
Abstract
Autistic adults who have a history of committing crimes present a major problem for providers of services in terms of legal disposal options and possible interventions, and greater understanding of this group and their associated needs is required. For this reason, we aimed to investigate the face validity of a proposed sub-typology of autistic adults detained in secure psychiatric hospitals in the United Kingdom. Initially, a focus group was completed with psychiatrists, clinical psychologists, healthcare workers, family members and autistic adults who had been detained in hospital, leading to revisions of the sub-typology. Following this, a consensus rating exercise of 10 clinical vignettes based on this sub-typology with three rounds was completed with 15 psychiatrists and clinical psychologists; revisions to the vignettes to improve clarity were made following each round. The findings indicated that these subtypes possess face validity and raters were able to classify all 10 clinical case vignettes into the sub-typology, and percentage of agreement ranged from 96% to 100% for overall subtype classification. This study suggests that the further validity of the sub-typology should be investigated within a larger study, as these subtypes have the potential to directly inform the hospital care pathway such that length of stay can be minimised.
Lay abstract
Autistic adults who have a history of committing crimes pose challenges for the criminal justice system in terms of disposal and treatment. For this reason, we investigated the validity of a proposed sub-typology of autistic adults detained in secure psychiatric hospitals. Initially, we ran a focus group with psychiatrists, clinical psychologists, healthcare workers, family members and autistic adults who had been detained in hospital to consider a sub-typology of autistic adults who may come into contact with secure psychiatric hospitals. We asked 15 psychiatrists and clinical psychologists to rate 10 clinical vignettes based on our sub-typology with three rounds; revisions to the vignettes to improve clarity were made following each round. The findings indicated that these subtypes possess face validity and raters were able to classify all 10 clinical case vignettes into the sub-typology and percentage of agreement ranged from 96% to 100% for overall subtype classification. The findings suggested that the further validity of the sub-typology should be investigated within a larger study using a clinical sample. These subtypes may help inform treatment and care pathways within hospital.
Keywords
It has been reported that around 40% of individuals in specialist commissioned secure services in the United Kingdom have an autism spectrum disorder (ASD; NHS Digital, 2019). This is markedly higher than the estimated prevalence of autistic adults within the community in England (i.e. 9.8 per 1000; Brugha et al., 2012). It is therefore notable that there are no specific care pathways described by the National Institute for Health and Care Excellence (NICE, 2016) for people with ASD detained in psychiatric hospitals, including those with a history of criminal offending (Alexander et al., 2016). Current research about this group is sparse in terms of aetiology, clinical presentation, risk profile or treatability (Gunasekaran, 2012). The limited evidence that does exist points to the heterogeneous nature of difficulties faced by these individuals. While some researchers have sought to compare individuals with and without ASD in these settings (e.g. Cheely et al., 2012; Murphy, 2003; North et al., 2008; Woodbury-Smith et al., 2005), there have been no attempts to examine differences within this particular population, nor any theoretical efforts to understand whether there are differing subgroups or types within this population which has the potential to inform clinical interventions.
There are advantages associated with typological classifications as they reduce complex information about a heterogeneous group into meaningful, more homogeneous categories by (a) providing practicing professionals, criminal justice officials and others with concise information to aid defensible decision-, policy- and law-making, (b) offering guidance about risk assessment and treatment interventions and (c) helping to make theory development more manageable (Helfgott, 2008). Furthermore, quantitative and qualitative differences between those with a history of forensic mental health problems may suggest differential aetiological factors, intervention strategies and management approaches and serve to inform the development of more complex multi-factor theories (Ward & Hudson, 1998). In particular, a typological classification of people with ASD in secure psychiatric services would increase knowledge and understanding regarding the relationship between ASD and forensic risk in terms of aetiology and prognosis of forensic mental health problems, thus having the potential to augment clinical care pathways and the commissioning process (Alexander et al., 2016).
Alexander et al. (2016) proposed a potential typological classification of people with ASDs in secure psychiatric services developed from the authors’ accumulated clinical experience and existing research literature. These authors hypothesised people with ASD in secure psychiatric services can be classified into eight potential subtypes according to three factors: (1) psychopathic traits conceptualised on a spectrum ranging from higher to lower, with particular focus on the interpersonal-affective (IA) features of the disorder (i.e. manipulative, deceitful, superficial, callous and unemotional); (2) the presence or absence of psychosis and (3) behavioural problems, also conceptualised on a spectrum ranging from higher to lower where infrequent behavioural problems with high intensity are characterised as lower (see Figure 1).
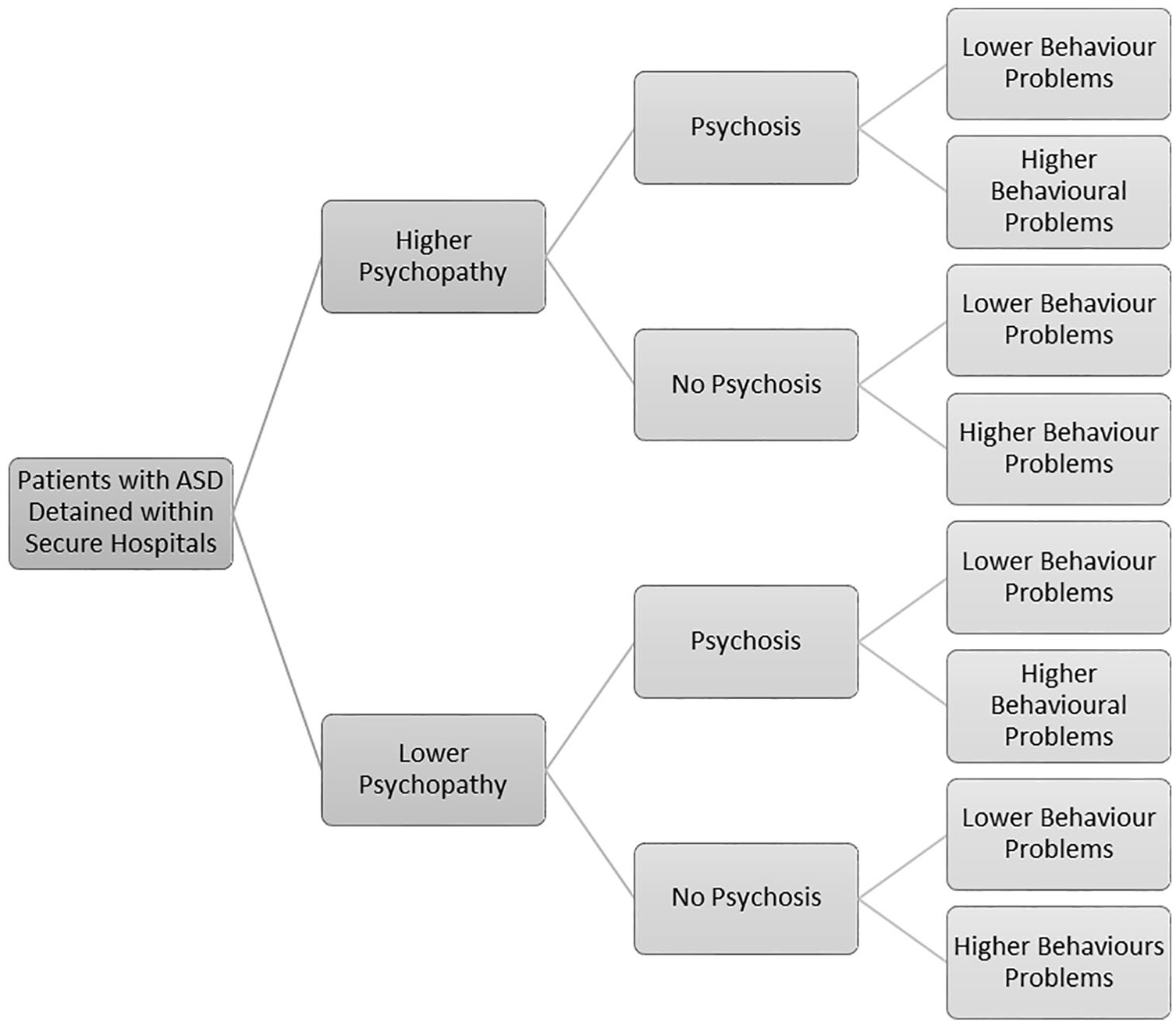
Descriptive subtypes of patients with ASD detained in secure hospitals (Alexander et al., 2016, p. 206).
