
Abstract
Although the evidence of parent training programmes for families of autistic children has continued to grow, little is known about the experiences and perceptions of key stakeholders, especially in low- and middle-income countries. This qualitative study was part of a larger real-world evaluation of a short-term intensive parent training programme in routine services delivered to caregivers of autistic children aged 3–6 years in China. It aimed to provide insights into programme acceptability, reasons for participant involvement, and factors related to programme implementation. Fourteen caregivers participated in the in-depth interviews, and two focus group discussions were conducted with eight practitioners. Data were analysed using a combination of data- and theory-driven approaches. Findings point to the needs in low autism resource settings for substantial practice and feedback; group support; individualised coaching; more autism-related knowledge, resources and activities for children and extended family members; and organisational support to practitioners. Further research is suggested to address the recommendations and assess their effectiveness empirically.
Lay abstract
While much knowledge about autism derives from high-income countries, most people diagnosed with autism reside in low- and middle-income countries, where little is documented in terms of local interventions. This is also true for parent training programmes for families of autistic children. An evaluation was conducted to understand the effects of a short-term intensive parent training programme delivered in routine services for families of autistic children in China. This study reported results from the in-depth interviews with 14 participating caregivers and group discussions with eight group leaders. The interviews and discussions were aimed at learning (1) to what extent the programme components were deemed acceptable, (2) what affected caregivers’ attendance and engagement in the programme and (3) what affected group leaders’ delivery of the programme. Findings suggested that future parent training programmes provide adequate opportunities for caregivers to practice and receive feedback; group support; coaching experience tailored to individual challenges; more autism-related knowledge, resources and activities for children and extended family members; and organisational support to group leaders. This study highlights the value of qualitative research and points to the need for more empirical studies to address the recommendations, so that research findings can be better utilised to promote practices.
Keywords
A large regional study recently conducted in China showed a prevalence rate for autism of 1% (approximately 3.1 million children), which is in line with the estimate for Western countries (National Bureau of Statistics of China, 2021; Sun et al., 2019). Families of autistic children in low- and middle-income countries (LMICs) tend to face more accumulated adversities than those in high-income countries (HICs), including problems such as resource constraints and social marginalisation (Walker et al., 2011). Autistic children are more likely than their non-autistic cohorts or cohorts diagnosed with other developmental disabilities to experience co-occurring externalising behaviours (Totsika et al., 2011). These behavioural challenges are linked to increased parenting stress and have an impact in terms of child development (Hayes & Watson, 2013).
Early interventions have been advocated to optimise child outcomes in autism (Courchesne et al., 2011). Early behavioural treatment models for young autistic children, such as Early Intensive Behavioural Interventions and Early Start Denver Model, have shown promising effects in terms of improving behaviours, cognitive performance and language skills (Warren et al., 2011). However, the intensive delivery over several consecutive years makes such programmes unfeasible for many families. Moreover, the common shortage of specialist providers and infrastructure in low-resource settings limits access to intensive specialist care (Morris et al., 2011). As such, relatively shorter parent training and education has been identified to be an important strategy to address this significant unmet need (Zwaigenbaum et al., 2015).
Components of parent training programmes differ, ranging from information sharing to teaching primary caregivers parenting techniques and involving them as the change agent for child outcomes. Systematic reviews have been conducted to evaluate the effectiveness of such programmes in terms of promoting child behavioural adjustment, improving parent–child interactions, reducing autism symptoms and promoting child skills (Fang et al., 2020; Nevill et al., 2018; Oono et al., 2013; Parsons et al., 2017; Postorino et al., 2017; Ratliff-Black & Therrien, 2020; Strauss et al., 2013). Fang et al. (2020) also focussed on programmes in China, found no significant group differences between programmes that originated outside and within China or between programmes with and without clinically qualified deliverers in terms of reducing child challenging behaviour, thereby supporting the use of parent training across cultures and resource settings.
While the growing evidence base for such programmes is promising, much less is known about the views of key stakeholders with regard to the acceptability and feasibility. Qualitative research can identify components that are meaningful to beneficiaries and that have the potential to maintain participant engagement (Butler et al., 2020). However, there are few qualitative studies focussed on autism, especially in LMICs (Makombe et al., 2019). This current study aims to address this gap by investigating the experiences and perceptions of key stakeholders with regard to a short-term intensive parent training programme, named SREIA (Stars and Rain Education Institute for Autism), which has supported thousands of families of young autistic children in China over the course of two decades.
Research question
This qualitative study was aimed at answering the following overarching research question: What are stakeholders’ experiences of participating in and delivering the SREIA programme within a routine service context? It was investigated with specific reference to the extent to which the programme content and delivery methods were deemed to be acceptable; and the extent and nature of the facilitators of and barriers to participant involvement and programme implementation (Berkel et al., 2011).
Methods
Study design
This qualitative study was embedded within a larger quasi-experimental evaluation of the SREIA parent training programme, delivered from September to November 2020 (ClinicalTrials.gov CT04257331). The programme was shown to be associated with improvements in child behavioural adjustment, parental mental health, parental knowledge and parental over-reactivity (under review). In-depth interviews and focus group discussions (FGDs) were conducted immediately after the completion of the programme to provide insights into the intervention process and outcomes (Creswell et al., 2011). Ethical approval was provided by the University of Oxford (R67619/RE001) and Beijing Normal University (SSDPP-HSC2020001).
Programme
The SREIA short-term intensive parent training programme has been delivered to Chinese families of autistic children aged 3–6 years since 1993 by a long-established non-governmental organisation (NGO). It is based on applied behaviour analysis, social learning theory, operant conditioning, developmental and cognitive behaviour theory. It is aimed at reducing child challenges and promoting child development by increasing parental knowledge, improving parenting skills, changing parental attitudes, promoting parental mental health and creating social support. A range of techniques are delivered using a variety of methods in an intensive format, involving 5 days a week for 11 consecutive weeks (Table 1). Such an intensive approach is feasible in China due to the fact that around two-thirds of Chinese families of autistic children have at least one parent who is a full-time caretaker (Guo et al., 2014). Chinese parents are often the primary instructor and advocator for their autistic child, which highlights the need for such programmes to increase their self-efficacy.
