
Abstract
Content validity describes the extent to which a measure represents, and is relevant to, the construct it aims to assess. The International Classification of Functioning, Disability and Health and derived Core/Code Sets (Sets) for autism, attention deficit-hyperactivity disorder, cerebral palsy and early developmental delay and disability are adequate to establish the content validity of measures aiming to assess functioning in young children with neurodevelopmental conditions (NDCs). This article aimed to assess the content validity of comprehensive assessments of functioning for young children with NDCs against these standards. Twenty-two common measures of functioning were evaluated for content validity against the International Classification of Functioning, Disability and Health at a domain level, with 10 measures analysed at the item-level and compared to the Sets relevant to young children with NDCs. Measures covered between 21% and 57% of the combined Set codes and 19% to 63% of codes from specific Sets. Much of this variation was between measures, with some variation due to differences between individual Sets. The percentages reflect that measures heavily focus on activities and participation areas, with environmental factors rarely assessed. These findings are useful for clinicians, policymakers, and researchers in identifying the most appropriate measures for assessing functioning in young children with neurodevelopmental conditions.
Lay abstract
Young children who have developmental delay, autism, or other neurodevelopmental conditions can have difficulties doing things in different areas of their life. What they can and cannot do is called their level of functioning. There are lots of assessment measures that aim to assess functioning. But, we are not sure if these measures assess all the things we need to know about these children’s functioning. Other research has identified lists of items (codes) that need to be assessed to understand functioning for young children with different neurodevelopmental conditions fully. These lists include body functions (the things a child’s body or brain can do), activities and participation (the activities and tasks a child does) and environmental factors (parts of the environment that can influence functioning). In this study, we looked at the items from these lists assessed by different functioning measures to see how they compared to what should be assessed. The measures that we looked at covered 21%–57% of all the codes and 19%–63% of the codes for lists specific to different conditions. Most of the measures focused on activity and participation codes, and they rarely assessed environmental factors. Knowing which codes and how much of the lists the measures assess can help researchers, clinicians and policymakers to choose measures that are more appropriate for young children with neurodevelopmental conditions.
Keywords
Introduction
Children with neurodevelopmental conditions and delays (NDCs), including autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), developmental coordination disorder (DCD) and global developmental delay (GDD), vary widely regarding their skills and abilities for functioning in everyday life (Ashwood et al., 2015; Licari et al., 2019, 2020; Riou et al., 2009). Being able to accurately and comprehensively assess the functioning of children with NDCs is an essential part of diagnostic assessments, intervention planning, and funding processes (Commonwealth of Australia, 2013; Miltenberger et al., 2016; Msall, 2005; National Institute for Health and Care Excellence, 2011; Whitehouse et al., 2018). It is important for assessment, and subsequent intervention provision, to occur as early as possible to take advantage of critical windows for brain development in the years before preschool (Spittle et al., 2012). Preschool children who have received an NDC diagnosis, and those who may not yet received a diagnosis (or will go on to receive additional diagnoses), both require comprehensive and trans-diagnostic assessments of functioning, as symptomology and functional impairment may not be directly related (Alvares et al., 2020; Whitehouse et al., 2018; Zander & Bölte, 2015).
Measures of functioning are commonly classified according to their aims and theoretical underpinnings, such as measures of ‘adaptive behaviour’ (e.g. Vineland-3; Sparrow, Cicchetti, & Saulnier, 2016), or ‘occupational performance’ (e.g. Canadian Occupational Performance Measure; Law et al., 2005). It should be noted that these concepts may be defined differently between contexts and over time (Price et al., 2018). In addition to their clinical use, these measures are frequently used as outcome measures in intervention studies for children with NDCs (McConachie et al., 2015; Whitehouse et al., 2020).
Content validity is defined according to the Consensus-based standards for the selection of health measurement instruments taxonomy as ‘the degree to which the content of [a measure] is an adequate reflection of the construct to be measured’ (Mokkink et al., 2010, p. 743). While psychometric studies of these measures often address other properties, content validity is rarely examined but implicitly assumed despite its fundamental importance (McConachie et al., 2015; Price et al., 2018). A systematic review of outcome measures for young children on the autism spectrum by McConachie et al. (2015) found no studies reviewing the content validity of measures of global functioning or daily living skills. This paucity of literature could be due to the absence of a widely accepted conceptual understanding of functioning in young children. The conceptual domains of adaptive behaviour, the most common theoretical construct underpinning these measures, are historically defined and remain the subject of ongoing debate (Price et al., 2018).
In recent years, a transdisciplinary conceptual framework, in the form of the International Classification of Functioning, Disability and Health (ICF) Core Sets and Code Sets has been supported and endorsed by the World Health Organisation (Selb et al., 2015). The ICF is a comprehensive and widely utilised biopsychosocial framework of functioning, shaping many national and international health, disability and education policies (Madden & Bundy, 2019; World Health Organization [WHO], 2007). The ICF promotes a holistic view of functioning acknowledging the influence of, and interaction between, an individual’s ‘body functions and structures’, ‘activities and participation’, ‘environmental factors’, ‘personal factors’ and ‘health conditions’ (WHO, 2007). The ICF framework, designed to be transdisciplinary, mirrors common occupational therapy models and, to some extent, definitions of adaptive behaviour (Maritz et al., 2018; Price et al., 2018). As well as the overarching framework, the ICF defines 1685 codes classifying functioning across the body functions, body structures, activities and participation and environmental factor domains (WHO, 2007). Personal factors have no official codes or classifications, with the concept of classifying and rating personal factors in the same manner as other ICF components viewed as antithetical to the purpose of the ICF (Leonardi et al., 2015; WHO, 2007). Specific codes relevant to the developing child were added to the ICF children and youth version (ICF-CY) but have now been absorbed into the main ICF document (WHO, 2012). The codes are nested, with level-1 codes (chapters) providing the broadest definitions and codes increasing in detail to the second, third or fourth levels. An overview of the structure of the ICF, its components, domains, chapters and codes are provided in Supplementary File 1.