It was hypothesised that individuals characterised by lower psychopathy (IA), no psychosis and higher behavioural problems would likely require relatively short lengths of stay in hospital as their difficulties are likely to be related to ASD and associated challenging behaviour which may include communication difficulties. Care and treatment may include implementation of psychological interventions for challenging behaviour. Conversely, individuals presenting with higher psychopathy (IA), psychosis and higher or lower behavioural problems are likely to require management in secure conditions, and longer lengths of stay in part due to their associated forensic mental health problems (Alexander et al., 2016), which may include risk to themselves and others, and these difficulties may be aetiologically distinct from ASD. It was considered that the latter group, especially those with higher psychopathy (IA), would present with increased forensic risk.
The typology draws evidence emphasising specific neurocognitive deficits and co-morbid psychopathology as explanations for forensic risk among individuals with ASD. Prevalence data examining offending behaviours among people with ASD suggest they are less likely to engage in criminal behaviour, compared to the general population (Im, 2016) or that the risk is at least not elevated (Hippler et al., 2010). In fact, extant findings indicate that it is in fact a range of other factors which contribute towards violence and criminal behaviour in this group, in particular co-morbid forensic mental health problems, rather than ASD per se (Allely et al., 2017; Mouridsen, 2012). Specifically, antisocial personality disorder and associated psychopathic traits (Dein & Woodbury-Smith, 2010; Gunasekaran, 2012; Rogers et al., 2006; Woodbury-Smith et al., 2005), as well as severe and enduring mental health problems (e.g. schizophrenia; Kincaid et al., 2017; King & Murphy, 2014), are thought to be prevalent in offenders with ASD (or those at risk of following that path) and provide a more valid theoretical justification to directly inform clinical treatment. There is evidence that schizophrenia spectrum disorders have an elevated incidence among the ASD population, which has been estimated to be 12.8% (Chisholm et al., 2015), while symptoms of psychosis, as well as dangerousness and difficulties with self-care, are frequently reported reasons for admission to psychiatric hospitals among the general population (Bowers, 2005). Considering behaviour problems, there is evidence that challenging behaviours (e.g. self-injury, aggression) are associated with a diagnosis of ASD in those who have intellectual disabilities (McClintock et al., 2003).
However, psychopathy may present differently with some offenders with developmental disabilities, specifically, those with intellectual disabilities (Morrissey et al., 2005). These individuals may not have difficulties with a parasitic lifestyle, many short-term relationships and a range of antisocial behaviours (Morrissey, 2003) while retaining many of the IA features of the disorder. Pouls and Jeandarme (2014) reported that Psychopathy Checklist – Revised (PCL-R) scores were lower for people with intellectual disabilities relative to others within forensic mental health services, and not all items on the PCL-R (Hare, 2003) could be scored. They recommended use of the short version of the PCL-SV, which has been supported by others (Alexander et al., 2012; Gray et al., 2007). For those with ASD, they may inadvertently score as having a callous lack of empathy and shallow affect which may not be associated with psychopathy in the way intended (Morrissey, 2003). Recent theoretical explanations suggest that behaviours that on surface can appear cold-hearted and uncaring could stem from theory of mind impairments (inability to understand another’s point of view or to react appropriately), rather than a genuine lack of distress as a consequence of failing to resonate with another person’s distress, which would be the case for those who have psychopathy (Bird & Viding, 2014). Many experienced clinicians may find it difficult to differentiate between the two in practice. Lockwood et al. (2013) demonstrated that difficulties with affective resonance (or affective empathy) tended to characterise those individuals with high levels of psychopathic traits, while difficulties with cognitive perspective taking characterised those individuals with high levels of autistic traits. Blair (2008) considered these differences by drawing on the ‘fine cuts’ technique which was used by Frith and Happé (1994) to explain why people with ASD may be able to successfully complete some tasks (e.g. elicited structured play) but struggle with other tasks (e.g. spontaneous pretend play), even though both sets of tasks may appear similar or related. The reason for the difference ability to complete some tasks, as opposed to other related tasks, was associated with the neurocognitive skills required to complete these tasks (e.g. mentalisation). Blair (2008) argued that both psychopathy and ASD are disorders of social cognition and argued that those with ASD have difficulties with cognitive empathy, while those with psychopathy have difficulties with affective empathy. These issues are likely to be related to difficulties in the functioning of the amygdala (Blair, 2006, 2008).
Considering these issues, it is important to be able to sensitively assess psychopathic (IA) traits when working with people who have ASD. Clinicians must be able to accurately differentiate whether seemingly cold-hearted and uncaring behaviours reflect a genuine indifference to others’ distress or whether they are a reflection of a poor understanding of other minds. Careful attention to these issues will help to ensure the validity of any associated typology.
