
Abstract
Autistic adults are significantly more likely to experience co-occurring mental health conditions such as depression and anxiety. Although intervention studies are beginning to be implemented with autistic adults to address mental health outcomes, little is known about what research autistic adults feel is needed, or what mental health outcomes are of value to them. The purpose of this article is to describe a project that involved more than 350 autistic adults and other stakeholders as coproducers of research priorities on mental health. Through a variety of methods including a large online survey, two large stakeholder meetings, and three face-to-face focus groups, the project team identified five top priorities for mental health research which should be incorporated by researchers and practitioners in their work with autistic adults. These included research to inform trauma-informed care approaches; societal approaches for inclusion and acceptance of autistic individuals; community-available approaches for self-management of mental health; evaluation of adverse mental health outcomes of existing interventions; and improvements in measurement of quality of life, social well-being, and other preferred outcomes in autistic adults.
Lay Abstract
Autistic adults commonly experience mental health conditions. However, research rarely involves autistic adults in deciding priorities for research on mental healthcare approaches that might work for them. The purpose of this article is to describe a stakeholder-driven project that involved autistic adults in co-leading and designing research about priorities to address mental health needs. Through a large online survey, two large meetings, and three face-to-face focus group discussions involving over 350 stakeholders, we identified five priorities for mental health research desired by autistic adults. These priorities and preferred outcomes should be used to guide research and practice for autistic adults.
Keywords
Introduction
Research suggests that autistic individuals 1 experience greater rates of anxiety than same-aged peers without autism (e.g. Croen et al., 2015; Joshi et al., 2013; Roux et al., 2017; Russell et al., 2016). In addition, autistic individuals experience high rates of depression and other co-occurring mental health conditions (e.g. Hollocks et al., 2019). These and other risk factors may also contribute to greater risk for suicidality (e.g. Cassidy et al., 2018); yet access to mental healthcare and appropriate supports are lacking for many autistic adults (e.g. Crane et al., 2019). Due to the increased risk for experiencing poor mental health outcomes such as those described above, there is a great need to identify the preferred interventions and approaches to improve mental health outcomes in collaboration with autistic adults.
The autistic adult community is generally not involved in co-producing research that informs subsequent practices or research priorities impacting their care. However, efforts to include autistic adult input have been made in some priority-setting research. For example, in the United States, Gotham and colleagues (2015) identified priorities from an online stakeholder survey registry of nearly 400 autistic and caregiver stakeholders, and recommended further work to include autistic perspectives in research activities. Indeed, co-produced research is much more likely to provide opportunities for identifying meaningful outcomes and approaches that are desired by the community (e.g. Jivraj et al., 2014) and successful research partnerships have significantly contributed to producing best practices when involving community participatory approaches (Nicolaidis et al., 2019). Fostering trust and mutual respect in the process of developing research results in higher quality products that are useful to the community, as exemplified by research priorities developed in collaboration with the autism community in the United Kingdom (e.g. Pellicano et al., 2014; Warner et al., 2019).
There has been limited published research aiming to identify health research priorities of autistic individuals through co-led approaches in the United States. This project aimed to involve the autistic community in defining and prioritizing specific desired outcomes for health research. The purpose of this article is to describe the multiple methods used to identify and ascertain autistic adult perspectives related to mental health practice and the specific mental health research priorities that emerged through this stakeholder-driven project.
Methods
Ethics and community stakeholders as co-developers of research
This 2-year stakeholder-driven project involved a Project Team composed of both autistic and non-autistic members, each of whom had complementary roles in the leadership of the project, and an 18-member Community Council comprised primarily autistic adults and several parents of autistic adults. Both the Project Team and the Community Council co-developed and led three project activities: (a) two large stakeholder meetings in Year 1 and Year 2 of the project; (b) an online survey; and (c) three face-to-face focus groups with autistic adults. Our methods proceeded from the assumption that each of these three iterative activities with the autistic adult community would yield additional relevant information to understand research priorities.
