
Abstract
Anti-Black racism is a pervasive issue in the autism field that affects the autism service pathway, which ranges from identification of concerns to ongoing service navigation. In this short report, we provide a working model of the autism service pathway and highlight ways in which anti-Black racism affects all components of the pathway. We summarize the literature that demonstrates the effects of racism within autism assessment, treatment, and quality of care. We end with six recommendations for systemic change that clinicians can take: (1) including and amplifying Black autistic voices within their organization, (2) continuously learning about and acknowledging the ways in which their discipline perpetuates anti-Black racism, (3) recognizing that cultural humility is a lifelong process, (4) being mindful of the complex pathway that families must navigate to receive autism services, particularly when working with Black individuals, and (5) advocating for system-level changes within their organization and refining changes that are made.
Lay abstract
Black autistic people experience anti-Black racism when interacting with service systems and the clinicians in those systems. In this article, we describe the various steps families take to get services and how anti-Black racism makes that process even harder. We discuss research that shows the negative effects of anti-Black racism in autism assessment, treatment, and quality of care. We then provide five recommendations that clinicians should follow to reduce anti-Black racism in the autism field: (1) find Black autistic people and listen to their opinions about your organization, (2) always keep learning about how your profession promotes anti-Black racism, (3) recognize that the process of a clinician learning to be culturally humble takes time and is never “complete,” (4) pay attention to all of the steps that families must take to receive autism services and how these steps are even harder for Black individuals, and (5) advocate for your organization to make systems-level changes in their policies and procedures.
Keywords
Introduction
The current service system has failed Black individuals on the autism spectrum and their families. As gatekeepers to the service system, clinicians have a responsibility to understand how anti-Black racism influences access to quality assessment, accurate and timely diagnosis, autism-related services, and high-quality care for Black individuals on the autism spectrum. The impact of anti-Black racism has significant ramifications on the autism spectrum disorder (ASD) service pathway. In order to illustrate how anti-Black racism is infused throughout the service system, we developed a model to illustrate the autism service system pathway, expanding upon the figure developed by Children’s Hospital of Pennsylvania (Figure 1; adapted from Levy et al., 2015).
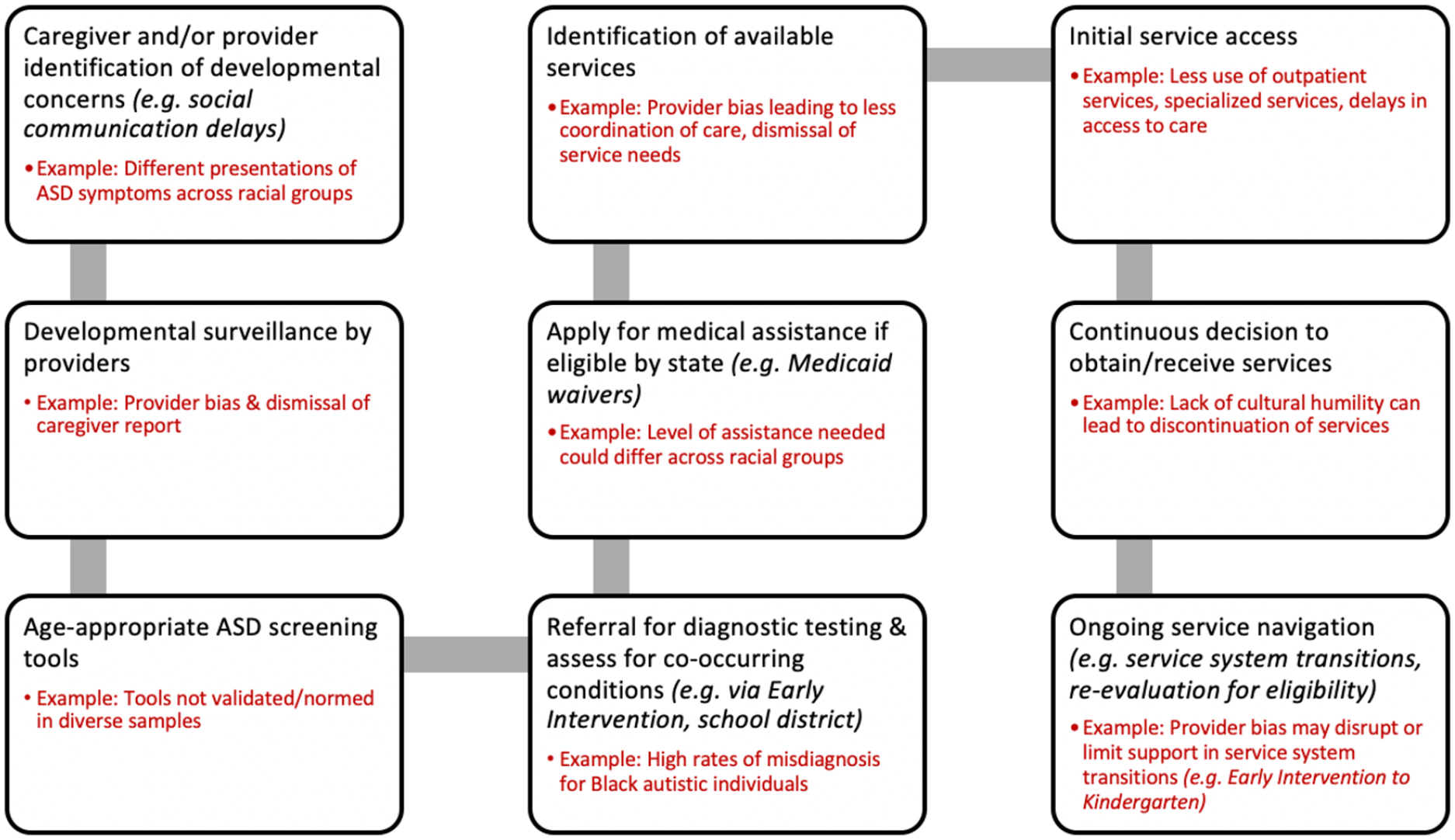
Pathway to access and utilize autism services, including examples of anti-Black racism. Adapted from Levy et al. (2015). Primary Care Clinical Pathway for Autism Screening and Referral, Children’s Hospital of Pennsylvania, https://www.chop.edu/clinical-pathway/autism-screening-and-referral-clinical-pathway.
We must borrow from anti-racist and feminist approaches to healthcare to adequately meet the needs of our Black clients. For example, practitioners may look to models such as the Critical Consciousness of Anti-Black Racism model (CCABR; Mosley et al., 2021) to inform clinical practices with Black autistic individuals. CCABR stems from both critical-ideological and Black feminist-womanist approaches to provide Black and non-Black individuals with a framework for witnessing, processing, and actively responding to anti-Black racism. While this model was initially developed for Black individuals, it has been recommended that practitioners utilize this model to support Black clients in preventing and resisting racial trauma, and to engage in assessment and treatment associated with racial trauma.
