
Abstract
Caring for children with developmental delays or disabilities places significant stress on caregivers, which is often exacerbated in low-resource settings. The World Health Organization developed a caregiver skills training for families of children with developmental delays or disabilities, which includes a three-session caregiver well-being module based on Acceptance and Commitment Therapy, that aims to help caregivers build psychological flexibility (i.e. the ability to focus on the present moment, make space for difficult thoughts and emotions and commit to value-driven actions that enrich their lives). We investigated whether this brief caregiver well-being programme was feasible, acceptable and contributed to positive outcomes for caregivers in a rural South African town. We adapted the intervention to the local context using a participatory approach. The ‘Well-Beans for Caregivers’ adaptation of the World Health Organization Caregiver Skills Training Caregiver Wellbeing module was then delivered by trained facilitators to a group of 10 caregivers in three weekly, 2-h sessions. Most caregivers were single and unemployed. Feedback from the facilitators, caregivers and trainee observers was obtained before, during and after the programme. Results suggested that this brief programme shows promise as a feasible and acceptable intervention, which may lead to improved caregiver well-being and mental health in communities in South Africa.
Lay abstract
Young children with developmental disabilities and delays who live in low- and middle-income countries are at significant risk of not reaching their full potential. We know that daily interactions with their caregivers (parents or other people taking care of them) play an important role in promoting their development. However, having a child with developmental disabilities can have a negative impact on carers’ mental health and well-being, which in turn can influence their capacity to care for their children. To date, very little attention has been given to the caregivers’ capacity to care. The World Health Organization developed a Caregiver Skills Training programme which includes a brief, three-session module that focuses on improving caregivers’ well-being and mental health. This well-being programme is based on acceptance and commitment therapy. Acceptance and commitment therapy shows increasing evidence of helping people respond to their stressors, thoughts, feelings and experiences a little differently and commit to small changes that are in line with their personal values. Acceptance and commitment therapy has shown promise in improving feelings of well-being in caregivers of children with developmental disabilities. We adapted the World Health Organization Caregiver Skills Training Caregiver well-being module to suit the South African context. The resultant ‘Well Beans for Caregivers’ was then delivered to caregivers from a rural, low-resource setting in South Africa. We found the intervention easy to implement, highly acceptable to caregivers and showed promising impacts on caregivers’ well-being and mental health. This intervention has the potential to be implemented widely and sustainably to build caregivers’ capacity to care for their children.
Keywords
Introduction
Young children with developmental disabilities and delays (DDs), including autism and intellectual disabilities, who live in low- and middle-income countries (LMICs) are at significant risk of not reaching their full potential (Lord et al., 2022; Olusanya et al., 2018). We know that daily nurturing interactions with their caregivers (parents or other people who are taking care of them) play a pivotal role in promoting their development (World Health Organization [WHO] et al., 2018). Globally, various policies and programmes are focussing on efforts to build and support caregiver capabilities and skills to promote child development (Dawson-Squibb et al., 2020; Jeong et al., 2021; Nevill et al., 2018; Salomone et al., 2019).
To date, very little attention has been given to the caregivers’ capacity to care. We know that caregivers of children with autism and other developmental disabilities in LMIC are at a high risk of sub-optimal health and mental health, higher levels of stress and burden and a lower quality of life than other caregivers (Mthombeni & Nwoye, 2018; Schlebusch et al., 2017; A. P. Simelane, 2020). Often, the complexities of disability, limited psycho-social support, poverty, unemployment and stigma negatively impact caregivers of children with DD, leaving them distressed and disconnected (Gladstone et al., 2018; Masefield et al., 2020; Mthombeni & Nwoye, 2018; Tekola et al., 2022). Caring for caregivers’ well-being and mental health may therefore represent a fundamental first step to support their capacity to provide nurturing care for their children. Accessible interventions that support caregivers to manage their stress and promote their well-being without adding additional burdens are desperately needed. Due to the enormous mental health treatment gap, the dissemination and implementation of evidence-based practices in LMICs have emerged as a global health priority (Lord et al., 2022; Patel et al., 2018).
The WHO developed a novel, open-access caregiver skills training, ‘Caregiver Skills Training for families of children with developmental delays or disabilities’ (WHO CST) (WHO, 2022b). The WHO developed this intervention with a global audience in mind by incorporating critical elements to make the intervention feasible in resource-constrained settings and adaptable to the world’s different cultural, linguistic, socioeconomic and geographical regions (Salomone et al., 2019). The WHO CST recognises the barriers and challenges to diagnosis and early intervention services in LMIC (Schlebusch et al., 2020). Therefore, the beneficiaries of the programme are deliberately inclusive and open to all families who are concerned about their child’s developmental difficulties – with or without a formal diagnosis. This includes children with autism and other developmental disabilities. The WHO CST was developed through a systematic evidence review, extensive stakeholder consultation and an iterative review process. Promising evidence from around the world is beginning to emerge regarding the feasibility and acceptability (Lau et al., 2022; Salomone, Ferrante, et al., 2022; Sengupta et al., 2021; Tekola et al., 2020) and effectiveness (Salomone, Settanni, et al., 2022) of the WHO CST. While the programme focuses mainly on caregiver skills to promote child development, it also includes an additional optional module focussing exclusively on caregiver well-being.
The three-session WHO CST Caregiver well-being module is based on acceptance and commitment therapy (ACT). ACT is an established mindfulness-based behavioural therapy that builds acceptance and promotes psychological flexibility (Hayes et al., 2013). Tools such as metaphors and experiential exercises help individuals learn how to make healthy contact with thoughts, feelings, memories and physical sensations that they have feared and avoided in the past. They learn how to make space for these thoughts, feelings and memories while developing greater clarity about their personal values and committing to small changes in behaviour in line with these values. A growing body of evidence suggests that ACT interventions can result in positive changes in the psycho-social well-being of caregivers of children with a range of psychological and physical difficulties, including autism, chronic pain and significant health needs; supporting its use as a transdiagnostic intervention (Brown et al., 2014; Byrne et al., 2021; Han et al., 2021; Juvin et al., 2022; Ruskin et al., 2021; Whittingham et al., 2016). These studies and reviews suggest that even very brief interventions can have psychosocial benefits for caregivers, including caregivers of children with autism (Blackledge & Hayes, 2006; Lunsky et al., 2018). A recent review revealed there are very few studies of ACT intervention in low-resource settings in general and none for caregivers of children with DD in Africa (Geda et al., 2021). Geda and colleagues suggest that there is some emerging evidence of the ability of non-specialists to implement ACT interventions and sound an urgent call for further studies of ACT in LMIC, including the role of non-specialists delivering ACT interventions in these settings.
The main ACT themes included in the WHO CST well-being module are (1) getting present; (2) identifying personal values; (3) small, committed actions one can take in line with these identified values; (4) ways to take care of yourself; (5) naming and noticing your thoughts and feelings; and (6) acceptance. The intervention is delivered by a trained specialist and/or non-specialist facilitators who meet once a week for 3 weeks with a group of caregivers. The 2-h sessions include stories, exercises and group discussions to convey key messages and skills to help car-egivers deal with stress and take committed action to support their mental health and well-being.
Our study was the first to adapt and evaluate the field-trial pre-publication version of the WHO CST Caregiver well-being module. We investigated whether this brief well-being programme was feasible, acceptable and showed promise of positive impacts when delivered to caregivers of children with DD in a rural South African town.
Overview of the broader study context and procedures
The limited human resources and financial limitations in LMIC require the utmost economy and creativity in the delivery and implementation of interventions (Murray et al., 2014). We conducted this study as part of a broader study entitled the Diamond Families Project, which aimed to investigate the WHO CST in a rural setting in South Africa. The Diamond Families Project used an implementation science approach, and the planning phase was characterised by a comprehensive set of implementation strategies to overcome multiple barriers to implementation that exist in the South African context. We discuss two important aspects in the planning of this study: adaptation of the original WHO CST well-being module materials and our task-sharing training model to begin addressing the need to include non-specialists in intervention delivery.
