
Abstract
Restrictive and Repetitive Behaviors and Interests represent a core feature of autism since the earliest conceptualization of the condition. Related behaviors, such as hoarding and self-injurious behaviors, are under-researched in adulthood, resulting in limited knowledge about their various manifestation through the life span. This study expands our understanding of hoarding and self-injurious behaviors through subjective experiences shared by autistic adults. Ten adults with an autism diagnosis (aged 18–55 years, five females) participated in semi-structured, in-depth interviews. Thematic analysis identified a cluster of behaviors related to hoarding and self-injurious behaviors. Further analysis sub-categorized each theme according to the underlying purpose of the behavior. Hoarding behaviors were motivated by (1) a need for emotional aids, (2) disposing difficulties, and (3) collecting items related to special interests. Reasons for engaging in self-injurious behaviors were (1) an urge for sensory stimulation and (2) emotional regulation purposes. Discussion focuses on the underlying motives of the participants for engaging in these behaviors, in respect to current research knowledge. Relations to the general construct of Restrictive and Repetitive Behaviors and Interests are discussed along with implications for research and practice.
Lay abstract
Hoarding and self-injurious behaviors are relatively common in autism, but knowledge about their expressions in adulthood is scarce. Through interviews collecting subjective experiences of autistic adults, these behaviors were explored, and categorized to their underlying purposes. Findings portray the occurrence of these behaviors in the lives of autistic adults, their self-regulatory purposes, and their relationship to other behaviors in the domain of Restrictive and Repetitive Behaviors and Interests.
Keywords
Restricted and Repetitive patterns of Behavior, Interests, or activities (RRBIs) represent a core feature of autism, since the earliest conceptualization of the condition. RRBIs form a cluster of characteristics distinct from social and communication difficulties, comprising of various behaviors such as repetitive motor movements, ritualistic behavior, resistance to change, and fixed interests (Shuster et al., 2014). In an attempt to characterize and establish an overall construct of RRBIs, Turner (1999) categorized RRBIs into low and high-level behaviors; low-level behaviors include repetitive motor stereotypes (e.g. hand flicking and body rocking), repetitive actions (e.g. repetitive vocalizations), sensory seeking, and self-injurious behaviors (SIBs), whereas high-level behaviors include restricted interests, rituals, and significant resistance to change.
Examinations of relationships between low-/high-level subtypes and other variables show that autistic children who also have intellectual disability (ID) present with the highest prevalence of low-level RRBIs, specifically stereotyped behaviors and SIBs, while high-level RRBIs, such as insistence on sameness, were not related to the level of intellectual functioning (Esbensen et al., 2009). Although the low-/high-level RRBIs dichotomy is common in the literature, some assert that this classification may obscure important differences among the specific forms and functions of RRBIs in autism, and therefore should be used with caution, and validated across cultures and older age groups (Berry et al., 2018).
Evidence of changes in RRBIs across the life span is inconclusive. Most studies to date have examined RRBIs during childhood, with fewer studying RRBIs in adolescence and adulthood (see Barrett et al., 2018). Some studies, supporting the two-dimensional construct described above, suggest that low-level behaviors, such as repetitive sensory/motor behaviors and SIBs, might diminish with age, while high-level behaviors such as insistence on sameness are more stable (Barrett et al., 2018). Other studies, in which RRBIs were measured as a unidimensional construct, did not identify an overall decrease of RRBIs with age (Hattier et al., 2011). Therefore, due to limited research, inconclusive outcomes, and the possibility that adult experiences of RRBIs are quite different from those of children, more insight into RRBIs in autistic adults is required.
The American Psychiatric Association (2013) categorizes RRBIs into four sub-categories: (1) stereotyped or repetitive motor movements, use of objects, or speech; (2) insistence on sameness, inflexible adherence to routine, or ritualized behavior; (3) highly restricted, fixated interests, that are abnormal in intensity or focus; and (4) hyper- or hypo-reactivity to sensory input or unusual interests in environmental sensory input. In addition, hoarding and SIBs are both prevalent in autism (La Buissonnière-Ariza et al., 2018; Minshawi et al., 2014; Storch et al., 2016) and share characteristics and mechanisms with RRBIs.
SIBs are self-inflicted behaviors that have the potential to result in physical injury, such as hand-biting, skin-scratching, self-hitting, head banging, and others. Prevalence of self-injury in autistic individuals may be as high as 42% (Steenfeldt-Kristensen et al., 2020), substantially higher than non-clinical samples which range from 17% in adolescence to around 5% in adulthood (Swannell et al., 2014). Minshawi et al. (2014) found the incidence of SIBs is positively correlated with the severity of co-occurring ID and the severity of autistic symptomatology. Perhaps because of this association, most research to date has examined SIBs in individuals with ID, commonly focusing on children with the intention of understanding the function of these behaviors. Specifically, studies differentiate SIBs that are socially mediated (e.g. for communication purposes) and SIBs that are automatic, in which the behavior is self-reinforcing (Hagopian et al., 2015). Establishing sensitive models that map the different functions of SIBs can help promote personal modifications of clinical interventions to enhance their effectiveness (Hagopian et al., 2017).
