
Abstract
Emerging research suggests autistic people are disproportionately represented in homeless populations. Less is known about how autistic people experience homelessness and what prevents them from exiting homelessness. This article presents findings from a narrative enquiry investigating the link between autism and homelessness. Ten autistic adults consented to participate in narrative interviews which explored their life histories and pathways through homelessness. This article considers how participants experienced rough sleeping and sofa surfing before attempting to access hostels. It then examines how participants navigated support systems, arguing that barriers to accessing services perpetuated homelessness. Because of these barriers, some participants disengaged with services, preferring to sleep rough. The extent to which participants could be said to have ‘chosen’ homelessness is balanced with consideration of the lack of autonomy autistic adults are able to exercise over their lives. This article concludes with discussion of practical implications for services and policy in England.
Lay Abstract
Recent research suggests many autistic people experience homelessness. However, little is known about the types of homelessness autistic people experience and what barriers autistic people face when trying to exit homelessness. This study involved gathering life stories of autistic people who had experienced homelessness. Ten autistic participants talked about their pathways through homelessness and the difficulties they had in accessing support. After first becoming homeless, participants tended to experience rough sleeping and sofa surfing. When participants approached housing and homelessness services, they were often told they were not eligible for support. This could happen when support workers were not aware of autism, or when autism was not considered ‘severe’ enough. Overcrowding, confrontation and lack of control over routine and environment were particular issues for participants when they entered homelessness hostels. Some participants chose to sleep on the streets rather than stay in environments which increased social anxiety and sensory difficulties. This study discusses ways in which homelessness and housing services can increase accessibility and improve engagement for autistic people. It is important to increase awareness of autism while understanding that autistic people who experience homelessness may have complex needs. In addition, services need to listen to autistic people with lived experience of homelessness to decide what changes will have the most impact.
Introduction
Autism is typically defined as a lifelong, neurodevelopmental condition, characterised by differences in social interaction and communication, as well as the presence of rigid and repetitive behaviour patterns and restricted interests (National Institute for Health and Care Excellence (NICE), 2021). There is no singular biological marker of autism (Hassall, 2016), and recent conceptualisations position autism as a form of human difference which is not defined by deficit (Waltz, 2013). However, recognising autism as a type of difference does not detract from the impact a few associated traits, such as sensory processing difficulties, rigid or repetitive behaviour patterns and interpersonal interaction difficulties, can have on day-to-day functioning (NICE, 2021). In addition, autism often co-occurs with physical, developmental and mental health conditions such as epilepsy, attention-deficit hyperactivity disorder (ADHD), learning disabilities and anxiety disorders (Gotham et al., 2015; Murphy et al., 2016). As such, autistic people may present with a range of complex needs.
In England, a person is regarded as homeless if they have no accommodation, or if it is not reasonable for them to continue occupancy of their accommodation. However, in order to be classed as legally (statutory) homeless, a person must present at their local authority to make a homeless application. They are then assessed to ensure that they are not intentionally homeless and that they meet ‘priority need’ criteria, such as being a care leaver or having dependent children (National Audit Office (NAO), 2017). Being accepted as statutory homeless, and thus owed a duty of support, enables referral to a range of support services; however, an autism diagnosis does not necessarily meet criteria. Instead, autistic people who do not meet other priority need conditions must prove they’re vulnerable for another ‘special reason’ (Shelter, 2021). Given that all homeless people are, arguably, vulnerable, the question of who is more at risk is open to interpretation (Meers, 2015). The assessment of priority need is further complicated by a lack of national legislation which can lead to subjectivity in the way eligibility criteria are applied, resulting in a postcode lottery of access to services (Wilson & Barton, 2018).
This question of support eligibility is crucial given that autism is overrepresented in homeless populations (Churchard et al., 2019; Kargas et al., 2019; Pritchard, 2010). Research suggests autistic people are at increased risk of homelessness due to socioeconomic disadvantage across the life course (Campbell, 2015, Stone, 2019). These disadvantages are beginning to be explored in relation to how autism intersects with social exclusion to increase risk of homelessness (Garratt & Flaherty, 2021; Stone, 2021). Furthermore, current provision may be unsuitable for autistic people, with barriers to access and engagement prolonging homelessness (Campbell, 2015; Garratt & Flaherty, 2021; Kargas et al., 2019). However, research in this area is in its infancy. There is a dearth of information on how autistic adults experience homelessness and a need to identify barriers to service access for this population (Kargas et al., 2019). This article aims to bridge this gap, examining the autistic experience of homelessness within the context of English policy and service provision.
Although prevalence of autism is similar in adults to children (estimated between 1% and 2%), adults are significantly underdiagnosed (Brugha et al., 2016). Furthermore, autistic people who appear to be more able, or who mask autistic behaviours, are less likely to be identified and diagnosed (Lai & Baron Cohen, 2015). After becoming homeless, a clinical diagnosis is more difficult to obtain due to the lack of regular service access and requirement of additional information, such as developmental history (Nishio et al., 2015). In a recent screening study of 106 adult people in London, 12.3% of the sample met Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) autism criteria, but only one had a pre-existing diagnosis (Churchard et al., 2019). In consideration of service eligibility, the lack of clinical diagnosis could constitute a significant barrier to exiting homelessness for autistic people.
