
Abstract
Autistic people are over-represented at gender clinics, but there is limited research to guide clinical practice with this group. We investigated the perspectives of clinicians working with autistic patients who experience gender dysphoria. We asked clinicians about the relationship between autism and gender dysphoria, and whether they work differently with this patient group. We recruited clinicians from young person and adult gender clinics and autism services (n = 16). We analysed the interview transcripts using interpretative phenomenological analysis (IPA). The first overarching theme was clinician understanding of the intertwined experiences of patients, with four subthemes: (a) coming to an individualised understanding of autism, gender dysphoria, and mental health; (b) different ways of thinking about gender; (c) social differences as barriers and facilitators to gender comfort; (d) the challenge of sensory sensitivities and puberty. The second overarching theme was mismatch of patient and clinician communication styles and goals, with three subthemes: (a) different communication of gender needs; (b) changing clinical sessions to overcome barriers; (c) tension between clinician and patient aims and thinking styles. We conclude that autism adaptations should be made in gender settings, by increasing clinician understanding of how autism and gender dysphoria can intersect, as well as by making adjustments to clinic processes.
Lay Abstract
Autistic people are more likely to have a gender identity which does not match their sex assigned at birth. Some people experience distress about their sex and gender not matching, which is called gender dysphoria. Such individuals may wish to attend a gender clinic to access healthcare support for gender dysphoria. Currently, there is limited evidence to help clinicians best support autistic people who need healthcare for gender dysphoria. We wanted to find out what healthcare clinicians think about working with autistic patients with gender dysphoria. We interviewed 16 clinicians who work in healthcare services with adults and young people who are autistic and experience gender dysphoria. We recorded the interviews and carefully analysed the content to find key themes. We found that clinicians worked with patients to try and better understand their experiences of gender dysphoria. Clinicians identified features of autism that they believed were related to gender identity and dysphoria including different thinking styles, social differences, and sensory sensitivities. Clinicians noticed that autistic people spoke about their gender in different ways to non-autistic people. Clinicians tried to adapt their practice to better meet the needs of their autistic patients. These adaptations tended to focus on differences in the assessment process, for example, offering longer or shorter appointments and changing their communication style. We conclude that clinicians were offering an individualised approach to autistic patients experiencing gender dysphoria. However, these clinicians were particularly interested in working with autistic people, and so may not be representative of the wider clinician population. Clinicians working in this area should receive training on autism adaptations and the intersection of autism and gender dysphoria.
Keywords
Gender clinics provide healthcare to gender-diverse individuals, who may be exploring their gender identity, or who are transgender and have a gender identity different to their sex assigned at birth. A subset of transgender people experience gender dysphoria, which is distress associated with an incongruence between sex and gender (5th ed.; DSM-5; American Psychiatric Association, 2013). Some transgender people may wish to access gender clinics in order to consider making a social and physical transition so that their gender expression, that is to say, behaviours expressing a particular gender, and bodies, are changed in line with their gender identity. Transgender and gender-diverse people are more likely to be autistic than cisgender people (Warrier et al., 2020). Research in this area has explored the co-occurrence of autism and transgender identities (for a review, see van der Miesen et al., 2016), and has also considered the co-occurrence of gender- and neuro-diversity more broadly, including attention-deficit hyperactivity disorder (ADHD; Thrower et al., 2020). There is further evidence of higher rates of mental health needs in autistic people who are transgender, as compared to other autistic people (George & Stokes, 2018; Murphy et al., 2020). This is significant given the elevated rates of mental health problems in both autistic people (Lai et al., 2019) and in transgender people (Nobili et al., 2018) compared to the general population. Furthermore, there is evidence of an increased rate of autism in adults and young people accessing gender clinics internationally, ranging from 5% to 26% (Cheung et al., 2018; de Vries et al., 2010; Holt et al., 2016; Kaltiala-Heino et al., 2015; Pasterski et al., 2014).
There has been much speculation and some research into the causes of the high co-occurrence of autism and being transgender and gender diverse in children, young people, and adults. It is important to note that gender has been conceptualised differently across time and in different contexts and that an individual’s experience of their gender identity is likely to be affected by a complex range of biological and environmental factors (Glidden et al., 2016). Some authors have suggested that certain features of autism may cause a predisposition to be transgender or gender diverse. For example, Bejerot and Eriksson (2014) suggested that the social differences associated with autism might lead to gender defiance. Walsh et al. (2018) argued that a resistance to social conditioning might contribute to higher rates of gender diversity. This aligns with the accounts of autistic adults who have experienced gender dysphoria, some of whom described experiencing more freedom to express their gender identities than might be available to non-autistic individuals (Cooper et al., 2021). Other theories have centred on the restricted and repetitive behaviours, interests, and activities domain of the autism diagnostic criteria: such research has tested hypotheses that differences in sensory profiles in autistic adults may be associated with gender diversity (Walsh et al., 2018). A large-scale study found that sensory sensitivities are higher in transgender and gender-diverse people as compared to cisgender people, and yet higher in transgender autistic individuals (Warrier et al., 2020). Qualitative research findings indicate that the relationship between sensory sensitivities and gender dysphoria may occur through experiences of sensory dysphoria, whereby the sensory sensitivities which accompany autism exacerbate feelings of gender dysphoria by heightening sensitivity to negative experiences of one’s body (Cooper et al., 2021).
In terms of the existing qualitative research, two studies have been published on the experiences of autistic adults of gender dysphoria in the United Kingdom (Coleman-Smith et al., 2020; Cooper et al., 2021), and two studies on the experiences of transgender young people in the United States (Strang et al., 2018b, 2021c). Autistic adults suggested that being autistic could complicate the experience of gender dysphoria and seeking transgender healthcare (Coleman-Smith et al., 2020). Some autistic adults have described that concrete thinking about gender categories could increase distress when they were exploring and uncertain about their gender identities and described sensory dysphoria (Cooper et al., 2021). In another study, some autistic young people explicitly stated that their gender identity was not influenced by obsessional thinking, nor autism more broadly (Strang et al., 2018b). Youth in this study wanted to ensure that their gender identities were taken seriously, without autism unduly influencing others’ perceptions of their gender identities.
