
Abstract
Low breastfeeding rates are driven by multiple bio-psycho-social factors. Experience of breastfeeding is known to differ by maternal demographic factors (age, education and ethnicity) but there is less recognition of factors such as neurodivergence. This review, prospectively registered with PROSPERO (registration number: CRD42021271465), systematically identified qualitative research, commentaries and personal accounts related to Autistic mothers and infant feeding. Database searching identified 1225 records, with thematic synthesis undertaken on 22 (eight peer-reviewed studies and 14 grey literature) pieces. Our analysis identified that maternity and infant feeding services were built on a lack of understanding of Autistic needs, and were often inaccessible at a time when Autistic mothers already felt a loss of control and lack of social support. Specifically relating to breastfeeding, knowledge and determination were often high, and a minority of mothers reported positive breastfeeding experiences. However, sensory challenges, pain and interoceptive differences (exacerbated by a lack of support) made breastfeeding impossible for some. Infant formula was viewed as second-best to breastmilk, but a minority of mothers found the ritual of preparing bottles of formula positive. There is an urgent need for maternity and infant feeding services to accommodate the needs of Autistic mothers, including service design and staff training.
Lay abstract
What is already known about the topic?
Mothers are encouraged to breastfeed their babies due to known health benefits for both babies and mothers. However, although breastfeeding is ‘natural’, that does not make it easy and many women experience challenges. Autistic women may face additional barriers to breastfeeding when compared to neurotypical women.
What this paper adds?
We reviewed all existing evidence on Autistic mothers’ infant feeding experiences (22 pieces) and found that although many Autistic women wanted to breastfeed, breastfeeding was difficult for Autistic mothers for three key reasons. First, maternity and infant feeding services were inaccessible and unsupportive to Autistic mothers, meaning they did not receive help when needed. Second, becoming a mother was challenging because of exhaustion, loss of control over routines and a lack of social support. Third, when breastfeeding Autistic mothers experienced sensory challenges, such as ‘being touched out’, and pain, which could feel unbearable. Despite these difficulties, many Autistic mothers had done a lot of reading about breastfeeding and were determined to breastfeed their babies; some mothers found breastfeeding positive. Infant formula was often viewed as second-best compared to breastmilk, but some mothers found the ritual of preparing bottles of formula to be calming.
Implications for practice, research or policy
The findings of this work show that Autistic mothers urgently need better support from health professionals to help meet their breastfeeding goals, including how to remove or reduce the extra barriers being Autistic brings to breastfeeding.
Background
Around 1%−2% of the population are Autistic, and diagnosis in adulthood is common for ‘the lost generation’ of Autistic women (Lai & Baron-Cohen, 2015), with almost a quarter of mothers of Autistic children identified as having Autistic traits (Pruitt et al., 2016). Regardless of autism being a lifelong neurotype, the majority of autism research is focused on children (Nicolaidis et al., 2019), with little research on the lived realities of Autistic adults (Taylor & DaWalt, 2020), including experiences of motherhood. Recent comparative work highlighted that Autistic mothers were more likely than non-Autistic peers to feel stigmatised and misunderstood by health professionals, experience selective mutism, and not know which details were important to share with health professionals or how to seek advice (Pohl et al., 2020). These behaviours can lead to ‘masking’ (suppression of natural Autistic coping responses), to reduce negative outcomes (Pearson & Rose, 2021). Pregnancy and birth can also lead to additional sensory processing challenges for Autistic mothers (Samuel et al., 2022).
Breastfeeding protects infant and maternal health and reduces healthcare costs (Renfrew, McCormick, et al., 2012). However, although in the United Kingdom over 80% of women begin breastfeeding their babies, rates reduce quickly and only 1% of women breastfeed exclusively for 6 months (Health & Social Care Information Centre, 2012) as recommended by the World Health Organisation (World Health Organization, 2017). Understanding barriers to breastfeeding is important. However, there is little understanding of the needs of Autistic women despite limited evidence that they may find breastfeeding more challenging. In a small-scale survey, 64% of 306 Autistic women reported difficulty breastfeeding their first child compared to 58% of 118 non-Autistic women (Pohl et al., 2020).
Several aspects of breastfeeding may be more challenging for Autistic women. Breastfeeding is a highly embodied and sensory experience, requiring significant work on the part of mothers (Shaw, 2004). Processing sensations has been highlighted as one of the main challenges for Autistic mothers (Gardner et al., 2016), increasing risk of breastfeeding aversion – a ‘visceral and overwhelming’ sensation to get the baby away from the breast (Morns et al., 2020). In addition, best practice to promote responsive feeding in relation to infant cues, may feel unpredictable and stressful (Grant, 2015). It has been recommended that clinicians tailor information directed to Autistic mothers, taking account of their individual sensory processing challenges (Gardner et al., 2016; Pohl et al., 2020). Therefore, we conducted a systematic review and qualitative thematic synthesis to gain greater understandings of Autistic experiences of breastfeeding.
Methodology
A systematic review was undertaken following guidance within the Preferred Reporting Guidelines for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021), with the protocol prospectively registered with PROSPERO (registration ID: CRD42021271465).
Aim: To undertake a qualitative systematic review exploring Autistic women’s experiences of infant feeding using thematic synthesis.
Community involvement and reflexivity
Aimee, Kathryn and Jennifer are Autistic. Kathyrn is a director of Autistic UK, an organisation led by Autistic people for Autistic people. In addition, Aimee sought feedback on the design of the research from Autistic women who were members of an online infant feeding support group ahead of applying for funding for this project. Members of the support group also contributed grey literature to the review. Three of the researchers had lived experience of infant feeding (Kathryn, Jennifer and Amy), Sara is a registered nurse and health visitor with experience supporting families with infant feeding and Jennifer ran perinatal support groups for 5 years. Aimee, Sara and Amy are infant feeding researchers.
