
Abstract
Autistic people experience more health conditions and earlier mortality. This study investigated views about a primary care health check for autistic adults to inform its design. Fifty-one people participated in consultation groups and interviews, comprising autistic adults (some with co-occurring intellectual disabilities), adults with intellectual disabilities, supporters and health professionals. Participants wanted the health check to cover physical and mental health and social functioning. They emphasised the importance of sharing information about individual needs and associated adjustments before the health check. They highlighted the need to change the way healthcare services communicate with autistic people, such as reducing phone contact and booking appointments online. They wanted individual choice in how the health check was completed, with video call or email offered alongside face-to-face. Participants raised the need for further training of primary care staff on autism, to highlight the diversity of experiences of autistic people and ways in which difficulties, such as pain, may present differently. Clinicians raised questions about the capacity of mental health and social care services to meet the additional needs potentially identified through the health check. This study represents a key step in the development and co-design of a UK primary care health check for autistic people.
Lay abstract
Autistic people are on average more likely to experience poor health than people who are not autistic. Health checks have been shown to improve access to effective healthcare. This study investigated people’s views about a primary care health check for autistic adults. We held discussion groups and interviewed autistic adults, adults with intellectual disabilities, supporters and health professionals. People wanted the health check to look at a person’s physical and mental health, and how they were doing socially. They thought people should be able to share information about their needs and the reasonable adjustments they would like before the health check. They wanted healthcare services to change the way they communicate with autistic people, such as being able to book appointments online rather than by telephone. They wanted a choice in how the health check was completed, with video call or email offered as well as face-to-face appointments. People thought further training of primary care staff on autism was needed, to increase awareness of the diversity of experiences of autistic people and ways in which difficulties, such as pain, may present differently to non-autistic people. Clinicians raised questions about whether mental health and social care services could meet the additional needs that might be identified through the health check. We used this information to design an NHS primary care health check for autistic people in collaboration with autistic people, supporters and health professionals.
Some mental and physical health conditions are more prevalent in autistic people than in non-autistic people (Croen et al., 2015; Hand et al., 2020; Rydzewska et al., 2021), leading to increased morbidity and earlier mortality (Hirvikoski et al., 2016; Schendel et al., 2016). Autistic people also have greater unmet healthcare needs and lower receipt of preventive health services, despite overall greater healthcare use (Gilmore et al., 2022; Zerbo et al., 2019). Such disparities may be partly explained by barriers preventing effective healthcare access, most notably challenges in interpersonal communication, sensory sensitivities and healthcare providers’ lack of autism knowledge (Mason et al., 2019; Nicolaidis et al., 2013).
Health checks can improve effective healthcare access for individuals with intellectual disabilities (Cooper et al., 2014; Lennox et al., 2007) and people at high risk of cardiovascular diseases (Mytton et al., 2018). A health check specifically developed for autistic people could address health inequalities and improve quality of life through improving access to and engagement with primary care services.
Researchers and clinicians have developed health assessment approaches for autistic people. In Australia, the Comprehensive Assessment Program (CHAP) (Lennox et al., 2007, 2010; Lennox, McPherson, et al., 2016), developed for people with intellectual disability, was adapted for autistic people with a co-occurring intellectual disability, although this has not undergone efficacy testing (Lennox, Urbanowicz, & van Dooren, 2016). Studies found the original CHAP led to increased health promotion, identified new health needs, health monitoring and improved disease prevention (Lennox et al., 2007, 2010). In the United States, the Academic Autism Spectrum Partnership in Research and Education (AASPIRE) used a community-based participatory research approach to develop the AASPIRE Healthcare Toolkit including an online set of resources and tools to help autistic people access primary health care. The centrepiece of the toolkit is the Autism Healthcare Accommodations Tool (AHAT), which allows autistic adults to create a customised report of reasonable adjustments to share with their healthcare provider. In preliminary studies, autistic adults reported fewer barriers to care, increased satisfaction with patient-provider communication and increased healthcare self-efficacy after using the Toolkit (Nicolaidis et al., 2016).
In the United Kingdom, Cooper et al. (2014) developed and evaluated an annual health check for people with intellectual disability. Annual health checks for people with intellectual disabilities have become part of routine care for people with intellectual disabilities in the United Kingdom to identify unmet health needs and increased access to healthcare services. However, this health check may not meet autistic peoples’ needs.
At a 2017 research priority-setting workshop held at Newcastle University, UK, autistic people, supporters and health professionals prioritised research to create and evaluate a health check for autistic people (Warner et al., 2018). Recent healthcare policy in England has also advocated for the development and evaluation of health checks for autistic people (as part of the NHS Long Term Plan and National Strategy for Autistic Children, Young People and Adults) (GOV.UK, 2021; NHS, 2019).
To meet this research priority, we undertook research to scope whether there is a need for a primary care health check for autistic adults (Mason et al., 2022) and to co-design and evaluate a health check. This article describes the design stage of the research (https://research.ncl.ac.uk/autismhealthchecks) including qualitative research findings from the co-design process. Our research objectives were to: (1) understand the views of autistic adults, adults with intellectual disabilities, supporters, and professionals about a health check for autistic adults and (2) use this information to design a health check that met the needs and preferences of all stakeholders.
Methods
We used an experience-based co-design method, which engages end users and encourages their active involvement through a collaborative partnership among users, practitioners and researchers (Ward et al., 2018). Health check development (a pre-appointment questionnaire and a health check appointment template) was iterative. The research team used the information gathered through multiple consultation groups and interviews to make decisions about content, structure and language. Information on the content and processes of other relevant health checks were taken into account during this process. We shared reiterations of the pre-appointment questionnaire and health check appointment template with participants in subsequent groups to gather their views, leading to further development. When there was a lack of consensus among or between stakeholder groups, the research team discussed the issue further and reached a decision.