There is limited evidence to guide clinicians working in gender clinics with autistic people, despite this burgeoning interest in the relationship between autism and transgender identities. In the United Kingdom, the National Health Service (NHS) provides gender-related healthcare. The World Professional Association for Transgender Health (WPATH, 2012) publishes clinical guidelines for healthcare practice supporting transgender and gender-diverse people. This includes a thorough assessment of gender dysphoria, including assessment of other factors such as mental health needs and autism and distinguishing these from gender dysphoria. If an individual meets diagnostic criteria for gender dysphoria, this can result in a referral to an endocrinologist to access hormone treatments, and in adults, access to surgeries to change one’s body in line with one’s gender identity. Reviews of such physical interventions in young people and adults have concluded that low certainty, observational evidence suggests positive effects on psychological well-being, and gender dysphoria symptoms (National Institute for Clinical Excellence [NICE], 2021; Nobili et al., 2018). Clinical guidelines differ depending on the age of the individual (WPATH, 2012), with extended gender exploration and developmental considerations applied to work with adolescents; therefore, clinicians working with adolescents will have a different approach to those working with adults. There is no specific advice in the WPATH standards of care for working with autistic people. Strang et al. (2018a) published a clinical consensus document to provide additional guidance for clinicians working with autistic adolescents experiencing gender dysphoria. This included advice that clinicians should assess for indications that the young person’s gender identity is caused by the features of autism or other co-existing conditions. This guidance is not necessarily reflective of practice in the United Kingdom, being based on a Delphi study with clinicians elsewhere.
Existing research has generally focused on quantitative work investigating how specific autism traits could contribute to higher rates of gender diversity in autistic people, and qualitative research has investigated the perspectives of autistic and transgender young people and adults. However, there is a dearth of evidence understanding the perspectives of clinicians. Given the crucial role that clinicians play in providing access to transgender healthcare, including in assessing gender dysphoria and its distinctiveness from other conditions including autism, it is important to understand their perspectives and clinical approaches to working with this group. Furthermore, in the absence of comprehensive guidance for working with autistic children, adolescents and adults experiencing gender dysphoria, thorough qualitative evidence is needed to begin to develop evidence-based clinical approaches.
In this study, we aimed to investigate the views of NHS clinicians working with autistic adolescents and adults who have been referred to gender clinics. We wanted to find out (a) their understanding of how autism and gender dysphoria intersect with one another in their patients and (b) how clinicians aimed to work with autistic people experiencing gender dysphoria in their clinical settings.
Method
Methodological approach
We used interpretative phenomenological analysis (IPA), a qualitative method (Smith et al., 2009), to investigate clinicians’ perspectives on the intersection of autism and gender dysphoria and clinical approaches when working with this group in healthcare settings. IPA is focused on the meaning of the phenomenon, in this case, gender dysphoria and autism, to the participant. IPA is a hermeneutic approach, which means that the researcher is actively making sense of the participants’ lived experiences. This paper is part of a larger project investigating the lived experience of gender dysphoria in autistic people from a range of perspectives. In this study, we were interpreting the clinicians’ understanding of autistic patients’ experiences of gender dysphoria. IPA is also an idiographic approach, which means that close attention is paid to the individual perspectives of each participant during the analysis and reporting of results.
Participants
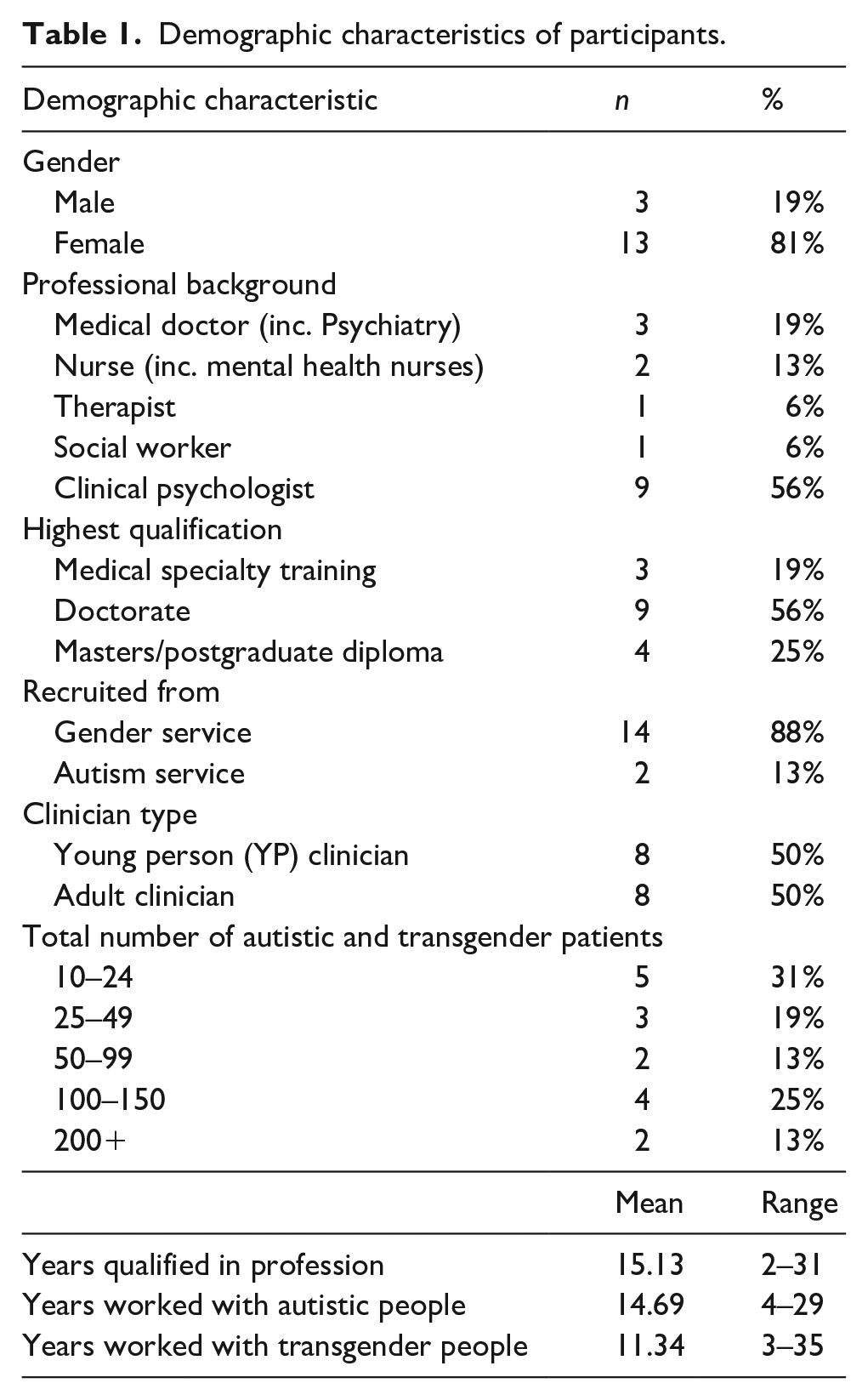
We recruited 16 healthcare clinicians who worked with autistic people who had experienced distress about gender incongruence (referred to as gender dysphoria in this paper). We aimed to recruit clinicians with a range of professional backgrounds and who worked with autistic and transgender people in various clinical settings. Participants needed to work in a setting where they had substantial contact with the patient group; for most clinicians, they were recruited from gender clinics (n = 14), but two were recruited from autism services to ensure a range of views were included. Half of the participants worked with children and young people (YP clinicians), and the other half worked with adults (adult clinicians). Of the adult clinicians, one had substantial experience working with young people, and of YP clinicians, none had substantial experience working with adults. Adult clinicians were recruited through adult gender and autism services, through personal contacts established by the research team, and by asking participants for recommendations of other potential participants. YP clinicians were recruited through a gender service and child and adolescent mental health services, particularly where clinicians specialised in working with autistic young people. The different recruitment strategy across clinician groups was due to there being a single gender service for young people, but multiple services for adults; adult clinicians came from a total of five different services, whereas YP clinicians came from two different services. To protect anonymity, limited demographic data for groups are presented together (see Table 1).