While ensuring that any typology is firmly grounded within the evidence base is vital, a robust typology should also meet the following criteria (Helfgott, 2008): (1) clarity and objectivity (i.e. each category should be sufficiently detailed and the criteria for category membership precise); (2) reliability (i.e. assignment of category membership should evidence inter-rater reliability); (3) mutual exclusivity (i.e. individuals should not meet the criteria for membership to more than one category); (4) comprehensiveness (i.e. all individuals should be successfully assigned to one category); (5) parsimony (i.e. few categories); (6) homogeneity of target population (i.e. individuals to be classified should represent a comparable set of behaviours); (6) empirical congruence (i.e. the typology should be supported by available data) and (7) clinical utility (i.e. treatment implications for subcategories). Consequently, the typology requires a robust and thorough qualitative and quantitative evaluation before recommending its use by practicing professionals working with individuals with ASD within secure psychiatric hospitals, or those at risk of admission to a secure psychiatric hospital.
To address some of the aforementioned issues, the current two-part study using qualitative methods aimed to: Study 1 – (a) evaluate the face validity of our typology (Alexander et al., 2016) with a sample of clinicians, carers and service users within a focus group and: Study 2 – (b) working with a sample of clinicians working with people with ASDs detained in secure psychiatric hospitals, the inter-rater reliability of the subtypes was examined by asking them to complete a consensus rating exercise of anonymised clinical vignettes of genuine cases of adults with ASD who are detained within a secure psychiatric hospital.
Study 1: evaluating the face validity of a typology of people with ASD detained within secure psychiatric hospitals
Method
Participants
Seven individuals (five males, two females) were approached and consented to take part in the focus group. Ages ranged from 22 to 62 (Mage = 45.14; SD = 13.98) years, and the majority was White UK/Irish (n = 5). All participants had experience of working with or caring for people with a diagnosis of ASD currently detained in secure forensic psychiatric hospitals, or they were service users. Participants were psychiatrists with experience of working with adults with ASD and/or intellectual disabilities within inpatient settings (n = 2), a clinical psychologist (n = 1) who had experience of working within inpatient settings with adults with ASD and/or intellectual disabilities, a healthcare worker (a person who provides care but does not necessarily appear on a register of professionals; n = 1) who was working within a secure forensic hospital with adults with ASD and/or intellectual disabilities, a family member of a person with ASD (n = 1) and two service users with a diagnosis of ASD (n = 2) who had been detained in secure forensic psychiatric hospitals. The two psychiatrists worked for the same private sector hospital, while the clinical psychologist worked within a different region in England and for a different National Health Service (NHS) Trust. An NHS Trust is an organisation that provide healthcare in the United Kingdom within a specific geographically region. The healthcare worker also worked within a different region and for a different NHS Trust.
Procedure
Informed consent was obtained for each participant, and demographic and background information was collected through questionnaire. A favourable ethical opinion was given by the Wales Research Ethics Committee 7 (Ref: 15/WA/0246). Participants were invited to take part in a 1-day focus group aiming to discuss and provide feedback on the proposed typology of people with ASD detained within hospitals. Participants were presented with a brief review of the study and the background literature by the first, second, and last authors, followed by a presentation about the subtypes and their descriptions. The first author facilitated a focus group discussion, using a semi-structured interview schedule, in which the participants were asked to consider each of the subtypes, discuss them until consensus was reached in terms of their validity and provide feedback as to whether any further characteristics should be considered (i.e. did they make sense, could they classify individuals into each subtype and were any additional factors or refinements needed). The focus group was recorded through digital audio recorder (Length = 2 h 19 min) and transcribed verbatim by a member of the research team.
Data analysis
Data were analysed using Deductive Thematic Analysis (TA; Braun & Clarke, 2006; Terry et al., 2017), and this is an appropriate and flexible method to analyse focus group data (Terry et al., 2017). The method seeks to identify, analyse and report themes within the data in the context of the research topic (Braun & Clarke, 2006). A key strength of TA is in its flexibility – it can be used within a wide range of theoretical frameworks and analytical approaches (e.g. inductive, deductive, semantic and latent; Terry et al., 2017). In particular, deductive TA seeks to examine the data from a theoretical perspective in which theoretical concepts inform the coding and theme development (Terry et al., 2017). In the current study, data analysis was informed by the typology evaluation criteria as specified by Helfgott (2008) to ascertain whether the typology holds true for a sample of professionals, carers and service users.
Theme development
First, data were broken down into conceptual components and these concepts arranged into categories (familiarisation and coding; Braun & Clarke, 2006). The relationships between the categories and typology evaluation criteria (Helfgott, 2008) were identified, and initial themes were generated (termed theme searching; Braun & Clarke, 2006). Second, the data were reviewed against the initial themes and typology evaluation criteria to ensure no new themes, properties, or relationships were required and saturation had been achieved (Terry et al., 2017).
Reliability and validity
Reliability checks were employed during the study to ensure strong levels of accuracy and reliability. First, inter-rater reliability checks were conducted during the first stage of coding. One independent rater familiar with TA was enlisted, IR1. To assess the reliability and validity of the open coding performed by the first author on the focus group transcript, IR1 was asked to independently perform open coding on 10 randomly selected pages from the focus group interview. An independent reliability check was subsequently performed by comparing the interview transcript coding of IR1 and the first author (e.g. for similarity/differences in coding); an inter-rater agreement of 81.90% was achieved. Second, reliability checks were conducted during the theme searching and reviewing stages of the analysis by the second author. The analytic process was reviewed and discussed until agreement was reached on the themes identified and the relationships between them (i.e. triangulation; Denzin, 1978), culminating in a qualitative evaluation of the typology.
Results
Analyses yielded six superordinate themes, which map onto the typology evaluation criteria and 10 subordinate themes within these.
Clarity and objectivity
Four subordinate themes were identified from the data pertaining to the clarity and objectivity of the typology: (1) the purpose of the typology, (2) its structure, (3) category assignment and (4) the accessibility of the typology.
Purpose
Participants generally agreed that the overall purpose of the typology was clear and sufficiently explicated. While one participant acknowledged a number of typologies could be potentially produced to classify people with ASD (e.g. sensory classifications), it was agreed among the group that the primary aim of the current typology was to differentiate subgroups of people with ASD in secure forensic mental health services according to severity of risk to themselves and/or to others (n = 3). The subtypes were viewed as unpicking the complexity of ASD in secure forensic mental health services (i.e. rather than other settings) by outlining differences within this group and thus allowing for a more sophisticated clinical understanding of the particular population and consequently differing treatment needs.
