
Abstract
It is widely believed that early diagnosis and treatment of autism spectrum disorder is essential for better outcome. This is demonstrated by the American Academy of Pediatrics recommendation to screen all 1.5–2.5-year-old toddlers for autism spectrum disorder. However, multiple longitudinal studies of children diagnosed with autism spectrum disorder at 1.5–6 years of age and treated in community settings have not reported any associations between earlier diagnosis and improved outcome in core symptoms. Here, we quantified Longitudinal changes in core autism spectrum disorder symptoms of 131 children diagnosed at 1.2–5 years of age using the Autism Diagnostic Observation Schedule–Second Edition Calibrated Severity Scores over a 1-2 year period. We examined the prevalence and magnitude of Calibrated Severity Scores changes across children who were diagnosed at different ages. The results revealed that age of diagnosis was significantly correlated with poorer outcome (r(129) = 0.41, p < 0.001). Approximately 65% of the children diagnosed before 2.5 years of age exhibited improvements in Autism Diagnostic Observation Schedule–Second Edition Calibrated Severity Scores (⩾2 points) in contrast to only 23% of the children diagnosed after this age. Changes in younger children were driven by improvements in social symptoms despite deterioration in restricted and repetitive behaviors. These findings reveal that autism spectrum disorder diagnosis before the age of 2.5 is associated with considerable improvement in social symptoms. We suggest that greater brain plasticity and behavioral flexibility enable younger children to benefit more from autism spectrum disorder interventions even in community settings with heterogeneous services. This motivates further prioritization of early autism spectrum disorder screening as recommended by American Academy of Pediatrics guidelines.
Lay abstract
It is widely believed that early diagnosis and treatment of autism spectrum disorder is essential for better outcome. This is demonstrated by the American Academy of Pediatrics recommendation to screen all 1.5–2.5-year-old toddlers for autism spectrum disorder. However, multiple longitudinal studies of children diagnosed with autism spectrum disorder at 1.5–6 years of age and treated in community settings have not reported any associations between earlier diagnosis and improved outcome in core autism spectrum disorder symptoms. In this study, we measured changes in core autism spectrum disorder symptoms over a 1–2-year period in 131 children diagnosed with autism spectrum disorder at 1.2–5 years of age, and treated in the community. The results revealed that children who were diagnosed before 2.5 years of age were three times more likely to exhibit considerable improvements in social autism spectrum disorder symptoms in comparison to children diagnosed at later ages. These results highlight the importance of early diagnosis and treatment of autism spectrum disorder even in community settings with heterogeneous services. In addition, these results motivate further prioritization of universal screening for autism spectrum disorder before 2.5 years of age.
Introduction
Earlier diagnosis of autism spectrum disorder (ASD) enables earlier access to ASD-interventions, which are thought to improve outcome (Hyman et al., 2020; Zwaigenbaum, Bauman, Choueiri, et al., 2015; Zwaigenbaum, Bauman, Stone, et al., 2015). A variety of studies have demonstrated that children with ASD younger than 3 years of age exhibit improvements, mostly in adaptive behaviors and cognitive abilities, following targeted ASD-interventions including applied behavioral analysis (ABA) (Reichow et al., 2018; Remington et al., 2007; Zachor et al., 2007) and the Early Start Denver Model (ESDM) (Dawson et al., 2010; Estes et al., 2015; Fuller et al., 2020). However, unlike results from highly controlled ASD-intervention studies, mostly carried out with small groups in academic settings (Reichow, 2012), intervention services in most communities (i.e. “treatment as usual”) have been associated with considerably weaker gains. In fact, it is unclear whether children with ASD in the community benefit at all from earlier diagnosis and intervention (Nahmias et al., 2019).
Indeed, several longitudinal studies of large community samples, with children diagnosed at 1.5–6 years of age, have not reported any association between the age of diagnosis and outcome in core ASD symptoms (Georgiades et al., 2021; Gotham et al., 2012; Kim et al., 2016, 2018; Szatmari et al., 2015; Venker et al., 2014; Waizbard-Bartov et al., 2021). These studies utilized Autism Diagnostic Observation Scale–Second edition (ADOS-2) (Lord et al., 2012) Calibrated Severity Scores (CSS), which enable assessment of changes in core ASD symptoms over time, regardless of the child’s age or language abilities (Esler et al., 2015; Gotham et al., 2009; Hus et al., 2014). They demonstrated that ADOS-2 CSS of children can change over a 1–4-year period such that 8%–33% of the children improve, 8%–36% deteriorate, and 31%–88% remain stable (Gotham et al., 2012; Kim et al., 2016, 2018; Szatmari et al., 2015; Venker et al., 2014; Waizbard-Bartov et al., 2021). This heterogeneity in outcomes, however, was not associated with the age of ASD diagnosis in any of the studies. Note that most of these studies focused on identifying distinct developmental trajectories of ASD symptoms rather than specifically comparing changes in core symptom severity across children diagnosed at different ages.
The potential benefits of early ASD diagnosis and treatment are at the heart of an ongoing debate regarding the necessity of universal screening for ASD in 1.5–2.5-year-old children (Coury, 2015; Mandell & Mandy, 2015; Powell, 2016). While the American Academy of Pediatrics (AAP) recommends screening for ASD at 18 and 24 months of age (Hyman et al., 2020), a US preventive services task force statement concluded that there was insufficient evidence to assess the benefits or harms of screening for ASD at 18–30 months of age (Siu, 2016). Demonstrating significant benefits in the outcome of children with ASD who were diagnosed and treated before 2.5 years of age would provide further motivation for early screening. To determine whether children with ASD in a community setting benefit from earlier diagnosis, we followed the development of 131 children diagnosed at 1.2–5 years of age and examined whether children diagnosed earlier exhibited larger improvements in ADOS-2 CSS.
