
Abstract
Autism is a heterogeneous diagnosis with symptoms that present in different ways. There is a large variety of interventions for autistic individuals. However, little is known about who chooses which specific interventions. We aimed to explore intervention prevalence and predict intervention use, based on demographic and autism-specific characteristics. This study used data on autistic children (N = 1464, aged 1–17 years) from the Netherlands Autism Register. Most children (88%) had received therapies, and about half had received medication. Intervention use was mostly related to additional factors (lower IQ, special education and co-occurring diagnoses). Children with a lower IQ received less therapies, children attending special education or with a co-occurring diagnosis received more therapies. Children in special education or with a co-occurring diagnosis were more likely to receive several types of therapy and medication. Older age, higher IQ and being female were related to more guideline (autism-specific) or mainstream (targeting co-occurring problems) therapy use. Lower parental education was related to more mainstream medication use. More severe sensory issues increased the chance of other medication use. Other autism-specific characteristics (autism severity, social skills, repetitive and restrictive behaviours) were not related to intervention use. More transdiagnostic interventions should be available for children with autism who have additional difficulties.
Lay abstract
Autism is a condition that is characterised by social communication difficulties and restrictive and repetitive behaviours or interests. Autism can present in many different ways and various interventions are available. Some interventions are conventional, and they are recommended to be used for children with autism (guideline therapies) or for other disorders such as anxiety or attention-deficit hyperactivity disorder (mainstream therapies or medication), while others are less conventional (other therapies or medication, they are discouraged, unknown or alternative). Little is known about who chooses which intervention. This study found that most autistic children use some kind of intervention. Children who attend special education or have an additional diagnosis (other than autism) tend to receive more therapies, while children with a lower IQ receive fewer therapies. Older children, children with a higher IQ and girls are more likely to use conventional (mainstream or guideline) therapies. Children whose parents have a lower educational level are more likely to have used conventional medication. Whereas, children with more sensory issues (e.g. sensitivity to sound, smell or movement) were more likely to have used unconventional medication. This study found that other autism-related characteristics such as the number of autism symptoms, social skills and repetitive and restrictive behaviours were not related to the interventions used. More treatments focussed on multiple problems should be available for children with autism who have additional difficulties.
Keywords
Autism is a heterogeneous diagnosis, and it is defined by atypical social communication as well as restrictive and repetitive behaviours or interests (American Psychiatric Association (APA), 2013; Lord et al., 2020). In addition, the majority of autistic children (70%) have at least one other psychiatric diagnosis (Simonoff et al., 2008). Many different interventions are available for autistic individuals (DeFilippis & Wagner, 2016), some aimed at reducing core autism symptoms while others target co-occurring problems. The diverse nature of autism and its treatment options justify the need to understand which individual characteristics are associated with the use of which intervention. In this study, demographic and autism-specific characteristics will be used to predict intervention use in autistic children.
The estimated total (personal and societal) lifetime costs of supporting a person with autism (without an intellectual disability) is US$1.4 million (Rogge & Janssen, 2019). The majority of these costs are accounted for by services, such as interventions. There is no intervention that can cure autism nor is this a desired outcome according to most people (Kapp et al., 2013). Interventions instead focus on reducing autism-specific symptoms, alleviating co-occurring problems or improving overall quality of life. Guidelines for autism treatment agree that interventions should start as early in life as possible. Most guidelines advise psycho-education to be used as a crucial step in treatment. In addition, guidelines state that interventions should also reduce core autism symptoms and stimulate social behaviour or social learning abilities. Furthermore, specific problems should be targeted, and long-term care should be established (see the Dutch Youth Institute (NJI; van Rooijen & Rietveld, 2017), the Dutch mental health care quality standards (GGZ Standaarden [GGZS], 2020), the European Society of Child and Adolescent Psychiatry (ESCAP; Fuentes et al., 2021), the British National Institute for Health and Care Excellence (NICE, 2013) and the Centres for Disease Control and Prevention (CDC, 2019)).
The majority of diagnosed autistic children between 2 and 17 years of age receive therapy (we define therapy as non-medication interventions) with estimates ranging from 64% to 96% (Monz et al., 2019; Patten et al., 2013; Xu et al., 2019). On average, young children (2 to 7 years old) have received 4.5 different therapies (ranging from 1 to 11; Patten et al., 2013). Medication use is less common than therapies among autistic children, ranging from 27% to 34% (Mayes et al., 2020; Monz et al., 2019; Xu et al., 2019). Medications generally included drugs for symptoms of attention-deficit hyperactivity disorder (ADHD), depression and anxiety (Eissa et al., 2018; Mayes et al., 2020). Unsurprisingly, people with autism who have co-occurring psychiatric problems were more likely to use medication (Houghton et al., 2017). While the use of therapies decreased with age, both in number (Mire et al., 2015; Xu et al., 2019) and intensity (Monz et al., 2019), medication use increased with age among those up to 24 years old (Houghton et al., 2017; Mire et al., 2015). A change in the manifestation of the child’s symptoms might make parents more comfortable giving medication to older children, or because medication is a last resort for parents who have tried a variety of interventions during their child’s younger years (Mire et al., 2015). One study found a higher percentage of autistic boys using medication than girls; however, in the same study, sex was not a significant predictor of medication use (Xu et al., 2019).
Treatment guidelines for autism are based on scientific evidence, general practice and the theoretical foundation underlying the interventions. Looking at – freely available – guideline directions for four different nations (the United Kingdom, the United States, Europe and the Netherlands), three categories can be distinguished that are included in all guidelines (CDC, 2019; Fuentes et al., 2021; GGZS, 2020; NICE, 2013; van Rooijen & Rietveld, 2017). First, there is a stable international agreement on what would be considered as guideline interventions for autism. These interventions are officially recommended by national government organisations/institutions for mental health, specifically for autism or target core autism symptoms, such as social skills and restrictive and repetitive behaviours and interests. These interventions can be directed at the child, family or community (Lord et al., 2022). In all referenced guidelines, these include psycho-education (for both child and family), social skills training and naturalistic developmental behavioural interventions (NDBIs) for the child, and parent and home trainings for the family. Second, mainstream interventions include interventions not specifically for autism, targeting associated symptoms (e.g. challenging behaviours such as aggression or hyperactivity) as well as co-occurring problems (e.g. epilepsy or sleep problems). These interventions are included in guidelines for autism to treat co-occurring problems. This category includes medication (Houghton et al., 2017) and, among others, physiotherapy (also referred to as physical therapy), speech therapy and mindfulness-based interventions. Third, other interventions are therapies or medications that are not included in the treatment guidelines or are actively discouraged by the guidelines (e.g. because they have shown to be harmful or ineffective). This includes alternative interventions such as diets, supplements, homeopathic medication (often referred to as complementary and alternative medicine (CAM)) and animal therapy (Höfer et al., 2017).
Factors that influence parents’ decision-making about interventions change over time as parents gain more expertise about autism (Edwards et al., 2018). Parents base their decisions on a variety of factors including recommendations from other parents, professionals and service providers, pragmatic issues (e.g. the availability or accessibility of the intervention, the costs and time), service characteristics (e.g. whether the staff seems experienced and professional), and their child’s individual needs (Carlon et al., 2013, 2015; Edwards et al., 2018; Lord et al., 2022). Furthermore, research suggests that higher parental education levels were associated with a higher number of interventions (Patten et al., 2013), and also more use of alternative interventions, including dietary and vitamin therapy (Höfer et al., 2017). Family income is not related to intervention use when taking parental education level or health insurance into account (Patten et al., 2013; Xu et al., 2019). Insured children are more likely to receive behavioural interventions in the United States (Xu et al., 2019).
Child characteristics also affect intervention use. Children with more severe autistic symptoms received a greater number of therapies regardless of their age (Green et al., 2006) and are more likely to have received a therapy, from any category, compared with children with less severe symptoms (Green et al., 2006). Children who have more sensory processing problems started using interventions earlier (Patten et al., 2013). Understandably, children with special communication and language needs often received speech therapy, whereas social skills training and play therapy were used when parents wanted to improve their child’s peer interaction (Carlon et al., 2013). These findings suggest that intervention use in autism is related to the presence and severity of autism-specific symptoms.
The use of alternative interventions is particularly interesting given that these interventions often have no or a dubious empirical foundation for their effectiveness and can sometimes even be harmful. There is some evidence that the use of CAM interventions is more common in autism compared with other disorders (Höfer et al., 2017). Overall, higher parental education level has been associated with more CAM use – in both autism and other populations (Höfer et al., 2017; Patten et al., 2013; Wang et al., 2018). Other predictors include parents’ own use of CAM interventions (Doering et al., 2013; Singendonk et al., 2013), female gender (Keene et al., 2019; Singendonk et al., 2013), higher level of education of the parent (Keene et al., 2019; Wang et al., 2018) and co-occurring medical conditions (Wang et al., 2018).