Participants
Participants were from four populations: (1) autistic adults with and without intellectual disabilities (aged ⩾18 years); (2) adults with an intellectual disability who were not autistic (aged ⩾18 years); (3) supporters of autistic adults; and (4) primary care health professionals working with autistic adults (referred to as ‘clinicians’). While we created a health check for autistic adults because the health check developed for people with intellectual disability may not adequately meet all the needs of autistic people, the literature suggests there are likely to be at least some consistencies in the barriers to accessing effective healthcare experienced by autistic people and individuals with intellectual disabilities (Doherty et al., 2020). We included adults with intellectual disabilities who were not who may have received a biopsychosocial health check or had discussions with others who had attended an annual health check (Cooper et al., 2014). Community organisations and local clinical networks recruited participants in North East England. Fifty-one people took part: 45 in consultation groups and 6 through individual interviews. This comprised 31 autistic adults (including 6 with a co-occurring intellectual disability), 8 adults with an intellectual disability who were not autistic, 7 supporters and 5 clinicians. Table 1 shows participant characteristics (gathered by self-report questionnaire; data on ethnicity and socioeconomic status were not recorded).
Participant characteristics.
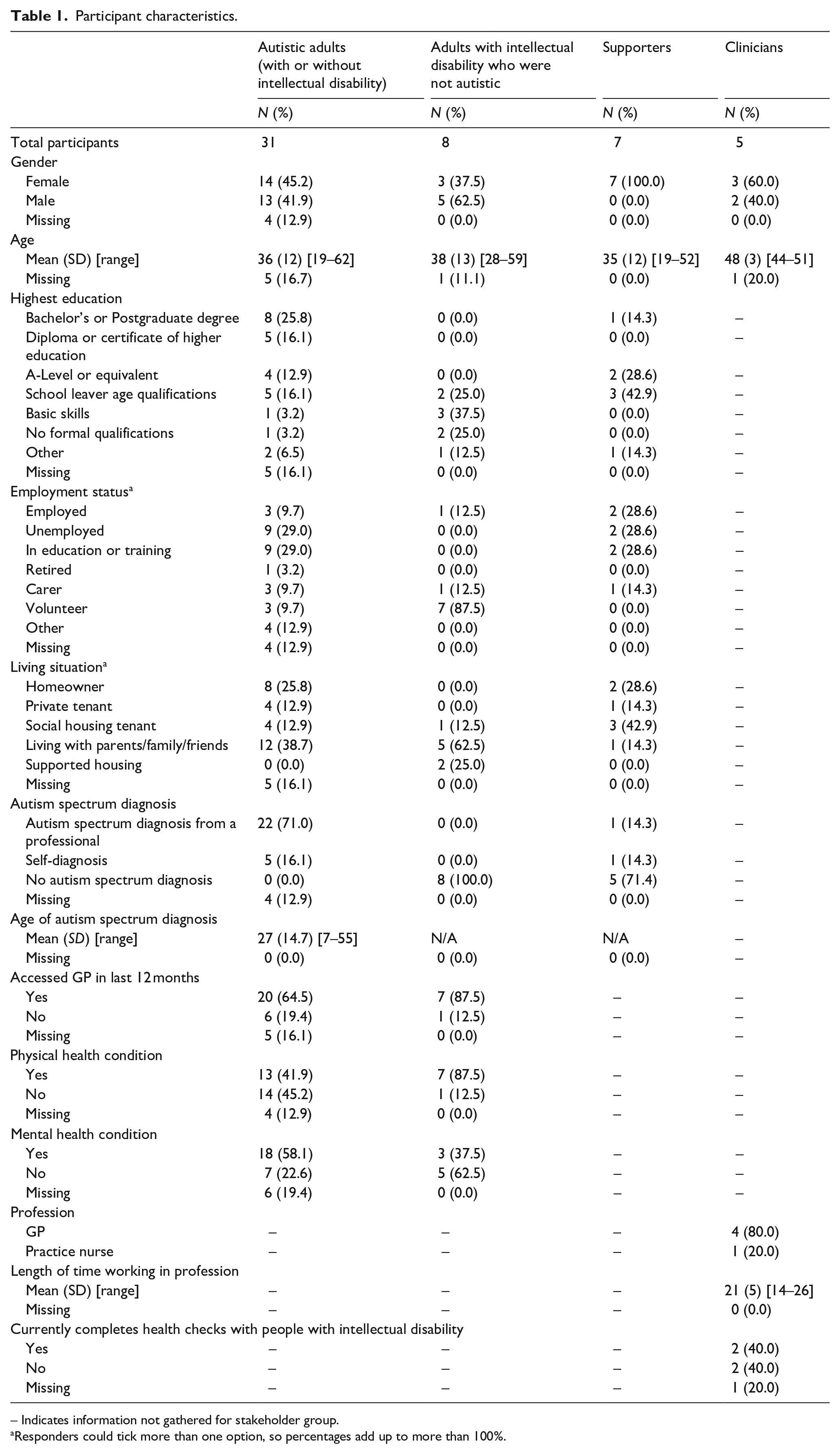
– Indicates information not gathered for stakeholder group.
Responders could tick more than one option, so percentages add up to more than 100%.
Procedure
We invited autistic adults, adults with intellectual disability who were not autistic, and supporters to participate in one or more of eight 2-h consultation groups. One autistic adult with an intellectual disability chose to have a 30-min interview alongside their supporter. Five participants participated in two consultation groups each. Between 2019 and 2020, Newcastle University undertook four consultation groups and advocacy organisations hosted four more. A research team member led each group and an autistic person or relative of an autistic person co-facilitated. To thank them for their time and cover travel costs, autistic adults, adults with intellectual disability who were not autistic, and supporters received a shopping voucher. A research team member also conducted semi-structured 30-min interviews with clinicians by telephone or face to face at the General Practice (between 2018 and 2020). One clinician was interviewed twice (about different topics by different interviewers).