The ICF Core Sets are shortlists of ICF codes relevant to particular health conditions and ICF Code Sets are those relevant to specific life stages or situations. Several ICF Core Sets are relevant for young children with NDCs: those for young children (aged 0–5 years) with ADHD (Bölte et al., 2018), ASD (Bölte et al., 2019) and cerebral palsy (CP; Schiariti et al., 2015). There is also an ICF Code Set for Early Delay and Disabilities (EDDs; Pan et al., 2015). The purpose of ICF Core and Code Sets (Sets) is to facilitate the use of the ICF in clinical practice (Bölte et al., 2014). Underpinning the development of the Sets is a standardised, multi-stage research process ensuring their content validity, making them an ideal standard by which to assess content validity of measures of functioning (Kielhofner, 2006; Mahdi et al., 2018; Selb et al., 2015). Therefore, this article aims to investigate the content validity of the most comprehensive measures of functioning in young children with NDCs in reference to the standard of the ICF and the relevant Sets. This understanding will assist clinicians and researchers in evaluating the suitability of these measures in measuring the functioning in young children with NDCs.
Methods
Grey literature search and comparison to ICF chapters
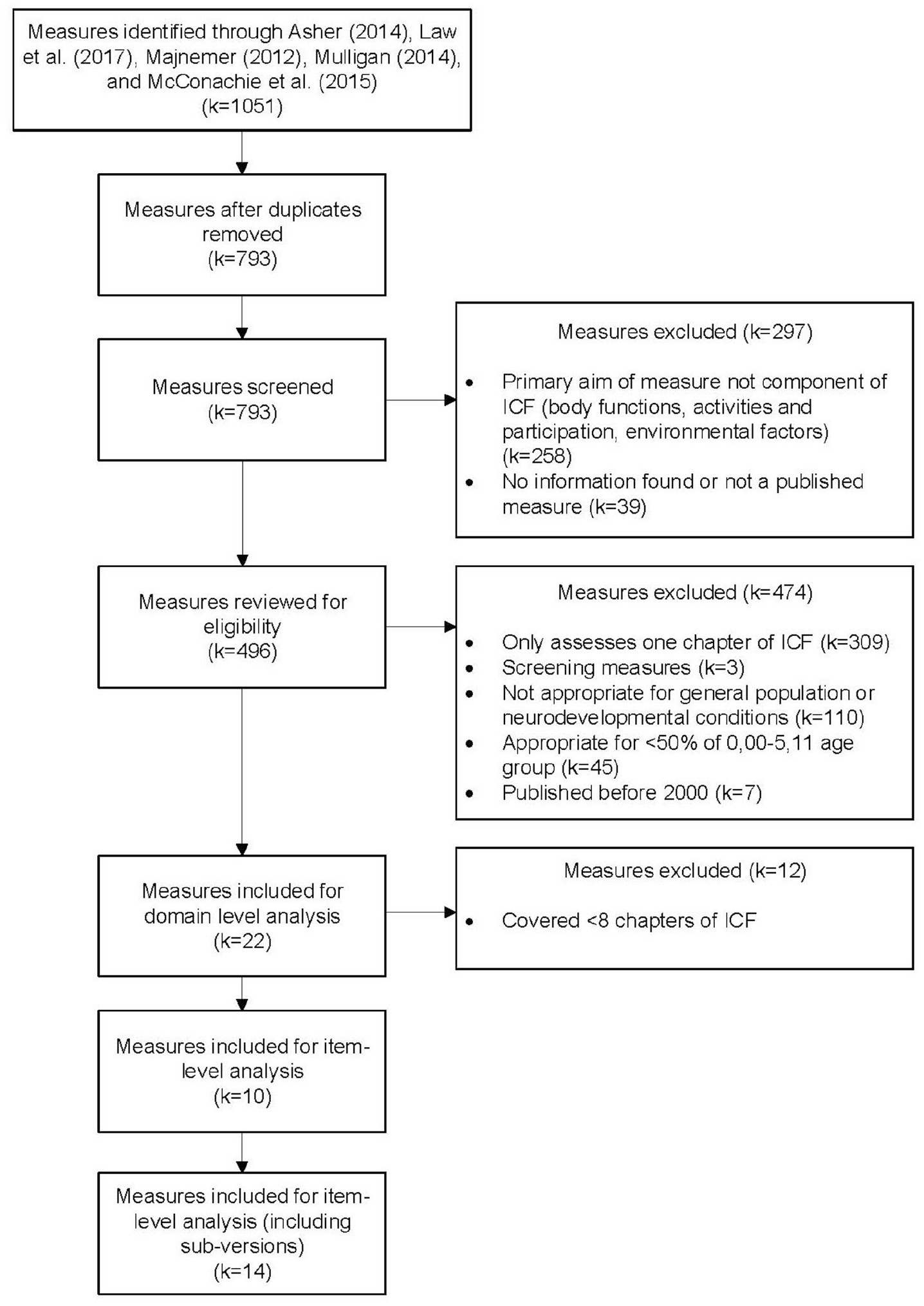
A grey literature search was conducted (Figure 1), with 1051 measures for consideration extracted from four books and a systematic review (Asher, 2014; Law et al., 2017; Majnemer, 2012; McConachie et al., 2015; Mulligan, 2014). A grey literature search was chosen over a review of the literature, to capture established measures available for clinical use and exclude those still in development. The sources selected were key works relevant to measures of functioning, identified through clinical experience and knowledge of the literature, including consultation with Curtin University’s School of Allied Health’s resource library.