SREIA programme topics and delivery techniques.
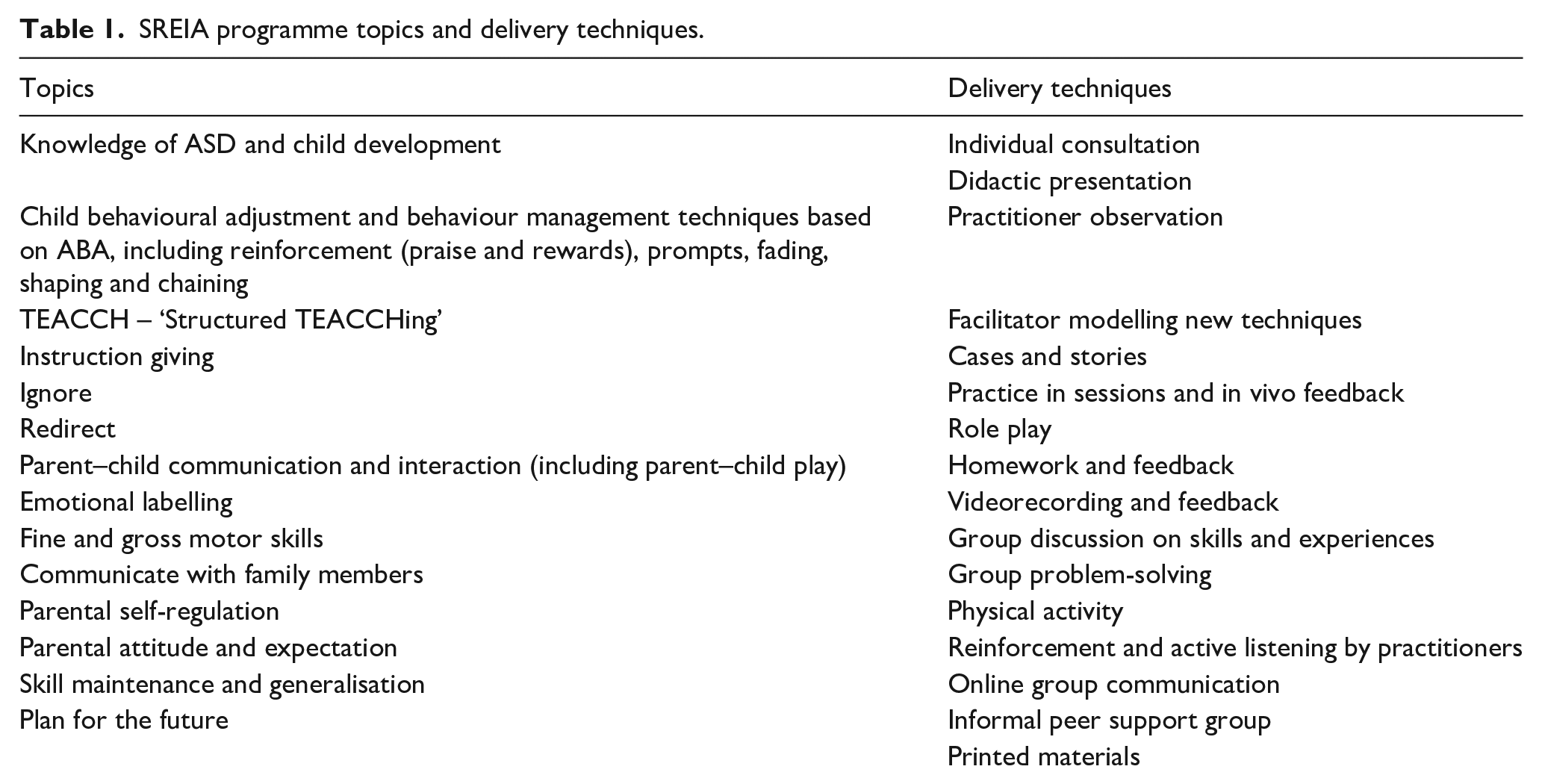
ASD = autism spectrum disorder; ABA = applied behaviour analysis.
Individual pre-consultations are offered with the aim of enabling programme practitioners to better understand family strengths and concerns. An individualised treatment plan is created for each parent–child dyad, covering targeted child behaviours, caregiver areas for improvement and other priorities identified by caregivers. Fourteen 2-h didactic presentations on the core themes are offered across the 11 weeks, with one or two topics each week. The large didactic presentations are then followed by additional training and in vivo practice in small groups of ten dyads to enhance the understanding and use of skills. Content delivered in small caregiver groups focus on the weekly topics, but are also tailored to various degrees for each group to address different needs. Group sessions often start with the practitioner revisiting the content in that week’s didactic presentation(s) and modelling the new techniques, followed by caregivers practicing the techniques in vivo and receiving comments from practitioners and other caregivers. Caregivers are assigned homework activities to practice after sessions. They are encouraged to submit written or video records of their practice at home for practitioners to provide feedback. Communications between caregivers and practitioners remain open and flexible. Opportunities for peer interactions are created by arranging group discussions, group problem-solving activities and an online social and messaging group. The programme is primarily delivered in person, with the 14 didactic presentations also streamed online to avoid mass gathering during COVID-19. The pandemic also led to a lack of childcare services, which used to be provided during the large didactic presentations. The programme had two versions of delivery, which were implemented concurrently and share the same programme content, with the purpose of exploring ways to reduce cost while improving outcomes. Parent groups in Version A attend didactic sessions together in a larger group but practice sessions separately, whereas in Version B, parents have all sessions delivered separately for each group.
Participants
Participants were drawn from practitioners and families involved in the SREIA programme delivered between September 2020 and November 2020. All programme practitioners (N = 8) were invited and consented to participate in the FGDs. They were employees of the SREIA implementing organisation and included Han females in their 20s–40s. They were from diverse educational backgrounds, having college or associate degrees unrelated to healthcare or autism, such as in social work and early education. Five of the eight practitioners had more than 5 years of experience in delivering the programme, whereas the other three practitioners were relatively young. All had been trained and certified by the implementation agency to deliver the programme. The training for the old and new practitioners differed, as the training has evolved over time, although the primary focus remained on knowledge about autism, programme content and programme delivery.