Each consultation group and interview was iterative, building on information from the previous session; therefore not all topics were covered at each. Participants were asked their views on (1) their previous experience of health checks and healthcare appointments; (2) potential barriers and facilitators to attending a health check appointment; (3) a health check for autistic adults, including what topics should be covered and reviewing iterative versions of the health check appointment template; (4) a pre-appointment questionnaire, including what topics should be included and reviewing iterative versions of questionnaire content; (5) factors important for use of the health check in a randomised controlled trial (RCT); and (6) training materials for use with primary care staff during the RCT. Details of topics covered in consultation groups and interviews are shown in Supplementary Table 1.
Participants received an information sheet and completed a consent form. We audio-recorded and transcribed each consultation group and interview and took field notes. One consultation group and one interview were not audio recorded because participants did not give consent; field notes were taken.
Ethics
NHS Ethical committee (Ref: 18/WA/0191) and the Newcastle University Ethics Committee (Ref: 19-DOW-048) gave approval for the study.
Community involvement statement
We used a participatory approach (Leask et al., 2019), with autistic people, supporters of autistic people, researchers, health professionals and service commissioners working together in the research team in co-designing the study, creating the research materials, conducting the research, analysing and interpreting the data and disseminating the findings.
Data analysis
We conducted a reflexive thematic analysis, using an inductive approach, at a semantic level, in an interpretivist paradigm (Braun & Clarke, 2006, 2019; Joffe, 2011). Three research team members (H.T., C.S. and T.F.) met twice to discuss their interpretations of two consultation group transcripts and jointly developed a coding framework to facilitate the analysis process. Using this framework, two researchers (H.T. and C.S. or R.L.) each coded the remaining transcripts (consultation groups and interviews); coding