This article presents findings from a narrative study which investigated the link between autism and homelessness. Although this study also examined why autistic adults are at increased risk of homelessness, this article will focus exclusively on the following questions:
How do autistic people experience homelessness?
What barriers do autistic people face to exiting homelessness?
In answering these questions, this article aims to consider wider implications for policy and services. While this is focused within the English context, presentation of rich detail on participants and their settings aims to increase transferability of findings.
Research process
Recruitment began after ethical approval was obtained from the SPS Research Ethics Committee at the University of Bristol in January 2019 (reference: SPSREC17-18.C41). Homelessness services identified potential participants who had a diagnosis of autism or self-identified as autistic. Participants were recruited from two cities in the South West of England. Sites were categorised as follows:
Level 1, high support, male hostel.
Level 1, high support, mixed hostel.
Level 2, medium support, mixed hostel.
Drug and alcohol support hostel.
Residence for homeless or vulnerably housed autistic adults.
Sites 1–4 were part of a network of hostels for those who meet government criteria of homelessness and are owed a duty of care by their local authority (NAO, 2017). Hostels were designated as high, medium or low support. High-support hostels imposed stricter regulations on residents while providing a more intensive package of support. Residents were expected to move through increasingly less-regulated hostels before being supported to apply for independent housing. The fifth site was a residence for adults, with a clinical diagnosis of autism, who had been referred by a local night shelter or were leaving care with nowhere else to stay. Residents could stay in this accommodation for a maximum of 2 years.
Ten participants provided written consent to take part in the study. An easy-read guide and information sheet was developed to aid informed consent, and consent was re-checked prior to each interview. Interviews took place in the sites listed above. Nine participants took part in two interviews with each interview lasting between 50 and 140 min. At their request, one participant took part in three interviews lasting around 30 min each.
A narrative methodology was chosen to study personal experience while acknowledging the embodiment of participants in social contexts (Clandinin, 2006). With regards to autism and narrative production a presumption of competence was adopted, recognising that allowing individuals to speak in their own way can lead to genuine discoveries about a phenomenon (Biklen & Attfield, 2005; Riessman, 2008). Considering the sensory processing issues, such as hypersensitivity to sound, associated with autism (NICE, 2021), interviews were held in quiet rooms that participants were familiar with. A topic guide, focussing on chronological life stages and events, including pathways through homelessness, was used to provide structure.
Interviews were conducted by the lead author. The interviewer attempted to take an anti-authoritarian position through the shifting of superior and inferior knowledge positions. This approach is congruent with narrative research which relinquishes the control of a fixed format interview and allows participants to take the lead, thus addressing power imbalance and encouraging equality (Riessman, 2008). In practical terms, this involved ensuring participants understood their experiences had inherent value and that there were no correct or incorrect responses to questions. Establishing this at the beginning of interviews was essential as participants explained that under different circumstances, there was usually an agenda to telling their stories, such as trying to obtain a diagnosis or access homelessness support. Participants were also encouraged to expand on areas of personal significance. In this way, the topic guide was not followed verbatim, but used to prompt participants where necessary. In addition, the interviewer answered participants’ own questions and took an active role in responding to, and emphasising with, participants’ accounts of their lives. Taking this approach, as well as conducting at least two interviews with each participant, helped to foster trust and rapport. While reminded that they did not have to, all participants discussed personal and sensitive areas of their lives, including past trauma. Additional support services were signposted where necessary.
Interviews were audio recorded before being transcribed and anonymised. Initial transcriptions were used to develop questions for further interviews based on gaps in information and areas of specific interest.
There was no community involvement in the reported study. However, this research was informed by a pilot study (Stone, 2018), which consulted with homeless, autistic, adults to establish how best to implement narrative methods with this population.
Data analysis
This study was framed by a critical realist perspective which attempts to explain social events through identification of wider causal mechanisms and examination of their impact (Fletcher, 2017). Thematic analysis was an appropriate method to identify connections between the real-life worlds depicted in narratives and larger social structures (Riessman, 2008). While Braun and Clarke (2019) caution against mixing incompatible approaches to thematic analysis, they note that rigid interpretations, such as assuming analysis must be either inductive or deductive, is a misapplication of this method. Traditional thematic analysis was carefully adapted from the main stages set out by Braun and Clarke (2006), in an approach similar to Fletcher (2017), to reflect the Critical Realist framework, this involved the following stages:
Data familiarisation.
Constructing narrative summaries.
Generating initial codes.
Identifying emerging themes.
Identifying superordinate themes.
Reiterative recoding.
Consideration of causation and existing theory.
Data familiarisation (stage 1) began during transcription and involved an immersive process of re-reading transcripts. Familiarisation was aided by construction of narrative summaries (stage 2) which presented key life events chronologically (Stone, 2021). Initial codes (stage 3) were applied inductively, allowing themes (stage 4) to emerge from the data. Coding trees organised themes as superordinate or subordinate (stage 5). Reiterative coding (stage 6) involved revisiting and refining codes and themes, as such, progression through the stages was not always linear. Finally, themes were considered in the context of wider causal mechanisms and existing theory (stage 7). This allowed for the development of theory on the intersection between autism and social exclusion in relation to risk of homelessness. For the purpose of this article, themes relating to the autistic experience of homelessness and barriers to rehabilitation are presented.