Methods
Setting and procedure
Families were recruited at the National Autism Research Center of Israel (NARCI) between 2017 and 2019. NARCI is located inside Soroka University Medical Center (SUMC) where approximately 150 children are diagnosed with ASD annually. SUMC is the only clinical center where children insured by the Clalit HMO (who cover 70% of the population in southern Israel) can receive an ASD diagnosis, thereby yielding a representative community sample of this geographical area (Dinstein et al., 2020; Meiri et al., 2017). ASD symptoms were assessed with the ADOS-2 (Lord et al., 2012) and cognitive abilities were assessed with the Bayley Scales of Infant Development–Third Edition (Viezel et al., 2014) or the Wechsler Preschool and Primary Scale of Intelligence (WPPSI) (Luiselli et al., 2013). All ADOS-2 assessments were administered according to guidelines, by the same trained clinician who has research reliability. Follow-up assessments were recommended to all families, 1–2 years after diagnosis, and were completed by approximately 40% of the children. This study included all children who completed a follow-up ADOS-2 assessment within the specified period. There was no community involvement in the design or interpretation of this study.
Participants
We examined data from 131 children with ASD who were 2.6 years old, on average, at diagnosis and 4.1 years old, on average, at follow-up (Table 1). We compared children who were diagnosed <2.5 years old (younger group) and those diagnosed ⩾2.5 years old (older group). This cutoff was selected because it corresponds to the upper age limit of early screening recommendations (Siu, 2016). All children fulfilled ADOS-2 and the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for ASD as determined by both a developmental psychologist and either a child psychiatrist or pediatric neurologist. The diagnostic procedure included four visits to SUMC including an initial intake meeting with a developmental psychologist or social worker, an ADOS-2 assessment performed by a speech therapist with research reliability, a cognitive assessment performed by a developmental psychologist, and a final diagnosis meeting with a physician. Parents of all children provided informed consent, and the study was approved by the SUMC Helsinki Committee.
Characteristics of the children who participated in this study.
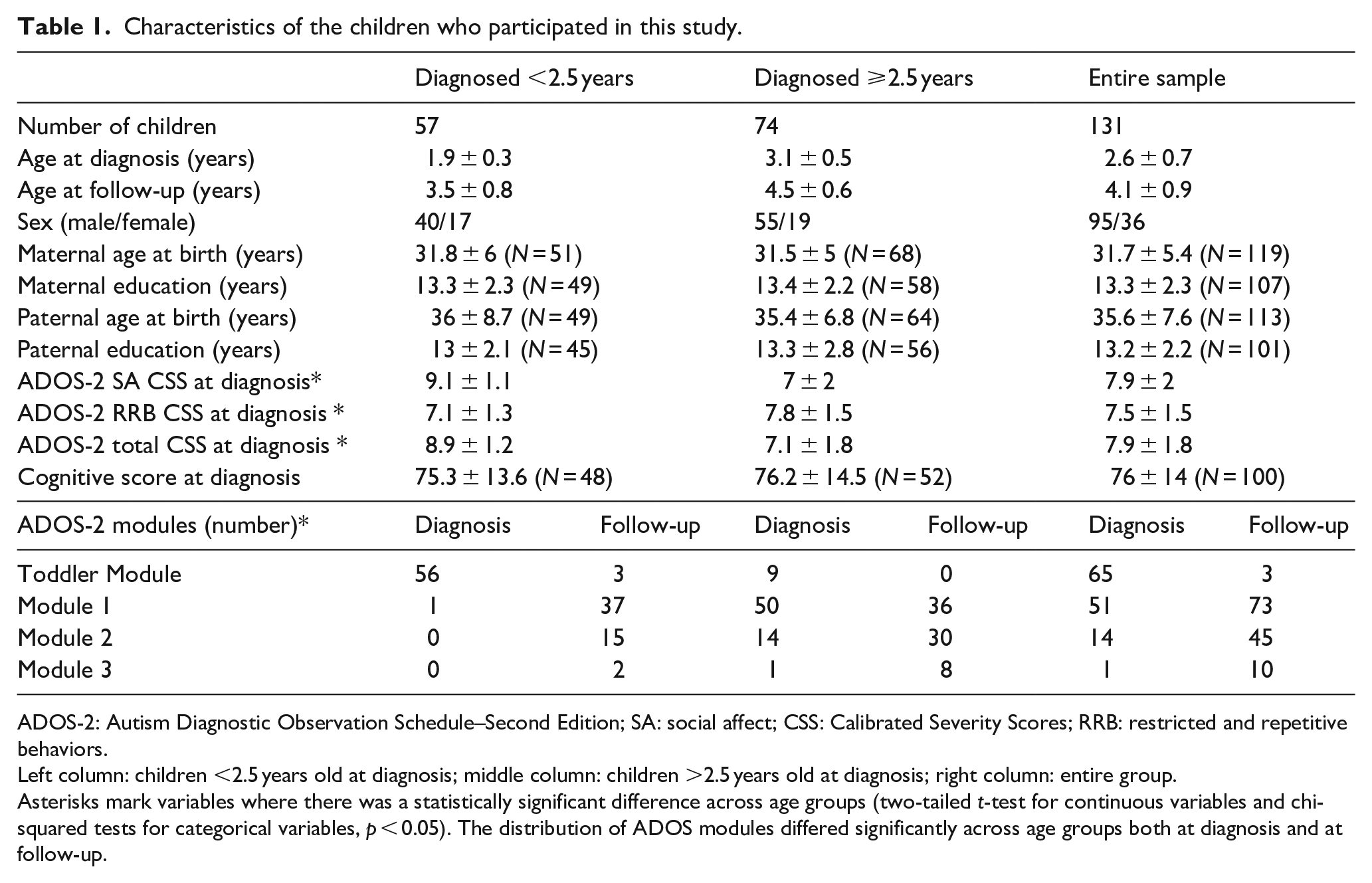
ADOS-2: Autism Diagnostic Observation Schedule–Second Edition; SA: social affect; CSS: Calibrated Severity Scores; RRB: restricted and repetitive behaviors.