Search
Search terms to be included in the review were identified by hand searching keywords of relevant articles. The search strategy, developed with the support of a specialist librarian, involved two main terms, relating to (1) Autistic women and (2) infant feeding:
TX (infant feed* OR breastfeed* OR breast feed* OR breastfed* OR breast fed* OR formula feed* OR formula fed* OR chest feed* OR tube feed* OR express* OR pump* OR Human milk OR mothers milk OR lactation)
AND
TX (Autistic women OR Autistic mother OR Autism in women OR Women with Autism OR Asperger* in women OR women with Asperger* OR neurodivergent woman OR neurodivergent mother OR neurodiverse women or neurodiverse mother)
Following publication of our protocol on the PROSPERO website, we searched five electronic databases to reflect the range of academic disciplines contributing to evidence in this area (Medline via OVID, PsychINFO via Ebscohost, CINAHL via Ebscohost, Web of Science via Clarivate and EThOS via the British Library). Databases were searched from 2000 to August 2021, and limited to humans. Evidence reviews identified in database searching were unpicked. We also received grey literature from our community contacts and hand searched using Google for additional content. All articles included in the review were subjected to forward and backward chaining.
Study selection and eligibility criteria
We included qualitative studies, commentaries and personal accounts focused on experiences and views of Autistic mothers in relation to infant feeding. Studies were assessed against inclusion and exclusion criteria.
Inclusion criteria
Population:
○ Autistic women and mothers (including adoptive and non-biological mothers, trans men and non-binary birthing people), and anybody who supports them with infant feeding.
Phenomenon:
○ Views and experiences of infant feeding (including formula, expressed breastmilk, breastfeeding and the use of donor human milk).
Exclusion criteria
Studies that did not focus on preferences, attitudes and experiences of Autistic women and infant feeding;
Not a qualitative study (i.e. not based on open text survey responses or a qualitative method) or report of personal experience by an Autistic woman;
Full text does not exist;
Full text not available in English language.
Quality assessment and data extraction
All studies and grey literature were included in the thematic synthesis. Data extraction was undertaken by Sara and Aimee comprising demographic characteristics of participants, methodological information, study characteristics that would impact on the findings, data quality and space for all findings relating to the review’s focus. In addition, the eight peer reviewed research studies were independently assessed by two authors (Aimee and Jennifer) against the CASP qualitative checklist (Critical Appraisal Skills Programme, 2018). Inter-rater reliability was 91.25%, with a Cohens Kappa (IBM SPSS Statistics V28) of K = 0.633 (95% CI, 0.371 to 0.895), p < 0.001. Disagreements were discussed and resolved.
Qualitative synthesis: thematic synthesis
We followed the Thomas and Harden (2008) thematic synthesis procedure: coding text, development of descriptive themes and analytical theme generation. Two researchers, one Autistic (Aimee) and the other neurotypical (Sara), with different disciplinary backgrounds (sociology/public health nursing) individually coded six of the included sources, three peer reviewed articles and three pieces of grey literature. We then met to discuss the codes individually created, which showed a high level of overlap but some different terminology and organisation. Following this, themes were discussed with the wider project team, before a final coding frame was developed and each study document (structured summary and qualitative findings) was added to NVivo R1 to allow for coding by Aimee. Each sentence of data related to infant feeding received at least one code (line-by-line coding), to reduce bias during analysis. Where new codes were identified during the analysis, previously coded studies were reviewed and recoded where necessary.
Two data analysis meetings were held during 2021 between the authors to refine the development of descriptive themes, enabling the translation of concepts between articles to emerge. One new article was added to the analysis between meetings one and two (Wilson & Andrassy, 2022). To promote analytical theme generation within a multi-disciplinary team, a summary of themes document was created by Aimee, and each researcher independently inferred barriers and facilitators to breastfeeding for Autistic women from these themes. Final themes were discussed and agreed by all researchers.
Results
Studies identified
Database searching identified 1225 records, 11 of which were fully screened against the inclusion criteria, with four included. Throughout the reporting of the thematic synthesis, sources are referred to by number based on the alphabetical order of items identified in Table 3. One dissertation was under embargo (Hampton, 2020), but a peer-reviewed article based on aspects of the thesis published after the searches, was included [10]. Online searching and personal communication identified 14 pieces of grey literature containing the firsthand accounts of Autistic women with experience of infant feeding. One additional newly published peer-reviewed article was identified following the first stage of the thematic synthesis [22]. Two additional peer reviewed articles were identified by forward and backward chaining and unpicking systematic reviews. The PRISMA flow diagram in Figure 1 illustrates this process (Page et al., 2021).
