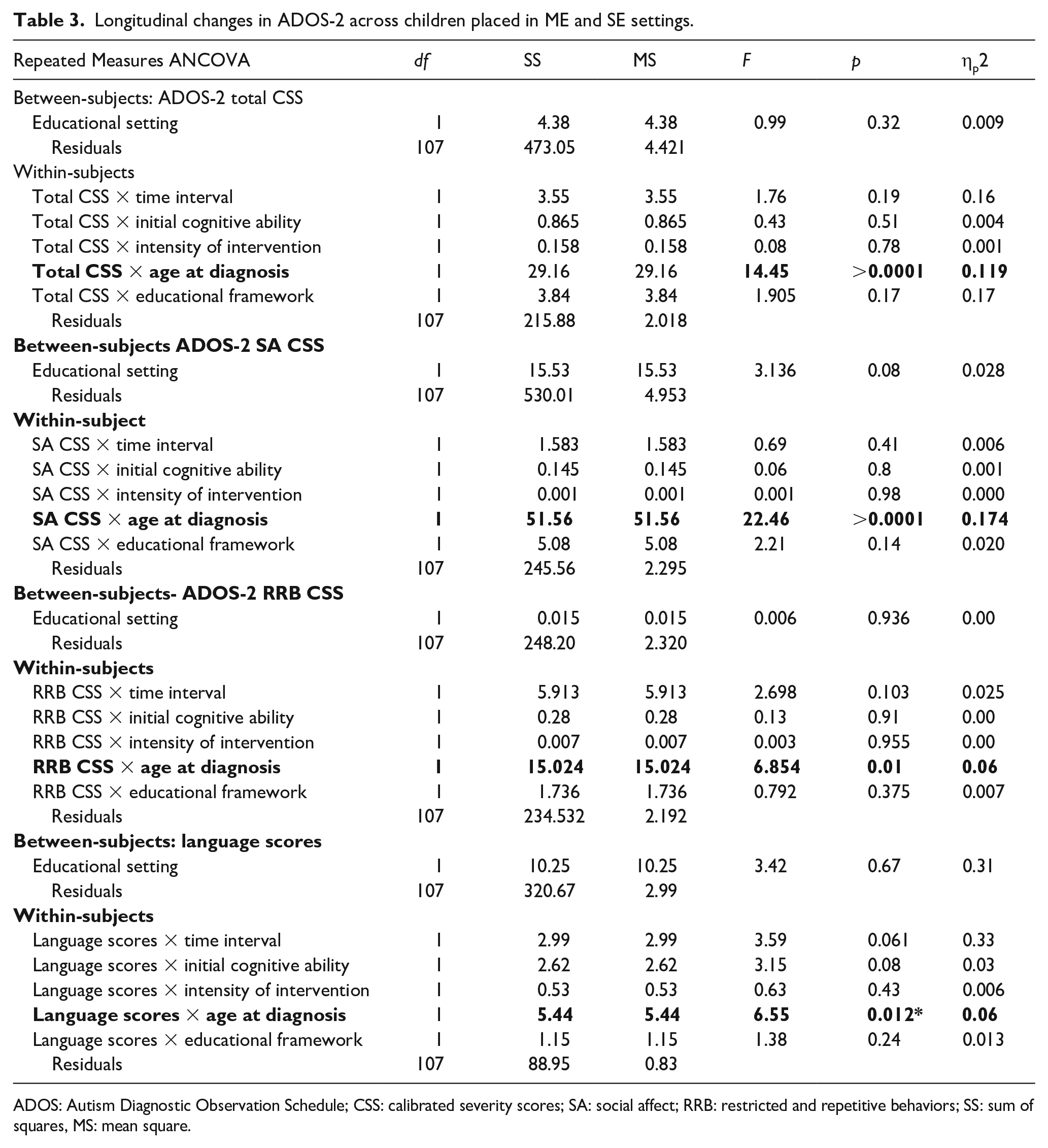
ADOS: Autism Diagnostic Observation Schedule; CSS: calibrated severity scores; SA: social affect; RRB: restricted and repetitive behaviors; SS: sum of squares, MS: mean square.