decisions were jointly discussed to reach agreement. We did not assess inter-coder reliability (ICR), as although ICR is commonly used in content analysis, it is not appropriate for use in thematic analysis, especially when using an interpretivist paradigm (Braun & Clarke, 2019; Morrow, 2005). Instead, team members discussed discrepancies in coding as a way to deepen their understanding of the text (O’Connor & Joffe, 2020). Subsequent analysis meetings with the research team were undertaken to agree with the final structure of themes and sub-themes.
The research team used the information gathered through multiple consultation groups and interviews to make decisions about content, structure and language. Information on the content and processes of other relevant health checks were taken into account during this process. We shared reiterations of the pre-appointment questionnaire and health check appointment template with participants in subsequent groups to gather their views, leading to further development.
Results
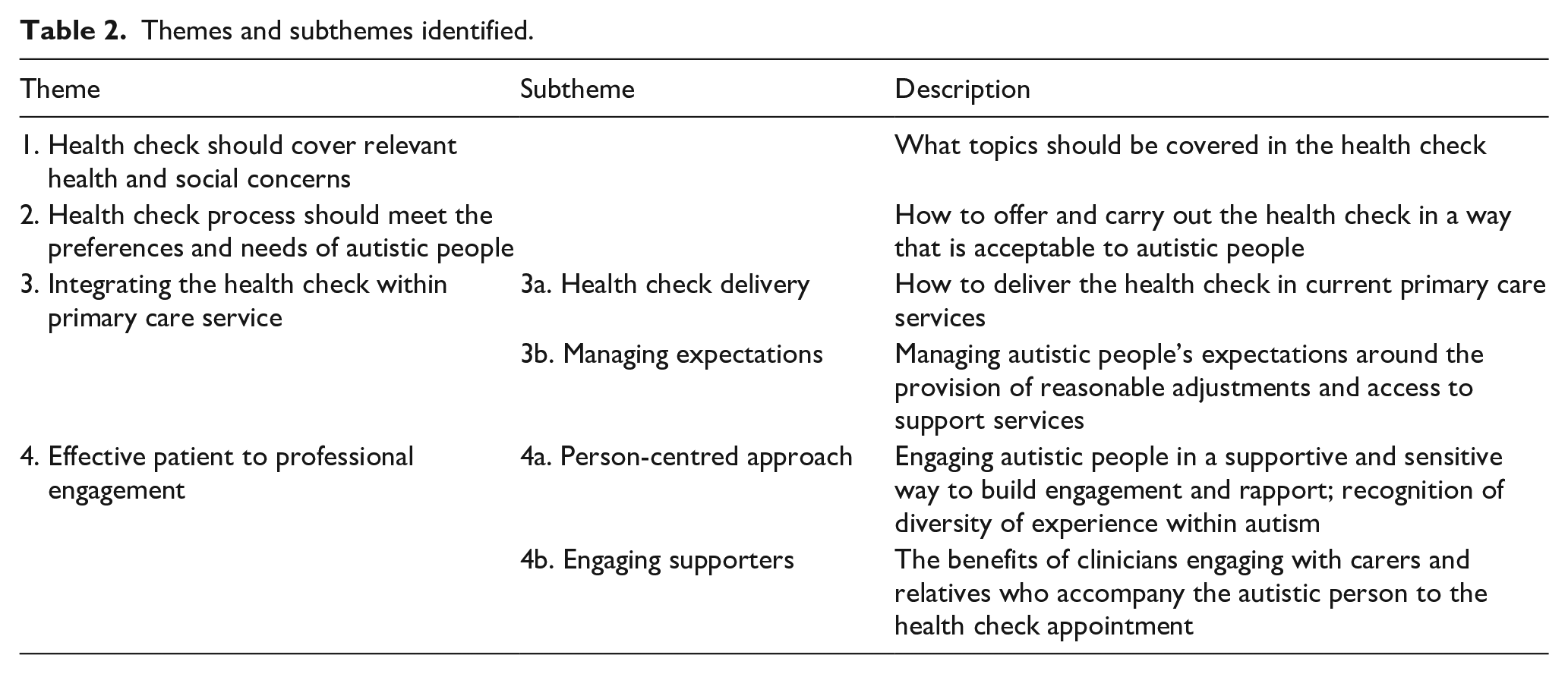
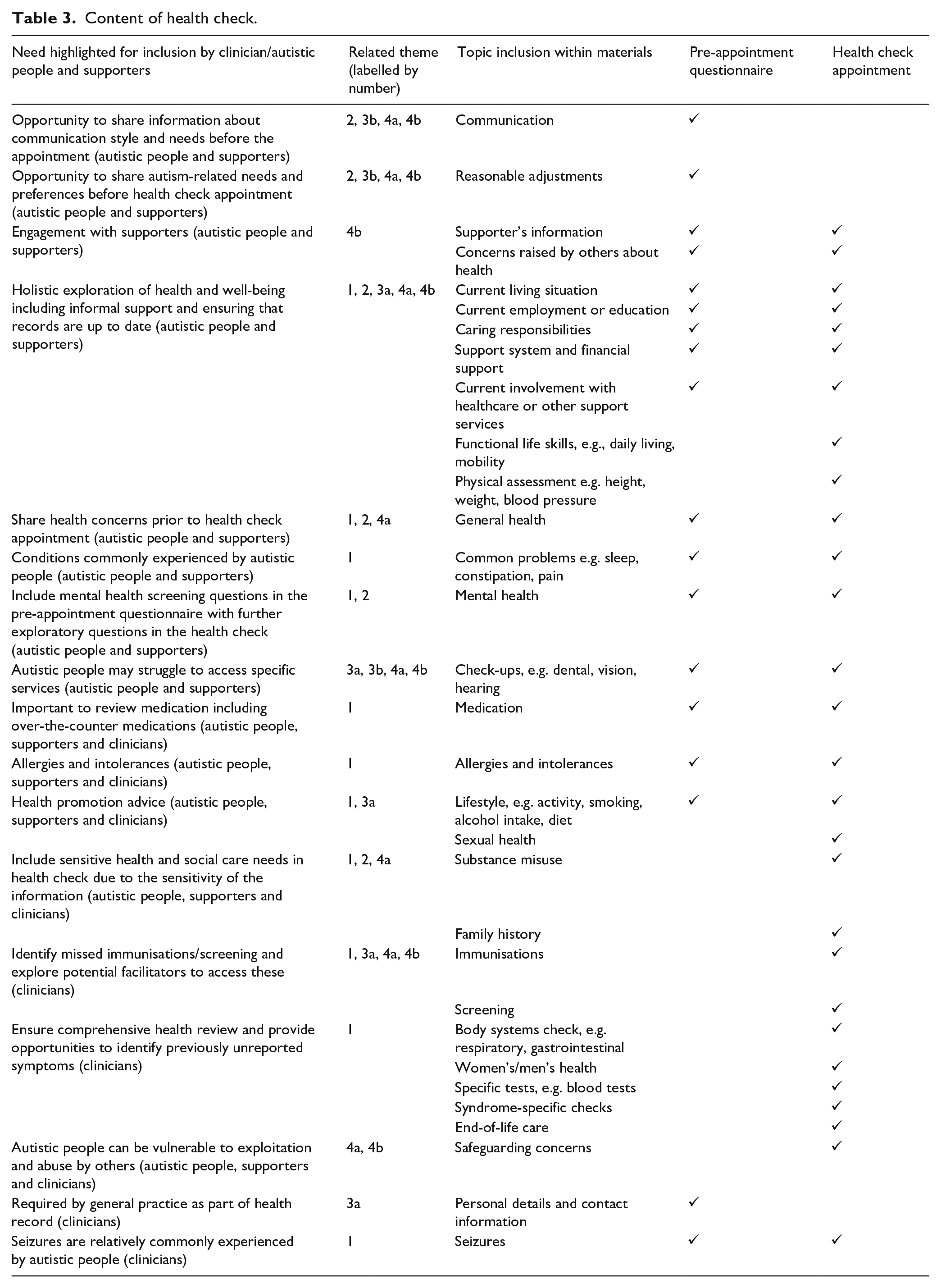
The health check was developed iteratively from the findings of the consultation groups and interviews (see Table 2 for the themes and subthemes identified and Table 3 for the content of the health check identified by autistic people, supporters and clinicians). The health check comprises a pre-appointment questionnaire (PAQ) (to gather information from the autistic person before the appointment) and a health check template (for clinicians to use during the appointment). Table 3 outlines the content of the PAQ and health check template, the needs highlighted by participants for inclusion and the themes outlined below that are associated with each need. The PAQ has been developed in paper and digital format and Supplementary Table 2 outlines the design features identified by autistic people and supporters to enhance the readability and usability of the digital version of the PAQ.
Themes and subthemes identified.
Content of health check.
We identified four main themes from the data collected during our consultation groups and interviews that informed the research team’s key decisions about the development of the health check.