The fidelity of their implementation was assessed using practitioner checklists. Practitioners reported whether they delivered the core components prescribed in the schedule each week. The fidelity scores (maximum = 1) comprised the overall ratio of delivered components to prescribed components. Quality of delivery was also measured by research staff observing parent group sessions and completing a quality of delivery survey. The survey contained 24 items, assessing the general skills of facilitating parent groups (such as knowledge of content, teaching skills and sensitivity to participants’ feelings and experiences) and skills of modelling parenting techniques and facilitating practice sessions (such as appropriately setting up the space and providing adequate support during participant practice). A total score is summed (maximum = 72). Two sessions for each practitioner were randomly selected and recorded for research staff to rate the quality of delivery. Their overall fidelity rate was 0.95 and the delivery was of medium quality, with a mean score of 51.86 (SD = 1.13).
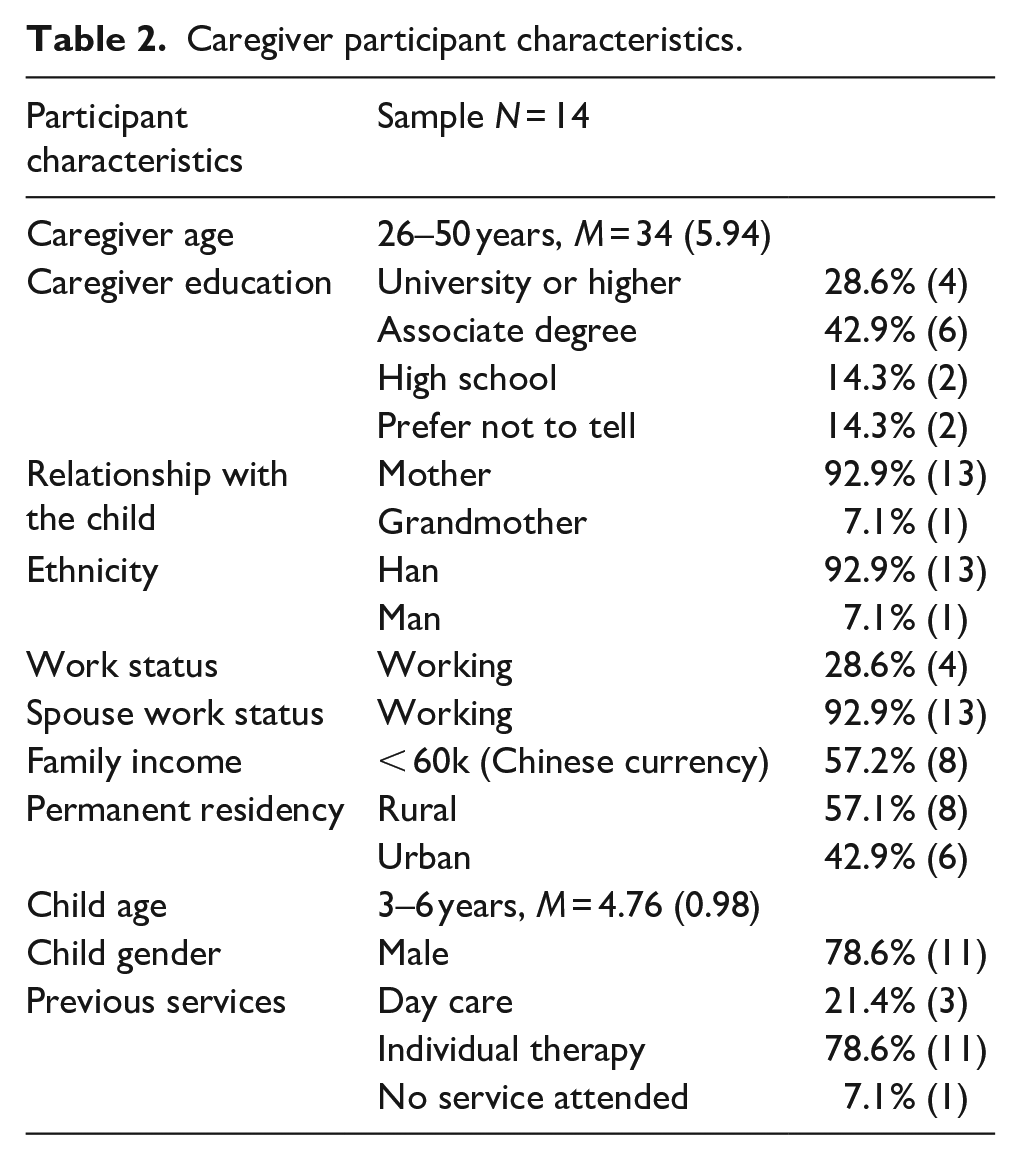
The programme was delivered to seven groups of 10 caregiver–child dyads – four groups in Version A and three groups in Version B. All participating children were diagnosed with autism aged between 3 and 6 years. Evidence shows that caregiver involvement is linked to the potential of programmes to produce desirable outcomes in interventions for autistic and non-autistic children (Baydar et al., 2003; Carr et al., 2016; Nix et al., 2009). As such, participants for the in-depth individual interviews were identified based on their overall attendance and engagement as rated by the programme practitioners. The practitioners recorded caregiver attendance using an attendance register and judged their engagement on a daily basis according to four criteria: responsiveness to practitioners, interactions with other caregivers, participation in group discussions and completion of homework activities. Three caregivers with the highest and lowest levels of involvement were identified in each parent group. However, it should be noted that the rates of attendance (0.98 out of 1) and engagement (5.58 out of 6) were generally high. Recruitment was conducted with the help of practitioners and stopped when data saturation – no additional data are found that can contribute to the emergence of new codes or themes (Glaser & Strauss, 1967) – was reached. The final sample consisted of 14 caregivers (eight from Version A and six from Version B) with different levels of involvement. Table 2 presents the characteristics of the caregivers. Oral informed consent was obtained from all participants.
Caregiver participant characteristics.
