
Abstract
Autism spectrum disorder is a developmental disorder that includes deficits in social communication and interaction, and restricted and repetitive behaviours, interests, or activities. This survey was done to assess autism spectrum disorder prevalence in 16- to 30-month-old children at an urban–rural distribution and determine the association of socioeconomic and demographic conditions. An observational cross-sectional study was conducted in 30 districts of Bangladesh. Three-stage cluster sampling was used with ‘Red Flag’, Modified Checklist for Toddlers and Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, respectively. Data editing and analysis were done using CSPro 6 and SPSS 23. The survey included 37,982 households (71% rural, 29% urban) with 38,440 children. ‘Red Flag’ was positive in 209/10,000 children. Modified Checklist for Toddlers was positive in 149/10,000 children. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition–positive autism spectrum disorder prevalence was 17/10,000 young children (boys 24/10,000, girls 9.8/10,000). Prevalence was higher in urban than rural (25/10,000 and 14/10,000 respectively). It was 77/10,000 in mothers aged 35–39 years and 23/10,000 in children of fathers aged 40 years. For families within the lowest wealth quintile, the autism spectrum disorder prevalence was 15/10,000. Autism spectrum disorder at very young ages in Bangladesh is still low. It was higher in urban areas, with the advanced age of parents, especially mothers, and in families with higher wealth quintiles.
Lay abstract
A nationwide survey was done in Bangladesh to assess autism spectrum disorder prevalence in 16- to 30-month-old children at urban–rural distribution and to determine the association with socioeconomic and demographic conditions. A three-stage cluster sampling method was used where districts from all divisions were selected in the first stage, census enumeration areas as blocks of households were selected in the second stage and households (within the blocks) were selected in the third stage. Thereby, it included 38,440 children from 37,982 households (71% rural, 29% urban) aged 16–30 months from 30 districts of eight divisions of Bangladesh. Screening was done with a ‘Red Flag’ tool and Modified Checklist for Toddlers and a final diagnosis using Diagnostic and Statistical Manual of Mental Disorders, 5th Edition for autism spectrum disorder. Autism spectrum disorder prevalence was 17 per 10,000 young children – in other words, one in 589 young children. Boys were found at higher risk of autism (one in 423 boys; one in 1026 girls). Prevalence of autism spectrum disorder was higher in urban environments than in rural ones – 25/10,000 and 14/10,000, respectively. More autism spectrum disorder children were found in advanced age groups of parents, especially mothers, and in households with a higher wealth quintile. This survey is significant as it covers both urban and rural areas and specifically targets very young children. The involvement of the Bangladesh Bureau of Statistics, as well as support from the entire healthcare system infrastructure, makes this survey more representative on a national level. Its results will form a database to support the development of an effective early intervention programme in Bangladesh. We hope it will prove useful for researchers, clinicians and frontline healthcare workers, and inform the decisions of policymakers and funders in Bangladesh.
Introduction
Autism spectrum disorder (ASD) is a developmental disorder that includes deficits in social communication and social interaction and the presence of restricted repetitive patterns of behaviour, interests, or activities that can persist throughout life (American Psychiatric Association, 2013). ASD and impairments associated with ASD often impose significant functional, social and financial impacts on affected individuals, their families and society (Ganz, 2007; Hoang et al., 2019; World Health Organization, 2018).
The prevalence of ASD has been increasing worldwide. It was reported as high as 168 per 10,000 or 1/59 in 8-year-old children in the United States in 2014 (Baio et al., 2018). The prevalence varies from 30 to 116/10,000 within the age range of birth to adulthood in Northern Europe (Elsabbagh et al., 2012). An overall prevalence of 36/10,000 with a higher prevalence in East Asia than in West Asia (51/10,000 and 35/10,000, respectively) was found in a meta-analysis of Asia (Qiu et al., 2019). A review study from South Asia, however, concluded that methodological differences in case definition, screening instruments and diagnostic criteria made it very difficult to compare the studies in this region (Hossain et al., 2017). In Bangladesh, in 2013, one survey reported the prevalence of autism in 0- to 9-year-old children was 15/10,000, with 6.8/10,000 in rural and 300/10,000 in urban areas (Non-Communicable Diseases Control (NCDC) Programme et al., 2013). A rural survey in 2016 reported autism in 7.5/10,000 cases among children aged 18–36 months (Akhter et al., 2018).
In recent years, a growing interest in the early detection of ASD has developed to implement early intervention (Dawson, 2008). Several longitudinal studies revealed that the majority of diagnoses made around the second birthday were stable during a re-evaluation of children at age 4 or older (Charman et al., 2005; Cox et al., 1999; Freeman & Cronin, 2002; Lord, 1995; Moore & Goodson, 2003; Stone et al., 1999). Intervention in the early years of life is associated with a more rapid and stronger response in learning language and social skills than the time of teaching these skills at a later age (Courchesne et al., 2011; Dawson, 2008; Lewis et al., 2014). Many researchers also believe feel that ASD is not necessarily a lifelong disabling condition (L. K. Koegel et al., 1999; R. L. Koegel & Koegel, 2012) and most research clinics reported that most of the children could be enrolled in regular education classrooms with intervention and around 25% of children would completely lose the diagnosis (Cohen et al., 2006; Helt et al., 2008; Lovaas, 1987; Sallows & Graupner, 2005).
This study was done to assess ASD prevalence in 16- to 30-month-old children in Bangladesh on a national level using the Bangladesh public health structure.
Methods
Survey design and population
This research was based on a cross-sectional observational survey, conducted in rural and urban areas of sampled districts nationwide to obtain the national prevalence of autism among children aged 16–30 months in Bangladesh. The survey was conducted in 85 primary sampling units (PSUs)/enumeration areas (EAs) distributed among 30 randomly selected districts of eight divisions of the country (Figure 1). Rural and urban areas were selected proportionately.