In autism, SIBs are often considered to be part of the RRBI construct and can be conducted in a repetitive manner (Minshawi et al., 2014). For autistic children, SIBs have been related to sensory abnormalities, also in the RRBI structure (Soke et al., 2017). They are included in widely used RRBI scales (Bodfish et al., 2000; Lam & Aman, 2007), but are not addressed by others (Barrett et al., 2018). Supporting this relationship, atypical sensory processing, and insistence on sameness, both sub-categories of RRBIs, contribute to the occurrence of SIBs (Duerden et al., 2012; Esbensen et al., 2009). Thus, SIBs seem to share common mechanisms with other RRBIs such as repetition and regulatory purposes (Gal et al., 2009), but their inclusion as part of the construct is not fully substantiated.
Recent studies examining SIBs of cognitively able autistic adults (typically referred to as Non-Suicidal Self-Injury (NSSI)) (Maddox et al., 2017; Moseley et al., 2019, 2020) describe occurrences of self-harming behaviors in the absence of suicidal intent (Zetterqvist, 2015). Maddox et al. (2017) compared NSSIs of autistic and typically developing (TD) adults. According to their findings, 50% of the autistic adults reported having engaged in at least one episode of NSSI. This prevalence was high in comparison to TD college students, TD adults in the community, and autistic adolescents, all found to be around 20%. They further found that autistic and TD adults shared similarities in the time of behavior onset, perceived reasons for the behavior, and types of behaviors. In light of these findings, they conclude that SIBs of cognitively able autistic adults are not related to RRBIs and are distinct from the SIBs that are widely researched within the autism literature. Due to the preliminary nature of studies addressing NSSIs, the preferred term and construct remain unclear, and the suggested distinctions call for further clarification. For the purpose of this study, we will refer all forms of behavior leading to self-injury as SIBs, including those that might resemble NSSI.
Similar to SIBs, hoarding behaviors have also been strongly associated with autism (Storch et al., 2016), while not being part of the autism diagnostic criteria. Hoarding Disorder (HD) is defined as a persistent difficulty discarding possessions, resulting in accumulation that leads to significant distress and impairments in functioning (American Psychiatric Association, 2013). It was recognized in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) as a standalone diagnosis (Pertusa et al., 2019). An individual can be diagnosed with HD, without displaying obsessive compulsive disorder (OCD) symptoms such as obsessions or anxiety-related compulsions, although the disorder is still in the same section of obsessive, compulsive and related disorders (Morein-Zamir et al., 2014). Another behavior characterized by accumulating objects is “collecting,” considered to be a normal behavior involving purposeful acquisition of a narrow range of items. Collecting may have psychological or social benefits (e.g. membership to a club of people with similar interests), while behaviors that fall under the diagnosis of HD have negative consequences such as severely disorganized clutter, anxiety, and social withdrawal (Nordsletten & Mataix-Cols, 2012).
In relation to autism, Storch et al. (2016) studied a population of children diagnosed with autism and a co-occurring anxiety disorder or OCD, finding that 34% of participants displayed moderate to severe levels of hoarding. Similarly, La Buissonnière-Ariza et al. (2018) found clinically significant hoarding behavior present in 25% of children with autism and co-occurring anxiety disorder. These findings suggest a prevalence substantially higher than in the general population, which is estimated to be about 2% in childhood, increasing with age up to an estimated prevalence of 6% among adults aged over 70 years (Davidson et al., 2019).
Hoarding behaviors are addressed in measures of RRBIs, usually considered as a behavioral expression of restricted interests (Bodfish et al., 2000; Mayes, 2018). HD diagnostic criteria also indicate the possible occurrence of hoarding behaviors in relation to autism and associate them specifically with restricted interests. In fact, DSM-5 (American Psychiatric Association, 2013) HD criteria specifically state that if hoarding behaviors are better explained by the symptoms of autism, HD diagnosis is denied. These guidelines negate the possible co-occurrence of autism with HD. Along with this possible relationship between hoarding behaviors and special interests, underlying mechanisms for hoarding behaviors in autism may also include excessive attachment to objects, social isolation, and executive-functioning deficits. Thus, it remains unclear if hoarding behaviors in autism form a type of RRBIs related to special interests, portray a co-occurring set of behaviors, share common mechanisms with HD, or differ from them. Therefore, more research on hoarding behaviors in autism in general, and hoarding behaviors of autistic adults in particular, is needed.
An important source of information regarding the questions and research gaps raised is the subjective experiences of autistic adults. Firsthand accounts collected using qualitative methodology have been useful in understanding various aspects of autism over the life span (DePape & Lindsay, 2016). Previous studies examined experiences in adulthood such as reaction to a diagnosis (Punshon et al., 2009), employment (Flower et al., 2019; Hedley et al., 2018), seeking friendship (Sosnowy et al., 2019), and aging (Hwang et al., 2017). Qualitative inquiries of firsthand experiences can potentially highlight the subjective underlying motives for engaging in certain behaviors, specifically RRBIs. For example, Kapp et al. (2019) examined autistic adults’ views on stereotyped or repetitive motor movements known as “stimming,” emphasizing the adaptive purpose of these behaviors which were found to serve as self-regulatory mechanisms.