Theme 1: the health check should cover relevant health and social concerns
Stakeholders thought the health check should cover physical, psychological and social functioning, and provide an opportunity to refer people to services for support. Stakeholders agreed the health check should focus on the following key areas: mental and physical health, diet and nutrition, sleep, social activities and support. Autistic adults and supporters also suggested asking about any significant life events the person may have experienced due to their impact on a person’s well-being, for example, pregnancy and childbirth, hospital admissions for physical or mental health conditions, domestic violence and unemployment Stakeholders raised the challenge of balancing all the key issues relevant to autistic people and an acceptable appointment length: Social, sensory, what’s going on in your life, that’s not related to just blood pressure and pulses and blood tests and things, more emotional stuff, mental health stuff. (Clinician)
On the basis of these findings, we developed the health check in a way that was biopsychosocial, ensuring that mental health and social needs were included alongside physical needs and that the most relevant concerns of autistic people were included (see Supplementary Tables 3 and 4 for details of the topics covered in the PAQ and health check template).
Theme 2: the health check process should meet the needs and preferences of autistic people
Stakeholders described the importance of preparing autistic people for the health check appointment, such as providing a paper or web-based opportunity to share information about their health needs and required adjustments. This would give people time to think about their answers in their own environment, create an account of their needs before attending the appointment and reduce pressure at the appointment and guide discussions during the appointment: Without that [sharing information about sensory and communication needs] they can’t even deal with your health, so those two are vital. (Autistic person)
However, autistic adults and supporters raised concerns that autistic people could feel frustrated or overwhelmed if asked for lots of information before the appointment: Big long lists turn it into an uncomfortable form. It becomes, ‘This is something I have to do and deal with’, rather than ‘this is going to help me’. (Autistic person)
Autistic adults and supporters also highlighted the importance of providing information about what the health check will involve before the appointment to increase the likelihood of attendance: You’d have more people turning up to appointments if they knew what to expect. Uncertainty rules a lot in our house and the unexpected is a big no-no really. (Autistic person)
Stakeholders agreed on adjustments to standard healthcare practice that should be offered (see Table 4) but felt these should be personalised to reflect the individual differences in the needs of autistic people. These adjustments included changing the way practices communicate with patients, and offering greater flexibility – such as providing reasonable adjustments, reducing phone contact and facilitating online appointment booking to manage cognitive demands: Text is ideal, but I really like email because you’ve got time to process it and think about what to say. Phone calls and face to face, you’re having to react quickly and that escalates anxiety and communication issues. (Autistic person) We’ve had an absolutely amazing experience with our practice nurse, she booked us in at the end of the day, booked an extra amount of time, made a plethora of reasonable adjustments. (Supporter)
Reasonable adjustments identified by all stakeholder groups.
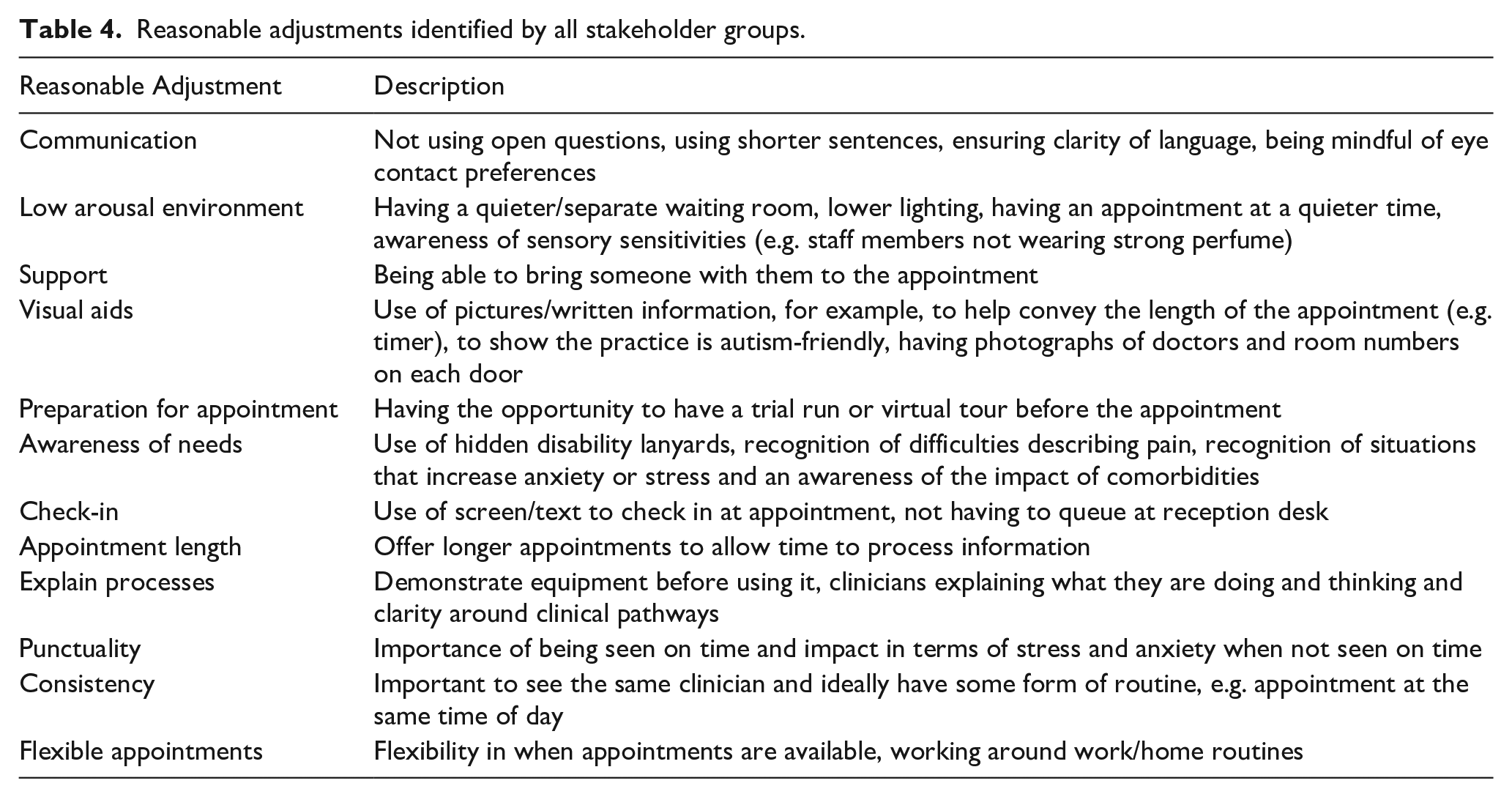
In line with these findings, we developed the PAQ in a digital and paper format and grouped reasonable adjustments within different sections of the health check process for readability on the PAQ.
