
Abstract
This study explores autistic women’s experiences of eating disorder services. Estimates suggest that 20%–30% of women in treatment for anorexia nervosa display diagnostic features characteristic of autism. Research suggests that autistic individuals’ needs are not being met by standard anorexia nervosa treatments. In the current study, in-depth interviews were conducted with 15 autistic women with experience of anorexia nervosa, 12 parents of autistic women with anorexia nervosa, and 11 eating disorder healthcare professionals. Using thematic analysis, three overarching themes were identified: misunderstanding autism and autistic traits, one treatment does not fit all, and improving accessibility and engagement within services. We found that there were diverse barriers facing autistic women when in treatment for anorexia nervosa, and these were accentuated by a lack of autism understanding within eating disorder services. Future research should focus on developing interventions that are tailored to the specific needs of autistic individuals with anorexia nervosa.
Lay Abstract
This study explores autistic women’s experiences of eating disorder services. About 20%–30% of people with anorexia nervosa are also autistic, and current treatments seem not to work as well for them. We interviewed 15 autistic women with experience of anorexia nervosa, 12 parents of autistic women with anorexia nervosa, and 11 healthcare professionals working in eating disorder services. We asked autistic women and parents about their experiences of eating disorder services, and we asked healthcare professionals about their experiences treating autistic women with anorexia nervosa. Participants’ views were represented by three overall themes: misunderstanding autism and autistic traits, one treatment does not fit all, and improving accessibility and engagement within services. We found that autistic women face many barriers when in treatment for anorexia nervosa, often because of a lack of autism understanding within eating disorder services. Future research should look at developing anorexia nervosa treatments that can specifically help autistic individuals.
Introduction
Anorexia nervosa (AN) is an eating disorder (ED) characterised by a significantly low body weight, fear of weight gain or persistent behaviour that interferes with weight gain, and a disproportionate influence of weight and shape on self-evaluation or a lack of recognition of the seriousness of own low weight (American Psychiatric Association, 2013). Co-occurrence of AN and autism is well established, with estimates of 20% to 30% of women in treatment for AN displaying diagnostic features characteristic of autism (Westwood & Tchanturia, 2017). This is a significant overrepresentation; approximately 1% of the general population are diagnosed with autism, of whom 0.2% to 0.3% are female (Baron-Cohen et al., 2009; Loomes et al., 2017). Moreover, evidence suggests that autistic traits are more generally elevated in AN populations. Individuals with AN scored significantly higher on the Autism Quotient (AQ; Baron-Cohen et al., 2001) and its shortened counterpart, the AQ-10 (Allison et al., 2012), than those without AN (Westwood et al., 2016).
It has been argued that the cognitive, social and behavioural deterioration associated with being in a state of starvation may mimic autistic traits, which resolve once weight is restored (Treasure, 2013). Furthermore, there have been mixed findings in adolescent populations. One study found little evidence to support the presence of autistic traits in adolescents with AN (Postorino et al., 2017), although it should be acknowledged that an earlier meta-analysis did find that autistic traits are elevated in young people with AN (Westwood et al., 2016). It is notable that several studies support the idea that the elevated rates of autism and autistic traits in ED populations cannot simply be considered a ‘phenocopy’ resulting from starvation. First, recent longitudinal research found that autistic social traits in childhood were a predictive risk factor for subsequent disordered eating in adolescence (Solmi et al., 2021). Second, studies that rely on retrospective reports of autistic symptoms, before the onset of starvation, continue to find high rates of autism and autistic traits in people with EDs (e.g. Vagni et al., 2016). Third, elevated autistic traits and high rates of autism are present in individuals recovered from AN compared to healthy controls (Bentz et al., 2017; Dinkler et al., 2019), suggesting that the autistic traits observed in some women with AN may represent ‘true’ autism as opposed to a pseudo-autistic state.
AN has the highest mortality rate of all psychiatric conditions (Arcelus et al., 2011), so access to effective treatment is paramount. However, high relapse rates in AN suggest that, long-term, treatment is often unsuccessful (Khalsa et al., 2017). Qualitative studies investigating patient experiences in the United Kingdom are often critical of ED services (Colton & Pistrang, 2004; Fox & Diab, 2015; Offord et al., 2006; Rance et al., 2017; Smith et al., 2016). Overarching themes across these accounts include: a lack of flexibility in treatment, for example, time-constrained sessions with a narrow focus on food and weight; the importance of the clinician–patient relationship; being seen as an individual rather than an ‘anorexic’; and the role of peers in treatment, which can be both helpful and detrimental in recovery.
Research suggests there is a need for better autism understanding within healthcare services (Tint & Weiss, 2018). Indeed, autistic adults face many barriers when accessing mental health services (Crane et al., 2019). Qualitative evidence suggests that autistic women have autism-specific factors underpinning their AN (Brede et al., 2020; Kinnaird et al., 2019), so their service needs will likely differ from those without autism. For example, common treatment approaches addressing body image and weight concerns, such as, ED-focused cognitive behavioural therapy (CBT-ED; Fairburn, 2008) may be unsuitable for autistic women, as they report these factors play less of a role in their AN (Brede et al., 2020).
One qualitative study has investigated ED service experiences from the perspective of autistic individuals, with a focus on treatment adaptations. Kinnaird et al. (2019) interviewed 13 participants in treatment for AN with an autism diagnosis (N = 9) or presenting with high levels of autistic traits (N = 4). Participants reported that current ED treatments did not meet their needs and that adaptations were required to provide adequate care. Kinnaird et al. (2017) also interviewed nine clinicians from the same ED service about their experiences working with autistic individuals. Clinicians reported lacking experience and confidence treating autistic individuals with AN. Finally, carers of autistic women with AN reported a lack of support for co-occurrence of autism and AN in ED services and emphasised the importance of treatment adaptations (Adamson et al., 2020).