Demographic characteristics of participants.
Procedure
The study received ethical approval from the Health Research Authority (North East – York Research Ethics Committee; 19/NE/0265). Participants were invited to take part in the study through personal contacts of the research team and snowballing. These individuals were emailed the study information sheet with a request to take part. Recruitment took place during the COVID-19 pandemic and so study participation was remote and participants were invited to a research meeting via a video (n = 14) or phone call (n = 2). Interviews lasted an average of 45 minutes, with a range of 31–54 minutes.
During the research meeting, participants were asked to read the information sheet, ask any questions that they had, and complete a consent form if they agreed to take part. Participants were reminded of their right to withdraw from the study. The first author interviewed all participants. The interview began with collecting some demographic details relevant to the research question, focused on the professional experience of each participant. Clinicians were encouraged to reflect on their experiences of working with transgender and autistic patients; for those in gender clinic settings, this could mean individuals who already had an autism diagnosis, or who later received a diagnosis. The interview topic guide (see Appendix 1) began with open questions and was flexible, following the experience of each participant, based on IPA guidelines. Topics included the clinician’s experience of working with autistic and gender-diverse patients; if and how they thought that autism and gender dysphoria interact; if they thought that autistic patients experience gender dysphoria or conceptualise gender differently; whether the clinician adapted their practice when working with autistic patients; barriers to supporting this group; information needed by clinicians to work with autistic patients experiencing gender dysphoria.
Data analysis
In this paper, we use a multi-perspectival IPA design, with adult clinicians and YP clinicians both being interviewed about their perspectives on the intersection of autism and gender dysphoria. Analysis followed the guidance of Larkin et al. (2019) and was conducted by the first author with support from the co-authors. Each individual transcript was first analysed by noting the descriptive, linguistic, and conceptual elements, focused on clinician interpretations of the lived experience of gender dysphoria in autistic people. We ensured an awareness of context, including clinician experience and work setting, when analysing the transcripts. The analysis took into consideration of the complex hermeneutics involved, that is, the researcher making sense of the clinician’s understanding of the experience of gender dysphoria in their autistic patients. Once the initial noting and theme development had been conducted, we drew together important themes for each individual participant. The themes reported in this paper are focused on clinicians’ perspectives on the experiences of their patients, although the experiences of clinicians were included in the analysis and are reported on in the following results section where relevant to the experiences of autistic people accessing gender healthcare. We drew together themes when the notes had similar or oppositional ideas or functions within the interview, and important contextual factors. We then developed overall themes for each clinician group, first adult clinicians (n = 8), and then YP clinicians (n = 8). At the synthesis stage, the two sets of themes were drawn together and combined into one set of themes, with a careful consideration of the similarities and differences between participant groups, which are described in the following results section. Quotes were selected when they clearly articulated the meaning of a theme, and in order to represent the range of clinicians interviewed. Participant numbers are provided in the following results section indicating whether they originated from an adult clinician (e.g. A1) or a YP clinician (e.g. YP1).
In order to ensure that we conducted a high-quality analysis, we practised reflexivity and discussed our positionality and assumptions throughout the research project. The research team consisted of clinical psychologists who are all cisgender and neurotypical. The first author, who conducted the data analysis, received postgraduate-level training in qualitative research methods, as well as receiving supervision from the co-authors who are experienced in qualitative research with autistic people. The first author attended IPA research groups and kept a reflexive diary, as well as taking the analysis to supervision and presenting it to research groups to ensure that it was grounded in the transcripts and participant experiences.
Community involvement
A group of transgender autistic adults (n = 6) provided advice on the research question and design of this study. This group were recruited from an NHS support group for transgender autistic adults and advised on the conduct of this and other related papers. We also asked clinicians with relevant expertise to advise on the structure and length of the interview schedule.
Results
The analysis resulted in two superordinate themes, both with subthemes (see Figure 1).