Data collection and analysis
The interviews and FGDs were conducted during the week immediately after the completion of the intervention. The caregivers were interviewed individually for a maximum of 1.5 h. Two FGDs were conducted, lasting for approximately 2 h (N = 4 practitioners per group). Semi-structured interview schedules were designed around acceptability, involvement and implementation. Each topic was started with broad open-ended questions followed by probes to evoke detailed responses. Questions evolved over the course of the study to adapt the interview approach based on participants’ responses (Green & Thorogood, 2014). The FGDs were facilitated by the first author and the caregiver interviews were conducted by the first author and a trained interviewer with a master’s degree in social work.
The analytic approach was underpinned by a contextualist framework, which involved combining the traditionally data-driven approach with a theory-driven approach (Braun & Clarke, 2006). As such, coding of the data was guided by a coding framework, while also allowed themes to emerge from the data, capturing the full range of responses. This hybrid approach has demonstrated rigour in previous research (Fereday & Muir-Cochrane, 2006). The data analysis integrated the development of a coding framework into the six phases of thematic analysis described by Braun and Clarke (2006). It involved the following six steps. First, several coding domains were outlined based on the theoretical concepts (programme acceptability, participant involvement and programme implementation) and research questions (facilitators and barriers; Boyatzis, 1998). In addition to these coding domains, a topic pertaining to the experience of having an autistic child in China emerged during data collection. Second, the transcripts were read and re-read to create a list of coding ideas. Third, initial codes were generated from a subset of data and organised in terms of the coding domains. Fourth, preliminary themes were created to develop an initial coding framework. Fifth, the coding framework was applied and constantly modified throughout the coding process. Finally, themes were refined and reported.
Reflexivity, quality and trustworthiness
The first author introduced the study to the participants and coordinated interview times. The interviews were conducted by the first author and a trained interviewer, who are both females, born and raised in China. The first author is a PhD candidate at an academic institute in the United Kingdom, and has been researching parent training programmes for children with and without disabilities. The other interviewer completed a master’s degree in social work in China, and has experience in working with families of autistic children and conducting qualitative interviews.
Given the diverse backgrounds of interview participants, we promoted reflexivity of this study by recognising and addressing power differentials between interviewers and participants. All interviews were conducted in a friendly and empathetic manner. Rapport was built prior to asking any questions. The interviews started with casual conversations, informing participants what to expect in the interview and addressing their concerns about confidentiality. The interviews were conducted in a space that was familiar to the participants. The purpose and anonymisation of recording, as well as their rights to erase the recording and/or withdraw the data, was fully explained. Light refreshments were also provided to create a welcoming and relaxed environment. Further, the coding software ATLAS.ti was used to document the entire coding procedures, including any evolving perceptions and critical decision points. The involvement of second coder and the discussion of discrepancies also facilitated the introspection process.
In addition, several steps were taken to improve the quality and trustworthiness of the results including the data being collected from both caregivers and facilitators and transcribed data being sent to participants for verification and additional inputs before data analysis was begun. To further improve credibility, data analysis was conducted by another researcher checking 50% of the initial coding categories, participating in the development of the coding framework and reviewing all codes and themes before they were finalised.
Community involvement
The implementation organisation took part in the planning of the overall research project, by contributing to the development of the research design, research questions and interview tools. The recruitment of participants was undertaken by the organisation using its existing resources. The programme was delivered by staff of the organisation and took place at the SREIA venues. The organisation did not take part in the data collection or analysis. However, it has been actively involved in the interpretation of results and taking the lead in conveying the research findings to a wider autism community in China. No other organisations were involved in this study.
Results
A summary of the themes and subthemes under each domain is presented in Figure 1 and discussed in the following sections. The identifiers of caregiver quotes start with C and those of practitioners start with FGD. Additional quotes for each theme are presented in the Online Appendix.
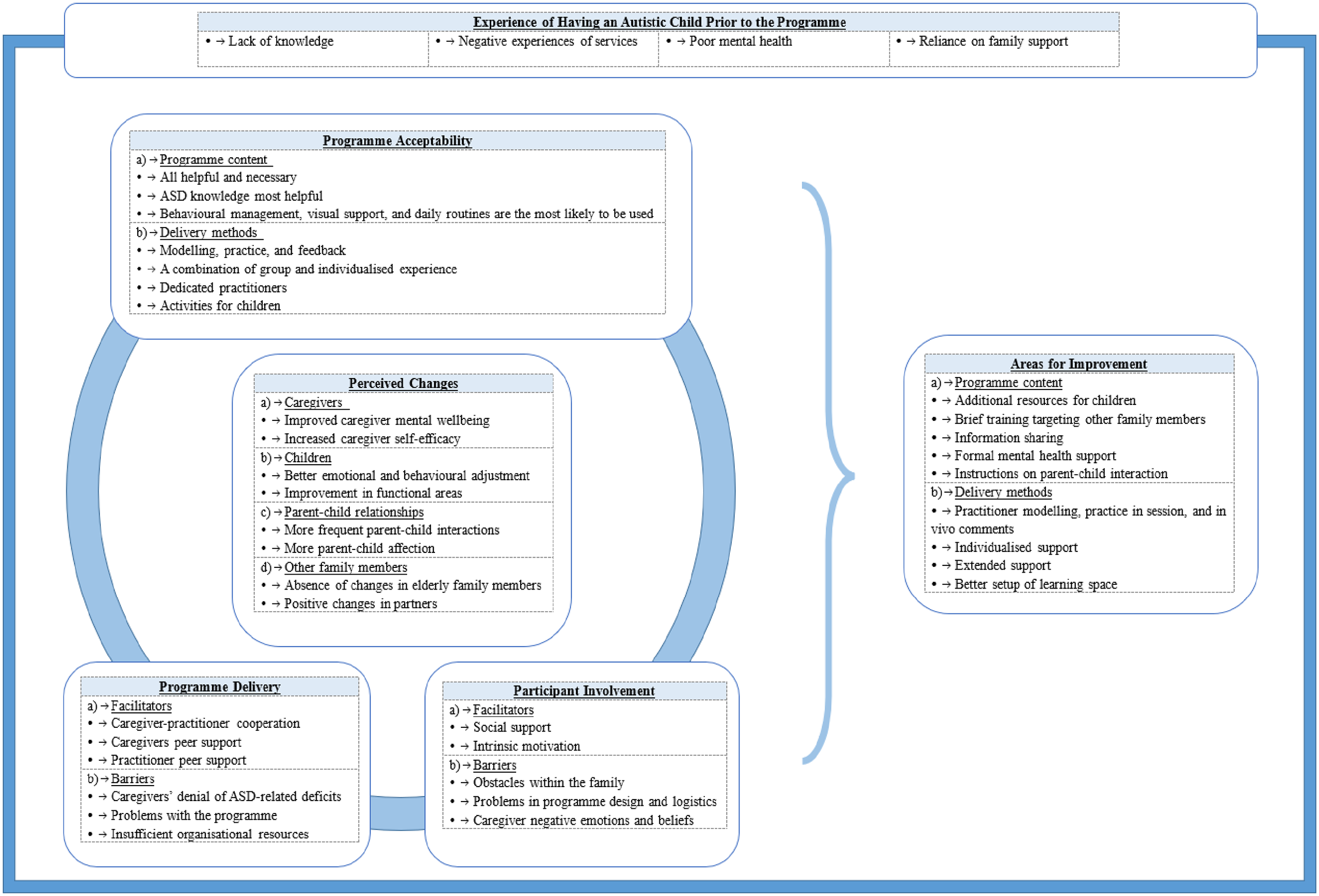
Overview of themes.