While Brede et al. (2020) explored the theoretical underpinnings of the development of AN in autistic women, the current study aims to explore autistic women’s experiences of ED services. It therefore builds on the fundamental groundwork laid down by Kinnaird et al. (2019), Adamson et al. (2020) and Kinnaird et al. (2017) by using a multi-perspective approach to further investigate autistic women’s experiences in a larger, independent sample from across the United Kingdom. We expand on their findings in three key ways: first, by including the perspectives of three stakeholders – namely autistic women themselves, parents of autistic women and healthcare professionals (HCPs) with experience working with autistic individuals in ED services – in one analysis, thereby utilising an efficient and streamlined approach; second, by ensuring the autistic women we interview all have a formal autism diagnosis, differing from Kinnaird et al. (2019)’s sample; and third, by utilising more extensive, in-depth interviews.
We utilised data source triangulation (Carter et al., 2014) to achieve a more rounded understanding of autistic women’s ED service experiences. Given that our overarching aim was to understand the experience of the autistic women, we positioned the autistic women with AN as the central thematic voice in our analysis. In doing so, we aim to substantially add to an evidence base that can inform service provision for autistic women. This research takes a participatory approach (Cornwall & Jewkes, 1995) via collaboration with two autistic advisors with lived experience of AN throughout the research process. A participatory approach is advocated particularly in autism research to ensure relevance to the affected community, sensitive and ethical conduct of the research, and to enhance the quality of data collected, analysis and communication of findings (Fletcher-Watson et al., 2019).
Method
Participants
We recruited three participant groups from across the United Kingdom: autistic women with experience of AN, parents of autistic women with experience of AN, and ED HCPs. Data collection was intended to serve two different but related studies, and all participants in this study overlap with the sample in Brede et al. (2020). Two autistic women and one parent were excluded from the final analysis as they/their daughter scored below the cut-off on the 10-item Autism Spectrum-Quotient (AQ-10; Allison et al., 2012). Researchers regularly reflected on the emerging data and recruitment stopped once we estimated that we had reached data saturation (Guest et al., 2006). Our final sample included 15 autistic women, 13 parents and 11 HCPs. Participants were recruited via social media (Twitter and Facebook), Autistica’s Discover network, our online blog (www.sedaf18.blogspot.com) and via existing contacts.
Autistic women
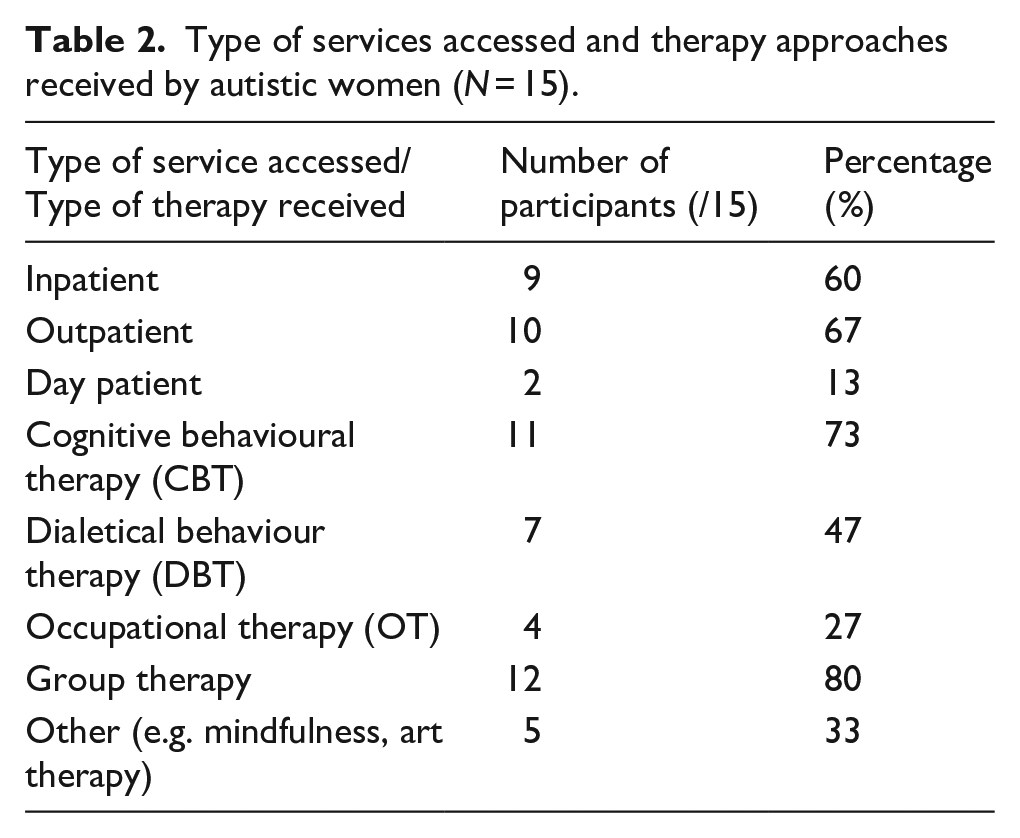
The inclusion criteria for autistic women were as follows: (1) above the age of 18, (2) clinical diagnosis of an autism spectrum disorder, and (3) past or current experience of AN. Participants were asked to confirm that they met these criteria prior to being recruited to the study. Participants were asked for more details on their autism and AN diagnostic experience during the interviews, and all participants accounts were consistent, giving researchers no reason to doubt the authenticity of their diagnostic status. Demographics are in Table 1. Notably, the average age of autism diagnosis was 12 years higher than the average age of AN diagnosis. ED status was varied at the time of study – some considered themselves recovered, while others reported that they were still living with an ED. All women reported having received ED treatment. Reported service types accessed and therapeutic approaches received are in Table 2.
Demographics for autistic women with experience of AN (N = 15).
