
Abstract
Sleep problems are one of the most common complaints in autistic adults. This study aimed to report the perspectives of autistic adults in the United Kingdom on treatment of their sleep problems. A total of 288 autistic adults living in the United Kingdom completed an online survey including assessments of their sleep quality using the Pittsburgh Sleep Quality Index, reporting their experiences and preferences of sleep treatment with UK healthcare professionals and, their experiences of self-management of their sleep. Self-report data revealed 58% of participants had not attended a consultation with a healthcare professional regarding their sleep problem despite 90% meeting the criteria for poor sleep quality (based on the Pittsburgh Sleep Quality Index). Of the participants who attended a consultation for their sleep, 72% were prescribed medication and 60% were not satisfied with the outcome. Self-management of sleep problems was not effective for 80% of participants; 41% reported a preference for non-medication options such as education, advice and talking therapies for sleep treatment. This report highlights the need for a fundamental shift in the consideration of sleep problems in autistic adults given the high levels of co-morbidity. The development of successful management strategies in adulthood that importantly considering autistic adults’ preferences could reduce sleep problems and overall improve quality of life for autistic adults. Long term this could also reduce the need for prescribed medication in this population.
Lay abstract
Sleep problems are one of the most common complaints by autistic adults. This study aimed to report the perspectives of autistic adults on treatment of their sleep problems; 288 autistic adults living in the United Kingdom completed an online survey which assessed their sleep quality. We also gathered data on experiences and preferences of sleep treatment with UK healthcare professionals and their experiences of self-management of their sleep; 58% of autistic adults never had a visit with a healthcare professional regarding their sleep problem, despite 90% meeting the criteria for poor sleep quality. Some of those who attended a consultation for their sleep were prescribed medication (72%), but 60% were not satisfied with the outcome. The participants also reported that sleep self-management was not effective (80%); 41% reported a preference for non-medication including education, advice and talking therapies for sleep treatment. This report highlights the need for a fundamental shift in treatment of sleep problems in autistic adults. The current treatments are not resolving sleep issues; hence, it is imperative to develop management strategies that considers autistic adults’ preferences, reduces sleep problems and thus improves quality of life for autistic adults.
Introduction
Increased rates of psychiatric disorders (e.g. anxiety, depression, bipolar disorder) and medical conditions (e.g. autoimmune conditions, gastrointestinal (GI) and sleep disorders) are reported in autistic adults when compared with neurotypical age and sex-matched peers (Croen et al., 2015). However, in the United Kingdom, services are significantly weighted towards diagnostic and paediatric services, rather than the treatment and support of adult care (Murphy et al., 2016). Specifically, there is an unmet need around common co-existing conditions in autistic adults and limited evidence of treatments for co-occurring symptoms of disorders in autistic adults (Howes et al., 2018).
Sleep problems are one of the most common complaints in autistic adults (Gotham et al., 2015) with prevalence rates of sleep problems reported as high as 79%. Sleep quality has been found to predict quality of life in both autistic and non-autistic adults (Lawson et al., 2020). Abnormalities in melatonin production and circadian timing may contribute to insomnia or circadian sleep disturbances (Murphy et al., 2016). In addition, sleep issues may also be further compounded by other health issues (e.g. GI, anxiety; Murphy et al., 2016). In the United Kingdom, sleep medications have been reported as one of the most commonly prescribed drugs to autistic adults, despite limited evidence of their efficacy or effectiveness in this adult population (Howes et al., 2018).
Treatment pathways for autistic adults with sleep problems have yet to be established in the United Kingdom. We report the findings from a short survey completed by autistic adults to identify recommendations for healthcare providers (HCPs) for the treatment of sleep problems in this population.
Methods
A cross-sectional survey of 288 autistic adults (Mage = 37.86 years, SD = 11.41 years), living in the United Kingdom (86 males, 169 females, 29 non-binary, 4 prefer not to say) was conducted. All participants identified as an autistic adult (250 were diagnosed by a healthcare professional, 38 were self-diagnosed). The survey included demographic information such as age, gender, ethnicity, employment, education status and socioeconomic status (SES) was assessed using the English Indices of Multiple Deprivation (IMD) 2019 Score, a validated tool for measuring SES (McLennan et al., 2019). Most participants were of ‘White’ ethnic background (91%) and had completed a minimum of secondary school education (88%). Over half reported being employed (55%).