Adaptation of the WHO CST Caregiver well-being module
We used the pre-publication version of the WHO CST Caregiver well-being module that had a text-heavy script with a dense graphical layout that would have made facilitation of the programme very difficult in a local context. Non-native English-speaking caregivers and those with limited literacy found it difficult to follow the materials. Therefore, the main objective of our adaptations was to create user-friendly manuals for non-specialist facilitators and caregivers with varying levels of English language proficiency and literacy. South Africa has 11 official languages, but English is the predominant language used by the government, business and the media. Thus, for our context, we decided to develop simplified English versions rather than translate the materials into all official languages. Facilitators and caregivers needed to follow the English scripts with ease while still being able to do real-time translations where necessary. While the programme is delivered in English and the materials are written in English, the facilitators and caregivers are free to easily switch to their home language for a better explanation or expression. This type of code-switching (or language alteration) happens often and naturally in everyday conversations and interactions. It was also important to break down the dense manualised scripts into easy-to-navigate step-by-step instructions to support intervention fidelity.
We used a participatory approach throughout the adaptation process. Input and feedback were sought from specialists, non-specialists and caregivers who understood and were part of the local culture, language and context. The adaptations (e.g. designing a different set of illustrations) and modifications (e.g. changes in the graphical layout of the materials, using online- and in-person modalities and delivering the programme as a standalone intervention) resulted in the ‘Well-Beans for Caregivers’ programme. Using wordplay on the term ‘well-being’, we developed a fictional ‘Well-Beans Team’. A series of bean characters were included in the ‘team’, each representing a different group activity, making it easier for facilitators to navigate the different activities (see Figure 1). We simplified the text, reduced jargon and used locally relevant analogies and examples following the Adaptation and Implementation Guide for CST (WHO, 2022a). However, we also modified the graphic layout of the original WHO CST well-being module and adapted the manuals to allow both online and in-person delivery. Another significant modification was to use the module as a standalone intervention. Importantly, the core content and structure of the programme remained exactly the same.
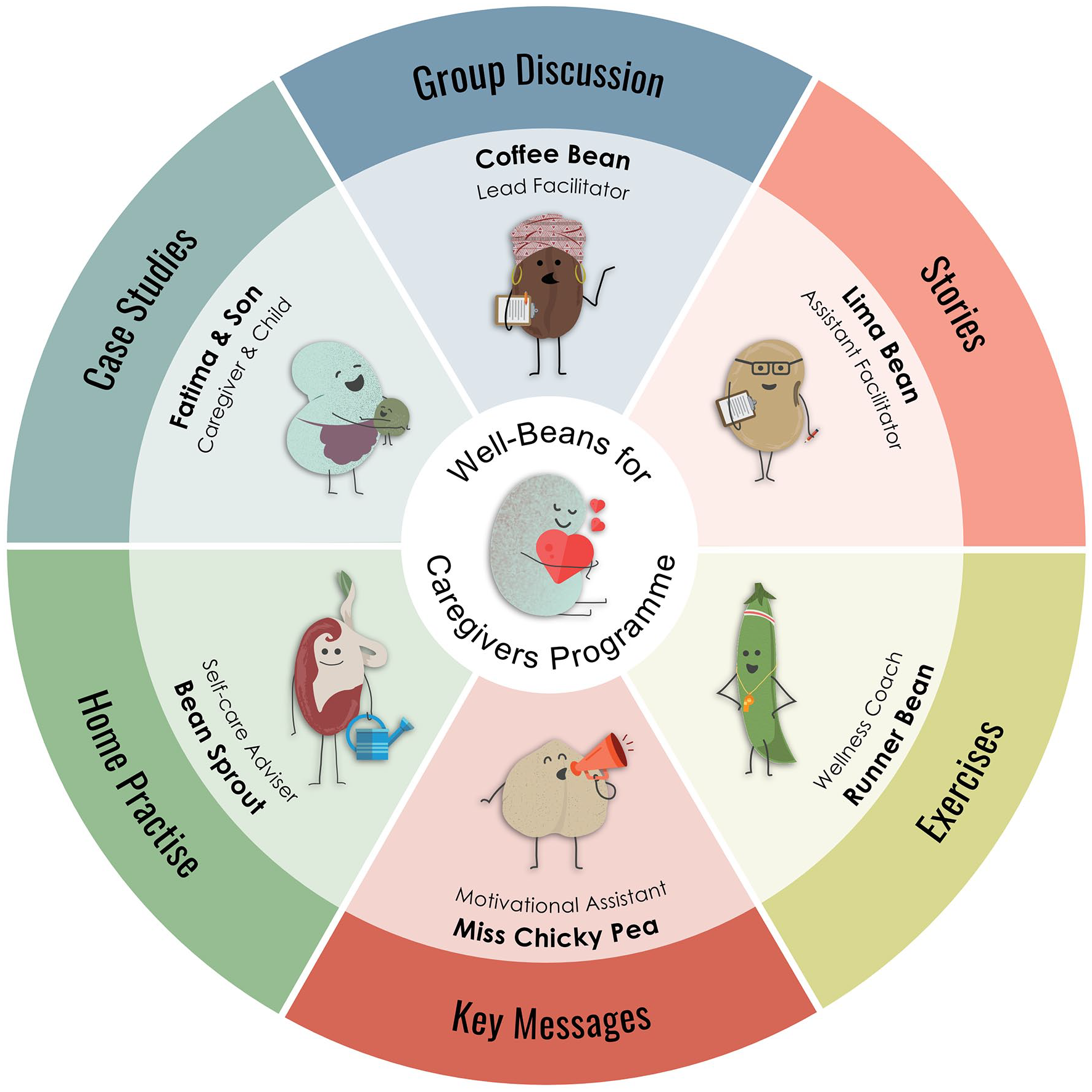
Characters of the ‘Well-Bean Team’ in the Well-Beans for Caregivers programme.
Task-sharing: training of specialist and non-specialist facilitators
ACT is embedded in relational frame theory (Hayes et al., 2013), which allows for a theoretical understanding of the psychological mechanisms that lead to improved well-being. Yet, it is possible to benefit from ACT without an in-depth knowledge of the theoretical underpinnings. Just like one might not need to know exactly how an engine works to drive a car, one can benefit from ACT without an in-depth knowledge of the theory and deliver a manualised intervention without an in-depth knowledge of the therapy. This makes ACT particularly suitable for LMIC, where there is a desperate shortage of individuals with mental health training (S. R. N. Simelane & de Vries, 2021). Task-sharing takes place where non-specialist facilitators (with little or no prior mental health training and often with little formal education) are trained to deliver simplified, manualised evidence-based interventions effectively with positive clinical outcomes, under supervision from more specialist practitioners. Task-sharing is well recognised as a feasible model in LMIC (Hoeft et al., 2018) and only just emerging for ACT interventions (Geda et al., 2021). A key principle of the WHO CST is a cascaded task-sharing training and supervision model that includes elements of both train-the-trainer and apprenticeship models (Salomone et al., 2019). One of the challenges of task-sharing is that individuals with limited training need more support. The apprenticeship model provides the added layers of support and supervision to address this challenge. In this model, training is a process that occurs over time (Murray et al., 2014).
To build a sustainable mental health workforce for the Well-Beans programme in the local community in this study, we adopted all these task-sharing, train-the-trainer and apprenticeship model principles. The training model included four groups: (1) an international ACT practitioner and supervisor, (2) specialist facilitators – community-based specialists who work actively in the public health disability-service sector, (3) non-specialist facilitators – community-based individuals from a national non-profit disability organisation and (4) non-specialist trainee observers – community-based individuals with a keen interest in child development and caregiver support. Training and intervention delivery took place in iterative concurrent phases (see Figure 2). The current study describes the third training and implementation evaluation phase. In this phase, the trained specialist facilitator delivered the intervention, the trained non-specialist facilitator was the co-facilitator (apprentice assistant) and four trainees learned through observing (trainee observers). We describe each group in more detail in the participant section.