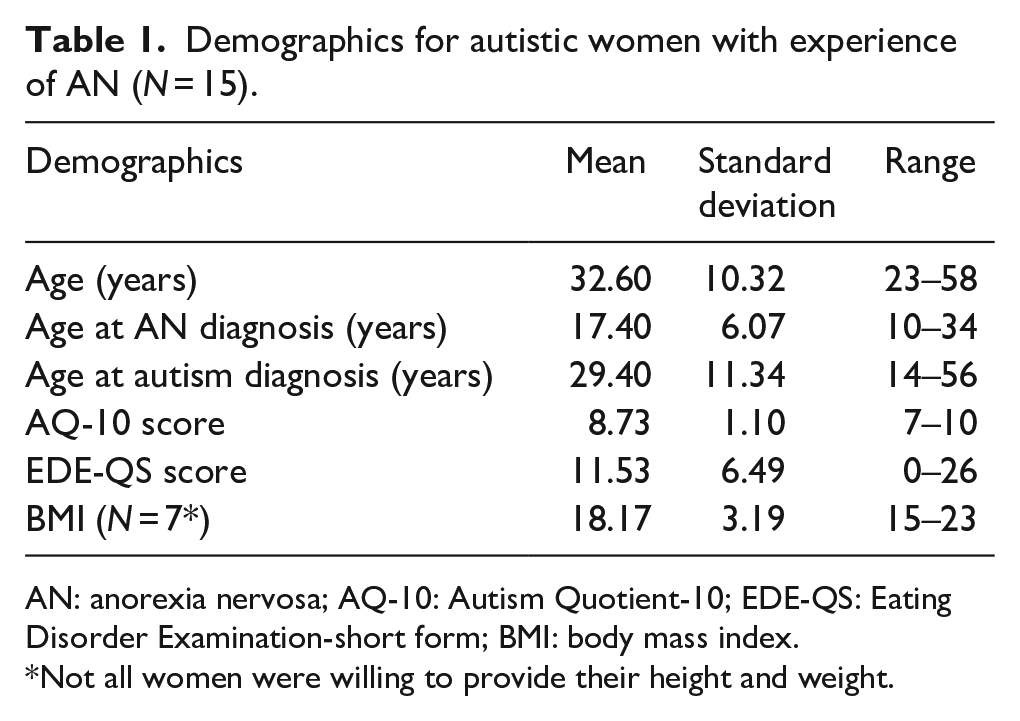
AN: anorexia nervosa; AQ-10: Autism Quotient-10; EDE-QS: Eating Disorder Examination-short form; BMI: body mass index.
Not all women were willing to provide their height and weight.
Type of services accessed and therapy approaches received by autistic women (N = 15).
Parents
The inclusion criteria for parents were as follows: a daughter with both (1) a clinical diagnosis of autism spectrum disorder and (2) current or past experience of AN. We included parents with a daughter under 18 years old. Five parents’ daughters participated in the autistic women group of this study. All parents interviewed were mothers, except for one interview where both mother and father were interviewed together. See Table 3 for demographics.
Demographics for parents of an autistic daughter with experience of AN (N = 13).
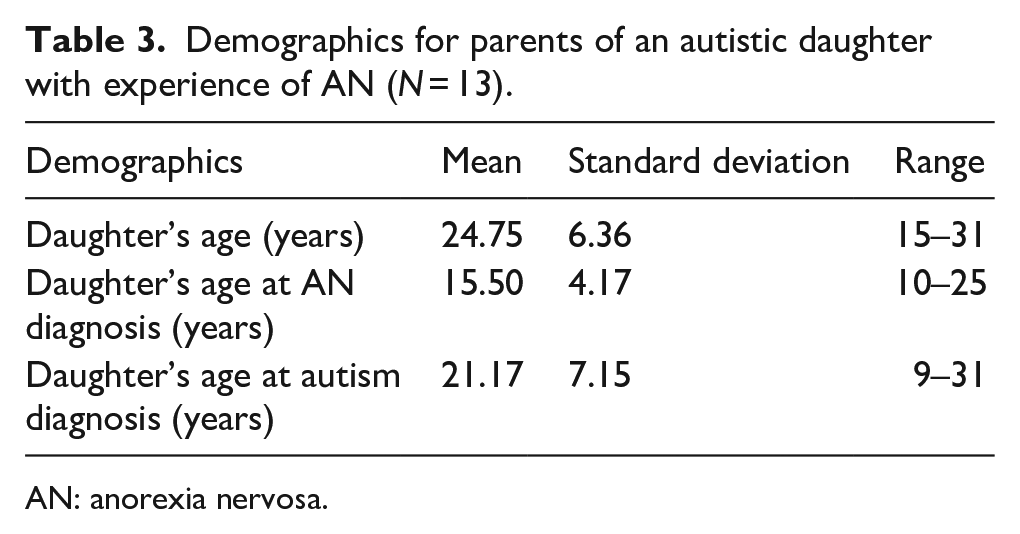
AN: anorexia nervosa.
Healthcare professionals
The inclusion criteria for HCPs were that they worked in ED services in a clinical capacity and had experience working with autistic individuals in this setting. Professions included clinical psychology (N = 6), psychiatry (N = 4), and counselling psychology (N = 1). Two HCPs worked across both ED and autism services. The mean length of time working in their role was 9.6 years (SD = 5.8 years; range = 4–23 years). All HCPs reported working with individuals with a formal autism diagnosis in ED services. Many also reported working with girls and women whom they suspected were autistic but did not have a formal diagnosis.
Materials
AQ-10
The 10-item AQ-10 was administered to all autistic women to measure autistic traits and supplemented a self-reported clinical diagnosis of autism (Allison et al., 2012). Scores range from 0 to 10, with scores of 6 or above being indicative of autism. The AQ-10 has excellent predictive validity (>90%), comparable to the full 50-item AQ (Booth et al., 2013). Internal consistency for the autistic women in our sample was low (α = 0.29).
ED Examination Questionnaire- short form (EDE-QS)
The 12-item EDE-QS measured autistic women’s current ED symptomatology. Scores range from 0 to 36, with higher scores indicating more severe ED symptomology (Gideon et al., 2016). The EDE-QS can successfully distinguish individuals with and without a clinical ED (Gideon et al., 2016). Internal consistency for the autistic women in our sample was acceptable (α = 0.77).