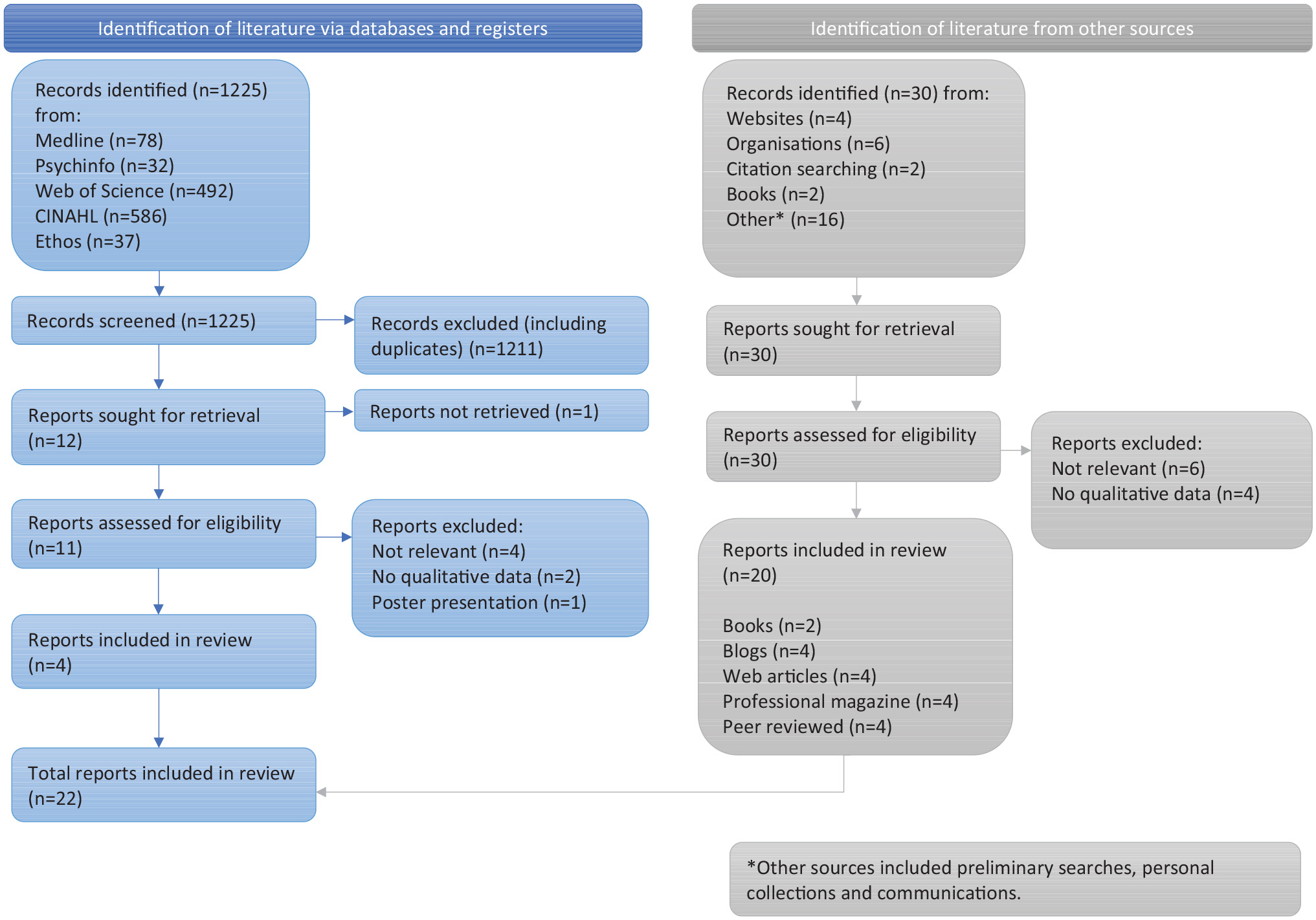
PRISMA flow diagram.
Included sources
Our sources included peer-reviewed research articles (n = 8) and other firsthand accounts (n = 14). We have produced two tables to outline the methods in research studies (Table 1) and the personal characteristics in firsthand accounts (Table 2). Studies and grey literature originated primarily from the United States, United Kingdom and Australia, and included data from 324 mothers and commentaries from 11 mothers; no data were identified by authors as originated from Autistic birthing parents of minority genders (e.g. trans men, non-binary people and so on).
Characteristics of research.
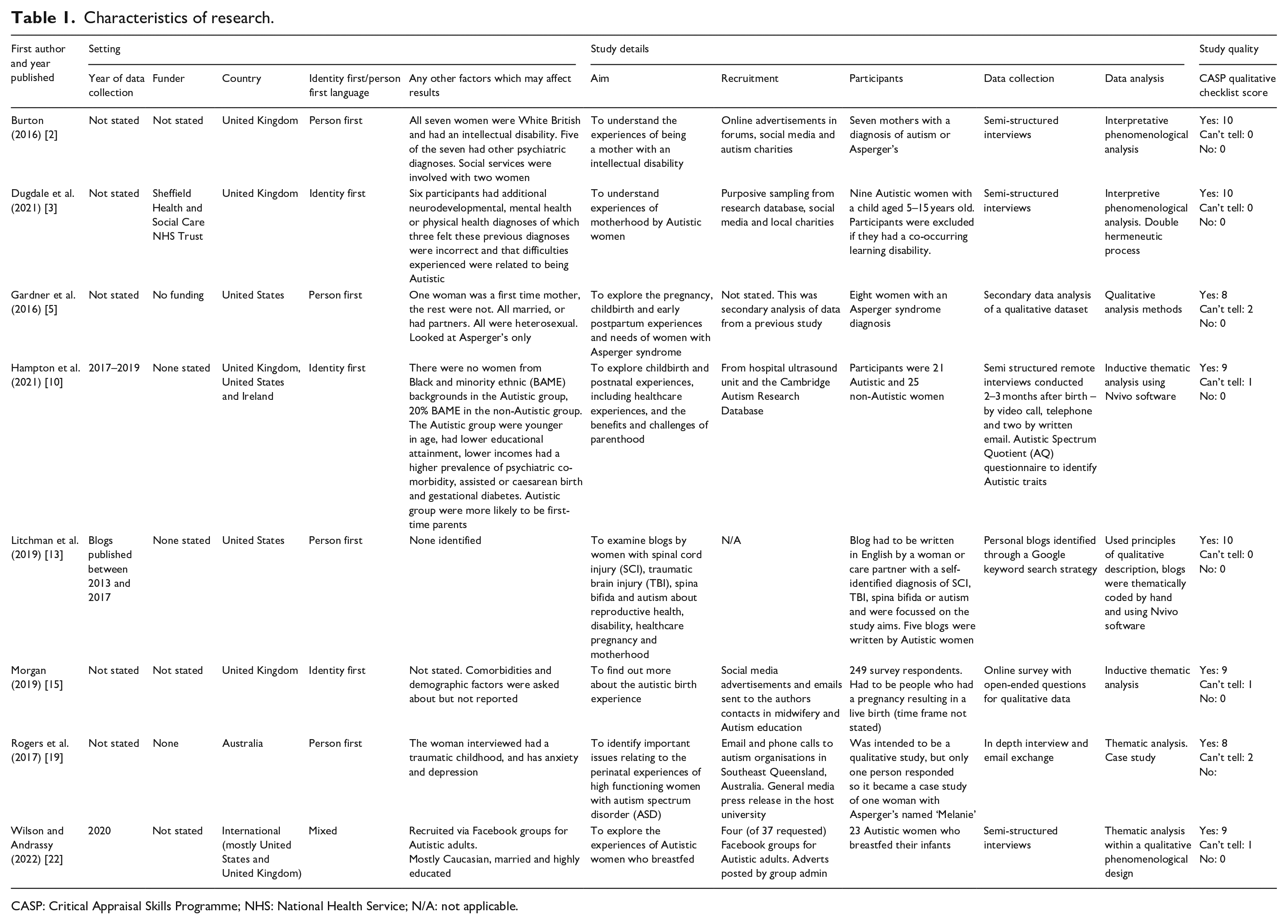
CASP: Critical Appraisal Skills Programme; NHS: National Health Service; N/A: not applicable.