To our knowledge, the subjective experiences of autistic adults regarding SIBs and hoarding behaviors have yet to be examined. Therefore, the aim of this study was to expand our knowledge and understanding of these two understudied behaviors, through firsthand accounts of autistic adults. Our research was driven by two broad questions: (1) “How do autistic adults experience SIBs and hoarding behaviors in their lives?” and (2) “How do they make sense of these experiences?”
Method
Participants
A purposeful sampling method was employed whereby participants were selected based on their willingness to share information about RRBIs (i.e. “the phenomenon”; note that participants were contacted regarding RRBIs in general, not specifically hoarding behaviors and SIBs) through personal experiences (Creswell, 2007). Criteria for inclusion were as follows: (1) formal diagnosis of autism spectrum disorder (ASD) by a psychiatrist or a psychologist, based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) or DSM-5 criteria (American Psychiatric Association, 1994, 2013) and (2) sufficient verbal ability to engage in an interview. Ten adults participated in the study (five females), aged 18–54 years. The study was conducted in Israel, and all of the participants were Israeli. Age of diagnosis ranged between 3 and 52 years. Participant demographic information is provided in Table 1. Pseudonyms are used to preserve anonymity.
Participants’ demographic data.
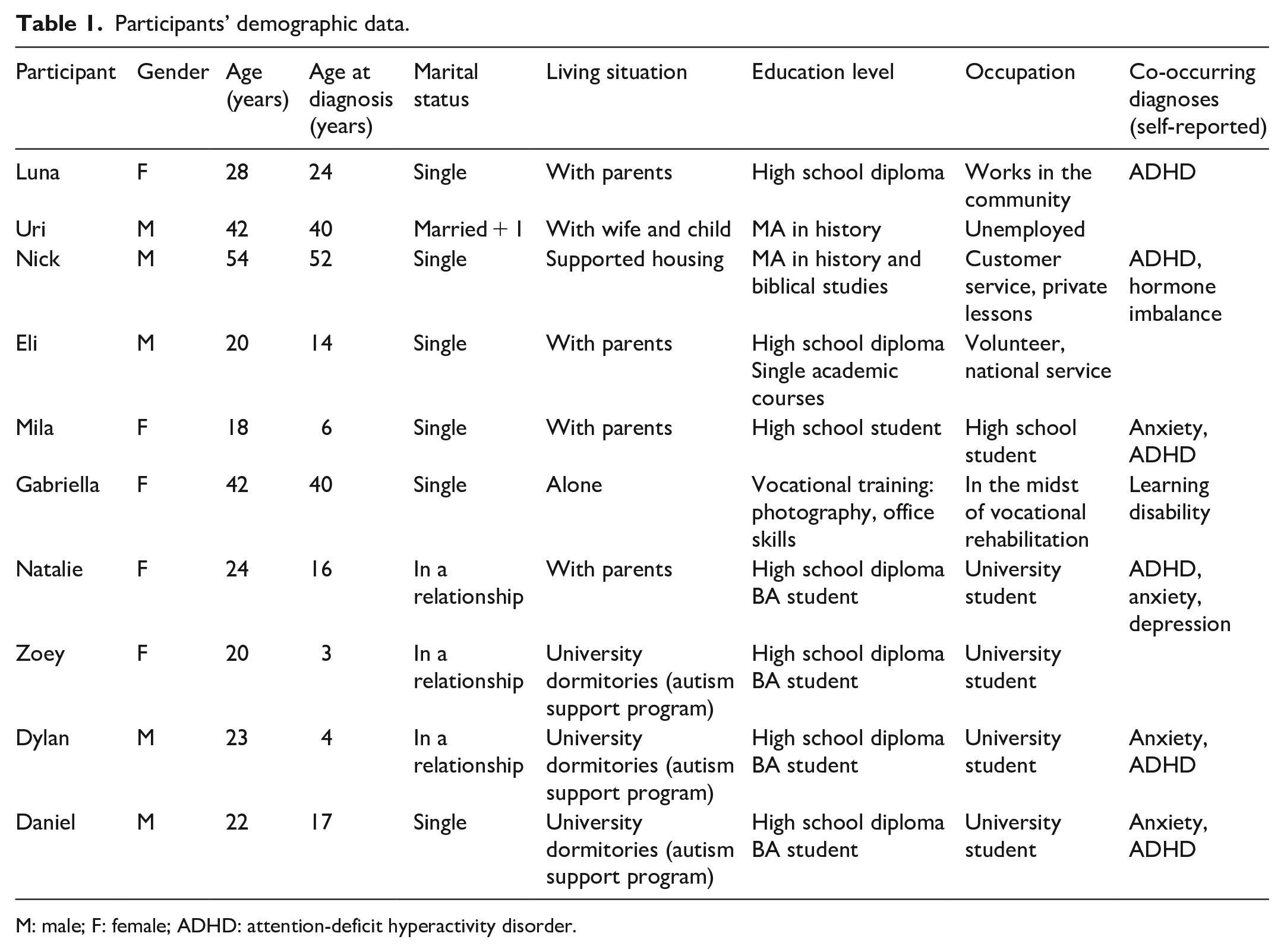
M: male; F: female; ADHD: attention-deficit hyperactivity disorder.
