
Abstract
The communication skills and styles of autistic people have been the focus of much research, but little work has explored the communication preferences of autistic adults themselves. This study examined how autistic adults prefer to communicate in multiple scenarios. Two hundred and forty-five autistic adults completed a novel questionnaire that required six communication modes to be ranked in order of preference across seven different scenarios. Participants also provided qualitative responses to further explain their rankings, and completed the Autism Quotient, the Generalised Anxiety Disorder scale and the Camouflaging Autistic Traits Questionnaire. Quantitative data indicated that email ranked highly when accessing services, seeking customer support and communicating about research. When communicating with family, friends, in employment and in education, both face-to-face and written modes (email or text message) were preferred. In the qualitative data, four main themes were identified: Not the Phone, Written Communication, Masking versus Autistic Communication and Avoiding Communication. There is a clear message that mode of communication can be either enabling or disabling for autistic people. A reliance on phone calls can create barriers to access, yet the option to adopt written forms of communication can improve accessibility. For known connections, the preference for face-to-face communication is dependent upon how close and accepting the relationship is.
Lay abstract
There has been a lot of research into things like how autistic people’s communication styles are different to those of non-autistic people, especially among children. This has tended to focus on parent reports and experiments, rather than asking autistic people about their own experiences and preferences regarding communication.
This article is the first to ask autistic adults how they prefer to communicate in different scenarios. We asked whether they preferred to use a range of methods, such email, phone calls, letters and live messaging, in scenarios from education to customer services to friends and family. When contacting unknown people or organisations, we found that generally email was preferred, and phone calls were very unpopular. However, for friends, family and people they felt comfortable with, they preferred both face-to-face and written forms of communication (e.g. email and text message).
The findings suggest that services should move away from a reliance on phone calls for communication. They should make sure that access to support is not dependent on the phone, and instead offer written options such as email and live messaging which are more accessible. Future research should investigate the impact of COVID-19 on autistic people’s communication preferences, as video calling has become much more commonly used and potentially combines benefits and challenges of other modes discussed in this article.
Communication difficulties are a core diagnostic feature of autism and are generally assessed in terms of face-to-face communication (Lord et al., 2012). These challenges manifest in a range of areas, such as reciprocity, non-verbal cues and pragmatics (American Psychiatric Association, 2013). The communication challenges autistic people experience are associated with increased anxiety, isolation and difficulties with education, employment and accessing services (Baldwin et al., 2014; Crawford & Manassis, 2011; Howlin, 2000; Sumiya et al., 2018).
In the modern world, there are myriad communication options available which are not face-to-face. Technology has transformed how the entire world talks to each other, and autistic people are included in that seismic shift. What is not known is how these changes affect autistic people’s communication. If we can identify the communication methods that autistic people prefer, we are likely to improve accessibility, experiences and interactions, and ultimately contribute to improving autonomy, quality of life and social inclusion.
The existing evidence suggests that autistic people may prefer written modes of contact. For example, autistic adults perceived success of healthcare interactions is associated with their willingness to provide written mode options (Nicolaidis et al., 2015), and a survey on Internet use indicated that autistic people typically preferred email over face-to-face interaction (Benford & Standen, 2009). It seems that written communication may diminish some of the social interaction challenges autistic people experience in face-to-face contexts. Benford and Standen (2009) interviewed autistic Internet users, who reported that written Internet-mediated communication provides more control, thinking time, clarity and fewer sensory issues and streams of information that must be processed and interpreted. Similarly, Gillespie-Lynch et al. (2014) reported autistic people to perceive computer-mediated communication as beneficial, as it provides more control and increased comprehension in interactions. Consequently, there are reports of autistic adults utilising Internet-mediated modes of communication to foster and develop social connectiveness and relationships (Burke et al., 2010). This previous research has focused on Internet usage, yet there are a range of similar communication modes available. This study aims expand this work and explore the autistic community’s communication mode preferences more broadly, in range of different scenarios.
Considering what is known from research with non-autistic populations, we will also examine several individual factors that may have an impact on communication preferences. Older adults tend to be less comfortable with online methods and instead prefer face-to-face, letters and phone communication (Hülür & Macdonald, 2020). It is unclear whether the same is true for autistic adults, as while they have grown up in the same time period as their peers, given the communication challenges experienced, autistic people may be more enthusiastic adopters of alternative methods.
Further to the potential role of chronological age, age of diagnosis may impact communication preferences. Without a recognised diagnosis, those around an autistic person are perhaps likely to make fewer adaptations to their needs (for a review on issues surrounding late diagnosis, see Lai & Baron-Cohen, 2015). This may mean that those with a later age of diagnosis (i.e. in adulthood) may have become used to different forms of communication to those with earlier diagnoses. For example, they may have spent a lifetime having been expected to make and answer phone calls, without other people recognising that this could be uncomfortable for them, so they have learned to manage this situation more so than people with an earlier diagnosis who have been able to ask to be contacted in other ways as an accommodation of their autism.
A related issue is camouflaging – this is when people mask autistic behaviour to conceal and compensate for communication and social difficulties (Hull et al., 2019), and is associated with a desire to ‘fit in’ and form connections (Hull et al., 2017). It therefore seems likely that the extent to which an individual camouflages may influence communication. High levels of camouflaging may be associated with an increased inclination to adopt communication modes that are perceived to be ‘normal’, such as face-to-face interaction. Alternatively, high levels of camouflaging may also be associated with reduced propensity to select communication methods that place higher demands on social processing (e.g. face-to-face), given the association between camouflaging and poor mental health (Lai et al., 2017).
It is estimated that 70%–80% of autistic people experience mental health difficulties (Lever & Geurts, 2016), with anxiety being experienced by most autistic people (Croen et al., 2015). Anxiety is known to influence communication preferences for non-autistic people, with higher levels being associated with a preference to use text messages as opposed to phone calls (Reid & Reid, 2007). It therefore seems likely the levels of anxiety an autistic person experiences may further influence their communication mode preferences and may exacerbate any avoidance of anxiety-provoking situations.
To summarise, autism is characterised by a range of communication challenges, which may influence an individual’s ability to access personal and professional support. Technological advances have made a range of communication mediums available, and there is evidence to suggest some channels may be more accessible to autistic people and potentially alleviate some of the challenges experienced in face-to-face contexts. However, whether this is true both for communication ‘out’ and receiving communication ‘in’ is currently unknown. This study will adopt a mixed-methods approach to address the following questions:
What are the preferred communication methods of autistic people in a range of situations?
Does age, age at diagnosis, camouflaging and anxiety influence preferred communication methods?
What reasons do autistic people give for their communication preferences?
Method
Design
A mixed-methods design was adopted. Quantitative data were collected on participant communication mode preferences (ranked data) and individual characteristics that may influence preference selection (age, anxiety, diagnosis age and camouflaging). Qualitative data were collected to allow participants to explain the justification and nuances of their preferences.