Performing the same analysis with ADOS-2 SA CSS as the dependent variable, revealed a trend for a difference across groups (f(107,1) = 3.05, p = 0.08), suggesting that children placed in ME improved in social symptoms slightly more than children in SE settings. In addition, there was a highly significant interaction between age at diagnosis and change in ADOS-2 SA CSS over time (f(107,1) = 26.65, p < 0.0001) indicating that children who were diagnosed earlier exhibited larger improvements specifically in ADOS-2 SA CSS. ADOS-2 RRB CSS changes did not differ significantly across groups (f(107,1) = 0.006, p = 0.93), but again there was an interaction between age of diagnosis and change in ADOS-2 RRB CSS over time (f(107,1) = 6.85, p = 0.01).
Table 3 Results of repeated-measures ANCOVAs comparing changes in ADOS-2 total, SA, and RRB CSS as well as language production scores across children placed in ME and SE settings. Covariates included age at diagnosis, initial cognitive ability, hours of intervention, and time interval between ADOS assessments. Significant findings are marked in bold and with asterisks, p < 0.05.
Longitudinal changes in language production abilities
One way of quantifying changes in language production is by comparing the percentage of children who transitioned from an assessment with an ADOS module requiring less verbal fluency to a module requiring more verbal fluency. Children who transitioned from the toddler’s module to module 2 or 3, those who transitioned from module 1 to module 2 or 3, and those who transitioned from module 2 to module 3 were all counted as demonstrating improvement in language production abilities (Figure 2).
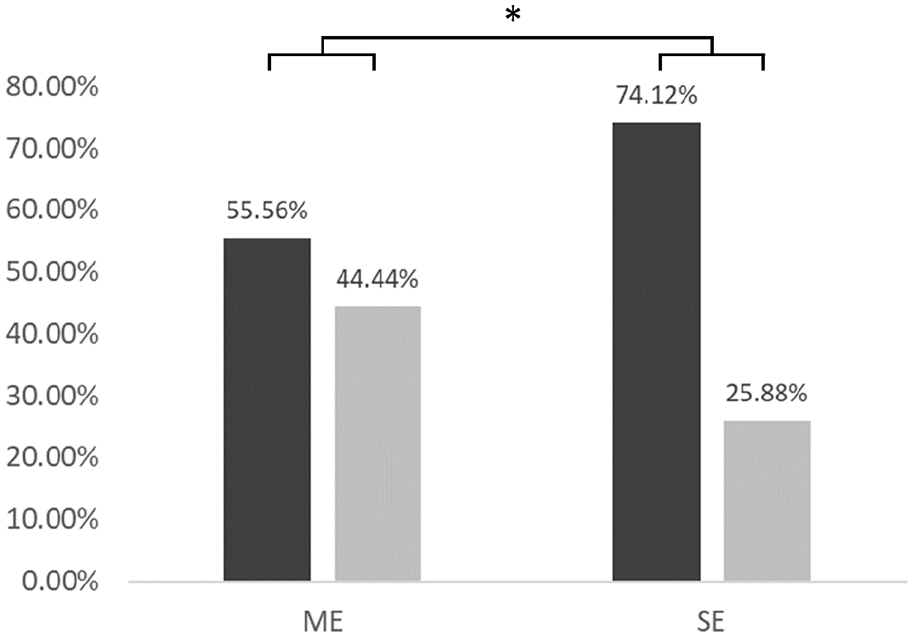
Transition to ADOS module requiring higher language abilities. Bar graph presenting the percent of children who transitioned to an ADOS module requiring higher language production abilities in ME versus SE settings.
A significantly larger proportion of children in ME transitioned to an ADOS module requiring higher language production abilities relative to children in SE (χ2 (121) = 4.045, p = 0.044). This difference was also significant when examining the matched groups (χ2 (54) = 4.207, p = 0.04).