Shared responsibility between the Project Team and the Community Council resulted in co-development of all methods and materials. The Community Council provided input to project activities through regular online Zoom® meetings and email requests for decisions and feedback. These methods were chosen for communication because the collaborators were from across the United States, Australia, and the Russian Federation. Community Council members were compensated for their time.
Each project activity was reviewed as a standalone project by the university Institutional Review Board (IRB); only some project activities were approved as human subjects research.
Year 1 stakeholder meeting
Purpose
The purpose of this stakeholder meeting was to provide an opportunity for autistic adults and researchers to identify broad knowledge gaps about health and healthcare needs, to develop preliminary research priority areas, and to discuss strategies promoting engagement of autistics in co-developed research.
Advertising methods and attendees
The meeting was advertised through listservs of large autism advocacy groups and through email, Facebook®, and in collaboration with Community Council members. Anyone was able to register and attend. Fifty-one attendees participated in the Year 1 meeting, which comprised in-person attendees (n = 39) and virtual attendees (n = 12). Priority-setting activities occurred only with in-person attendees, of whom 17 were autistic adults, 8 were family members of autistic adults, 12 were researchers or organizational partners, and 4 had unknown stakeholder roles. Several individuals had multiple stakeholder identities as reflected in the totals.
Setting
The meeting was held the day prior to a large annual autism conference in order to promote attendance of autistic individuals. We offered an opportunity to participate online through Zoom for those that could not attend in person. Attendance was free, and we provided in-person attendees stipends to offset the costs of travel and attendance.
Activities
The primary method of discussing broad health research priorities was through breakout sessions. We used large infographic posters displaying known health outcomes experienced by autistic adults placed throughout a large room, and encouraged attendees to examine the infographics. We used sticky notes as an approach to allow attendees to communicate preferred areas for future research while reducing the demand for interaction. We gave each attendee five sequentially numbered notes each. The attendee then prioritized their interest with “1” representing the more important topic for them. If there was an important topic that was not present in the infographics, we invited attendees to write it on a large pad of paper visible to all attendees. Participation did not require interaction or explanation. Following this activity, we invited attendees to discuss the priority areas. Autistic partners led these discussions with a script to promote consistency across breakout groups. Questions did not focus on any personal health questions or topics. Three topics emerged as areas for future priority-setting activities: addressing mental health needs, access to healthcare, and defining outcomes such as well-being and quality of life (QoL) for all autistics.
Online survey
Purpose
Between August 2017 and March 2018, the Project Team and Community Council developed a survey with consultation by a statistical epidemiologist to capture (a) research priorities, including preferred interventions and outcomes for physical and mental health, (b) self-reported personal health, satisfaction with providers, and access to healthcare, and (c) demographics.
Survey design and pilot testing
We selected a web-based survey as the most efficient method to reach as many people as possible. The design of the survey incorporated both closed and open-ended questions. Close-ended questions with response scales incorporated visual graphics instead of word anchors. Visual graphics have been found to reduce ambiguity when eliciting preferences and satisfaction from autistic adults (Nicolaidis et al., 2019). We selected face icons for perception of health and satisfaction questions and traditional “letter grades” used in the US educational system for rating health provider skills (e.g. grade of A as an excellent rating, to a grade of F, representing a poor rating). For questions eliciting priorities, we used a click-and-drag response option to allow respondents to categorize interventions and outcomes. Participants sorted each listed mental health intervention into categories of “I would participate in this intervention,” “I would not participate in this intervention,” or “I need more information to decide.” They sorted each listed mental health outcome into “Outcomes that matter to me,” “Outcomes that don’t matter to me,” or “I need more information to decide.” They then ranked the items in each category based on the most important item being put at the top (rank of 1), using a click-and-drag method. The higher the item on the list, the more important it was ranked.