Participants were asked 10 author created questions relating to their sleep quality (e.g., ‘Do you believe you have a problem with your sleep?’), the type of sleep problem(s) they have experienced (e.g. Please indicate whether you have any of the following sleep problems?), sleep treatment, (e.g. ‘Have you seen a healthcare professional about your sleep?’) and the outcome of seeking professional support for their sleep problems (e.g. ‘If you have seen a healthcare professional: How satisfied were you with the outcome?’) See Supplementary Material for full list of questions. Finally, participants completed a validated sleep questionnaire. The Pittsburgh Sleep Quality Index (PSQI; Buysse et al., 1989) is a 24-item retrospective questionnaire that assesses sleep quality over a 1 month time interval. A global score of ⩾ 5 indicates poor sleep quality. This scale has previously shown good internal consistency in high-functioning autistic adults (Cronbach’s α = 0.68; Baker & Richdale, 2015).
Ethical approval was received from the University College London Research Ethics Committee (REC: 1227). Prior to completing the survey, all participants provided informed consent.
Results
Sleep problems and quality
The majority of participants reported having a sleep problem (83%), which was supported by results of the PSQI data, suggesting 89% of participants met the criteria for poor sleep quality. The mean PSQI score across the sample was 10.79 (SD 4.05), which is above the threshold for poor sleep quality (Buysse et al., 1989). The most commonly reported sleep problems were insomnia (56%, n = 162) and restless leg syndrome (32%, n = 92). See Table 1 for full report of sleep problems.
Summary of autistic adults’ (diagnosed by HCP and self-diagnosed, n = 288) demographic information and average sleep score on the PSQI.
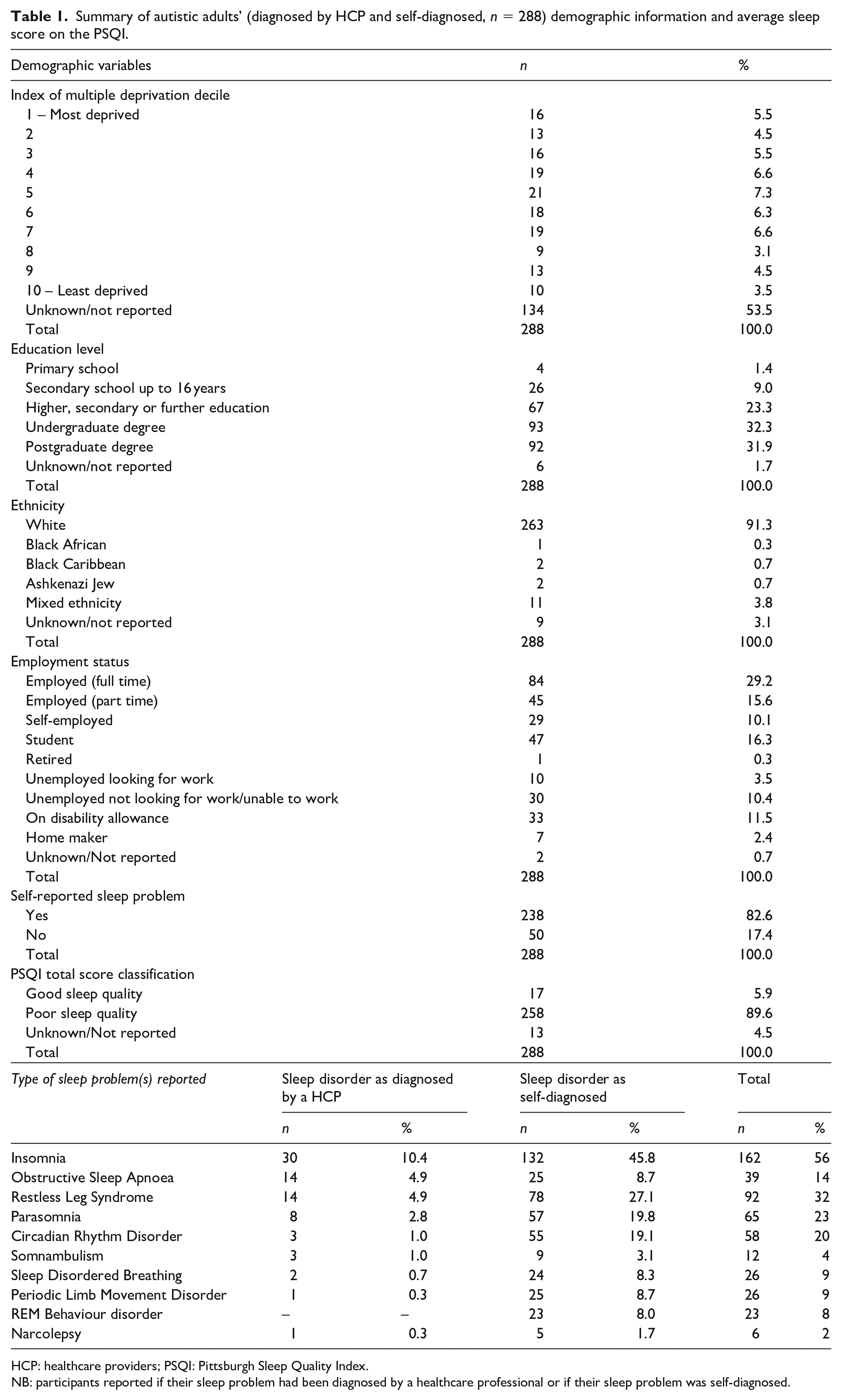
HCP: healthcare providers; PSQI: Pittsburgh Sleep Quality Index.
NB: participants reported if their sleep problem had been diagnosed by a healthcare professional or if their sleep problem was self-diagnosed.