Analysis was predominantly carried out by one researcher (lead author). However, emerging themes and theory were discussed with other named authors and refined. This reflexive approach to analysis was aided by the use of a detailed fieldwork diary which examined assumptions and researcher position in regard to both data collection and analysis (Braun & Clarke, 2019).
Description of included participants
Participant demographics are displayed by pseudonym in Table 1. Eight participants identified as male and two participants identified as female. Two participants identified with a different gender from the one they were assigned at birth. Participant age ranged from 22 to 40 with a mean age of 29.2. Nine participants were white British, one participant was white Irish.
Participant demographics.
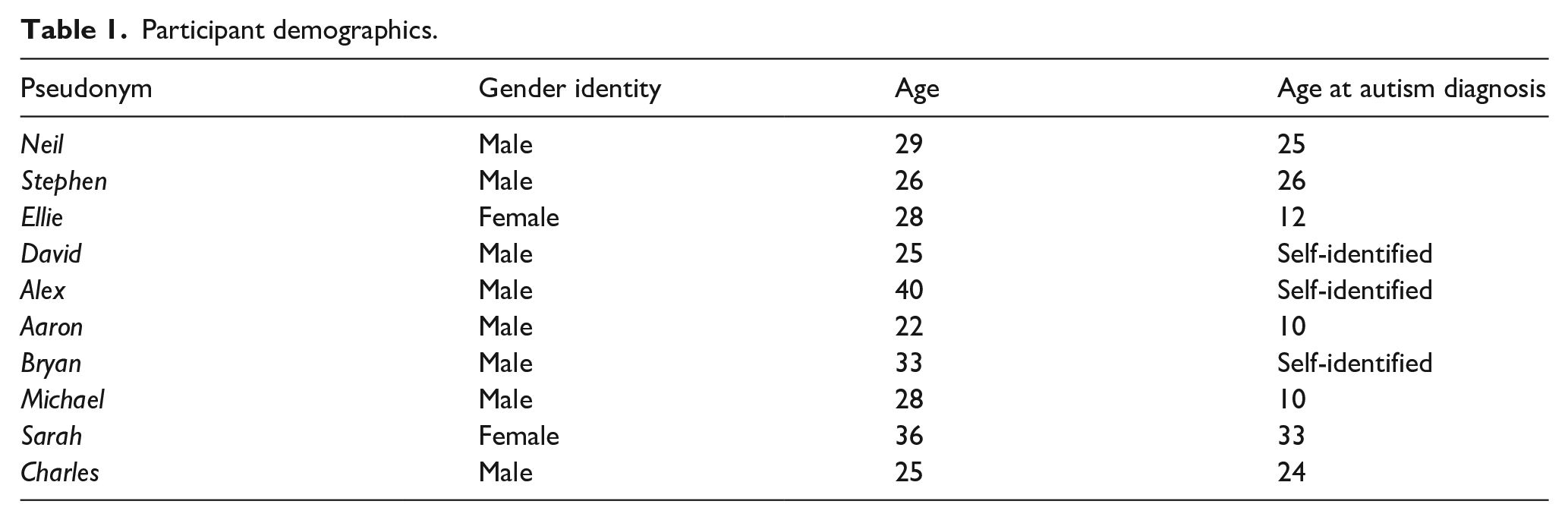
Seven participants had a clinical diagnosis of autism. The mean age at diagnosis was 20 which is higher than average. Age at autism diagnosis in the United Kingdom was calculated at 4.6 years between 2004 and 2014 (Brett et al., 2016), increasing to 14.5 years in 2018 (Russell et al., 2021). Three participants self-identified as autistic. Alex and Bryan had autistic family members and were undergoing diagnosis at time of interview. David self-reported scoring highly on multiple online autism tests including the Autism Quotient test (AQ) (Baron-Cohen et al., 2001). While the AQ is not a diagnostic tool, it has good discriminative validity and screening properties (Woodbury-Smith et al., 2005).
Table 2 describes participants’ experiences of homelessness and current housing. Sofa surfing referred to temporarily staying with friends, family or acquaintances. Rough sleeping included sleeping on the streets, in parks and staying in tents. Hostel stays included long-term hostels which required residents met legal definitions of homelessness and respite shelters accessed on a day-to-day basis. Column 3 denotes best estimates of homelessness duration as reported by participants. ‘Episodic’ refers to multiple instances of homelessness with periods of temporary or stable housing in-between. ‘Continuous’ concerns uninterrupted homelessness, but this often took different forms. For example, Ellie had been homeless for 14 years prior to interview, moving between different types of homelessness. Interestingly, six participants first experienced homelessness in childhood or adolescence. This occurred when participants ran away from chaotic or abusive home environments.
Participant experiences of homelessness.