Characteristics of grey literature and commentaries.
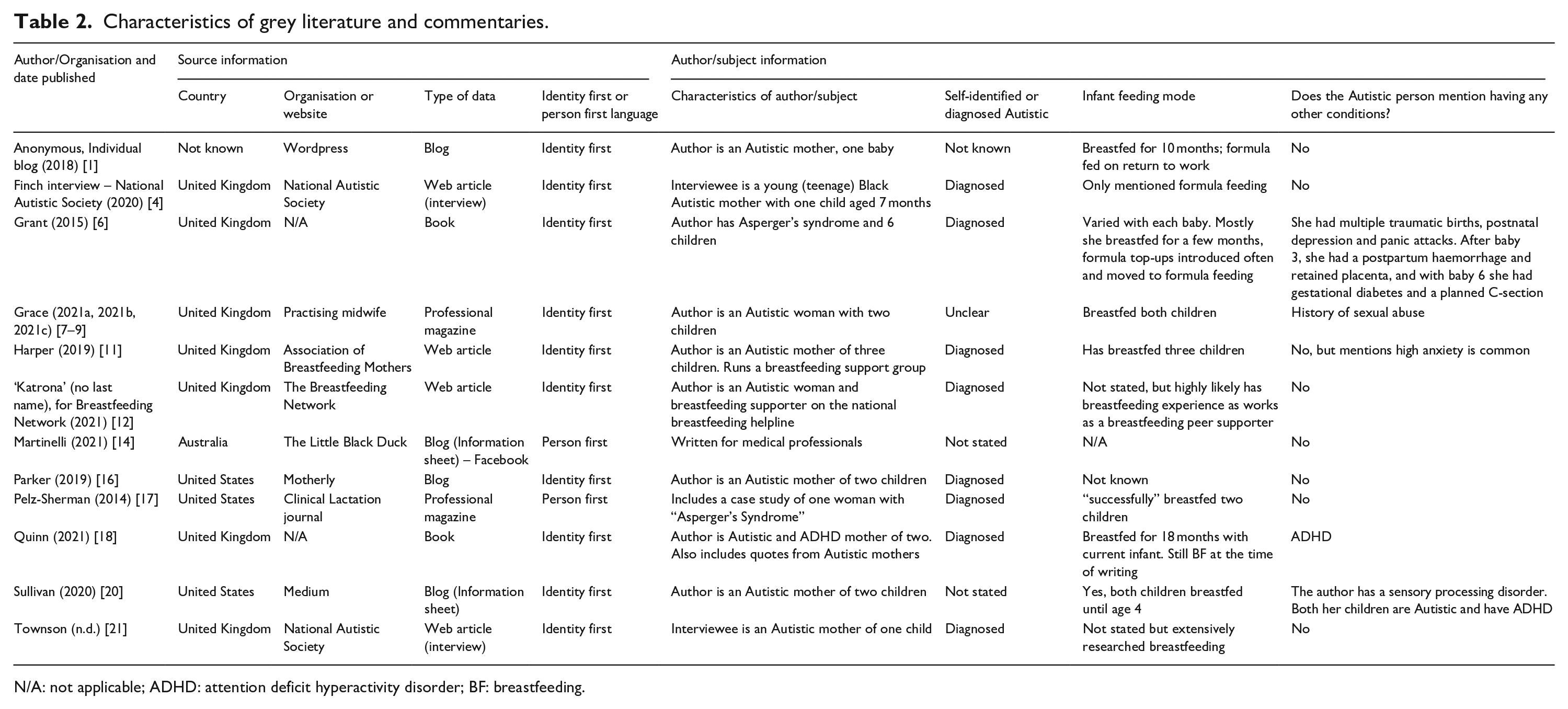
N/A: not applicable; ADHD: attention deficit hyperactivity disorder; BF: breastfeeding.
Thematic synthesis
We situate our thematic synthesis within two important social contexts. First, the societal stigma of Autistic people, including the invisibility of Autistic women in general and Autistic mothers in particular. Second, we identify that societal stigma and invisibility of Autistic women continues to be a factor within healthcare, with diagnosis in adulthood common; several mothers from the included studies and commentaries were diagnosed after the birth of their child(ren) [6, 13, 16]. Our findings are reported in relation to: maternity and infant feeding services, becoming a parent and infant feeding and are summarised in Table 3. We provide a model of barriers and facilitators to breastfeeding for Autistic women (see Figure 2).
Summary of thematic findings.