Structure
While participants agreed the typology was clearly presented pictorially, individuals expressed a preference to have the subtypes depicted as inter-related. The typology was likened to a cake with multiple layers, with one participant commenting ‘the more layers there are to cut through, the more complex the individual in terms of risk and treatment’ (n = 1). Furthermore, it was suggested that the priority of each of the factors needed to be highlighted within the diagram. For example, the following order of priority was suggested in terms of understanding risk and treatment: (1) psychosis, (2) psychopathy and (3) behavioural problems (n = 2) which was suggested by the focus group. When arriving at this order, they prioritised psychosis because they thought that successful treatment may lead to an improvement in both forensic risk and behavioural problems. Psychopathy and any associated forensic risk were ranked second, but seen as very important in terms of the safety and protection of others. Behavioural problems were ranked last, not because they were unimportant, but because they may reduce with treatment of psychosis and appropriate risk management.
Category assignment
The criteria for category assignment were considered generally clear by participants. The diagnostic labels for each category were deemed helpful in terms of describing the associated characteristics of individuals assigned to that category. It was felt the labels of each category favoured existing systems and processes in hospital (i.e. diagnosis and care pathway) which was in line with the overall purpose of the typology (n = 2). Furthermore, participants agreed category assignment aided individualised treatment formulation for clinicians and was helpful for service users in further understanding their own diagnoses (n = 4).
However, participants also provided a number of suggestions to improve the transparency of category assignment. Each of the category labels required individuals to have a good clinical understanding of the concepts of psychopathy, psychosis and behavioural problems. Consequently, it was advised that clinicians needed to have the same understanding of each of the categories to ensure category assignment was not open to interpretation (n = 1). By corollary, participants felt each of the factors needed to be accompanied by clear and precise definitions, particularly in terms of psychopathy and behavioural problems (n = 3). Some individuals felt treatment and care recommendations for each pathway would also increase the utility of the typology for professionals working with people with ASDs in secure services (n = 2).
Accessibility
The last subordinate theme relating to clarity and objectivity centred concerned the accessibility of the typology. Participants agreed the typology was developed for, and aimed at, clinically trained individuals with a specialist understanding of all the factors and their relationship to ASD. While the subtypes were considered accessible to clinicians, one participant felt using multiple diagnoses as a way of assigning category membership may be too complex for some individuals to understand (e.g. service users). The service user participants (n = 2) both agreed they struggled to understand the typology, with one commenting ‘I’m not up to this level, knowledge or understanding like you guys are’. However, it was suggested a narrative lay description to accompany the subtypes would improve the typology’s accessibility for service users and thus involvement in their own care plan.
Empirical congruence and reliability
In terms of empirical congruence and reliability, all participants agreed the typology required further quantitative evaluation. However, the data revealed participants considered the typology to possess clinical congruence, in that it was adequately supported in terms of their professional and clinical experience with people with ASD in secure forensic mental health services. Indeed, the majority of participants were able to think of multiple concrete cases within their services for each of the subtypes and were able to discuss these in detail according to all the factors (n = 4). However, the family carer and service user participants expressed difficulty in applying real-life individuals to some of the subcategories of the typology (e.g. psychopathy and behavioural problems), though all explained this was largely due to difficulties in understanding the traits associated with the subcategories themselves (i.e. accessibility; n = 3).
Comprehensiveness and parsimony
Two subordinate themes relating to the comprehensiveness and parsimony of the typology emerged from the data: (1) explanatory depth and (2) alternative factors.
Explanatory depth
The typology overall was felt to have good explanatory depth, with participants commenting the subcategories were relevant and comprehensive (n = 4), allowing classification of individuals without any unexplained subtypes. Participants were unable to think of examples of individuals with ASD in secure forensic mental health services who did not fit into at least one of the subtypes, with one participant commenting ‘I can’t think of anyone like that’ (i.e. completely different). Consequently, the eight subtypes were deemed comprehensive enough to encompass the range of individuals with ASD in secure forensic mental health services, without being overly complicated.
Alternative factors
A number of alternative factors were discussed for the typology: (1) mental health problems (n = 4), (2) alcohol and substance misuse (n = 1), (3) intellectual disabilities (n = 2), (4) personality disorder (n = 3) and (5) offence history and risk (n = 4). However, consensus was reached after discussion. Participants came to the conclusion that many of the aforementioned constructs would be captured by the existing categories within the typology. For example, participants considered whether the category of psychosis should be broadened to include other mental health problems, but thought that many mental health problems may not relate to forensic risk. Participants discussed some affective disorders, and there considered that when severe, patients may present with features of psychosis. Participants agreed individuals with intellectual disabilities in secure forensic mental health services were likely to be in the mild to borderline range (i.e. IQ > 50) and have associated behavioural problems (n = 2). Similarly, it was felt offence history, risk levels and the problematic traits of most personality disorders were covered in the assessments for psychopathic traits (e.g. impulsivity, aggression, low empathy and substance misuse), with one participant commenting ‘I think a lot of the features of other personality disorders will be covered in the PCL-R [The Hare Psychopathy Checklist-Revised] items, the twenty items, I think impulsivity is there, irresponsibility is there, poor behaviour control is there’. However, another participant noted psychopathy was poorly recognised and rarely referred to when working with people with ASD, though acknowledged the traits associated with psychopathy were more comprehensive.
Mutual exclusivity
Participants felt subtype assignment was mutually exclusive; individuals with ASD in secure forensic mental health services would not meet the criteria for membership of more than one subtype based on their accumulated professional and clinical experience. However, two participants felt the typology could be conceptualised as moving from static factors (i.e. ASD and psychopathy) through to more dynamic factors (i.e. psychosis and behavioural problems). As a result, it was felt that service users could fluctuate between subtypes throughout their length of stay in hospital. For example, where a service user was admitted with a drug-induced psychosis, they would be assigned to the Psychosis category of a particular subtype. However, once the psychosis was treated (e.g. through medication or by the cessation of use of illicit substances), that service user would move to the relevant No Psychosis category within the subtype. Similarly, it was thought that service users could potentially fluctuate between the higher and lower behavioural categories during their length of stay, with one participant commenting he had a ‘patient from [Forensic Secure Unit] I think, antisocial personality also psychopathy he will score at least moderately high in psychopathy I would guess, no psychosis. He goes through phases of low and high behavioural’.