We pilot tested the online survey of 59 items in Qualtrics with the Community Council members providing feedback regarding question flow and logic structure. Recommendations to revise questions, shorten the length of the survey, and to clarify logic and branching in several questions resulted in 30 survey items with 15 demographic questions (see Supplemental Appendix A for relevant survey questions). Although the survey length was seen as a concern, the retention of open-ended questions was desired by the Community Council to allow respondents an opportunity to provide other responses if the closed-ended questions were not comprehensive enough.
Participants
Individuals were eligible to participate in the online survey if they were adults aged 18 years and older and if they reported a formal autism diagnosis or a self-diagnosis. We excluded caregivers of adults because the intended sample was autistic individuals who were able to self-report their preferences. Both purposive and convenience approaches were used for recruitment between August and December 2018. Purposive sampling was accomplished with Community Council and Project Team members sharing the survey link via online and social media posts with known autism groups and individuals. We used convenience sampling by posting the survey link on Facebook. No compensation was offered for participation.
We asked participants to confirm diagnosis prior to beginning the survey by checking a box corresponding to how and when they were officially diagnosed (educational classification, medical diagnosis, or self-identified; diagnosed during childhood, adulthood). A total of 236 participants agreed to participate. Among those who started the survey, 130 respondents (55%) completed the survey entirely, which primarily impacted demographic questions asked at the end. The median response time was 18 min. In this article, only analyses related to mental health priorities and demographics are presented, and all available responses were included.
Data analysis
We used frequencies and percentages of responses to describe demographics. Ratings of preferred interventions and outcomes were analyzed based on relative rank. Ranked items were weighted to allow for relative comparison with other ranked items. Weighting for ranks were calculated as the sum of the number of participant responses ranking that item as “1,” “2,” . . . “18” multiplied by the weight. A rank of “1” was given a weight of 18, and a rank of “18” was given a weight of “1.”
We coded open-ended responses using Microsoft Excel© and MaxQDA version 12 for the following questions: “If there is another intervention that research should evaluate to address mental health in autism, what would that be?”; “Is there another outcome that you think researchers should measure to assist in their understanding of mental health in autism?”; and “Imagine a breaking news headline about Autism Research. . . . What headline would you most want to see?” We coded using in-vivo codes for individual responses and then collapsing these codes into categories of responses reflecting similar content. We report the most frequently occurring categories.
Focus groups
Purpose
To enhance the validity of the priority-setting activities with autistic adults by increasing the representativeness of our sample, we also hosted three face-to-face focus groups between August and November 2018. Written informed consent was obtained for participants of face-to-face focus groups prior to participation; if the participant had a legally authorized guardian, their consent was also obtained.
Question development and protocol
Focus group questions first concentrated on an individual’s perception of “health,” and then led into priority-setting activities (see Supplemental Appendix B for focus group questions and activities). We designed all focus group activities so that non-speaking individuals and/or those with varying degrees of verbal speech could participate fully, which we defined as the participant having the opportunity to contribute their perspective in the manner and time span in which they communicate best. This involved ensuring that both focus group leaders were familiar with working with non-speaking autistic individuals, keeping the groups small, providing questions in advance of the group for more processing time, and developing activities that did not require spoken language to provide a response. Participants were also encouraged to take breaks when needed, and if desired, to contact the group leader after the focus group if they had additional thoughts after the end to share.
The focus group was conducted with a discussion about health, followed by two activities allowing priority-setting to occur. For the initial discussion about health, one leader verbally asked the question and displayed the same question on a white board. The leader asked participants to write their response on an index card, and gave participants approximately 3–5 min to write a response; the leader invited participants to share what was written. Participants were not required to provide a response. Participants could share their response by either reading out loud, or by handing the cards to the leaders, who read responses in random order once collected, so that responses were not attributed to any particular individual. We did have plans in place to accommodate individuals using augmentative-and-alternative communication to type their response, but no individuals used this method to communicate.