Participants
Participants were recruited via advertisements via Bristol Autism Research Group social media and the Autistica Discover Network. Inclusion criteria were that participants must have ranked communication mode preferences for at least one of the seven communication scenarios. This resulted in a sample of 245 adult participants (M age = 40.44 years, standard deviation (SD) = 13.14, range = 16–74). All participants identified as autistic, with 205 reporting a formal diagnosis from a clinician (110 autism spectrum disorder, 92 Asperger’s syndrome, 2 Pervasive developmental disorder – not otherwise specified (PDD-NOS) and 1 was on a waiting list or mid-assessment), and 40 reported self-diagnosis (20 autism spectrum disorder, 9 Asperger’s syndrome, 6 were on a waiting list or mid-assessment and 5 did not specify). Age at diagnosis 1 ranged from 2 to 63 years (M diagnosis age = 34.38, SD = 14.16). The sample predominantly identified as female (151 female, 61 male, 31 non-binary, 2 did not respond and 5 people additionally identified as transgender) and native English speakers (91%). Specific data on ethnicity and socioeconomic status were not recorded.
Community involvement statement
We approach this project as non-autistic autism researchers who prioritise community involvement in our work. This project was discussed with an autistic consultant who reviewed the questionnaires to check for accessibility of materials and read over the qualitative results to evaluate whether our interpretations were appropriate.
Procedure and materials
Ethical approval was attained via the University of Bristol Faculty of Social Sciences and Law Ethics Committee and each participant provided written informed consent. Data were collected via an online survey hosted by Qualtrics (Qualtrics, 2020). Measures were completed in the order presented below. In total, this was estimated to take approximately 20 min to complete.
Autism Quotient Adult 10
The Autism Quotient Adult 10 (AQ-10; Allison et al., 2012) measured levels of autistic traits and consists of 10 statements relating to characteristics associated with autism including attention to detail, attention switching, communication, imagination and social interactions. It was designed as a screening tool to identify autistic traits in the general population. Participants answered ‘Yes’ or ‘No’ (adapted for simplicity) as to whether they identify with each characteristic. Scores range from 0 to 10, with a cut-off score of six or above being considered to reflect potentially clinical levels of autistic traits. Previous research reports good sensitivity (0.88), specificity (0.91) and internal consistency (Cronbach’s α = 0.85; Allison et al., 2012). Internal consistency for the current sample was acceptable (Cronbach’s α = 0.66, 95% confidence interval (CI) = 0.60–0.72).
Generalised Anxiety Disorder-7
The Generalised Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006) measured levels of anxiety, and was designed for the general population. The questionnaire asks participants to identify how many times they have experienced seven symptoms of anxiety in the past 2 weeks on a four-choice scale (not at all to nearly every day). Scores range from 0 to 21, with scores of 5, 10 and 15 reflecting mild, moderate and severe anxiety, respectively. This scale has been reported to have excellent internal consistency (Cronbach’s α = 0.92) and good stability (intraclass correlation coefficient (ICC) = 0.83), and when a cut-off score of 10 is adopted, good sensitivity (0.89) and specificity (0.82) (Spitzer et al., 2006). Internal consistency for the current sample was good (Cronbach’s α = 0.89, 95% CI = 0.87–0.91).
Camouflaging Autistic Traits Questionnaire
The Camouflaging Autistic Traits Questionnaire (CAT-Q) measured the extent to which participants compensate for their autistic behaviours during social interactions (Hull et al., 2019), and was designed specifically for autistic people. This questionnaire consists of 25 statements about compensation, masking and assimilation behaviours. Participants rated their agreement with each item using a 7-point scale (strongly disagree to strongly agree). Scores range from 25 to 175, with higher scores indicating more camouflaging behaviours. This scale has been reported to have excellent internal consistency (Cronbach’s α = 0.94) and good stability (ICC = 0.77; Hull et al., 2019). Internal consistency for the current sample was excellent (Cronbach’s α = 0.90, 95% CI = 0.88–0.91).
Communication preference rankings
Participants were presented with seven scenarios when communication is often required: accessing services, employment, education, research, family, friends and when seeking customer services. We designed this measure in collaboration with an autistic consultant, with autistic people in mind. For each scenario, participants were asked to rank six communication modes (face-to-face, phone call, letter, email, text message and online instant messaging) in order of preference, with one indicating the most preferred way to communicate and six indicating the least preferred way to communicate. Supplementary Information presents the full scenario descriptions presented to participants. Following each scenario, participants were provided the opportunity to give more detailed and nuanced information about how they communicate via two free response questions:
What are the reasons for selecting your first choice?
Is there anything more you would like to tell us about how you prefer to communicate in this situation?
Results
Study pre-registration, quantitative data and R scripts (R Core Team, 2019) can be viewed on the Open Science Framework: https://osf.io/rgcke/.
Quantitative results
Descriptive statistics for survey measures can be viewed in Table 1. Key points to highlight are that 92% of participants met the cut-off for potential clinical levels of autistic characteristics on the AQ-10, and on average, the sample reported moderate levels of anxiety. Participants who were self-diagnosed reported fewer autistic traits relative to clinically diagnosed participants (W = 5494, p < .001); but the average score for this sample still fell above the cut-off (self-diagnosed M = 7.30, SD = 2.09; clinician diagnosed M = 8.38, SD = 1.69). We decided to retain those participants who did not meet the AQ-10 cut-off and/or did not have a clinical diagnosis due to known challenges autistic adults can face in accessing formal diagnosis (Jones et al., 2014).
Descriptive statistics for AQ-10, GAD-7 and CAT-Q survey measures.
M: mean; AQ-10: Autism Quotient Adult 10; GAD-7: Generalised Anxiety Disorder-7; CAT-Q: Camouflaging Autistic Traits Questionnaire; SD: standard deviation.
To identify whether preferences differed between communication modes in each scenario, a Friedman test was conducted on ranked data, followed by post hoc Nemenyi tests. To examine how individual differences influenced preferences, a multi-nominal logistic regression model was built for each scenario, with age, age at diagnosis, GAD-7 scores and CAT-Q scores specified as predictors (each very approximately normally distributed; see Supplementary Material for distribution plots), and participant first choice specified as the outcome. For each scenario, the most popular communication mode was coded as the reference level, which allowed us to examine whether predictors influenced the likelihood a participant would make a first preference selection that differed from the sample norm. For brevity, only significant effects are reported.