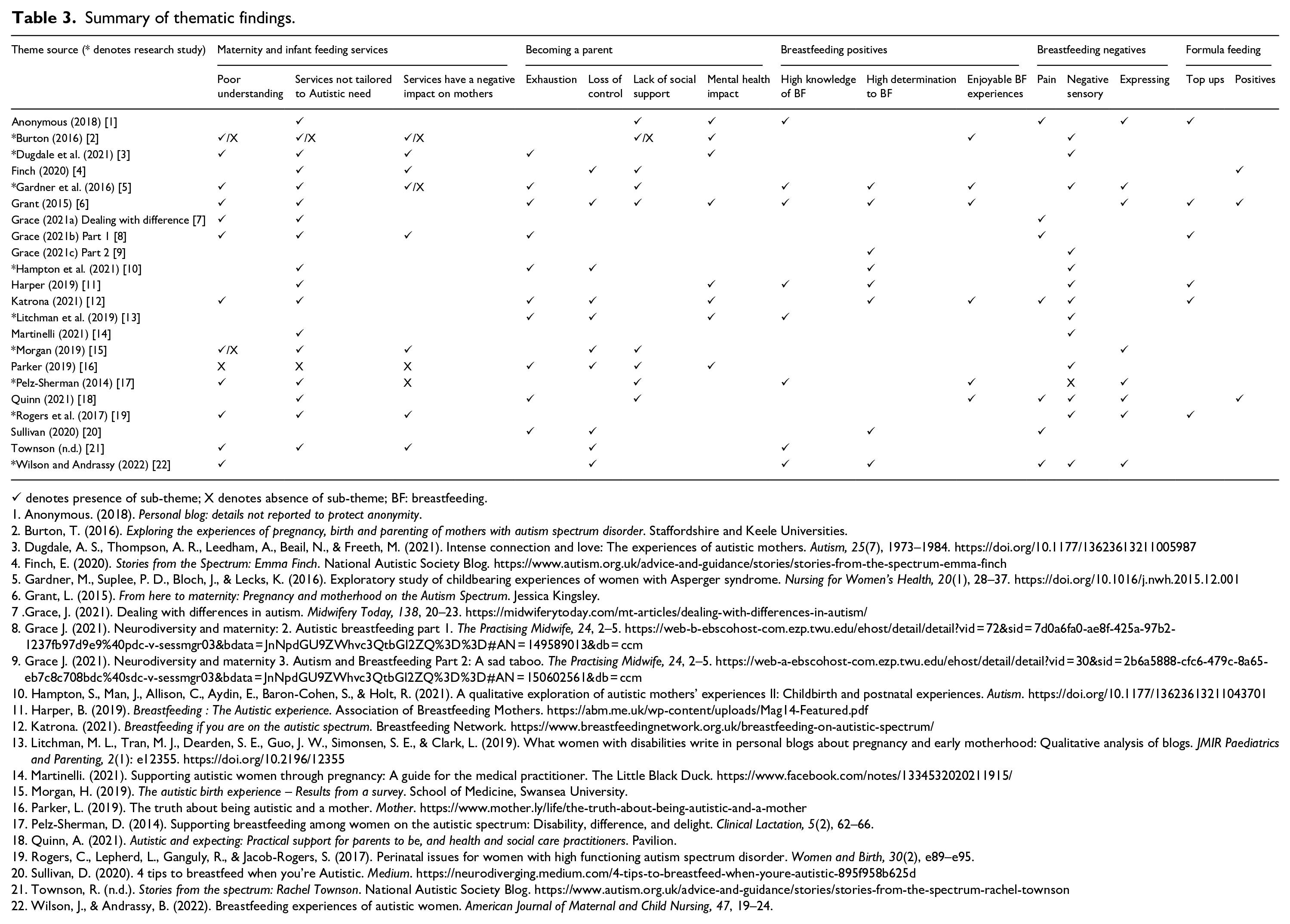
✓ denotes presence of sub-theme; X denotes absence of sub-theme; BF: breastfeeding.
Anonymous. (2018). Personal blog: details not reported to protect anonymity.
Burton, T. (2016). Exploring the experiences of pregnancy, birth and parenting of mothers with autism spectrum disorder. Staffordshire and Keele Universities.
Dugdale, A. S., Thompson, A. R., Leedham, A., Beail, N., & Freeth, M. (2021). Intense connection and love: The experiences of autistic mothers. Autism, 25(7), 1973–1984. https://doi.org/10.1177/13623613211005987
Finch, E. (2020). Stories from the Spectrum: Emma Finch. National Autistic Society Blog. https://www.autism.org.uk/advice-and-guidance/stories/stories-from-the-spectrum-emma-finch
Gardner, M., Suplee, P. D., Bloch, J., & Lecks, K. (2016). Exploratory study of childbearing experiences of women with Asperger syndrome. Nursing for Women’s Health, 20(1), 28–37. https://doi.org/10.1016/j.nwh.2015.12.001
Grant, L. (2015). From here to maternity: Pregnancy and motherhood on the Autism Spectrum. Jessica Kingsley.
Grace, J. (2021). Dealing with differences in autism. Midwifery Today, 138, 20–23. https://midwiferytoday.com/mt-articles/dealing-with-differences-in-autism/
Grace J. (2021). Neurodiversity and maternity: 2. Autistic breastfeeding part 1. The Practising Midwife, 24, 2–5. https://web-b-ebscohost-com.ezp.twu.edu/ehost/detail/detail?vid=72&sid=7d0a6fa0-ae8f-425a-97b2-1237fb97d9e9%40pdc-v-sessmgr03&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3D%3D#AN=149589013&db=ccm
Grace J. (2021). Neurodiversity and maternity 3. Autism and Breastfeeding Part 2: A sad taboo. The Practising Midwife, 24, 2–5. https://web-a-ebscohost-com.ezp.twu.edu/ehost/detail/detail?vid=30&sid=2b6a5888-cfc6-479c-8a65-eb7c8c708bdc%40sdc-v-sessmgr03&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3D%3D#AN=150602561&db=ccm
Hampton, S., Man, J., Allison, C., Aydin, E., Baron-Cohen, S., & Holt, R. (2021). A qualitative exploration of autistic mothers’ experiences II: Childbirth and postnatal experiences. Autism. https://doi.org/10.1177/13623613211043701
Harper, B. (2019). Breastfeeding: The Autistic experience. Association of Breastfeeding Mothers. https://abm.me.uk/wp-content/uploads/Mag14-Featured.pdf
Katrona. (2021). Breastfeeding if you are on the autistic spectrum. Breastfeeding Network. https://www.breastfeedingnetwork.org.uk/breastfeeding-on-autistic-spectrum/
Litchman, M. L., Tran, M. J., Dearden, S. E., Guo, J. W., Simonsen, S. E., & Clark, L. (2019). What women with disabilities write in personal blogs about pregnancy and early motherhood: Qualitative analysis of blogs. JMIR Paediatrics and Parenting, 2(1): e12355. https://doi.org/10.2196/12355
Martinelli. (2021). Supporting autistic women through pregnancy: A guide for the medical practitioner. The Little Black Duck. https://www.facebook.com/notes/1334532020211915/
Morgan, H. (2019). The autistic birth experience – Results from a survey. School of Medicine, Swansea University.