A chi-square test of independence was performed to examine the association between gender and classification of sleep quality on the PSQI. The association between these variables was significant χ2(1) = 5.37, p = 0.020, Cramer’s V = 0.15. Females were more likely than males to be classified as poor sleepers on the PSQI. Furthermore, a chi-square test of independence was performed to examine the relation between autism diagnosis (diagnosed by a HCP or self-diagnosed) and classification of sleep quality on the PSQI. The relation between these variables was non-significant χ2(1) = 0.27, p = 0.601, Cramer’s V = 0.03. There were no differences between participants who were diagnosed by a HCP or self-diagnosed with autism on whether they were classified as poor sleepers or good sleepers on the PSQI.
Accessing HCP for sleep problems, appointment outcomes
For the following section, we analysed participants who confirmed diagnosis by a healthcare professional and those who reported self-diagnosis separately.
1. For participants who reported a HCP diagnosis of autism (n = 250):
Self-report data revealed 56% (n = 141) of participants had not attended a consultation with a HCP regarding their sleep problem despite 90% (n = 224) meeting the criteria for poor sleep quality using the PSQI and 83% of participants perceiving a sleep problem (n = 208); 109 (44%) respondents sought advice from a HCP for a sleep problems, received varied treatment options. The most common outcome was prescription of medication reported by 64% (n = 70), this was split between medication targeted for sleep (35%, n = 38) and medication targeted at other conditions which could indirectly improve sleep outcomes (e.g. antidepressants; 29%, n = 32). Nearly one-third of the sample received education and advice regarding sleep hygiene strategies (28%, n = 31) and 12% of participants were referred to psychological therapies targeted at sleep problems (12%, n = 13). A smaller portion of the sample was recommended a medical device (e.g. CPAP machine; 9%, n = 10), and where further investigation was needed, eight participants were referred to specialist sleep services (7%). Close to one-fifth of the sample reported lack of treatment or advice from their HCP (n = 21).