Autism treatment is expensive and early intervention can be crucial. Most previous studies have been conducted in the United States or the United Kingdom (e.g. Patten et al., 2013; Wang et al., 2018; Xu et al., 2019), and this is the first study of its kind focusing on Dutch families. Although many different and divergent predictors of intervention use have been found in a variety of studies, we aim to increase our understanding of intervention use among autistic children by combining demographic and autism-specific characteristics to predict the use of therapy and medication. We aim to study predictors of the number, type and load (total number of hours) of interventions used among autistic children. Predictors are demographic characteristics (age, sex, parental education level, educational setting) which also include diagnostic information (IQ, co-occurring diagnosis) and autism-specific characteristics (autism severity, social skills, repetitive and restrictive behaviours and interests, and sensory issues). Based on the above-discussed literature, we expect co-occurring diagnosis, higher autism severity and increasing age to be associated with a higher number of interventions used. We also expect higher parental education level to predict the use of other therapies and medication. The impact of the other predictors will be explored as there is insufficient evidence from previous literature to formulate a hypothesis.
Method
Participants
Participants included 1464 children (below the age of 18 years) and/or their parent(s) (Tables 1–3) who filled in questionnaires from the Netherlands Autism Register (NAR). Of these participants, 1225 reported on therapy use and 1450 on medication use. All participants received a formal diagnosis of autism spectrum disorder (ASD) by a qualified clinician unaffiliated to this study according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). The diagnosis was reported by the informant, and the follow-up questions ensured the diagnosis was given by a qualified clinician at a professional location, in addition to questions about the age of first suspicion and diagnosis. A subgroup (N = 632; this number is lower when predictors are added due to missing data) was further analysed because information on intervention use from multiple years was available for these participants (Table 1). There were no significant differences between this group and the complete sample on the variables included in this study. Within the subsample, participants who completed the Autism Spectrum Quotient–28 (AQ-28) were younger, and participants who completed the Strengths and Difficulties Questionnaire (SDQ) were slightly older than those who did not complete these measures. There were no other age differences or differences in sex and parental education level.
Demographic information.
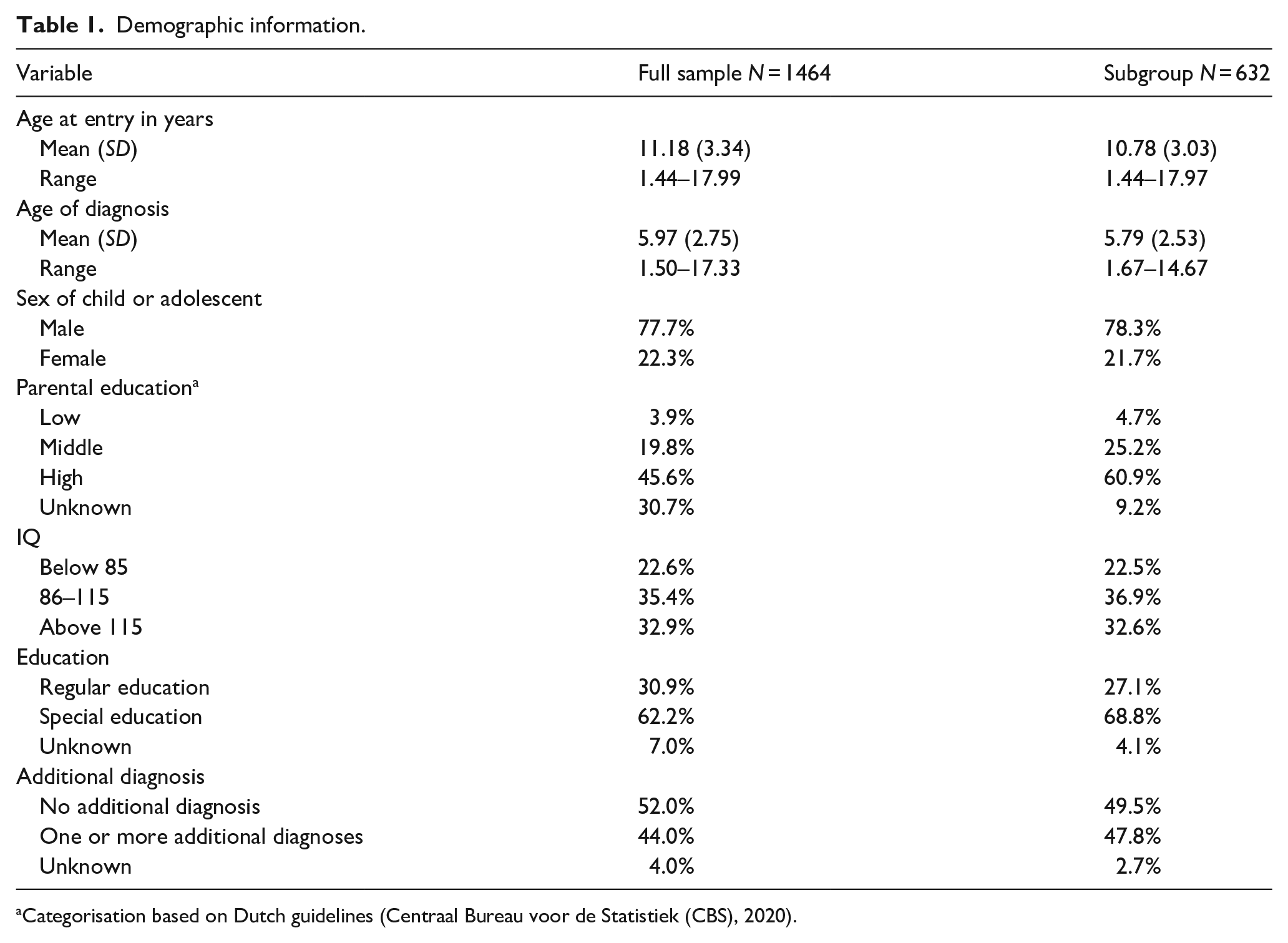
Categorisation based on Dutch guidelines (Centraal Bureau voor de Statistiek (CBS), 2020).
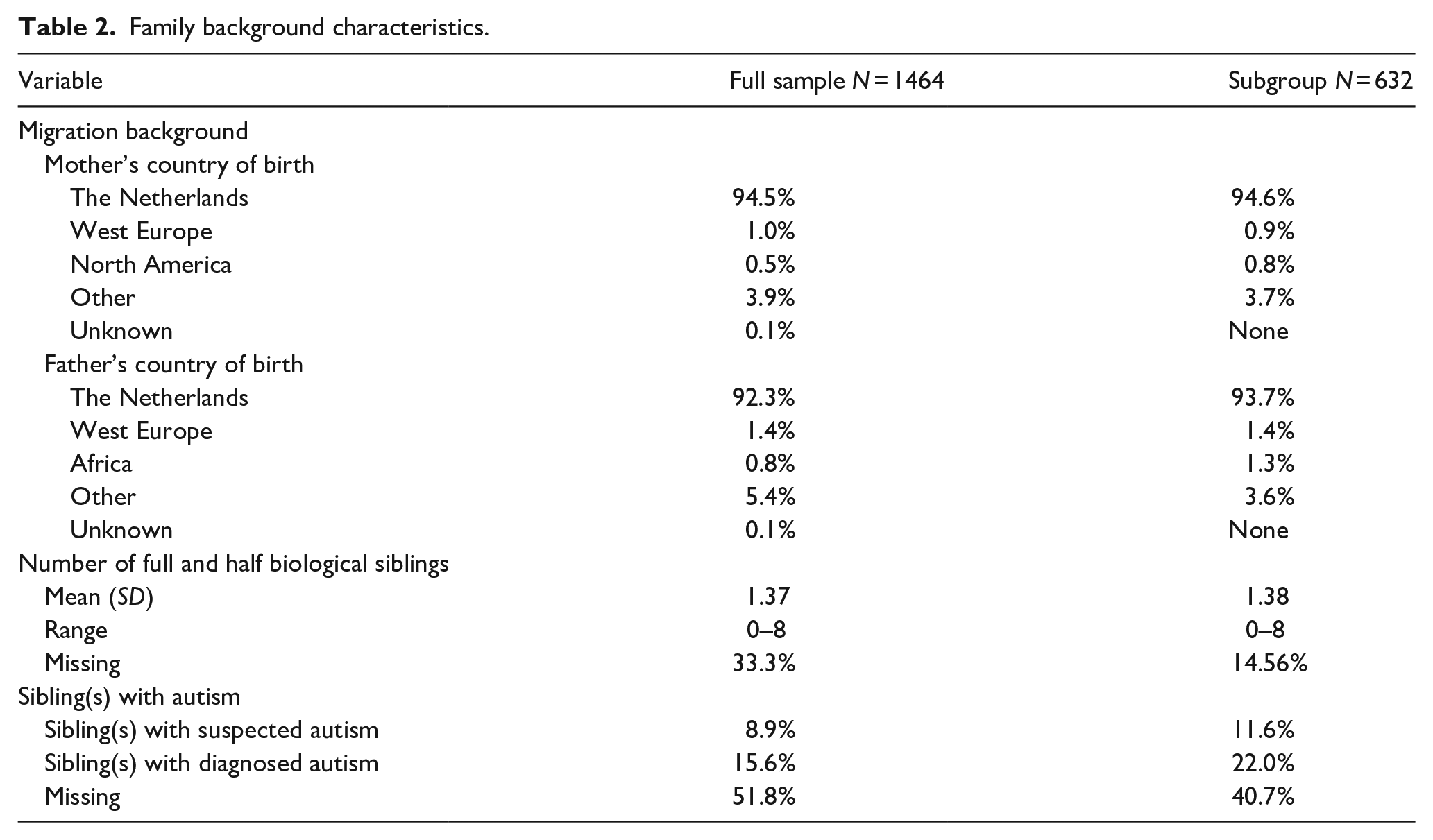
Family background characteristics.