Procedure
This study was part of a broader research addressing subjective experiences of RRBIs portrayed by autistic adults. All procedures were approved by the last author’s university institutional review board (IRB). An invitation to participate in the study was published in social media and through organizations offering services to autistic people. The researcher also contacted autistic people who are authors of blogs or actively participate in social media, and openly share their diagnosis. Prior to the interview, a short telephone conversation with the interviewer was conducted, providing information about the study and assuring confidentiality. Active screening or selection was not performed by the researcher following the telephone conversation; interviews were scheduled with all willing participants. All of the participants signed informed consent forms.
Interviews were conducted by the second author, an Occupational Therapist with extensive experience working with autistic people. Prior to the interview, participants filled out a demographic questionnaire and completed the Repetitive Behavior Scale–Revised (RBS-R; Bodfish et al., 2000), a self-report questionnaire consisting of 43 items that describe RRBIs commonly reported by autistic people. The questionnaire was meant to serve as a probe, raising awareness of the participants to possible experiences of RRBIs in their lives, and to assist the researcher in asking relevant questions anchored in specific concepts and stories. This procedure was chosen due to possible difficulties autistic people may have when replying to open-ended questions or processing information in real time (Nicolaidis et al., 2019).
After completing the questionnaires, in-depth interviews were conducted, lasting approximately 90 min each. The initial part of the interview included open questions, followed by more specific and targeted questions (Appendix 1). Interviews were audio-recorded and transcribed verbatim. Out of the full breadth of behaviors shared by the participants in the interviews, this study focuses on the specific information regarding SIBs and hoarding behaviors, which emerged as prominent themes.
Data analysis
The study utilized an interpretive phenomenological approach, aimed at understanding participants’ experiences of RRBIs, including SIBs and hoarding, in their everyday lives, and how they make sense of these experiences (Creswell, 2007). A thematic analysis was conducted identifying categories and major themes in the data (Howard et al., 2019). At the first stage of analysis, data were coded according to themes arising from the text, identifying patterns that were repeated across participants. The themes were then clustered into a list of superordinate and sub-themes. Data were re-reviewed according to the identified themes, assigning relevant quotes and excerpts in order to validate the identified patterns (Howard et al., 2019). Several measures were taken to enhance the reliability of the study: a detailed, trackable description of the process, including citations from the original text (Higgs et al., 2009); a reflective diary sketched by the researcher, documenting her thoughts and feelings and their impact on study process and conclusions, in order to identify potential bias (Howard et al., 2019) acknowledging that the interviewer is neurotypical, as are the other authors. Autistic people or other community stakeholders were not actively involved in the implementation of the study. A review of the categories and coding themes was carried out by the first and second authors. Themes were discussed until agreement was achieved regarding the categories.
Results
As part of the broader research addressing subjective experiences of RRBIs, participants portrayed a wide variety of behaviors, clustering into themes consisting of different types of RRBIs. Emerging themes aligned with the four clusters of the RRBI definition in DSM-5: repetitive behaviors, insistence on sameness, special interests, and unusual sensory processing. Two additional themes emerged from the data: SIBs; and collecting and hoarding. Out of the full scope of the data collected, SIBs and hoarding behaviors were chosen as the focus of this article. Further analysis of these themes revealed sub-categories, each describing different reasons and motivations for engaging in these behaviors. Table 2 specifies the different categories and representative quotes.