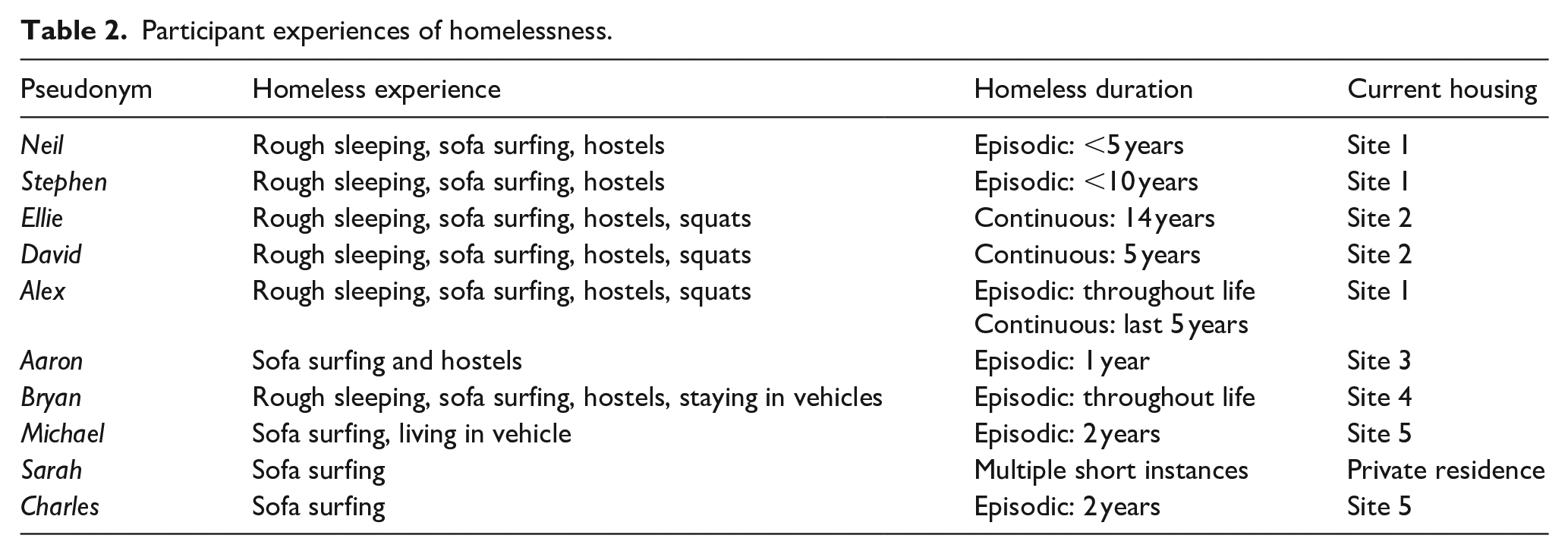
The final column in Table 2 records current housing. Site number refers to the recruitment sites listed above. Under the ‘current housing’ categories, seven participants were still homeless (sites 1–4). Participants in the autism residence (site 5) were vulnerably housed and possibly facing homelessness after their residency ended. Sarah, who was recruited through her links with the autism residence, had a private residence and was the only participant with a history of stable employment.
Participants had multiple co-occurring conditions, including anxiety, depression, bi-polar disorder and ADHD. The majority of participants also reported a historic or current substance dependency. These are discussed where relevant below.
Results
The autistic experience of homelessness: sofa surfing, rough sleeping and transience
While sofa surfing was the most common form of homelessness, the instances were short in duration due to relationship breakdown. Breakdown could result from overcrowding or participant substance use. Alex, who struggled with addiction throughout his life, explained how this quickly led to rough sleeping:
That all runs dry quite quick, you end up overstaying your welcome . . . you end up causing arguments in their house from being there . . . so it’s just easier not to. (Alex)
Other reasons for relationship breakdown were more closely linked to autism. Illustrating the link between autism and manipulation or abuse (Pearson et al., 2020; Roberts et al., 2015), Aaron explained how after he disclosed autism, the person he was staying with became controlling and he chose to move out. Reflecting rigid behaviour patterns associated with autism, Neil described being kicked out of a friend’s home due to his need for routine and cleanliness. These examples of relationship breakdown were concerning as they served to limit already small support networks. Following breakdown, participants did not seek support, instead attempting to stay with others or sleeping rough. Bryan explained how over a short period of time, he moved between sofa surfing and street homelessness:
I came over and me sister has a place in (area 1), I was staying there for a couple of weeks and then she fucked me out and so I was staying in the streets in (area 2) then me brother in law . . . got his cousin to put me up in (area 3) . . . I was there for about two, three weeks. (Bryan)
This transience meant participants were often unable to open bank accounts, access welfare and find and maintain employment, which ultimately prolonged homelessness.