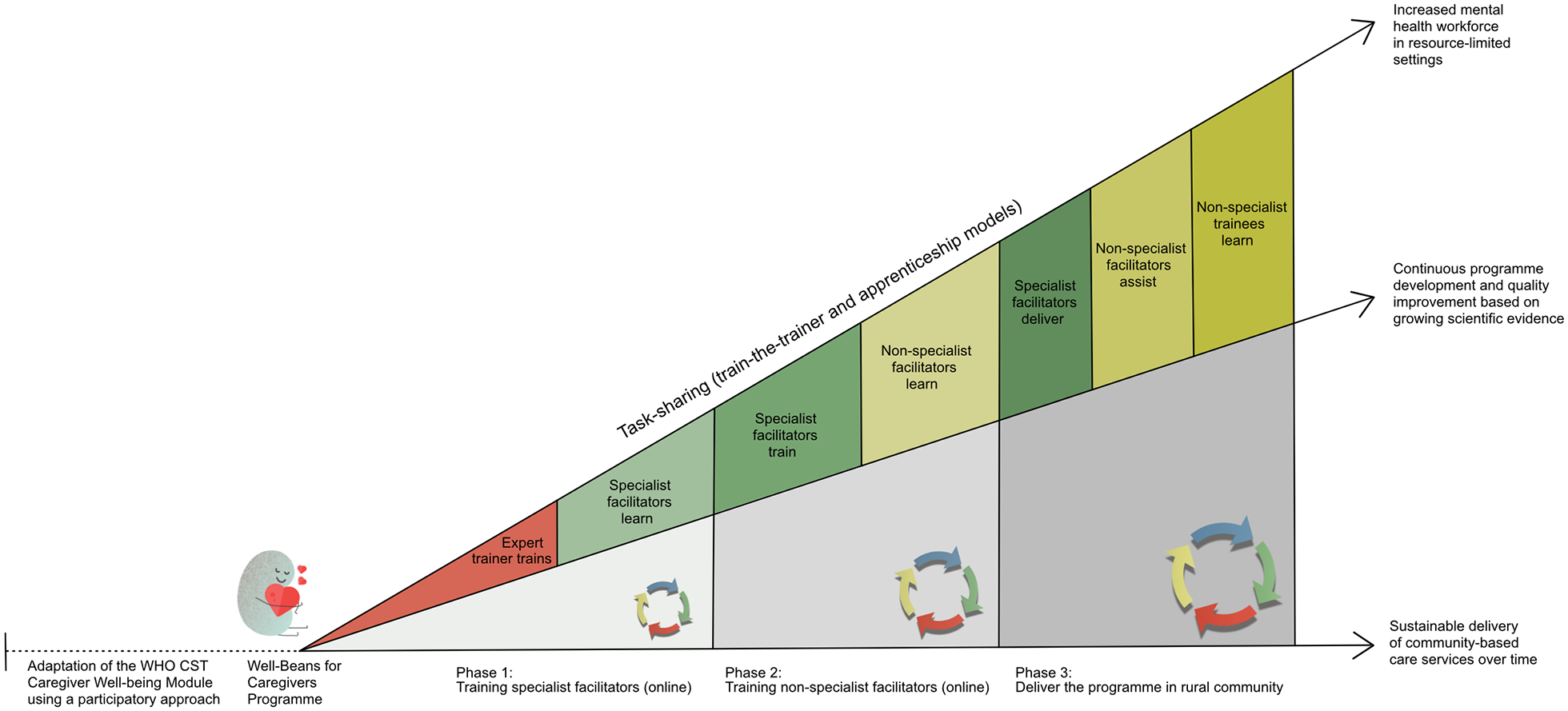
Overview of the Well-Beans study context and process.
Methods
Design
To explore the programme’s acceptability and feasibility, we used a descriptive study design including several measures and multiple informants (caregivers, facilitators and independent observers). We used a pre-/post-test study design without a control group to measure the potential effects of the intervention. The Research Committee of the University of Cape Town provided ethics approval, and all participants signed a consent form before participating in the study (Reference: 313/2020).
Study site
The ‘Well-Beans for Caregivers’ was delivered in a low-resourced, rural town in South Africa. Caregiver participants were recruited from a community site in Mahikeng, the capital city of the North West province of South Africa. The North West is home to about 1,382,000 children, and 67.1% of them live in income-poor households – living below the upper-bound poverty line of households with a monthly per capita income of less than R1183 (approximately 80 USD) in 2018 (Shung-King et al., 2019). Most households speak Setswana, one of the 11 official South African languages. Previous work in similar rural contexts in this province suggested that the population, in general, had low levels of psychological well-being (Khumalo et al., 2012; Koen et al., 2022). Although pockets of disability-related services were available within the province, most children with DD and their families had limited or no access to care.
Participants
Specialist facilitator
The specialist facilitator who delivered the programme was part of the first online training group that attended a 2-day training with an experienced ACT trainer and experienced the intervention with the trainer as a participant in the training phase 1 (see Figure 2). She was identified as a key specialist in the local community and played an active leading role in delivering the programme. She is an educational psychologist with doctoral-level training. She had over 30 years of experience working directly with families and children with developmental disabilities in clinical and research settings and was involved in the local Mahikeng community.
Non-specialist co-facilitator
A non-specialist co-facilitated the session. She is a mother of a child with autism, an employee of a national autism non-profit organisation (i.e. the organisational implementation partner) and from the local community. She attended the ‘Well-Beans for Caregivers’ programme as a participant during the second training phase (Figure 2). In her role as a regional development officer for the national autism non-profit organisation, she has gained experience in working directly with caregivers of children with developmental disabilities and often facilitates caregiver training courses.
Non-specialist trainee observers
Four non-specialist observers were included to observe the sessions as part of the apprenticeship training model. These non-specialist observers were from the local community. They were known by either the specialist or non-specialist facilitator and had either volunteered before or communicated an interest in child development and supporting parents in their communities. None of the observers had any formal training in child development or mental health.
Caregivers of children with DD
Caregivers were invited to participate in the study if they were older than 18, had a long-term caring responsibility for a child aged 2–11 years with DD and were either known to the specialist facilitator, non-specialist facilitator or a local paediatrician. We used a convenience sample to identify the caregivers and did not exclude any caregivers based on their prior mental health status. We also followed the recommended size of the caregiver group (i.e. 6–12 caregivers per group). While the typical age of children in the WHO CST programme is 2–9 years, we have adapted the age range to include children with DD up to 11 years of age based on the Adaptation and Implementation Guide for CST (WHO, 2022a). This included children with developmental delays, sensory impairments, intellectual disabilities and autism. In line with the philosophy of the WHO CST, no formal diagnoses were required. Apart from the outcome measures used in this study, we did not assess caregivers’ mental health as part of the participant selection process. We did not think it was ethical or socially responsible to exclude caregivers with existing mental health difficulties. To mitigate the risk, we have only invited caregivers known to either the specialist facilitator, non-specialist facilitator or the local paediatrician. While none of the caregivers received any prior direct mental health support from these individuals, we felt that an existing relationship with them would increase their willingness to reach out for further professional help should it be necessary. All families interested in participating in the study were asked to complete an informed consent form.
Caregivers completed a demographic form and the 23Q (Kakooza-Mwesige et al., 2014) – a 23-question screening questionnaire to confirm developmental concerns and briefly characterise the nature of the children’s difficulties. Table 1 summarises the description of the participating caregivers and their children.
Demographic characteristics of caregivers and children with disabilities (n = 10).