Categories and examples of RRBIs.
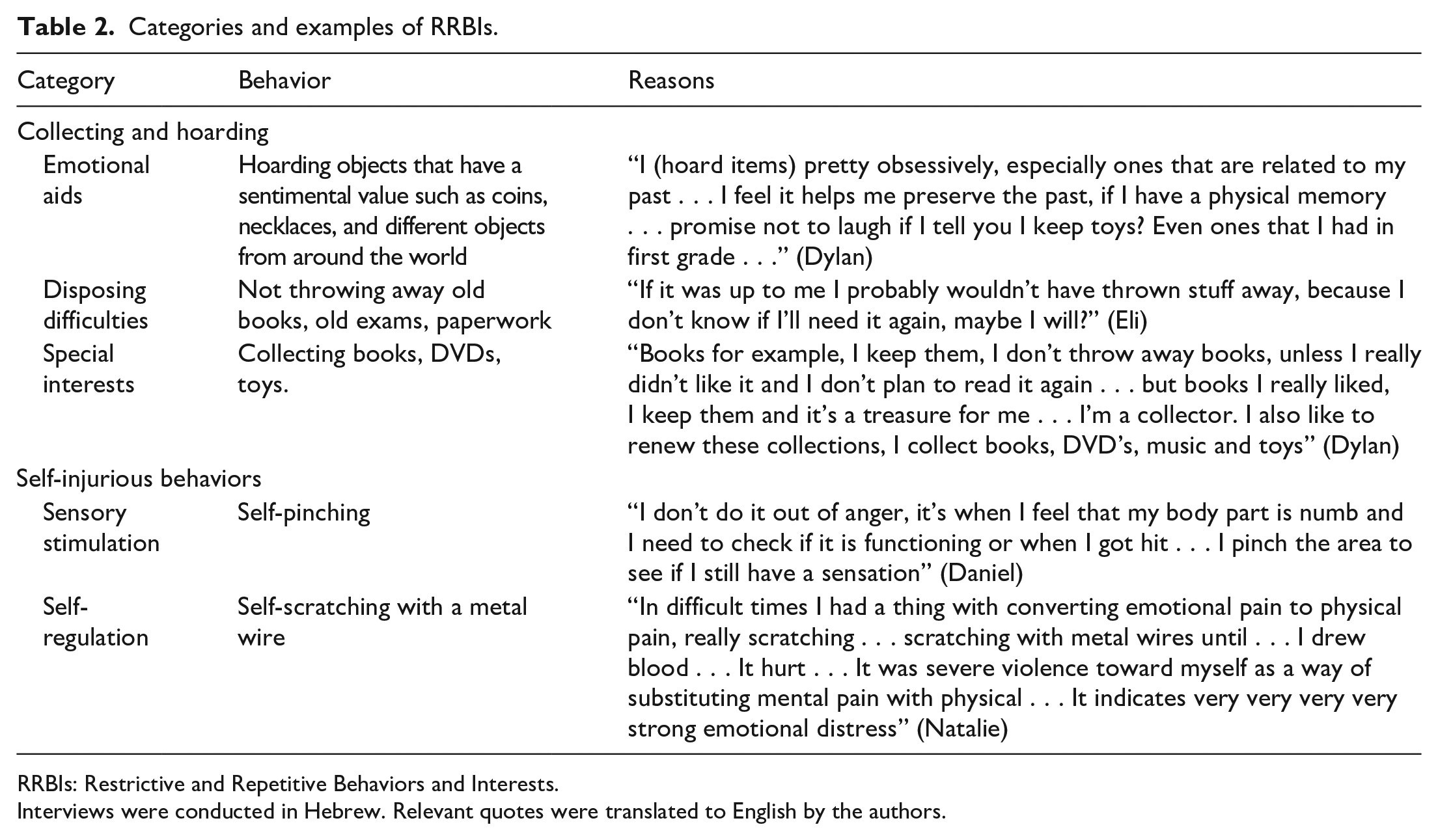
RRBIs: Restrictive and Repetitive Behaviors and Interests.
Interviews were conducted in Hebrew. Relevant quotes were translated to English by the authors.
Theme 1: collecting and hoarding objects
Many behaviors of accumulating objects were described, shared by nine out of ten participants. Participants used the terms “collecting” and “hoarding” interchangeably, and are quoted according to their chosen term, without implying the intensity or severity of the behavior in respect to a clinical diagnosis. Some of the examples given were as follows: accumulating boxes of papers, books, old drawings, used pens, learning materials and notebooks, childhood toys, and unused music sheets. Participants expressed difficulties discarding items, “keeping everything that isn’t plain trash” (Natalie), and also shared the feeling that the need to discard items is accompanied by considerable discomfort (e.g. when moving to a different apartment). This general category was further sub-categorized according to different motives, reasons, and meanings given by the participants to these behaviors:
Behaviors that serve emotional needs
In this sub-category, participants described collecting and hoarding behaviors that help support the need for sameness, familiarity and well-being, or function as a souvenir that may hold significant emotional value, such as drawings and old presents. A unique relationship and attachment to objects was associated with the need to keep and collect them, promoting a sense of comfort and security: I am more attached to objects than people . . . even though I can be very friendly . . . objects give me a sense of security . . . they are altogether more predictable than people, you can know how they will react . . . and they are always there, available, you don’t need to chase them . . . they will go anywhere with me. (Zoey) Hoarding is often a matter of security. It gives me confidence that I am surrounded with areas that I have control over, and I am surrounded with things which I feel tightly connected to . . . I have this net of energy, a web of memories, an emotional web that can be manifested through objects. (Daniel)
Along with the positive feelings described, objects were sometimes given symbolic, even spiritual meanings: If it’s collections, it’s a matter of comfort and security . . . for me it’s a horcrux [a magical object from Harry Potter books]. You take an object, or a song, and you hide a part of your soul . . . a certain physical or mental state . . . this amulet for instance, it hasn’t come off my neck since I was . . . I give it a symbolic meaning, it holds my soul, emotions, energy. (Daniel)
Several participants mentioned they collect and hoard as a mean of preserving memories from the past: There are many things I am attached to . . . because they are somehow a physical presence for abstract values . . . I need it for keeping the memory . . . it will be difficult to extract the memory without engaging with the item . . . even looking at it, I feel like a non-existing hand touches it and it generates a flash of a memory . . . up to a level I can obsess about finding these objects. (Dylan)
As vividly portrayed in the above quotes, objects hold different meanings for the participants. The objects serve an emotional purpose such as a sense of security and a key to past memories and experiences.
Difficulty discarding of objects
In this sub-category, participants described keeping daily items that were no longer functional, not necessarily ones that had personal significance or value. Examples given were old bus tickets, broken pens, and old documents. Zoey explained that “you can never know when you will need things—that’s why I keep them.” Some of the participants also acknowledged the possible problematic aspect of these behaviors, stating that at times, external intervention is required, and only someone else can throw away these items. Gabriella shared her thoughts about the habit of collecting old papers and documents: The worst thing about me, is that I hoard . . . I know I can potentially be organized and not hoard, right? So the house won’t look like a storage room . . . I just don’t pay attention . . . there are many documents that piled up five years, ten years ago. I keep them. One day I’ll deal with it . . .