In addition, models such as CCABR highlight the need for practitioners to approach clinical work with cultural humility, a process of self-reflection that includes examining one’s own beliefs and cultural identities and having curiosity and genuine regard for other cultures (Foronda et al., 2016). Moreover, we must respect intersectionality, a framework for understanding the ways in which multiple social identities (e.g. race and disability status) overlap (Crenshaw, 1989). The intersectionality of being autistic and holding additional marginalized identities uniquely impacts quality of life and health outcomes for Black individuals on the spectrum (Bishop-Fitzpatrick & Kind, 2017). By utilizing models such as CCABR, embracing a culturally humble approach, and positioning intersectionality at the forefront of our clinical work, we may advance our efforts to improve access to care for Black individuals on the autism spectrum. This call to action challenges clinicians to serve Black families in a culturally humble manner throughout each step of this service system pathway.
Positionality and community involvement
Both authors hold master’s degrees in psychology and identify as cisgender heterosexual women of color pursuing doctorate degrees in clinical psychology. The first author, D.S., identifies as a multiracial Afro-Latina woman (Dominican and White), and the second author, A.S., identifies as an immigrant Southeast Asian woman. As clinical trainees, both authors provide assessment and psychotherapy services to autistic individuals in a university-affiliated community clinic in the Midwest. This Short Report was adapted from a presentation developed by both authors that was provided to an audience of clinicians and researchers within an academic department at a public university. There are no individuals in the department who have self-disclosed that they identify as autistic; thus, to the best of the authors’ knowledge, no autistic individuals were involved in preparing and/or providing feedback on the presentation that was then adapted for this Short Report.
Assessment and diagnostic considerations
Anti-Black racism significantly impacts the assessment/diagnostic process for Black autistic people. There are high rates of misdiagnosis for Black children on the spectrum. For example, Black autistic children are 2.6 times more likely to be misdiagnosed than White autistic children, including being more likely to receive a misdiagnosis of adjustment disorder or conduct disorder (Mandell et al., 2007). However, despite Common misconceptions regarding race and externalizing behaviors, research illustrates that Black autistic children are not more likely to have externalizing behaviors (e.g. aggression and hyperactivity) than White children on the spectrum (Sell et al., 2012). Black children are also more likely to be diagnosed when displaying clinical presentations of ASD that require more substantial support; this may be due to limited identification of those who require less support, highlighting how racial stereotyping and anti-Black racism impacts accurate diagnosis for this population (Jarquin et al., 2011). In addition, research consistently shows delays in ASD diagnosis that can take between 1.5 and 3 years between age of concern and age of diagnosis for Black children (Mandell et al., 2002). Black caregivers report longer wait times and three times the number of provider visits to receive a diagnosis compared to their White counterparts, and Black children are diagnosed with ASD later than White counterparts despite similar clinical presentations at the time of assessment (Constantino et al., 2020; Fombonne & Zuckerman, 2021). Overall, research suggests that disparities in the ASD assessment/diagnostic process may be largely attributed to anti-Black racism in the form of misconceptions and racial stereotypes, which then impede accurate assessment and diagnosis for Black autistic children.