Left column: children <2.5 years old at diagnosis; middle column: children >2.5 years old at diagnosis; right column: entire group.
Asterisks mark variables where there was a statistically significant difference across age groups (two-tailed t-test for continuous variables and chi-squared tests for categorical variables, p < 0.05). The distribution of ADOS modules differed significantly across age groups both at diagnosis and at follow-up.
Longitudinal change in ADOS scores
ADOS-2 CSS enable comparison of ASD severity across time-points as children grow older and are evaluated with different ADOS modules (Esler et al., 2015; Gotham et al., 2009; Hus et al., 2014). We calculated the difference between the ADOS CSS at follow-up and diagnosis (i.e. Change = follow-up − diagnosis), such that negative values indicated improvement (i.e. decrease in symptom severity). Following a similar recent study (Waizbard-Bartov et al., 2021), we classified children with changes greater than −/+2 ADOS-2 CSS points into groups that improved/deteriorated in symptom severity, respectively. This change threshold was selected because it corresponds to approximately one standard deviation of the ADOS-2 CSS in our entire sample at diagnosis (Table 1) and in samples reported by other studies (Szatmari et al., 2015; Venker et al., 2014; Waizbard-Bartov et al., 2021). We also performed analogous calculations separately for the social affect (SA) and the restricted and repetitive behaviors (RRB) domains using their respective CSS scales (Esler et al., 2015; Hus et al., 2014).
Baseline measures, intensity of intervention, and type of educational framework
Scores from cognitive assessments at diagnosis were available for 100 of the children (Table 1). In the remaining cases, children did not complete cognitive testing due to low cooperation with the clinician or missed appointments. Information regarding parental education and age was available for more than 100 of the children (Table 1). Parents of 78 children (34 children in the younger group and 44 children in the older group) completed a follow-up questionnaire within 3 months of the follow-up ADOS-2 assessment. Parents reported the average number of weekly treatment hours that the child received since their diagnosis including speech therapy, psychological treatments, occupational therapy, and developmental or behavioral interventions. In addition, parents indicated whether their child was in a special or mainstream/inclusive education setting. There were no significant differences in the ADOS-2 CSS longitudinal changes of children for whom data were missing and those for whom the data was complete (Table S1). Data regarding socioeconomic status and ethnic origin were not recorded.
Statistical analyses
Statistical analyses were performed using SPSS (Version 26.0) and Rstudio (Version 1.1.463). Comparisons of continuous variables across groups were performed with two-sample, two-tailed, t-tests, assuming equal variance across groups. We used Levene’s test to identify groups with unequal variance and in these cases performed t-tests assuming unequal variance. We calculated Cohen’s d to assess effect sizes and Pearson’s correlation coefficients to assess the relationships between continuous variables. Chi-square analyses were used to compare proportions across groups. We performed an analysis of covariance (ANCOVA) analysis to assess whether ADOS-2 SA CSS changes differed significantly across children diagnosed early and late, while controlling for their sex, initial cognitive scores, initial ADOS-2 SA CSS, and length of time between diagnosis and follow-up. This analysis was performed with 100 children for whom all data were available. Statistical significance was set to a p-value of 0.05 for all tests.
Results
The age of diagnosis was significantly correlated with longitudinal change in ADOS-2 CSS (r(129) = 0.41, p < 0.001, Figure 1) such that children diagnosed earlier exhibited larger improvements over time (i.e. more negative ADOS-2 CSS changes). Separating the ADOS-2 CSS into its SA and RRB components revealed a clear dissociation such that children diagnosed earlier exhibited significantly larger improvements in ADOS-2 SA CSS (r(129) = 0.44, p < 0.001), and also exhibited a trend for larger deterioration in ADOS-2 RRB CSS (r(129) = −0.12, p = 0.18).