Zoey also expressed her difficulty discarding of items, even though the chances she would reuse them were very slim: I might need it sometime . . . even the pens that are out of ink . . . maybe sometime they will have ink . . . even though, actually, they won’t have . . . [do you throw them away?] not until my mom tells me to . . . it’s difficult . . . only after I convince myself I won’t use it anymore I can allow myself to throw it away. I usually need the help of someone else in order to give things away.
Difficulty discarding of objects that have no clear worth or value is noticeable from the participants’ experiences. The participants’ accounts include descriptions of cognitive processes such as difficulties attending to clutter, prioritizing the activity of disposing of unnecessary items or foreseeing future needs and actions.
Items that relate to special interests and hobbies
Some of the participants shared behaviors of collecting items that are related to areas of interest such as comic books, cameras, learning materials, old coins, and music. While these behaviors were mentioned, they were the least common among the given reasons for hoarding behaviors. Gabriella, who has a special interest in photography, described strong feelings relating to her object of interest: I am very possessive of my camera. I even have recurring nightmares about it . . . it’s also because I’m autistic . . . and also because three years ago I placed it in the back of a car I was in, and it was stolen. I am still traumatized from the possibility that someone will steal my camera.
While behaviors of collecting and hoarding of items related to special interests were mentioned by several of the participants, they were relatively brief and descriptive.
Theme 2: SIBs
Half of the participants described current and past SIBs. Although prevalence is lower than that of other RRBIs, disclosures of SIBs were very meaningful in light of the possible harmful implications of the behavior, the severity of distress caused, and the profundity of the insights shared by the participants. Examples included behaviors such as self-hitting (sometimes with an object), scratching till bleeding, pinching, and vomiting. Participants described two main motivations underlying their SIBs: sensory stimulation and self-regulation.
Sensory stimulation
Participants described an elevated pain threshold, or a different perception of pain so that SIBs were experienced as activating, awakening, and providing intense physical sensation that is sometimes needed. Luna described a need for intense pressure in a very specific moment, and she used a paper clip or a drawer door to fulfill the need. She emphasized that it did not hurt—thus she described a high pain threshold; however, she was aware that for others this action would be perceived as painful: My mom thought we should have this checked . . . . now she’s less concerned, she’s even laughing about the clips. It’s just that I needed this pressure right now. Or needing to close the drawer on my hand. It doesn’t hurt, I just feel that I need it, don’t even know why.
Natalie described SIBs that help her elicit body sensations and physical awareness. Not only is the act of deeply scratching her skin not painful, but it is also physically rewarding: I scratch my back hard . . . my boyfriend he doesn’t understand how it doesn’t hurt! There are times when at night I’ll scratch hard and I’ll see him the next day and he’ll ask—what are all these scratches? And I’m like, what? I have scratches on my back? And he will take a picture just to show me what I did. It’s fine, I’m used to it, I didn’t feel pain so I don’t have a problem with it . . . I scratch really deep and hard . . . because otherwise I don’t really have a sensation . . . the pain is what tells me to wake up.
Self-regulation
Participants portrayed behaviors that were meant to regulate unbearable distress, either emotional or sensory. Participants acknowledged that the behaviors are considered to be destructive and, as a result, the need to reduce them, and their efforts to do so. Daniel mentioned situations of high anxiety accompanied by physical, emotional, and sensory stimuli: I attack myself with an object or with my bare-hands. I usually do it so that I don’t hurt other people when I’m in a state of anger or intolerable anxiety . . . it happens after panic attacks . . . the whole body trembles, I’m suffocating, can’t breathe . . . higher awareness to sounds and vision . . . and there are other moments of detachment from the environment.
Dylan describes a behavior of self-hitting with an object, in the head or the stomach. He suggests this behavior is an attempt to elicit self-control in situations involving difficulties in sensory, emotional or behavioral regulation: It happens when I feel frustrated, or when I feel atomic pressure inside my head, when things go out of control or I feel I did something inappropriate, or when I fail . . . the physical pain might be a way to screen out the mental pain, I know how to deal with physical pain . . . I hate failing, it makes me hostile towards myself . . . because I can’t stand myself at that moment . . . it’s a maladaptive attempt to find a way to communicate with myself.
Natalie also described vomiting as a form of SIB that helps her regulate negative emotions, with the benefit of the injuries being internal, and remain undetected by others: I don’t do it often because it is perceived by others as strange, but if I feel bad, or don’t want to deal with something it seems to me like a great solution because vomiting soothes the whole system . . . it’s like an internal self-injury . . . and it’s easy because I don’t see the injury that I’m causing myself, so why not?
Disclosures of the participants in relation to SIBs provide some striking examples of these behaviors and the thoughts and feelings that accompany them. Along with acknowledgment of their harmful consequences, they hold personal purpose underlying benefits that are important in understanding and attending to these behaviors.
Discussion
The study examined experiences of hoarding and SIBs that were shared by autistic adults from Israel, offering rich portrayals that illuminate the diversity of their characteristics and the various motives underlying them. These firsthand experiences are fundamentally important as a basis for understanding these unique behaviors in adulthood.