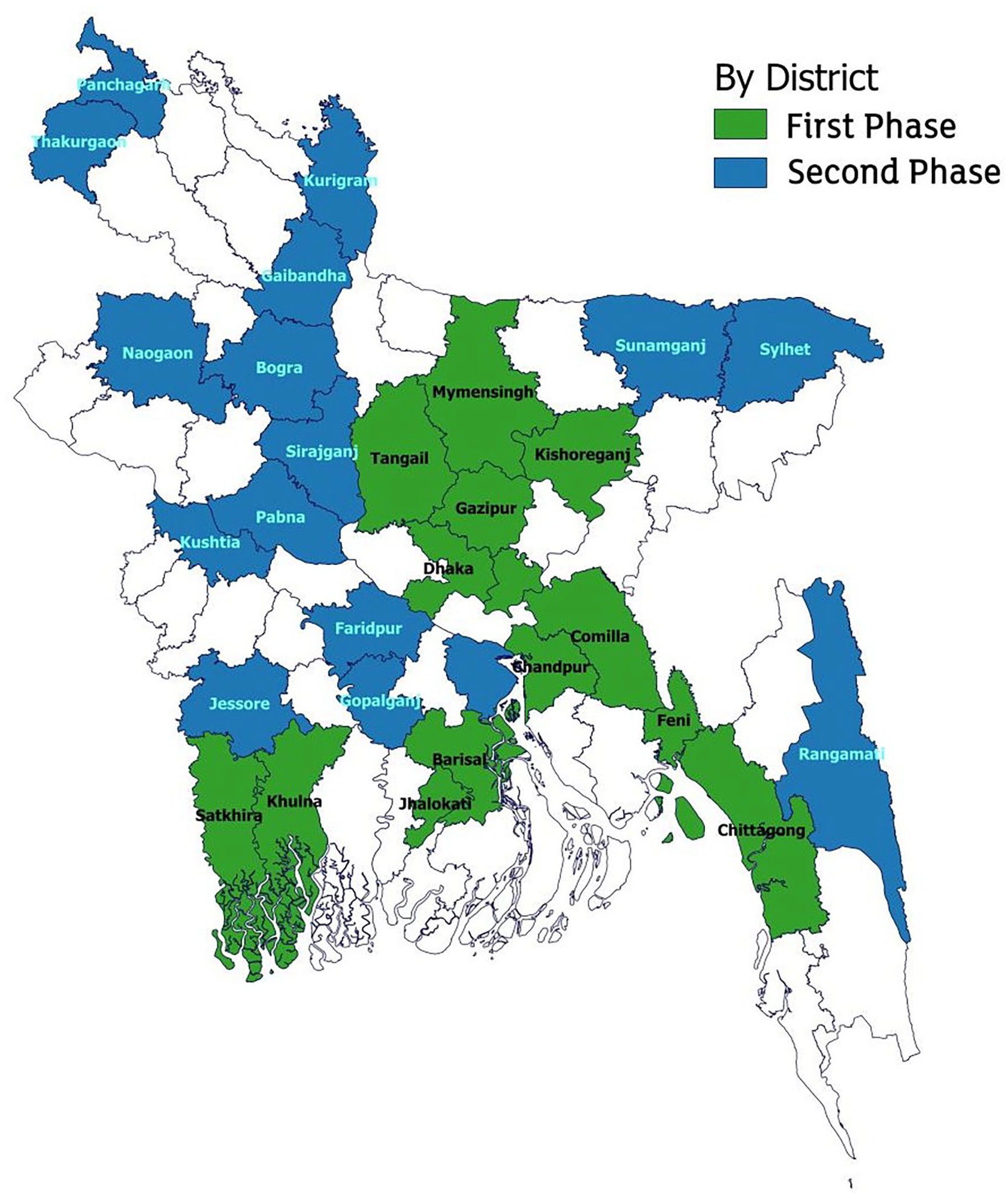
Map of the study area.
The population covered in this survey was children aged 16–30 months. So, only households (HHs) with children aged 16–30 months were selected.
Sample size and sampling design
The required sample size (n) was determined by the usual sample size determination formula for estimating proportion, which is given below:

where p is an a priori proportion for autism in 8-year-old children in the United States in 2014 = 147/10,000 or 1.47%; z (α/2) is the critical value of the Normal distribution at α / 2 (for a confidence level of 95% and α of 0.05) = 1.96; d, allowing a maximum relative error of ±10%, = 0.0147 and f is the design effect = 1.5.
Thus,
n = 1.47 (1 − 0.0147) [1.96/0.0147]2 × 1.5 = 38,624.
For operational feasibility, the sample size was rounded to 38,250.
For operational feasibility, the sample size was rounded to 38,440. The survey followed a three-stage cluster sampling method, where districts from all divisions were selected in the first stage. The census EAs as blocks of HHs were selected in the second stage and HHs (within the blocks) were selected in the third stage.
Training of survey staff
Three-day training of the trainers (ToT) was conducted with the participation of Medical Officers, Clinical and Education Psychologists, Instructors, Senior Teachers of Autism Schools and Therapists of the Institute where the training was conducted by the Project Director/Paediatric Neurologist, Deputy Project Director, Research Consultant and Research Medical Officer imparted the training.Then, a team of two Master Trainers subsequently was engaged for training 55–65 survey staff, including Medical Officers (MOs), Health Inspectors (HIs) and Health Assistants (HAs) for 2 days on the topics mentioned above at the respective district Civil Surgeon office. Each Master Trainer covered training in two sample districts one after another. After completing 2 days of training at the Civil Surgeons (CS) office, each survey team started enumeration in one of their assigned sample areas on the third day, where Master trainers, Quality control Officers (QCO) and Coordinators (MOs) closely monitored their field operation and made corrections where needed. Before conducting field-based training, all the assigned MOs (Coordinators & QCOs) were given 3 days of training on Autism & NDDs, including the survey questionnaire by the senior officers of the concerned Institute. The training of about 280 MOs in 30 districts was arranged in two phases before commencing field training and survey. A 1-day training of all the CS of sample districts (30 CS) was also done before field data collection, which helped them with effective coordination of the survey.