Participant’s scores on autism-specific measures.
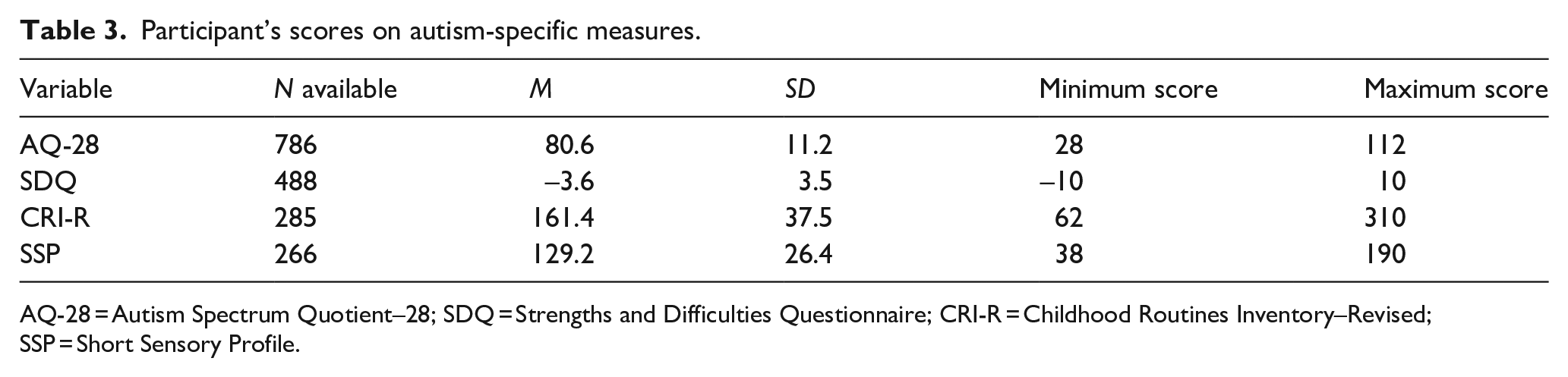
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SSP = Short Sensory Profile.
Measures
Demographic variables
For all measures, parents reported on their child if they were younger than 16 years, and adolescents aged 16 or 17 years reported on themselves. For the category of sex, participants could choose from male or female. Parental education level was categorised as high, middle and low (using the highest from the two parents), based on Dutch guidelines (CBS, 2020). The educational setting was categorised as special or mainstream education. Children who reported attending special education in at least one questionnaire were included in the special education category. Some diagnostic information was also included as ‘demographic variables’: participants were asked to choose their (child’s) most recent IQ test score from seven categories. For 6.6% of the children, no recent IQ test result was available, and these participants were asked to estimate their (child’s) IQ. The different answer options were then combined into three categories: 1 = below 85, 2 = 85–115 and 3 = above 115. For co-occurring diagnosis, children were divided in two groups: those who had no additional diagnoses and those who had at least one additional diagnosis (any diagnosis including psychiatric and physiological diagnoses).
Autism severity
Autism severity was measured by the AQ-short (Hoekstra et al., 2011). The AQ-short has 28 items that assess social behavioural difficulties (23 items) and a fascination for numbers/patterns (5 items). The social behaviour factor includes social skills (7 items), routine (4 items), switching (4 items) and imagination (8 items). Each item has a 4-point Likert-type scale from ‘definitely agree’ to ‘definitely disagree’. Children could score anywhere between 28 and 112 with a higher score reflecting greater autism severity. The AQ-short has been validated to assess autistic traits in three independent samples from the Netherlands and the United Kingdom (both clinical and controls; Hoekstra et al., 2011). The AQ-short highly correlates with the full-scale AQ, and it has shown a good internal consistency with a Cronbach’s alpha between 0.77 and 0.86.
Sensory issues
Sensory issues were measured using the Short Sensory Profile (SSP; McIntosh et al., 1999). This questionnaire has 38 items about observable child behaviours including tactile sensitivity (7 items), taste/smell sensitivity (4 items), movement sensitivity (3 items), underresponsive/seeks sensation (7 items), auditory filtering (6 items), low energy/weak (6 items) and visual/auditory sensitivity (5 items). The behaviours are scored based on their frequency on a scale from 1 (always) to 5 (never). This results in a score between 38 and 190 with a higher score representing less sensory abnormalities, meaning a low frequency of sensory issues. The SSP is widely used to assess sensory impairments and has shown excellent reliability and validity (McIntosh et al., 1999).
Social skills
The Strengths and Difficulties Questionnaire (SDQ; Goodman, 2001; a brief behavioural screening questionnaire) was used to measure social skills. To reflect social skills, two scales of this questionnaire were combined: peer problems and prosocial behaviour. The peer problems scale has five items that focus on how well the child gets on with other children. The prosocial scale has five items that focus on being helpful, kind and considerate towards others. The items on the prosocial scale are recoded to ensure that the combined score of the two scales represents problems with social skills (a higher score reflects more problems). The reliability and validity of the self-report and parent-report SDQ were judged to be satisfying, making it an appropriate short measure for psychological problems and skills in clinical assessment or as a research tool (Goodman, 2001).
Repetitive and restrictive behaviours and interests
The Childhood Routines Inventory–Revised (CRI-R, Evans et al., 2017) was used to measure the child’s repetitive and restrictive behaviours. The questionnaire has 62 items concerning possible restrictive or repetitive behaviours. The items question to what extent the child or adolescent engages in behaviours with the answer options ranging from 1 ‘Never’ to 5 ‘Always’. The CRI-R has two scales: repetitive motor behaviours and compulsions, and rigidity/insistence on sameness. For this study, we use the total score of all 62 items resulting in a score between 62 and 310 with a higher score representing more repetitive and restrictive behaviours. The CRI-R has shown excellent psychometric properties for assessing restricted and repetitive behaviours in children below 18 years with neurodevelopmental disorders (Evans et al., 2017).
Intervention use
Type of intervention
Participants could report on 16 types of therapies and 30 types of medication. At entry, participants reported on their intervention use up to that point. After that, intervention use was surveyed yearly. The total number of therapies was based on the number of therapies used at entry and the average yearly use. Interventions were grouped into three categories: (1) guideline therapies (therapies for core characteristics of autism, for example, social skills training, there is no guideline medication), (2) mainstream therapies or medication (interventions aimed at other associated problems) and (3) other therapies or medication (discouraged, alternative or rare interventions; see Appendices 1 and 2 for a full overview).
Intervention load
Participants reported the duration of each selected therapy with the following options: 0 to 4 months, 4 to 7 months, 7 to 12 months and more than 12 months. They were also asked to report the intensity of the therapy: 0 to 1 h a week, 1 to 4 h a week, 4 to 8 h a week or more than 8 h a week. For the intervention load, the duration of therapies was calculated in weeks by taking the median of the category (e.g. 0–4 months = 2 months) and multiplying this by 4.348 to convert months into weeks. A similar transformation is applied to the therapy intensity by determining the median of the category to get a single value for hours per weeks (e.g. 0–1 h/week = 0.5 h/week). Intervention load was then calculated by multiplying the duration by the intensity to obtain the total number of hours of therapy. The number of hours was then added per year, and the different years were then added. This total number of hours of therapy was corrected for by the number of years that the participant had participated in the questionnaire as mentioned before.
Procedure
Participants are made aware of the NAR by recurrent professional and lay publications in national and local media. People who want to participate in the NAR questionnaires can register on their website (https://www.nederlandsautismeregister.nl/english/). Upon entering the NAR, participants receive a link to fill out the baseline questionnaire, followed by yearly invitations. The content of the yearly questionnaires differs, and every year the participant can decide whether they want to participate or not (without having prior knowledge of the questionnaire content). For this study, data from 2013 to 2019 were used. The study was preregistered at the OSF/Centre for open science (https://osf.io/2uqkg). The NAR has been reviewed and approved by the ethics committee of the Vrije Universiteit Amsterdam (VCWE 2020-041R1).
Statistical analyses
The following analyses were performed on the subsample (N = 632). Multiple linear regression was carried out predict the number of therapies used and intervention load with 10 predictors mentioned in the introduction (age, sex, parental education level, IQ, educational setting, co-occurring diagnosis, autism severity, social skills, repetitive and restrictive behaviours and interests, and sensory issues). Binary logistic regressions were used to predict whether participants used guideline (yes/no), mainstream (yes/no) or other therapies (yes/no) and to predict the use of mainstream (yes/no) and other medication (yes/no). For these analyses, the demographic characteristics were put in the model first. The four autism-specific predictors were then added to the models separately because when they are combined, the sample size decreases significantly. Post hoc power analyses were performed for each regression, and they are reported in Appendix 3.