Screening process to identify measures.
Prior to the search, inclusion criteria were determined to identify measures that were (a) relevant to the ICF’s concept of functioning; (b) comprehensive (i.e. exclude measures only targeting one area of functioning); (c) appropriate for the target age group and (d) available for clinical use. It was expected that the criteria would need to be modified based on the initial results to capture measures congruent with the aim of the research. Once measures were extracted, duplicate results were removed leaving 793 measures. The following final inclusion criteria were determined and then applied: measures needed to (a) have a primary aim related to at least one domain of the ICF: body functions, activities and participation or environmental factors; (b) cover at least two chapters of the ICF; (c) not be a screening tool; (d) be stated as appropriate for individuals with NDCs or the general population; (e) be applicable for more than 50% of the 0–5 years and 11 months years age group and (f) be published in 2000 or later and be available for download or purchase at the time of data collection (2020).
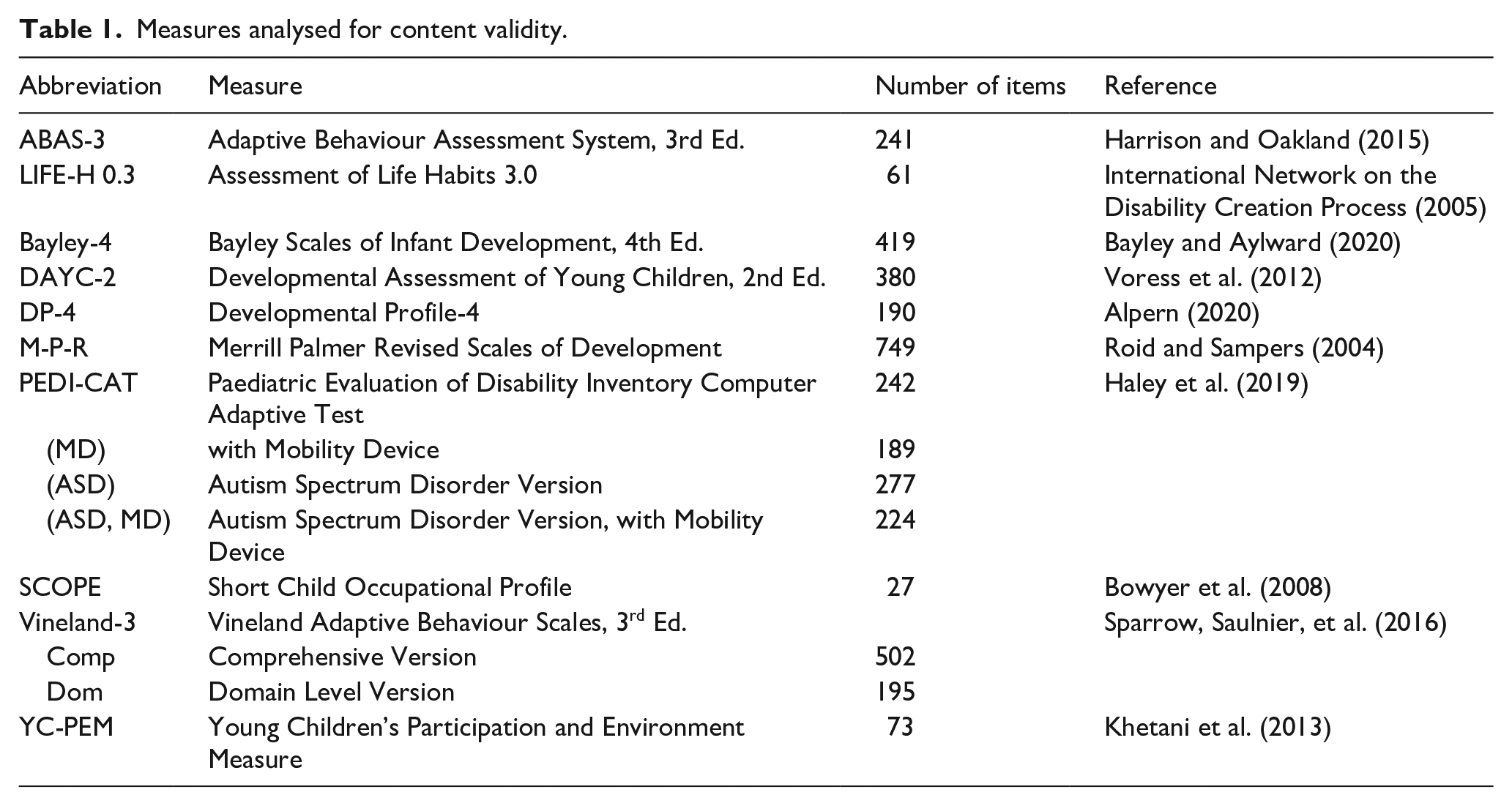
Twenty-two measures met the inclusion criteria and were analysed by two researchers using information available on publishers’ websites (e.g. domains of the measure) to determine how many chapters of the ICF they covered. Once this was completed, an inclusion criterion for item-level linking of eight or more chapters of the ICF was decided, in order to select the most comprehensive measures. Ten measures met this standard and were included for full content validation (Supplementary File 2). Where measures had versions with different questions, these were assessed as individual measures (e.g. Comprehensive and Domain versions). Therefore, the Vineland-3 comprehensive and domain-level forms, and PEDI-CAT original and PEDI-CAT (ASD), both with and without the mobility device domain were considered individually. This resulted in 14 measures included for detailed analysis are presented in Table 1.