2. For participants who reported a self-diagnosis of autism (n = 38):
Self-report data revealed 71% (n = 27) of participants had not attended a consultation with HCP regarding their sleep problem despite 90% (n = 34) meeting the criteria for poor sleep quality using the PSQI and 79% of participants perceiving a sleep problem (n = 30). Of the 11 (29%) respondents who had sought advice from a HCP for a sleep problem, treatment options varied. All participants reported that the most common outcome was prescription of medication (n = 11), and this was split between medication targeted for sleep (82%, n = 9) and medication targeted at other conditions which could indirectly improve sleep outcomes (e.g. antidepressants; 27%, n = 3). Five participants received education and advice regarding sleep hygiene strategies (45%) and two were referred to psychological therapies targeted at sleep problems (18%). One participant reported lack of any treatment or advice from their HCP.
Accessing HCP: satisfaction rates
To determine the treatment options of those individuals who reported being somewhat or very satisfied with their treatment outcome we filtered the data to look at treatment outcomes only in these individuals (n = 22). The most common outcome reported was prescription of medication (73%, n = 16), and this was split between medication targeted for sleep (50%, n = 11) and medication targeted at other conditions which could indirectly improve sleep outcomes (e.g. antidepressants; 23%, n = 5). Five participants reported to receive education and advice regarding sleep hygiene strategies (23%) and four were referred to psychological therapies targeted at sleep problems (18%). Four participants were recommended a medical device (e.g. Continuous Positive Airway Pathway (CPAP) machine; 18%). Therefore, individuals receiving sleep medication seemed to be most satisfied with their treatment outcome.
Barriers to seeking treatment for sleep problems
The 168 participants who had not sought treatment for sleep problems were further asked to state reasons for not seeking treatment. Over one-third reported not feeling the need to pursue healthcare advice or did not consider their sleep a health priority (35%, n = 59). A significant portion of the group were reluctant to either visit a HCP, undergo more medical treatment or diagnoses (28%, n = 45), and nearly one-fifth were unconvinced seeking professional advice would help (17%, n = 28). Some participants were unaware of the treatment options available or that HCPs could address sleep issues (9%, n = 15). When participants had mentioned their sleep concerns during a healthcare consultation but not directly sought treatment for sleep problems (n = 13), only four felt the matter had been addressed. A small sample found that they were unable to access care (3%, n = 5) or did not have time to do so (1%, n = 2).
How did respondents report self-managing their sleep problems?
The whole sample was asked to report (a) whether they had tried any self-treatment options for sleep issues in the past and present and (b) rate the effectiveness of any tested strategies; 31% (n = 89) were currently self-treating their sleep problems, 33% (n = 96) had attempted to self-treat in the past, and 36% (n = 103) had never attempted any self-treatment strategies (e.g. herbal supplements, white noise, meditation). A five-point Likert-type scale was used to enquire the effectiveness of self-treatment for 185 participants who reported using this strategy in the past or present, of which 149 participants responded; 25% (n = 37) stated their self-treatment was ‘very’ or ‘somewhat’ effective, 34% reported feeling neutral (n = 51) and the majority reported felt ‘very’ or ‘somewhat’ unsatisfied (41%, n = 61) with their self-treatment strategy.
Preferences for sleep treatment among autistic adults
All participants were asked what a preferred treatment option would be for sleep-related issues. One participant did not respond to this question (n = 287). The majority of the sample reported a preference for non-medication options such as education, advice and talking therapies (41%, n = 118), and only 7% (n = 21) chose medication-only as their preferred treatment, although a significant portion (38%, n = 109) opted for a mixed approach utilising both pharmacologic and non-pharmacologic therapies. A smaller proportion of the group stated they would not want treatment for sleep-related issues (14%, n = 39).
Discussion and recommendations
The results provide insight into the perspectives for the management of sleep from the perspectives of autistic adults in the United Kingdom. Based on the results, four key recommendations are outlined in the following:
1. Sleep as part of a routine clinical assessment for autistic adults.
Despite the high prevalence of sleep problems that co-exist alongside autism, these go largely unrecognised or treated in autistic adults, leading to an acceptance that sleep disorders/problems are part of autism both by autistic adults and HCPs. Recognition of sleep disorders/problems and their impact and subsequently the treatment could improve quality of life in autistic adults.