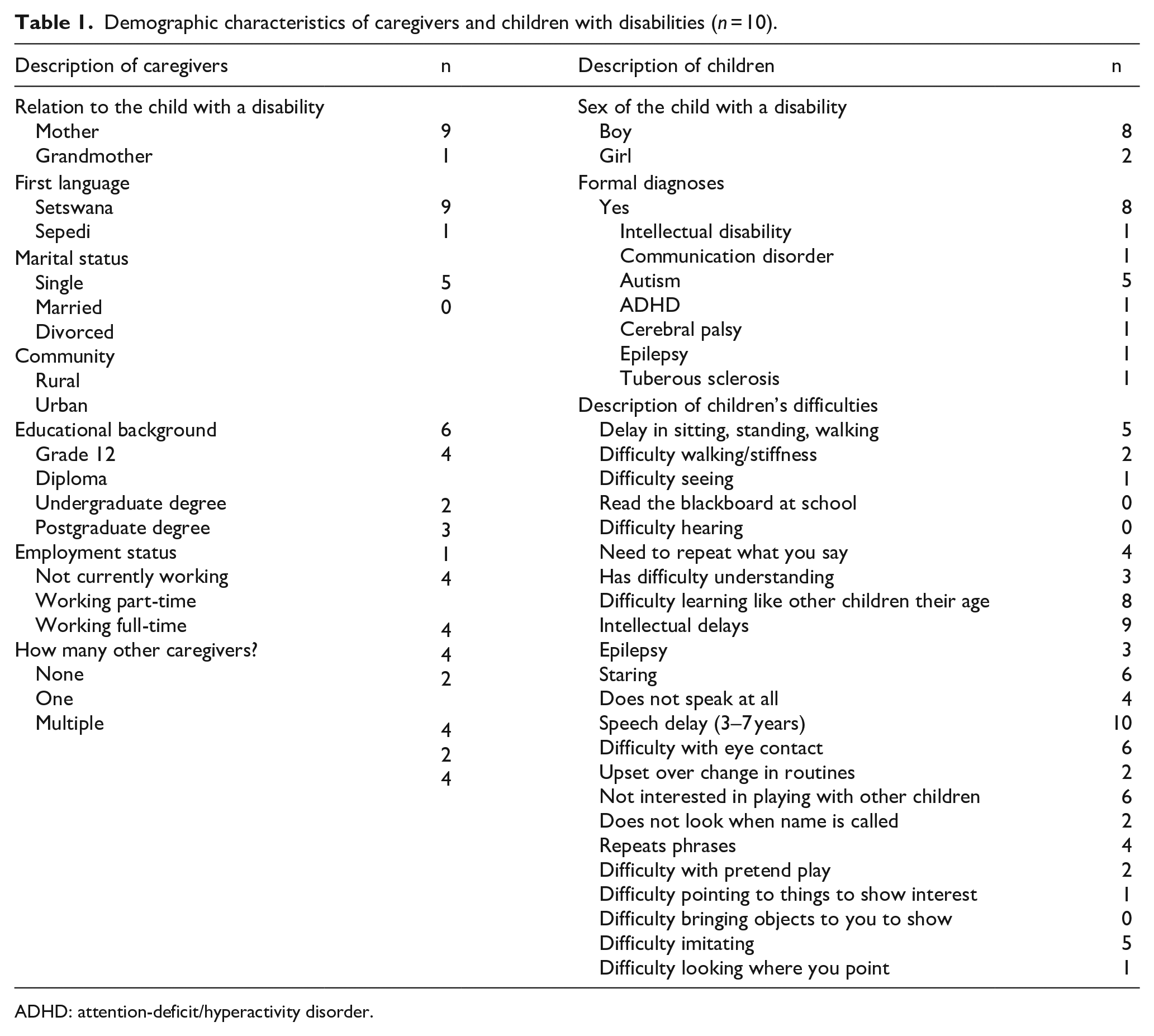
ADHD: attention-deficit/hyperactivity disorder.
Ten families consented to participate in this round of the programme. All caregivers were Black South African women, 10 mothers, and one grandmother, with a mean age of 41.27 years (SD = 11.07). Just over half the caregivers were single parents and just under half had no university education. Only two were in full-time employment outside the home.
Children
The overall mean age of the children cared for in this study was 8 years (SD = 2.36) with a range of 4–11. Only three children were of preschool age (4–6), while most were aged between 8 and 11. They were mostly boys (n = 8). Eight children in the sample had received a clinical diagnosis by a specialist clinician. Diagnosis included autism, intellectual disability, communication disorder, attention-deficit/hyperactivity disorder, cerebral palsy, epilepsy and tuberous sclerosis complex. The group’s most commonly reported child difficulty was speech delay (n = 10), and four of the children were reported not to use any words. Other reported difficulties included intellectual delays (n = 9) and difficulty learning like other children their age (n = 8). Many car-egivers reported difficulties consistent with ASD, such as difficulty with eye contact (n = 6), lack of interest in playing with other children (n = 6) and difficulty imitating (n = 5). Almost half also had developmental delays in their physical milestones of sitting, standing or walking (n = 5).
Intervention delivery
The specialist facilitator, non-specialist co-facilitator and non-specialist trainees (observers) met once a week in-person for three consecutive weeks for 2-h sessions with the group of caregivers. The sessions followed the scripts in the adapted facilitator and caregiver booklets. They included stories, exercises and group discussions to help convey the key ACT-informed messages and skills designed to help caregivers engage differently with their stressors and challenges and take small, committed actions in line with their values to support their emotional well-being. We provided small tokens of appreciation for attendance by offering a transportation fee for those caregivers who travelled by public transport and provided snacks.
Measures
Participants completed all measures electronically using the Research Electronic Data Capture (REDCap) tools hosted at the University of Cape Town (Harris et al., 2009). REDCap is a secure, web-based application designed to support data capture and had been developed during the online implementation of phases 1 and 2. It was especially helpful in this in-person phase 3, where the implementation site was at a distance from the university setting and could be assessed for feasibility in this rural setting. Caregivers completed all measures themselves via electronic links, usually on their smartphones. This was typically done at the venue where the sessions were held and where they had access to free Wi-Fi. Data vouchers were provided when this was not possible.
Feasibility
Attendance tracking
We tracked the attendance of caregivers and observers for the three sessions.
Completion rate of digital data collection
We calculated the proportion of all forms completed as a percentage of those sent to measure digital data collection feasibility. Most form links were sent to participants’ email addresses (n = 8), but where participants did not use email, links were sent via a messaging app WhatsApp (n = 2).
Feasibility of group sessions (rated by the specialist facilitator)
Session feasibility, in terms of the amount and comprehensibility of information covered in the session and the facilitator’s sense of preparedness in facilitating the session, were rated by the specialist facilitator directly after each group session using the WHO CST Group Session Feedback Form for Facilitators, a bespoke unpublished measure included in the WHO Measurement and Evaluation (M&E) Framework. The facilitator rated these constructs on a slider scale ranging from 0 to 100. Each question allowed for comments for each rating.
Competence of the specialist facilitator (rated by non-specialist facilitator and observer trainees)
This was rated for each session using the adapted ENACT (ENhancing Assessment of Common Therapeutic factors) (Kohrt et al., 2015) included in the WHO M&E Framework to measure the common competencies such as active listening, verbal tone, paraphrasing, rapport building, empathy and responding to caregiver’s feelings with validation/normalisation. Intervention-specific competencies were added, including ratings of logistical management of the group session, including review at the start of the session, content delivery, structuring and managing the session. Each item is rated on a scale of 1–4, where 1 represents a lack of competence in the skill, and 4 represents ideal competency. Mean scores are calculated by summing the ratings and dividing by the number of applicable items. Ratings were not checked for reliability or validity but were not shared with the facilitator to reduce socially desirable responses.
Acceptability
Acceptability of group sessions (rated by the specialist facilitator)
The facilitator rated each group session for its perceived relevance and acceptability to the caregivers and their agreement with the session content using the WHO CST Group Session Feedback Form for Facilitators. The facilitator rated these with a slider scale ranging from 0 to 100, and opportunities for comments were given for each question.
Acceptability of group sessions (rated by caregivers)
The WHO CST Group Session Feedback Form for Caregivers (adapted from Kasari et al., 2010) was used to evaluate aspects of acceptability. Caregivers completed it after each session. This form contains items assessing sessions for comprehensibility (how easy the session was to understand), relevance to the caregiver and their child, and a rating of how closely the session’s messages agreed with the caregivers’ personal and family values, all rated on a 5-point scale. Open-ended questions were also provided for any unsolicited feedback from caregivers.
Potential impact
We utilised a range of measures to characterise participants’ psychological flexibility and well-being before and after the intervention to assess the potential impact of the intervention. Given that this study was set up as a pilot, it has a very small sample size, and there was no control group. We consider these measures as evidence of potential impact or potential signals of change. Measures were selected based on the programme’s aims, that is, to improve overall well-being through acceptance and commitment therapy and if they were open access and freely available. Previous use in South African samples was also considered. All measures were self-completed by participants in their original English, but the facilitators and observers were present to assist.
Acceptance and Action Questionnaire II
A measure of cognitive flexibility, which is the primary target of ACT (Bond et al., 2011). It has seven items, each rated on a 7-point scale (1–7). The total score is a sum of the seven items, and higher scores indicate higher levels of psychological inflexibility. Cronbach’s alpha for this sample was 0.90, suggesting excellent internal consistency.
Patient Health Questionnaire
A measure of depression severity that has been used extensively in South Africa (e.g. Kroenke et al., 2001; Makhubela & Khumalo, 2022). It has nine items, each rated on a 4-point scale (scores ranging from 0 to 3). Scores are summed into a total score. Higher scores indicate greater depression. Cronbach’s alpha for this sample was 0.80, suggesting good internal consistency.
Generalised Anxiety Disorder 7-item Scale
To assess car-egivers’ degree of anxiety. It has also been used extensively in South African samples (e.g. Tadi et al., 2022) and has seven items, each rated on a 4-point scale with scores from 0 to 3 (Spitzer et al., 2006). The total is the sum of each individual score. Higher scores indicate greater anxiety. Cronbach’s alpha for this sample was 0.91, suggesting excellent internal consistency.