Theme 3: integrating the health check within primary care services
Health check delivery
Stakeholders thought it would be beneficial for the health check to be delivered in a standardised way across the United Kingdom. They thought it should be available to all autistic adults, with or without an intellectual disability, but participation should be optional: I think everybody should get time to have a check on the autistic health check, it’s important the doctor asks if you’d like one. (Person with intellectual disability who was not autistic)
Autistic adults and supporters thought the health check should be delivered in different formats (face-to-face and online) to help with engagement: Some people might not be able to go to a surgery for lots of different reasons, and if those people could still have a health check, either using Skype or even you email your form back and somebody emails back some questions or advice. (Autistic person)
Clinicians thought health checks should be offered annually, in line with other health checks although autistic adults and supporters varied in their views on frequency (from 3 monthly to annually), with some raising concerns that people might save issues for a health check appointment rather than accessing healthcare in a timelier manner: I would probably save those physical things up till I had a six month check or annual check. I’d end up going in with a bit of a list. (Autistic person)
Clinicians’ views varied regarding who should deliver the health check and whether it should be completed by a single clinician or co-delivered by two clinicians. Clinicians reported similar variability in how health checks for people with intellectual disabilities are delivered within the NHS currently. Clinicians highlighted that adequate funding to support the delivery of the health check and associated tasks (arranging appointments, chasing up non-attendances and implementing reasonable adjustments) would be vital.
Autistic adults and supporters thought that creating a register of clinicians trained in autism would improve autistic peoples’ confidence in the clinicians they see. Clinicians suggested it would be useful to have an ‘autism champion’ at each practice to lead on raising autism awareness and implementing reasonable adjustments. Clinicians thought that a small number of people delivering the health check at each practice would be most beneficial. They also suggested it may be helpful to deliver the health checks within specific clinics to reduce the time taken to organise appointments and implement reasonable adjustments: If you were running it as a clinic, you’d have more possibility of specific arrangements that suit the clientele for that clinic. There might be a checklist of things for the practice to try and think about in setting up the clinic, which might be lower level of lighting, try to have less going on and so on. (Clinician)
Clinicians also raised concerns about being able to successfully identify all eligible autistic adults for health checks due to issues around coding on patient records. For example, some patients might be coded as having ‘developmental delay’ and only have ‘autism’ or ‘possible autism’ mentioned in the free-text section of their notes.
To take account of these results, we created a standardised template of topics to be covered within the health check appointment for clinicians to use to structure the appointment and to record the information gathered (see Supplementary Table 4 for details of the topics covered in the health check template).
Managing expectations
Clinicians expressed the importance of managing expectations around reasonable adjustments, acknowledging not all general practices will be able to offer every adjustment requested: You go shopping and they turn the lights down low, and the music off; you can go to trampoline parks when no one else is allowed and it’s very quiet but we can’t do that, we can’t say ‘no other patients for an hour’ – that’s very difficult. (Clinician)
Clinicians also voiced concerns about raising expectations about being able to meet the mental health or social needs of autistic people through the health check due to a lack of capacity within mental health and social care services: If we do the health check and then problems come from that and concerns, and then we signpost patients to somewhere else – is there the capacity to signpost them to somewhere because waiting lists are so long? We’re going to identify mental health concerns as well and that service isn’t the best at the moment because of waiting lists. (Clinician)
Theme 4: effective patient to professional engagement
Person-centred approach
Some clinicians suggested taking a person-centred approach in the delivery of the health check to build engagement and rapport with the autistic person: I start off saying “What’s your concerns today? What do you need help with?” Because then they can just say it: “Thank God, somebody’s asked us what’s wrong, I’ve got this problem going on can you help?” And if that’s all I got done, great, that’s fine if that was what they wanted to do and the rest of the stuff I’ll get done another time. It’s very individual. (Clinician)
Autistic adults and supporters described how information should be gathered in a sensitive and supportive way to avoid putting people off attending their health check and to minimise anxiety caused by health-related questions, especially for those with health anxiety: It needs to be done in a particular way that wouldn’t put people off. If you’re told to fill in a form and there’s a question that can’t be answered, some people think, “I can’t go to the appointment because I haven’t filled in the form that they said I need to bring with me”. (Autistic person)
Autistic adults and supporters highlighted that clinicians taking a supportive and sensitive approach could also potentially impact health outcomes through better communication: If they tell us why they’re asking the questions, then (a) we’ll be more relaxed, and (b) we’ll give the information they need. We’ve got so much information in our brains that we’re having to filter but because we’re presenting what we think they want to hear; they might miss something of clinical significance. (Autistic person)
Autistic adults and supporters also highlighted the importance of in-depth exploration of key issues, such as lifestyle behaviours (e.g. diet and sleep patterns), as some autistic people may not self-report any issues in these areas: With a lot of questions, it’s about self-awareness. I could say to you, ‘Yeah, I don’t have any difficulty sleeping’, where in reality I don’t go to sleep until 01.00. (Autistic person)