Hoarding behaviors
Hoarding behaviors were reported by most of the participants in this study. Some regarded themselves as “collectors” and others as “hoarders,” but the extent to which the behaviors described meet the criteria for HD or influence functioning cannot be determined from our study. Generally, we found that participants did not report significant distress due to these behaviors, or significant impairments in functioning deriving from them. Demographic information revealed that the majority of the participants were living with other people. Perhaps, the presence of a third party reduced the negative consequences of hoarding behaviors by supporting actions of sorting objects and discarding them, and actively minimizing clutter. Nevertheless, the detailed experiences highlight the functional and emotional meanings hoarding behaviors have in the lives of autistic adults, and offer insight into their underlying mechanisms and purposes.
The HD diagnosis refers to the behavior of accumulating objects as a result of difficulty discarding possessions, without specifically addressing the types of objects or the reasons for their accumulation. The DSM-5 (American Psychiatric Association, 2013) HD diagnostic criteria state that hoarding behaviors that are related to autism, specifically to circumscribed areas of interest, should be differentiated from an HD diagnosis. While our findings support the notion that autistic people may excessively acquire or retain possessions that correspond to their special interests (Pertusa et al., 2012), autistic adults may also engage in hoarding behaviors for additional reasons.
The most prominent experience shared by the participants in relation to hoarding behaviors was an emotional attachment to physical objects. While it is reasonable to assume that in the general population possessions commonly hold sentimental value, the intensity and vividness of the descriptions in this study suggest that there might be greater emotional significance to collecting and retaining objects for autistic people. In support of this finding, Skirrow et al. (2015) proposed that for this population, collecting and hoarding behaviors serve the need for a sense of continuity over time. They suggest that autistic people may hoard items that help them “code” autobiographical memory and form an integrated “sense of self” over time. While this notion is not widely studied, it aligns with experiences described in this study, which highlight the role of physical objects in maintaining memories.
Difficulties disposing of possessions were revealed, apart from their value, necessity, or relation to a topic of interest. These behaviors are considered central to the core diagnosis of HD. Looking into the participants’ articulation of these experiences, cognitive difficulties were commonly reported. Participants expressed difficulty planning the future, not knowing if and when an item might be needed, and being unable to prioritize activities, leading to procrastination of the act of discarding of items. Such executive-functioning difficulties have been suggested to contribute to the co-occurrence of autism and HD in youth (Zaboski & Storch, 2017) and seem to surface through the experiences of adults in this study as well. Possible similarities between the manifestation of hoarding behaviors in HD and autism emerge from the data, rather than a discriminant approach.
SIBs
Considerable experiences of SIBs were described by the participants. Participants discussed their awareness of these behaviors and underlying motives, including an urge for sensory stimulation and response to severe emotional stress. Our findings are consistent with Moseley et al.’s (2019) findings concerning SIBs of cognitively able autistic adults (referred to as NSSIs), suggesting that the most common self-reported functions of these behaviors were regulating affective states and self-punishment. The regulatory purpose vividly portrayed in this study is also consistent with previous findings that SIBs are linked to anxiety and may reflect maladaptive coping strategies (Kerns et al., 2015). Whether these behaviors are considered part of the core symptoms of autism or a common co-occurring condition, they often lead to possible negative consequences, physical, emotional, and social (Maddox et al., 2017; Moseley et al., 2020).
The purpose of sensory stimulation expressed in this study, as well as in Moseley et al.’s (2019) findings, suggests a positive relationship between sensory under-responsivity and SIBs. Additional studies associate SIBs with atypical sensory processing (Duerden et al., 2012), supporting our participants’ reported experiences of these behaviors as serving to increase body awareness. Atypical reaction to pain was oftentimes documented in the literature (Duerden et al., 2015) and includes qualitative studies whereby autistic people cite very high pain thresholds (Elwin et al., 2012). In this study, under-responsiveness to pain was mentioned in relation to self-inflicted injuries (contrary to uncontrolled environmental sensory stimuli). Thus, having a sense of control might play a role in the often-contradictory reactions of autistic individuals to sensory stimuli in general, and specifically to pain.
Hoarding and SIBs in relation to RRBIs
As detailed above, hoarding and SIBs are often related to RRBIs, but do not form part of the autism diagnostic criteria. Data in this study tentatively suggest a relationship between these behaviors and current RRBI categories, and subsequently their relationship to one another, broadening the scope and adding other elements that should be considered when evaluating RRBIs. Previous research has reported a relationship between restricted and repetitive behavior and self-injury in autistic children and adults (Gal et al., 2009; Richards et al., 2017). While these were considered low-level RRBIs associated with ID (Esbensen et al., 2009), the current results demonstrate their occurrence in cognitively able adults, thereby supplementing our understanding of the presentation of RRBIs and self-injury in this specific group.
Along with the recognized relationship between hoarding and special interests, our data suggest that collecting objects may serve the “need for sameness” by providing a familiar and consistent surrounding. Objects are described as offering a reliable safety net in an unreliable world. Hoarding severity was found in previous studies to be positively correlated with intolerance for uncertainty (Wheaton et al., 2016), which is also known to play a central role in RRBIs, specifically, mediating the need for sameness (Wigham et al., 2015).