ASD providers often attribute delays in diagnosis to parents’ lack of resources or motivation to seek services, while many Black parents attribute diagnostic delays and misdiagnosis to providers’ racial biases (Burkett et al., 2017; Dababnah et al., 2018). Indeed, Black caregivers of autistic children highlight their willingness and ability to prioritize their child’s needs and advocate across multiple systems to seek services for their child (Burkett et al., 2017; Lovelace et al., 2018). Many Black families of children on the spectrum discuss taking necessary steps to protect their child from harm in the healthcare system, taking action to ensure their child receives the best healthcare possible, and facing numerous barriers when seeking healthcare services for their children, including racial discrimination such as dismissal by providers (Burkett et al., 2017; Dababnah et al., 2018; Lovelace et al., 2018).
Importantly, many Black caregivers of autistic children emphasize the provider–caregiver relationship, expressing their belief that stronger relationships help parents feel their child is protected in the healthcare setting (Burkett et al., 2017). Furthermore, the process of shared decision-making (e.g. parents and providers jointly making decisions related to the assessment process) between parents and providers can drive accurate ASD detection and diagnosis (Sheldrick et al., 2019), highlighting the importance of increased collaboration between parents and providers. Overall, accurate and timely assessment and diagnosis are critical for families of autistic individuals, as early intervention is associated with significant improvements and can significantly improve short- and long-term outcomes. Therefore, addressing anti-Black racism in the diagnostic process should be a priority for ASD researchers and clinicians to meet the needs of Black autistic individuals.
Access to healthcare services and quality of care
For many autistic individuals, the ultimate goal of the diagnostic process is to provide access to healthcare services that may improve their quality of life. As depicted in Figure 1, experiences of racism earlier in the pathway have downstream effects on service access and utilization. Unfortunately, anti-Black racism directly affects service access and quality of care for Black individuals on the spectrum, and this can occur across multiple systems of care (i.e. education, medical, and behavioral health). Given that ASD healthcare services occur across numerous systems of care, Black caregivers must navigate many groups of providers who have limited training in cultural humility.
Trends in service utilization demonstrate additional disparities for children of color beyond those seen in the diagnostic process. Overall, Black and Latinx/Hispanic families, families of lower-income backgrounds, and families in rural areas utilize less services and are delayed in accessing services (Smith et al., 2020). Black and Latinx/Hispanic children are also less likely to access specialty services (e.g. neuropsychiatric testing) and more likely to have difficulty accessing acute care compared to White autistic children (Smith et al., 2020). Black autistic children are also less likely to see gastroenterologists, nutritionists, neurologists, psychiatrists, and psychologists (Smith et al., 2020). These disparities are worse when families of color are multiply marginalized due to being from lower-income backgrounds; Medicaid-enrolled children of Black, Asian, and Native American/Pacific Islander backgrounds receive fewer outpatient, autism-related services (e.g. outpatient psychotherapy, wraparound services) compared to White children (Bilaver et al., 2021). These disparities add additional barriers to an already complicated pathway to healthcare services.
Just as Black families must interact with a racist service system that perpetuates diagnostic and service disparities, they also experience poor quality of care once they actually access services. Black caregivers experience racist interactions with clinicians when receiving healthcare services (Jones et al., 2020). Black families report lower quality of autism-related care which they attribute to dismissal of parent concerns due to racial bias from clinicians (Stahmer et al., 2019). Black families also report less access to quality healthcare (e.g. access to a doctor who listens carefully to concerns; Bishop-Fitzpatrick & Kind, 2017). A recent systematic review demonstrated that autistic individuals from Black and Hispanic/Latinx backgrounds and those from low-income backgrounds report lower quality of care compared to White autistic individuals; these families also report that their providers lack knowledge and sensitivity regarding their culture (Smith et al., 2020). Autistic individuals note that the lack of cultural humility of autism clinicians is a major challenge to accessing and utilizing services for Black autistic people that contributes to disparities in quality of care (Jones et al., 2020). These disparities result in sub-optimal care and quality of life for these families.