Measures analysed for content validity.
Full linking and comparison to ICF and ICF Sets
The content validity of the measures was evaluated by mapping items against the ICF according to the established ICF linking methodology (Cieza et al., 2019). This methodology allows the content of qualitative data sources to be compared to the ICF and any ICF Sets. For this study, measures were compared to the Sets for young children (0–5 years) with ASD (Bölte et al., 2019), ADHD (Bölte et al., 2018), CP (Schiariti et al., 2015) and EDD (Pan et al., 2015), and a combined ‘Early Neurodevelopmental’ (eND) Set generated by the authors by combining the items of the above Sets.
Questions from each measure were extracted from the manual or form and entered into a Microsoft Excel template. Two reviewers (E.D. and K.W.) who had completed training relating to the ICF and linking methodology, assessed the meaningful concepts of each item, including examples, and linked these to the ICF (Cieza et al., 2019). A small sample of items was discussed between the two reviewers to facilitate consistency of approach before linking all items of the measures. The measures’ perspectives and response options were reviewed and classified as part of the linking process and considered when determining meaningful concepts (Cieza et al., 2019). Where applicable, ‘non-specified’ and ‘other specified’ codes were used. If a meaningful concept was not relevant to the ICF, it was classified as ‘not covered’ and if was covered by the ICF but did not provide sufficient detail to support linking to a code, it was classified as ‘not definable’. After linking the measures’ items independently, the reviewers met to discuss any discrepancies and reach a consensus for each measure. If agreement could not be reached, a third reviewer (A.C.) reviewed the items and the ICF to reach a final consensus. Once the consensus process was completed, reviewer agreement was 100%. This produced a final list of codes (from levels two, three and four of the ICF) that described the content of each measure.
For each measure, frequency distributions were made for each ICF code to summarise their content. The content of the measures compared to the ICF domains and chapters was assessed using these frequency distributions. Before assessing the measures’ content validity using the Sets, the lists of codes were simplified by reducing any level three or four codes to their corresponding second-level ‘parent’ code. From these level two codes, frequency distributions for codes included in the 0–5 years ASD, 0–5 years ADHD, 0–5 years CP, EDD and eND Sets were calculated for each measure to identify the percentage of the Sets they assessed. This percentage was calculated for each overall Set and for the codes from each ICF domain within the Set.
Community involvement
Two of the authors of this article are parents to autistic children. There was no other involvement from the autistic or autism communities in this research.
Results
Full linking and comparison to ICF and eND, ASD, CP and EDD Sets
Perspectives of measures
The perspectives and response options of the measures evaluated varied (Supplementary File 3), with all taking a descriptive perspective for at least one question or domain. Measures taking a descriptive perspective most frequently assessed performance (‘what an individual does in his or her given environment’; Cieza et al., 2019, p. 579), with the exception of those including a standardised clinician-administered component, which instead assessed capacity (‘individual’s ability to execute a task or action . . . [in] a standardised environment’; WHO, 2007, pp. 13). Other perspectives included the need for or dependency on supports (PEDI-CAT and LIFE-H), and appraisal of satisfaction with current performance (LIFE-H). Response options usually included confirmation/agreement (yes/no if a child performs a behaviour), or the frequency that the child performs a behaviour, with the ABAS-3 scale combining the two. Other less-common response options were intensity (how difficult a task was for the child or the level of satisfaction with the performance), qualitative responses describing different behaviours (Bayley-4) or the type of impact an environmental factor had on participation (YC-PEM).
Content validity compared to the ICF domains and chapters
Results showed that for all measures, with the exception of the YC-PEM, the majority of items fell under the activities and participation domain (range = 38%–96%, Mdn = 87%). Very rarely were questions related to environmental factor codes, with only two measures evaluating this domain: the SCOPE (26% of codes) and YC-PEM (49% of codes). The remainder of the codes fell under the body functions domain (Mdn = 11%, range = 4%–34%). Within the different domains, the distribution of codes across the chapters was not consistent.
For items coded as body functions, the majority of items fell under the ‘Mental functions’ chapter (range = 50%–95%, Mdn = 81%), with the next most common being the ‘Neuromusculoskeletal and movement related functions’ (range = 0%–37%, Mdn = 3%). All other body function chapters were rarely assessed. The activities and participation chapters were more consistently assessed than the body function chapters, however there was still moderate variability between the distribution of codes. While ‘Mobility’, ‘Learning and applying knowledge’ and ‘Self-care’ chapters shared the highest median of coverage (18%), measures ranged of coverage varied widely (range = 5%–49%, 6%–36%, and 6%–26%, respectively). ‘Communication’ items were also frequently assessed (range = 3%–33%, Mdn = 13%). The chapters ‘Major life areas’ and ‘Domestic life’ were the least commonly assessed, with some measures failing to assess theses chapters at all (range = 0%–11%, Mdn = 3% and range = 0%–12%, Mdn = 5%, respectively). Only the SCOPE and YC-PEM assessed environmental factors, most frequently assessing ‘Products and technology’ (Mdn = 34%) and ‘Support and relationships’ (Mdn = 25%) and less frequently ‘Attitudes’ (Mdn = 12%). The ‘Natural environment and human made changes to the environment’ was only covered by the YC-PEM.