Strengths and limitations
Information shared in this study sheds light on the phenomena of hoarding behaviors and SIBs of autistic adults that, to date, have gained relatively less attention in the literature. The qualitative approach uncovered the participants’ experiences of hoarding and SIBs in the context of their natural occurrence in everyday lives, illuminating various aspects and purposes of these behaviors, and offering an in-depth portrayal of these phenomena. The high level of insight was possible due to the verbal abilities of the participants, mostly being cognitively able and educated adults. Although the existence of hoarding behaviors and SIBs was not a specific criterion for enrolling in this study, the many reports of these behaviors are striking and support further attempts to assess their prevalence in a broader autistic population.
The study includes a relatively high ratio of females, which does not represent the current gender distribution in autism. Given the growing body of evidence suggesting that a female phenotype of autism might be different from the male phenotype, the high ratio of females in this study might have affected the kinds of experiences shared. Gender differences in the general structure of RRBIs are inconsistent across studies (Barrett et al., 2018; McFayden et al., 2019), but some suggest that hoarding and SIBs are more prevalent in autistic girls, distinguishing them from autistic boys, who display heightened stereotyped behaviors and restricted interests (Antezana et al., 2019). The relatively high representation of females in this study may have contributed in highlighting behaviors that were overlooked in previous studies.
The sample of this study is small and relatively homogeneous (i.e. includes autistic people who are cognitively able). Findings are therefore limited in scope, and may not represent the experiences of the wider autistic population. Specifically, experiences and functions of the behaviors in non-verbal and less cognitively able populations may be very different; therefore, research among autistic adults with ID is necessary in order to compare and validate the results. Nonetheless, our findings point to important directions for further examination among diverse populations and more representative samples, also using quantitative methods to validate and generalize the preliminary findings revealed in this study.
Implications and future directions
The study supplements a growing body of research collecting subjective perspectives of autistic people, allowing us to learn from their experience and inform research and practice. Although transferability to other populations is limited due to the nature of the study design, the extensive portrayals of hoarding and SIBs, together with previous data, suggest these behaviors are prominent in the lives of autistic adults. Implications for daily life are notable; we suggest hoarding and SIBs should be considered during clinical evaluations of autistic adults.
Hoarding behaviors can cause impairment and distress in everyday life, and should be assessed thoroughly. An initial evaluation of their occurrence and possible maladaptive consequences is necessary in order to assess if there is a need for clinical intervention. If hoarding behaviors do not have negative implications for the individual’s everyday life, emotional well-being, or relationships with others, clinical intervention may not be needed. In circumstances that do call for clinical intervention, understanding the underlying reasons of the behavior can indicate the most suitable approach to treatment. Specifically, acknowledgment of the self-regulatory purpose of the behavior suggests careful attention should be paid to behaviors that could be substituted for alternative, more adaptive behaviors, rather than eliminated. Specified treatments have been found to be effective for HD (e.g. Cognitive Behavior Therapy; Pertusa et al., 2019). These include psychoeducation regarding the possible negative consequences of hoarding and behavioral strategies offering guidance on how to distinguish between what should be kept and what should be discarded. Accommodations of treatment approaches for hoarding behaviors of autistic individuals should be considered and further validated.
In order to avoid negative responses, some RRBIs, including SIBs, are actively concealed by the individuals engaging in them. Self-aware autistic adults may not reveal their distress, or their way of dealing with it, even to family members, and might prefer to engage in behaviors that are less apparent, like vomiting. Thus, information provided by parents may be incomplete, and SIBs might be less inclined to surface in research or clinical encounters. Due to their potentially detrimental effects, careful attention should be paid to the possible occurrence of these behaviors, regardless of the subjective feelings of self-injury as a positive or neutral behavior. This calls for clinicians who provide services to autistic individuals to ask direct questions and encourage disclosure about potentially harmful behavior. Alternate coping strategies can address the urge for sensory stimulation or severe distress without leading to self-harm. It is important to ensure that autistic adults have means of meeting their emotional needs, other than with maladaptive or potentially harmful behaviors.
Further research should expand the understanding of overarching similarities in hoarding and SIBs of autistic people who present different levels of cognitive ability. Attributions of behaviors to the autism diagnosis may overshadow a more comprehensive understanding of their occurrence. This could be the case for hoarding behaviors that are automatically attributed to special interests, thus not considering possible cognitive deficits that may underlie the maladaptive behavior, or failing to suggest effective HD treatments. Similarly, attributing SIBs to RRBIs may disguise the possibility of suicidal intent, that calls for urgent attention (Hedley et al., in press). The heterogeneity of autism characteristics, along with common co-occurring conditions, makes efforts to establish clearer constructs and conclusions especially challenging. Ongoing research to expand knowledge in this area should include self-report measures and avoid depending solely on reports from informants other than the individual. Given the limited scientific knowledge about hoarding behaviors and SIBs in autistic adults, further research is necessary, in order to develop sensitive diagnostic tools, validate diagnostic criteria, and inform practice that will improve functioning and well-being of autistic adults.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the institutional ethics committee, University of Haifa.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.