Homogeneity of target population
In terms of homogeneity of the target population, all the focus group participants agreed the typology clearly targeted individuals with an ASD detained in secure forensic mental health services (i.e. not any other settings). For example, one participant commented ‘we could use lots of different things to split people up. . .whether they are colour blind or not. . .but won’t affect whether you’re dangerous or not, won’t affect how long you need to be in hospital’. Furthermore, while the typology was clear in the target population, some participants acknowledged it was also important the subtypes allowed for the heterogeneity of ASDs (n = 4). In particular, it was deemed important to have a specialist understanding of the role of ASD in the classification and how it may affect other diagnoses (e.g. individual strengths and difficulties, provision of person-centred care).
Clinical utility
Our analysis of the focus group data suggested the typology to be clinically useful in terms of assessment, treatment and care pathways for people with ASD in secure forensic mental health services. Four subordinate themes were identified within the data: (1) diagnostic application, (2) risk, (3) setting and length of stay and (4) treatment approaches.
Diagnostic application
A number of participants (n = 3) felt the typology usefully translated common patterns of behaviour associated with people with an ASD in secure services into manageable diagnostic categories (i.e. psychopathy, psychosis and behavioural problems). For example, one participant described the typology as mapping onto Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) diagnostic criteria, by moving the now discarded Axis I diagnoses (e.g. psychopathy) to Axis II diagnoses (i.e. psychosis and behavioural problems). The use of diagnostic categories in the subtyping of people with ASD was also deemed helpful for staff in secure forensic mental health services, enabling a better understanding of service user behaviour and thus improved care provision. For example, one healthcare worker from a medium secure unit commented, ‘I think anything that’s going to help staff who are delivering the care to perhaps understand a bit better what behaviours might be presented I think that can only be good’.
Risk
Participants agreed that the typology was clinically useful in differentiating between low- and high-risk individuals in secure forensic mental health services. While ASD was not considered a risk factor in itself, participants expressed the level of risk associated with an individual with an ASD in secure forensic mental health services was proportional to the number of factors present (e.g. psychopathy, psychosis and behavioural problems). Furthermore, a number of participants agreed the subtypes enabled the targeting and prioritisation of risk factors to address in treatment (n = 3). First, higher psychopathy was believed to override all other factors when present and considered the most important factor in terms of risk of violence. Second, psychosis was deemed to be associated with higher risk levels. However, some participants felt there were differing levels of risk according to the type of psychosis (n = 2). For instance, one participant commented a drug-induced psychosis may be treated relatively quickly and thus could be considered lower risk, compared to an individual with enduring psychosis. Third, lower behavioural problems were considered to be higher risk than higher behavioural problems as the behaviours were likely to be more severe in terms of violence and harder to predict. Where psychopathy and psychosis were also present, participants felt behavioural problems were likely to be a by-product of these (n = 2). Conversely, in the absence of these factors, behavioural problems were thought to be associated with the characteristics of ASDs in terms of risk (e.g. poor insight and lack of understanding) and thus naturally lower in risk. Interestingly, two participants believed behaviour within a secure environment was not the best predictor of future violence due to the restricted opportunities available to service users to engage in risky behaviours (e.g. firesetting behaviour).
Setting and length of stay
Participants felt the typology was useful in determining the appropriate setting and recommended length of stay for each subtype. The group largely agreed detention in secure services was appropriate for a number of the subtypes (i.e. those with higher psychopathy and/or psychosis) in terms of risk and rehabilitation and was often associated with longer lengths of stay due to the complexity of treatment required. Conversely, participants agreed other subtypes (i.e. those with only behavioural problems) would benefit from community placements with robust care packages in place and consequently time spent in secure forensic mental health services should be relatively short (n = 5). In particular, for service users with only lower behavioural problems (i.e. lower psychopathy and no psychosis), it was felt assessment in a secure environment may be appropriate for a short period to manage behavioural problems and determine an appropriate care pathway in the community (n = 3). For those service users with only higher behavioural problems (i.e. lower psychopathy and no psychosis), detention in hospital was viewed as inappropriate but occurred due to poor community services. If community assessment and treatment teams were adequately funded and provisioned, then individuals in this subtype could be more appropriately managed without the need for detention in hospital (n = 4). However, it was also noted that ASD and behavioural problems were frequently associated with longer lengths of stay in hospital and poorer outcomes as service users were often hindered by poorly implemented NICE guidelines and tight government regulations surrounding discharge. For example, one participant commented, some of them on restricted orders from the Ministry of Justice and err, you have to have a reasonable length of time with no behaviours before you apply for step down and all that and sometimes that is a real difficult to achieve because something will happen again, you know in the time.
Treatment approaches
The final subordinate theme for clinical utility pertained to treatment approaches. Participants agreed that the typology was useful in terms of determining and improving different treatment approaches for the different subtypes, in terms of complexity and length, and consequently improving treatment outcomes for service users. Clinicians (n = 3) felt subtypes with higher psychopathy and psychosis were likely to require intense and long-term treatment, whereas those with only behavioural problems were likely to require careful assessment (i.e. severity and nature of the behaviour), but comparatively less complex and shorter treatment which could be delivered in a community setting.
Three participants agreed each of the categories within the subtypes were informative in terms of treatment approaches. While often hard to diagnose in people with ASD, psychosis was seen as taking priority in treatment by two participants, with one participant commenting ‘that’s something that can be straightened out quite quickly and you can get into the work around the offence or the risk or whatever and you don’t have anything else to complicate things’. Furthermore, those with higher psychopathic traits were largely considered hard to engage in treatment due to certain traits (e.g. lack of insight, disruptive) and consequently treatment was likely to last much longer. Finally, participants generally agreed behavioural problems could be managed within a positive behavioural support framework, especially for those presenting with higher behavioural problems.
Study 2: evaluating the inter-rater reliability of a typology of people with ASD detained within hospitals
Method
Participants
In total, 15 individuals (10 males, 5 females) consented to take part in the consensus rating exercise, and five of these participants were allocated to each of the three rounds of the consensus rating exercise (i.e. first, second and third round) such that each set of participants were different across the rounds. Ages ranged from 30 to 66 (Mage = 50.73; SD = 10.48) years and were Caucasian (n = 9), Indian (n = 4) or Asian (n = 2). All participants had to have experience of working with people with a diagnosis of ASD currently detained in UK secure forensic mental health services and worked for different NHS Trusts or private sector healthcare providers. Participants were psychiatrists (n = 9) and practicing clinical or forensic psychologists (n = 6) currently working within forensic inpatient services.
Materials and procedure
Participants were invited to take part in a consensus rating exercise using methods similar to those of Cooray et al. (2000). Informed consent was obtained for each participant, and demographic and background information was collected through questionnaire.