The majority of participants used routines to provide structure and relieve anxiety but struggled to maintain this while homeless. Aaron’s mental health deteriorated while sofa surfing as he was unable to follow his usual routine. Stephen also explained how the lack of routine and fear he experienced when rough sleeping had a lasting impact on his mental health:
I couldn’t do that [routine] . . . because I didn’t know where I was the next day, let alone the next few days . . . I tried laying down on the bench, the wind would blow the leaves across the floor and I am up straight away . . . it brought so much fear into me that even today I still struggle. . . now I am more fearful because of being on the streets and having to have my own back and not knowing what’s going to happen from one minute to the next. (Stephen)
Interestingly, two participants, who identified as female at first point of homelessness, described entering manipulative or abusive relationships in order to secure housing. Sarah explained how she would form relationships with strangers to secure temporary housing. This was concerning, given Sarah’s admission of low risk awareness. Sarah considered whether her experiences may have broader implications for autistic women experiencing homelessness:
you might find that quite a lot of them end up in relationships that they might not necessarily want to be in because it’s better than the other option . . . women I guess tend to find it a bit easier to find other ways of not being on the streets. (Sarah)
Navigating support systems: lacking knowledge and barriers to access
Participants felt unprepared for homelessness and unsure of how to access and navigate services. Stephen described how becoming homeless as a teenager and not knowing how to get help undermined his self-worth:
I didn’t feel like I was worth anything whatsoever, because at the time I just wasn’t getting any help, I didn’t know where to look for help, no one was helping me . . . I had to try and find it all on my own. (Stephen)
Ellie explained how when she became homeless at 14, she thought that meant she would be homeless for the rest of her life. Ellie’s lack of knowledge was a barrier to rehabilitation which severely impacted her physical health:
I didn’t know how to start, I didn’t know who to talk to . . . I went four years without benefits, without a bank account, without ID, because I didn’t know what the fuck to do, I went down to five and a half stone, I was literally emaciated, you could see all the bones in my body. (Ellie)
Participants tended to approach their local authority and other support services, such as emergency night shelters, following guidance from a friend or family member. However, this often took a long time and was difficult for participants with small support networks. Once participants did approach services they encountered multiple barriers to access. One such barrier was not being considered ‘needy’ enough to warrant support. David explained how his mental health and substance use difficulties were not considered to be ‘severe’ enough for access to statutory support. These findings were concerning, given that participants’ substance use escalated, and their mental health deteriorated, during periods of street homelessness. It illustrated a damaging approach to eligibility; meaning participants’ conditions had to worsen before they were helped.
Participants who had an autism diagnosis when they approached their local authority explained how this did not usually qualify them for support. They also reported high levels of social anxiety and found it difficult to explain how autism impacted day-to-day functioning. Neil told a housing officer he enjoyed rough sleeping, a preference which is explored in more detail below. Instead of thinking of adaptations to make hostels more appealing, Neil’s admission was used as a reason to deny support:
I enjoy being on the street, they knew that, they knew that it wasn’t a problem for me, my sister said that I shouldn’t have said that because that’s why they are holding me back . . . she said they don’t understand who you are and your autism. (Neil)
Most participants adopted masking techniques to disguise autistic behaviours. For example, Ellie explained how she would supress stims to stop people perceiving her as ‘childlike’. However, this could downplay need when attempting to access support. Overall, participants reported a lack of awareness of the difficulties autistic adults face in their day-to-day lives. This issue was eloquently explained by Sarah who highlighted how, as a hidden disability, the impact of autism is often underestimated:
autistics who appear to be functioning like me, society just goes well you are fine you don’t need support, and then there’s nothing, we fall through the cracks, especially as adults . . . [the way that] labels are applied, is generally not how the person is functioning but how well they appear to be functioning, so mild autism is having a mild effect on other people and severe autism is having a severe effect on other people, it’s nothing to do with the individual themselves. (Sarah)
Unsuitable accommodation and support
Once housing support was accessed, a common concern was the hostel, shelter or supported living environment. Overcrowding and support needs of other residents led to concerns around confrontation, interpersonal interaction and social anxiety. Stephen found the high-support hostel he lived in overwhelming and struggled with panic attacks and blackouts. Similarly, despite having low support needs, Ellie and David were placed in a high-support hostel due to space availability. Ellie explained how interaction with other residents was detrimental to her mental health:
noise, confrontation and drug abuse, and I have had my issues but I have been clean for ages and I just don’t want to be involved, and it’s kind of hard when you are locked in a box . . . yeah I have had panic attacks since being here because it gets really full on and kicking off and it’s like screaming and shouting at 4am. (Ellie)
Unsuitable accommodation provision could also aggravate sensory processing difficulties and mental health issues. Michael explained how being moved to a ground floor room exacerbated his hypersensitivity to sounds and triggered his psychosis:
[I felt] like I was an animal in a zoo, and people sort of peering down and looking . . . I’m very sensitive to sounds . . . so it might just be that the hum of the bass of a telly, and quite often that sound will turn into a phrase . . . it all comes under that sphere of change I guess and not having the capacity . . . to be able to deal with those things. (Michael)
With limited control over their housing options, participants were also fearful about where they might be placed in the future. Charles was concerned that his autism may make him an easy target for others:
those people you just get mixed in with, and that makes it very hard. I’m not saying all autistic people are saints, they’re not, but a lot of us are quite timid and vulnerable and not aggressive and these other people are very aggressive and they are not reasoners. (Charles)