The distribution of codes from the measures across the domains and chapters of the ICF is outlined in Table 2. The distribution of ICF Codes across each measure and its domains is provided in Supplementary File 4.
Distribution of codes assigned to measures across the ICF domains and chapters.
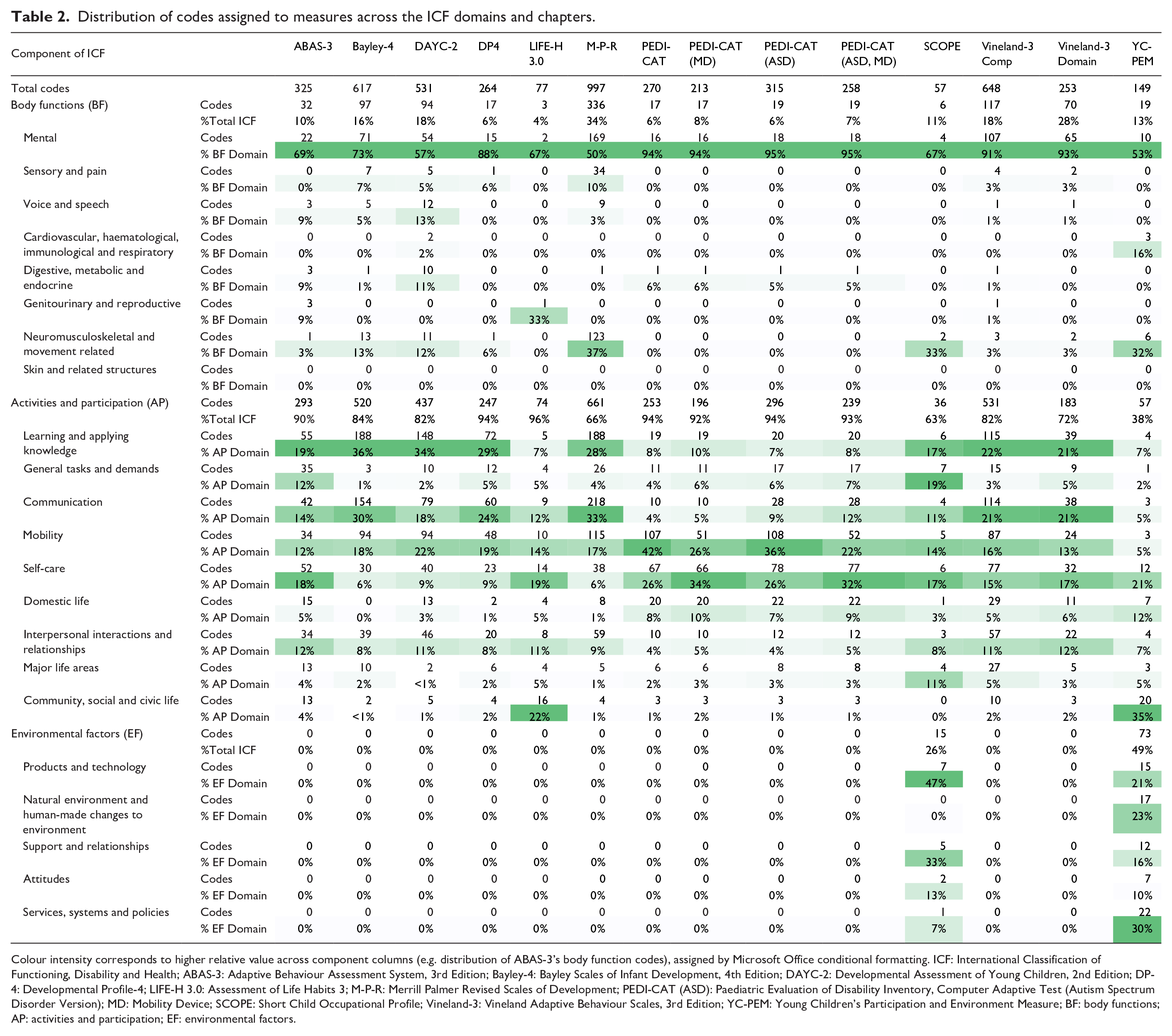
Colour intensity corresponds to higher relative value across component columns (e.g. distribution of ABAS-3’s body function codes), assigned by Microsoft Office conditional formatting. ICF: International Classification of Functioning, Disability and Health; ABAS-3: Adaptive Behaviour Assessment System, 3rd Edition; Bayley-4: Bayley Scales of Infant Development, 4th Edition; DAYC-2: Developmental Assessment of Young Children, 2nd Edition; DP-4: Developmental Profile-4; LIFE-H 3.0: Assessment of Life Habits 3; M-P-R: Merrill Palmer Revised Scales of Development; PEDI-CAT (ASD): Paediatric Evaluation of Disability Inventory, Computer Adaptive Test (Autism Spectrum Disorder Version); MD: Mobility Device; SCOPE: Short Child Occupational Profile; Vineland-3: Vineland Adaptive Behaviour Scales, 3rd Edition; YC-PEM: Young Children’s Participation and Environment Measure; BF: body functions; AP: activities and participation; EF: environmental factors.
Content validity compared to the NDC-related Sets
The content validity of individual measures against the 0–5 years NDC Sets varied (values provided in Table 3). While the median coverage (ranging between 37%–42%) and minimum coverage (19%–28%) of each set was consistent, there was variability across measures of their maximum coverage of the Sets (48%–63%). The coverage of different ICF domains within the Sets reflected a similar distribution as when compared to the full ICF, with measures focussing most frequently on activities and participation items (Mdn = 71%–77%), followed by body functions (Mdn = 17%–44%) with environmental factor codes the least frequently assessed (Mdn = 0%) being covered by only two measures.