Perceived changes
The interviewees described numerous ways in which the programme had produced changes in themselves, their child, parent–child relationships and other family members.
Caregivers were viewed as having improved mental wellbeing after participating in the programme, as a result of having better emotion regulation, moral support from peers and practitioners and a sense of hope in relation to the progress in their child. Caregivers also reported increased acceptance of their child’s diagnosis:
I haven’t even told my parents. I couldn’t accept that my son has Autism. I was afraid that we would be discriminated. Now I feel much more peaceful. Last week my neighbour asked me where we went, and I told her . . . I plan to tell my parents. (CH3, 5-year-old boy)
Caregivers described increased parental self-efficacy characterised by more positive parenting practices and less harsh discipline. In addition, they highlighted the ability to make decisions about which other services to use as a result of having more knowledge about autism.
Perceived changes in children included better emotional and behavioural adjustment and more adaptive living skills, which were perceived to be the result of more positive parenting practices and an increase in child communication skills. More parent–child interactions and affection were commonly referred to by the caregivers, which were similarly considered as being attributable to positive parenting and an increase in parent–child play.
Some caregivers who shared information from the programme with their partner described positive changes in partners, such as less stress and more collaborative parenting. These perceived positive changes may have created a ‘virtuous circle’ in which the occurrence of one led to that of another, which further promoted a continuous process of improvement. These interactions were also well described by one of the practitioners:
What we are hoping to do is to create a virtuous circle . . . The core is centred around getting to know your child, know his deficit, and the signals he tries to give you through his behaviours . . . based on the signals, you apply the skills. During the process, you will know even more about your child, and see all the challenges he has been struggling with, then you know that you should control your own emotions and help him . . . You will have more strength and confidence, which in turn improves your emotions . . . With better emotions, you will also communicate with your family in a better way . . . then there is a better environment at home for your child to develop . . . So you can see there is a virtuous circle – improvement in one area can ultimately lead to the improvement of their overall functioning. (FGD2)
Despite attempts to share their learning, there was generally perceived to have been a lack of change in elderly family members:
I’ve tried to explain, Autism and the techniques, to his grandparents, but I don’t see any changes . . . Some concepts, like Autism, are just difficult for them to understand. In their opinion, if a child does not communicate, it’s only because he doesn’t want to. No other excuse. (CH8, 5-year-old boy)
Programme acceptability
Programme content
All aspects of the programme were perceived to be helpful by both parents and practitioners, with many of the techniques being seen as interrelated. The session that focussed on knowledge about autism at the beginning of the programme was perceived to be central to understanding the diagnosis and its implications, thereby promoting the acceptability of techniques taught at later stages:
[the knowledge of Autism] is like the central nervous system, without which you won’t be able to receive other information or coordinate any activity. (FGD1) Those who skipped the session always don’t accept their children and are more sceptical about whatever we say. (FGD2)
Skills reported by the caregivers as being the most likely to be used included behaviour management techniques, visual supports and daily structure and routine, which were consistent with the perceived changes in children, such as fewer internalising and externalising behaviours and improved communicational skills.
Delivery methods
A number of delivery methods were perceived to have been important in establishing new skills in caregivers, including modelling, practice and feedback, as well as a combination of group experience and individualised support to promote social inclusion and address diverse concerns.
The caregivers and practitioners both highlighted the importance of practitioner modelling, which was perceived to have involved a demonstration of the application of skills, build trust and promote caregiver understanding of their child:
. . . it made me see how it was like for my child to interact with other people. (CL5, 3-year-old boy). . . . because they would only believe us when they saw us successfully applying the skills to their child. (FGD2)
In-session practice and in vivo feedback were also identified as being central to their learning, as they were perceived to have scaffolded caregivers’ engagement with targeted skills. The caregivers also explained that the parent groups provided an experience of social inclusion and belongingness, which was felt to have nurtured a greater acceptance of their children and themselves:
(the caregiver group) were like a family . . . We learn from each other about how we should treat our child and ourselves. (CH1, 5-year-old girl)
Ongoing and flexible communication was also referenced by both groups of participants. The constant close communication between practitioners and caregivers was described as being like one-to-one coaching:
They coached me on things that my child needed most. Every time I thought I could not make it, I messaged her, and she would rebuild my confidence. (CH6, 4-year-old boy)
Furthermore, the flexibility within the programme was described by the practitioners as being core to implementation success, in that the programme provided sufficient space to accommodate individual need. Other aspects of the delivery that were described as being helpful by the caregivers included dedicated practitioners and activities for children. The practitioners were perceived to be knowledgeable, responsive to caregivers’ concerns and as treating participants equally. Activities for children freed caregivers from childcare:
That is when I felt most relaxed. I take care of him 24/7. Only when they were doing activities, I could catch a breath. (CH7, 3-year-old boy)
Facilitators and barriers to participant involvement
Facilitators
Facilitators of participant involvement included social support and intrinsic motivation. Caregivers emphasised social support as a major facilitator of their involvement, especially with regard to programme enrolment. Support from a variety of sources – spouses, extended families, relatives, peers and employers – made enrolment possible. Social support was also perceived to have promoted participant engagement by enhancing their learning experience through collective problem-solving. They also considered familial support as being necessary to help them to maintain consistency of practice at home. In terms of intrinsic motivations, caregivers overwhelmingly talked about a sense of urgency, as they were aware of the importance of early intervention and the role of caregivers in influencing their child’s development. Children’s progress was commonly identified as another major reason for continuing to attend the sessions, as it was described as motivating their learning and use of skills.