Multidimensional Scale of Perceived Social Support
This is a measure of the caregiver’s perceived support from prominent people in their lives and was selected to identify support as a strategy covered in the programme, and the measure has shown validity and reliability in other South African samples (Bruwer et al., 2008; Zimet et al., 1990). It has 12 items; each scored on a 7-point scale with scores from 1 to 7 and yields three sub-scores reflecting perceived support from a significant other, family members and friends and a total score. Sub-scale and total scores are mean totals. Higher scores indicate greater perceived support. Cronbach’s alpha for this sample was 0.83, suggesting good internal consistency.
Family Impact of Childhood Disability Scale
A measure of how a child’s disability impacts the family (Trute et al., 2009). This measure has 20 items consisting of 10 positive and 10 negative statements, each rated on a 4-point scale with scores ranging from 1 to 4. The positive and negative total scores are sum scores. Higher scores indicate more positive appraisal and more negative appraisal, respectively. Cronbach’s alpha for the positive subscale was 0.79 and 0.87 for the negative, suggesting acceptable to good internal consistency. This measure was selected as it has shown promising reliability and validity in a sample of South African parents of children with autism and because positive appraisal of disability may increase as a result of the programme (Schlebusch & Dada, 2018).
Brief Measure of Parental Well-being
A short measure of subjective well-being selected for its high face validity and pragmatic value (brevity) (McConkey, 2020). It includes eight items on health, stress and quality of life, each rated on a 10-point scale with scores ranging from 1 to 10. The total score is the sum of the eight items. Higher scores indicate better well-being. Cronbach’s alpha was 0.91 for this sample, suggesting excellent internal consistency.
Data analysis
We used descriptive statistics for the quantitative data on the feasibility, acceptability and potential effects, including a word cloud analysis for responses to open-ended questions. Due to the small sample size, the non-parametric Wilcoxon Signed Ranks Test for repeated measures was used to consider potential evidence of change, and the non-parametric effect size index:
Statement on community involvement
The Diamond Families Project was a multi-partner project which included community involvement from research, non-profit and governmental sectors. The adaptation of the WHO CST caregiver well-being module into the ‘Well-Beans for Caregivers’ programme specifically, as well as the training and apprenticeship model, also included extensive consultation with community members, including caregivers of children with DD that represented eight of the nine provinces in South Africa.
Results
Feasibility
Attendance rates
Attendance rates for the three sessions were 91%, 100% and 91% for sessions 1, 2 and 3, respectively.
Form completion rates
There was 100% digital form completion in response to links sent to caregivers, facilitators and observers. In total, caregivers completed nine links – four links before the intervention (demographic and assessment forms), a feedback form link after each session (three links) and another two links for post-intervention well-being measures. The specialist facilitator, non-specialist facilitator and observers completed four links each (a demographic form and one feedback form per session).
Feasibility of group sessions’ delivery (rated by the specialist facilitator)
The facilitator gave high ratings for the comprehensibility of the content delivered in each session, the amount of content delivered according to the manuals, and her sense of preparation to facilitate each session supported by her comments on these constructs (see Table 2). Following each session, the facilitator also gave very high ratings of her sense of competence to facilitate the sessions (M = 92.67; SD = 6.43) and train someone else to facilitate the sessions (M = 93.33; SD = 4.51).
Feasibility of group sessions (rated by the specialist facilitator).
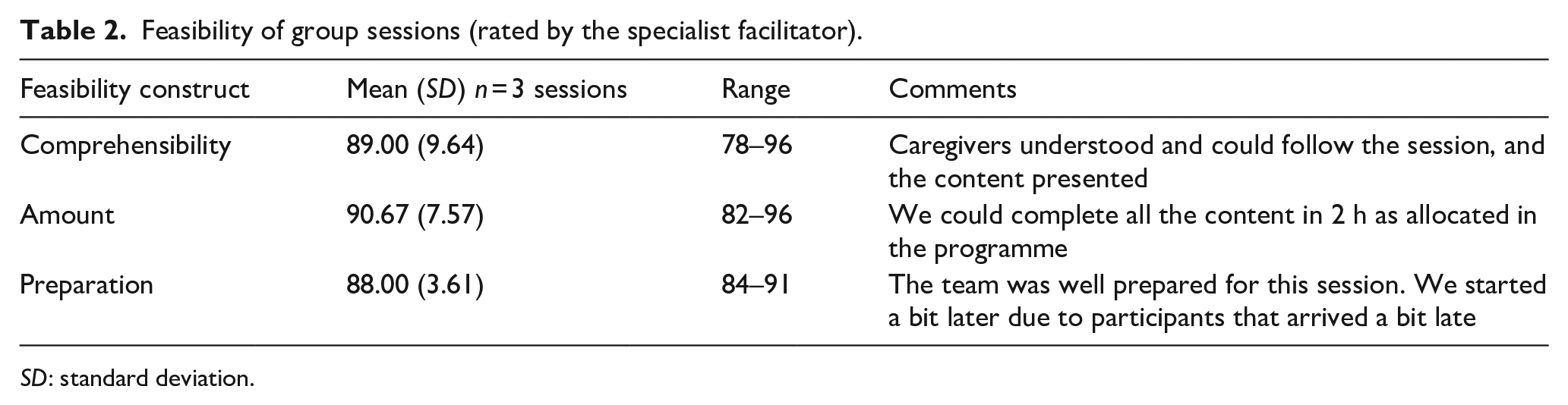
SD: standard deviation.
Competency of the specialist facilitator
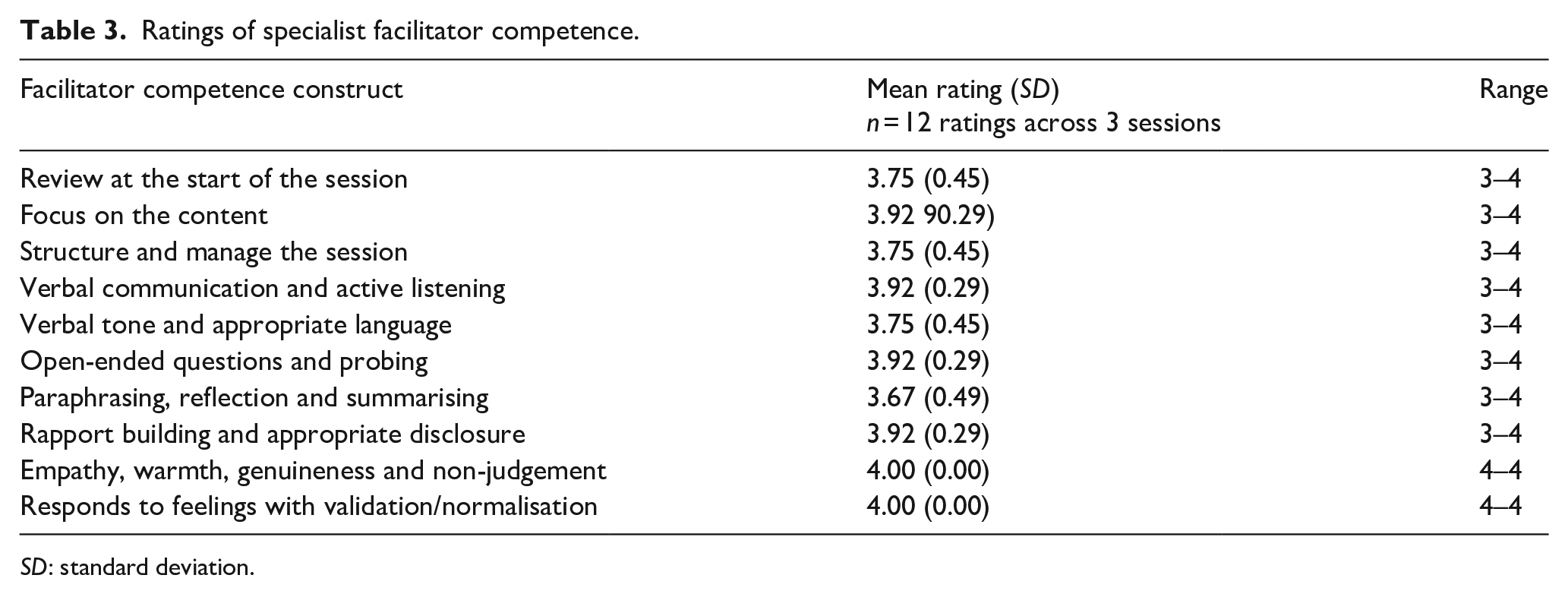
Ratings of the facilitator competency are summarised in Table 3. Ratings across the non-specialist facilitator and observers for the three sessions were generally high and varied between ratings of 3 (done adequately) and 4 (done well). Ratings of empathy and warmth were unanimously rated as 4. An open-ended comment by the co-facilitator of the facilitator illustrates these high ratings as follows: I think (specialist facilitator) is a natural at this as her tone of voice is just perfect and warm. She has a sense of engaging the caregivers and making them feel safe to share and let go. We had a very emotional session as one parent cried and two others were teary thus showing that these sessions work and are reaching caregivers’ hearts.