Three rounds of consensus rating exercises were undertaken; the rounds were discontinued when no further feedback was given by raters The first consensus rating exercise aimed to develop a series of clinical case vignettes, test the clarity of the clinical case vignettes, consider whether the vignette as described fit with the typology and provide initial reliability ratings between raters. Our initial five participants were asked to prepare 10 anonymous clinical vignettes (i.e. two each) based on the service users with ASD detained in hospital. The 10 clinical vignettes were then collated together in a rating pack. Each rating pack consisted of (1) some background literature on the typology (i.e. Alexander et al., 2016), (2) 10 anonymised clinical vignettes of people with ASD detained in hospital, (3) a tree diagram of the typology for each vignette and (4) a blank space for open-ended feedback for each rating. Participants were asked to independently assign each vignette according to the typology by completing the tree diagram. Participants were also asked to provide some open-ended feedback in terms of the clarity of each vignette and their ability to classify them according to the typology, including if they felt the vignette did not fit into the typology at all.
The second consensus rating exercise focused on refining the clarity of the clinical case vignettes based on the findings from the first exercise and re-testing the reliability of the ratings with new raters. All the clinical vignettes were refined based on the reliability ratings and feedback from the first round of ratings. Five participants were asked to complete the revised vignette rating pack independently, collated in the same format as for the first round of consensus ratings.
The third consensus rating exercise focused on further refining the clarity of the clinical case vignettes based on the findings from the second exercise and re-testing the reliability of the ratings with new raters. All the clinical vignettes were refined based on the reliability ratings and feedback from the second round of ratings. A further five participants were asked to complete the revised vignette rating pack independently, collated in the same format as for the first two rounds of consensus ratings.
Data analysis
Participant background and demographic data were analysed using IMB Statistics (version 24).
Inter-rater reliability statistics were calculated using Fleiss’ Kappa (κ; Fleiss et al., 1981) and average pairwise agreement percentages. Fleiss’ Kappa is frequently used for calculating reliability coefficients for nominal data coded by three or more raters (McHugh, 2012). For each consensus rating exercise, reliability statistics were calculated for overall classification of all 10 clinical case vignettes, and for subcategory classification. Kappa ratings were interpreted according to Landis and Koch’s (1977) guidelines: poor agreement (κ < 0), slight agreement (κ = 0.01–0.20), fair agreement (κ = 0.21–0.40), moderate agreement (κ = 0.41–0.60), substantial agreement (κ = 0.61–0.80) and almost perfect agreement (κ = 0.81–1.00).
Results
Consensus rating exercise 1
Inter-rater reliability coefficients
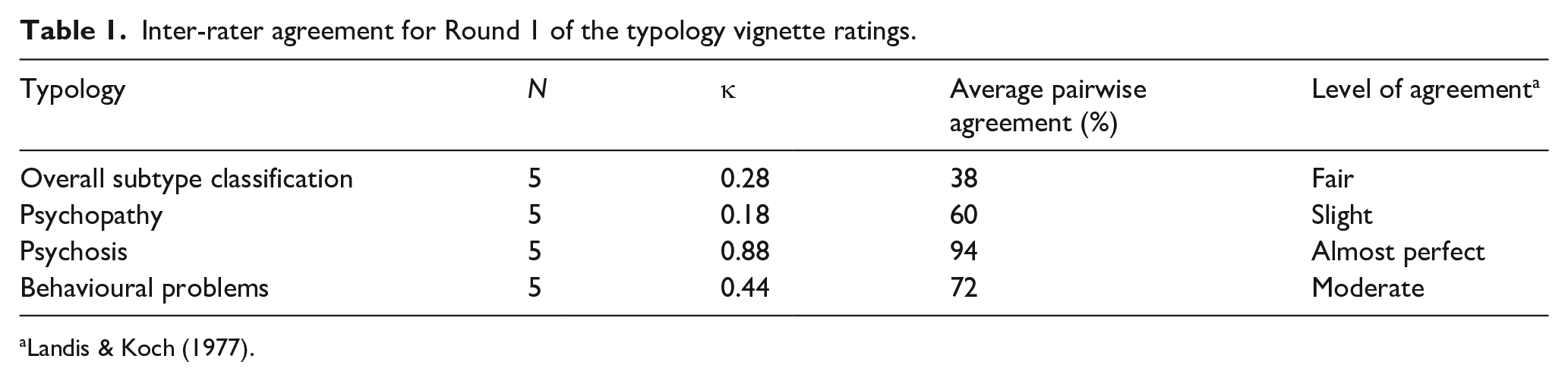
All five raters were able to classify all 10 clinical case vignettes into the typology. Raters’ percentage of agreement ranged from 38% to 94% for overall subtype classification and individual factor classification. Table 1 outlines the inter-rater reliability statistics yielded using Fleiss’ Kappa and average pairwise agreement percentages.
Inter-rater agreement for Round 1 of the typology vignette ratings.
Rater feedback
All five raters provided open-ended feedback regarding their experiences of classifying the clinical case vignettes according to the typology. Raters agreed the typology worked from a clinical perspective for service users with ASD detained in secure forensic mental health services. All 10 vignettes were classified into the typology and none met the criteria for membership to more than one subtype across or within raters. However, raters found psychopathy and behavioural problems as the hardest categories to assign. For both subcategories, raters advised more information was needed within the clinical case vignettes to make a clinically informed decision.
Consensus rating exercise 2
Inter-rater reliability coefficients
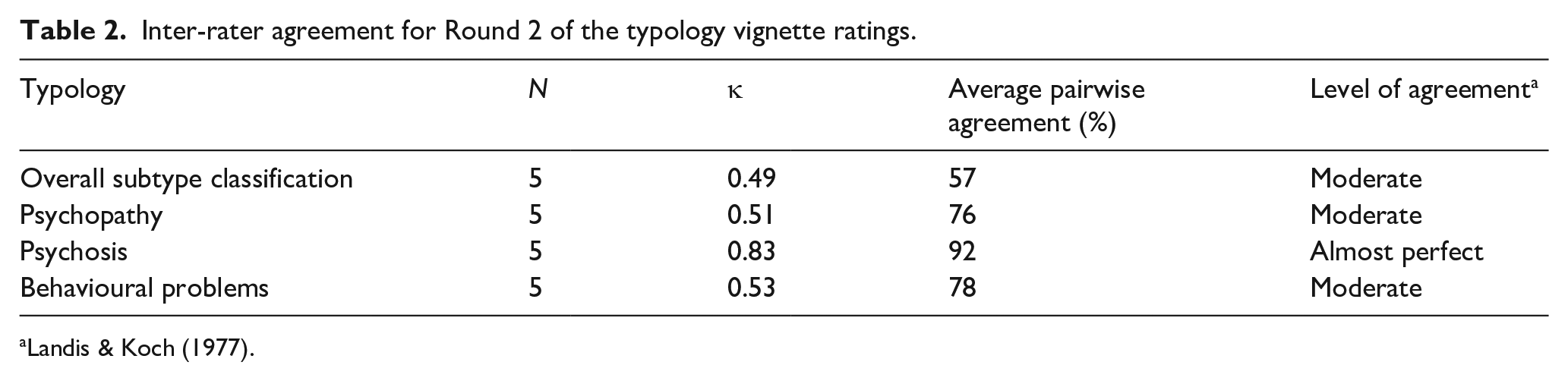
Four raters were able to classify all 10 clinical case vignettes into the typology. One rater was unable to classify the psychopathy subcategory of one case vignette. Raters’ percentage of agreement ranged from 57% to 92% for overall subtype classification and individual factor classification. Table 2 outlines the inter-rater reliability statistics yielded using Fleiss’ Kappa and average pairwise agreement percentages.