Interview schedules
Our autistic advisors consulted on the interview schedule development to ensure that participation was accessible. The autistic women’s interview covered their experience and diagnosis of autism and AN, how their AN and autism may interact, and the ED services they had encountered. This interview schedule was adapted for the parent group to be applicable to their daughter’s and family’s experience. The HCP interview schedule covered their experiences and knowledge of autistic women in ED services. Prompts were used to expand on the answers given, where necessary. Full interview schedules can be found as supplementary material in Brede et al. (2020).
Procedure
All autistic women and parents completed a demographic questionnaire, and autistic women additionally completed the AQ-10 and EDE-QS. Interviews were conducted by one of two non-autistic female researchers (C.B. and J.B.) either face-to-face, via Skype, or over the phone. They lasted on average for 1 h 23 min (range: 43 min to 2 h 26 min) with autistic women, 1 h 27 min (range: 43 min to 1 h 54 min) with parents, and 1 h (range: 53 min to 1 h 15 min) with HCPs. Participants were offered £10 to thank them for participation. All interviews were audio-recorded with participant consent.
Analysis
Interviews were transcribed verbatim and entered into the qualitative data analysis programme NVivo 12 (QSR International Pty Ltd., 2018) for analysis. Thematic analysis (TA; Braun & Clarke, 2006) was used to identify patterns and themes across the data. TA was chosen for its flexibility and because it allowed generation of new ideas and insights from the data. An inductive, essentialist approach to TA was adopted when analysing the data, with theme development driven by the participants’ experiences, insights and the overarching research aim.
C.B. and J.B. coded transcripts in reverse order to one another, so that different insights and perspectives could be utilised when emerging themes were discussed. Discussions about coding occurred regularly between C.B. and J.B., and with the wider research team. All transcripts were double-coded. At two points during analysis, our two autistic advisors provided feedback on the clarity of emerging themes and whether themes accurately reflected the autistic voice. These insights were taken into consideration when finalising the themes.
Themes were initially generated from the codes in the autistic women datasets. These initial themes were used to synthesise the codes in the parent and HCP datasets. Themes were refined to establish the final themes and sub-themes.
Results
Analysis of the three datasets resulted in three interrelated themes: misunderstanding autism and autistic traits, one treatment does not fit all, and improving accessibility and engagement within services (Table 4). Participant quotes are labelled as ‘AW’ (autistic women), ‘HCP’ (healthcare professional) or ‘P’ (parent) followed by a number to represent individual participants anonymously.
Main themes and subthemes.
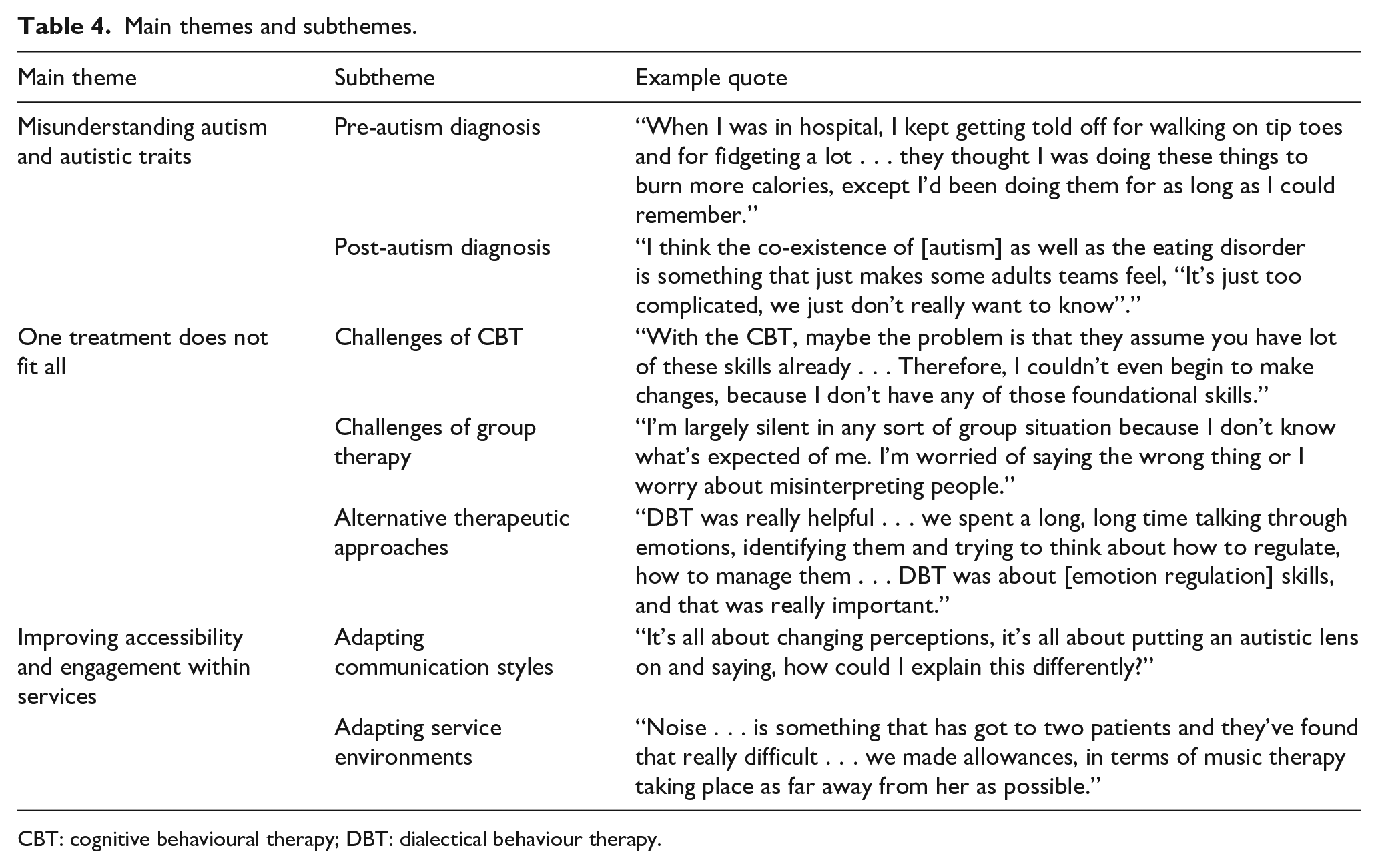
CBT: cognitive behavioural therapy; DBT: dialectical behaviour therapy.