Percentage of 0–5 NDC ICF Sets covered by measures.
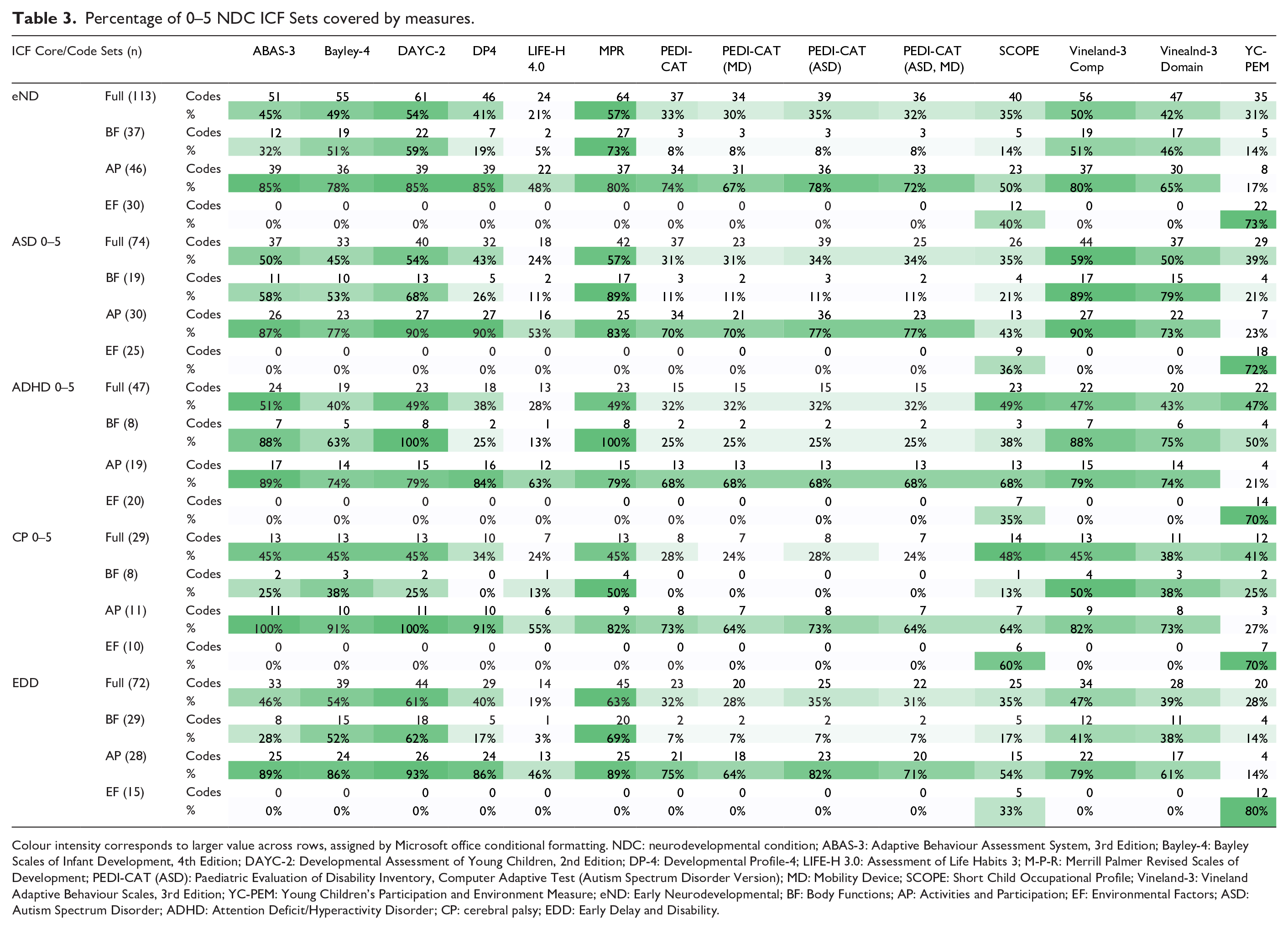
Colour intensity corresponds to larger value across rows, assigned by Microsoft office conditional formatting. NDC: neurodevelopmental condition; ABAS-3: Adaptive Behaviour Assessment System, 3rd Edition; Bayley-4: Bayley Scales of Infant Development, 4th Edition; DAYC-2: Developmental Assessment of Young Children, 2nd Edition; DP-4: Developmental Profile-4; LIFE-H 3.0: Assessment of Life Habits 3; M-P-R: Merrill Palmer Revised Scales of Development; PEDI-CAT (ASD): Paediatric Evaluation of Disability Inventory, Computer Adaptive Test (Autism Spectrum Disorder Version); MD: Mobility Device; SCOPE: Short Child Occupational Profile; Vineland-3: Vineland Adaptive Behaviour Scales, 3rd Edition; YC-PEM: Young Children’s Participation and Environment Measure; eND: Early Neurodevelopmental; BF: Body Functions; AP: Activities and Participation; EF: Environmental Factors; ASD: Autism Spectrum Disorder; ADHD: Attention Deficit/Hyperactivity Disorder; CP: cerebral palsy; EDD: Early Delay and Disability.