Barriers
Participant involvement was perceived to have been inhibited by (1) obstacles within the family, (2) problems with the programme design and logistics and (3) caregiver negative beliefs and emotions.
Lack of family support was one of the barriers to involvement described by caregivers who described that grandparents were not exposed to any programme content and did not understand the diagnosis or new skills, thus limiting wider support from within the family.
In terms of the programme design and logistics, caregivers felt that it was not long enough to support their learning of targeted skills, pointing to the need for more opportunities to practice and receive feedback, and also for the opportunity to address their lack of confidence:
Less than three months . . . We had no chance to be supervised on many of those skills . . . We will need to keep practicing and refer to the notes. (CH9, 5-year-old boy) I’ve heard it and understood it, but I still don’t think I can do it well. (CH2, 5-year-old boy)
Children being present in sessions where they were not directly involved in the demonstration and practice of skills was also reported by caregivers to be distracting:
I was about to take some notes and he started to yell. (CH7, 3-year-old boy)
Online delivery during COVID-19 was identified as another barrier by caregivers who were less able to maintain their focus online and whose learning was often disrupted by technological failure. Another perceived common barrier to participant engagement that was caregiver negative emotions, which were often perceived to have been caused by child non-compliance and the lack of family support:
Overall, it’s mainly their mental state that determines if they can develop solid skills. . . . Although we practitioners need to guide them towards better mental state, their family environment plays a more decisive part in it. (FGD2)
Pre-existing knowledge of the diagnosis or effective practices also made some caregivers resistant to the introduction of strategies:
(previous service providers) said making the child speak was the most important thing . . . So I skipped some sessions that I thought not related to language skills. I did not realise until now that there can be so many ways for us to communicate. (CL1, 4-year-old boy)
Programme implementation
Facilitators
Programme delivery was described by practitioners to be facilitated by (1) caregiver–practitioner cooperation, (2) caregiver peer support and (3) practitioner peer support.
Caregiver–practitioner cooperation was perceived by practitioners to improve the programme delivery and be promoted by caregiver trust:
It took less time for us to build trust this time . . . Perhaps it’s because the COVID quarantine made them realise what they need to learn . . . Shared goals were established right away and I found it easy to communicate with them . . . (FGD2)
Peer support among caregivers was also perceived to be important in terms of implementation because it increased participants’ responsiveness during sessions:
There is a feeling of solidarity among them . . . I don’t need to do much to coordinate. They influence each other and help each other. (FGD1)
At the practitioner-level, peer support among practitioners involving the discussion of difficult cases and sharing of stress-reduction strategies, was perceived to have improved the quality of delivery.
Barriers
The major obstacles to programme delivery that were identified by practitioners were (1) caregivers’ lack of acceptance of their children, (2) problems with the programme and (3) insufficient organisational resources.
A lack of knowledge with regard to the diagnosis was viewed as resulting in denial of the autism-related deficits, which was in turn perceived to make it difficult to convince caregivers of the relevance of the skills during the delivery of the programme:
Sometimes they don’t accept the deficits. Even if the child couldn’t speak, she wouldn’t use pictures (to communicate), because otherwise she was admitting that her child was different. Other people would also notice his difference . . . It’s hard to deliver unless they accept the diagnosis. (FGD2)
In terms of programme design, practitioners highlighted the dilemma of having children present in the sessions. As with the caregiver reports, the practitioners noted the distractions caused by children being present, but also stressed that their presence allowed for substantial opportunities to practice new skills. The practitioners further discussed the difficulties of having to cover a wide range of topics. Thus, even though all the content was perceived as being helpful and necessary, having too many topics within one programme was also felt to be overwhelming and challenging.
At an organisational level, the heavy workload and lack of organisational support were highlighted as significant barriers to programme delivery. The shortage of personnel was perceived to have resulted in an intense workload and high levels of practitioner stress. Practitioners also described an absence of formal supervision and mental health support. This may explain in part why practitioners identified peer support among practitioners as essential for programme delivery.
Areas for improvement
Programme content
Given that children being present in the session was one of the major barriers to participant involvement, it is possibly not surprising that the caregivers predominantly asked for additional resources for children, such as structured activities and childcare, when their child was not involved in modelling and practice. Such activities were also deemed to be an opportunity to develop children’s social skills. The caregivers also highlighted the need for brief training targeting other family members to reduce resistance with the family and maximise child opportunities to learn:
Other family members also need to learn, but they won’t listen to us. They’ll listen better if it’s someone with more experience. (CH7, 3-year-old boy)
In addition, some participants suggested the need for more sharing of information on autism treatments, such as other evidence-based interventions and interventions for older children. They also emphasised the need for formal mental health support, such as counselling and referral. Furthermore, they wanted more instructions about parent–child interaction:
Parent–child relationship is the foundation . . . We noticed that many caregivers did not know how to play, although they really wanted to interact with the child, they did not know where to start. . .We need to work on that. (FGD2)
Delivery methods
In terms of delivery methods, caregivers identified the need for more practitioner modelling, practice in session and in vivo comments to enhance skills. More individualised support was also perceived to be required to address individual concerns.
Caregivers identified a need for the support to be extended after the completion of the programme to facilitate the use of skills at home and keep up a positive attitude:
But when the programme ends and we stay back at home, we have to again face all the challenges we had before. It is hard to make sure we still have the strength to do all these (new skills) or even to stay in a good emotional state. (CH5, 4-year-old boy)
Caregivers also highlighted the need for a better setup of the learning space, including arranging for an offline venue to better demonstrate skills and improving the quality of online sessions.