Parker, L. (2019). The truth about being autistic and a mother. Mother. https://www.mother.ly/life/the-truth-about-being-autistic-and-a-mother
Pelz-Sherman, D. (2014). Supporting breastfeeding among women on the autistic spectrum: Disability, difference, and delight. Clinical Lactation, 5(2), 62–66.
Quinn, A. (2021). Autistic and expecting: Practical support for parents to be, and health and social care practitioners. Pavilion.
Rogers, C., Lepherd, L., Ganguly, R., & Jacob-Rogers, S. (2017). Perinatal issues for women with high functioning autism spectrum disorder. Women and Birth, 30(2), e89–e95.
Sullivan, D. (2020). 4 tips to breastfeed when you’re Autistic. Medium. https://neurodiverging.medium.com/4-tips-to-breastfeed-when-youre-autistic-895f958b625d
Townson, R. (n.d.). Stories from the spectrum: Rachel Townson. National Autistic Society Blog. https://www.autism.org.uk/advice-and-guidance/stories/stories-from-the-spectrum-rachel-townson
Wilson, J., & Andrassy, B. (2022). Breastfeeding experiences of autistic women. American Journal of Maternal and Child Nursing, 47, 19–24.
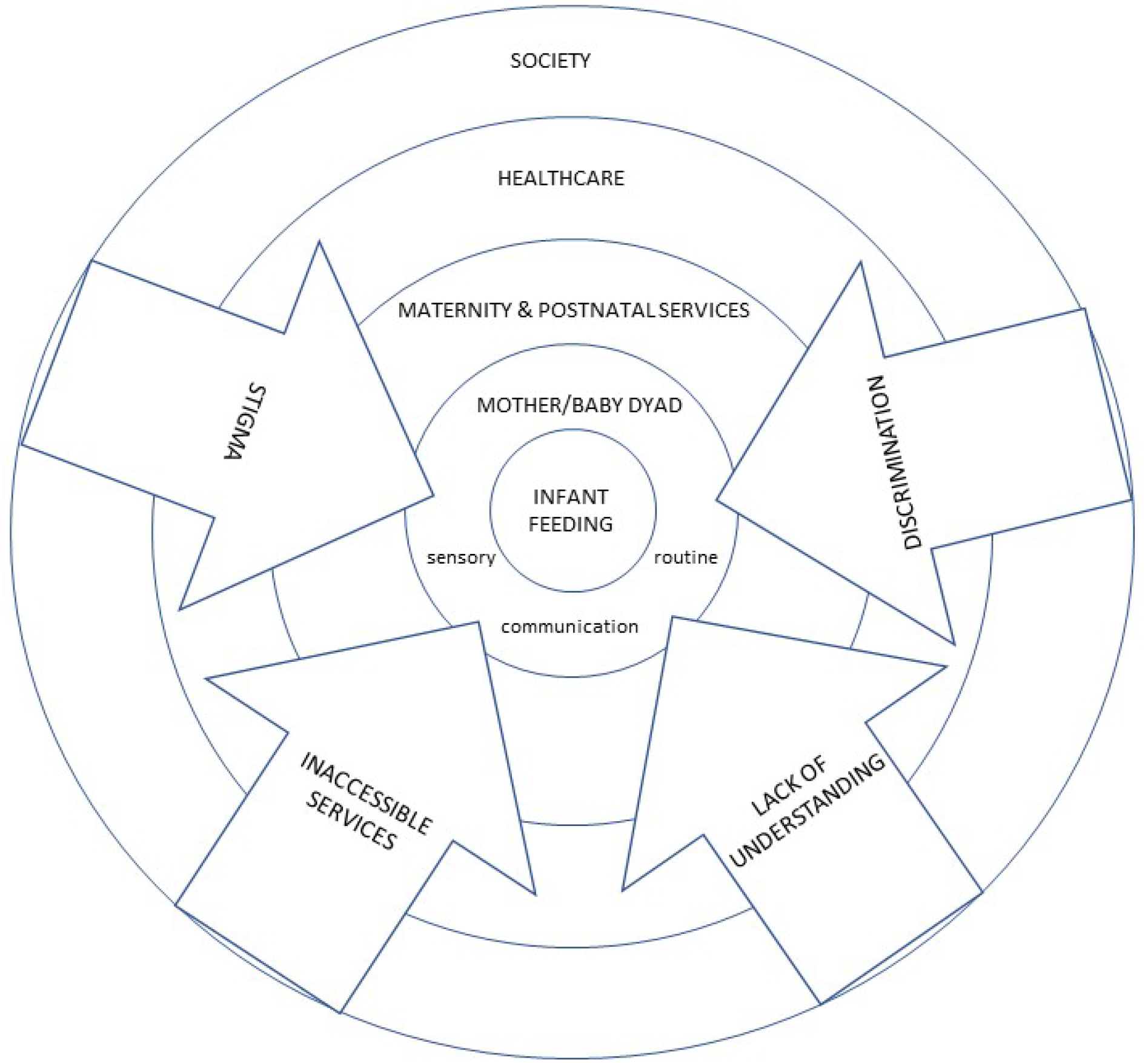
Model of barriers and facilitators to autistic mothers breastfeeding.
Maternity and infant feeding services
Data reported on both general maternity care and forms of care were infant feeding specific, which were sometimes provided by maternity services. We report on both types of care together, as mothers described maternity care experiences when discussing their infant feeding.
Low understanding of autism and lack of acceptance of Autistic needs
Although occasional reports identified clinicians who positively supported Autistic women [2, 15, 16], it was strongly reported that the majority of clinicians did not understand the lived reality of being Autistic. This included a lack of awareness of sensory differences [2, 5, 7, 12, 15, 19], differences in experiencing and reporting pain [7, 8, 12, 19] and communication differences [8, 15, 21].