Autistic adults and supporters also highlighted that some experiences (such as pain) are different for autistic people and therefore the way clinicians investigate these phenomena should reflect these individual differences. They described the difficulties autistic people experience in making links between actions or responses to situations and symptoms of health conditions. These differences need to be understood by clinicians to ensure they ask for relevant information and in a supportive and sensitive manner: Understanding that everybody has different pain thresholds, different interpretations of pain, and also the masking side of it as well is a huge issue and not to go with the complacent textbook version of what it should look like. (Supporter) Sometimes it’s hard for an autistic person to make the link between a lifestyle behaviour and symptoms. I started the ketogenic diet because I’d read it’s good for autistic kids with epilepsy. I was having physical and mental health problems, so I thought, ‘Oh, I’ll try that’. But I ended up with tachycardia – I don’t know if there’s a link. (Autistic person)
Stakeholders agreed that practice staff should be trained about autism to ensure those involved in delivering the health check do so in a supportive manner. Training was specially focussed on in one consultation group and interview (see Supplementary Table 1) but was brought up by stakeholders in other consultation groups and interviews. Autistic adults and supporters highlighted that training should cover the diversity of experiences within autism and include key topics such as masking, reasonable adjustments, the presentation of anxiety, hidden difficulties and mental health. They thought that by understanding the diversity of autistic people, this could also reduce the risk that clinicians resort to common autism stereotypes, interpret guidance literally and apply adjustments to all autistic people without considering individual needs: I think the quality and the reception of some of the training as well, people think ‘Yes, I’m autism aware’. You might be aware of the name of it but you’re not aware of the diversity. (Supporter) I’ve seen people follow these instructions far too literally. Speaking in short sentences for example, isn’t necessarily good advice if there’s no understanding behind why you’re speaking in short sentences because the quality of the communication’s still quite low. And it’s the same for a lot of information, it’s the way that people understand it. (Autistic person)
On the basis of this information, we developed the training package for primary care staff to reflect the diversity of experience within autism, including information about hidden difficulties, differences in the experience of pain and reasonable adjustments, alongside the delivery of the health check itself.
Engaging supporters
Autistic people, adults with intellectual disabilities and supporters highlighted the benefit of having a supporter attend the health check appointment to help support the autistic person and facilitate effective communication. They however raised the importance of clinicians not solely communicating with the supporter to the detriment of engaging with the autistic person: I supported an autistic person and when we got there, they asked if they wanted to go in on their own and the person said, ‘I don’t mind, it’s up to you’. I said, ‘Well, I can do whatever you want’ – and the healthcare person said, ‘It would be better if you came in on your own’, so they went in, and I sat outside. When they came out, they had a form to fill in to access something. I said, ‘How was it?’ and they said, ‘I don’t know, they just gave us loads of information and talked really fast, I don’t know’. (Supporter) If I’m getting my blood pressure took, the doctors don’t talk to me if I go with my sister, they go, ‘What’s his disability?’ I goes, ‘Excuse me, I’m sat here, I have a got a mouth’. (Person with intellectual disabilities who was not autistic)
On the basis of these findings, we included a section in the PAQ asking for details of supporters and clarity around their role in supporting the autistic adult with their healthcare needs, to support engagement with supporters during the health check (see Supplementary Table 3).
Discussion
This is the first substantial qualitative study to specifically investigate the views about designing a multi-component primary care health check for autistic people. It represents a key step in co-designing a health check for autistic adults and addresses the policy goals outlined in the NHS England Long-Term Plan (NHS, 2019). We found autistic people, supporters and clinicians supported a health check for autistic adults and thematic analysis provided key findings into how the health check should be designed. The first key finding was that the health check should cover health and social concerns which is unsurprising given the higher prevalence of health conditions experienced by autistic people (Rydzewska et al., 2021) and high levels of unmet social needs (Schott et al., 2021). Second, people wanted the opportunity to share information about the adjustments they would like, to improve access to healthcare, such as those identified by Brice et al. (2021). Third, we identified the need to find ways of integrating the health check into primary care delivery to manage expectations around the provision of services and reasonable adjustments (building on learning from the development of health assessments for autistic people internationally (Nicolaidis et al., 2016) and UK health checks for people with intellectual disabilities (Cooper et al., 2014). Finally, we identified the importance of facilitating positive relationships between healthcare professionals and patients, including their supporters, and the need for further primary care staff training to understand the way that differences in the experiences of autistic people may lead to barriers to healthcare (Mason et al., 2019, 2021). In addition, we gathered key information about how adjustments should be implemented and managed, highlighting the need for a personalised implementation approach. Our main themes emerged from data from autistic people with and without intellectual disability, but they were supported and enhanced by data from people with intellectual disability who are not autistic, supporters and clinicians. As such we presented themes together, noting within the text, as appropriate, any nuances related to how comments from different stakeholder groups differed.
This study highlighted the need for adjustments to standard healthcare practice for autistic people, in line with recent studies (Brice et al., 2021; Mason et al., 2021; Nicolaidis et al., 2015), which categorised adjustments as relating to the sensory environment, clinical and service context, and clinician knowledge and communication. In keeping with the AHAT (Nicolaidis et al., 2016), the PAQ requests information about adjustments the person would like to support them at their health check appointment. We have developed a training package about autism and health check delivery to ensure primary care staff understand the importance and context behind offering these adjustments. The adjustments offered on the PAQ could be incorporated into the individual’s health records, such as through the reasonable adjustments flag (https://digital.nhs.uk/services/reasonable-adjustment-flag). In the future, the adjustments and the training package could potentially be adapted and used in other healthcare settings where they are not commonly provided. The health check materials will be made available under licence to healthcare practitioners.