We also performed a more refined comparison of changes in language production skills, using the coding system developed by Visser et al. (2017), which uses information from the A1 item of the ADOS that quantifies language production abilities in each of the modules (see Method section). This comparison revealed that language production scores improved similarly in children placed in ME (mean change = −1.61, SD = 1.52, t(35) = 6.37, p < 0.0001, d = 0.73) and SE (mean change = −1.24, SD = 1.21, t(84) = 9.40, p < 0.0001, d = 0.74) settings. Similar improvements were also apparent in the matched sub-groups in ME (mean change = −1.85, SD = 1.56, t(26) = 6.16, p < 0.0001, d = 0.95) and SE (mean change = −1.22, SD = 1.37, t(26) = 4.64, p < 0.0001, d = 0.75) settings (Figure 2). These longitudinal changes in spoken language scores did not differ significantly across children placed in ME and SE when examining the entire sample (t(119) = 1.44, p = 0.15) or matched sub-groups (t(52) = 1.576, p = 0.12) (Figure 3).
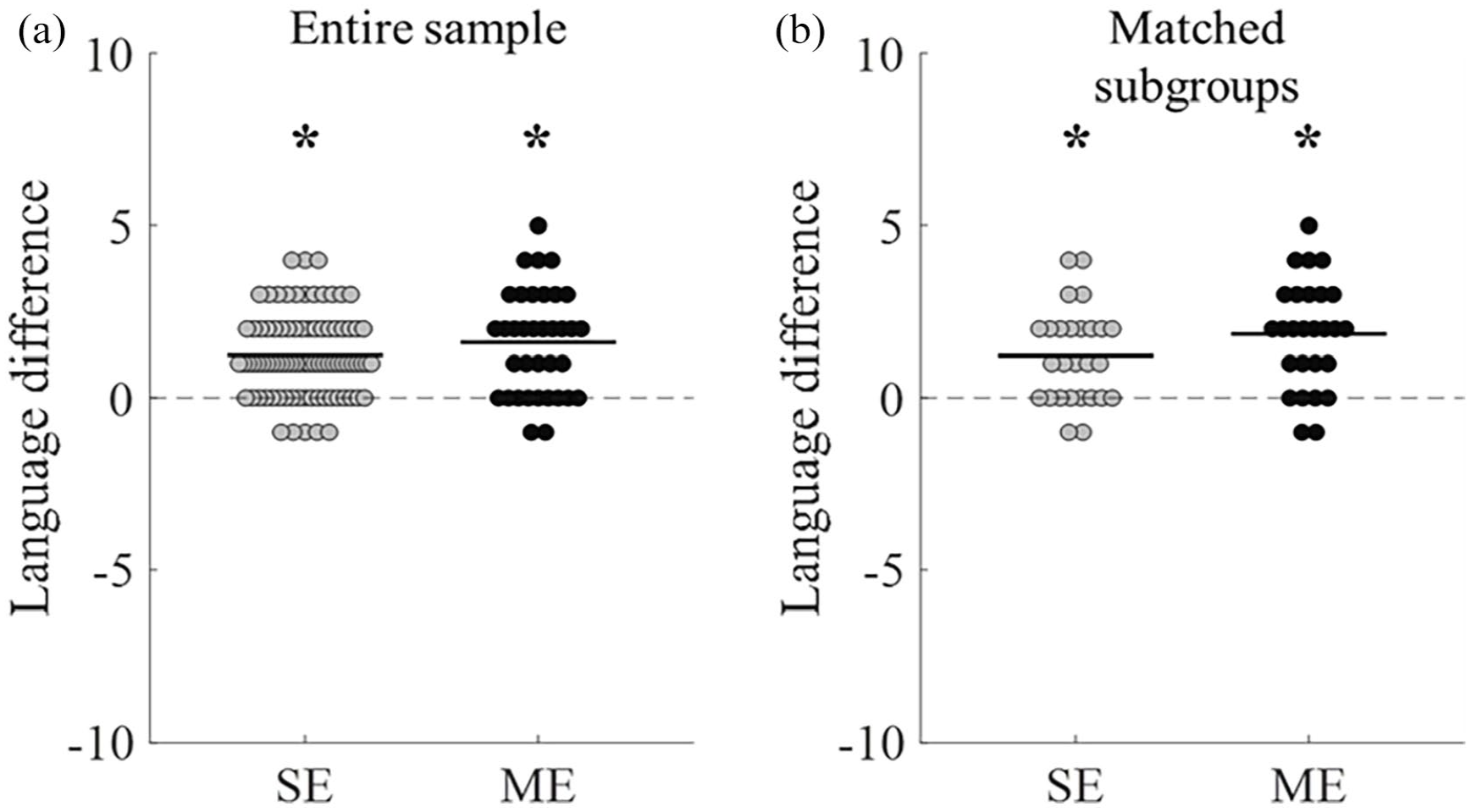
Longitudinal changes in language production. Bee swarm plots of longitudinal changes in language production scores (Time 1–Time 2). Comparison of children with ASD placed in SE (gray) and ME (black) when examining the entire sample (a) or matched sub-groups (b).