Inter-rater agreement for Round 2 of the typology vignette ratings.
Rater feedback
Four raters provided open-ended feedback regarding their experiences of classifying the clinical case vignettes according to the typology. Raters felt the typology worked well, and classification into the subtypes was clear. In addition, the vignettes were found to reflect the dynamic nature of the subtypes in relation to psychosis and behavioural problems. However, participants generally felt some of the cases were harder to classify compared to others due to the level of information provided, particularly in terms of psychopathy (n = 3) and psychosis (n = 1), where more historical information would have been helpful.
Consensus rating exercise 3
Inter-rater reliability coefficients
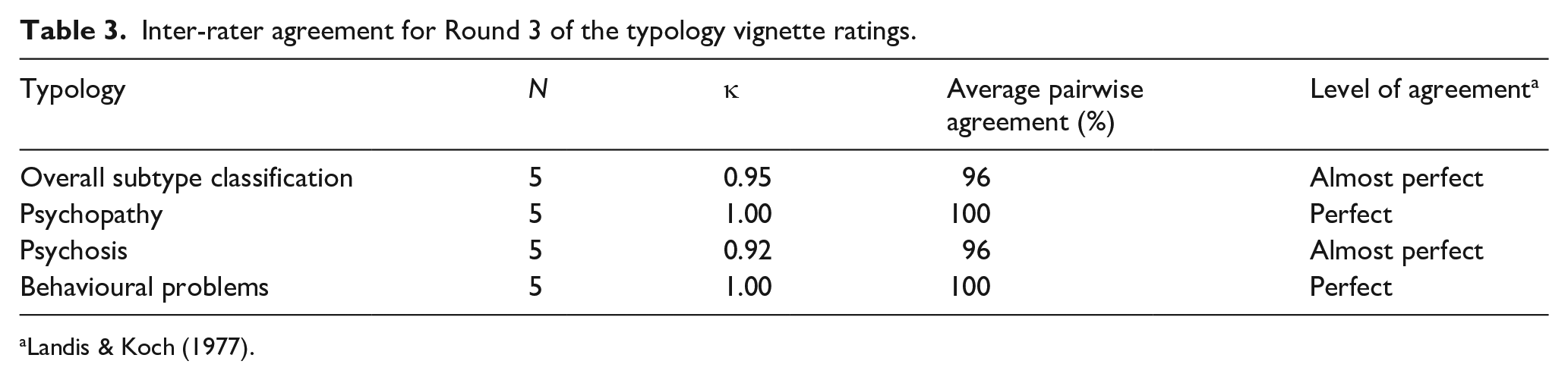
All five raters were able to classify all 10 clinical case vignettes into the typology. Raters’ percentage of agreement ranged from 96% to 100% for overall subtype classification and individual factor classification. Table 3 outlines the inter-rater reliability statistics yielded using Fleiss’ Kappa and average pairwise agreement percentages.
Inter-rater agreement for Round 3 of the typology vignette ratings.
Rater feedback
None of the raters provided open-ended feedback regarding their experiences of classifying the clinical case vignettes according to the typology. All 10 vignettes were accurately classified into the typology and none met the criteria for membership to more than one subtype.
Discussion
In this two-part study, a qualitative evaluation of Alexander et al.’s (2016) typology of people with ASD detained in secure forensic mental health services was undertaken using a focus group discussion and a consensus rating exercise. Using established typology evaluation criteria (Helfgott, 2008), findings indicated that the typology possessed face validity and good inter-rater reliability. First, findings from Part I of the study indicated the subtypes met the majority of Helfgott’s (2008) evaluation criteria. The subtypes were found to be clear and objective in terms of purpose, structure and category assignment; clinically congruent; comprehensive in terms of explanatory depth, with no need for alternative or additional factors; mutually exclusive but dynamic in nature; homogeneous in terms of targeting individuals with ASD detained in secure forensic mental health services and clinically useful in terms of diagnostic application, risk assessment and treatment approaches. The findings from this study did not enable us to make a definitive judgement on parsimony and empirical congruence. Recommendations and further considerations for the refinement of the typology were also highlighted. The inter-relatedness of the subcategories needed to be appropriately reflected in the pictorial presentation of the typology, in particular, in terms of highlighting an order of priority for the factors in terms of risk (i.e. higher psychopathy, psychosis and lower behavioural problems) and treatment (i.e. psychosis, psychopathy and last behavioural problems) which would need to be considered in a future study. As a corollary, subcategories needed precise definitions and information about the suggested setting, length of stay and treatment recommendations. While the typology is intended for use by individuals with high levels of expertise in ASD and co-morbid psychopathology, refining its accessibility to service users was deemed important, particularly for involvement in their own care plans.
Second, in Part II of the study, three consensus rating exercises yielded percentage agreements ranging from 38% to 100% for overall subtype classification and individual factor classification; bearing in mind that there was a substantial improvement in agreement following feedback collected during the first two rounds. This led to revision of the clinical vignettes to ensure they contained appropriate information specifically about IA and behavioural problems. Inter-rater reliability statistics using Fleiss’ Kappa yielded slight to perfect agreement for overall subtype classification and individual category assignment across all three consensus rating exercises. However, within the initial consensus rating exercises, some raters provided feedback that they had difficulties rating psychopathy and behavioural problems. As for behavioural problems, this was associated with how the raters understood the dimension; higher behavioural problems are those which occur at a high frequency and can have a lower intensity (e.g. shouting, screaming and banging furniture), while fewer behavioural problems occur with a lower frequency but are of a higher intensity (e.g. attempted murder), and raters needed greater clarification. Rating psychopathy also proved difficult and appeared to reflect the diagnostic overlap between some of the features of ASD and the characteristics of psychopathy. Again, greater clarification was needed focusing on the IA features of psychopathy.