Data collection methods, instruments and screening of ASD
A survey team of three members (two Health Assistants as interviewers and one Health Inspector as team supervisor) was assigned to each PSU/EA to collect data from HH heads or mothers or caregivers of children aged 16–30 months. The HHs of each PSU/EA were updated by the survey team. To collect data, face-to-face interviews took place with a structured questionnaire.
The survey covered 85 PSUs/EAs in each district completing 2550 PSUs in 30 districts (30 × 85). There were 17 teams to cover 85 PSUs. A total 1530 survey staffs from 30 sample districts were assigned from the Directorate General Health Services (DGHS). Regarding the screening of ASD and identification of autism cases, the survey teams performed the first stage screening of ASD among the surveyed children using the ‘Red Flag’ tool (Autism Speaks, 2018). Trained MOs applied ‘Modified Check Lists for Toddlers’ ‘M-CHAT’ (Robins et al., 2004) on the referred ‘Red Flag’-positive children. An expert group of trained Neurologists, Medical Doctors or Psychologists performed a final diagnosis of ASD in the third stage using the Diagnostic and Statistical Manual for Mental Health, 5th Edition (DSM-5) for ASD (Kulage et al., 2014) (Figure 2).
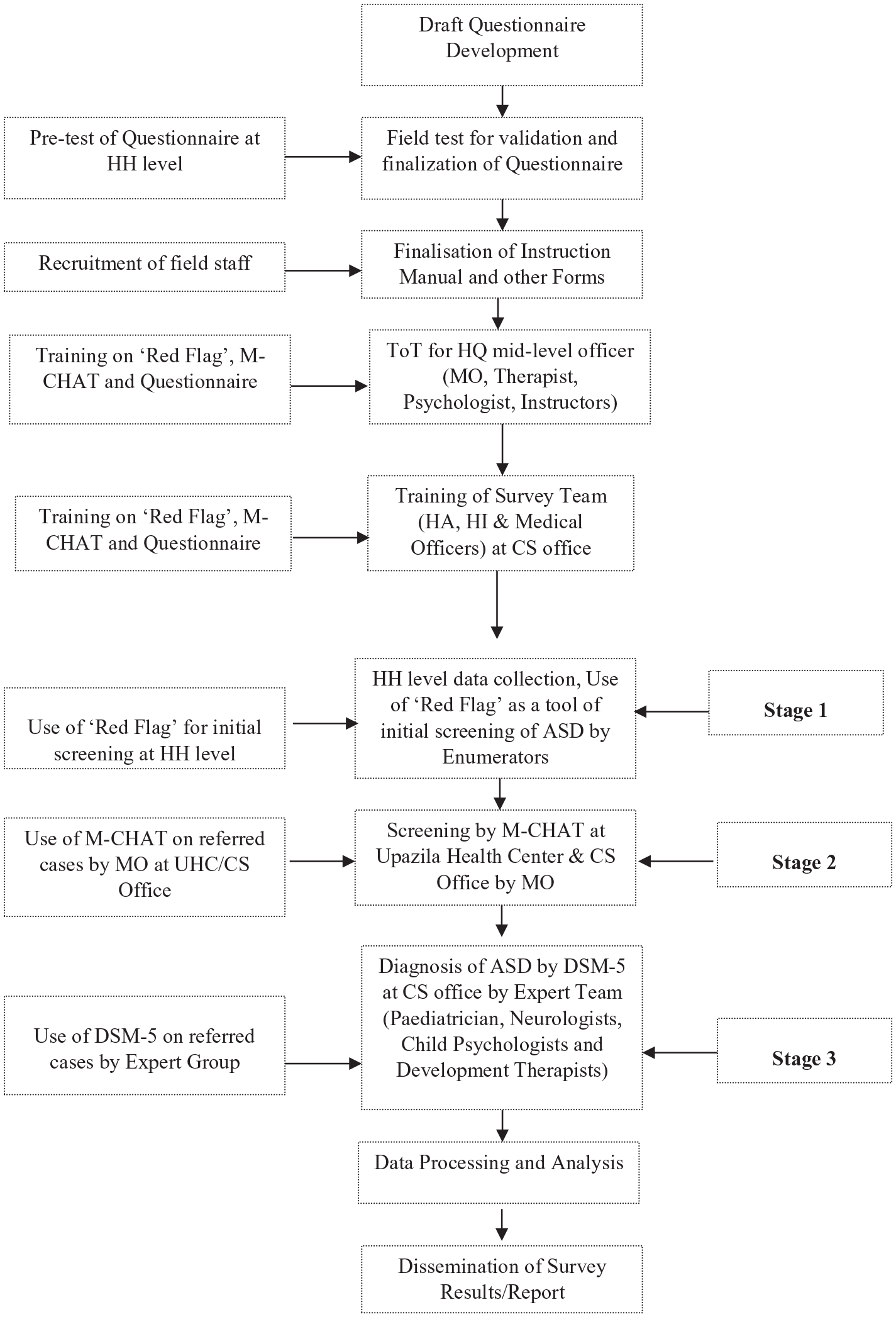
Flow chart of survey activities.
Survey period
The preparatory phase of the survey was between January and April 2017. The field data collection took place in two phases: first phase from May to June 2017 and the second phase from October to December 2017.
Supervision, coordination and quality assurance
Thirty (30) District Coordinators (MOs of Civil Surgeon Offices) and 250 Quality Control Officers (MOs of Upazila Health Complexes) acted as supervisors in the data collection operation, where 250 Upazila Health and Family Planning Officers (UHFPO) acted as Upazila Coordinators and 30 Civil Surgeons (CS) acted as District Chief Coordinators (DCCs).
To validate collected data, a ‘post enumeration check’ (PEC) was conducted both in rural and in urban areas at least in 2% of the surveyed HHs within a week after completion of the main survey.