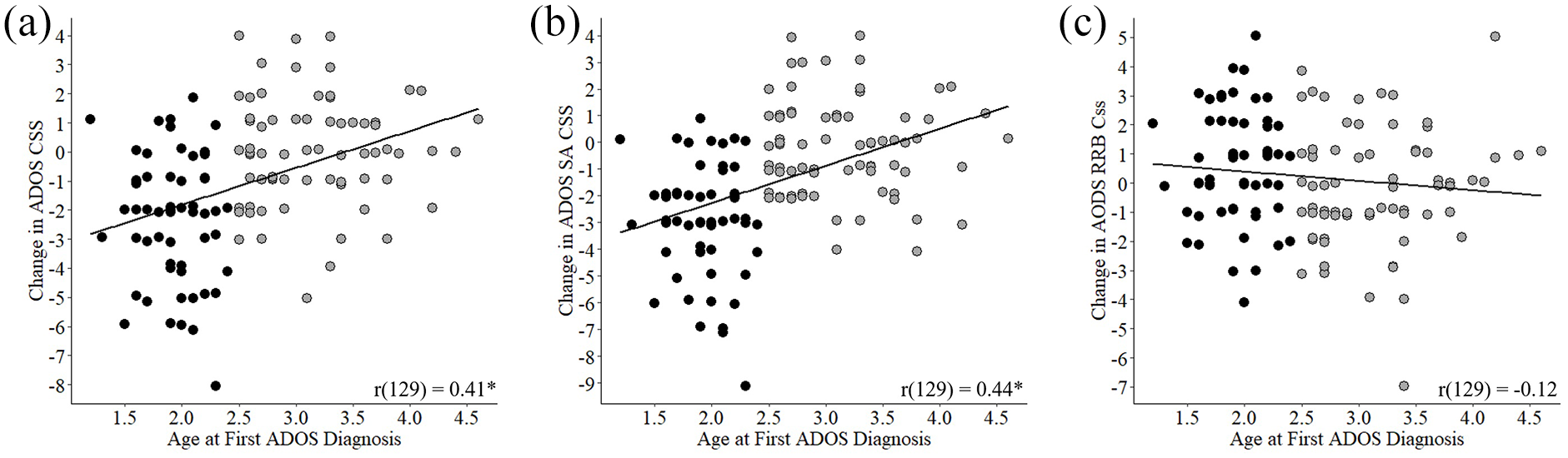
Longitudinal changes in ADOS-2 CSS versus age of diagnosis. Scatter plots presenting longitudinal change in ADOS-2 CSS versus age of diagnosis. Negative changes indicate improvement in ASD severity over time. (a) Change in total ADOS-2 CSS. (b) Change in ADOS-2 SA CSS. (c) Change in ADOS-2 RRB CSS. Each point represents a single child. Black: children diagnosed <2.5 years of age. Gray: children diagnosed >2.5 years old. Line: least squares fit. Asterisk: significant Pearson’s correlation (p < 0.05).
To further assess the importance of early diagnosis, we separated children into those diagnosed before 2.5 years-old (younger group) and after (older group). Most baseline measures were similar across the two groups (Table 1). There were no significant between-group differences in parental age at birth (t < 0.46, p > 0.73), parental education levels (t > −0.62, p > 0.53), or sex (χ2(1, N = 131) = 0.11, p = 0.74). There were also no significant differences in cognitive scores (t(98) = −0.3, p = 0.77) or in the amount of children who completed cognitive testing (χ2(1, N = 131) = 2.74, p = 0.09). Total ADOS-2 CSS, however, were significantly higher in the younger group (t(126.4) = 6.68, p < 0.001, d = 1.12), as were the ADOS-2 SA CSS (t(114) = 7.79, p < 0.001, d = 1.27). In contrast, ADOS-2 RRB CSS were significantly lower in the younger group (t(129) = −2.66, p = 0.01, d = −0.47). Hence, younger children exhibited more severe SA symptoms and less severe RRB symptoms at diagnosis.
Changes in ADOS-2 CSS over time
We quantified the prevalence and magnitude of longitudinal ADOS-2 CSS changes in each of the groups (Figures 2 and 3). The percentage of children who exhibited improvements (i.e. ADOS-2 CSS decreased by ⩾2 points) was significantly higher in the younger group (65%) compared to the older group (23%, χ2(1, N = 131) = 21.7, p < 0.001). ADOS-2 CSS improvement was significantly larger in the younger group (M = −2.3, standard deviation (SD) = 2.2) compared to the older group (M = −0.07, SD = 1.9, t(129) = −6.26, p < 0.001, d = −1.1). The younger group improved in SA CSS (M = −2.95, SD = 2.1) significantly more than the older group (M = −0.19, SD = 1.8; t(129) = −8.01, p < 0.001, d = −1.4), but deteriorated in RRB CSS (M = 0.63, SD = 1.93) significantly more than the older group (M = −0.16, SD = 2; t(129) = 2.2, p = 0.03, d = 0.4).