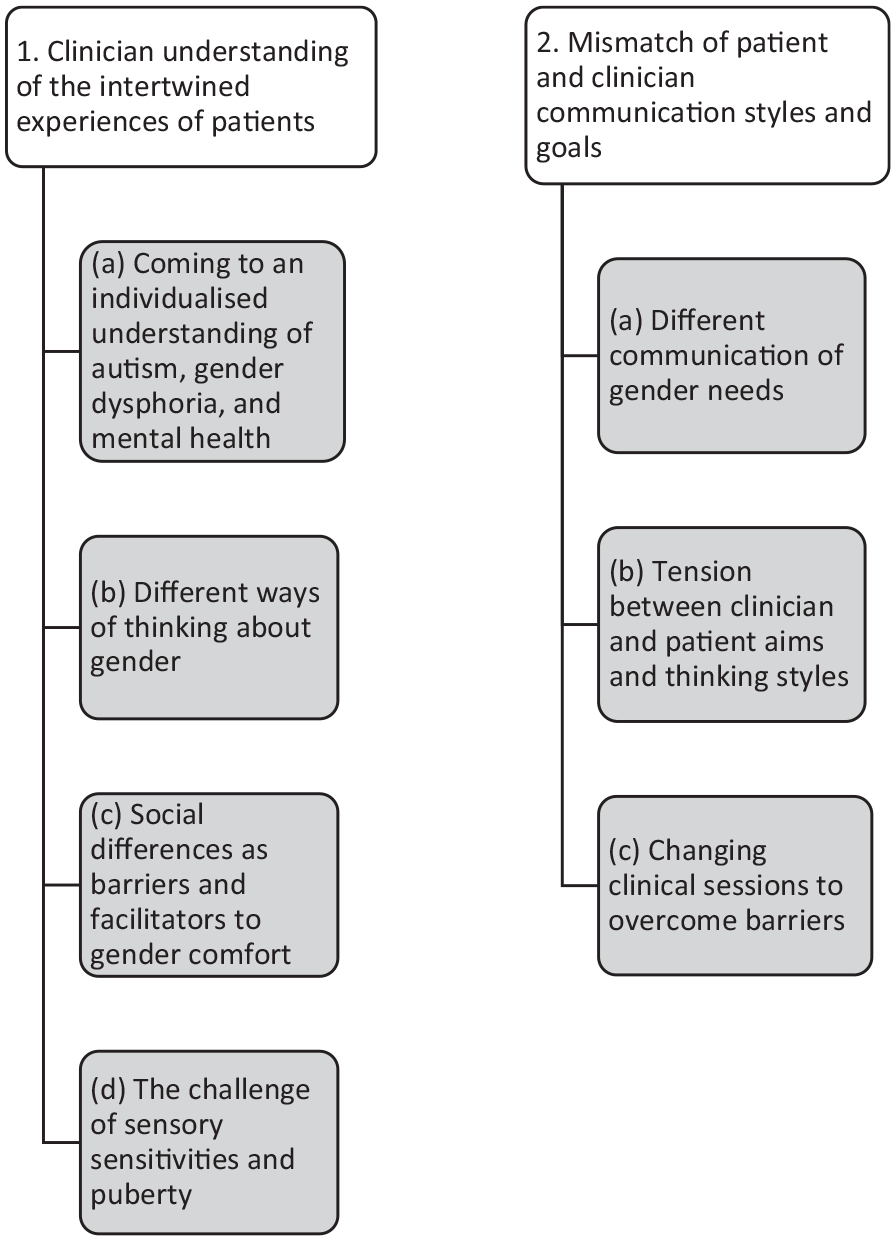
Themes and subthemes identified through IPA analysis.
Clinician understanding of the intertwined experiences of patients
Clinicians were invested in better understanding their patients’ experiences. Clinicians described how they thought about the relationship between autism and gender identities and gender dysphoria and conceptualised these different facets of their patients as related to one another. Many clinicians noticed differences between autistic and non-autistic patient experiences and so thought deeply about how specific features of autism related to gender, including through different thinking styles, social, and sensory differences.
Coming to an individualised understanding of autism, gender dysphoria, and mental health
All clinicians interviewed described how they conceptualised the relationships between autism, gender dysphoria, and mental health. It was important to clinicians that this conceptualisation was individualised and based on the particular experiences of each patient. The context and age of patients influenced their viewpoints, with adult clinicians more ‘zoomed in’ on gender dysphoria and YP clinicians focused on understanding distress more broadly.
Many adult clinicians described the need to understand a person’s autism as an integral part of themselves, which was intertwined with their gender identity. Most adult clinicians framed autism and gender dysphoria as interrelated rather than one causing another. Participant A5 emphasised the way in which they conceptualised being autistic and experiencing gender dysphoria as related but distinct:
You know how a rope is made of separate strands closely wound round each other, if you stand back at a distance it looks like one thing but on closer examination the two things are distinct, it’s just that they wind round each other a lot so you can sort of think of them as working in unison or being a problem in unison.
The use of the metaphor of a rope to clarify the clinician’s position suggests deep analytic thought on the topic, indicating the importance to clinicians of understanding these facets of their patients’ identities.
YP clinicians emphasised the need to understand the young person’s gender identity, experiences of distress, and the role of autism within this. Clinicians expressed that their patients’ feelings about their gender were in flux and warranted exploration. The aim was to understand if all the distress was about gender, or whether other factors were also contributing to distress. For example, clinician YP7 noted that they tried to understand all distress the young person was experiencing:
I suppose my experience is often first just think about the distress and where it’s from and is the distress getting in the way of doing further thinking and exploration? And so sort of think about making sure that the young people have got the skills to deal with distress full stop.
This aim linked to YP clinicians’ assertions that young people were often focused on gender dysphoria as the main cause of distress, but that other causes of distress often existed. For example, clinician YP8 described:
I’ve had young people who have really come to understand themselves that way, who have spotted ‘oh I have shutdowns, I really find social situations really overwhelming’ . . . without that understanding of themselves as autistic they’ve assigned lots of the distress to gender and then as we’ve talked about autism, they’ve come to see that actually there are lots of things contributing to distress.