Regarding validation of screening of ASD, an expert group of Medical Officers and Psychologists from Dhaka re-examined 10% of M-CHAT-negative cases (i.e. one in 10) using DSM-5.
Data editing and analysis
Manual editing and coding were performed as per the editing guidelines and code book. The data entry, cleaning and duplication detection were performed using CSPro 6. Data analysis and tabulation process were carried out using SPSS 23.
Ethical implications
Ethical clearance was obtained from the ethical committee of the Bangladesh Medical Research Council. Furthermore, prior to its commencement, approval for conducting the nationwide survey was obtained from the Bangladesh Bureau of Statistics (BBS).
Patient and public involvement
Children with ASD and without ASD and their families were involved in setting the research questions and the outcome measures. They were actively involved in field-level data collection and screening processes. Patients and their families were also central to the dissemination of the baseline information, which helped to motivate community involvement during and beyond the survey. Participants were all residents in a stratified last stage random sample of enumeration areas (the geographical area canvassed by one census representative) from the latest census. Before the baseline survey, permission was received from the authentic government authority (Ministry of Health and Family Welfare and Bangladesh Bureau of Statistics). Individual consent forms were read and signed by every respondent, all of whom were told that they were free to decline to answer any question. Parents or caregivers gave individual consent for each child who contributed to the screening process. All sorts of privacy for the data providers were maintained. Confidentiality of data was strictly ensured. Data were used only for the purpose of this survey and research.