Misunderstanding autism and autistic traits
None of the autistic women had an autism diagnosis when they were first seen by ED services. They noted that some of the autistic traits and behaviours that they displayed were misconstrued. Contact with ED services varied for the women; some only encountered services for a few months, but the majority described multiple referrals across many years. Some autistic women received an autism diagnosis during this time period and consequently experienced ED services with and without a diagnosis of autism. Even with a diagnosis, some women still felt that their autistic traits were dismissed.
Pre-autism diagnosis
This sub-theme relates to autistic women’s experiences in ED services before they received an autism diagnosis. Many women felt that their autistic behaviours and traits were misjudged by some staff as driven by their ED. This led to these women being labelled as ‘resistant’ or ‘naughty’, which in turn made them feel unheard. In particular, coping mechanisms the autistic women adopted to appease sensory sensitivities were misinterpreted by staff: When I was in hospital, I kept getting told off for walking on tip toes and for fidgeting a lot . . . they thought I was doing these things to burn more calories, except I’d been doing them for as long as I could remember. (AW09)
Other autism-related traits, such as communication difficulties or a lack of flexibility, were often misinterpreted as disengagement from treatment: I felt . . . very criticised. I was being very resistant – or labelled as being very resistant. I don’t think they took into account how . . . difficult I found it seeing lots of different people. (AW08)
Although they did not realise that they were autistic at the time, the autistic women expressed that they were aware that many of the traits they displayed were not driven by their ED. These misinterpretations of behaviours were noted by some HCPs, who described the difficulties of disentangling ED-fuelled behaviours and behaviours that might be related to autism: For example, she would want to put a pea on each of the prongs of the fork, but [staff] said ‘oh no you can’t be doing that, you shouldn’t be doing that’ and corrected her when she was doing it, because they thought it was being driven by the eating disorder. (HCP03)
Some HCPs expressed their concerns around distinguishing autistic traits from being in a state of starvation: One of the interesting things with people with particularly low weight is that the cognitive inflexibility that comes with it may sometimes be mistaken. . . Whether it is something that is a developmental condition or whether it’s something that is caused by the effect of starvation. (HCP05)
Recognising the overlap in AN and autistic presentations was described by HCPs as ‘murky’ and a ‘grey area’, which makes it ‘difficult to separate them all out’.
Post-autism diagnosis
Some autistic women spoke about their experiences of ED services once they had received their autism diagnosis. In some cases, they felt that their diagnosis was still not taken into consideration in their treatment: It felt like they didn’t care . . . I used to like to sit in the same seat, just because I knew where it was, and every day a different staff member would go and sit there. And they wouldn’t understand why I was getting upset. (AW18)
Indeed, some HCPs reflected on the challenges for other staff in understanding autism in their workplace: People who are interested in working with eating disorders don’t necessarily have an interest in, or a great deal of knowledge, working with autism. (HCP05)
Furthermore, some HCPs emphasised that ED services, which were described as stretched for time and resources, may feel unable to support these individuals: I think the co-existence of [autism] as well as the eating disorder is something that just makes some adults teams feel, ‘It’s just too complicated, we just don’t really want to know’. (HCP01)
Indeed, some autistic women highlighted their experiences of being ‘too complex a case’ for individual clinicians that they had encountered.
It is important to note that not all the autistic women had negative experiences with clinicians understanding their autism. Once a diagnosis had been given, this did in some cases lead to a better understanding of the individual and their needs: When I explained about needing the food separate, they were very good about accommodating that. And they would separate out the food, and they didn’t necessarily challenge that . . . but they also gave me the opportunity to try it differently if I wanted to. (AW03)
However, this understanding tended to reflect a minority of autistic women’s experiences in ED services, with adaptations being dependent on individual clinician’s experiences.
In summary, many of the autistic women stressed the importance of feeling heard and validated within services, as often their needs would differ to those of other service users. This particularly related to social communication and sensory sensitivities. However, an understanding of autism tended to depend on staff’s personal experience and knowledge. For some HCPs, there seem to be difficulties understanding the overlap between AN and autism.
One treatment does not fit all
This theme relates to different treatments that autistic women had received and the challenges they experienced.
Challenges of CBT
Most autistic women said they received CBT as part of their treatment, but nearly all described negative experiences of it. Some expressed that CBT was not accessible or effective for them: With the CBT, maybe the problem is that they assume you have a lot of these skills already . . . Therefore, I couldn’t even begin to make changes, because I don’t have any of those foundational skills. (AW17)
Interviewer: Is that something you found difficult, to transfer the skills [learnt in CBT]?