This quote shows the clinician as considering their patients’ evolving self-understanding, and emphasis on the many causes of distress for the young person. The three above quotes demonstrate the ways in which all clinicians were thinking deeply about the relationship between autism and gender dysphoria but that adult clinicians tended to zoom in specifically on gender dysphoria, whereas YP clinicians often saw their roles as to understand distress more broadly, including but not limited to the role of autism and gender dysphoria. These different perspectives between clinicians are evident throughout the following findings analysis and themes, although there were differences within the two groups as well as between them.
Different ways of thinking about gender
Most clinicians noted that specific features of autism including detail focus, concrete thinking, and a need for certainty and control could all increase gender dysphoria. These factors could also cause difficulties when undertaking a gender transition. Some YP clinicians described how they felt that different thinking styles in autism could contribute to seeing oneself as transgender, such as YP4:
I guess maybe if you’ve got a more black and white concrete way of thinking about this stuff, then it may be easier to reach a conclusion [about being transgender], you know, whereas someone who’s neurotypical might be able to consider things in a more complex way or a more nuanced way.
This quote demonstrates how the clinician felt that nuanced thinking about gender identity was needed to come to a full understanding of one’s gender and that they thought that autistic young people may be less likely to think in this way. However, another YP clinician felt that cognitive profiles in autism could have the opposite effect, leading a more rigorous and reflective approach to understanding gender identity in autistic young people:
I would say that maybe I’ve met more autistic people who have maybe done a bit more systematic questioning potentially of their gender. Maybe might describe the process more of like figuring things out and working through different options and maybe might be quite reflective about different parts of things and why they feel the way they do. (YP6)
These two quotes together show that clinicians identified particular thinking styles in autism and noticed that these same thinking styles could contribute to divergent outcomes: either a rigorous and thoughtful, or a less-complex thinking process behind gender identity. Implicit in these quotes is the emphasis that YP clinicians placed on helping their patients reach a full understanding of their identities in general.
Some of the adult clinicians and YP clinicians described how this style of thinking could lead to high expectations of a gender transition, increasing distress. One clinician described how a specific, rigid, and detailed vision of what should happen during a gender transition could reduce satisfaction in the outcomes:
I think that all of this comes down to either specific focus or cognitive rigidity, and where people struggle with flexible thinking or accepting themselves as different but equal, that cognitively people with autism struggle harder to make that adjustment and that that can lead to people feeling that they are less able to say good enough is good enough. (A1)
Social differences as barriers and facilitators to gender comfort
Social differences associated with autism were described as causing challenges to autistic patients. Most adult clinicians described reciprocal relationships between social differences and gender dysphoria. For example, clinicians explained how difficulties with understanding others’ thoughts and feelings could lead to idiosyncratic gender expression and more incidents of being misgendered, thereby increasing gender dysphoria. One adult clinician (A2) described how one of their patients was frustrated by others misgendering them, and that difficulties understanding others’ perspectives increased the likelihood of being misgendered:
Somebody I was working with would wear facial hair even though they very much identified with a binary . . . gender as female and they couldn’t understand why, when they told people that they were female, people was still referring to them as male.
Moreover, undertaking a gender transition led to more complex social situations to navigate, increasing social challenges, as described by the same clinician:
I’m already feeling an outcast from society because of my autism. If I then start making moves to do something about changing my gender expression I’m going to be further making myself a target, vulnerable, excluded from society and it’s hard enough as it is. Why would I want to put myself through that process? (A2)
While adult clinicians often described specific interactions between social differences and gender dysphoria, YP clinicians tended to focus on the broader impact of social differences on a young person. YP clinicians often spoke about how patients felt different to their peers and that this could affect their feelings about their gender:
They get to puberty and they start questioning gender and wondering if some of the differences that they’ve noticed between them and their peers might be about gender. (YP5)
An adult clinician also described the relationship between feeling generally different and how this could contribute to feelings of gender difference:
I think some people on the spectrum have talked about feeling very different, feeling like an alien on the planet, feeling like they don’t understand the social rules and they didn’t get the handbook about how to be human . . . some people have talked about gender stuff coming secondary to that but then some people on the spectrum have talked about that being at the forefront. (A8)
These two quotes show how clinicians actively considered the social differences due to autism and their relationship to feelings of gender difference, with a need to ‘unpick’ (YP5) these experiences and position different needs within a hierarchy of importance and urgency. Clinicians therefore wanted to understand whether gender needs were ‘secondary’ to autism needs or in the ‘forefront’ (A8) when meeting patients.
Most adult clinicians and some YP clinicians felt that autistic people had strengths when considering their gender identities, and autism could contribute to a feeling of freedom from gender norms:
Autistic people being sometimes just kind of matter of fact about things and not necessarily overthinking things and getting themselves caught up in societal expectations of how to be and who to be and what to do. . . If they feel, you know, trans, non-binary, gay, whatever it is they might be, they sometimes just don’t overthink it in the same way that other people would in society that might stop them from pursuing that kind of part of themselves. (A4) Autistic people describe themselves as being more critical of social norms and constructs than neurotypical people and some people have said that that might lead them to just question things more in the world and that includes everything. So you know, their gender. Other parts of identity. (YP6)
Again, these quotes indicate that the social differences that come with being autistic could have divergent effects; feeling like an outsider could make it more difficult to fully understand one’s gender identity, while also allowing freedom from societal expectations around gender.
The challenge of sensory sensitivities and puberty
Clinicians in both groups identified that an individual’s sensory sensitivities could contribute to both difficulties making a transition and to dysphoria. YP clinicians tended to focus on the development of gender dysphoria, while adult clinicians focused more often on the impact on gender transition. For example, one adult clinician described how taking cross-sex hormones impacted on sensory issues, which without the clinician having a clear understanding of autism, could have led to a halt to gender treatment:
one person who didn’t like the feeling when air went across their skin with hair on so . . . that was the thing they didn’t like about the effects of testosterone so they would remove their body hair and you would think or because you’re not happy with the effects of treatment, no they were happy, they just didn’t like it was the flow of air across their skin with hair on. (A3)
YP clinicians highlighted sensory differences, and other changes during puberty, as a ‘tipping point’ (YP5). At this developmental stage, the autistic experience of adolescence, with heightened distress due to new sensory experiences, changing bodies and different adolescent social experiences, was thought to contribute to increased gender dysphoria. One YP clinician described the challenges of puberty for gender-diverse autistic young people:
puberty can be really problematic for autistic young people, for all sorts of reasons to do with change, body, smell, periods, all sorts of stuff to do with sexual feelings that feel like unmanageable. (YP2)
Moreover, clinicians wanted to explore and better understand the relationship between distress about puberty which was due to autism and a dislike of change and new sensory experiences, versus distress which was due to gender dysphoria:
one of the things that we’ve had to really carefully unpick is how much of this is about that this is gender signifying body hair, facial hair or thicker body hair and how much of this is because you don’t like the feel of body hair. Or you know, is the change at puberty in itself distressing? (YP7)
Unlike with social differences and different thinking styles, sensory differences were described as causing only challenges, and clinicians did not link these to strengths or positive experiences in relation to gender identity or dysphoria.