Accessing services
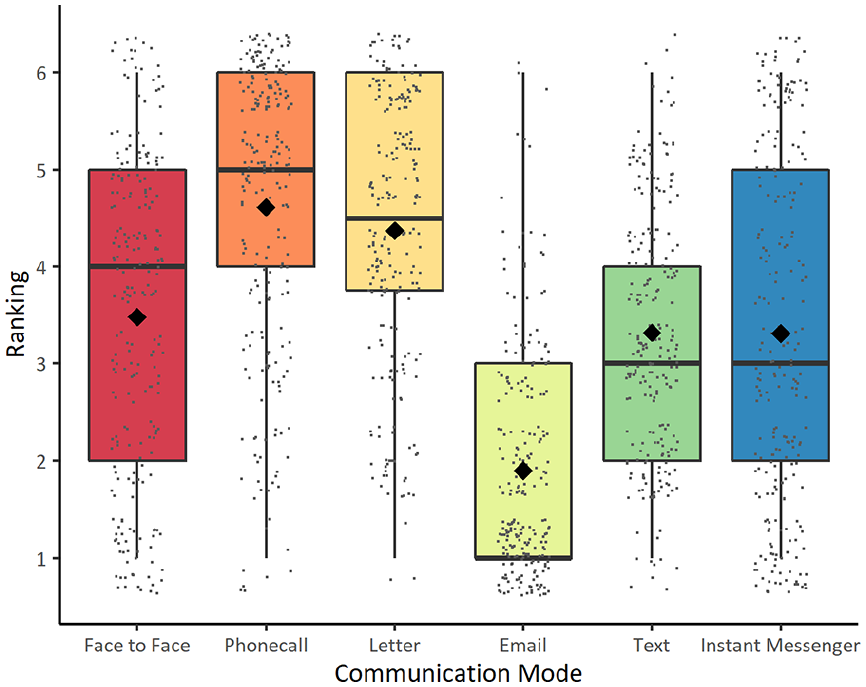
Preference rankings differed between communication modes when accessing services (χ2(5) = 315.47, p < .001) (242 respondents; see Figure 1). Email was the most preferred option relative to all other modes (p’s < .001). Text messaging was preferred relative to face-to-face communication (p = .020), phone calls and letters (p’s < .001). Online messaging was preferred relative to phone calls and letters (p’s < .001). Both letters and face-to-face communication were preferred in comparison to phone calls (p = .001 and p < .001, respectively).
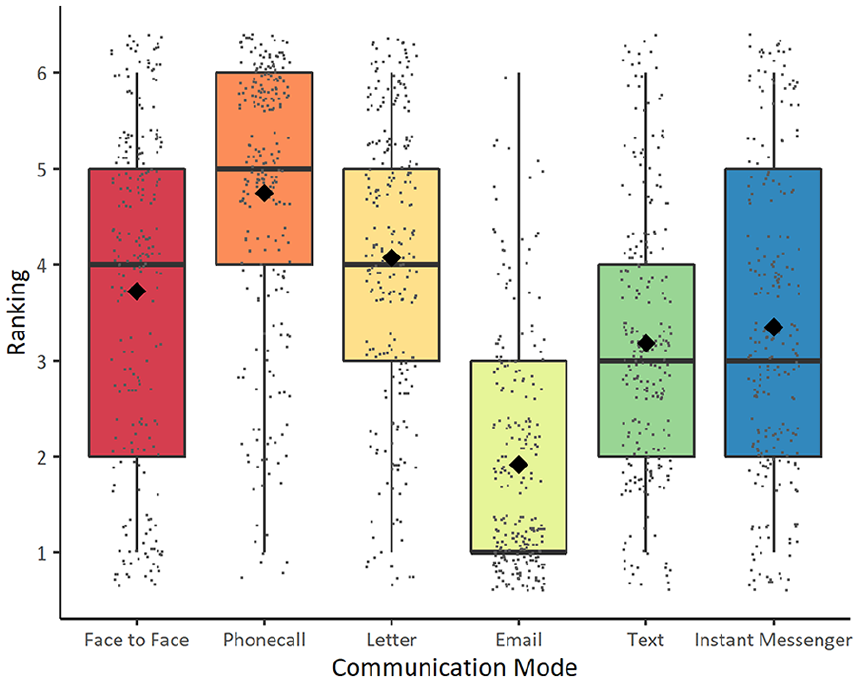
Communication mode preference rankings when accessing services.
The regression model was significant (χ2 = 52.62, p < .001, McFadden’s R2 = 0.08). A full report of these and subsequent coefficients for significant models can be viewed in the Supplementary Material. To summarise, increased age was associated with an increased likelihood to select a phone call as a first preference relative to email (B = 0.10, standard error (SE) = 0.04, p = .014, odds ratio (OR) = 1.10 (95% CI = 1.02–1.19)). Later age at diagnosis was associated with an increased likelihood to select face-to-face communication, relative to email (B = 0.10, SE = 0.05, p = .047, OR = 1.11 (95% CI = 1.00–1.23)). 2 Higher levels of anxiety were associated with an increased likelihood to select a letter as a first preference, relative to email (B = 0.12, SE = 0.05, p = .033, OR = 1.12 (95% CI = 1.01–1.25)). Higher levels of camouflaging behaviour were associated with a reduced likelihood of selecting face-to-face (B = −0.03, SE = 0.01, p < .001, OR = 0.97 (95% CI = 0.95–0.99)) and letter communication (B = −0.03, SE = 0.01, p = .043, OR = 0.97 (95% CI = 0.95–1.00)), relative to email.
Employment
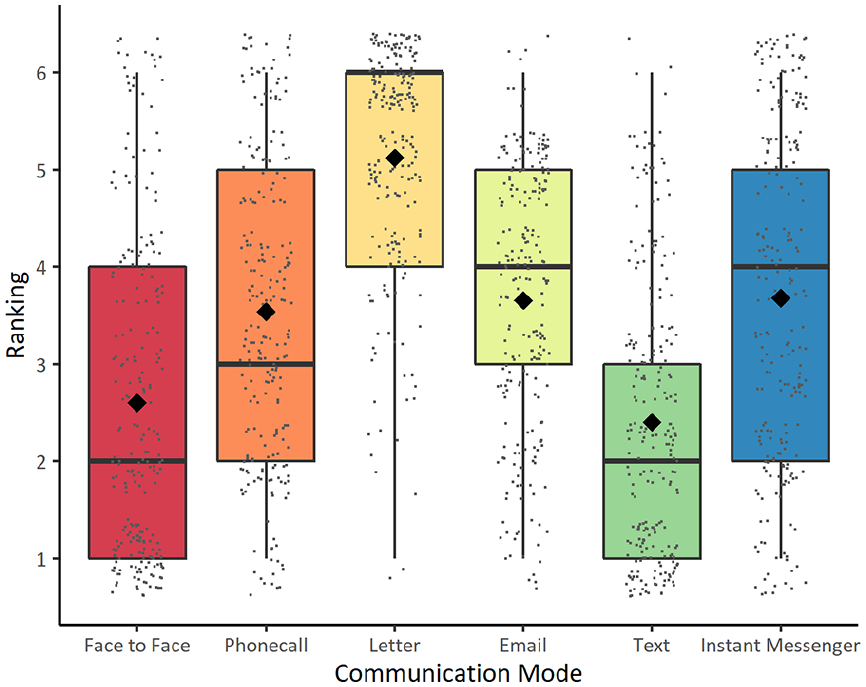
Preference rankings differed between communication modes χ2(5) = 297.28, p < .001 (204 respondents, see Figure 2), with email ranked as preferred relative to all other modes (p’s < .028). Excluding email, face-to-face communication was the second most preferred mode, relative to all other modes (p’s < .001). Text messaging was preferred in comparison to phone calls and letters (p’s < .001). Instant messaging was preferred relative to letters (p < .001).