Community involvement statement
The NAR works closely together with autistic people. We rely on input from the autism community and provide yearly feedback to all participants regarding the general findings of the questionnaires and personal feedback on how the participants scored on the subjects included in the latest questionnaire. This study is in line with the Dutch Autism Research Agenda, which was developed by autistic researchers using data from the NAR (Van den Bosch & Weve, 2019), which indicated that support, treatment and medication were key themes requested by autistic people and parents of autistic children. Autistic individuals work in the NAR team and are consulted through panels.
Results
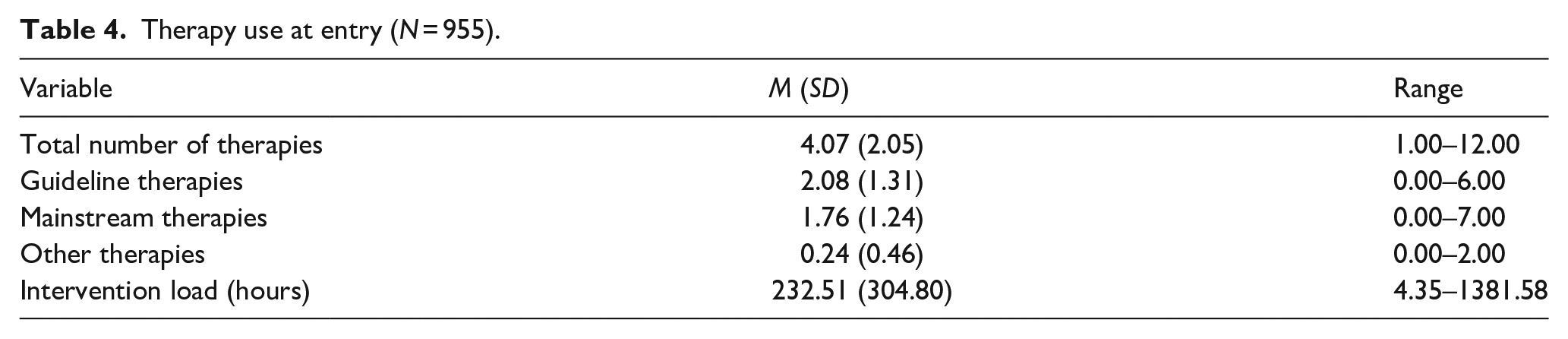
Data on therapy use on at least one time point were available for a total of 1225 children. With respect to these children, 88.1% reported using some type of therapy, 76.6% of the children had used mainstream therapies, 77.2% had used guideline therapies and 27.7% had used other therapies. Only 0.8% received only other therapies. A total of 1450 children reported on medication use of which 51.9% had received medication, 51.4% had used mainstream medication, 4.8% had used other medication and 0.5% received only other medication. When entering the NAR, children had received an average of 4.07 therapies (SD = 2.05, range 1–12). They had used on average 2.08 guideline therapies, 1.76 mainstream therapies and 0.24 other therapies amounting to an average total intervention load of 232.51 h (Table 4). The most commonly reported therapies included physiotherapy, parent training and social skills training (see Figure 1).
Therapy use at entry (N = 955).
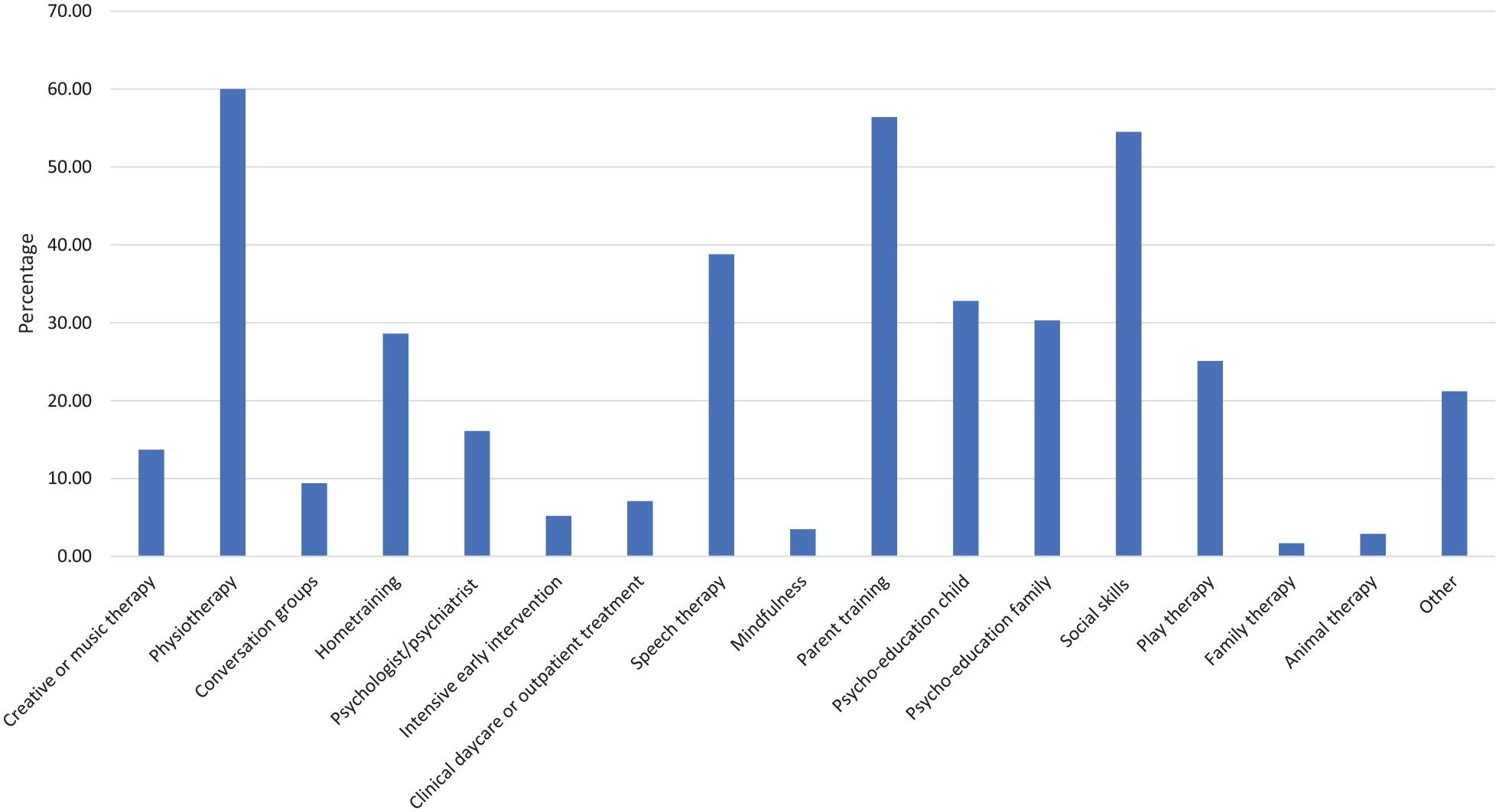
Percentage of children using each type of therapy when entering the NAR (N = 955).
For all analyses of the subsample (N = 632), demographic predictors included age, sex, IQ, educational setting, parental education level and co-occurring diagnosis, and autism-specific predictors included autism severity, social skills, repetitive and restrictive behaviours and interests, and sensory issues. The latter were separately and individually added. The autism-specific predictors were correlated to each other, and some correlated with age (Table 5). However, there was no indication of multicollinearity as all variance inflation factors (VIFs) for the predictors were below 10. Only statistically significant (p < 0.05) results are reported.
Correlations among the continuous predictor variables.
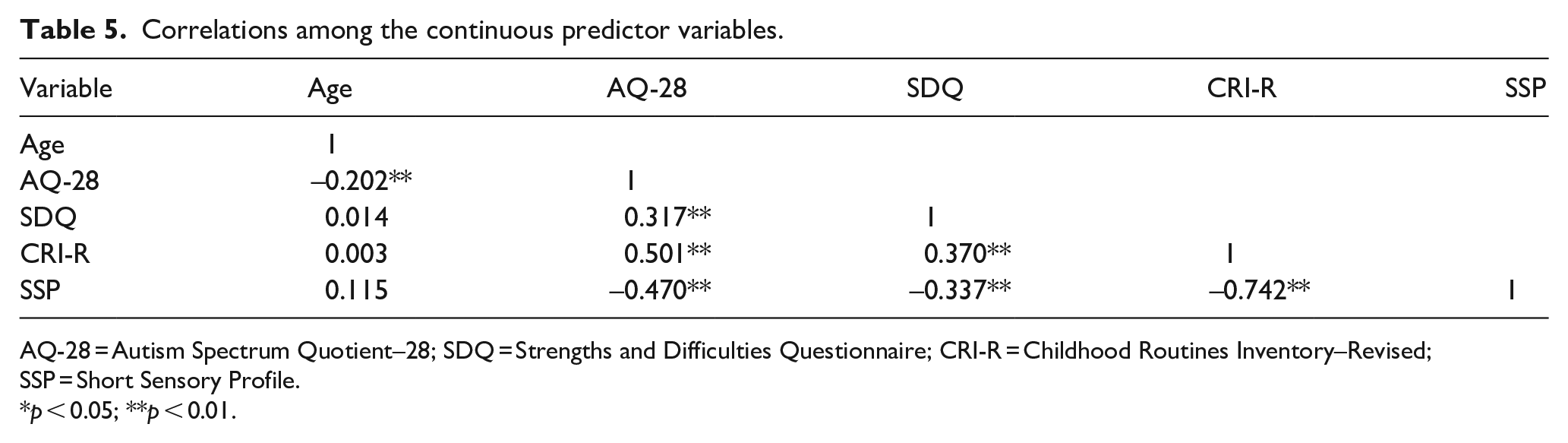
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SSP = Short Sensory Profile.
p < 0.05; **p < 0.01.