We also performed a repeated-measures ANCOVA with language scores as the dependent variable (Table 3). There were no significant differences across groups (f(107, 1) = 3.422, p = 0.67) and no significant interactions with any of the other variables, except for age at diagnosis (f(107, 1) = 6.55, p = 0.012). This demonstrates that children diagnosed earlier exhibited larger improvements in language production over time.
Age at diagnosis and changes in ADOS-2 CSS over time
Significant negative correlations were apparent between the age at diagnosis and changes in the total ADOS CSS for children in ME (r(36) = −0.449, p = 0.006) and SE (r(85) = −0.32, p = 0.003) settings. These correlations were driven by correlations in ADOS SA CSS in the ME (r(36) = −0.55, p = 0.001) and SE (r(85) = −0.362, p = 0.001) settings. Correlations with ADOS RRB CSS exhibited nonsignificant trends in the opposite direction in ME (r(36) = 0.259, p = 0.128) and SE (r(85) = 0.191, p = 0.08) settings (Figure 4).
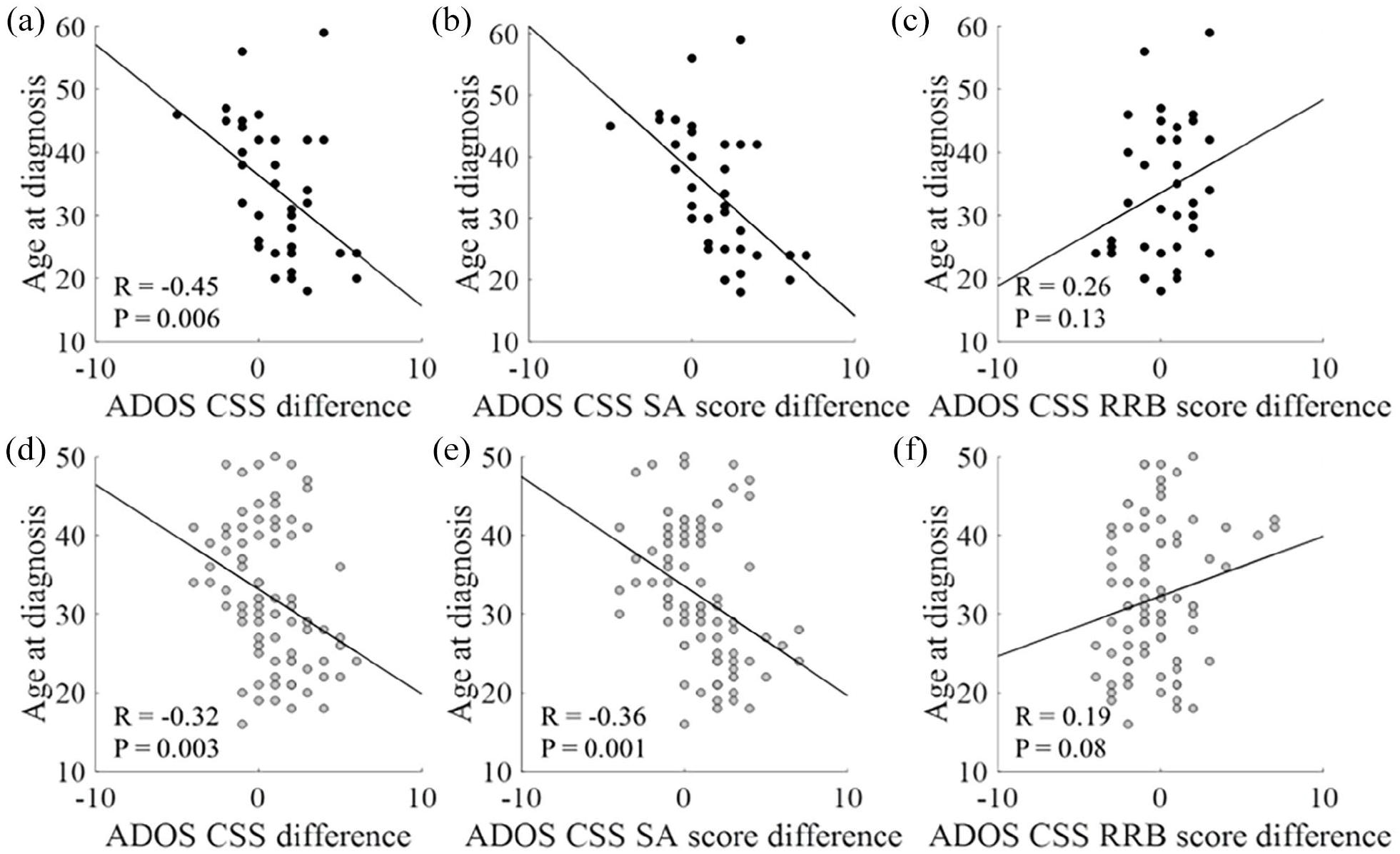
Correlations between changes in ADOS-2 CSS and age at diagnosis. Scatter plots demonstrating the correlations between changes in ADOS-2 CSS and age at diagnosis for children placed in ME (black) or SE (gray) settings. (a, d): Total ADOS-2 CCS. (b, e): SA CSS. (c, f): RRB CSS. Pearson correlation coefficients and corresponding p values are presented in each panel.
Initial cognitive abilities and changes in ADOS-2 CSS over time
In line with the repeated-measures ANCOVA analyses, we did not find any significant correlations between initial cognitive abilities and changes in the total ADOS-2, SA, or RRB CSS of children in ME (total CSS: r(34) = −0.11, p = 0.51; SA CSS: r(34) = −0.19, p = 0.28; RRB CSS: r(34) = −0.05, p = 0.78) or SE (total CSS: r(78) = 0.03, p = 0.76; SA CSS: r(78) = 0.01, p = 0.95; RRB CSS: r(78) = 0.01, p = 0.91) settings (Figure 5). Moreover, children with an initial cognitive score <70 did not differ significantly from children with an initial cognitive score >70 in their total ADOS-2 CSS changes over time (t(111) = −0.49, p = 0.62, d = −0.10).