AW03: I didn’t realise anybody would need me to. I wasn’t realising that I was being taught a general technique rather than to alleviate a particular problem. (AW03)
These women believed they did not benefit from CBT as they did not have the skills needed to fully engage with the therapy, e.g. the ability to transfer learnt information to real-life situations. In contrast, a couple of autistic women felt that they did benefit from CBT, noting that they found it to be helpful: [CBT] helped me to understand why I thought and felt the way I did . . . that understanding helps you to kind of . . . restructure your thoughts and made me realise what wasn’t true. (AW14)
HCPs also reflected on difficulties that autistic women might face with CBT treatment: In theory, they can demonstrate that they can switch between one way of thinking to another. When you put that dynamically into a daily life situation, they can’t generalise it, it becomes different. So, they look as if they’re making progress, but they’re not. (HCP02)
Parents tended to echo the negative view held by autistic women, describing the CBT their daughter received as a ‘one size fits all’ approach, overlooking individual differences. They felt that their daughters, who did not fit the treatment ‘mould’, were left behind: [Daughter has] not been able to go through the sausage machine of evidenced-based care . . . [she] keeps falling off the conveyor belt. (P03)
Challenges of group therapy
Many autistic women were offered group therapy and described how the social demands impacted their ability to engage with the treatment: I’m largely silent in any sort of group situation because I don’t know what’s expected of me. I’m worried of saying the wrong thing or I worry about misinterpreting people. (AW08)
This links with the theme of ‘Misunderstanding autism and autistic traits’, in which autistic women and HCPs described how HCPs can misconstrue social difficulties as reflecting lack of engagement or ‘rudeness’, which further exaggerated their anxiety in this setting. Some HCPs acknowledged the social information-processing difficulties for autistic individuals within groups: Processing information from others can be very arduous anyway . . . bring in a dozen more people into that room, it becomes impossible . . . a lot of people I see just go into shutdown in these groups, become silent, become withdrawn and find it hard to properly engage. (HCP03)
Similarly to the theme of ‘Misunderstanding autism and autistic traits’, this recognition typically reflected the HCP’s own experience of autism, rather than representing a service-wide awareness.
Some autistic women noted that a lack of structure in a group setting affected their ability to engage with therapy: They had other groups as well, one which was just a general talking group, which I found was really unhelpful because they had no structure to it. (AW11)
Similarly, HCPs highlighted the importance of structure, and suggested that specific types of group may still be beneficial for autistic individuals: Groups differ . . . if they were in a [dialectical behaviour therapy] group that’s highly structured, they know exactly what to expect, it’s all done from handouts, it’s all teaching sessions, so that might be more tolerable or comfortable than say our contemplation groups, which are more of the social interaction. (HCP14)
These sentiments were echoed by one autistic woman who shared her experience of group therapy for her ED. Adjustments were made so that handouts were given to her in advance and she met with a staff member outside beforehand to reduce her anxiety.
Alternative therapeutic approaches
Alternatives to common ED treatment options, such as CBT, were discussed by many autistic women. For example, dialectical behaviour therapy (DBT) (Linehan, 1993) was often described as helpful: DBT was really helpful . . . we spent a long, long time talking through emotions, identifying them and trying to think about how to regulate, how to manage them . . . DBT was about [emotion regulation] skills, and that was really important. (AW17) Emotion regulation was really important to me . . . when I was in distress, I would just self-harm, just become very unwell. But after that, I actually started to think what was going on . . . I think that’s what really helped to improve my eating at the time. (AW01)
Therapy emphasising developing skills in recognising, managing and regulating emotions was perceived by many autistic women as particularly beneficial. In addition, occupational therapy was positively received due to its practical focus: [The occupational therapist] helped me get a volunteer placement at my old primary school . . . that was the best therapy I ever got, because it was practical and gave me something to do. (AW09)
Moreover, autistic women seemed to prefer a therapeutic focus away from food, weight and body image. For many, these were not as relevant as other underlying issues relating to the AN: She basically didn’t believe me when I said this is not about [body image] . . . she wanted to do body image therapies with me and I . . . found it humiliating, and also irritating and condescending that I was being not listened to. (AW13) We didn’t really focus on my eating. . . They made me focus on emotion regulation, and just mindfulness really, and social aspects, and that really helped me. (AW01)
In the first quote, feeling unheard is recurrent from the theme of ‘Misunderstanding autism and autistic traits’, whereby women felt their difficulties were being misconstrued by some staff as classic ED behaviours. In contrast, the second quote illustrates the benefits of focusing away from typical therapeutic content and towards issues that are more relevant to autistic difficulties.
To summarise, many autistic women felt they did not benefit from the typical therapeutic approaches. Engagement in group therapy was difficult due to social demands. Therapeutic models such as DBT and occupational therapy were favoured by many women due to the focus on regulating emotions and practical aspects, respectively. Moreover, focusing therapy away from food and body image was described as beneficial. A clear therapeutic structure seemed to be an important element for successful engagement, regardless of the type of treatment received.
Improving accessibility and engagement within services
The final theme relates to adjustments that can be made within services to accommodate autistic individuals. This theme links to the sub-theme of ‘Post-autism diagnosis’ in the ‘Misunderstanding of autism and autistic traits’ theme, where HCPs who adjusted usual practice to accommodate autistic needs were praised.
Adapting communication styles
Communication with HCPs appeared key to the autistic women’s engagement with services. Autistic women spoke highly of HCPs who adapted their usual communication style to meet their needs: She understood how best to communicate with me, so she gave me written summaries after my appointments, she gave me written information and we used goal setting to help plan my care. (AW11)
Moreover, some HCPs identified communication barriers with autistic clients and suggested how to overcome these: It’s all about changing perceptions, it’s all about putting an autistic lens on and saying, how could I explain this differently? (HCP02)
Despite these insights, the autistic women’s experiences tended to reflect that effective communication was not typical of the whole multidisciplinary team – a common thread seen throughout the results.
Parents were also aware of communication difficulties that their daughter may have with staff, including the importance of language used to start a conversation and build rapport: ‘How are you?’ is a very annoying question to my younger daughter. What on earth does that mean? If it’s something more specific, like, ‘What have you been doing this morning?’ [it] is likely to make you feel comfortable and start a conversation. (P09)
This relates to the narrative seen in the first theme, whereby autistic women describe their social communication difficulties being misunderstood by some staff.
Adapting service environments
Many autistic women talked about the service-level adaptations that were, or could have been, made to accommodate their autism, particularly relating to sensory sensitives and their need for predictability and routine. This relates to the ‘Misunderstanding of autism and autistic traits’ theme, in which some staff’s understanding of autism allowed for adjustments to be made.