Following the discussion of health and well-being, participants were invited to use sticky notes to provide input on their top areas for future research, inclusive of those topics found on the online survey. A white board was available to write additional approaches not already listed. Discussion of the areas garnering the most stickies resulted in qualitative data about priority areas.
Participants
Purposive sampling to recruit a sample of autistic adults across the lifespan and in different geographic areas was accomplished through identification of support groups serving autistic individuals in rural, suburban, and urban settings. Because “access to healthcare” was a topic of importance, the need to assure a sample who may have differential access due to geographical location affordances was important. We selected New York State due to the availability of support groups in both urban, suburban, and rural communities and due to access of the Project Team and Community Council members involved in recruitment and data collection. Inclusion criteria were the same as for the survey group. Autism diagnoses were confirmed prior to participation in the focus group because recruitment occurred only with support groups in which diagnosis was required to participate; none of the focus group participants reported participating in the online survey. A total of 26 unique individuals contributed to the three focus groups (n = 10, n = 8, and n = 8 participants, respectively), one of each held in a rural, suburban, and urban area. We provided a $50 gift card to compensate participants for the 90-min focus group.
Data analysis
We transcribed all focus group sessions verbatim using an online transcription company, and we also transcribed index cards with written responses. We used MaxQDA version 12 for analysis. Coding was approached using four waves of analysis (Saldana, 2015). The first wave involved reading the focus group transcripts and index card responses completely to get a sense of the data. The second wave involved in-vivo coding for each respondent’s answer within questions in order to assign a meaningful code while reducing the volume of available data. The third wave involved organizing the codes by looking for repetitive patterns in in-vivo codes and combining the codes into themes. Waves 1 through 3 were completed by the first author (T.B.). The fourth wave involved sharing the themes with the Project Team and members of the Community Council interested in participating in the analysis, along with the de-identified transcripts and open-ended responses that fell into identified themes. Discussion, revision, and consensus of themes and priority topics occurred online through Zoom and email.
Year 2 stakeholder meeting
Purpose
A large stakeholder meeting held in Washington, D.C. aimed to engage stakeholders in additional prioritization of areas and topics identified from the survey and focus groups in the areas of mental health, gender and sexual health, and access to healthcare. This was timed to occur the day before the 2018 Association of University Centers on Disability Annual Conference, which would likely provide a broader outreach with greater inclusion of self-advocates, parent stakeholders, researchers, and those representing grassroots disability organizations.
Advertising methods and attendees
We advertised the meeting through paid advertisements on Facebook and emailing known autism advocacy groups and contacts. We offered attendees stipends to offset the costs of travel and attendance. We capped registration at 80 people, of whom 64 (80%) attended. Of the 64 attendees, 22 identified as autistic at registration, 15 were family/caregivers/support persons of an autistic adult, 23 were researchers, 5 were academic affiliates (e.g. graduate students, faculty with clinical and teaching roles), and 14 were representatives of non-academic disability organizations. Most attendees fell into more than one stakeholder type. Thirteen attendees had previously attended the Year 1 meeting.
Setting
The Community Council and Project Team worked with the hotel to ensure that the event was welcoming to autistics. An event guide provided information in advance of the meeting to ensure successful participation of all attendees.
Activities
Among other activities, attendees participated in breakout sessions that discussed and contributed to the prioritization of topics. Year 2 meeting stakeholders who participated in the mental health breakout session were presented with the top 10 topics for addressing mental health based on the focus group and survey results. In small group discussions and rankings, these individuals revised the priorities and ranked them for inclusion as the top research priorities.
Results
Demographic characteristics
Across all methods, a total of 377 individuals participated in the project activities over the 2-year period, the majority of whom were autistic adults (n = 297, 79%). No demographic information was obtained from large meeting attendees because the meetings were not research activities and only information from registration records was available to identify the individual’s stakeholder group. We present demographic information for online survey and focus group participants in Table 1.