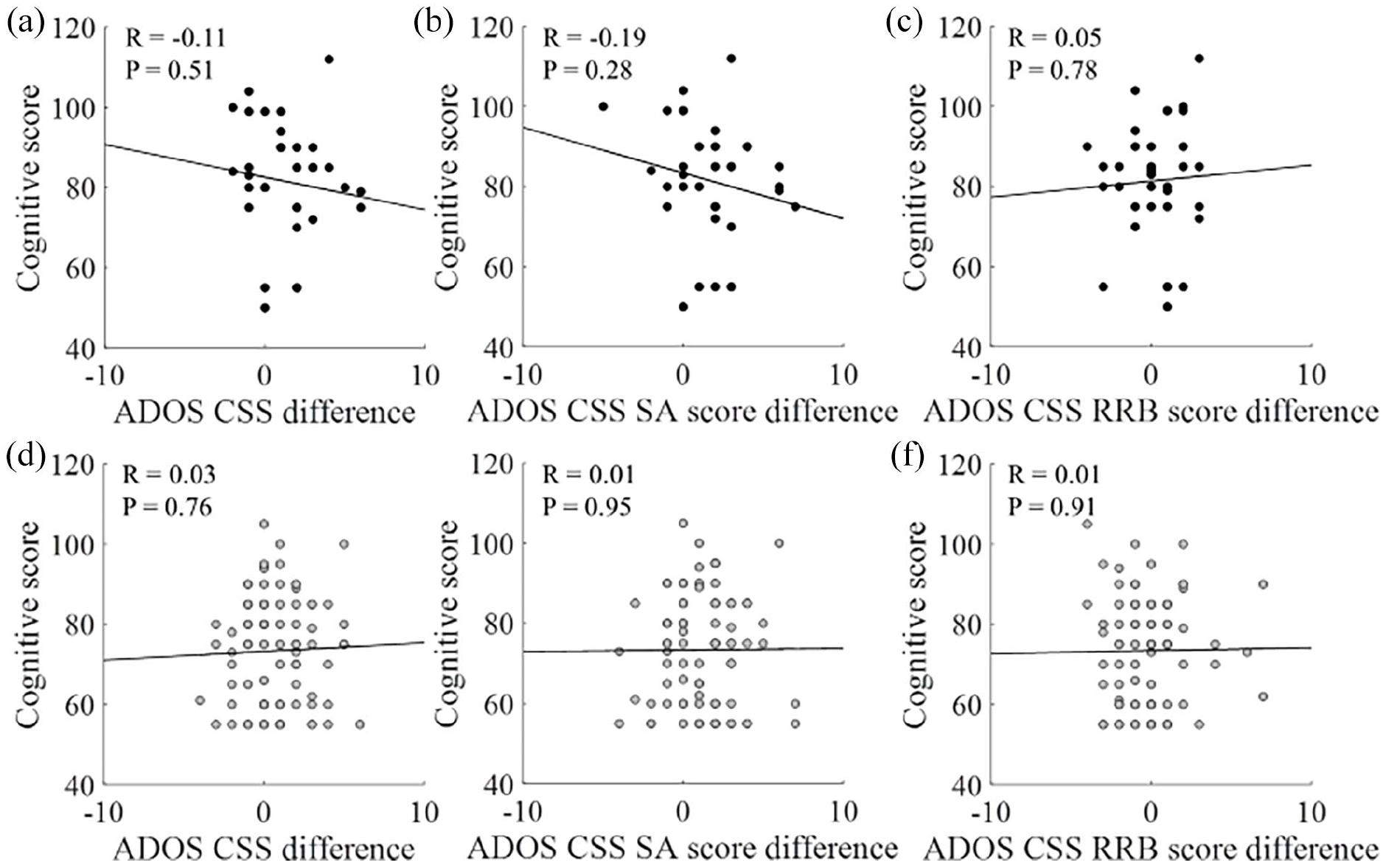
Correlations between changes in ADOS-2 CSS and initial cognitive abilities. Scatter plots demonstrating the correlations between changes in ADOS-2 CSS and initial cognitive abilities of children placed in ME (black) or SE (gray) settings. (a, d): Total ADOS-2 CCS. (b, e): SA CSS. (c, f): RRB CSS. Pearson correlation coefficients and corresponding p values are presented in each panel.
Discussion
Our results reveal that young, 2- to 5-year-old children with ASD attending ME and SE settings display similar longitudinal changes in core ASD symptoms. Specifically, children in both settings exhibited significant improvement in social ASD symptoms over time, but not in RRBs (Figure 1). These changes did not differ across educational settings when analyzing the entire sample (Table 1), when analyzing a sub-group of children matched on initial cognitive abilities and age of diagnosis (Table 2), or when including potentially intervening covariates in repeated-measures ANCOVA analyses (Table 3). There were also no significant differences across groups in language production scores as estimated from the clinician reports on the A1 item of the ADOS-2 (Figure 3). Nevertheless, a significantly higher proportion of children in ME transitioned to ADOS-2 modules requiring higher language production abilities (Figure 2). Taken together, these results demonstrate that the considerable differences in the structure of the two educational settings seem to have relatively little impact on the longitudinal development of core ASD symptoms. Gross spoken language abilities also seem to develop similarly in both educational settings, yet children in ME may be making slightly larger gains than their peers in SE (Figure 2).