Relating to the ward environment, more routine and structure was desirable, such as a more rigid daily timetable: Although I found the groups more challenging, I knew what I had to do during my day. I found unstructured time difficult, and I used to spend my time making my own structure. (AW08)
This relates to the ‘One treatment does not fit all’ theme–although group therapy was difficult, the structure it gave was helpful. Routine and structure resonated as an important factor for many autistic women in their ability to engage with treatment. Moreover, small adjustments to support the unpredictability of a new environment helped autistic women to engage with services: The adjustments they agreed were . . . agreeing a time and day for key work sessions, giving me plenty of notice of change . . . and I could bring my soft duvet cover in and that then meant that I was comfortable and I could sleep and it’s just minor things like that that can make a really big difference. (AW11)
Furthermore, many HCPs reflected on practical adjustments made to better accommodate autistic traits within therapeutic settings: Noise. . . is something that has got to two patients and they’ve found that really difficult . . . we made allowances, in terms of music therapy taking place as far away from her as possible. (HCP08)
To summarise, autistic women’s engagement with services was facilitated by staff adapting the way they communicate with autistic clients. In addition, the implementation of environmental adjustments to accommodate needs, e.g. sensory sensitivities, were praised by those who received them. This ties in with the previous themes, highlighting the need for an adaptive, individualised and autism-informed approach to treatment.
Discussion
This study aimed to deepen our understanding of autistic women’s experiences of ED services by synthesising the views of autistic women with experience of AN, parents and HCPs working in ED services. One of the strengths of this study was the triangulation of the three stakeholder perspectives recruited from across the UK, representing a wide range of service experiences. Parent interviews enabled us to explore the extent to which the service experiences of autistic women with AN was reflected in close family members, and gain insight into periods of time when autistic women with AN were severely ill in ED services, which autistic women themselves may be unable to recall. HCP interviews allowed us to gain insight into the treatment of autistic women with AN from the perspective of relevant services. Another strength of this study was its participatory approach, which ensured that questions asked were considerate, relevant and clear to participants. Our research was enhanced by our advisors’ lived experience and their understanding of the experiences of others within the community. Using TA (Braun & Clarke, 2006), we generated three interrelated themes: ‘Misunderstanding autism and autistic traits’; ‘One treatment does not fit all’; and ‘Improving accessibility and engagement within services’. The overriding message emerging was that the ability to recognise autistic traits and understand autism in ED services is paramount to allowing autistic women to engage effectively, whether they have an autism diagnosis at the time or not.
Our findings broadly support previous staff adapting way they communicate, 2019), strengthening claims for the need to adapt current therapeutic approaches, with an emphasis on a better understanding of the cooccurrence of AN and autism, through validation in a large independent sample. In addition, by having a sample of clinically diagnosed autistic women, the current study adds insight into how the women’s autism diagnosis in particular affected their experience in ED services. The participants in the current study described that common therapeutic approaches for AN may be less accessible to them. Moreover, the close overlap in the way that autistic traits and the symptoms of AN manifest often led to misinterpretations of behaviour by staff. Taken together, these experiences endorse a need to adjust and adapt current service provision to meet autistic women’s needs.
There are similarities in our findings to the ED service experiences of non-autistic individuals with AN, suggesting some findings reflect service-wide issues. ED service-users in other qualitative studies reflected that staff treated them as an ‘anorexic’, without taking into account their individual differences (Offord et al., 2006; Smith et al., 2016). This is comparative to our finding that women’s autistic traits were misinterpreted as ED-related behaviours, i.e. viewing the individual as a stereotypical anorexic patient and interpreting behaviours through this lens. However, it is important to note that although autistic and non-autistic women with AN may superficially report similar experiences, the reasons for their dissatisfaction may be distinct. For example, women with AN described a desire for therapeutic focus away from food and weight, as it reinforced ED-related ideas and behaviours that were of critical importance to them (Rance et al., 2017). For our autistic participants, this was due to the insignificance of weight concerns to their AN (Brede et al., 2020). Moreover, Ranche and colleagues noted that CBT was unpopular for women with AN due to its rigid structure. However, for many of our participants, a rigid structure was endorsed, and it was the requirement for abstract thinking abilities within CBT that held them back. The impact of other ED service-users on an inpatient ward was not as pertinent in the autistic women’s narratives in this study, as is seen in other qualitative research (Colton & Pistrang, 2004; Smith et al., 2016), further emphasising their need for individualised care.
An unexpected finding in our data was that all the autistic women, and most of the autistic daughters of parents, had received their autism diagnosis after they were first seen by ED services. For many, their autism was not recognised until years after their ED was recognised, and there are a couple of potential explanations for this. First, this could be explained by the presence of autism merely being an epiphenomenon arising from the ED alone, rather than being present prior to the ED onset (Dinkler et al., 2020) – that is, autistic traits are exacerbated due to the consequences of the ED, and not indicative of ‘true’ autism. For an autism diagnosis to be given, traits must be present in early childhood (American Psychiatric Association, 2013), yet recent findings have suggested that this does not seem to always be the case with those who present with autistic traits after the onset of their ED (Dinkler et al., 2020). Alternatively, and in line with our participants’ narratives, it could reinforce findings that, particularly for women, mental health diagnoses act as a barrier to an autism diagnosis, known as diagnostic overshadowing (Bargiela et al., 2016; Leedham et al., 2020). Recent thinking suggests that a dimensional, heterogeneous characterisation of autism is warranted, rather than relying on a categorical autism definition (Happé & Frith, 2020). Recognising and accommodating the presence of autistic traits, rather than relying on formal diagnosis, could allow those without (as well as those with) a diagnosis to be supported more appropriately. Indeed, autistic women and parents in our study reported that consideration of autistic traits would have helped them to access more appropriate care when being treated for AN.
Our results imply a culture within some ED service teams that may lack capacity to accommodate autism and recognise autistic traits. We can draw parallels from previous qualitative research conducted with HCPs working in ED services (Graham et al., 2020). HCPs described working in ED services as emotionally draining, which lead them to form negative and stereotyped judgements of patients. To avoid these negative feelings, HCPs described shutting off and becoming task-oriented, subsequently overlooking patient’s individual differences. Relating to the current study, both stereotyped judgements and neglect of individual differences meant that autistic traits were often attributed as ED-fuelled behaviours. This suggests a need for a culture shift towards an individualised, holistic approach to care.