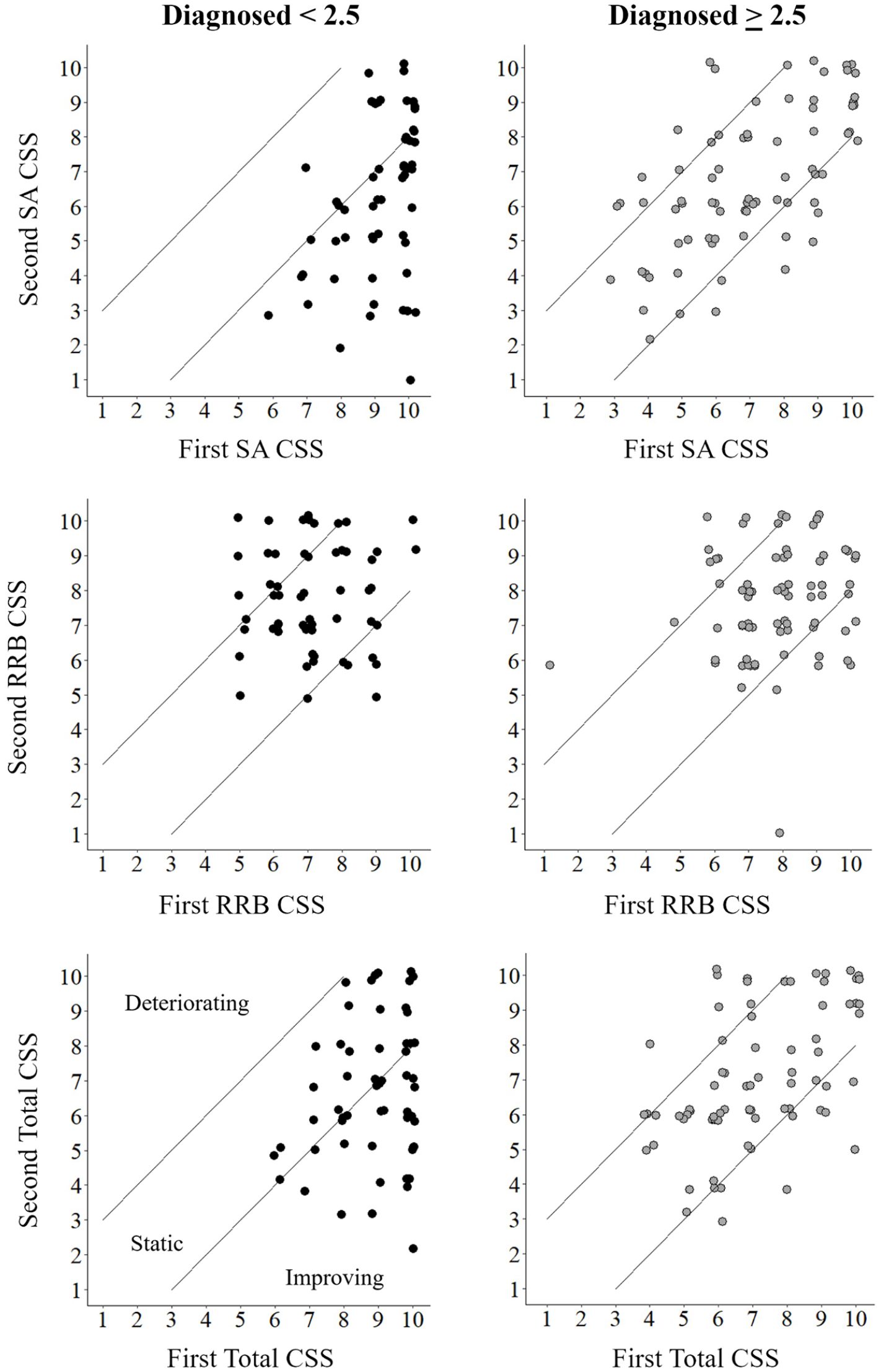
Individual changes in ADOS CSS between diagnosis and follow-up. Scatter plots demonstrate the change in ADOS-2 CSS of individual children between diagnosis and follow-up assessments. Top row: ADOS-2 SA CSS. Middle row: ADOS-2 RRB CSS. Bottom row: total ADOS-2 CSS. Left column: children diagnosed <2.5 years old. Right column: children diagnosed >2.5 years old. Diagonal lines: upper and lower boundaries of considerable change across assessments (+/− 2 points on the ADOS-2 CSS). Children located between the lines remained static (i.e. changed <2 points) while children above the top line deteriorated considerably and children below the bottom line improved considerably. Each point represents a single child.
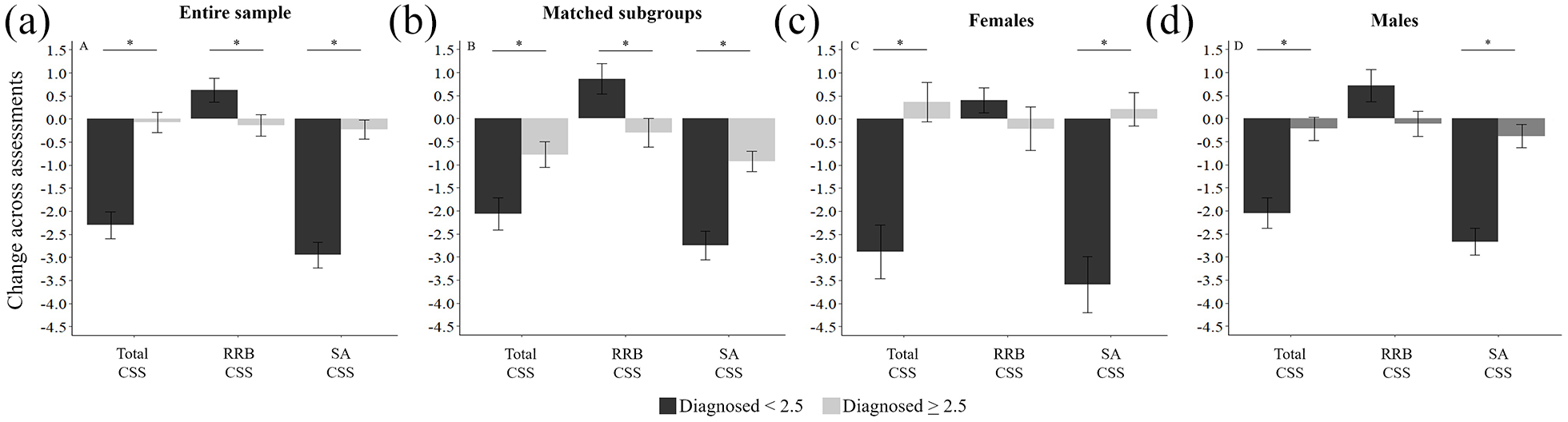
Magnitude of changes in ADOS CSS. Comparison of the magnitude of ADOS-2 CSS changes across age groups. (a) Results from the entire sample. (b) Results from subgroups of children matched on sex and initial ADOS-2 severity. (c) Females only. (d) Males only. Each panel contain the comparisons of the total ADOS CSS (left), RRB CSS (middle), and SA CSS (right). Black: children diagnosed <2.5 years old; gray: children diagnosed >2.5 years old; asterisk: significant difference across groups (two-tailed t-test, p < 0.05).