Recommendation: Sleep disorders/problems should be included in routine clinical assessments by HCPs. Future research to consider the associations between sleep and cognitive functioning, well-being, physical and mental health as well as employment and daily living in autistic adults.
2. Support from HCP in treating co-existing conditions.
The survey highlights considerations for the relationship between autistic adults and HCPs; 28% were reluctant to visit a HCP and this should be investigated further as may reflect barriers to seeking healthcare beyond sleep problems specifically. Similar to a survey on the treatment of insomnia in the United Kingdom (Stinson et al., 2006), our results indicated a belief by participants that going to a HCP will not help resolve their sleep issues and, of those who sought treatment, 60% were not satisfied with the outcome of seeking treatment for their sleep problems. However, participants who were satisfied with the outcome of seeking treatment for their sleep problems were mostly prescribed medication or received a targeted sleep intervention (such as a CPAP machine). These findings potentially suggest a lack of understanding of the importance and the impact of sleep problems on the overall health of autistic adults. Given that some participants were satisfied with their treatment, these results suggest that when appropriate targeted treatments are provided, treatment may result in a satisfactory outcome.
Recommendation: Clinical training and awareness for assessment of the sleep problem and appropriate/treatment management should be widely available to both HCPs and the autistic population.
3. Availability of sleep management education for autistic adults.
Although many participants had reported self-treatment strategies, only 20% reported these as somewhat or very effective. Our findings indicate information available for self-management is not efficacious for the majority of this population.
Recommendation: The development of evidence-based sleep management education tailored for autistic adults to be provided as a first line of support for addressing sleep problems may be beneficial.
4. Development of a practice pathway for sleep in autistic adults and implementation of interventions targeted at sleep.
The majority of autistic adults that sought treatment for their sleep reported being prescribed medication; however, the majority would prefer a non-medication option (41%) with 38% opting for a mixed approach. The current recommended pathway for autistic children includes assessment and behavioural approaches as a first-line approach, with pharmacologic therapy indicated in certain situations (Malow et al., 2012). Behavioural therapies have been successful with autistic adults (Cooper et al., 2018); therefore, behavioural approaches such as Cognitive Behavioural Therapy for Insomnia could also be considered for autistic adults. Correct assessments of the sleep problem leading to appropriate treatment would be beneficial to include in a treatment pathway (e.g. CBT-I, circadian rhythm disruption with chronotherapy and melatonin; Guénolé et al., 2011).
Recommendation: Future research on the feasibility and efficacy of treatment for sleep problems in autistic adults, and to consider if sleep difficulties act as a barrier to the success of other interventions in this population. Treatment efficacy and preferences should inform a standardised recommended pathway.
The sample in this survey comes from the United Kingdom; thus, our findings are limited to how sleep problems are treated in UK healthcare settings. It should be noted that higher ratio of female to male participation in this study, and therefore, under-representation of males might be due to convenience sampling. Also, given the fact that females reported higher sleep problems than males on the PSQI, further research to explore how and if sleep problems may present differently in males and females, and the impact this may have on pathways to sleep treatment, is warranted. Having a diagnosis of autism was self-reported and therefore we are unable to establish if autism severity and symptoms related to the results. This report highlights the need for a fundamental shift in the consideration of sleep problems in autistic adults given the high levels of co-morbidity. The development of successful management strategies in adulthood, that importantly considering autistic adults’ preferences, could reduce sleep problems and overall improve quality of life for autistic adults
Supplemental Material
sj-pdf-1-aut-10.1177_13623613211007226 – Supplemental material for The treatment of sleep problems in autistic adults in the United Kingdom
Supplemental material, sj-pdf-1-aut-10.1177_13623613211007226 for The treatment of sleep problems in autistic adults in the United Kingdom by Elizabeth Halstead, Emma Sullivan, Zoe Zambelli, Jason G Ellis and Dagmara Dimitriou in Autism
Footnotes
Acknowledgements
Thank you to all the autistic adults who participated in our survey, special thanks to Jon Adams and Cos Michael who have consulted on the survey design.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by The John and Lorna Wing Foundation, UK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.