A higher number of overall therapies used was predicted by older age (B = 0.14, SE = 0.04), having a co-occurring diagnosis (B = 0.50, SE = 0.25) and special education (B = 1.12, SE = 0.29), while children with a lower IQ used less therapies (B = –0.71, SE = 0.33; Table 6). The use of guideline therapies was predicted by older age (OR = 1.13). Children with a lower IQ were less likely to have used guidelines therapies (OR = 0.41). Boys were less likely to have used a mainstream therapy (OR = 0.28) while children who attend special education were more likely to have used a mainstream therapy (OR = 3.49). Children with a co-occurring diagnosis were more likely to have used other therapies (OR = 1.70). None of the autism-specific variables were predictive for therapy use (Table 7).
Multiple linear regression to predict the number of therapies used.
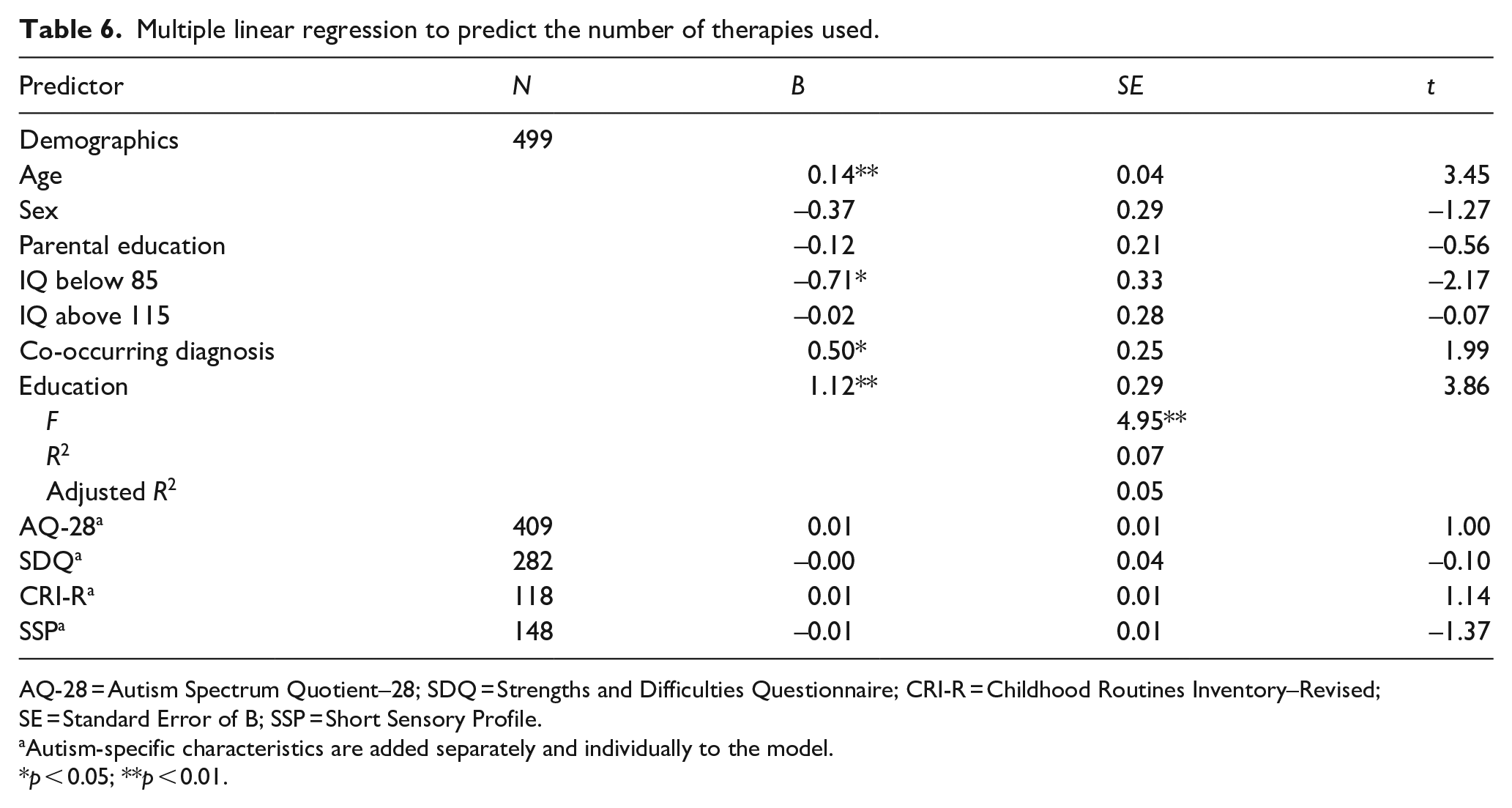
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SE = Standard Error of B; SSP = Short Sensory Profile.
Autism-specific characteristics are added separately and individually to the model.
p < 0.05; **p < 0.01.
Binary logistic regressions to predict use of guideline, mainstream and other therapies.
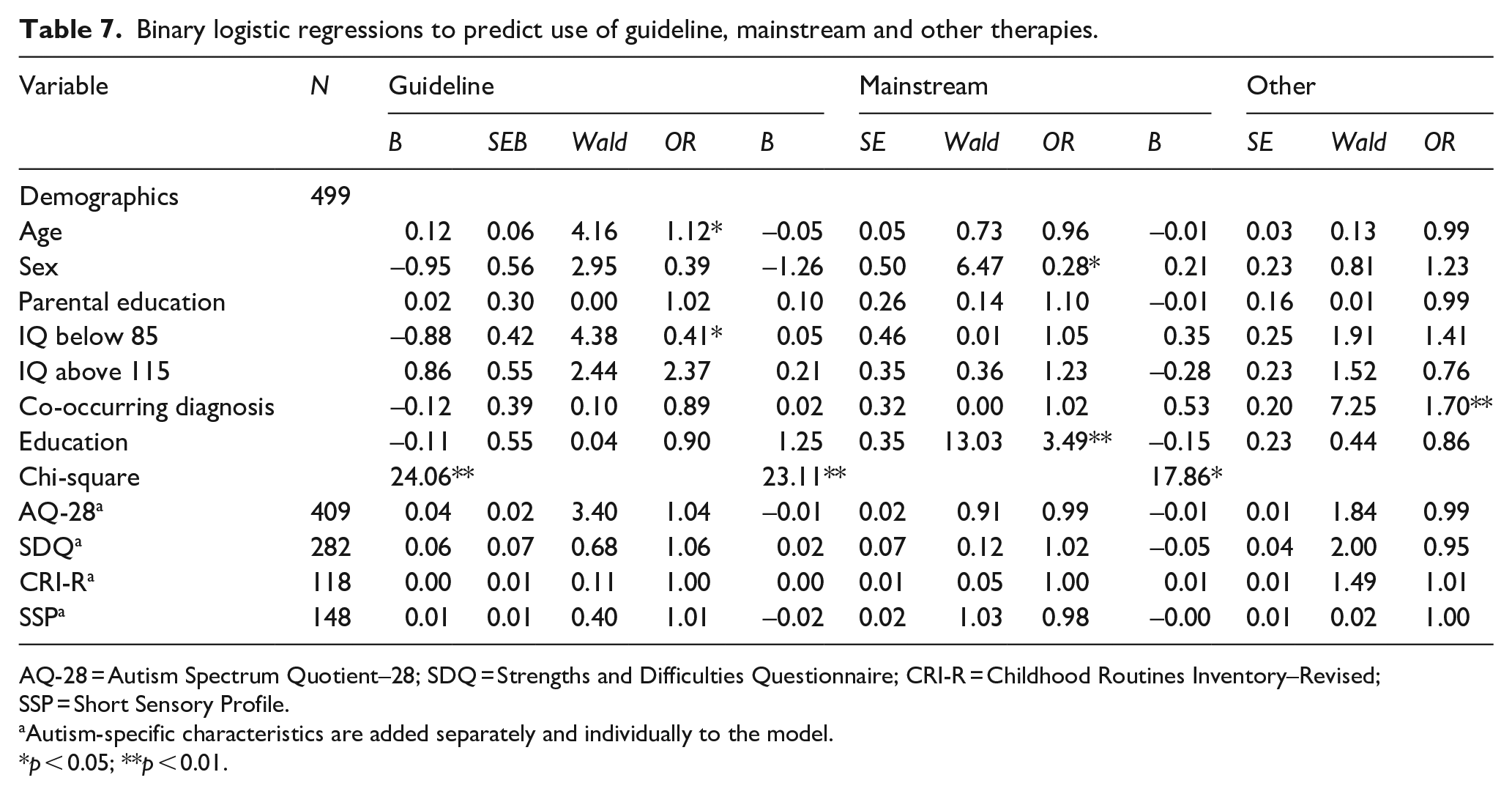
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SSP = Short Sensory Profile.