In the following discussion, theoretical considerations, clinical implications and limitations of the findings are considered. First, the current findings highlight Alexander et al.’s (2016) typology as the first validated classification system seeking to describe the differing risk profiles and clinical presentations of people with ASD detained in secure forensic mental health services. The qualitative and quantitative differences between the subtypes may serve to inform aetiological differences between offenders with ASD and act as the foundation for the development of more complex theories in the field. Typological classifications in the broader offending literature have served to inform more complex theoretical models (e.g. sexual offending; Ward & Siegert, 2002) and their utility has been widely accepted in line with the scientist–practitioner model (Jones & Mehr, 2007). However, very few have been investigated with offenders who broadly have developmental disabilities (e.g. sexual offending pathways model; Langdon et al., 2007) and there have been no efforts to develop a theoretical model specifically for offenders with ASD. Consequently, Alexander et al.’s (2016) typology makes the first important step towards informing future theoretical developments in the relatively underdeveloped field of ASD and offending behaviour. In particular, future theory development will allow practicing professionals to understand the complexity of psychological factors in ASD and offending behaviour, thus contributing to effective assessment and management of this complex group of individuals.
Second, findings from the focus group data and rater feedback from the consensus rating exercise highlight the clinical implications of Alexander et al.’s (2016) typology. Indeed, the classification further evidences the complexity of the relationship between ASD and forensic risk. Risk assessment and treatment approaches for this group of individuals were suggested to be related to co-morbid psychopathology, rather than traits associated with ASD, a finding echoed in existing research (Mouridsen, 2012). Indeed, it has previously been demonstrated that individuals with ASD are no more likely (Hippler et al., 2010) or in fact less likely to commit criminal offences compared to those without ASD (Im, 2016), suggesting that the traits associated with ASD are not necessarily pre-disposing factors for offending behaviour (Pearce & Berney, 2016). Rather, the findings from this study highlight there are potentially alternative factors likely to contribute towards violence and risk of offending in this population (e.g. co-morbid forensic mental health problems and psychopathic traits). For instance, for those without ASD, psychopathic traits are a known risk factor for offending behaviour (Hare, 2003; Peters et al., 2016; Porter & Porter, 2007) and there is a small but significant evidence base to suggest these co-occur in individuals with ASD (Kincaid et al., 2017; Woodbury-Smith et al., 2005), yet with differing neurocognitive underpinnings. There is tentative evidence to suggest empathy deficits differ in individuals with ASD compared to those with psychopathy (Rogers et al., 2006). Those with ASD may experience difficulties with theory of mind and consequently the ability to correctly read and appropriately react to someone’s emotions, whereas psychopathic individuals appear to lack the ability to resonate with other people’s emotions (Lockwood et al., 2013). Within the context of Alexander et al.’s (2016) typology, individuals with ASD presenting with psychopathic traits are likely to display difficulties in both domains. However, the inability to resonate with affect may be considered more clinically meaningful in terms of forensic risk and management and may not be consistently captured as institutionalisation or disability may reduce the opportunity to display the associated behaviours. Thus, by providing a classification system based on co-morbid psychopathology, Alexander et al. (2016) unpick the complexity of the overlapping traits between ASD, psychopathy, psychosis and behavioural problems and thus facilitate the tailoring of risk management, treatment approaches and care pathways.
Finally, the strengths and limitations of the current study merit consideration. First, the generalisability of the findings is limited due to the subjective nature of qualitative research and small sample size. However, the use of an independent rater and triangulation during the TA represents a notable strength in terms of the reliability of the findings. Furthermore, sample sizes in qualitative research tend to be small and 9–15 participants are considered to be in fact a relatively large sample (Terry et al., 2017). Second, the mixed reliability ratings in the second part of this study are likely to be associated with the known limitations around the use of clinical case vignettes. Information provided in clinical case vignettes tends to be inherently partial and static and thus not comparable to the in-depth knowledge a clinician may have regarding their own service users (i.e. psychosocial history, risk profile or clinical presentation). Consequently, participants are likely to rely on their own experience to supplement the information provided and thus inform their ratings (i.e. potentially increasing error rates). However, a notable strength of the current study was to test the clarity of clinical case vignettes themselves in the first consensus rating exercise and subsequently refine them for the second and third rating exercises to ensure as far as possible the reliability of the ratings, which led to perfect agreement between raters in the final round. Furthermore, consensus rating exercises are a widely accepted methodology (Wainwright et al., 2010) and carefully constructed vignettes can be as effective as any other case presentation within the confinements of the approach (Wainwright et al., 2010).
While the current research suggested the typology possessed face validity and good inter-rater reliability, a robust quantitative evaluation is required before recommending its use by practicing professionals, demonstrating validity with a clinical sample. This work is currently being completed as part of a large-scale cohort study funded by the National Institute for Health Research to further evaluate the typology, in which patient data, clinical variables, hospital data and service user outcomes will be compared according to the subtypes. It is anticipated that the findings from this significant quantitative evaluation will complement the current findings and ultimately contribute to the development of evidence-based clinical pathways in NICE guidelines for service users with ASD detained in secure forensic mental health services.
Footnotes
Acknowledgements
The authors thank all the participating sites, staff and participants for their valuable contribution to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research led by Prof. Peter Langdon funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference No. PB-PG-0214-33040). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Participating sites
Hertfordshire Partnership University NHS Foundation Trust, Leicestershire Partnership NHS Trust, Kent and Medway Partnership NHS Trust, 2gether NHS Trust, Avon and Wiltshire NHS Trust, Betsi Cadwaladr University Health Board, Birmingham and Solihull NHS Trust, Black Country NHS Foundation Trust, Cambridgeshire and Peterborough NHS Foundation Trust, The Huntercombe Group, Central and Northwest London NHS Trust, Coventry and Warwickshire Partnership NHS Trust, Cumbria Partnership NHS Trust, Derbyshire Foundation NHS Trust, Devon Partnership NHS Trust, East London NHS Foundation Trust, Leeds and York Partnership NHS Foundation Trust, Lincolnshire Partnership NHS Trust, Merseycare NHS Trust, Norfolk and Suffolk NHS Foundation Trust, Northumberland, Tyne and Wear NHS Trust, Nottinghamshire Partnership NHS Trust, The Priory Group, Somerset Partnership NHS Trust, St Andrews Healthcare, Sussex Partnership NHS Trust, Tees, Esk and Wear Valley NHS Trust and Worcestershire Health and Care NHS Trust.