Services are not tailored towards Autistic needs
Experiences of maternity services were described almost entirely negatively. At its most extreme, Autistic mothers reported interactions that felt dehumanising [2, 19] with examples of bullying by staff [19] and a more general feeling of being ‘told off’ [6, 19] or not listened to [3, 15, 18]. Autistic sensory needs around touch were not always respected. Health professionals sat too close to women [5], touched them without asking [2, 6, 15, 22] and caused pain during examinations [19]. Services did not provide clarity around care pathways or facilitate control over experiences for Autistic patients [11], with policies followed ahead of respecting individual needs [2], lack of continuity of care requiring the need to repeatedly educate staff [21] and a lack of clarity regarding what would happen at appointments [21]. Home visits were not restricted to defined times, causing anxiety [6, 10].
One major way in which services were inappropriate for Autistic mothers was using neurotypical communication. This meant that misunderstandings occurred between the health professional’s spoken words and the Autistic woman’s understanding of them [3, 6, 12, 21]. Furthermore, vague questions from clinician, such as ‘how are you?’, were not understood by Autistic patients to be part of the clinical encounter, with opportunities for support missed [7]. Written information was described in one source as being all-or-nothing, which was overwhelming when too much, and anxiety producing when too little [21]. Two sources reported that partners, who were essential in facilitating communication during times of stress, were sent away from the hospital [1, 2].
The period immediately following birth when most of the women were in hospital trying to establish breastfeeding, was described as difficult in relation to understanding social norms, staff facial expressions [1], and the sensory environment [1, 3, 7]. Inconsistent breastfeeding advice received from health professionals was experienced as frustrating and upsetting [6, 10]. Community infant feeding support was identified as inaccessible, with telephone support viewed negatively [7, 8, 11]. One mother reported receiving good breastfeeding support in a German hospital in the immediate postnatal period [8]. Instances of incorrect advice, giving babies formula within the postnatal hospital period without asking mothers [6] and strongly pushing formula top-ups on mothers [6, 19] were reported. One woman reported being refused formula feeding support [15].
Alongside health services, voluntary sector and grass roots organisations provided support services to pregnant women and mothers. These were described as inaccessible due to the need to navigate social norms within group support [7, 8, 10, 11, 17]. One Autistic mother set up her own breastfeeding peer support group to overcome the deficit in her local services [11]. By contrast, support which could be accessed one-to-one outside of the group setting, or through well-designed written materials, was described as valuable [17].
Autistic mothers’ views of maternity services
Autistic mothers reported multiple ways that maternity care service interactions negatively affected them. First, Autistic mothers felt they were not heard or believed by health professionals [3, 5, 15, 22], and felt that they were perceived as aloof [5]. Autistic women also felt judged [15], reluctant to disclose their diagnosis [15], feared their babies being taken into social care [15, 19] and felt that they had to mask their autism [8]. Unsurprisingly, in this context, women found it difficult to assert their needs [2, 19] and dreaded appointments [19, 21] with one woman reporting trying to disengage with services [19]. Two mothers reported that they tried not to mask with maternity staff [4, 5].
Becoming a parent
The transition to becoming a parent was mostly described through a series of challenges, intertwined with infant feeding experiences, which in combination with inaccessible healthcare had an impact on the mothers’ mental health. Some mothers identified significant mental ill-health[1, 12]. This had an impact on the feelings of competence as a mother for some [15].
Exhaustion
The early weeks and months of parenting were described as challenging for Autistic mothers because of the exhaustion of being a new mother. This was specifically related to a lack of sleep [3, 6, 10, 12, 16], although one woman used co-sleeping with an infant as a solution [6]. Babies could also be a source of sensory overwhelm [16, 20], and some mothers felt anxious about not being able to understand and respond to their babies’ cues [5, 8, 10, 13, 18].
Control and routines
One challenge of parenthood was in the disruption of routines, which were necessary to prevent overwhelm. This related to babies’ changing and unpredictable needs [4, 10, 12, 13, 16]; and lack of time to decompress [13, 16]. Some mothers attempted to introduce routines into their parenting, relating to sleep [10], expressing breastmilk [15], feeding babies on a schedule [20] and making up bottles of infant formula [4, 6].
Social support
No mother reported feeling well supported. Formal support was rarely present, but when it was, it was not tailored to Autistic needs, resulting in anxiety and misunderstandings [4–6]. Family and friends who were not sensitive to Autistic needs were an additional source of disruption for some, which drained their energy [1, 2, 15]. Others felt negatively judged in public [15, 17, 18]. Some reported feeling unable to make friends with other mothers [15, 16] and feeling isolated and lonely [15].
Breastfeeding
Knowledge [1, 5, 6, 11, 13, 21–22] and determination to breastfeed [5, 6, 10–12, 20, 22] was often high, sometimes linked to external pressure [9]. It was suggested, however, that it could be difficult for Autistic mothers to translate knowledge into practical skills [5, 22]. A small number of women reported positive experiences of breastfeeding [17], including the ease of calming an upset baby [12, 18], breastmilk always being safe for baby [12], supporting bonding [2, 5, 6, 12, 18], providing a reason to rest [18] and increasing positive maternal identity [12].
However, many women found breastfeeding difficult for multiple reasons. Pain, sometimes severe [8, 22], could be related to latch [1, 7–8, 18, 22] and baby’s behaviour including biting [20]. Hypersensitivity to touch could result in pain [22], and the advice that breastfeeding should not hurt if done correctly distressed two women who were hypersensitive to touch [11, 19]. Interoceptive differences could also mean that women did not experience sensations such as pain or engorgement in the same way that neurotypical mothers would [8, 12, 18]. Similarly, breastfeeding could introduce new unpleasant sensory sensations, including the overwhelming sensation of the baby’s body touching the mothers’ body (known as ‘touched out’) [5, 12, 16, 18, 22]; feelings associated with the baby’s latching [5, 9–11, 16, 18, 22], sucking [22] and milk let-down reflex [18, 22]. The unpleasant sensory sensations were worse for those who had been victims of sexual assault [9].