Autism-specific characteristics are added separately and individually to the model.
p < 0.05; **p < 0.01.
Higher parental education level decreased the chances of having received mainstream medication (OR = 0.48). Children who had a co-occurring diagnosis or attended special education had increased chances of having used mainstream medication (OR = 2.14 and OR = 1.97, respectively). Children with more sensory issues were more likely to receive other medication (OR = 0.98, note the SSP is scored reversely; a higher score indicates less sensory issues). None of the other autism-specific variables were significant predictors for medication use (Table 8). There were no significant predictors of intervention load (Table 9).
Binary logistic regressions to predict use of mainstream and other medication.
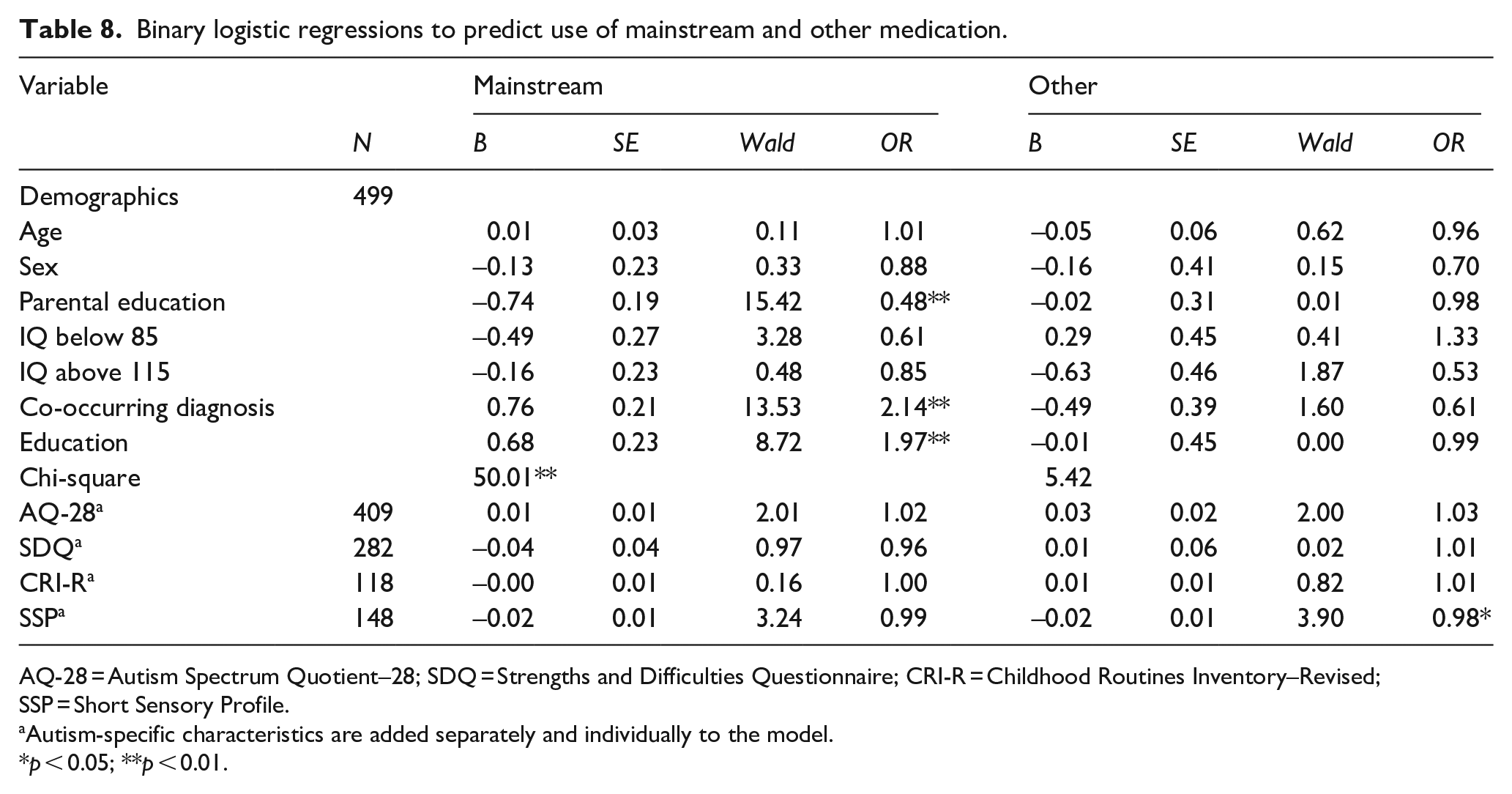
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SSP = Short Sensory Profile.
Autism-specific characteristics are added separately and individually to the model.
p < 0.05; **p < 0.01.
Multiple linear regression to predict intervention load.
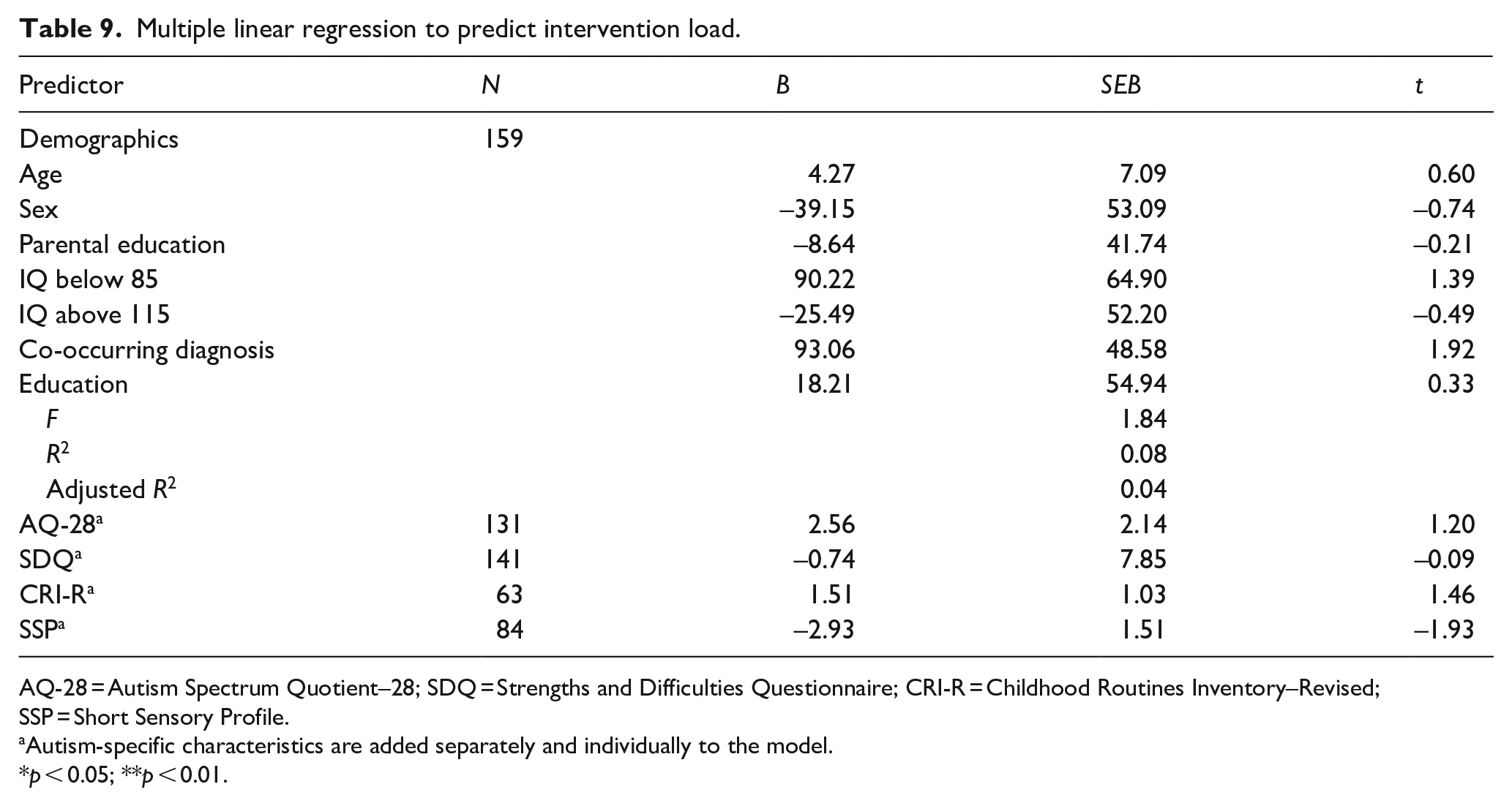
AQ-28 = Autism Spectrum Quotient–28; SDQ = Strengths and Difficulties Questionnaire; CRI-R = Childhood Routines Inventory–Revised; SSP = Short Sensory Profile.
Autism-specific characteristics are added separately and individually to the model.
p < 0.05; **p < 0.01.
Moreover, all analyses were rerun using only parent-reported data (children younger than 16 years) to ensure the results are not influenced by the self-reported data. There were no significant differences in the results between the sample including 16- and 17-year-olds and the sample excluding them, and the same predictors for intervention use were found. See Appendix 3 for the post hoc power analyses.