Results
The survey was undertaken in 37,982 HHs in 30 districts distributed across eight divisions. House-to-house interviews, including ‘red flags’, were completed in 38,440 children aged 16–30 months. Subsequently, 804 were screened positive for ‘Red Flags’, 574 were M-CHAT-positive and 67 were DSM-5-positive (Table 1).
Distribution of districts, Upazila, HHs surveyed, and children screened positive by Red Flag, M-CHAT and diagnosed as ASD by DSM-5.
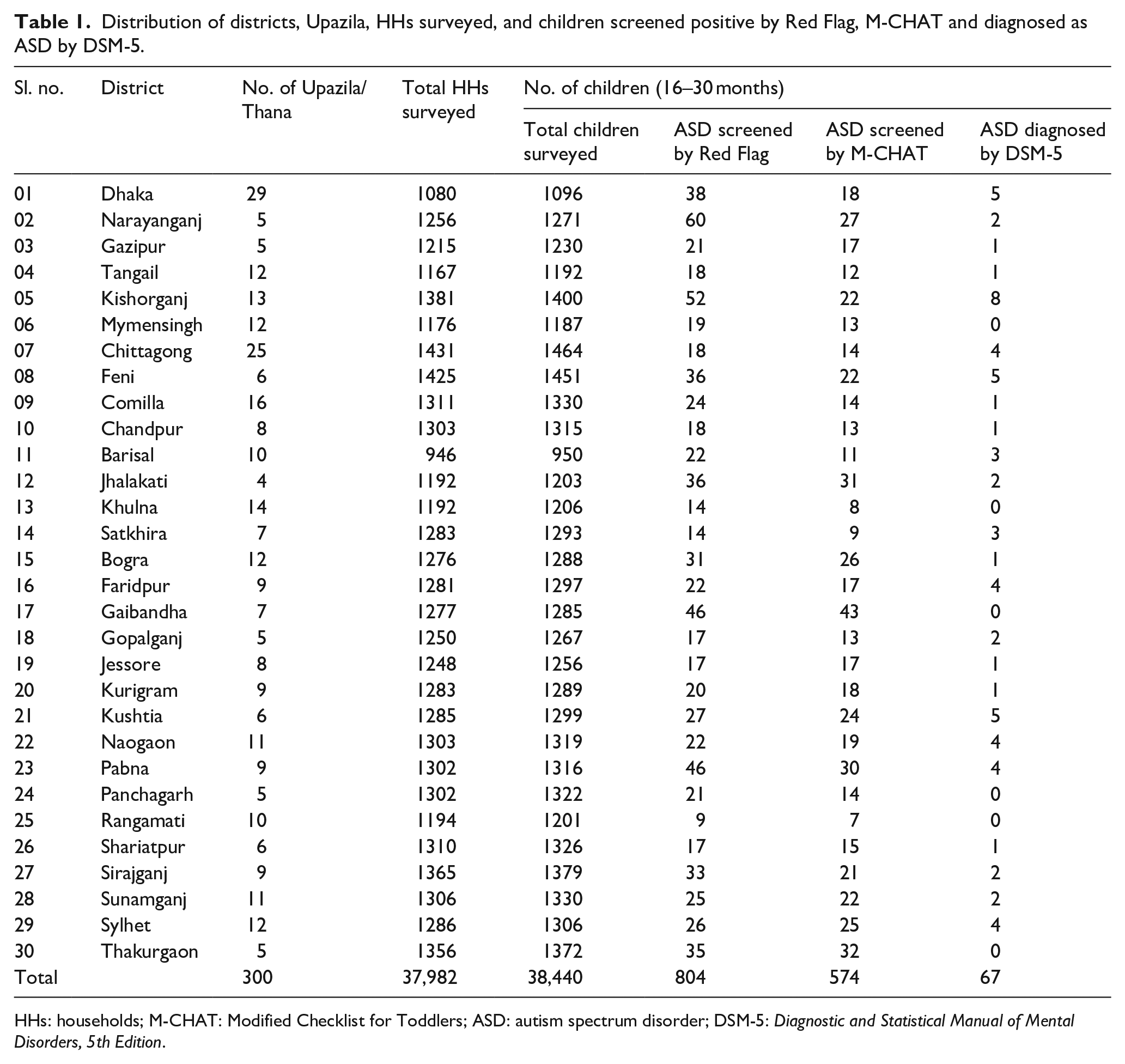
HHs: households; M-CHAT: Modified Checklist for Toddlers; ASD: autism spectrum disorder; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
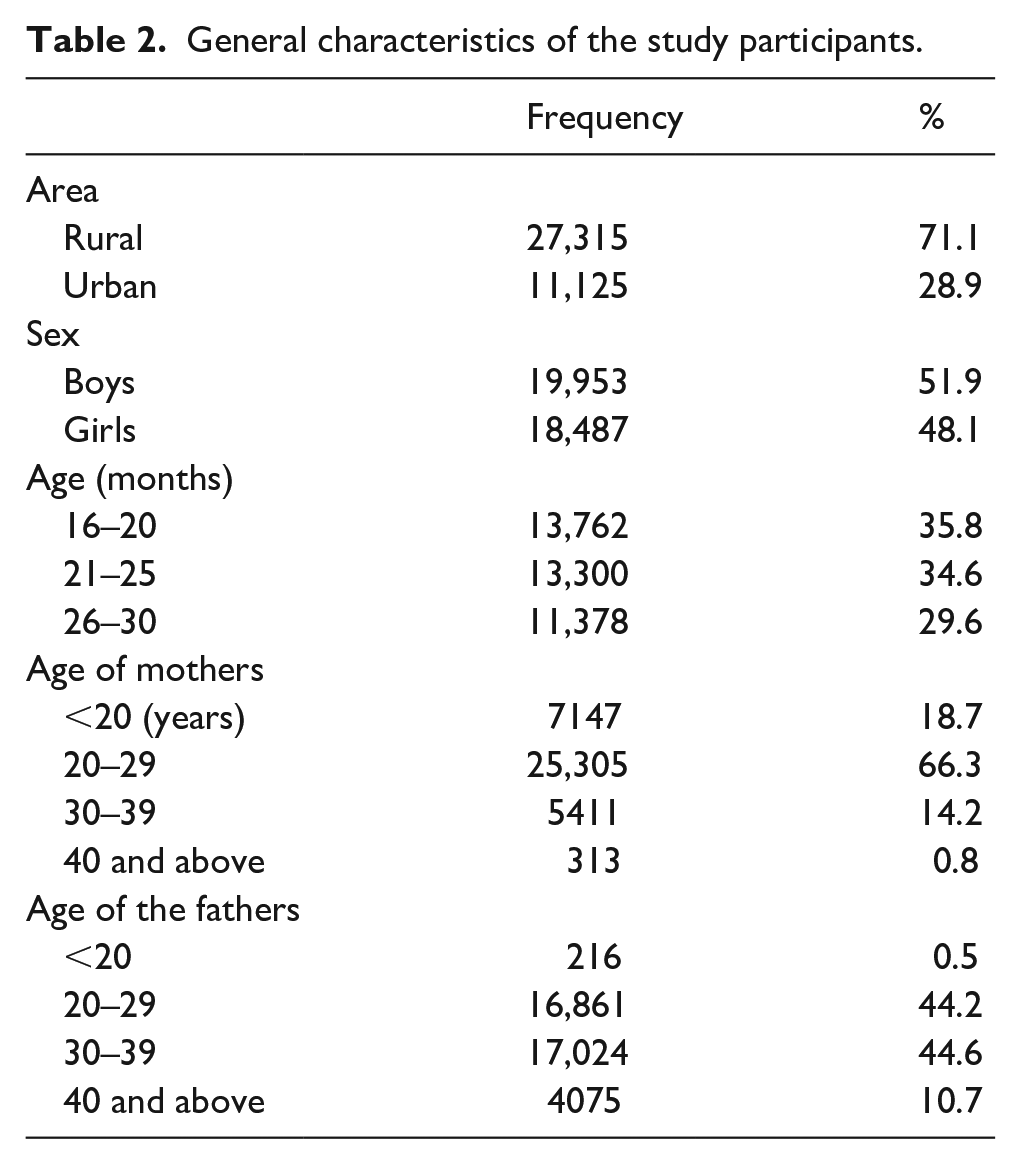
Table 2 presents the general characteristics of the study sample. Notably, 71.1% of children lived in rural areas with 51.9% boys and 48.1% girls.
General characteristics of the study participants.
a. Prevalence of ASD
Red Flag screen was positive in 209 per 10,000 young children (boys 242; girls 172). M-CHAT screen was positive in 149 per 10,000 young children (boys 174; girls 122).
ASD prevalence was 17.4 per 10,000 young children (boys 24/10,000, girls 9.8/10,000) – that means one in 589 young children (one in 423 boys; one in 1026 girls). Rural prevalence was 14/10,000 and urban was 25/10,000 (Table 3).
Distribution of screened positive and diagnosed ASD children by sex and area of residence using Red Flag, M-CHAT and DSM-5.