Discussion
As the evidence in relation to autism treatments has evolved, an understanding of the intervention experiences of stakeholders has become more important. This is especially true in LMICs, where most autistic children reside but little is documented in terms of local interventions and how they are provided. To the best of our knowledge, this study is one of the few to investigate the experience of participating in and delivering a short-term intensive parent training programme for families of autistic children in an LMIC. The findings of this study provide valuable information about the acceptability and feasibility of autism treatments and can be used to address the substantial unmet needs of young autistic children for interventions in low autism resource settings where families face similar challenges.
Summary and implications
The results indicate that caregivers and practitioners highly valued the comprehensiveness of the programme, describing all topics as being helpful and necessary. This may reflect the general lack of autism information and local services more widely (Clark et al., 2019). Indeed, many parents described the programme as being the major source of information for them and wanted the opportunity to participate in future programmes to secure more resources and support. Two previous studies on parenting interventions for families of autistic children in HICs also showed that parents often valued additional information, such as the technique of social stories and advice on the seeking and selection of services (Dababnah & Parish, 2016; Whittingham et al., 2006). However, practitioners were concerned that the comprehensive cover of the programme could potentially compromise the quality of delivery, suggesting the need to help caregivers maintain focus by encouraging them to closely relate the programme content to their own personal goals.
The results also highlighted the importance of learning about autism, which enabled caregivers to better understand and accept the diagnosis and their children’s behaviours, thereby paving the way for learning autism-related parenting techniques. This is consistent with previous research, which showed that introducing autism terms helped establish a ‘common ground’ (Dababnah & Parish, 2016). Moreover, as parents in China typically receive inadequate guidance on the selection of appropriate treatments for their children (McCabe, 2012), getting to know autism and their child better may support their future decision-making. In accordance with other research that found high caregiver rating of content on behavioural management, visual support and structured routines (Lachman et al., 2016), caregivers in this study also identified these techniques as the most likely to be used. At the same time, respondents identified the need for more sessions on teaching parent–child interaction to go beyond the theoretical principles and increase caregivers’ skills in initiating and maintaining interactive play.
As a central aspect of their learning and engagement, participants emphasised the importance of practitioner modelling, the opportunity for in-session practice and feedback. This corresponds with previous studies that also identified the role of modelling as a core programme component (Dababnah & Parish, 2016; Lachman et al., 2016). Despite this, caregivers asked for additional coaching, indicating a general lack of confidence in using all the taught techniques, which might be one of the drawbacks of delivering many topics within a limited timeframe. Participants also highlighted the value of combining group experience with individualised support during and after the programme. Having an autistic child was experienced by participants as leading to social marginalisation, and programmes of this kind were perceived to provide an inclusive environment for caregivers to normalise their experience and expand their social support networks (Mytton et al., 2014). Practitioners further identified caregiver group support as facilitating programme delivery, as it was perceived to enhance caregiver learning through the sharing of resources and problem-solving strategies. The importance of individualised support was evident in themes about programme flexibility and ongoing communication sustained beyond the duration of programme. Previous qualitative systematic reviews identified a consensus across providers, researchers and parents that such programmes should be tailored to account for individual ability and cultural differences (Durlak & DuPre, 2008; Mytton et al., 2014). However, this presents a challenge to programme delivery, especially given the lack of resources and the absence of research on the key intervention components in LMICs.
Past research has indicated that a collaborative and therapeutic relationship established by knowledgeable and non-judgmental group leaders contributes to programme success (Mytton et al., 2014). Caregivers in this study also highlighted the dedication of practitioners, who were perceived to be conversant, responsive and unprejudiced, as playing a critical part in their overall positive experience of the programme. Furthermore, multiple caregivers in this programme described how practitioners improved their mental health, suggesting that, in low-resource settings, practitioners do not only teach skills, but provide the type of support that can lead to wider changes in parental functioning.
Having children participating in the sessions was, however, experienced in a number of ways. Although it was identified as a core component in a review on general parent training programmes (Kaminski et al., 2008), it may be more challenging to implement effectively when delivered to parents of autistic children. While children being present in sessions offered substantial opportunities in terms of in vivo practice and feedback, it was also regarded as one of the major barriers to engagement and delivery. Therefore, caregivers commonly requested more playful and structured activities for children when they were not involved in modelling and practice. Childcare needs in parent training programmes for autism may also differ from programmes designed for the general population. Unlike caregivers of children without autism who need regular childcare services to promote attendance (Mytton et al., 2014), due to the core deficits of autism, caregivers of autistic children may expect more structured activities arranged in childcare services to promote child development. For example, parents in a study conducted to evaluate a parent training programme for autistic children in the United States also requested such activities to be included in the programme to engage children in social interactions (Dababnah & Parish, 2016). Moreover, findings from a systematic review of parent training programmes delivered in China to parents of children with a wider range of developmental disabilities, found that components directly targeting child social skills have the potential to further reduce child externalising and international problems (Fang et al., 2020).
With regard to facilitators of participant involvement, findings suggest that caregivers predominantly considered child progress as their major motivation to participate and learn. This is consistent with the quantitative assessment of the SREIA programme process which found a connection between higher levels of engagement and improved child behavioural adjustment (under review). Similarly, a qualitative study in South Africa found that perceived improvement in child development contributed to participant buy-in and might increase the likelihood of behavioural changes in caregivers of autistic children (Makombe et al., 2019).
Qualitative systematic reviews of parent training programmes for children without disabilities have indicated that familial support can influence participant involvement (Butler et al., 2020; Mytton et al., 2014). Caregivers in this study also highlighted the impact of support from other family members on the level of engagement, describing that the lack of support as inhibiting them from signing up for the programme, engaging in the targeted skills practice and maintaining consistent parenting practices. This may also explain the recurrent request for brief training sessions for other family members, alongside the need to enable other family members to be aware of, and to use, the new skills being taught.