Mismatch of patient and clinician communication styles and goals
This theme captures how clinicians noticed that autistic patients communicated in different ways about gender, as compared to other patients accessing gender healthcare. Clinicians actively tried to understand these differences in communication to make sense of their patients’ experiences of gender dysphoria, and to address the mismatch between their clinical practice and patient needs. For YP clinicians, there was a further gap between patient thinking styles around accessing gender affirming treatment, and clinician aims of exploring gender.
Different communication of gender needs
Most clinicians spoke about how communication about gender was different in autistic patients compared to other patients. Expressions of distress were described as more rational, cognitive, and abstract:
I think, some of my clients that are autistic, are probably better at describing it, in the way that they reel stuff off but actually it’s very detached from an embodied experience. . . . They can be quite descriptive, but it feels like it’s in quite a superficial way, in terms of not being able to get to the bottom of it, or apply it to different things. You know that kind of joined up thinking. (YP3)
This clinician’s quote also speaks to the mismatch between their aim of helping the patient develop ‘joined up’ thinking about gender and the patient’s communication style. One adult clinician said that autistic patients might provide less emotional detail but were able to describe physical experiences:
So some people might report more prominent physical symptoms rather than be able to describe their emotional state. (A3)
Another adult clinician said that dysphoria might be expressed more through behaviour and gestures due to difficulties finding the words to express their feelings:
I’ve had a patient go into the foetal position while they’ve been in the room, totally shut down. I’ve seen others get quite aggressive because of their frustration that they can’t get the words out. As I’ve said I’ve seen people beating their chest because they’re trying to tell me that they’re so dysphoric. (A7)
Tension between clinician and patient thinking styles and aims
Many of the clinicians working with young people in gender services spoke about their feeling of responsibility to introduce uncertainty and flexibility into young people’s thinking about their gender identities, with a fear that young people could make life-changing decisions about their bodies without having thought about all potential gender journeys and types of transition. Clinicians discussed how concrete thinking linked to autism could create difficulties when trying to have these sorts of conversations, with a mismatch of approaches. For example, one clinician said:
. . . [this] results in quite a significant clash of therapeutic approach and so, I suppose then, the barriers to exploration become much more – so it’s generally acknowledged that, young people who want to have access to this intervention, should be encouraged to explore their gender and explore some of those early experiences to ensure . . . and yet I suppose that explorative process with autistic young people can be doubly hard and take a lot longer and have to be very slow and more intensive. Perhaps they are all the things that are currently very impaired in terms of the resources available to them. (YP2)
Some YP clinicians shared that they felt a tension between their aim of exploring gender identity and their patients’ aims of accessing physical interventions so that they could change their bodies in line with their gender identities. One YP clinician explained:
Especially for young people who are very keen on medical intervention, I felt my work was often about wanting to help them have a kind of richer sense of their gender experience to help them link it with other aspects of their lives, like their autism. But particularly where young people were wanting medical intervention, I think they found that quite hard to tolerate because it felt to them as though I was; as though acknowledging those aspects might make it less likely they’d get the medical treatment. (YP8)
YP clinicians highlighted that parents also had a crucial role to play in introducing curiosity about gender and that this depended on parental ability and willingness to think in flexible ways about their child’s gender. They stated that it was important to consider the wider societal context in their work with young people, including polarised views on transgender health, long waiting lists for gender, mental health, and autism services, family circumstances and attitudes, and discrimination against autistic people in society and health services. These factors further complicated their role in introducing a curious and questioning approach with autistic young people in gender sessions. One clinician described this dilemma, demonstrating their commitment to developing a positive working relationship with their patient while also helping them explore their gender identity:
how can we negotiate a relationship that involves questioning and exploration but that’s understood as being not unaffirmative and unsupportive. (YP7)
Both quotes underscore the difficulties clinicians experienced in supporting autistic young people who have a preference for certainty and may think inflexibly, while also committing to gender exploration with the young people they worked with.
Changing clinical sessions to overcome barriers
Both adult and YP clinicians described how they made adaptations to their usual communication style, in response to the above communication differences. Clinicians knew that their typical ways of working could be unhelpful for autistic patients, with one clinician highlighting that neurotypical clinicians could be barriers to autistic patients in gender settings:
maybe some neurotypical people might shift themselves around the needs of the therapist to work in a particular way and that maybe some autistic people don’t. The therapists, mostly the barriers of the therapists, the barrier because they’re having to do some changing too you know if they’re neurotypical and yes so maybe it’s just the therapists are the main barrier. (A1)
All clinicians described ways that they had proactively worked differently with autistic people to try and overcome such barriers to improve the quality of meetings. Adaptations included changes to the way clinicians spoke: some clinicians tried to be direct and clear in their use of language; used open questions with specific prompts; used special interests to increase engagement; minimised gesture; used an even tone of voice; minimised eye contact. One adult clinician described these communication adaptations:
If you’re using inflections and gesturing, etcetera, again if someone’s got body language difficulties you just make it worse and then of course that classic thing if someone doesn’t understand what you do is you just talk louder, which of course if you’ve got sensory sensitivities again that’s the worst thing to do in the world. Even just little understandings around things that someone, when they’re really listening to you, may not look at you. (A6)
Sometimes the content of sessions was changed, with clinicians providing information to patients without expecting an immediate response. Many clinicians said that they used written and visual resources including videos, charts, pros and cons lists, tables, diagrams, and gender maps to explore gender in more detail. One clinician described such visual adaptations:
We’re using visual aids and doing as much as possible like writing things out. Drawing things out. Using scales. Trying to really simplify things as much as needed. So like, when we’re talking about body distress, literally drawing out a body and getting them to colour bits in that relate to how they feel. (YP5)
Adaptations to the clinic setting included having an initial introduction session, structural changes to sessions (considering their length, frequency, and number), ordering the agenda of sessions to not overwhelm patients and considering the physical environment including waiting area and toilets, for example:
Breaking it down particularly if someone’s got a learning disability you know someone to talk to you for an hour or an hour and a half or two hours. Sometimes there’s no value beyond 20 minutes, so keeping really short. (A3)
Discussion
We found that adult and YP clinicians alike described autism and gender dysphoria as meaningfully interrelated. For some clinicians, their thinking was about how autism contributed to gender dysphoria, and for others, the focus was on how the two related to one another. All clinicians interviewed had thought about how to adapt their practice when working with this group and were actively trying to reduce communication and other barriers to better support autistic patients.