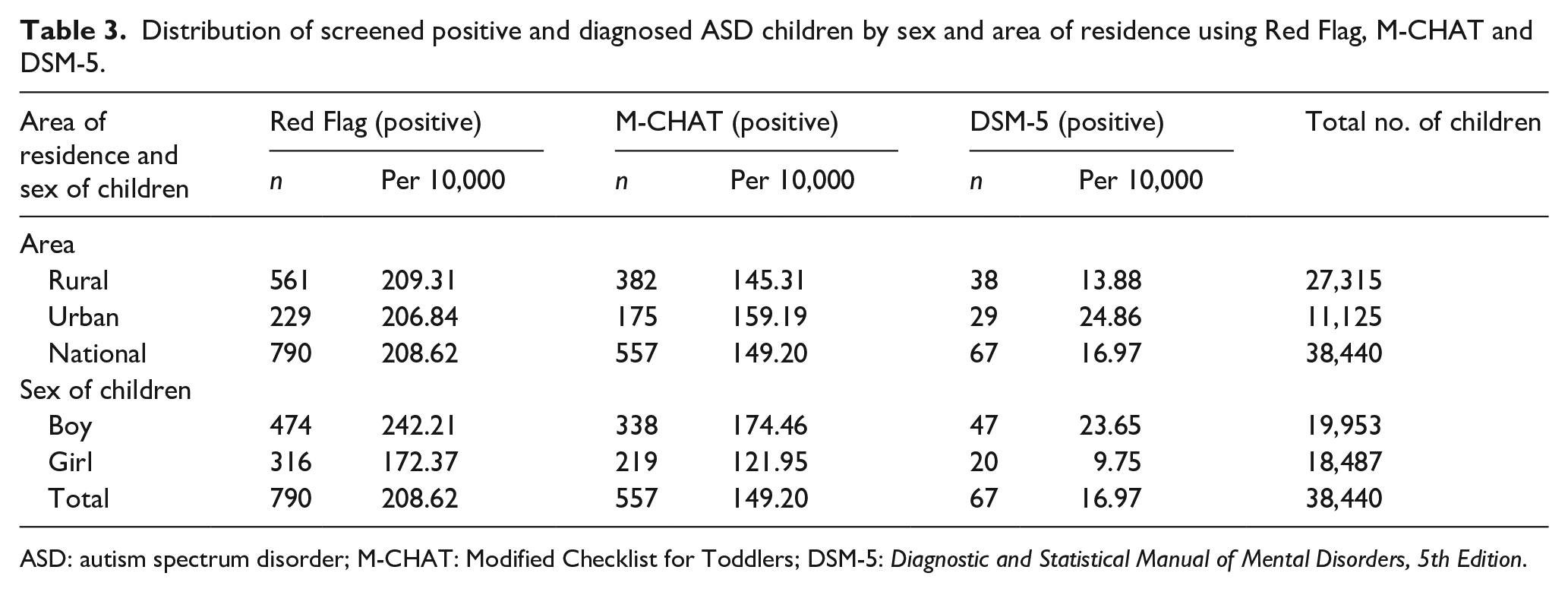
ASD: autism spectrum disorder; M-CHAT: Modified Checklist for Toddlers; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
b. Associations of ASD
Age of children
ASD prevalence was 13/10,000 in the age group 16–20 months and this rose to 25/10,000 in the age group 26–30 months (Table 4).
Distribution of screened positive and diagnosed ASD children (by age range) using Red Flag, M-CHAT and DSM-5.
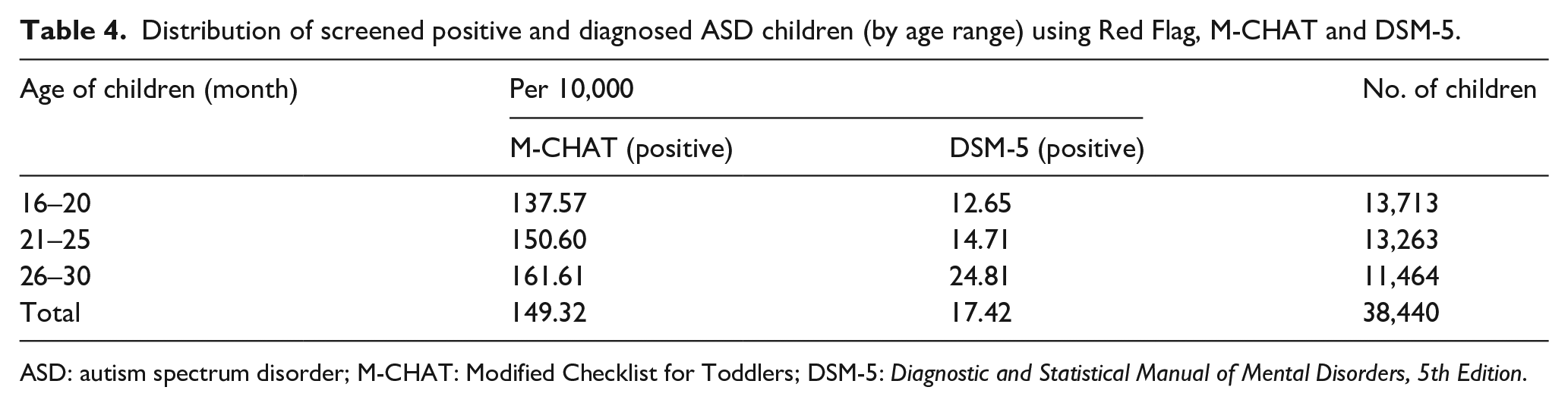
ASD: autism spectrum disorder; M-CHAT: Modified Checklist for Toddlers; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
Parental age
ASD prevalence was high in children of mothers aged 35–39 years (77/10,000) compared with that in children of mothers aged less than 20 years (14/10,000). Similarly, it was more prevalent in children of fathers aged 40 years and above (23/10,000), whereas it was 14/10,000 in children of fathers aged 20–24 (Table 5).
Distribution of ASD children by parent’s age (by DSM-5).