Comparison of matched subgroups
To ensure that our results were not due to differences in ASD severity at diagnosis, we analyzed a subset of 36 children from each group who were matched on sex and had identical ADOS-2 CSS at diagnosis. This revealed equivalent results to those reported above (Figure 3). Improvement in total ADOS-2 CSS was significantly larger in the younger group (t(70) = −2.82, p = 0.006, d = −0.66) and was driven by a significantly larger improvement in SA CSS (t(70) = −4.8, p < 0.001, d = −1.13), despite a significantly larger deterioration in RRB CSS (t(70) = 2.58, p = 0.01, d = 0.6).
Comparison across boys and girls
Separating male and female children yielded equivalent results (Figure 3). Improvement in total ADOS-2 CSS was significantly larger in the younger group in males (t(93) = −4.48, p < 0.001, d = −0.93) and females (t(34) = −4.57, p < 0.001, d = −1.53). This was driven by significantly larger improvements in SA CSS of males (t(93) = −5.99, p < 0.001, d = −1.24) and females (t(34) = −5.47, p < 0.001, d = −1.82), despite a non-significant trend for larger deterioration in RRB CSS of males (t(93) = 1.91, p = 0.06) and females (t(34) = 1.11, p = 0.27).
Initial symptom severity
Significant negative correlations were apparent between the ADOS-2 CSS at diagnosis and their change over time (Figure 4) in both the younger (r(55) = −0.38, p = 0.003) and older (r(72) = −0.44, p < 0.001) groups. This indicated that children with more severe initial symptoms improved to a larger extent in both groups. In contrast, initial cognitive scores were not significantly correlated with changes in ADOS-2 CSS in the younger (r(46) = −0.03, p = 0.82) or older (r(50) = 0.01, p = 0.95) groups.
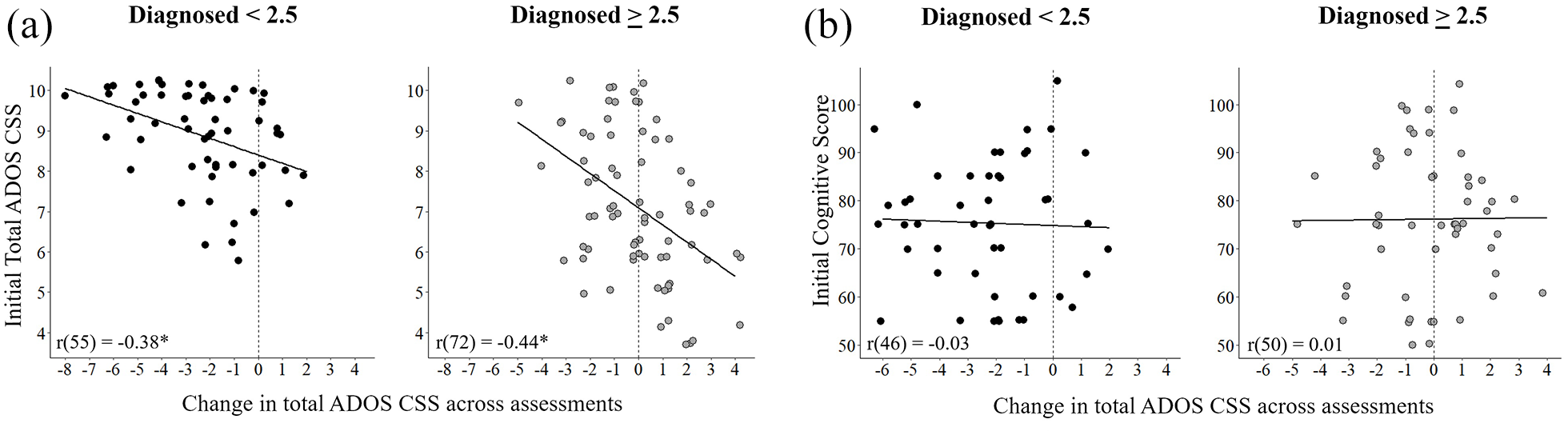
Predictors of change in ADOS CSS. (a) Scatter plots demonstrating the relationship between initial ADOS CSS and change in ADOS CSS for the younger (left) and older (right) groups. (b) Scatter plots demonstrating the relationship between initial cognitive scores and change in ADOS CSS for the younger (left) and older (right) groups. Pearson’s correlation coefficients are noted in each panel. Line: least squares fit; asterisk: significant correlation (p < 0.05).