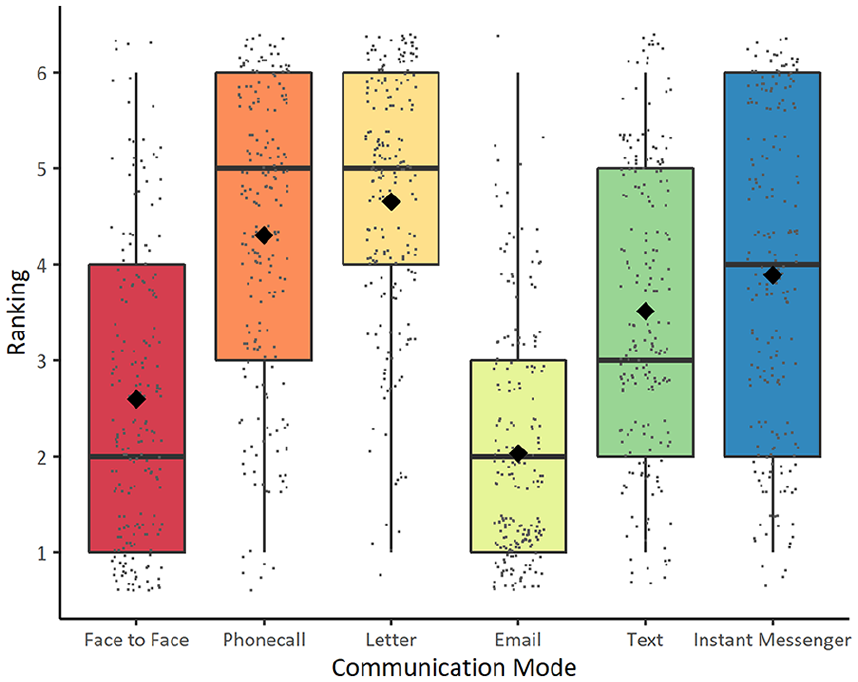
Mode preference rankings when communicating in employment.
The regression model was significant (χ2 = 36.94, p = .012, McFadden’s R2 = 0.07), with higher levels of camouflaging being associated with an increased likelihood of selecting letters (B = 0.10, SE = 0.05, p = .037, OR = 1.11 (95% CI = 1.01–1.22)), online messaging (B = 0.04, SE = 0.02, p = .019, OR = 1.04 (95% CI = 1.01–1.08)) and text messages (B = 0.04, SE = 0.02, p = .021, OR = 1.04 (95% CI = 1.01–1.07)), as the preferred communication choice relative to email.
Education
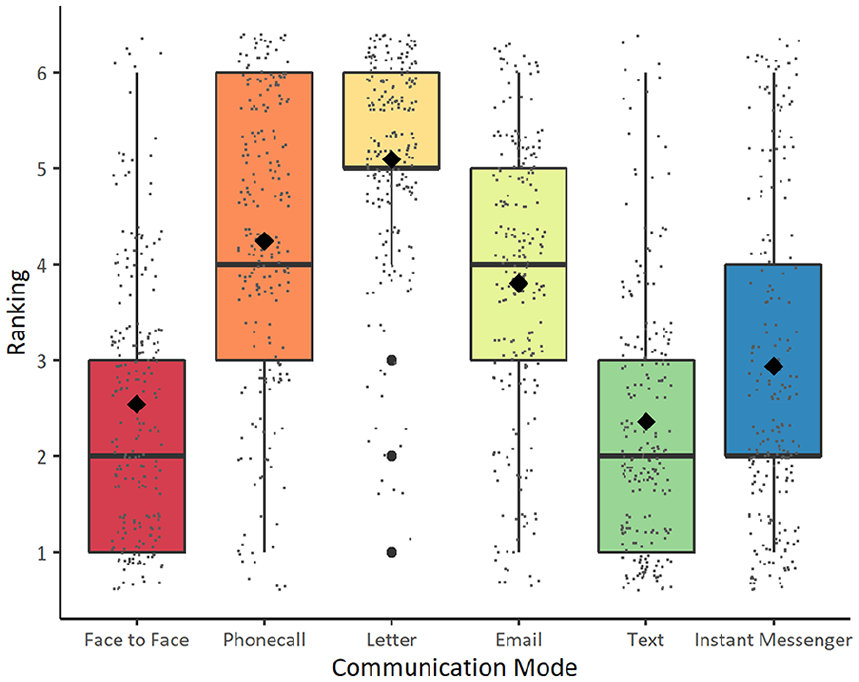
Preferences differed between communication modes for the education scenario (χ2(5) = 153.40, p < .001) (144 respondents, see Figure 3). Overall, email and face-to-face communication were the preferred methods, relative to all other modes (p’s < .001), and text messaging was preferred relative to letters (p = .006). The regression analysis was not significant, indicating that including the predictor variables did not contribute to explaining individual variation in first choice selection (χ2 = 28.74, p = .093, McFadden’s R2 = 0.08).
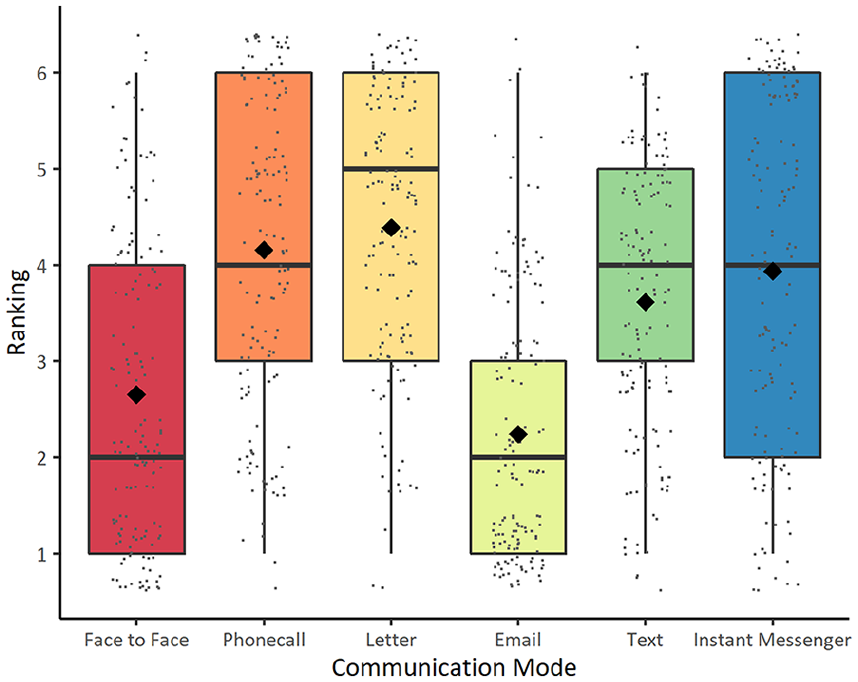
Mode preference rankings when communication in education settings.