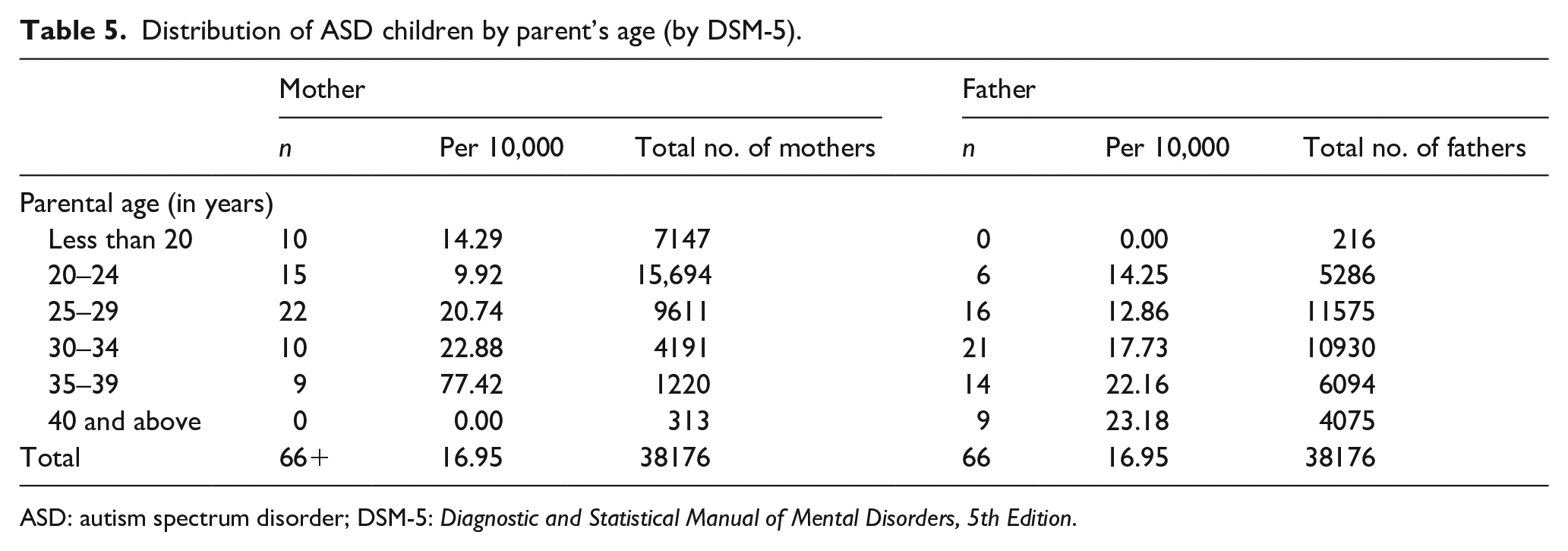
ASD: autism spectrum disorder; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
In the lowest wealth quintile, ASD prevalence was 15 per 10,000, while in the highest it was more than double this − 33 per 10, 000 (Table 6).
Distribution of ASD children by wealth quintile (by DSM-5).
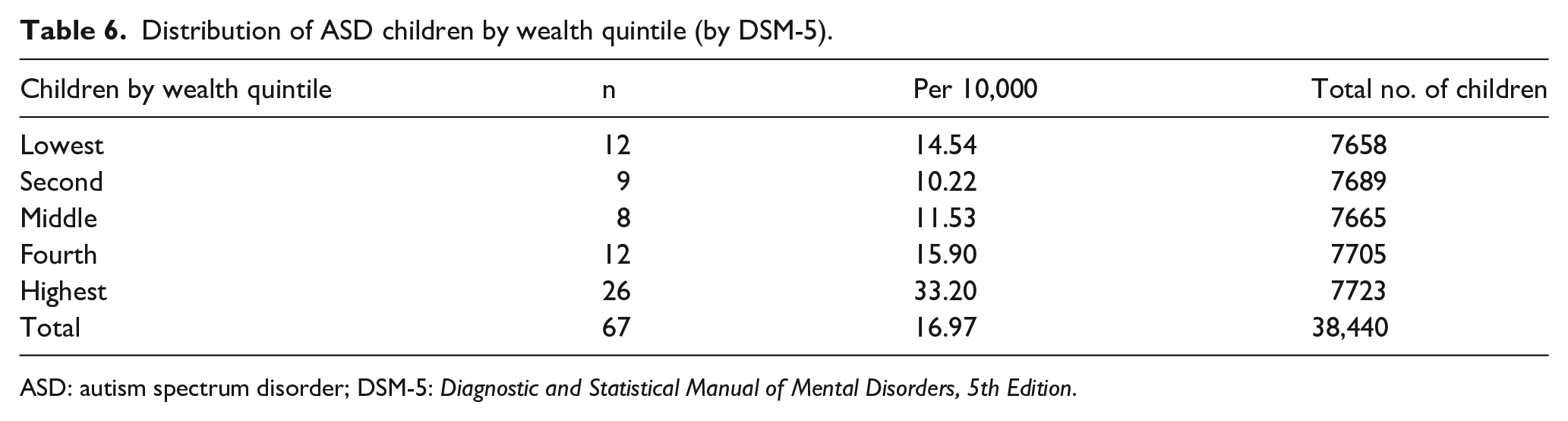
ASD: autism spectrum disorder; DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.
Maternal healthcare in pregnancy
A higher ASD prevalence was found in children of mothers who did not receive any antenatal care (ANC) (22/10,000) compared with that in children of mothers who had ANC from trained personnel (received at least 6-month-long training) working in the field (13/10,000).
Prenatal maternal physical and/or mental health
ASD prevalence was 15/10,000 in children of mothers who experienced no physical or mental stresses in pregnancy but 44/10,000 in children whose mothers faced physical stresses, 42/10,000 in children of mothers who faced mental stresses and 52/10,000 in children of mothers who experienced both. The relationships were found to be statically significant at <0.5 levels determined using the chi-square test.
Discussion
Principal findings
Among 38,440 children, 804 (209/10,000) had early signs of ASD. Using M-CHAT, 574 were screened positive for ASD, and ASD was diagnosed in 67 (17 per 10,000) cases (Table 1). ASD was highest in the 26–30 months age group, followed by 21–25 months and 16–20 months (Table 3). Prevalence was higher in urban environments (Table 4). It was 5.5 times higher for children with 35–39 years old mothers than for those of <20 years. A higher prevalence was also found in fathers aged above 40 years compared with fathers in the 20–24 age group (Table 5). Families within the lowest wealth quintile had more than double the number of children with ASD than families within the highest quintile (Table 6), whereas ASD prevalence was 15/10,000 of children of mothers who experienced no physical or mental stress in pregnancy but 44/10,000 in children whose mothers faced physical stress, 42/10,000 in children of mothers who faced mental stresses and 52/10,000 in children of mothers who experienced both. The relationships were found to be statistically significant.