Parental characteristics and time across assessments
We did not find any significant correlations between the magnitudes of change in ADOS-2 CSS and parental characteristics in either group, including maternal (r < 0.25, p > 0.07) and paternal (r > −0.16, p > 0.26) age at birth or maternal (r < 0.14, p > 0.35) and paternal (r < −0.09, p > 0.5) education. Magnitudes of change in ADOS-2 CSS were also not correlated with the amount of time between ADOS-2 assessments in either group (r < 0.12, p > 0.3).
Treatment intensity and type of educational setting
There was no significant difference between the number of parent-reported weekly treatment hours (i.e. treatment intensity) in the younger (M = 3.5, SD = 3.5) and older group (M = 2.78, SD = 2.16, t(52.71) = 1.08, p = 0.28). Furthermore, the percentage of younger children who were placed in special versus inclusive education settings (76% vs 24%, respectively) was nearly identical to that of the older children (77% vs 23%, χ2(1, N = 78) = 0, p = 1).
Combined analysis
In a final ANCOVA analysis, we tested whether longitudinal changes in ADOS-2 SA CSS differed across the two age groups when accounting for the children’s sex, cognitive score at diagnosis, ADOS-2 SA CSS at diagnosis, and the length of time between diagnosis and follow-up. This analysis demonstrated that significant differences between children diagnosed early and late (F(1,94) = 18.52, p < 0.001,
Discussion
Our results demonstrate that children with ASD who were diagnosed earlier exhibited a larger reduction in the severity of social ASD symptoms within 1–2 years. Specifically, children diagnosed before 2.5 years of age were nearly three times more likely to exhibit considerable reductions in the severity of social symptoms as compared with children diagnosed at older ages. Equivalent results were evident when examining boys and girls, suggesting that boys and girls benefit similarly from early diagnosis. Furthermore, equivalent results were evident when accounting for initial ASD severity and cognitive abilities using an ANCOVA analysis and when comparing subgroups of children who were strictly matched on initial ASD severity and sex.
These findings are particularly encouraging given that participating children received heterogeneous clinical and educational services (i.e. “treatment as usual”) that were available in their community. To the best of our knowledge, children diagnosed at younger ages did not receive different services from those diagnosed at older ages. Both age groups exhibited equivalent placement ratios in special versus inclusive educational settings, and there was no significant difference in the number of treatment hours per week reported by parents. Taken together, these results reveal that early ASD diagnosis is associated with better outcome, even in a community setting where children receive heterogeneous services. Hence, these findings strengthen the motivation to screen for ASD at 18–30 months of age in order to reduce the mean age of ASD diagnosis (e.g. Guthrie et al., 2019), which often occurs after 4 years of age (Constantino et al., 2020; Kerub et al., 2020; Sheldrick et al., 2017).
Early diagnosis, early intervention, and improved outcome
Previous studies, typically performed in university settings, have reported that early intervention with structured programs such as ABA (Remington et al., 2007; Zachor et al., 2007) or ESDM (Dawson et al., 2010; Estes et al., 2015) are effective in improving social functioning, cognitive abilities, and adaptive behaviors of children with ASD. Clinical and educational care in the community, however, tends to be less structured and more variable, yielding poorer improvements over time (Nahmias et al., 2019).
Several large longitudinal studies have reported that between the ages of 1.5 and 6 years, only 8%–33% of children with ASD exhibit improvements in ADOS-2 CSS while the vast majority remain stable or deteriorate over time (Gotham et al., 2012; Kim et al., 2016, 2018; Szatmari et al., 2015; Venker et al., 2014; Waizbard-Bartov et al., 2021). Most importantly, these studies did not report any significant relationship between the magnitude of improvement in core ASD symptoms and the age of diagnosis. Our results were in line with some of these studies in demonstrating relatively modest rates of improvement in ADOS-2 CSS scores of children diagnosed after 2.5 years of age (i.e. 23%). However, in our sample, improvement in ADOS-2 CSS of children diagnosed before 2.5 years of age was almost three times as prevalent (i.e. 65%).
We believe that this considerable difference in the outcome of children diagnosed early was revealed in our study for two main reasons. First, we examined children who were diagnosed at earlier ages than those included in most previous studies. Only two previous studies have assessed changes in ADOS CSS of children diagnosed before the age of 2 years old (Kim et al., 2016, 2018). Second, this study specifically focused on the relationship between age of diagnosis and changes in symptom severity while all previous studies focused on the identification of distinct sub-types of ASD developmental trajectories. All of the studies noted above performed clustering analyses to identify sub-groups children with distinct initial ASD characteristics (e.g. Kim et al., 2016), or distinct changes in symptoms over time (e.g. Szatmari et al., 2015). In contrast, in our study, we specifically compared outcome across children diagnosed before and after 2.5 years of age.
Furthermore, our analyses revealed that the substantial improvement in ADOS-2 CSS of younger children was driven by even larger improvements in their SA CSS, despite deterioration in their RRB CSS (Figure 3). It has been reported that SA symptoms are easier to identify at early ages in contrast to RRB symptoms (MacDonald et al., 2007; Mishaal et al., 2014; Mooney et al., 2006). In addition, most early intervention protocols focus on improving SA impairments rather than RRB symptoms (Brian et al., 2017; Dawson et al., 2010; Harrop et al., 2017). We suggest that easier identification of SA symptoms and a stronger intervention focus on these symptoms may explain the substantial improvement in their severity despite a deterioration in RRB symptoms in younger children. These findings are in line with studies demonstrating that SA and RRB symptoms change independently over time (Fountain et al., 2012; Harrop et al., 2014) and motivate the development of early interventions that address RRB symptoms and effectively decrease their severity.