Discussion
This study aimed to explore and predict intervention use in Dutch autistic children by using demographic and autism-specific characteristics. The majority of children (88.1%) received some type of therapy and approximately half of the children had received medication. As expected, older children reported using more therapies, overall, and more guideline therapies. Boys were less likely to have used a mainstream therapy. Children with a lower IQ were less likely to use a guideline therapy and used a lower number of therapies overall. Children who attend special education used more therapies and were more likely to have used a mainstream therapy and mainstream medication. Parents of children with a co-occurring diagnosis reported using more therapies, and were more likely to have used other therapies and mainstream medication. Higher parental education level decreased the likelihood of mainstream medication use. More sensory issues were related to greater other medication. Against expectations, other autism-specific characteristics did not predict intervention use.
In our study, age was positively related to the total number of therapies used; older children have received more therapies. Older age also increased the likelihood of having received a guideline therapy. The guideline category includes psycho-education (for parents or child) and early intensive interventions, both of which are advised to be (an essential) part of any autism treatment (Fuentes et al., 2021; GGZS, 2020; NICE, 2013; van Rooijen & Rietveld, 2017). This means that all diagnosed children, regardless of their current age or age of diagnosis, should have received a guideline therapy. These findings suggest that guideline therapies might sometimes be used when the child is older. This could depend on the age of diagnosis, which should be taken into account in future research. Early (guideline) therapies are important, and it might be an area of improvement for clinical practitioners to ensure that children receive these therapies as early as possible after their diagnosis.
Previous studies did not provide a clear conclusion about the predictive value of IQ on intervention use. We found that children who had a lower IQ, as reported by parents, used less therapies and less often used guideline therapies. Guideline therapies might be less suited for children with a lower IQ. For example, a review showed that most social skills-groups for autistic children required children to have an IQ above 70 (Reichow et al., 2013). Social skills training is one of the most frequently used therapies (Figure 1). It raises some concerns if such a popular and effective therapy is not suitable for a considerable number of autistic children. This shows a clear point of improvement for practice; all (guideline) therapies should be adapted to suit children with moderate to profound learning difficulties. However, it should be acknowledged that this study did not test the children’s IQ directly but instead relied on parents to report their child’s IQ.
Boys were less likely to have used a mainstream therapy. The most commonly used mainstream therapies include physiotherapy (physical therapy), speech therapy and play therapy. There are no indications in the literature that boys would use these types of therapies less (or girls more). This difference could be related to variation in expression of autism symptoms or co-occurring problems between boys and girls (e.g. Hiller et al., 2014; Ormond et al., 2018). It could also be that parents expect more communication and language skills from girls and are therefore more likely to choose play or speech therapy for them.
Children who attend special education or reported co-occurring diagnoses use more therapies. Attending special education was related to having used more (mainstream) therapies and medication, which might be better suited for additional problems which children who attend special education are likely to have. As expected, children with co-occurring diagnoses more often used mainstream medication or other therapies. Having an additional diagnosis most likely complicates the process of finding suitable interventions as the child might present with multiple main symptoms whereas interventions usually focus on one problem at a time. Medication and other therapies could be a last resort for these children (Mire et al., 2015). It is important that more transdiagnostic interventions (interventions focussed on multiple diagnoses or problems) are developed. These would simplify the intervention choice for children with autism who have additional and thus prevent them from receiving an array of interventions that each only treats part of their symptoms.
While previous studies showed that current medication use increases with age within childhood (Houghton et al., 2017; Mire et al., 2015; Xu et al., 2019), age did not predict medication use in this study. It could be that this trend found in the literature is specific for the autistic population in the United States, where the previous studies were conducted, whereas, this study was conducted in the Netherlands. Perhaps, the trend was not found because attending special education and having a co-occurring diagnosis were controlled for, both of which increase the likelihood of using mainstream medication. It should be acknowledged that the current findings only inform us about whether children used medication and not about whether they used more or less of it when they were older.
Higher parental education level was previously found to predict alternative medication use (Höfer et al., 2017; Patten et al., 2013), and in our study, it predicted lower likelihood of mainstream medication use, but not more other interventions. These findings are problematic, as all children should receive the interventions they need, regardless of their parents’ level of education. When medication is prescribed, it is important that the parents and the child are adequately informed about the short- and long-term pros and cons of the medication. This ensures that the involved clinicians, parents and the child can make a well-considered joint informed decision.
Children with more sensory issues received more other medication. Severe sensory issues can disrupt daily life in home, social and educational settings. Children with more sensory issues might need medication to reduce stress. Parents of these children might be more likely to look beyond mainstream medication to find medication to improve their child’s daily functioning. Interestingly, sensory issues was the only autism-specific characteristic that was predictive of intervention use, none of the other autism-specific characteristics were related to either therapy or medication use. Our findings suggest that intervention use is mostly guided by additional factors (co-occurring diagnoses, special education and lower IQ) and demographic characteristics (age, sex and parental education level). Although autism-specific characteristics are suggested to guide intervention use (Fuentes et al., 2021; GGZS, 2020; van Rooijen & Rietveld, 2017), co-occurring problems may also be a legitimate reason to choose specific interventions. However, demographic factors and IQ levels should not refrain autistic children from receiving appropriate care. Interventions might have to be adapted to suit all demographic groups, as they should be available and accessible for children of all ages, sexes and levels of intelligence, and with all levels of parental education.
Limitations
When interpreting the results from this study, various points should be considered. First, the three categories of interventions (guideline, mainstream and other) are very broad and include very diverse therapies. However, these categories are not exhaustive, and some types of guidance and support were not included. Second, the sample that was used for this study is a convenience sample and as participation is voluntary, self-selection bias could be present. Participants of the NAR are relatively highly educated. Third, there was a lot of missing data for the autism-specific predictors, reducing the power to detect possible effects of these characteristics. Fourth, alternative social skills measures could have been used, as the SDQ is only a brief behavioural screening questionnaire. These limitations may have contributed to the current findings and affect their generalisability.
Other factors – not included in this study, such as the availability of interventions, recommendations from others and the emergence of new innovative interventions – can also affect intervention use. Therefore, more research is needed to clarify the reasons behind intervention choices. Future research should further investigate how different co-occurring diagnoses (e.g. ADHD or anxiety) or problems (e.g. internalising problems vs externalising problems) could affect intervention use, and subscales of sensory issues may elucidate the relation between sensory issues and therapy and medication use.
Conclusion
By combining demographic and autism-specific predictors, we were able to conclude that intervention use is mostly related to IQ, special education attendance and the presence of co-occurring diagnoses but also to age, sex and parental education level. Autism-specific child characteristics do not influence intervention use, except for an increased chance of using other medication among children with more sensory issues. This study was the first of its kind focusing on Dutch families and draws attention to possible shortcomings of current autism interventions. Nearly a third of the participants reported using other interventions including alternative interventions that can be harmful (Jonkman et al., 2022). Guideline interventions should be available and accessible for children of all ages, sex and with all levels of intelligence. Transdiagnostic interventions could be beneficial for autistic children who have additional problems. Furthermore, parents should be accurately informed about medication to ensure that the use of mainstream medication does not depend on parental level of education. Overall, intervention use seems to be guided more by co-occurring problems rather than by autism-specific characteristics.
Footnotes
Therapies included in the NAR questionnaire.