Based on medians, the measures that had the best content validity across the four full individual NDC Sets were the MPR (Mdn = 57%), DAYC-2 (Mdn = 54%), and Vineland-3 Comprehensive (Mdn = 47%). These measures also covered the most body function codes across the Sets. However, the DAYC-2, ABAS-3 and DP4 had the best median coverage of the Sets’ activity and participation codes (Mdn = 90%; 89% and 86%, respectively). When considering environmental factors, the YC-PEM consistently covered more codes (Mdn = 72%) than the SCOPE (Mdn = 36%).
Linking revealed that none of the identified measures consistently and comprehensively assessed codes across the individual Sets, with the MPR most comprehensively covering the eND and EDD Sets, the Vineland-3 Comprehensive the ASD and CP Sets and ABAS-3 the ADHD Set. The MPR was the, or one of the, most comprehensive measures for all five of the Sets’ body function codes, joined by the Vineland-3 Comprehensive for the ASD and CP Sets, and the DAYC-2 for the ADHD Set. When considering only the activity and participation codes, multiple measures covered the highest percentage of most Sets. The ABAS-3, DAYC-2 and DP4 were most comprehensive for the eND Set, and the DAYC-2, DP4 and Vineland-3 Comprehensive covering the most activity and participation codes of the ASD Set. Only the ABAS-3 was the most comprehensive of the ADHD Set, while it and the DAYC-2 were both the most comprehensive of the CP Set’s activity and participation domain. Finally, the DAYC-2 was the most comprehensive in covering the EDD Set. Considering the environmental factor domains of the Sets, the YC-PEM was consistently the most comprehensive.
The percentage of each Set each measure covered, including a breakdown by the domains of the ICF, is outlined in Table 3. In addition to the inclusion of all relevant concepts, content validity includes the exclusion of irrelevant concepts, so the percentages of codes assigned to each measure that were relevant to the Sets are outlined in Supplementary file 5.
Discussion
Content validity is a foundational property of assessment measures, which should be considered alongside other psychometric properties when determining the suitability of a measure for a specific purpose (Mokkink et al., 2010). Despite the important role that measures of functioning play in the clinical pathway of young children with NDCs (Commonwealth of Australia, 2013; Miltenberger et al., 2016; Msall, 2005; National Institute for Health and Care Excellence, 2011; Whitehouse et al., 2018), the content validity of these measures is rarely established (McConachie et al., 2015; Price et al., 2018). The ICF and associated Code and Code Sets provide a gold standard against which to assess the content validity of common measures of functioning for young children with NDCs.
The linking results demonstrated that the measures reviewed had varying levels of content validity when compared to the standard of the Sets. None of the measures were comprehensive enough to cover all concepts across the three domains of the ICF, with even the most comprehensive measures covering less than 60% of the eND Set codes. When considering only the body function codes or activities and participation codes within the Set, different measures were better suited to assessing different domains. Even measures designed to assess the same concept (e.g. the Vineland-3 and ABAS-3 both assess adaptive behaviour) differed in regard to their focus on body functions and activities and participation (Harrison & Oakland, 2015; Sparrow, Cicchetti, & Saulnier, 2016). Identified measures most comprehensively assessed the activities and participation domain of the Sets. Given that the performance of activities and participation is the ‘result’ of functioning and is readily observed, this finding is not surprising (Law et al., 2017; WHO, 2007).
While only two of the measures of functioning included in the present review directly assessed environmental factors, several measures assessed a child’s level of functioning alongside the presence of supports (e.g. LIFE-H) or through explicit instructions to rate the child’s functional performance with (e.g. PEDI-CAT) or without (e.g. ABAS-3 and Vineland-3) supports. The ICF and other models related to functioning emphasise the interplay between an individual’s skills, abilities or body functions, the activities and tasks they participate in, and their environment on their overall functioning (Townsend & Polatajko, 2013; WHO, 2007). The ICF in particular also includes personal factors as a contextual component alongside environmental factors as an influence on functioning (WHO, 2007). Adaptive behaviour, although less focused on the interplay between these components, is still generally accepted to be defined as ‘the skills an individual requires . . . to be able to cope with the social and natural demands in their environment’ (Price et al., 2018, p. 1). Without assessing if specific environmental supports and barriers are present and how they interact with and individual’s skills and activities, providing an accurate and holistic picture of an individual’s abilities and support needs is not possible (Anaby et al., 2013; Turpin & Iwama, 2010; WHO, 2007). An assessment of functioning without considering the environment or personal factors can impact funding and intervention when assessments are used in clinical practice and may lead to misinterpretation of results when used as outcome measures in research studies.
The co-occurrence of NDCs is common, and young children may go on to receive a diagnosis not identified at the time of the initial assessment (Licari et al., 2019; Miodovnik et al., 2015). Furthermore, NDCs can have a diverse impact on functioning not captured in diagnostic criteria (Andrews et al., 2015; Flynn & Healy, 2012; Licari et al., 2020). In the absence of a new assessment with greater content validity in comparison to the eND Set, a transdisciplinary approach using a battery of measures alongside clinical reasoning is recommended. While the use of a battery or comprehensive tool in assessing the functioning of young children with NDCs adds to the resources required to assess functioning, this approach likely provides a more valid and holistic picture of a child’s functioning, and more reliably informing intervention planning. Therefore, sufficient funding should be made available to facilitate the use of appropriate measures in order to avoid inaccurate or inappropriate findings and associated funding or therapeutic consequences (Whitehouse et al., 2018). When a full assessment is not required, careful consideration of the purpose of the assessment and needed information should be used to determine appropriate measures through clinical reasoning (Kramer et al., 2009). The selection of appropriate assessments to include in a battery, or for more specific assessment purposes can be aided by the linking results presented.