We found that clinicians interviewed in this study had engaged in deep thought and analysis about their autistic patients who had experienced gender dysphoria; however, it should be noted that this group were recruited due to their interest in this area. There were differences in the approaches of clinicians depending on the age group of patients; notably YP clinicians tended to focus more on their responsibility to help patients explore their gender and that this could cause tension with autistic patients in particular. These differences are in line with the WPATH standards of care 7, which indicate that gender exploration is particularly important with children and young people. Clinicians tended to acknowledge the complexity and individual nature of gender identity, and many emphasised the need to take an individualised approach with patients. This is in line with the biopsychosocial model incorporated into most medical and psychological clinical training courses (Engel, 1977), which involves understanding the many factors contributing to a patient’s needs. This individualised approach could be seen to be at odds with the more polarised and binary media narratives around transgender healthcare and rights in the UK context, exemplified by strong responses to the Gender Recognition Act consultation in 2018 (Pearce et al., 2020). Such narratives sometimes imply that clinicians hold a particular stance which is then applied to every patient that they see, for example, providing too much or too little access to physical interventions, such as puberty blockers, cross-sex hormones, and surgery, irrespective of the circumstances of each patient. However, in these interviews, clinicians were thoughtful about each patient’s particular circumstances, gender experiences, beliefs, and context.
Clinicians identified ways in which the specific features of autism, as well as co-occurring conditions and experiences, interacted with gender dysphoria in their patients. In fact, most features of autism were described as interacting with gender by at least some clinicians. There may have been selection bias for seeing such links, in that clinicians offered to participate due to a pre-existing interest in the intersection of autism and gender diversity. In line with previous quantitative (Bejerot & Eriksson, 2014) and qualitative research (Cooper et al., 2021), clinicians felt that social and cognitive differences in autism contributed to different gender experiences and in some cases, heightened gender dysphoria. Social differences were seen as having positive effects by some clinicians, contributing to more freedom of gender expression, while also having a negative impact, increasing the risk of being misgendered, or difficulties understanding one’s differences to peers. Moreover, cognitive differences were described as contributing to either more systematic, or less complex, thinking about one’s gender identity. However, clinicians did not endorse the idea that autistic patients experienced gender dysphoria due to a special interest or obsession about gender. These findings largely align with accounts of autistic transgender adults, who described both positive and negative impacts of social differences on their experience of gender identity and dysphoria, and who described cognitive differences affecting their experience of gender dysphoria, for example, with a need for certainty increasing distress when exploring gender (Cooper et al., 2021).
These findings indicate the importance of young people and adults having access to autism diagnostic services and to assimilate such diagnoses into their self-understanding, alongside transgender healthcare. Such an understanding allows for an exploration of the ways in which social and cognitive differences linked to autism might impact on one’s gender journey. Clinicians also described sensory differences as impacting on experiences of gender identity and dysphoria, in line with qualitative findings from autistic adults with gender dysphoria (Cooper et al., 2021) and of higher sensory hypersensitivity in autistic transgender people compared to non-autistic transgender people (Warrier et al., 2020). Clinicians should be aware of the different sensory profiles present in autistic people and keep these in mind during discussions about social and physical transition in this group. Participants working with young people highlighted that sensory differences in autism could cause particular difficulties in puberty for gender-diverse young people. Autism-adapted support to help manage the challenges of puberty may benefit autistic people across the gender spectrum (e.g. Visser et al., 2017).
Clinicians highlighted that autistic patients may have differences in how they describe dysphoria, with descriptions more physical, and emotionally detached; this fits with the higher rates of alexithymia found in autistic people (Kinnaird et al., 2019). Clinicians described working differently with autistic patients in terms of the structure of consultations, communication style, and changes to the clinic environment, rather than on treatment options. However, in line with WPATH guidance, treatment is contingent on an assessment of gender dysphoria, which depends on effective communication during consultations. The adaptations described by clinicians are in line with recommendations for adapting psychological practice for autistic people (NICE, 2012, 2013) and which have been described as helpful by autistic adults accessing gender clinics (Cooper et al., 2021). Adaptations such as changing the structure of sessions also demonstrate that clinicians are adapting for the higher rates of executive function needs in autistic and transgender young people which could create barriers to accessing gender clinics (Strang et al., 2021a, 2021b). The findings are somewhat concordant with previously published clinical guidelines for working with adolescents with co-occurring autism and gender dysphoria (Strang et al., 2018a), in that YP clinicians described assessing the intensity of gender dysphoria, providing space for exploration of gender, using autism adaptations and structure to facilitate exploration, and exploring the relationship between autism and gender dysphoria but did not routinely involve an autism expert and gender expert working together. There is a need for a more robust evidence base investigating outcomes in autistic people who access gender clinics, across the lifespan, to inform more specific clinical guidance for working with this group.