Demographic characteristics of online survey and focus group participants.
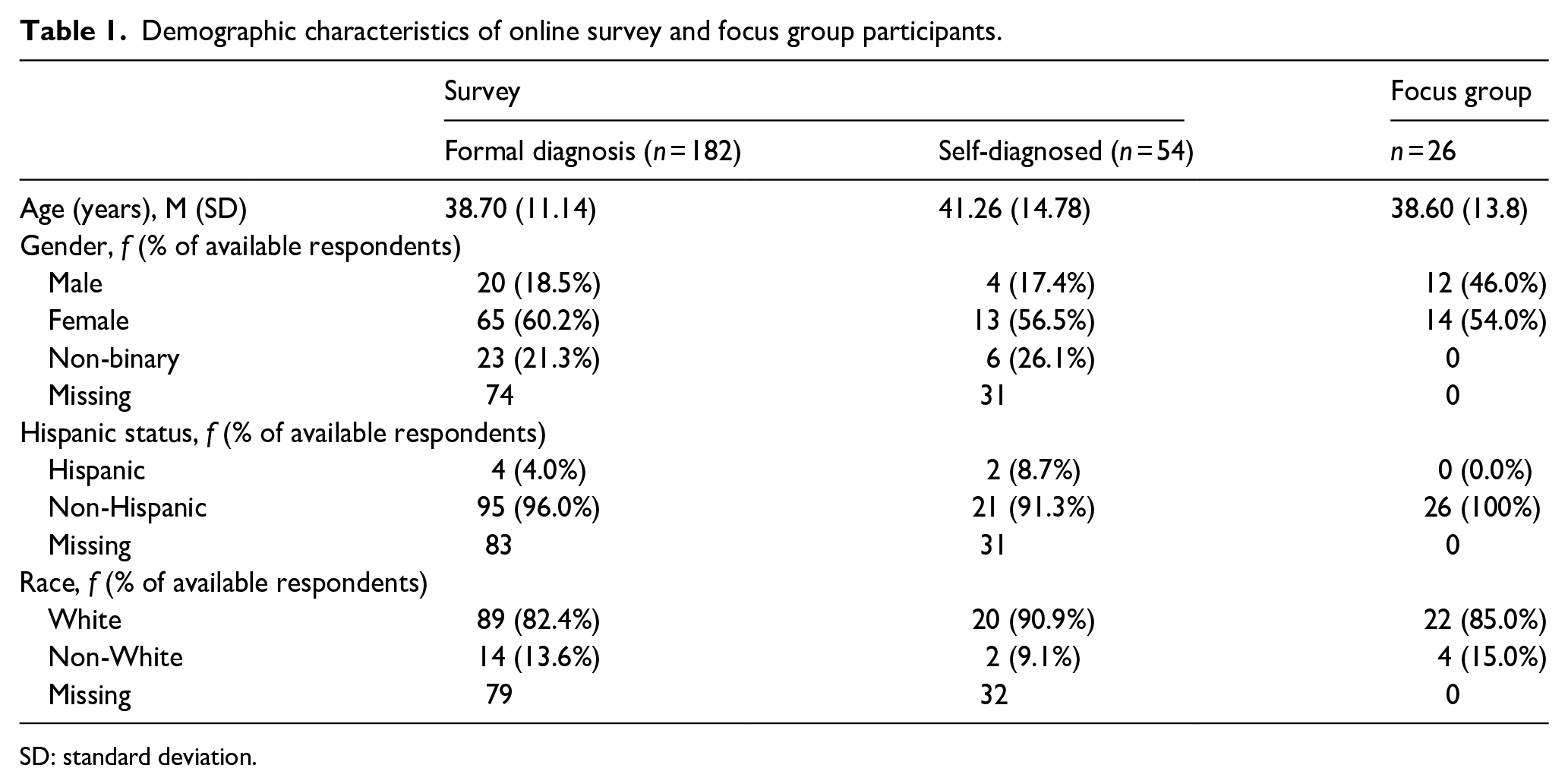
SD: standard deviation.