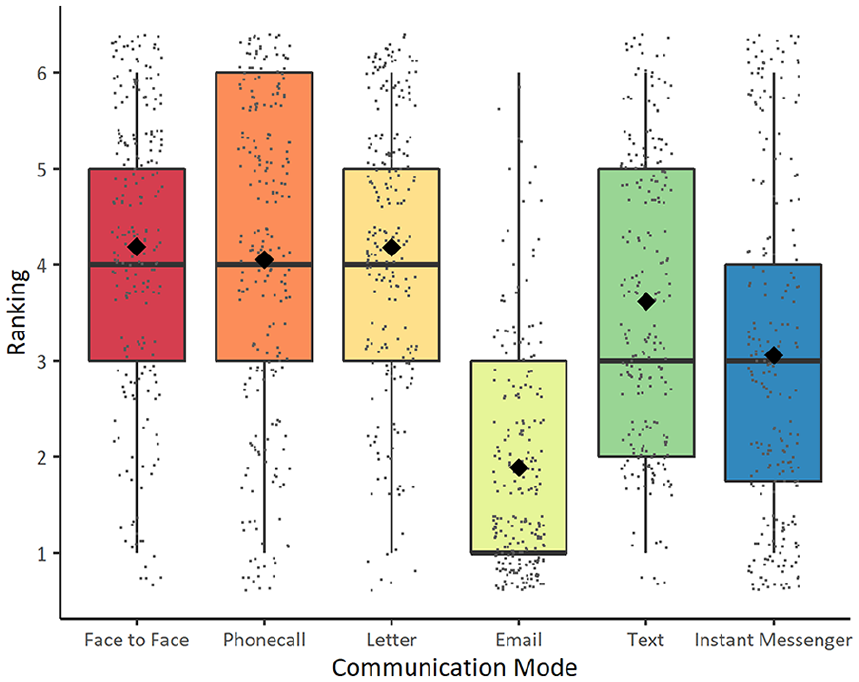
Research
Preference rankings differed between communication modes when communicating about research (χ2(5) = 307.46, p < .001), with email ranked as the preferred method, relative to all other modes (p’s < .001) (232 respondents, see Figure 4). Text messaging, instant messaging and face-to-face communication were preferred relative to phone calls and letters (p’s < .001). The regression analysis was not significant, indicating that there is no evidence that age, age at diagnosis, anxiety or camouflaging behaviours influence research communication preferences (χ2 = 30.00, p = .070, McFadden’s R2 = 0.05).
Mode preference rankings when communicating for research purposes.
Family
Preference rankings differed between modes when communicating with family (χ2(5) = 311.34, p < .001), with text messaging and face-to-face communication ranked as the most preferred methods, relative to all other modes (p’s < .001) (232 respondents, see Figure 5). Phone calls, emails and instant messaging were preferred relative to letters (p < .001). The regression model was significant: χ2 = 29.72, p = .020, McFadden’s R2 = 0.05 (text messaging as the reference level). 3 Coefficients revealed that as camouflaging behaviours increased, the likelihood of a participant selecting email (B = −0.04, SE = 0.01, p < .001, OR = 0.96 (95% CI = 0.94–0.98)) or phone call (B = −0.02, SE = 0.01, p = .049, OR = 0.98 (95% CI = 0.95–1.00)) to communicate with their families decreased, relative to text messages.
Mode preference rankings when communicating with family.
Friends
Preference rankings differed between communication modes when communicating with friends (χ2(5) = 364.24, p < .001) (223 respondents, see Figure 6), with face-to-face communication and text message being ranked most highly. Text messaging was preferred relative to phone calls, letters, emails (all p’s < .001) and instant messaging (p = .014). Face-to-face contact was preferred relative to phone calls, letters and email (p’s < .001). Instant messaging was preferred relative to phone calls, letters and email (p’s < .001), and both email and phone calls were preferred to letters (p’s < .001). The regression analysis was significant: χ2 = 50.68, p < .001, McFadden’s R2 = 0.08 (text message as the reference level) and indicated that as anxiety increases, the tendency to prefer to communicate with friends via online messaging decreased, relative to text messages (B = −0.07, SE = 0.04, p = .041, OR = 0.93 (95% CI = 0.87–1.00)).
Mode preference rankings when communicating with friends.
Customer services
Finally, preference rankings also differed between modes when communicating with customer services (χ2(5) = 263.82, p < .001) (245 respondents, see Figure 7), with email being the preferred method of contact, relative to all other options (p’s < .001). Excluding email, instant messaging was ranked as preferable relative to all other modes (p’s < .018). Text was ranked as preferable in comparison to face-to-face (p = .014) and letter communication (p = .016). The regression analysis was not significant (χ2 = 24.22, p = .233, McFadden’s R2 = 0.04), suggesting there is no evidence that age, age at diagnosis, anxiety and camouflaging behaviours influence the preferred communication methods for seeking customer support.
Mode preferences when communicating with customer services.
Qualitative results
Qualitative data were analysed using Thematic Analysis (Braun & Clarke, 2006). Four themes were identified from the responses to our open-ended questions: Not the Phone, Written Communication, Masking versus Autistic Communication and Avoiding Communication (see Figure 8).
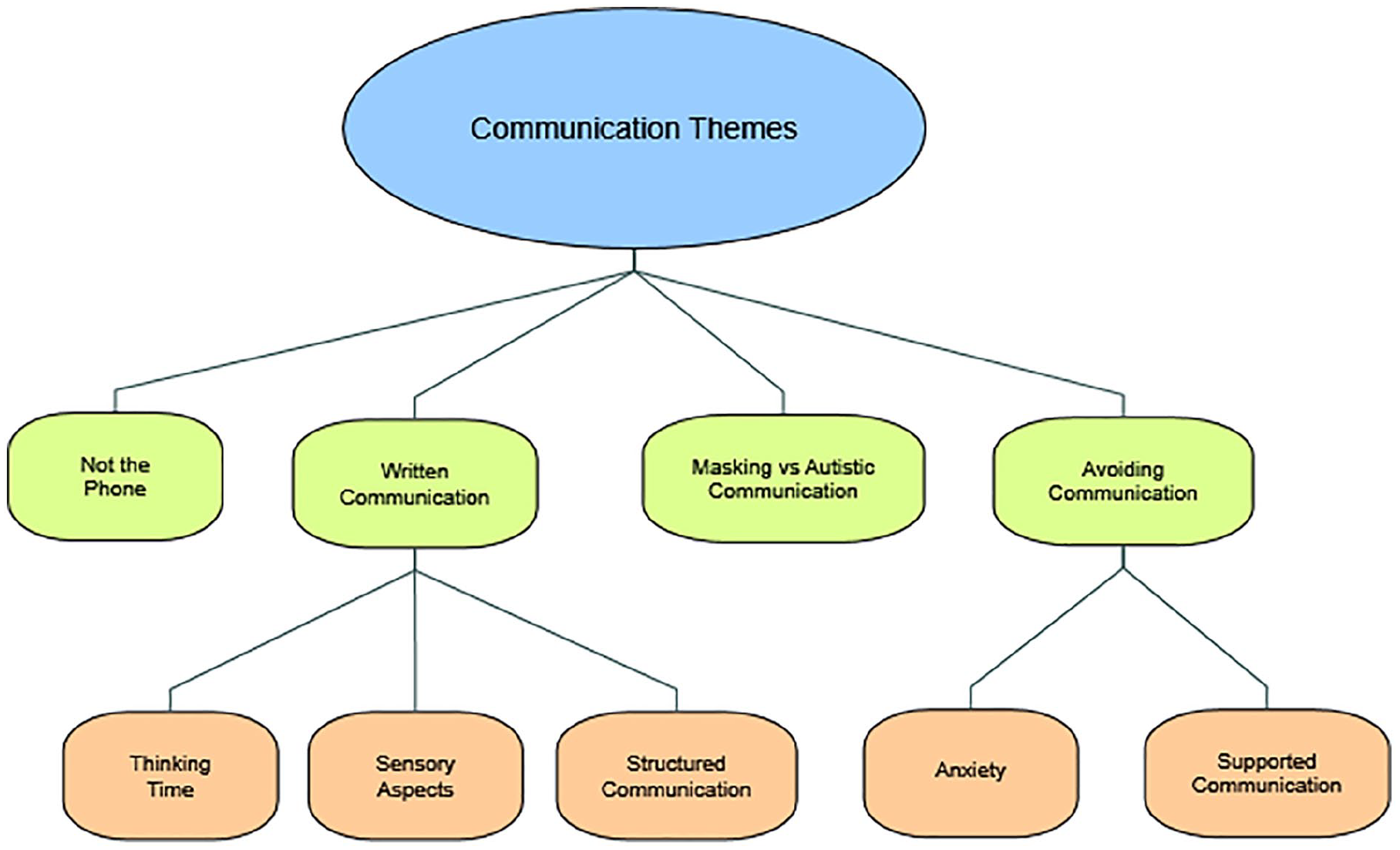
Thematic map of themes and subthemes.