Recommendations for systematic change
Clinicians who service individuals on the autism spectrum have a duty to educate themselves about the intersection of anti-Black racism and autism services. We must learn about anti-Black racism, pursue adequate training in cultural humility, and speak out when we see racism perpetuated in our organizations. Many clinicians wonder about concrete actions that they can take to address this pervasive problem. Here, we provide recommendations for training and clinical practice:
Include and amplify Black autistic voices within your organization. Identify Black autistic individuals to serve on an advisory committee to improve your organization’s quality of care for Black autistic people (e.g. receive feedback on policies). To promote organizational change, advisory board members should meet with organization leaders and clinicians. Advisory board members should be adequately compensated for their labor; this is particularly important when recognizing that expectations of free labor from Black autistic individuals perpetuate the exploitation of Black labor that has continued in the United States since slavery.
Continuously learn about and acknowledge the ways in which your discipline perpetuates anti-Black racism—both in the past and in the present moment. Pre-service training programs and clinical supervisors have a responsibility to understand discipline-specific anti-Black racism history. This knowledge should be considered in competency evaluations for trainees and should also be addressed in continuing education programming. Systematic change to address anti-Black racism cannot occur without this training.
Recognize that cultural humility is a lifelong process and take actionable steps each year toward increasing your own cultural humility. A central tenet of cultural humility is that it does not focus on competence or confidence, but rather recognizes that with increased exposure to other cultures, one realizes how much they do not know about others. Thus, this process is never “complete.” There is no “magic number” of workshops or evaluations that one can complete to become anti-racist. However, we can further our journey in becoming anti-racist clinicians through continuously reflecting on and challenging racist actions from ourselves and colleagues, actively listening to Black autistic individuals and their families, and using our power and privilege to affect change. We have compiled a number of materials related to cultural humility, implicit bias, and anti-Black racism as an initial set of resources for clinicians (Appendix 1). We also recommend inviting and compensating Black autistic individuals and Black clinicians for in-service training and professional development opportunities.
When working with Black autistic individuals, be mindful of the complex pathway that families must navigate to access and utilize clinical services (Figure 1). Ask questions at intake regarding previous experiences with the service system(s) earlier in the pathway. Explicitly name experiences of anti-Black racism when you hear them. Provide concrete steps for navigating the healthcare service systems that follow later in the pathway and/or occur concurrently with your services. Do not assume that families already have this information. Encourage your colleagues to discuss this pathway with their clients as well. Explicitly ask about experiences of racism and help clients to name oppressive systems at work. Encourage your colleagues to discuss this pathway with their clients as well. Clinicians may also refer to resources provided in Appendix 1, as a number of these materials may be helpful to share directly with families (e.g. YouTube videos about Autism in Black Families).
As anti-Black racism is systemic, advocate for system-level changes to address it within your organization and continue to re-assess and refine changes that have already been made. These system-level changes will vary by discipline. Some examples include screening for developmental concerns at preschool well-child visits rather than discontinuing at the 24-month visit since many Black autistic children are not identified until preschool or school age (Zuckerman et al., 2021), using group parent training models to address the needs of families on long waitlists (Straiton et al., 2021) and auditing language on Individualized Education Programs (IEPs) for Black students to identify and correct anti-Black language. Another critical systems-level change is to increase the number of Black clinicians in your organization and monitor your progress annually, at minimum. This likely will help to address health disparities for Black autistic people (Jones & Mandell, 2020) and can be addressed through focused recruitment. Families of autistic individuals of racial and ethnic minority backgrounds feel that cultural and linguistic matching with providers enhances family–clinician relationships and helps families feel comfortable and understood (Stahmer et al., 2019); thus, increasing the Black clinician workforce at your organization will also likely result in greater client satisfaction and engagement with services.
Conclusion and moving forward
While the current state of autism services for Black families is poor, clinicians can help to address this throughout the pathway to services. We hope that this call to action will help make the autism service landscape a less racist space. We have the opportunity to promote systematic change in our own organizations. Moreover, we have the ethical imperative to actively listen and respond to calls from the Black autistic community regarding all forms of racial harm, from racial microaggressions to acts of clinical misconduct due to racism. Clinicians should use the recommendations above to proactively address anti-Black racism. However, we must also actively confront and address incidences of racial harm that have occurred and continue to occur in our own disciplines and organizations. We must leverage our power (e.g. authority) and considerable privilege as clinicians (e.g. White privilege, class privilege, and educational privilege) to uplift the personhood and dignity of Black autistic folk who deserve quality care.
Footnotes
Appendix 1
Acknowledgements
This work is made possible because of the Black autistic community who shared their experiences with autism researchers and clinicians.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.