While differences across educational settings were relatively small, we found a large and significant interaction between the age of diagnosis and the magnitude of improvement in social ASD symptoms and spoken language abilities in both groups (Table 3 and Figure 4), as also reported in a previous paper from our group (Gabbay-Dizdar et al., 2021). In contrast to the age of diagnosis, initial cognitive ability at diagnosis was not significantly associated with these longitudinal changes (Table 3 and Figure 5). Hence, children diagnosed earlier improved more in social ASD symptoms and spoken language abilities regardless of their initial cognitive abilities or their selected educational setting.
Educational placement of ASD children
Many factors influence the decision to initially place a young child with ASD in ME or SE settings. Factors include not only ethical and societal considerations (Ravet, 2011), but also practical considerations. For example, in Israel, the availability of professionals delivering targeted ASD interventions within SE settings is much higher than their availability in ME settings. This means that parents of young children placed in ME settings often have to invest considerable time and resources in attaining additional intervention hours for their child, outside the educational setting. Indeed, children placed in ME settings tend to have more educated parents with higher socioeconomic abilities not only in Israel (Ilan et al., 2020), but also in France (Rattaz et al., 2020) and the US (Kurth et al., 2016).
While it is often assumed that children with more severe ASD symptoms and lower cognitive and language abilities may require the additional support available in SE settings (Mesibov & Shea, 1996), there are currently no clear clinical guidelines for placing specific ASD children in one educational setting or the other. In this study, we did not find any significant differences in the severity of core ASD symptoms across children placed in the two educational settings (Table 1) and similar finding were also reported in a previous study from our group (Ilan et al., 2020). While gross language production and cognitive abilities were significantly higher in children placed in ME in current (Table 1) and previous (Ilan et al., 2020) samples, the mean difference across groups was equivalent to half a standard deviation with a medium effect size across groups. This means that there is large heterogeneity and considerable overlap in the language and cognitive abilities of young children placed in the two educational settings. This overlap enabled us to easily match sub-groups of children from the two educational settings according to the severity of initial symptoms and cognitive abilities (Table 2).
Perhaps the most important consideration in deciding where to place a child with ASD is outcome. The motivation to initially place preschool children with ASD in SE settings was driven by studies demonstrating that early intensive behavioral interventions (EIBIs) administered by SE teams are effective in improving core ASD symptoms, language abilities, adaptive behaviors, and cognitive abilities (Dawson et al., 2010; Reichow et al., 2014; Zachor et al., 2007; Zachor & Itzchak, 2010). However, these studies compared outcome between highly specialized EIBI programs in universities and medical centers versus SE settings that delivered eclectic “treatment as usual” programs in the community. Indeed, the implementation of structured EIBI programs in community settings, where expertise and resources are more limited, often yields poorer outcome in comparison to that reported in university studies (Nahmias et al., 2019). Moreover, previous studies did not directly compare outcome across ASD children placed in special and ME settings.
To the best of our knowledge, only one study to date has directly compared the outcome of preschool children in special versus ME settings in the community. This study reported that preschool children with ASD exhibited larger cognitive gains when placed in ME settings, but did not measure changes in core ASD symptoms or language abilities (Nahmias et al., 2014). Given that daily exposure to typically developing peers is expected to be particularly important for social and language development (Ravet, 2011), we focused our study on these measures.