Not the phone
The pattern that was clearest among all participants and scenarios was that autistic people are highly averse to making or receiving phone calls. Participants said things like ‘I absolutely hate having to call anyone and I hate it when [they] call me too!’ and ‘phones are TERRIBLE’. This was felt to be such a universal that one participant commented: ‘I’d be amused to see a phone survey of autistics which managed to recruit’.
This dislike of phone calls was often linked to the difficulties the medium caused: ‘my auditory processing is poor, and trying to say what I want/need verbally is difficult’ and ‘phone calls . . . tend to be paced quite quickly, which can overload me’. The most frequent difficulty was that phone calls caused ‘debilitating anxiety’, with the phrase ‘extreme stress/extremely stressful’ being used repeatedly. One participant stated that general insistence on phone calls as the medium of communication is ‘disabling to the point of outright discrimination’ because the anxiety forms such a barrier.
Some participants linked these challenges directly to aspects of being autistic – especially difficulty inferring social contexts, such as how it is ‘extremely difficult to interpret’ someone’s tone or intentions ‘without other signs to point you in the right direction’. Other participants said that ‘it’s better when I can see the person I’m communicating with’ because then you ‘see the facial and body language of the speaker’. Similarly, a preference for planning and predictability is a key element of being autistic, and phone calls can inherently challenge this: ‘if I’m disturbed by a phone call . . . it’s quite jarring and it can take time afterwards to get back into the flow’. Interestingly, there were almost no participants who stated that the phone was their preferred form of communication, and those who reported that they did use the phone often expressed reluctance and doing so out of necessity: ‘I call them (healthcare) because it’s the only way to get it done’.
Written communication
In contrast to the strong dislike for phone calls, Written Communication was consistently a preferred form of communication, with participants saying: ‘I prefer the written form in general’ and ‘I communicate best through writing’. The reasons for this fell into three subthemes: Thinking Time, Structured Communication and Sensory Aspects, and were common across all forms of written communication – email, letters, online messaging and texting.
Thinking time
This was the most given reason for preferring written communication – writing gave people ‘time to think about what I want to say’, provided the opportunity to ‘arrange my thoughts and ask all my questions before sending’ and the ability to ‘make sure it looks good and reads well’ so their words ‘have the effect that [they] are looking for’. These aspects of written communication were invaluable, as many participants said they had difficulties with the speed of verbal communication, and so using the written form gave them ‘time to process’ what was said to them, their reaction and their response. The time it gave them to form a response was frequently highlighted, with several people pointing out that ‘there is no expectation of an immediate reply’, even in a live online chat, because there is the ‘lag’ time of typing. Removing this immediacy reduced anxiety: ‘I can think of the response . . . without panicking or struggling to find the words I need’.
Structured communication
Another major factor in favour of written communication was it being a ‘structured way to interact’ compared to face-to-face or phone calls, with some participants saying that they ‘research templates for what [they] need’ or ‘find phrases [they] can borrow’. They felt it followed clearer rules of formality (‘texting is not formal . . . would be weird to do with someone who’s above you, but easy to do with someone you work with’) which meant that it felt ‘safe’ because it is often the ‘official’ preference for organisations.
Participants also felt that the structured nature of written communication was helpful because it gave them a greater sense of control over the exchange. For example, many participants talked about how with the written word, they ‘have the information to go over again in the future’, that they have ‘a clear record of what was said’, and that this gives them the chance to ‘correct misunderstandings’ or ‘hold people to account’ (especially when working with services). Written communication was much more predictable for autistic people, commenting: ‘I write my emails all the same, with same starting and ending text’, which made it ‘easier and less anxiety-provoking’. Communicating within the recognised structures of written exchanges allowed participants to express themselves more fully and effectively, providing the opportunity to self-advocate if necessary.
The few participants who expressed reservations about written communication related these to the anxiety of ‘waiting a long time for a response’ (most often regarding letters) or that they ‘can’t be sure they’ve got your email’. Despite these worries, participants often still said that they preferred written communication, but specifically more instant forms such as WhatsApp or live chat where you can see when your message is opened.
Sensory aspects
Also important were the sensory aspects of communication. Several people found verbal communication overwhelming, sharing that ‘I can’t block out other sounds in the background’. In contrast, written communication was often framed as enabling participants to communicate while ‘in a comfortable environment’ for example, without ‘loud noise and bright lights’ as in face-to-face settings. Communicating from your ‘own space’ was ‘a nicer environment’ where ‘chances of being overwhelmed [are] very low’. When autistic people were communicating from a familiar sensory environment, their anxiety was lower, meaning that they ‘can stay calmer and concentrate more’. As with the structured communication subtheme, this led to communicating their needs and ideas more effectively, and the theme was consistent throughout the entire sample.
Masking versus autistic communication
Masking (or camouflaging) when communicating with strangers or non-autistic people was often brought up by participants, especially in direct contrast to the way in which they felt masking was not necessary when communicating with other autistic people. With non-autistic people, participants described feeling ‘forced into an unsuitable conversation pace’, being ‘uncomfortable making eye contact’ and exhausted by ‘having to pull the right face’. One participant said that ‘the more neurotypical they are, the harder it is to communicate’, with others emphasising that they feel there is a ‘performance demand’ when communicating with neurotypical people, leading them to ‘mask a lot’, such as ‘masking tone of voice’, having to do an ‘emotional performance with my face’ and ‘performing neurotypicality to put others at ease’. Maintaining this mask was tiring, and most felt that it had a negative impact on their ability to communicate – because they were thinking about how to ‘modulate [their] behaviour or vocal tone’, they had less capacity to focus on what was being communicated.