Among the survey participants, we compared the “diagnosed” group (reporting a formal diagnosis in childhood or adulthood) and the “self-diagnosed” group. There were no statistically significant differences in mean age, gender, ethnicity, or race for these two groups. We found differences between the online survey group and the focus group in gender ratio. The survey group included significantly fewer males than the focus groups (Fisher’s exact test, p = 0.02), and significantly more individuals self-reporting gender than the focus groups (Fisher’s exact test, p = 0.005). There were no significant differences in age between the focus group and online survey participants (t = –0.39, p = 0.69).
Desired approaches and interventions from survey respondents
Ranked mental health preferred interventions from quantitative online survey data are displayed in Table 2, and not-preferred interventions and relative rankings are displayed in Table 3.
Online survey participants who endorsed “I would participate” in mental health interventions and weighted rank (n = 136).
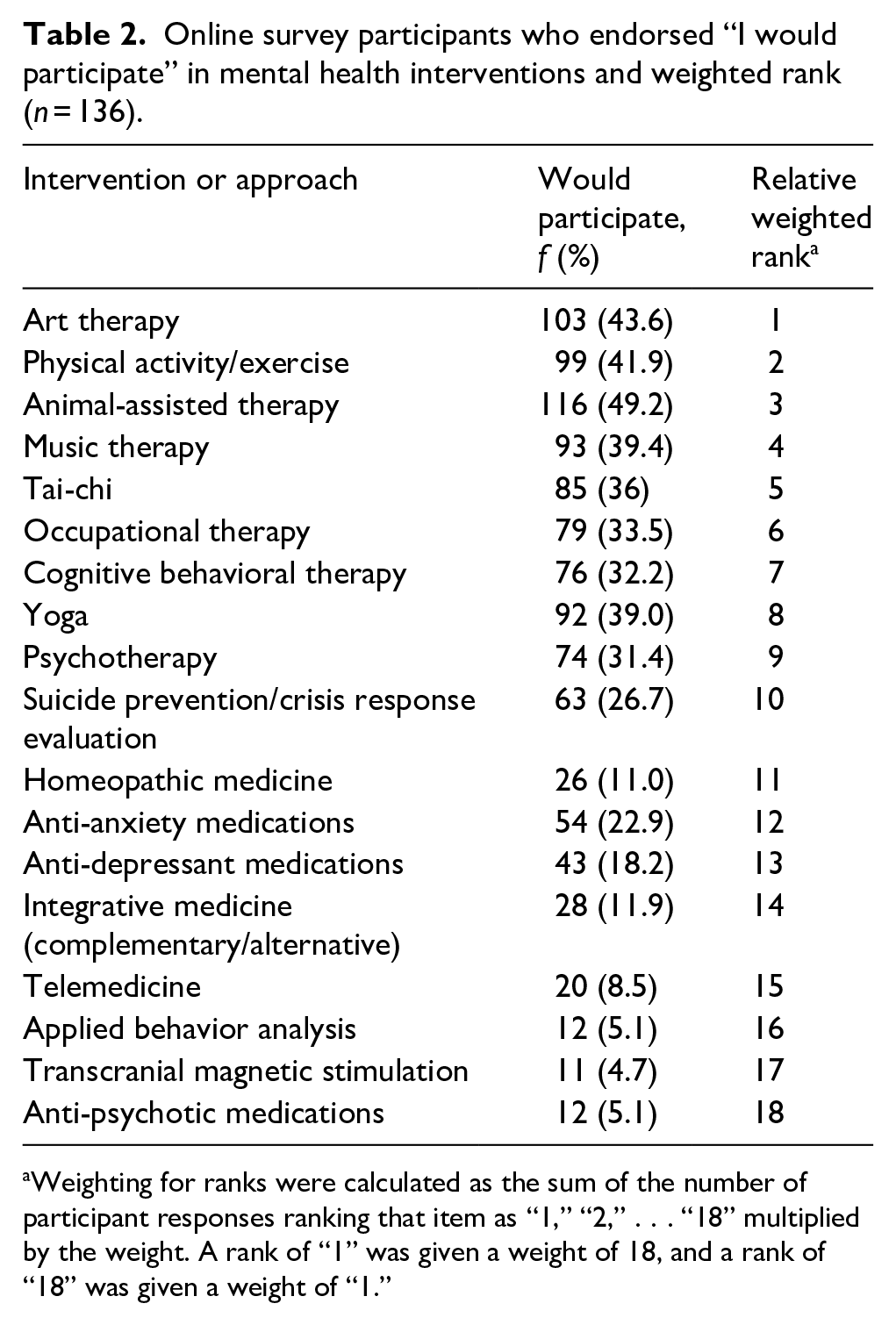
Weighting for ranks were calculated as the sum of the number of participant responses ranking that item as “1,” “2,” . . . “18” multiplied by the weight. A rank of “1” was given a weight of 18, and a rank of “18” was given a weight of “1.”
Online survey participants who endorsed “I would NOT participate” in mental health interventions and weighted rank (n = 136).
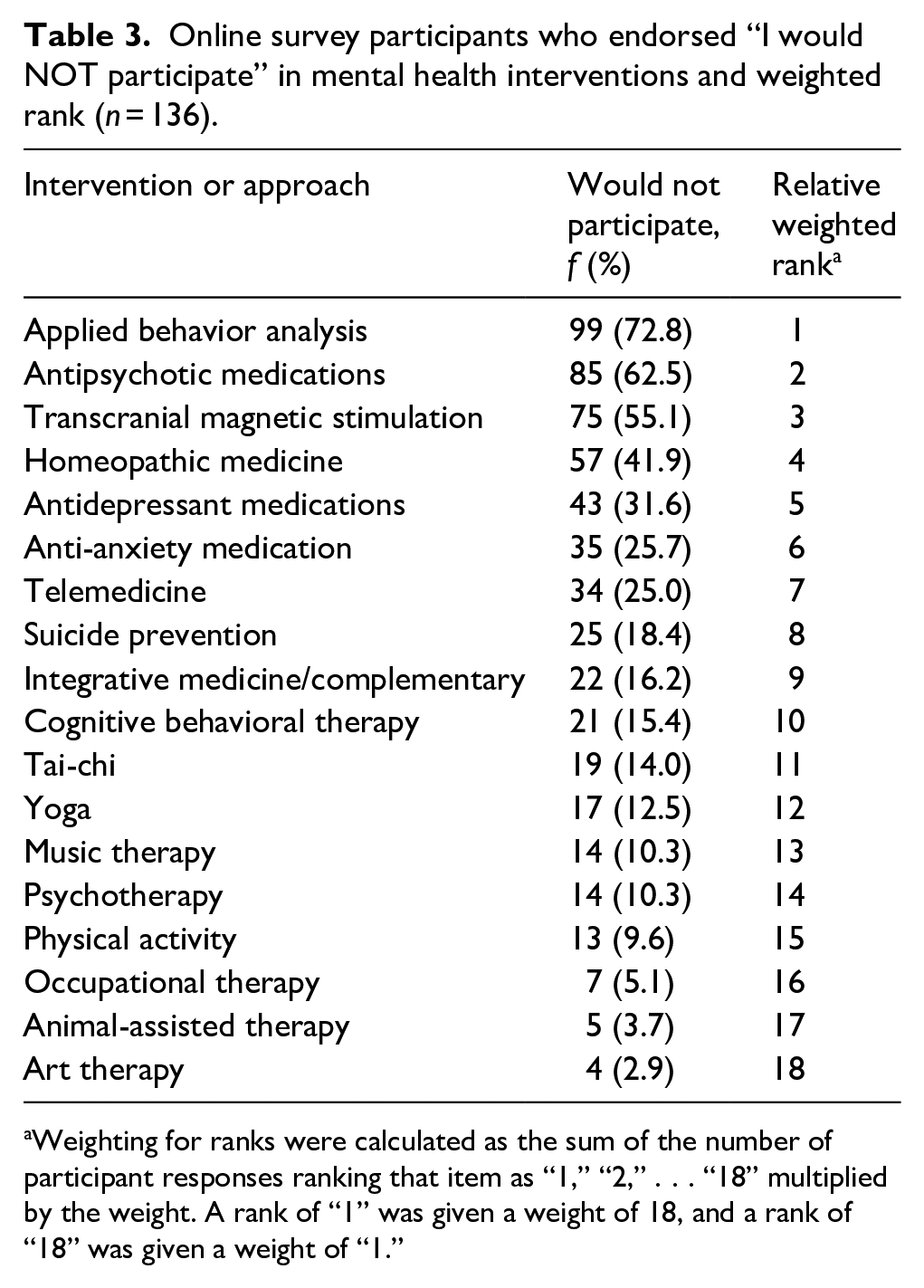