One mother reported her partner holding the baby while she nursed to reduce physical contact [22]. Using products, such as a tolerable type of nipple pads and nipple shields that suited sensory needs was important to continue breastfeeding for some [1, 18, 22]. Reducing other sensory stimuli [22] or distraction could also help [9, 22]. Setting short-term goals, and knowing that things would get better after around 6 weeks was helpful for some women [1, 18]. Some mothers expressed their breastmilk [1, 5, 6, 15, 17–19, 22], because their baby was in the NICU [5] and also on the advice of health professionals [6, 17, 19]; this was described as unbearable by one mother [22].
Formula feeding
Mothers in nine sources reported formula feeding. Formula feeding was often positioned as second choice [11], if breastfed babies were losing weight and health professionals recommended formula ‘top ups’ [6, 8, 11, 12, 19] once breastfeeding had ‘failed’[6] or the mother had returned to work [1]. Although it was emphasised that formula feeding was safe and should be used when breastfeeding negatively affected mothers’ mental health [18, 20]. The ritual of formula feeding was identified as beneficial [4, 6], allowing mothers more rest while somebody else fed the baby [18]. However, it could also be a source of anxiety, relating to safely preparing formula [12] and seeing how much milk babies had drunk [6].
Discussion
Our systematic review, based on the experiences of over 300 Autistic mothers, identified the inaccessibility of infant feeding support services, challenges associated with the transition to motherhood, and specific challenges linked to infant feeding. Although some of these issues are common experiences of many mothers navigating maternity care and infant feeding (Renfrew, McCormick, et al., 2012), our findings suggest that these issues are likely to be exacerbated for Autistic mothers. Furthermore, specific challenges related to autism were also identified, including changes in routines, loss of control, sensory processing, interoception and pain experiences. Overall, our review identified the importance of adapting services to better support Autistic women with infant feeding.
The methodological quality of sources relating to Autistic experiences of infant feeding
Overall, there was limited peer-reviewed evidence, with only eight articles included accounting for over 300 participants. One article (Wilson & Andrassy, 2022) focused exclusively on infant feeding experiences; the remaining articles contained varying amounts of infant feeding content. Demographic data were not always present, but it appeared that, in general, participants were White, cis-gendered, heterosexual and in long-term relationships.
Clinical implications: supporting Autistic women to meet their infant feeding goals
The women in the included literature all planned to breastfeed where stated, and many were very determined. NICE guidelines (NICE, 2008) recognise that supporting this intention is important as breastfeeding protects infant and maternal health (Renfrew, Pokhrel, et al., 2012) while not being able to meet breastfeeding goals can have a negative impact on maternal mental health (Brown, 2019). However, we found that Autistic mothers had very limited support from their personal networks (which typically did not expand to include new friends made in postnatal groups) or health professionals when they encountered breastfeeding difficulties.
There is an urgent need for health services to be better informed and organised to accommodate Autistic mothers and for health professionals to understand Autistic differences, including sensory processing challenges, different pain presentations, communication differences and different help-seeking presentations to neurotypical women. Our review suggests the following considerations:
Communication should be clear, direct and specific and ideally followed up with written information.
Mothers should not be touched, (for example, when demonstrating breastfeeding attachment) without explicit consent.
Staff should receive training and tools related to autism, but this also needs to be specific to infant feeding and able to be tailored to each Autistic mothers’ individual needs.
Autistic mothers should have a named provider of maternity and infant feeding support to avoid needing to repeat their needs to new members of staff.
Guidance on communication and sensory needs to be included in maternity notes (‘handheld notes’ in the United Kingdom) and child health records (‘the red book’ in the United Kingdom) for all mothers, would also lower the burden on Autistic mothers required to regularly reassert their needs.
These recommendations, while focused on the needs of Autistic women, will improve maternity and infant feeding services more widely, with many accessibility measures benefitting all (Bracken & Novak, 2019). This is important because of the presence of undiagnosed women at the time of birth, stigmatisation and fear associated with disclosing an autism diagnosis, which may lead to lack of disclosure from Autistic women to healthcare services, and healthcare providers’ lack of linked information systems across departments. We propose service improvement in general, rather than setting up bespoke separate services.
Directions for future research
Our review highlights that Autistic women’s infant feeding experiences are under-researched and there is a need for further firsthand accounts of Autistic motherhood to be included in research. In addition, quality improvement interventions to meet the needs of Autistic mothers should be developed and evaluated in line with best practice guidance (Skivington et al., 2021).
Conclusion
Our systematic review of the infant feeding experiences of Autistic women identified multiple barriers to breastfeeding and few facilitators. Some of these barriers were intrinsically related to sensory processing and pain, but others were typical barriers to breastfeeding, which were exacerbated by Autistic mothers’ lack of social support and the inaccessibility of infant feeding support services. Accessibility measures should be urgently introduced into infant feeding services to support Autistic women to meet their breastfeeding goals.
Supplemental Material
sj-xlsx-1-aut-10.1177_13623613221089374 – Supplemental material for Autistic women’s views and experiences of infant feeding: A systematic review of qualitative evidence
Supplemental material, sj-xlsx-1-aut-10.1177_13623613221089374 for Autistic women’s views and experiences of infant feeding: A systematic review of qualitative evidence by Aimee Grant, Sara Jones, Kathryn Williams, Jennifer Leigh and Amy Brown in Autism
Footnotes
Acknowledgements
The authors wish to thank the members of the Autistic Breastfeeding, Chestfeeding and Bodyfeeding Parents online support group for their feedback on the design of the study. We also wish to thank Ellie Downes, subject librarian, for support in developing the systematic search strategy.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: K.W. is a director of Autistic UK, an organisation that provides consultancy on a not-for-profit basis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This systematic review was funded in part by the Research Wales Innovation Fund, who funded Jones’ time. Grant’s post is funded by the Higher Education Funding Council for Wales, which also supported Brown’s time on this project. Open access publishing was partially funded through an agreement between Sage and Swansea University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.