Communicating with other autistic people, or accepting non-autistic people, was presented as the opposite experience. One participant summed up time with autistic friends as ‘No masking. All fun!’ Others echoed this sentiment, saying ‘thank god for finding my tribe’ because other autistic people did not judge them for autistic behaviours, such as stimming, or for idiosyncratic communication styles, instead often sharing them: ‘we all talk really fast’. Some participants felt that they had created ‘[their] own societal rules within our home’. Being in these comfortable and accepting environments ‘allows [them] to relax be able to communicate effectively and honestly’. Several participants pointed out that they were more comfortable with face-to-face communication with other autistic people, even making distinctions between autistic and non-autistic family members. What was crucial to how comfortable autistic people were communicating with someone, essentially, was how well understood they felt by that person: ‘once I have an established relationship . . . face-to-face becomes much easier’, ‘when I have a good relationship . . . it maybe allows them to pick up on my true mental and emotional state’ and ‘since I trust them and feel safe . . . I can be myself without being judged’.
Avoiding communication
The final theme was Avoiding Communication, which was split into two subthemes – Anxiety and Supported Communication. Some participants said that they had ‘found it hard all my life to talk to people’ and ‘tend to just avoid communicating as it overloads me’.
Anxiety
The most common reason people gave for avoiding communication was the anxiety it caused them, with one saying ‘[the methods] all cause great amounts of anxiety . . . I wish there were a way to communicate without having to feel so bad’. Due to this anxiety, participants talked about how they ‘put off [communicating] as long as possible’. This anxiety, and especially the aversion to phone calls, had serious consequences for some people, such as missed hospital appointments, failing to get therapy because it was delivered by phone (‘my access to healthcare is undermined’) and losing money because the only way to request a refund was through a customer service telephone number (‘I haven’t done anything about it . . . far too anxiety provoking!’).
Supported communication
The other side of the difficulties many people reported were the support they often called on to enable them to engage in communication. Both informal and formal supports were mentioned, from ‘confer[ring] with trusted parties, e.g. my mother’ to ‘I let my advocate deal with it’. Many participants said that they ‘get someone else to check’ high stakes written communications, such as emails or letters dealing with healthcare or financial matters, and that often in face-to-face situations they ‘want someone with [them] for moral support’. The need for supported communication was often linked to aspects of being autistic, as was the case when discussing difficulties with phone calls, and these two themes overlapped. Examples included ‘I can take someone else with me to a face-to-face meeting, being on the phone feels starkly alone with a disembodied voice’ (showing difficulties interpreting voice without other cues) and ‘I need supported communication when I’m sensory overloaded as I am unable to verbally communicate’ (showing challenges around sensory processing). Having support available to call on was invaluable, with participants saying how this could make them ‘feel part of the conversation’, building relationships and improving their overall sense of wellbeing.
Discussion
This article presents the first large-scale exploration of the communication mode preferences of autistic adults in a range of everyday scenarios. Findings indicate that communication mode preferences differ dependent upon whether the scenario involves people who are typically known (e.g. family, friends, educators and employers) or unknown (e.g. accessing services, research purposes and customer support). When unknown, both the quantitative and qualitative responses indicated an extreme dislike for using the phone, and a strong preference for the written form. When known, both face-to-face and written forms were ranked as preferable. Notably, few individual differences were found to influence mode preference selection, which indicates that communication across most scenarios were independent of age, age at diagnosis, anxiety and camouflaging behaviours. These findings present a clear picture for how to make communication easier and more accessible for this potentially vulnerable group.
The first major theme identified in both the ranking data and the qualitative responses was that autistic people were averse to using the phone, particularly when communicating with unknown contacts. Quotes such as ‘anything but a phone call!’ show how passionately participants felt about this. It is important to highlight though that regression analysis indicated older participants may be more likely to prefer phone calls relative to alternate means when accessing services. This is consistent with patterns observed for the typical population (Hülür & Macdonald, 2020) and indicates that the availability of phone calls as a communication option remains important for inclusion and accessibility. It is also noteworthy that letter communication was ranked as similarly unpopular to phone calls in the quantitative data. We can speculate from the qualitative data that letters were ranked as unpopular given the practical disadvantages of this method (e.g. long waiting times), which is quite different to the explanations given for the dislike of phone calls, which seemed to exacerbate communication challenges.
Considering this strength of adverse responses to phone calls, it is interesting to note that there is very little existing research on autistic people’s views on phones as communication devices, especially since many services rely on their use. Most work to date has looked instead at social media use (often accessed through smartphones) among autistic young people (Kuo et al., 2014) or ‘electronics’ usage in general, with smartphones as one category (Macmullin et al., 2016). What these papers do not address, and this study begins to explore, is attitudes to phone calls – the original function of a phone, rather than the more ubiquitous and varied usage of smartphones in general. Our findings suggest that understanding the ways in which phone calls result in significant anxiety and exacerbate challenges for autistic people is important in developing other communication channels which may be more effective. Whether these are accessed via a smartphone itself appears from our data to be less important, as it is difficulties with phone calls specifically that matter.
The above papers on smartphone usage are often presented in tandem with work on so-called ‘Internet addiction’ (Young, 1998) among autistic young people, where it has been argued that they may face ‘special risks’. A recent review has found that autistic young people spend more time on screens, from an earlier age, than their non-autistic counterparts (Slobodin et al., 2019). There is a wealth of papers about the dangers of screen-time for autistic children and young people, finding that more time on screen-based media is associated with behavioural problems in autistic boys (Mazurek & Engelhardt, 2013), with lower levels of physical activity (Dreyer Gillette et al., 2015) and with worse sleep hygiene (Richdale & Schreck, 2019).
In contrast to this overwhelmingly negative narrative about screen- and Internet-usage, the autistic adults in our research emphasised repeatedly how the Internet was a key mode of communication for them, and how it had a positive impact in their lives. The ease-of-use and structured, predictable nature of email made it the strongly preferred mode in many scenarios, and this was supported by the extensive quotes about how email, live chat or messaging gave people ‘thinking time’ and ‘control over things’. These positives of written communication online have been borne out in other studies of autistic Internet engagement. For example, Benford (2008) also found that email was the preferred mode of communication in their sample of 138 autistic adults, and that communicating online was in some ways liberating because it created a more equal basis of interaction by removing the disadvantage of needing to interpret body language. Similarly, research has shown that autistic adults use the Internet to build supportive relationships, often around shared interests, with people who would not otherwise have been accessible due to geography or challenges in joining face-to-face groups (Burke et al., 2010; Gillespie-Lynch et al., 2014; Jordan & Caldwell-Harris, 2012). Research has shown that social media use for social connection is common among autistic adults, and is associated with greater happiness (Ward et al., 2018), and friendship quality (van Schalkwyk et al., 2017), which highlights the importance of making such means accessible.