Strengths and limitations
This study included autistic adults from a wide age range and with good representation across educational attainment and employment status. Alongside those with a formal diagnosis of autism, we included people with a self-diagnosis of autism, thereby increasing representation from the wider autistic community (Brice et al., 2021; Mason et al., 2018). We also included people who had and had not accessed their GP recently and those with, and without, physical and mental health conditions. This study was limited by including participants only from the Northeast of England, although it is unlikely that the views of autistic people and clinicians from other UK areas would be substantially different. This study did not gather information about participants’ ethnicity and may have missed views on the health check from different ethnic groups which are often under-represented in research, impacting its applicability to those groups. The acceptability of the health check for people from different ethnic groups will form part of our evaluation of the health check within a future RCT and we will actively encourage the recruitment of autistic adults from a range of ethnic and social backgrounds. Most autistic people were not asked whether they had an intellectual disability, and their education attainments suggest that most did not; however, this study included eight participants with intellectual disability who were not autistic and reached data/theme saturation with all stakeholder groups. Importantly, the health check design took account of the content of existing health checks developed for people with intellectual disabilities and the learning related to their use in NHS practice.
Conclusion
This study represents a key step in co-developing a primary care health check for autistic people that addresses the policy goals outlined in the NHS England Long-Term Plan. Stakeholders supported a health check for autistic adults and results influenced health check design. The next step is to evaluate the clinical and cost-effectiveness of the health check and the factors important for implementation through an RCT. If the health check is clinically and cost-effective, future studies could explore its use in other healthcare settings and other countries, alongside the adaptations needed to implement it within their health systems. In the meantime, our development work has led to novel and useful information that can be used now by clinicians and policy-makers to design innovative, effective and acceptable services for autistic people.
Supplemental Material
sj-pdf-1-aut-10.1177_13623613221132921 – Supplemental material for Co-design of an NHS primary care health check for autistic adults
Supplemental material, sj-pdf-1-aut-10.1177_13623613221132921 for Co-design of an NHS primary care health check for autistic adults by Helen Taylor, Barry Ingham, David Mason, Tracy Finch, Colin Wilson, Clare Scarlett, Sebastian Moss, Carole Buckley, Anna Urbanowicz, Dora Raymaker, Charlotte Seiboth, Rhianna Lees, Deborah Garland, Malcolm Osbourne, Nicholas Lennox, Sally-Ann Cooper, Christina Nicolaidis and Jeremy R Parr in Autism
Supplemental Material
sj-pdf-2-aut-10.1177_13623613221132921 – Supplemental material for Co-design of an NHS primary care health check for autistic adults
Supplemental material, sj-pdf-2-aut-10.1177_13623613221132921 for Co-design of an NHS primary care health check for autistic adults by Helen Taylor, Barry Ingham, David Mason, Tracy Finch, Colin Wilson, Clare Scarlett, Sebastian Moss, Carole Buckley, Anna Urbanowicz, Dora Raymaker, Charlotte Seiboth, Rhianna Lees, Deborah Garland, Malcolm Osbourne, Nicholas Lennox, Sally-Ann Cooper, Christina Nicolaidis and Jeremy R Parr in Autism
Supplemental Material
sj-pdf-3-aut-10.1177_13623613221132921 – Supplemental material for Co-design of an NHS primary care health check for autistic adults
Supplemental material, sj-pdf-3-aut-10.1177_13623613221132921 for Co-design of an NHS primary care health check for autistic adults by Helen Taylor, Barry Ingham, David Mason, Tracy Finch, Colin Wilson, Clare Scarlett, Sebastian Moss, Carole Buckley, Anna Urbanowicz, Dora Raymaker, Charlotte Seiboth, Rhianna Lees, Deborah Garland, Malcolm Osbourne, Nicholas Lennox, Sally-Ann Cooper, Christina Nicolaidis and Jeremy R Parr in Autism
Supplemental Material
sj-pdf-4-aut-10.1177_13623613221132921 – Supplemental material for Co-design of an NHS primary care health check for autistic adults
Supplemental material, sj-pdf-4-aut-10.1177_13623613221132921 for Co-design of an NHS primary care health check for autistic adults by Helen Taylor, Barry Ingham, David Mason, Tracy Finch, Colin Wilson, Clare Scarlett, Sebastian Moss, Carole Buckley, Anna Urbanowicz, Dora Raymaker, Charlotte Seiboth, Rhianna Lees, Deborah Garland, Malcolm Osbourne, Nicholas Lennox, Sally-Ann Cooper, Christina Nicolaidis and Jeremy R Parr in Autism
Footnotes
Acknowledgements
The authors are grateful to all the participants who gave their time to take part in the study. We would also like to thank the following organisations for supporting recruitment to the study and organisation of the consultation groups: The Kayaks Support Group (South Shields, UK), Skills for People (Newcastle upon Tyne, UK), Autism Able (South Shields, UK), and the Lawnmowers Independent Theatre Company (Gateshead, UK). We are grateful to Andy Dow and Dalya Al-Shahrabi for co-facilitating some of the consultation groups and taking field notes.
Author contributions
B.I. and J.R.P. were the chief investigators. B.I. and J.R.P. led the application for funding. B.I. and J.R.P. oversaw governance and both B.I. and J.R.P. co-designed the study and supervised the research team. H.T., and D.M. led the consultation groups. C.W., M.O. and D.G. co-facilitated the consultation groups. H.T. and D.M. conducted the interviews. H.T., C.S. and T.F. developed the coding framework. H.T., C.S. and R.L. coded the transcripts. T.F. supervised the qualitative analysis. H.T. drafted the manuscript; all authors contributed to, reviewed and finalised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the UK autism research charity Autistica (London, UK) and the Peter Sowerby Foundation (London, UK) (grant number 7257).
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.