Clinical implications
While the scope of the current study did not focus on the mechanisms underlying anorexic behaviours in autistic women (see Brede et al., 2020) we did note that autistic women reported a lack of concern about body image, reflecting that anorexic behaviours in autism may have unconventional antecedents or maintaining factors for some individuals. Research suggests that treatments for autism-related anxiety should be developed that are distinct from those for ‘common’ anxiety, although both can occur in autism (Lau et al., 2020). Similarly, there may be autism-related mechanisms driving at least some anorexic behaviours in autistic women or those with high levels of autistic traits (e.g. selecting food based on sensory properties) which would require different treatments to ‘common’ anorexic behaviours (e.g. selecting food based on calorific content).
Our results suggested that AN treatment recommended by the UK’s National Institute for Health and Care Excellence (NICE, 2017) like traditional CBT tended to be unsuccessful for autistic women. However, CBT has been successfully modified to treat autistic individuals for other mental health disorders such as anxiety (Lang et al., 2010), depression (Russell et al., 2020) and obsessive-compulsive disorder (Kose et al., 2018), suggesting there may be scope for modifications to CBT-ED (Fairburn, 2008). Furthermore, our findings highlight the potential value of other treatment options, such as DBT (Linehan, 1993). Other therapeutic approaches are being trialled for autistic individuals with AN, such as Cognitive Remediation Therapy which aims to address specific cognitive difficulties, rather than directly addressing the ED (Dandil et al., 2020).
Our results highlight the need for more understanding and recognition of autism within ED services to provide effective treatment for autistic service users. We know that autistic traits are overrepresented within AN populations (Westwood et al., 2016), and this should be considered when offering treatment for AN. Moreover, considering the high number of women who have a late autism diagnosis, an understanding of how autistic traits might present in ED services will allow these women to seek advice and a diagnosis, if appropriate. Indeed, some of this work is currently being piloted through the implementation of the Pathway for Eating disorders and Autism developed from Clinical Experience (PEACE) at the South London and Maudsley NHS Trust, which aims to address autism and AN comorbidity clinically through better autism identification and staff training, treatment adaptations and improved service experiences (Tchanturia et al., 2020).
Limitations
A limitation to this study was the sampling of participants. Our online recruitment technique excluded those who did not use social media. There is also potential for a volunteer bias whereby autistic women who were particularly dissatisfied with their care may have been more inclined to participate. Furthermore, we did not collect any measures of intelligence quotient (IQ), but the autistic women’s reported education levels suggest generally high levels of intelligence. A meta-analysis found that individuals with AN have higher average IQ scores compared to the average of normative data (Lopez et al., 2010). This suggests that there may be a subconscious recruitment bias to exclude those with lower intellectual abilities, which should be addressed in future research. Moreover, because of the bias in recruitment towards HCPs with experience working with autism and AN, their reflections may be different to HCPs with less experience with this client group or those who did not resonate with the aim of this study. A strength of our recruitment technique, however, was the ability to recruit participants from across the country, and therefore investigate a broad range of experiences and expertise.
Given the interpretive nature of qualitative research, we acknowledge that researcher bias may shape the results to some extent. While we put techniques in place to control for this, e.g. having two coders to analyse data and involving the wider research team with a range of backgrounds in theme development, we recognise that our own beliefs, values and experiences can shape our analysis, and this should be taken into consideration when interpreting the findings.
While the AQ-10 is recommended as an autism screening tool (NICE, 2016) and endorsed in its use in AN populations (Westwood et al., 2016), other research has suggested that the measure may not be an effective tool to use in a clinical population, with particular concern being raised with its use in AN populations (Kerr-Gaffney et al., 2020; Sedgewick et al., 2019), which has implications for the validity of the AQ-10 used within the current study. Moreover, our sample’s low internal consistency contrasts with that reported by the developers of the AQ-10 (Allison et al., 2012), who reported a Cronbach’s alpha of 0.85. It has been suggested by other authors who also found low internal consistency (Lundin et al., 2019) that this contrast may be due to differences in sample characteristics across studies. To combat this, future research should implement a more robust, reliable measure of autistic traits, such as the Autism Diagnostic Observation Schedule-2 (ADOS-2; Lord et al., 2012).
Future studies could also consider including a control group of non-autistic women with AN. This would allow researchers to tease out where difficulties experienced are autism-specific, and where these are more universally experienced, e.g. whether difficulties with generalising CBT techniques, as stipulated by participant AW03, is specific to autistic individuals, or whether there are other factors influencing this, such as therapist characteristics or competency. Moreover, to improve the veracity of self-reported clinical diagnosis of autism, future studies should contemplate using more stringent checks to validate this, e.g. validating via health records.
While our study focused on autistic women with experience of AN, further research should consider the views of autistic men, non-binary and transgender individuals to understand any discrepancies in their experiences of ED services. In the general population, there are gender-specific issues that men face in ED services (Robinson et al., 2013), and transgender clients in ED services face their own difficulties, with many clinicians being unequipped to appropriately treat them (Duffy et al., 2016). It is unknown whether this study’s findings would translate to the experiences of these individuals and future research is needed.
Conclusion
This study explored the experiences of autistic women in ED services, from the perspectives of autistic women themselves, their parents and HCPs. Our findings, combined with other research, emphasise that autistic women’s needs are not being met in ED services and better awareness and understanding of autism is needed within these services, including recognising women without a formal diagnosis. Future research should focus on developing AN interventions that are specifically targeted and/or appropriate for autistic people and those with high levels of autistic traits.
Footnotes
Acknowledgements
We would like to thank the autistic women, parents and healthcare professionals who participated and generously shared their insights, Lauren Huff for her help with transcribing, and the Autistica Discover network for their support with recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Autistica (7252). The funder had no involvement in the study design and analysis, writing of the manuscript, and in the decision to submit the manuscript for publication.
Ethical compliance
Written informed consent was obtained from all participants in this study. The study obtained ethical approval from UCL (12973/001) and Cardiff University (EC.18.05.08.5302) ethics committees.