Ratings of specialist facilitator competence.
SD: standard deviation.
Acceptability
Acceptability of group sessions (rated by specialist facilitator)
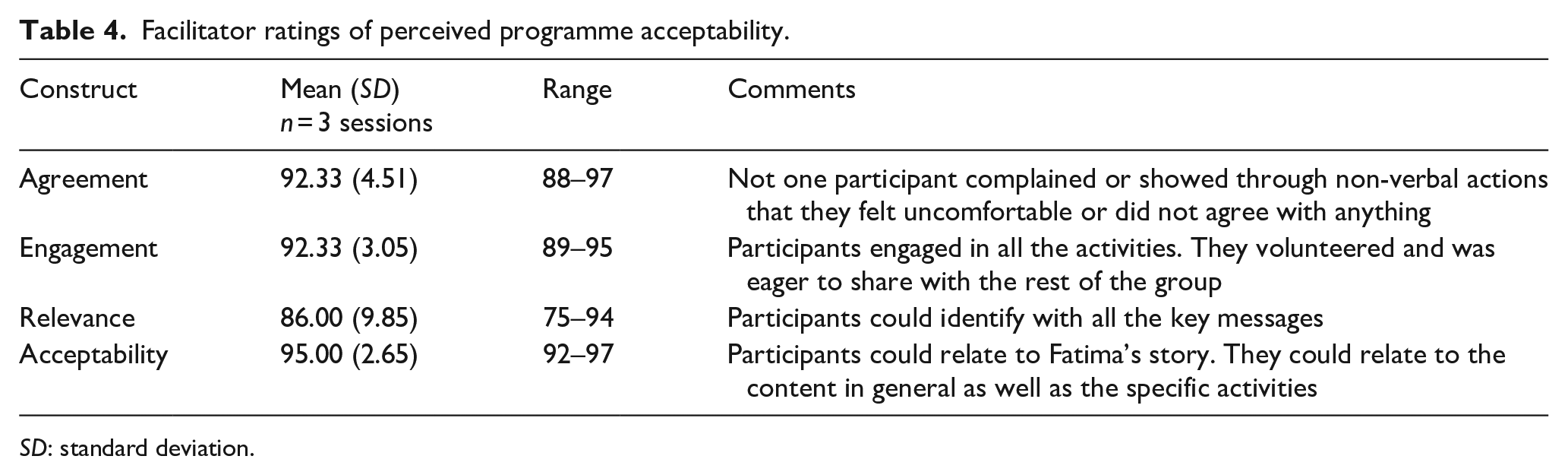
The facilitator gave high ratings of perceptions of the acceptability of the course to caregivers. Her ratings and illustrative comments are summarised in Table 4.
Facilitator ratings of perceived programme acceptability.
SD: standard deviation.
Acceptability of group sessions (rated by caregivers)
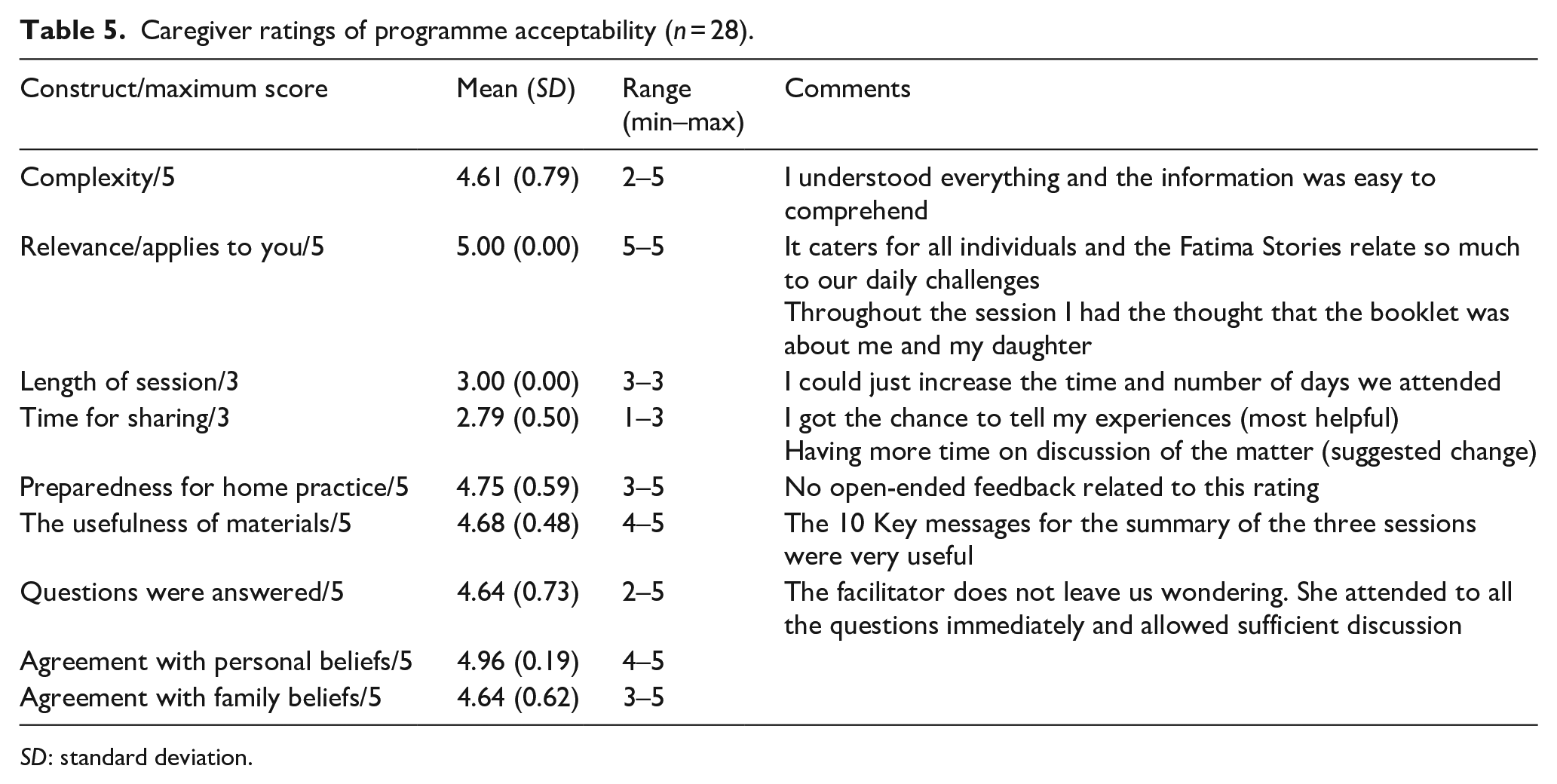
Caregivers also gave high ratings of acceptability constructs (see Table 5). Although everyone reported being satisfied with the length of the session, one of the lower ratings was for ‘time for sharing’. Recommendations in the open-ended comments all related to wanting more time for sharing and group discussion.
Caregiver ratings of programme acceptability (n = 28).
SD: standard deviation.
In response to the open-ended question ‘What was most useful to you in this session?’, caregivers gave many detailed comments highlighting the benefits of different facets of the programme. A prominent comment was an appreciation of the opportunity simply to share their experiences within a supportive group, for example, ‘I got the chance to tell my experiences’, as well as to listen to other caregivers’ experiences, for example ‘The stories caregivers share about their feelings and experiences’, which together reinforced a strong sense of ‘I’m not alone on this journey’. It is noteworthy that no recommendations for changes were suggested for 21 of 31 session ratings.