Treatment as usual in Israel
In Israel, parents can place children with ASD either in special education classes, which include eight ASD children who are cared for by a relatively large professional staff, or in inclusive education, where the child is accompanied by an aid to classes with up to 30 typically developing children. Eclectic combinations of ABA (Reichow, 2012; Zachor et al., 2007), Floortime/DIR (Mercer, 2017), NDBA (Schreibman et al., 2015), and TEACCH (Virues-Ortega et al., 2013) techniques are implemented in the majority of special education classes and in a minority of inclusive education classes. In addition, all children with ASD are eligible for 3 weekly hours of government-funded therapy from a speech therapist, occupational therapist, psychologist, and/or physical therapist. This demonstrates the large heterogeneity of clinical and educational services that children with ASD receive in most Western countries (Nahmias et al., 2019). The main contribution of this study is in quantifying the benefit of early diagnosis apparent despite this heterogeneity.
Brain plasticity and maturation
In line with previous proposals (Dawson, 2008), we believe that the benefit of early ASD diagnosis is due to the application of targeted ASD-interventions during early periods of development where brain plasticity and behavioral flexibility are at their peak. Early developmental periods with extensive exploration, behavioral flexibility, and remarkable capacity for learning are followed by maturation, which reduces plasticity and flexibility in order to solidify knowledge (e.g. language in humans (Gervain, 2015) or singing in birds (London, 2019)). Our results suggest that intervening before 2.5 years of age is important for taking advantage of early flexibility in the development of social capabilities.
An interesting alternative explanation is that better outcome in younger children may be due to natural maturation (i.e. spontaneous improvements) rather than early intervention. We cannot rule out this explanation because we did not measure longitudinal changes in children who were diagnosed early and did not receive any intervention. Nevertheless, we believe that this alternative explanation is unlikely for two reasons. First, numerous studies have shown that early interventions, administered at 18–30 months of age, are effective in improving social symptoms, adaptive behaviors, and cognitive abilities of children with ASD (Zwaigenbaum, Bauman, Choueiri, et al., 2015). This has motivated governments to establish early ASD-intervention services at considerable cost (Manning et al., 2011; Piccininni et al., 2017). Second, studies of infants at high risk of developing ASD have demonstrated that most children who develop ASD exhibit continuous decline relative to typically developing peers during their second year of life (Landa & Garrett-Mayer, 2006; Ozonoff et al., 2016). Hence, spontaneous improvements without intervention are unlikely.
Limitations
This study had several limitations. First, we assessed changes in outcome using only the ADOS-2 CSS, which involves a limited clinical observation. Corroborating the clinical impression with parent and teacher reports may further strengthen the reported findings. Second, in addition to the ADOS-2 assessments, a more comprehensive evaluation of outcome should include additional measures of cognitive abilities, language abilities, and adaptive behaviors, which are known to improve significantly following early intervention (Dawson et al., 2010; Estes et al., 2015; Zachor et al., 2007) and were not included in this study. Third, we estimated the intensity of early intervention services with parent reports that did not address the type or quality of intervention, which are likely to explain additional variability in longitudinal ADOS-2 CSS changes. While parents of younger children did not report that their children received more services, we acknowledge that community services may be more readily allocated to children with more severe symptoms as reported by some studies (Kim et al., 2016). Finally, since the selection of appropriate ADOS-2 module is dependent on the age and language abilities of the child, we acknowledge that children diagnosed before 2.5 years of age were assessed with distinct ADOS-2 modules than those used with the children who were diagnosed at later ages. Hence, the conclusions of this study are reliant on the accuracy of the calibrated severity scores that have been developed to enable comparisons across modules (Esler et al., 2015; Gotham et al., 2009; Hus et al., 2014).
Conclusion
This study demonstrates that diagnosis of ASD before 2.5 years of age is associated with considerable benefits for children diagnosed within a community setting. While reliable ASD diagnoses can be performed during the second year of life (Steiner et al., 2012), most diagnoses are currently performed after the age of four (Constantino et al., 2020; Kerub et al., 2020; Sheldrick et al., 2017). This study offers strong evidence in support of calls to reduce the age of ASD diagnosis and intervention in the community as an imperative initial step for improving clinical outcomes in children with ASD (Klin et al., 2020).
Supplemental Material
sj-docx-1-aut-10.1177_13623613211049011 – Supplemental material for Early diagnosis of autism in the community is associated with marked improvement in social symptoms within 1–2 years
Supplemental material, sj-docx-1-aut-10.1177_13623613211049011 for Early diagnosis of autism in the community is associated with marked improvement in social symptoms within 1–2 years by Nitzan Gabbay-Dizdar, Michal Ilan, Gal Meiri, Michal Faroy, Analya Michaelovski, Hagit Flusser, Idan Menashe, Judah Koller, Ditza A Zachor and Ilan Dinstein in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by a National Autism Knowledge Center grant from the Israeli Ministry of Science and Technology awarded to I.D., I.M., and G.M.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.