We suggest that outcome during preschool years depends on a complex combination of factors including the age of diagnosis, type and quality of intervention that children receive, and the amount and quality of exposure that they have to typically developing peers. The relatively weak outcome differences across educational settings, despite the large differences in their structure and costs (Buescher et al., 2014), suggests that there is considerable room for improving the effectiveness of existing ASD educational settings. Large-scale longitudinal assessments of children with ASD in community settings are essential for substantiating evidence-based practice that can improve outcome, yield clear placement recommendations for children with different abilities and needs, and optimize public health investments in specific educational settings.
Intensity of early ASD interventions
Previous studies have demonstrated that intensive early interventions involving >20 weekly hours of one-on-one treatment by trained therapists using structured programs such as ABA (Reichow et al., 2012; Waters et al., 2020; Zachor et al., 2007) and ESDM (Dawson et al., 2010; Waddington et al., 2016) are effective in improving language, cognitive, social, and/or adaptive behavior abilities of preschool children with ASD. While some have reported that ASD outcomes improve with higher intervention intensities (Linstead et al., 2017), several recent studies have reported that the intensity of intervention did not have an impact on outcome (Darrou et al., 2010; Fernell et al., 2011; Robain et al., 2020; Trembath et al., 2021). In line with the later studies, parents in our sample reported that children in SE settings received twice as many intervention hours as children in ME settings. This suggests that the effectiveness of intervention is not necessarily associated with its intensity and that additional factors such as the type and quality of intervention, parental involvement (Brian et al., 2017), and facilitated exposure to typically developing peers (Bauminger-Zviely et al., 2020), may have considerable impact on social, language, and cognitive outcomes.
Educational setting and spoken language abilities
Previous studies have reported that exposure to typically developing peers is particularly important for improving language skills of children with ASD (Gonzalez-Barrero & Nadig, 2018; Stahmer et al., 2011). Our results are partially in agreement with these studies in demonstrating somewhat better development of spoken language abilities in children placed in MEal settings when quantifying changes in ADOS modules over time (Figure 2). However, this assessment of language production was very gross and a finer estimation of changes in language abilities using language abilities reported on the A1 item of the ADOS-2 did not reveal any significant difference across the two groups (Figure 3). Moreover, previous studies have suggested that the ADOS-2 cannot accurately estimate language skills in children with ASD (Kover et al., 2014).
Proper estimation of early spoken language abilities is critical, because spoken language skills are one of the few predictors that have been consistently associated with improved long-term outcomes of children with ASD (Itzchak & Zachor, 2009). We therefore suggest that a more systematic and sensitive longitudinal assessment of language abilities, using standardized language tests across the different educational settings, is highly warranted.
Limitations
This study had several limitations. First, we focused on changes in core ASD symptoms and did not examine other measures of outcome including changes in cognitive abilities, adaptive behaviors, and aberrant behaviors. Second, as noted above, our estimation of language abilities was gross, relying on transitions in ADOS-2 modules and a gross language scale created from a single item in the ADOS-2 assessment rather than a formal language assessment. Finally, this study did not examine the potential impact of educational placement on the family. Even if there are no differences in the outcome of children placed in either setting, there may be important benefits for specific settings in reducing parental stress, ease of care, accommodating parental beliefs, and improving the family’s quality of life. Moreover, integrating ASD children in ME can also have benefits for typically developing children (Koegel & Oliver, 2019). Hence, the utility and effectiveness of educational settings need to be examined from multiple perspectives of all relevant stakeholders.
Conclusion
Special and ME settings differ dramatically in their structure and cost. Yet there are remarkably small differences in the outcome of preschool children with ASD across settings in terms of their core ASD symptoms and gross spoken language abilities. This suggests that the effectiveness of ASD educational programs in community settings is poorly understood. It highlights the necessity to perform large-scale studies that will be able to identify specific factors that contribute to better outcome and substantiate clinical guidelines for placing preschool ASD children with specific characteristics in particular educational settings. Such studies are critical for improving ASD care, optimizing services, and improving the quality of life for affected families.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Azrieli National Center for Autism and Neurodevelopment Research is funded by grants from the Azrieli Foundation and the Israeli Ministry of Science and Technology