Participants also voiced concerns over interactions with staff and inadequate support. For participants without a diagnosis of autism, interpretation of behaviour as confrontational resulted in sanctions and could lead to eviction. Bryan had recently received a sanction from his hostel following a disagreement with support staff. He explained that he was being assessed for autism and asked for adaptations to the way staff worked with him. However, this request was refused on the basis the diagnosis was not yet official. Similarly, prior to his diagnosis, Stephen explained how he fell out with his support worker who could not understand Stephen’s need to stick to a pre-agreed meeting time. Stephen was moved, with no warning, to a high-support hostel, meaning he was no longer eligible to bid for independent housing. He explained how he felt he was stuck in the system:
The night before I moved they told me that I am moving, didn’t even give me a whole day notice . . . so I have put everything else on hold in trying to deal with this, which wasn’t the right thing to do really but when too much happens I just can’t cope . . . I have been in the homelessness system for ten years, I still haven’t got my flat and that’s really frustrating for me because I have tried jumping though all their hoops, I have tried doing everything everyone has asked me to do, one mistake and I am . . . back to square one. (Stephen)
For the majority of participants, the accommodations offered by services were seen as something to endure as opposed to a positive step towards independent living. As issues went unresolved, participants tended to isolate themselves which could have detrimental impact on mental health. However, despite the difficulties they encountered, participants expressed a desire to change the system, challenging discriminatory practice and pushing for adaptations to services. In addition, some participants wanted to become key workers at homelessness services, noting they were in a unique position to offer support:
I actually want to become a key worker here, which is odd for someone who has my difficulties but it is because I fucking get it, I get what it feels like, I get where the barriers are . . . you can’t equip someone with tools if you don’t carry them. (Ellie)
Reclaiming autonomy and ‘choosing’ homelessness
Due to the lack of choice and unsuitability of available support, most participants expressed a level of distrust and resentment towards services. Alex explained how he often refused to follow the rules of his hostel. In doing so, he was able to claim back some autonomy, but this also impeded progression to independent housing:
your face fits, sound, if you do like they tell you, like you are a fucking robot, like you can’t think for yourself, then you get a lot further, but sorry I ain’t like that and I won’t be that way. (Alex)
Some participants also referred to ‘choosing homelessness’, opting to sleep rough or stay in squats or vehicles, as opposed to accessing hostels. This was beneficial due to the reduction in forced social interaction and control over sensory environment. David explained how he would travel long distances to find quiet and safe places to sleep. While this was not ideal, he was able to exercise control in a way which was not possible in hostels and shelters. Other participants agreed that rough sleeping allowed them to have the space they needed and relieved anxiety around meeting social expectations. Neil explained why sleeping on the streets was preferable to staying in hostels:
I just enjoy it . . . just chill, just everything is calm, there is nobody watching over your back like waiting to have a pop at you because you are not doing this or you are not doing that. (Neil)
Neil had a wish to live self-sufficiently, without interference from society. Interestingly, he spoke about his experiences of rough sleeping in a romanticised way which emphasised freedom. By contrast, participants who were placed in supported accommodation or hostels were expected to apply for benefits, budget and repay debts. While homeless, Michael explained how he felt he could be himself:
I was unhappy but I didn’t have to answer to anyone, I didn’t have to feel guilty for being who I was because I had chosen to walk away from all of that . . . I was living out the back of my van or I was living out of a rucksack . . . and that was quite stress free, I didn’t have any obligation to be anywhere. (Michael)
With perhaps the exception of Neil, data revealed that participants’ choice to become, or remain, street homeless can be viewed in the context of the limited options available to them. This ‘choice’ was informed by negative experiences of housing support, and participants cited multiple negative impacts of street homelessness on their mental and physical wellbeing. In addition, most participants were recruited through hostels and were thus attempting to persevere through the difficulties they encountered. Ellie described her attempt to stay in the system in the hopes of eventually gaining independent housing as an internal struggle:
I really do struggle with it, like there has been a few times I have almost been like fuck it I am going back down to the (area for rough sleeping), but I’m not going to, but the temptation is there because it’s normal, but normal doesn’t necessarily mean good, which is what I am aware of, *whispers* I am not going back to that . . . I refuse. (Ellie)
Discussion
Study findings suggest the autistic experience of homelessness varies according to personal circumstance. The forms of homelessness participants experienced were not unusual and reflect reported trends in the general homeless population (Bramley, 2017). However, findings highlighted how some participants preferred rough sleeping to hostel environments which aggravated social anxiety and sensory processing difficulties. This tentative finding may explain the high prevalence of autism reported in rough sleeping populations (Churchard et al., 2019; Pritchard, 2010). The fact that many participants experienced sofa surfing is a novel finding which suggests autistic adults may be susceptible to ‘hidden homelessness’ and thus less visible to services and less likely to be counted in official statistics (Downie, 2018).
Only a minority of participants had a clinical diagnosis of autism at first point of homelessness. This mirrors research that has recorded low rates of diagnosis among homeless, autistic people (Campbell, 2015; Churchard et al., 2019). As noted by Garratt and Flaherty (2021), an autism diagnosis can be a pre-requisite for housing support. However, participants of this study did not report swift access to support when a diagnosis was disclosed to a local authority. This contrast suggests it is not the diagnosis itself which secures service access but the extent to which autism is recognised by a local authority, or individuals within that authority, as warranting priority for support. When homelessness services had low autism awareness, access was contingent upon how well participants were able to explain their needs. This represented a significant barrier, given the association between autism and interpersonal interaction difficulties as well as participants’ use of masking techniques to hide autistic behaviours. While some participants accessed services with help from family or friends, these support networks could be an anomaly, given the high rates of social isolation reported in the wider autism literature (Howlin & Magiati, 2017). Furthermore, the onus to increase accessibility should reside with services as opposed to service users. Unfortunately, these concerns are not unique to autism as applicants to housing services are often denied the opportunity to explain their needs (Mackie et al., 2017).