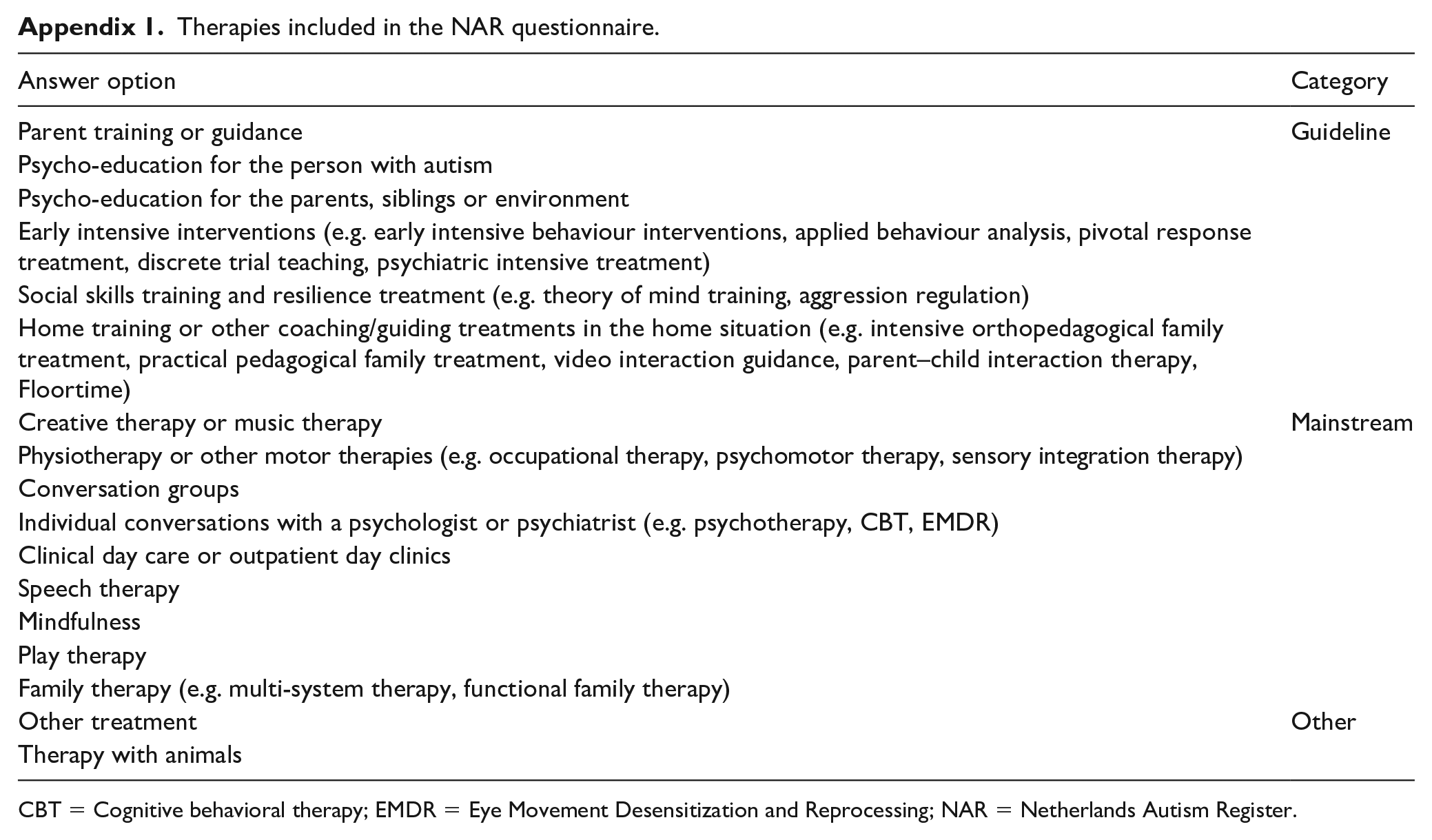
| Answer option | Category |
|---|---|
| Parent training or guidance | Guideline |
| Psycho-education for the person with autism | |
| Psycho-education for the parents, siblings or environment | |
| Early intensive interventions (e.g. early intensive behaviour interventions, applied behaviour analysis, pivotal response treatment, discrete trial teaching, psychiatric intensive treatment) | |
| Social skills training and resilience treatment (e.g. theory of mind training, aggression regulation) | |
| Home training or other coaching/guiding treatments in the home situation (e.g. intensive orthopedagogical family treatment, practical pedagogical family treatment, video interaction guidance, parent–child interaction therapy, Floortime) | |
| Creative therapy or music therapy | Mainstream |
| Physiotherapy or other motor therapies (e.g. occupational therapy, psychomotor therapy, sensory integration therapy) | |
| Conversation groups | |
| Individual conversations with a psychologist or psychiatrist (e.g. psychotherapy, CBT, EMDR) | |
| Clinical day care or outpatient day clinics | |
| Speech therapy | |
| Mindfulness | |
| Play therapy | |
| Family therapy (e.g. multi-system therapy, functional family therapy) | |
| Other treatment | Other |
| Therapy with animals |
CBT = Cognitive behavioral therapy; EMDR = Eye Movement Desensitization and Reprocessing; NAR = Netherlands Autism Register.
Medications included in the NAR questionnaire.
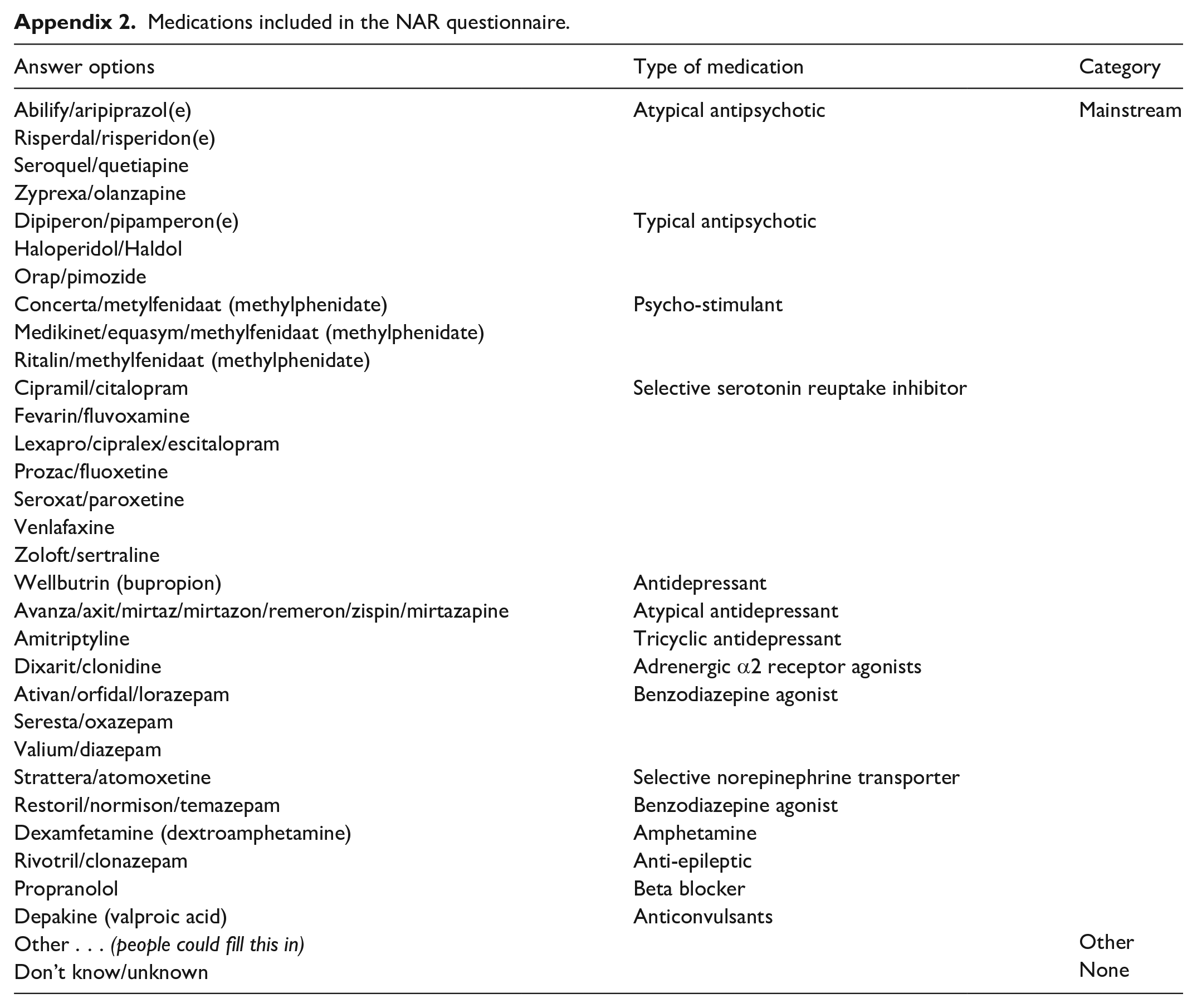
| Answer options | Type of medication | Category |
|---|---|---|
| Abilify/aripiprazol(e) | Atypical antipsychotic | Mainstream |
| Risperdal/risperidon(e) | ||
| Seroquel/quetiapine | ||
| Zyprexa/olanzapine | ||
| Dipiperon/pipamperon(e) | Typical antipsychotic | |
| Haloperidol/Haldol | ||
| Orap/pimozide | ||
| Concerta/metylfenidaat (methylphenidate) | Psycho-stimulant | |
| Medikinet/equasym/methylfenidaat (methylphenidate) | ||
| Ritalin/methylfenidaat (methylphenidate) | ||
| Cipramil/citalopram | Selective serotonin reuptake inhibitor | |
| Fevarin/fluvoxamine | ||
| Lexapro/cipralex/escitalopram | ||
| Prozac/fluoxetine | ||
| Seroxat/paroxetine | ||
| Venlafaxine | ||
| Zoloft/sertraline | ||
| Wellbutrin (bupropion) | Antidepressant | |
| Avanza/axit/mirtaz/mirtazon/remeron/zispin/mirtazapine | Atypical antidepressant | |
| Amitriptyline | Tricyclic antidepressant | |
| Dixarit/clonidine | Adrenergic α2 receptor agonists | |
| Ativan/orfidal/lorazepam | Benzodiazepine agonist | |
| Seresta/oxazepam | ||
| Valium/diazepam | ||
| Strattera/atomoxetine | Selective norepinephrine transporter | |
| Restoril/normison/temazepam | Benzodiazepine agonist | |
| Dexamfetamine (dextroamphetamine) | Amphetamine | |
| Rivotril/clonazepam | Anti-epileptic | |
| Propranolol | Beta blocker | |
| Depakine (valproic acid) | Anticonvulsants | |
| Other . . . (people could fill this in) | Other | |
| Don’t know/unknown | None |
Appendix 3
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a ZonMW Research grant (The Netherlands; grant no. 636340005) and by the Senior Research Advancement Fund/Research Development Allowance, School of Law, Social and Behavioural Sciences, Faculty of Business and Social Sciences, Kingston University, UK.