One of the key qualitative findings which explained the statistical preferences for written communication formats was that of Anxiety. Participants reported that modes such as email, messaging and live chat were all ‘far less anxiety inducing’ than phone calls or face-to-face meetings in general, especially in more formal circumstances. The anxiety associated with communication among autistic people is well-documented, with high levels of social anxiety being common across the lifespan (Kuusikko et al., 2008; Maddox & White, 2015). Greater social anxiety is correlated with worse communication skills in non-autistic (Koç & Dündar, 2018) and autistic people (Spain et al., 2018). This anxiety and concomitant difficulties have been found to lead to higher levels of loneliness (Zakahi & Duran, 1982) as people may avoid engaging in social interaction to mitigate their anxiety. This is seen in our participants, as many people discussed Avoiding Communication in part due to being anxious, even if this was to their detriment. It seems that the reduced reliance on non-verbal cues for written communication reduces anxiety, but the removal of these cues in spoken communication (e.g. on the phone) increases anxiety. This may be because everyday spoken communication often integrates non-verbal cues, and some of these remain present (e.g. tone of voice) while some are removed (e.g. body language). This means that autistic people may feel they are working with ‘partial information’, which is harder to interpret, whereas in written communication, there is no expectation that they will be able to interpret beyond what is explicitly written down. While there were many qualitative reports of anxiety, there was little statistical effect on mode preferences, although this may be because most participants scored highly so there is little variation for the model to explain.
Importantly, when communicating in scenarios when people are typically known, such as family, friends, in education and in employment, participants often ranked face-to-face modes as preferable, in addition to various written modes. Understanding the nuances as to when face-to-face versus written methods are preferred in these specific scenarios goes beyond the scope of these data, but we can speculate based on the qualitative data that this may relate to how familiar and trusted these individuals were. Participants discussed feeling much less anxiety when they were engaging with familiar trusted people, especially if those people were also autistic. This finding sits within a growing body of recent research which finds that autistic people are more comfortable communicating with others on the spectrum because they feel more accepted and therefore more able to be themselves (Crompton, Hallett et al., 2020). Interestingly, it has also been shown that autistic-to-autistic information transfer is just as effective as non-autistic-to-non-autistic information transfer in a communication chain, in comparison to mixed autistic-to-non-autistic chains where there was significantly more loss of detail in what was passed on (Crompton, Ropar, et al., 2020). This article also showed that autistic people felt greater rapport with other autistic people – despite the other person’s diagnostic status not being disclosed – which is supported by work finding that autistic adults disclose more information about themselves to other autistic adults than to non-autistic research partners (Morrison et al., 2020).
Further to the findings that autistic-to-autistic communication is characterised by greater acceptance and effectiveness, there has recently been work looking specifically at autistic communication through online media. Studies looking at the communication patterns of autistic young people while gaming online have found that they build idiosyncratic worlds of shared intersubjectivity, with norms around communication which work for the members of the game that often build rapid rapport (Heasman & Gillespie, 2018; Ringland et al., 2016). These shared ‘safe spaces’ should be encouraged, as suggested by research which has found that autistic communication styles which may be considered ‘atypical’ can actually contribute to better first impressions with other autistic teenagers and lead to better friendships (Granieri et al., 2020). Therefore, social skills programmes should seek not to ‘normalise’ the communication styles of autistic young people, but instead focus on supporting young people to find those who are accepting of their differences, something which is associated with better mental health and wellbeing outcomes long-term (Cage et al., 2019).
Masking and ‘performing neurotypicality’ was a strong theme in the qualitative responses. Statistically, there were small increases in preferences for different types of written communication as camouflaging increased, but these were out of line with the clarity of the qualitative data about the importance of camouflaging in communication choices. Many participants talked about how written communication was preferred as it required less camouflaging and masking, such as not needing to ‘do eye contact’ or ‘make my face and hands do the right thing’, in line with work on linguistic and gestural camouflaging (Parish-Morris et al., 2017; Rynkiewicz et al., 2016). It may be that although participants are aware of camouflaging when they are using different communication modes, this is so pervasive in their lives that it does not significantly change how they choose to communicate because other factors, such as speed and convenience, are more important in their decisions.
Arising from our research are recommendations for services, organisations and researchers to avoid having systems which rely solely or predominantly on people either making or answering phone calls. A range of contact options should be provided that includes online written modes. For example, making email addresses prominent on a website, through to offering live online chat. Doing this would improve the experiences of autistic users, with potentially important positive impact on their health and wellbeing. Also, following the principles of Universal Design (Steinfeld & Maisel, 2012), these changes are likely to make engaging with organisations better for all users, not just those on the autism spectrum.
Limitations
This was a novel piece of research which sought to answer important questions about autistic people’s lived experiences. Despite this, there are some limitations to the project. First, the sample is not representative of the breadth of lived experiences of autistic people – it was an online written study, meaning that participants had to have the literacy ability and technical skills to engage. This may have excluded those who have lower intelligence quotient (IQ) or educational achievement and accentuated the preference for Internet-mediated modes. We were unable to verify clinical diagnoses of autism, although the ‘check’ of including the AQ-10 suggested that nearly all participants met criteria despite known biases against non-males in diagnostic screening tools (Agelink van Rentergem et al., 2019). We have also chosen to respect self-identification as many autistic adults can face barriers to formal diagnosis (Bargiela et al., 2016). A final issue regarding our sample is that it was predominantly female, which could introduce a potential bias as women may have communication preferences which differ to those of men and non-binary people. There has been little research to date into gender differences in communication preferences, and what recent work there is tends to focus on things like differences in usage of social media platforms rather than communication generally, as we did in this study. Examining whether and what these differences may be would be an interesting avenue for future research. Second, we sound a note of caution when interpreting the regression analysis – the effect sizes are very small, and more data are needed to make conclusions considering the number of predictors and the lack of variation in responses. Thirdly, our data were collected before the COVID-19 pandemic took hold, which has necessarily changed communication for everyone, both autistic and non-autistic. Video calls are now an incredibly common and regularly used communication type in all scenarios, and it would be interesting to explore autistic people’s views on this development in future research. It is also worth noting that while the GAD-7 is widely used in autism research, and has been validated in the general population, it has not been specifically validated with autistic people. This means that it may not be as sensitive to anxiety in this group as non-autistic people. Finally, it would be valuable for future research to conduct a similar study with a non-autistic sample so that comparisons could be drawn between the two populations, which were beyond the scope of this study.
Conclusion
Overall, our data highlighted the challenges around communicating with services and organisations when these rely on phone call–based methods. There is a clear preference for written communication in many scenarios, as this provides structure, increases thinking time and reduces both sensory issues and anxiety. This work also highlights the ways in which autistic people and their networks adapt to support them, and that it is possible for autistic people to interact successfully and positively when the situation supports them to do so.
Supplemental Material
sj-pdf-1-aut-10.1177_13623613211014995 – Supplemental material for ‘Anything but the phone!’: Communication mode preferences in the autism community
Supplemental material, sj-pdf-1-aut-10.1177_13623613211014995 for ‘Anything but the phone!’: Communication mode preferences in the autism community by Philippa L Howard and Felicity Sedgewick in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.