Other open-ended comments highlighted specific features of the programme that were helpful to caregivers and included most of the ACT constructs included in the programme, including ‘knowing how to deal with my stress’, ‘identifying thoughts and feelings’, ‘accepting my situation and allowing myself to move on’, ‘I can start to think about important things [rather] than things I can’t change’, ‘values for caregivers and taking one step at a time’, ‘being present’, and ‘tips on being able to take care of myself as a caretaker’. The responses to the open-ended question ‘What was most useful or helpful to you?’ were consolidated in a word cloud. As illustrated in Figure 3, the comments on acceptance, thoughts, feelings and values were mentioned most often by the caregivers.
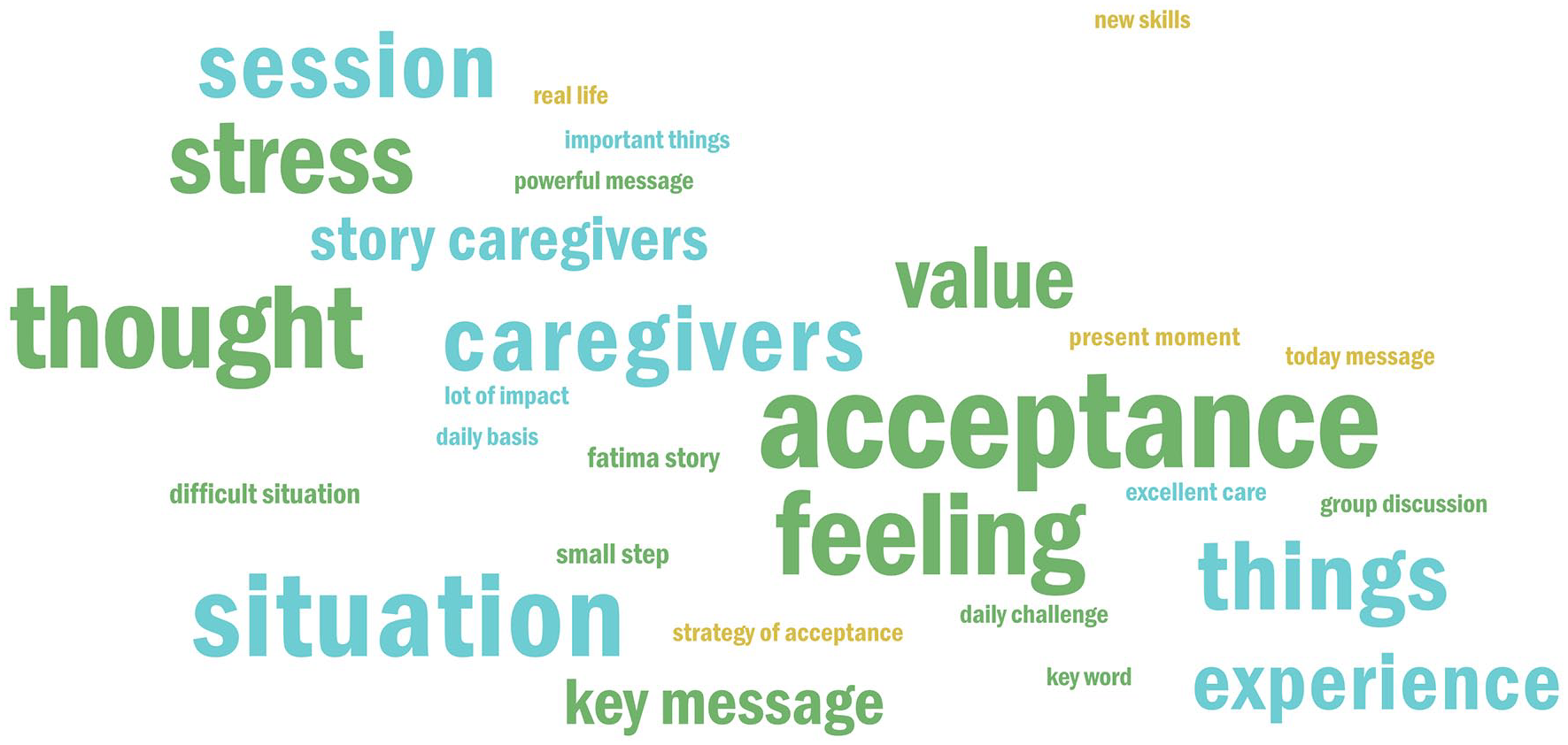
The relative prominence of concepts reported as useful to caregivers following the sessions.
The usefulness of the key concept of acceptance is exemplified in the following comments: Acceptance does not mean liking the situation or giving up but concentrating on the things to be changed. This is the most powerful message to take home and practice. Throughout the session, I had the thought that the booklet was about me and my daughter, and session 3 made a lot of impact as Acceptance is my keyword.
Potential impact
The mean pre- and post-intervention scores on the quantitative parent-report measures are presented in Table 6, along with the non-parametric change analyses. The pre-intervention mean scores fell in the moderate range for depression on the patient health questionnaire (PHQ) and just below the moderate range cut-off (10) for anxiety on the generalised anxiety disorder (GAD). The pre-intervention mean score on the Acceptance and Action Questionnaire-II (AAQ-II) was also within the range suggestive of clinically relevant psychological distress (Bond et al., 2011). Post-intervention, all mean score changes were in the expected direction (i.e. indicating a positive change from pre- to post-intervention) and large effect sizes were noted for changes in PHQ-9, GAD-7, Perceived Social Support (PSS) (significant other subdomain and the total score), and rating of positive impacts of the child’s disability on the family (FICD). Clinically, the mean scores of the post-intervention AAQ-II and GAD-7 fell below levels for clinical concern, while the depression mean score on the PHQ-9 fell into the ‘mild’ category. Statistically, change in one measure was significant according to Wilcoxon’s signed ranks test, namely the positive appraisal of the impact of childhood disability on the family, indicating more positive appraisal following the programme.
Pre- and post-intervention scores (n = 10).
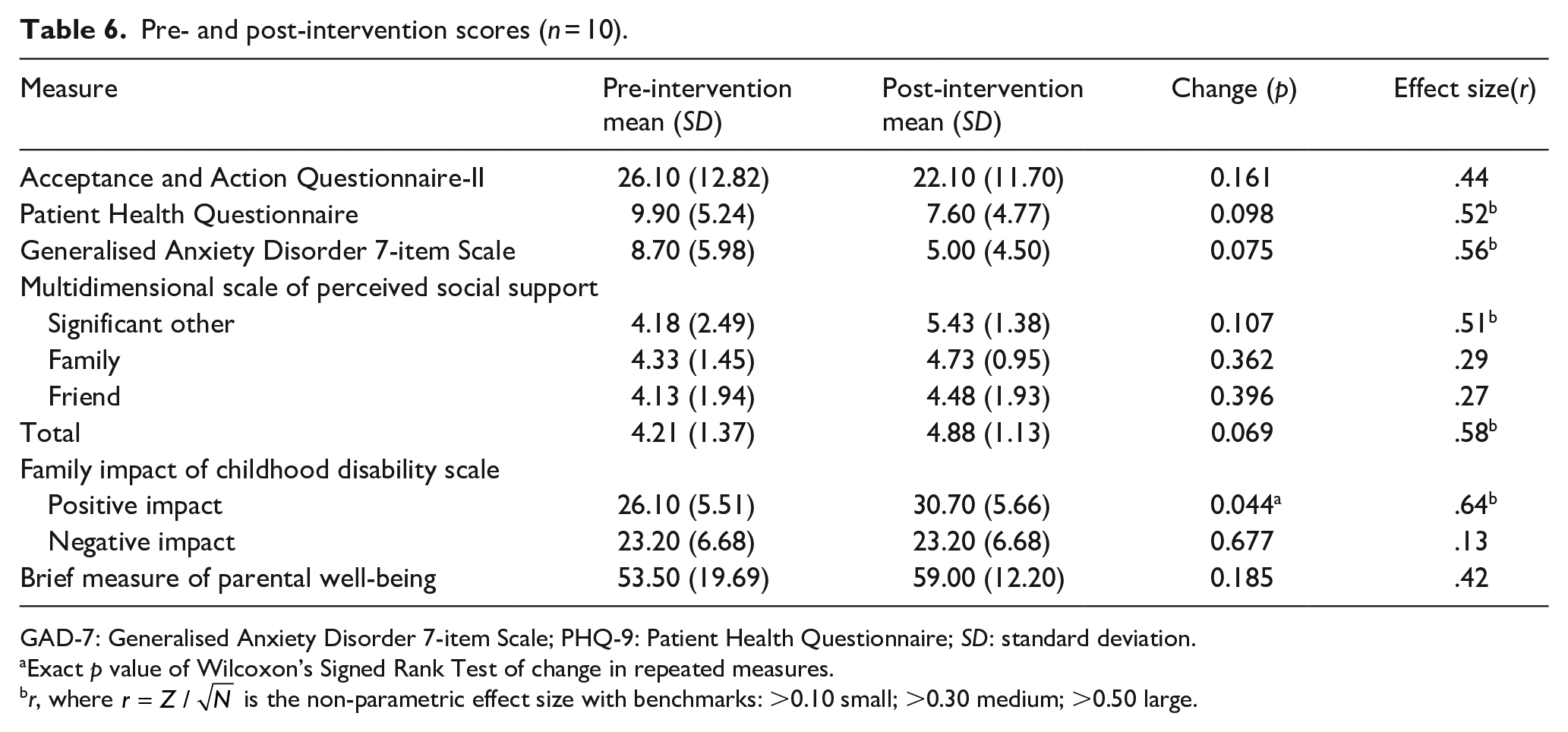
GAD-7: Generalised Anxiety Disorder 7-item Scale; PHQ-9: Patient Health Questionnaire; SD: standard deviation.