Strengths and limitations of this study
With the help of the Bangladesh Bureau of Statistics, this study covered a large and representative sample of the country which was a strength of the study. Support from the whole health system, including field-level staff who are familiar with house-to-house visits, was taken. The population sampled was a very young age group in which interventions would be more beneficial.
A limitation of the study was the age group, which was children aged 16–30 months, which could not represent ASD prevalence in all age groups of the country. Full clinical features of ASD might not appear at this low age range and the diagnosis might be difficult at this age. As there were 1700 data collectors, as well as 250 quality control medical officers, who were all part-time – working in regular government jobs, and sometimes transferred, standardization of the data collection faced limitations. In addition, in busy government health facilities, the location of M-CHAT assessments was not ideal. Furthermore, some areas like Kishoreganj were hard to reach because of natural calamities and the urban sampling was challenging because people were reluctant to allow access to their homes.
Comparison with other studies
The prevalence rate in this study was in agreement with the prevalence rate of the DSH 2013 survey which was 15.5/10,000 (NCDC Programme et al., 2013) and it is difficult to compare this rate because of different and limited sampling frames. The 2013 survey looked for autism in 0- to 9-year-old children and was conducted in seven Upazilas and one urban ward in eight districts, whereas this survey covered 300 Upazilas and 11,000 urban areas. The prevalence found in this study is comparable with a community study done in Northwest India (15/10,000) with an age group of 1–10 (Raina et al., 2017). Another study in South India found 15/10,000 in their 1- to 5-year age group (Poovathinal et al., 2016). Prevalence in this study is in disagreement with the very high findings of 168/10,000 in the US survey (Baio et al., 2018) and 264/10,000 in a South Korean survey (Kim et al., 2011). This might be due to the lower age range when full clinical features might not appear and cause diagnosis difficulties. Other important causes of variation were the methodological differences in the case definition and case-finding procedures and diagnostic criteria. Hoang et al. (2019) and Perera et al. (2009) found high levels of ASD at this young age, which was contrary to our findings (75/1000 and 105/10,000 respectively). This might be due to the use of Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) instead of DSM-5 (Kulage et al., 2014; Wilson et al., 2013; Worley & Matson, 2012). Rural prevalence in this study (Table 4) was roughly double that of the 2016 IPNA rural survey (6.8/10,000) (Akhter et al., 2018) and 2013 DSH survey (7.5/10,000) (NCDC Programme et al., 2013). Comparisons here were inappropriate as the sampling frames were different and limited in both studies. The higher urban population in this survey was in agreement with a few other studies (Becker, 2010; Hoang et al., 2019; Lauritsen et al., 2014). Environment-related factors might contribute to this difference. Hazardous air pollutants usually concentrate in urban environments causing exposures during pregnancy and early childhood, which might have a potential association (Kalkbrenner et al., 2010; Windhamet al., 2006). The association of ASD with aged mothers (Table 5) was in agreement with the results of a meta-analysis by Sandin et al. (2016) where there was an association between advancing maternal age and the risk of autism. Many discussions with explanations were given regarding maternal age and chromosome anomalies (Sandin et al., 2016), variation and other genomic alterations, including epigenetic dysfuncions (Christian et al., 2008; Marshall et al., 2008), and the accumulated exposure to various toxins over time which could also result in genomic and epigenetic alterations in germ cells of older parents (Williams & Ross, 2007; Yauk et al., 2008). The association between ASD and paternal age (Table 5) was consistent with the finding of Reichenberg et al. (2006) where de novo mutations with advancing age or alterations in genetic imprinting were mentioned as the possible cause. Results regarding the wealth quintile on ASD were conflicting. Our findings (Table 6) agreed with some studies (Durkin et al., 2010; Thomas et al., 2012)and disagreed with others (Rai et al., 2012; Sun et al., 2014).
Conclusions
The prevalence of ASD in the very early years of life was still low in Bangladesh. ASD prevalence was higher in urban areas, with mothers of higher age groups and families in the lowest wealth quintiles. It was also higher in mothers who had physical and mental stress during the pregnancy period.
Recommendations
Further studies would be needed to elucidate the reasons for these findings. This survey might help in the development of an effective programme through which the government and NGOs could be able to work together. Early intervention could be started if these children with ASD could be identified at an early age. They could substantially contribute to society and the nation with proper training and education.
Footnotes
Acknowledgements
We would like to express our very great appreciation to the Ministry of Health and Family Welfare of Bangladesh, in particular, the Directorate General of Health Services to conduct this survey as part of the project ‘Establishment of Institute of Paediatric Neurodisorder and Autism’. We are thankful to the Bangladesh Bureau of Statistics, A House of Survey Research (SURCH) for their statistical support. We are also grateful to Psychiatrists from the National Institute of Mental Health, the Community Health Care Initiatives in Bangladesh, Civil surgeons of the selected 30 districts and their colleagues and the Bangladesh Medical Research Council. We would also like to extend our thanks to the Medical officers, Psychologists, Therapists, Teachers and all other staff of IPNA, BSMMU for conducting this door to door survey. Finally, we are grateful to all the parents of children who cooperated with their valuable time.
Data editing and analysis
Manual editing and coding were performed as per the editing guidelines and codebook. The data entry, cleaning, duplication detection was performed using CSPro 6. Data analysis and tabulation process were carried out using SPSS 23.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclaimers
The views expressed in this article are our own and do not repreent the official positions of any institutions or funders.
Ethical implications
Ethical clearance was obtained from the ethical committee of the Bangladesh Medical Research Council. Furthermore, prior to its commencement, approval for conducting the nationwide survey was obtained from the Bangladesh Bureau of Statistics (BBS).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This survey was funded by the Ministry of Health and Family Welfare, the Government of the People’s Republic of Bangladesh.
Patient and public involvement
Children with ASD and without ASD and their families were involved in setting the research questions and the outcome measures. They were actively involved in field-level data collection and screening processes. Patients and their families were also central to the dissemination of the baseline information, which helped to motivate community involvement during and beyond the survey.