The study is the first to use carefully conducted qualitative methods to better understand the perspectives of two groups of clinicians working with autistic people with gender dysphoria. This has provided a window on clinical practice in this area, which is important, given the assertion in clinical guidance that clinicians should distinguish between gender dysphoria and co-occurring conditions, including autism, before making referrals for physical interventions. There are a number of limitations, including that IPA and qualitative methods more broadly focus on lived experience, rather than hypothesis testing; that the recruited sample are not representative of all clinicians, as they were recruited due to having a particular interest or experience in working with autistic and transgender people and only from NHS settings; that clinicians came from both gender and autism settings; that it was not possible in the interviews to understand differences between patients who had pre-existing autism diagnoses and those who later received a diagnosis.
There are important directions for clinical research and practice emerging from these findings. First, it is important that clinicians should receive training on the intersection of autism and gender dysphoria, given our finding that experienced clinicians had complex conceptualisations regarding how autism and gender dysphoria interact with one another, as explored in the first theme of the results. Clinicians working in gender settings should also receive training in autism awareness, adapting clinic practices and communication style. Research evaluating the efficacy of such training in improving patient experiences is warranted. Given that there were differences between views of clinicians working with young people and adults, more research regarding different approaches in these two clinician groups in gender settings is required. Furthermore, research into the different gender journeys of autistic people accessing transgender healthcare, as well as the efficacy of physical interventions for this particular patient group, are needed to better support clinical decision-making for autistic people experiencing gender dysphoria.
In conclusion, clinicians identified specific ways in which autism and gender identities and dysphoria intersect, which align with the lived experiences as described by autistic adults. Clinicians described attempts to make autism adaptations to better meet the needs of autistic patients, which tended to focus on changes to the assessment phase of clinical work in gender settings.
Footnotes
Appendix
Topic guide.
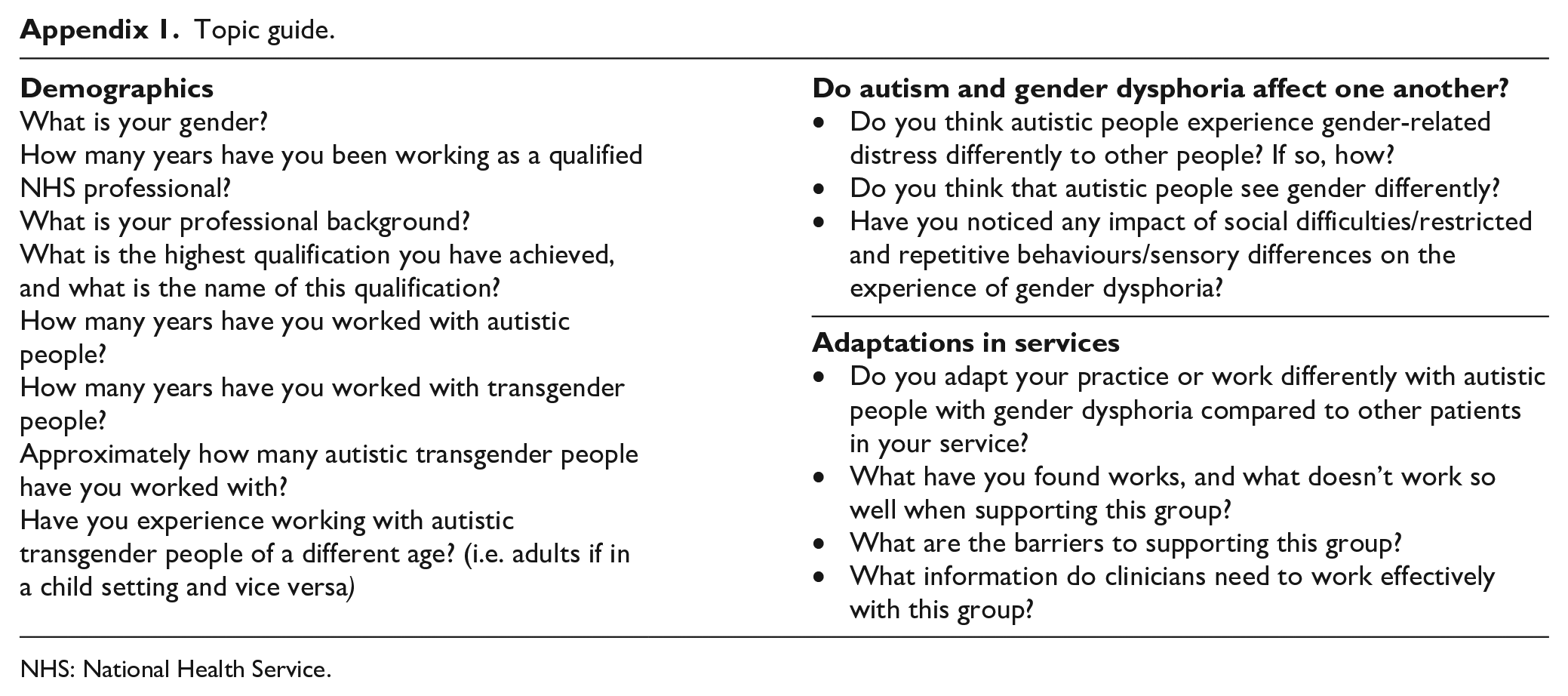
What is your gender? How many years have you been working as a qualified NHS professional? What is your professional background? What is the highest qualification you have achieved, and what is the name of this qualification? How many years have you worked with autistic people? How many years have you worked with transgender people? Approximately how many autistic transgender people have you worked with? Have you experience working with autistic transgender people of a different age? (i.e. adults if in a child setting and vice versa) |
Do you think autistic people experience gender-related distress differently to other people? If so, how? Do you think that autistic people see gender differently? Have you noticed any impact of social difficulties/restricted and repetitive behaviours/sensory differences on the experience of gender dysphoria? |
Do you adapt your practice or work differently with autistic people with gender dysphoria compared to other patients in your service? What have you found works, and what doesn’t work so well when supporting this group? What are the barriers to supporting this group? What information do clinicians need to work effectively with this group? |
NHS: National Health Service.
Acknowledgements
The authors thank the Spectrum Support Group for helping develop the research question and methods and all the people who took part in the interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.C. is funded by a National Institute for Health Research (NIHR) Clinical Doctoral Research Fellowship for this research project (ICA-CDRF-2018-04-ST2-047).