Exact p value of Wilcoxon’s Signed Rank Test of change in repeated measures.
r, where
Discussion
Many children in LMIC have DD, and the burden on caregivers is vast. Efforts such as the WHO CST have started to provide caregivers with skills and knowledge to promote their children’s learning. However, little attention has been paid to caregiver well-being and their capacity to care for their children. As a starting point, and part of our larger Diamond Families Project evaluating the WHO CST, we decided to focus on the ACT-informed caregiver well-being module. Using a participatory approach, we adapted this module into a contextually appropriate ‘Well-Beans for Caregivers’ programme. We embedded the training for and delivery of the programme within an iterative train-the-trainer and apprenticeship model with both specialist and non-specialist providers. In this study, we found that the Well-Beans programme was feasible, acceptable, and potentially effective when delivered to a group of 10 caregivers in a low-resourced rural setting in South Africa.
The inclusive group modality of the programme was a good fit for the participants. The tendency to focus interventions exclusively on one established diagnostic category (e.g. autism) may be a barrier to the sustainability of services in LMIC. The WHO CST programme that uses an inclusive transdiagnostic approach and includes children without a formal diagnosis enhances its potential applicability in LMIC. Although the caregivers who participated in the study had children with different difficulties, they shared many commonalities and could all relate to the programme.
Although it was beyond the scope of this study to evaluate the impact of factors influencing the feasibility and acceptability of the programme, we do want to recognise the motivation, commitment and openness to learning of the whole group. The group displayed a strong sense of coherence that may have contributed to high attendance and digital form completion rates. The comprehensiveness and clarity of the manuals could potentially contribute to other field-testing initiatives of the WHO CST programme in the region and beyond and support rapid dissemination and possible scale-up of the intervention. The ratings of the specialist facilitator’s competence demonstrate an active ingredient of the apprenticeship model, where a specialist facilitator is modelling the skills needed for successful group facilitation. The WHO CST programme’s task-sharing training approach could potentially be a helpful approach to build a non-specialist mental health workforce in the local community by investing in community-based individuals. It is also important to note that the programme’s feasibility was supported by using existing platforms and people in the community. Both practices could support rapid scale-up in other communities.
The cultural fit of an intervention is critical for uptake and sustainability (Schlebusch et al., 2020). Evidence on the acceptability and cross-cultural relevance suggests that the ‘Well-Beans for Caregivers’ programme adapted from the WHO CST caregiver well-being module was acceptable in a rural South African town and that existing models of cultural adaptation (i.e. modifying the peripheral elements of the original programme) enhanced acceptability. Both the specialist facilitator and the caregivers indicated high ratings of acceptability and relevance. The open-ended feedback from caregivers supports the quantitative findings, and caregivers were able to give detailed feedback highlighting the different facets of the programme that they felt were most helpful. Of particular importance was the aspect of acceptance. The programme helped caregivers accept situations they could not change and take small steps consistent with their values to realise their own potential and cope with life’s stresses.
The high rate of mental health problems among caregivers of children with autism and other developmental disabilities in LMIC is not surprising, given the high prevalence of many risk factors and other stressors and is consistent with previous studies in similar communities (Khumalo et al., 2012; Koen et al., 2022). Failing to meet their needs carries a significant cost of lost human potential. Our small group of caregivers reported high levels of psychological distress, depression and anxiety before the programme. After the programme, caregivers showed positive improvements in the expected directions on all the mental health and well-being measures. We noted statistically significant changes on the Positive Appraisal of the Family Impact of Childhood Disability Scale with a large effect size. This suggests that the intervention may allow caregivers to perceive and appreciate more positive benefits of having a child with a disability.
Limitations and future recommendations
In a setting where services were highly limited, we cannot discount the real possibility of caregivers providing socially desirable responses simply because they were able to access this service. We used multiple informants to mitigate this phenomenon. Due to the small sample size, a careful interpretation of the clinical impact of the intervention is warranted, and effect sizes should be considered in light of limitations. The effect size for the change in the AAQ-II indicated a moderate effect, even though it was not statistically significant. Ideally, more efficacy and effectiveness evaluations are needed, and future studies should be designed according to a hybrid evaluation and implementation model that includes dissemination and implementation outcomes (Curran et al., 2012). An important next step is to replicate and expand these early findings.
Because this was the very first time to explore the feasibility and acceptability of using the ‘Well-Beans for Caregivers’ adaptation of the CST well-being module as a standalone intervention, the specialist facilitator played an active leading role in the delivery of the programme, while the non-specialist facilitator played a supporting role only in the group discussions. We did not ask the non-specialist facilitator to complete the group feedback feasibility form. The consideration of non-specialist facilitators facilitating the programme would be the next step.
All our participants were mothers who were already connected to some form of disability-related information or services. Looking at ways to increase engagement, attendance and motivation for those caregivers who are not already accessing services will be an important next step. Although fathers were not excluded from the invitation to participate in the study, it is typical that the caregiving responsibility mainly falls onto mothers. Special efforts to include fathers in future studies should be prioritised. Similarly, most of the children were between 8 and 11 (only three were between 4 and 6 years old). Therefore, future studies could explore whether the feasibility, acceptability and potential impact will be different for caregivers of much younger children.
As is often the case in LMIC, we provided small tokens of appreciation for attendance which might have helped to increase the feasibility (Murray et al., 2014), although we did not directly assess the potential impact. We offered a transportation fee for those caregivers who travelled by public transport and provided snacks as appreciation. It is important for future studies to take this into consideration, particularly in resource-limited communities where transport costs can be a direct barrier to attendance.
Another important observation is that our training model included training by an experienced specialist with a strong background in ACT as a first step. This could be a barrier for many LMIC countries or communities that do not have access to such a skilled professional. However, the suitability of using an online training platform can potentially overcome this challenge by allowing access to international experts, thus making more efficient use of the available human resources.
Conclusion
The ‘Well-Beans for Caregivers’ adaptation of the WHO CST Caregiver well-being module shows promise as a feasible, acceptable and potentially effective intervention for improving caregiver mental health and well-being in communities in South Africa with the potential to be implemented widely and sustainably.
Footnotes
Acknowledgements
The authors gratefully acknowledge the WHO CST Team (Felicity L. Brown, Laura Pacione, Erica Salomone, Stephanie Shire, Chiara Servili), Andy Shih and Pamela Dixon, and the Diamond Families Team (Manthipi Molamu, Krish Shunmugam, Jonathan Govender, Sandy Uswald, Juliet Carter, Dineo Mosiane, Tumelo Leeuw, Claudia Ceresa, Zanmari Norman, Jaco Dreyer, Rehana Effendi, Hanlie Degenaar and her team, David Griesel, and his team). Thank you for fulfilling your essential part towards this project.
Author contributions
The study was conceptualised and planned by L.S., N.C. and P.J.d.V. Training in the ACT model was provided by D.R., and the intervention was delivered by P.E. N.C. contributed to data analysis and all authors contributed to manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics approval for the study was obtained from the University of Cape Town (HREC Ref 313/2020).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study is part of a broader project (the Diamond Families Project) partnered between the National Department of Social Development, Autism South Africa, and the Centre for Autism Research (CARA) at the University of Cape Town. Funding for this project was received from the National Department of Social Development (Fund number 10/2/48/2018/19 Rights of Person with Disabilities).