Raising an autistic child is stressful irrespective of geographical location, but the severe lack of information and resources (McCabe, 2007) and the long-held negative attitude towards disabilities in China (Huang & Zhou, 2016) may have created additional sources of pressure for the caregivers in the current study. Despite research suggesting that parental mental health can influence treatment adherence (Hackworth et al., 2018), and the fact that the quantitative SREIA assessment found an improvement in mental wellbeing following the course (under review), only a few caregivers explicitly linked their improved mental health status with the course. One potential reason is that many caregivers of children with developmental and behavioural challenges focus less on their own needs, as was shown in the study of Incredible Years for autistic pre-schoolers, where parents reported that there was little time to attend to their own self-care needs (Dababnah & Parish, 2016). However, receiving more formal mental health support was among the most important post-programme needs for caregivers in this study, which may be related to their concerns about the potential fade-out of programme effects in both child and parental domains (van Aar et al., 2017).
Disagreement about the skills being taught was perceived as another barrier to participant involvement. The finding is in line with previous research showing the negative impact of a mismatch between programme philosophy and parental expectations (Lachman et al., 2016), pointing to the importance of clarifying the programme goals at an early stage of intervention. Online delivery was considered by caregivers as less helpful, because of technological failures and the difficulty in maintaining focus. Nonetheless, online delivery of evidence-based intervention has become a global trend driven by the efforts to promoting equal access to healthcare services and accelerated by the COVID-19 pandemic. This highlights the need to address technical challenges, especially in LMICs where there is a lack of infrastructure, and to explore ways to promote participant engagement in digital intervention initiatives.
In terms of programme implementation, research shows that practitioner peer support can promote long-term skill development and the sustainability of autism early interventions in other low-resource contexts (Makombe et al., 2019). Practitioners in this programme recognised the benefits of seeking advice and wider support from peers. However, the lack of organisational resources may have led to their overdependence on peer support. Capacity building has been consistently shown by the literature as a key ingredient to implementation success, especially in terms of the delivery of complex interventions (Mytton et al., 2014). Therefore, it is of particular importance that implementing organisations provide adequate and ongoing supervision and training, especially given that the use of less qualified programme providers has been increasingly advocated to close service gaps in LMIC contexts (Tomlinson et al., 2018). Other aspects of organisational support related to the need for a reduction in their workload and the improvement of practitioner mental health. Despite their dedication, practitioners in this study perceived the quality of their work as being limited by an intensive workload and stress. This was further reflected by their high fidelity score but medium quality of delivery. The stress may be alleviated by, for instance, organisational mental health support and rest breaks. Alternatively, the intensity of the programme can be reduced by spreading out the programme sessions, providing the same number of sessions and content over a slightly longer period of time. Lower intensity may also increase the accessibility of the programme, as well as provide caregivers with longer support and more opportunities to establish and generalise new skills. More fundamental solutions to reduce workload are also needed at a state-level, including investment in autism-related professional training and incentivisation of service provision.
Strengths and limitations
This study was conducted within a routine service setting and involved participants who were representative of a real-world population, thereby improving the generalisability of the findings. The study nevertheless has several limitations. There was a lack of male caregiver interviewees thereby limiting our ability to comment on their experiences and perceptions. Also, the data were collected retrospectively, which might have introduced recall bias. In addition, the interviews were conducted in Chinese thereby necessitating translation, which could have resulted in more bias. To improve validity, the data analysis was conducted in Chinese, involving two bilingual co-authors, who were born and raised in China. The English report was prepared by one bilingual co-author in discussion with the other, and further checked by co-authors who are native English speakers. Also, we did not identify distinct patterns between caregivers with different rates of attendance and engagement, potentially due to the high levels of involvement in general. Future studies may consider assessing participant involvement using standardised tools to increase sensitivity. Future research can also stratify participants by demographic characteristics and explore how participant experience may differ by background. Moreover, the involvement of stakeholders in this study was insufficient. Stakeholders were limited to organisation staff, who provided only basic inputs into the research design and interpretation of results. Family beneficiaries and stakeholders in the wider community could have been included. More opportunities could also have been sought at every stage to deepen the partnership, so that we could further improve the relevance of the research to the community and shorten the time it took to translate the findings into practice.
Conclusion
This study provides important insights on key stakeholder perceptions about a short-term intensive parent training programme for parents of autistic children in an LMIC. A number of suggestions are provided for future parent training programmes for families of autistic children. In terms of programme design, adequate opportunities for caregivers to practice and receive feedback, as well as a mixture of group and individualised support, are central to creating an overall positive and empowering experience. It is also recommended that support be extended beyond the duration of the programme, or the programme sessions be spread out over a slightly longer period of time, to maintain programme effects. Autism knowledge and programme goals should be introduced at an early stage to help caregivers maintain focus and increase the likelihood of collaborative relationships between practitioners and caregivers. More instructions on parent–child interaction may also promote parent–child relationships and parental use of targeted skills at home. Structured activities can be arranged separately for children, except when parents need to practice skills directly with children with the support of a practitioner. Resources should be shared to help caregivers navigate the service system and improve mental health. Other family members may also need to be briefly involved to strengthen family support. In addition, helping caregivers identify progress in children may promote participant engagement. To improve the quality of programme delivery, more organisational resources – including adequate and ongoing supervision and training, and mental health support – should be provided to practitioners. Practitioner stress could also be reduced by spreading out the programme sessions. Support at a national level is needed to address the human resource challenges. Finally, creative solutions are needed to overcome technical barriers and to engage participants via online platforms. More mixed-methods research is needed to evaluate the impact of the recommended changes and assess their effectiveness using experimental designs, such as micro-trials and factorial experiments.
Supplemental Material
sj-docx-1-aut-10.1177_13623613211070869 – Supplemental material for A virtuous circle: Stakeholder perspectives of a short-term intensive parent training programme delivered within the context of routine services for autism in China
Supplemental material, sj-docx-1-aut-10.1177_13623613211070869 for A virtuous circle: Stakeholder perspectives of a short-term intensive parent training programme delivered within the context of routine services for autism in China by Zuyi Fang, Jamie M Lachman, Cheng Zhang, Dongping Qiao and Jane Barlow in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: ZF’s involvement was partly funded by the Swire Charitable Trust. JML’s involvement was supported by the University of Glasgow Social and Public Health Sciences Unit Complexity and Relationships in Health Improvement Programs of the Medical Research Council MRC UK and Chief Scientist Office (Grant: MC_UU_00022/1 and CSO SPHSU16, MC_UU_00022/3 and CSO SPHSU18). The funders played no role in the design, conduct, or interpretation of the analyses.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.