Participants who were accepted as statutory homeless noted significant concerns about the hostel environment and accompanying support. These findings reflect several studies examining neurodevelopmental disabilities and homelessness, which found placements are often unsuitable and unsustainable in the long term (Colman et al., 2007; Hebblethwaite et al., 2007; Oakes & Davies, 2008). More specifically, this study substantiates Kargas et al.’s (2019) finding that shared accommodation with large groups is a significant barrier to autistic people engaging with homelessness services. Unsuitable service provision could cause participants to disengage with services and return to rough sleeping, resulting in cycles of episodic homeless which are unlikely to be broken without targeted intervention. This is particularly concerning, given the association of rough sleeping with increased physical and mental health issues (Homeless Link, 2014).
The experiences of participants in this study suggest that improvements to service access and engagement should be driven by three key principles: increasing awareness, removing barriers and prioritising autism. These are set out in Figure 1, and discussed in further detail below.
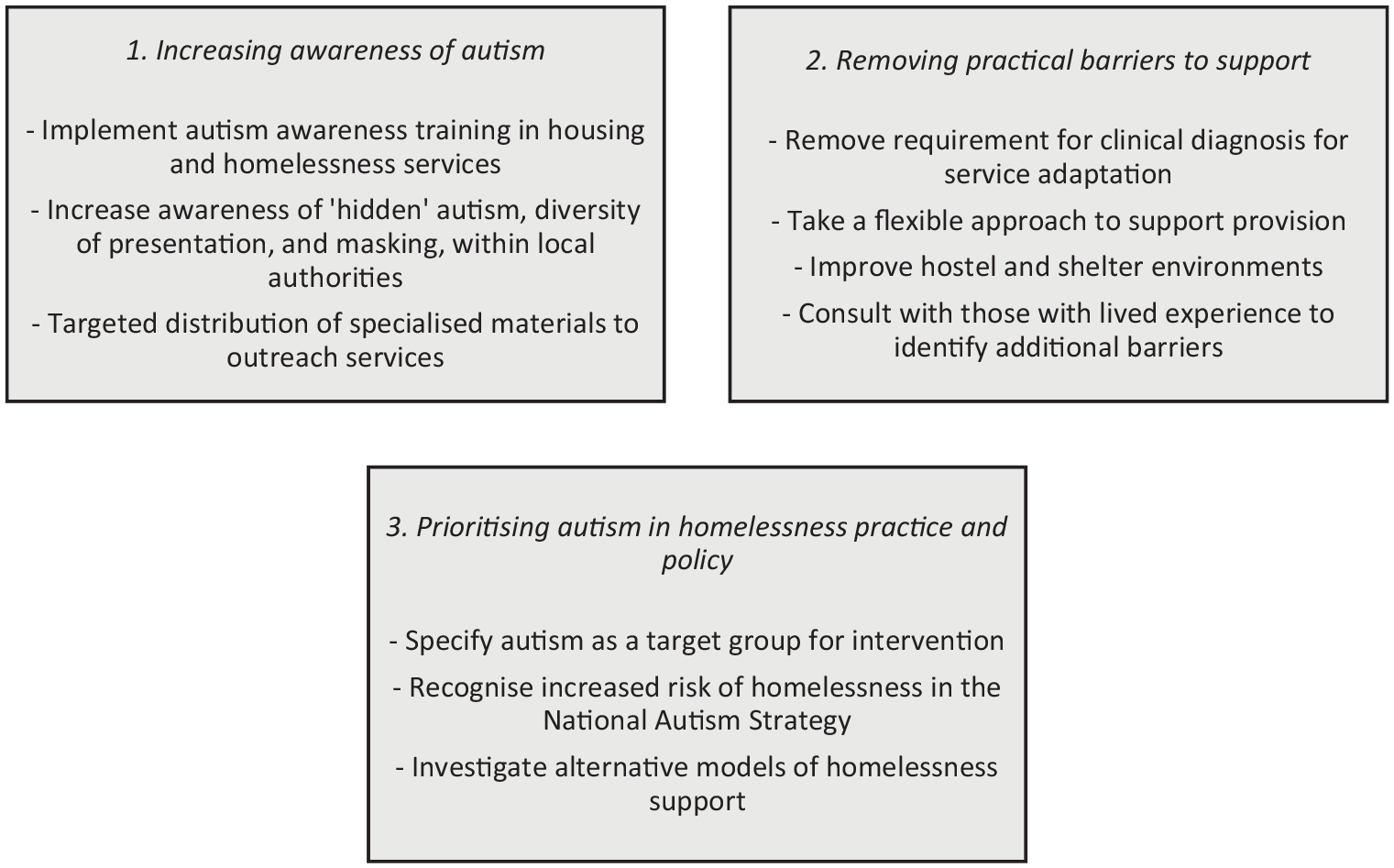
Principles to improve service access and engagement.