When selecting assessments, their original design should also be considered, including their perspectives, response options and whether they are designed to be a broad comprehensive assessment (Cieza et al., 2019; Law et al., 2017). For example, the PEDI-CAT and PEDI-CAT (ASD) are not designed to capture a specific and detailed picture of functioning. Instead they use item response theory and high internal consistency to estimate a child’s broader level of functioning based on a relatively small number of question responses (Haley et al., 2020). Also to be considered is the difference between functional performance and capacity, and whether functioning is rated with or without supports (WHO, 2007). The difference between these two approaches is especially relevant when using these assessments to determine support needs, a base level of functioning or to measure change resulting from an intervention. Lack of clarity between functioning with and without supports could impact comparisons to norms and potentially influence the appropriateness of funding and supports available to the child.
Limitations
A proportion of items from the measures were not able to be linked to defined ICF codes. The other specified codes were used to account for limitations of the ICF regarding the early stages of infant and toddler development and changes in activities of daily life over time (e.g. use of technology). While updates to the ICF have been made, most notably the addition of items relevant to children and youth, this finding supports the continued revision of the ICF and Sets to maintain their applicability over time, and for more specific populations, such as infants (WHO, 2007). However, this use of other specified codes did not significantly influence the results of this study, as they were usually converted to their parent second-level code before comparison to the Sets.
Due to the Sets consisting of second-level codes, this research only evaluates the measures’ content validity at this level of detail. Many ICF codes have third, and sometimes fourth level, subcodes which provide greater levels of detail. In the present review, if measures assessed these third and fourth level codes, they were collapsed into their parent second-level code before comparison to the Sets. Therefore, while a measure may have assessed a second-level code, this is not necessarily an indication that the measure assesses all the details within that code.
While this study assessed the content validity of measures’ full item banks against the ICF and Sets as a gold standard, this will not always be a true reflection of the measures’ content validity in clinical practice. The CAT design of the PEDI-CAT versions, and the basal and ceiling administration methods of other measures (including the MPR, Vineland-3, and DAYC-2), influence how many, and which, questions are scored (Haley et al., 2020; Roid & Sampers, 2004; Sparrow, Saulnier, et al., 2016; Voress et al., 2012). Therefore, areas of the ICF and Sets covered by the full item bank will not always be assessed for an individual. Given this, results presented in this article will generally be an overestimation of the content validity of the measures. Further work to assess the content validity of the measures, as administered to a representative sample of young children with NDCs, is needed, and is currently being undertaken for the PEDI-CAT (ASD).
Clinical significance
The results of this review can be used by clinicians, researchers and policymakers when selecting assessments to assess the functioning of young children with NDCs, or as outcome measures in research. While an important consideration, content validity is not the sole indicator in determining the appropriateness of assessments. The whole range of psychometric properties and clinical utility should be evaluated before using an assessment (Mokkink et al., 2010; Smart, 2006). In addition, the context in which the assessment is being utilised will determine the assessment properties best suited to practice and how appropriate the ICF Sets are as a gold standard for content validity (Mokkink et al., 2010).
Supplemental Material
sj-docx-1-aut-10.1177_13623613211036809 – Supplemental material for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions
Supplemental material, sj-docx-1-aut-10.1177_13623613211036809 for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions by Emily D’Arcy, Kerry Wallace, Angela Chamberlain, Kiah Evans, Benjamin Milbourn, Sven Bölte, Andrew JO Whitehouse and Sonya Girdler in Autism
Supplemental Material
sj-docx-2-aut-10.1177_13623613211036809 – Supplemental material for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions
Supplemental material, sj-docx-2-aut-10.1177_13623613211036809 for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions by Emily D’Arcy, Kerry Wallace, Angela Chamberlain, Kiah Evans, Benjamin Milbourn, Sven Bölte, Andrew JO Whitehouse and Sonya Girdler in Autism
Supplemental Material
sj-docx-3-aut-10.1177_13623613211036809 – Supplemental material for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions
Supplemental material, sj-docx-3-aut-10.1177_13623613211036809 for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions by Emily D’Arcy, Kerry Wallace, Angela Chamberlain, Kiah Evans, Benjamin Milbourn, Sven Bölte, Andrew JO Whitehouse and Sonya Girdler in Autism
Supplemental Material
sj-docx-4-aut-10.1177_13623613211036809 – Supplemental material for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions
Supplemental material, sj-docx-4-aut-10.1177_13623613211036809 for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions by Emily D’Arcy, Kerry Wallace, Angela Chamberlain, Kiah Evans, Benjamin Milbourn, Sven Bölte, Andrew JO Whitehouse and Sonya Girdler in Autism
Supplemental Material
sj-docx-5-aut-10.1177_13623613211036809 – Supplemental material for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions
Supplemental material, sj-docx-5-aut-10.1177_13623613211036809 for Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions by Emily D’Arcy, Kerry Wallace, Angela Chamberlain, Kiah Evans, Benjamin Milbourn, Sven Bölte, Andrew JO Whitehouse and Sonya Girdler in Autism
Footnotes
Acknowledgements
The authors would like to thank the measures’ publishers for their permission and support in obtaining assessments for analysis. This research will be used towards obtaining a Doctor of Philosophy (Occupational Therapy) by the first author.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support of the Cooperative Research Centre for Living with Autism (Autism CRC), established and supported under Australian Government’s Cooperative Research Centres Programme. A.J.O.W. is supported by an Investigator Grant from the National Health and Medical Research Council (grant no. 1173896).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.