The examples given in Figure 1 are not exhaustive but provide a foundation from which to improve support. The first principle involves increasing autism awareness across housing and homelessness services. This could be achieved through implementing training to help staff both recognise autism and adapt support in accordance with need. Training should consider how service users may mask autistic symptoms and address use of language such as ‘high-functioning’, which can lead professionals to make assumptions about how a person is coping and has been associated with exclusion from mental health services (Camm-Crosbie et al., 2019; Kenny et al., 2016). Increasing autism awareness must therefore include recognition of the impact of autism and co-occurring conditions. In addition, frontline staff should be aware that autistic people may be prone to rough sleeping and sofa surfing, and that they may lack knowledge on how to access support services. The development of recent guides for practitioners and autistic service users (Autism Wales, 2019; Westminster Homelessness and Health Coordination Project, 2018) should be utilised to support rehabilitation.
Second, there is a need for the identification and removal of individual barriers to housing and homelessness services for autistic people. The requirement for clinical diagnosis before services were willing to recognise eligibility or implement adaptations represented a significant barrier to service access and engagement. This was surprising, given that requested adaptations, such as keeping to agreed times and giving forewarning of change, are relatively easy to implement. Taking a flexible approach to support in recognition of individual need, and considering environment prior to placement could help to prevent autistic people returning to street homelessness. Furthermore, the willingness of participants in this study to use their lived experience to support others could represent an untapped resource which should be utilised to identify additional barriers to service engagement.
Finally, research on addressing complex needs in homelessness services suggests subcategories should be created for targeted intervention. This would allow services to focus on creating suitable housing environments, increasing training and prioritising housing allocation (Mackie et al., 2017). Given the unsuitability of current provision autism should be recognised as a distinct subcategory by homelessness and housing services. A recent initiative in London introduced personalised support for people with identified needs, including autism. The initiative aims to reduce homelessness, helping service users to access community resources and build support networks as well as providing an autism drop in centre (Single Homelessness Project 2018). This co-ordinated approach acknowledges the multitude of difficulties facing homeless, autistic adults and there is merit in developing similar schemes across the United Kingdom.
Suggested changes should be supported by policy amendments which recognise the disproportionate representation of autism in homeless populations and set precedence for local initiatives. Homelessness is not addressed in the Autism Act of 2009 (UK) and its subsequent updates, or the National Strategy for Autistic Children and Adults (Department of Health and Social Care & Department for Education, 2021). However, given mounting pressure on homelessness services in England, prioritising autism as a category for targeted intervention would require large amounts of additional funding, or risk diverting existing resources away from other service users (Wilson & Barton, 2018). Alternative models of housing support, beyond the provision typically offered in the England, may be more suited to the rehabilitation of homeless, autistic people, but have yet to be investigated.
Limitations and implications for future research
The authors acknowledge several limitations to this study and gaps in research findings. While underrepresented in this study, findings suggest homeless autistic women may form relationships to secure temporary shelter. This is of note, given the lower risk awareness reported among autistic adults (Ratto & Mesibov, 2015), and tendency of homeless women to enter romantic relationships to avoid rough sleeping (Clement & Green, 2018). In addition, in forming these relationships, autistic homeless women may be less visible to homelessness services and at risk of sexual exploitation (Clement & Green, 2018; Garratt & Flaherty, 2021). Further research is necessary to explore the homeless experience of autistic women.
Exploring youth homelessness was beyond the remit of this article but may be associated with the adverse childhood experiences (ACEs), such as emotional and physical abuse, reported by participants who first experienced homelessness in childhood or adolescence (Embleton et al., 2016; Llamau, 2015; Stone, 2021). Two participants identified with a different gender to the one they were assigned at birth, thus representing another marginalised group who experience disproportionately high rates of homelessness (Bachmann & Gooch, 2018). These complexities suggest autism cannot be considered in isolation, and that the autistic experience of homelessness is a multifaceted phenomenon which may intersect with multiple factors including age, race, gender, sexual identity and past trauma.
The lack of national legislation in homelessness policy and resulting regional variation may reduce the generalisability of this study. However, while participants were recruited in the South West of England, a narrative methodology allowed for examination of homelessness over a prolonged period. For some participants this included time spent homeless in London, the surrounding South East, Wales and Ireland.
Similarly, while most participants were recruited from hostels for the statutory homeless, the use of narrative methods gave insight into multiple forms of homelessness experienced across the life course. It is acknowledged, however, that there is likely a subset of autistic, homeless people who are not accepted as statutory homeless. The experience of autistic people in hard-to-reach homeless populations, such as entrenched rough sleepers, or those in insecure or temporary accommodation, warrants further investigation.
Finally, issues relating to self-reporting and the role of the researcher in the co-construction of narratives has traditionally lead to an emphasis on narrative context as opposed to questions of fact (Miller, 2000). The authors acknowledge, but ultimately reject, this position on the basis that it disregards historical truths as an important component of narratives and serves to undermine the voices of an already marginalised group. The nuanced and detailed accounts relayed by participants demonstrate how those with lived experience are best placed to identify barriers to housing and homelessness support and actualise social change.
Footnotes
Acknowledgements
The authors extend their deepest gratitude to the participants of this study whose generosity of time and insight made this research possible. We hope we have done their words justice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Economic and Social Research Council (grant no: ES/P000630/1).