Weighting for ranks were calculated as the sum of the number of participant responses ranking that item as “1,” “2,” . . . “18” multiplied by the weight. A rank of “1” was given a weight of 18, and a rank of “18” was given a weight of “1.”
A total of 120 survey respondents (51%) qualitatively named other preferred mental health approaches for future research in the follow-up open-ended questions about desired research. The most frequently occurring qualitative categories of preferred interventions, making up more than 60% of the available responses, included (a) stigma-reduction and societal education about autism; (b) trauma-informed care and posttraumatic stress disorder (PTSD) approaches; (c) complementary and alternative approaches, primarily mindfulness and meditation; and (d) peer-led (autistic-led) support groups and interventions.
Desired approaches and interventions from focus groups
Focus group participants (n = 26) identified that they desired research on psychological therapies, including cognitive behavioral therapy (CBT) and trauma-informed care practices, endorsed by 69% of focus group participants, with the caveat that these practices were adapted for and led by autistic individuals. One participant said, as the focus group leader was writing “trauma-informed care” on a white board, “I want you to write ‘sexual assault.’ Straight up. Let’s just be real” (middle-aged female). Some focus group participants indicated that healthcare provider lack of understanding and sensitivity to previously experienced trauma exacerbated those experiences. For example, one participant noted, “Like, I feel ganged up on, like the nurses are like, ‘well you need to do this now,’ and I’m like, ‘why?,’ and they won’t explain it to me. They just do what they want, and I have no control over the situation” (middle-aged female).
The second desired focus for intervention research in the focus groups was on cannabinoids (e.g. CBD) and medical marijuana, endorsed by 65% of focus group participants, specifically as an intervention to address generalized anxiety and social anxiety. The third desired topic for intervention research endorsed by 50% of focus group participants was on side effects of prescription medications, as well as investigation into the appropriate dosage of commonly prescribed medications. One participant in the focus group clarified this topic by noting that little information exists on side effects experienced by autistic individuals: Very often when we are prescribed treatment, a medication or anything, and we have a bad negative effect from it, a bad side effect . . . and we talk to the doctor. You know, you gave me this pill and my problem still exists, and oh, my problem got worse . . . yeah, you gave me this pill for seasonal affective disorder, and it gave me suicidal thoughts . . . (middle-aged autistic female)
Desired mental health outcomes identified as priorities for research
Both online survey participants and focus group participants identified the need to focus on mental health outcomes and conditions. Survey respondents ranked the top mental health outcomes that mattered to them (Table 4).
Online survey participants who endorsed “This Outcome Matters to Me” and weighted rank (n = 136).
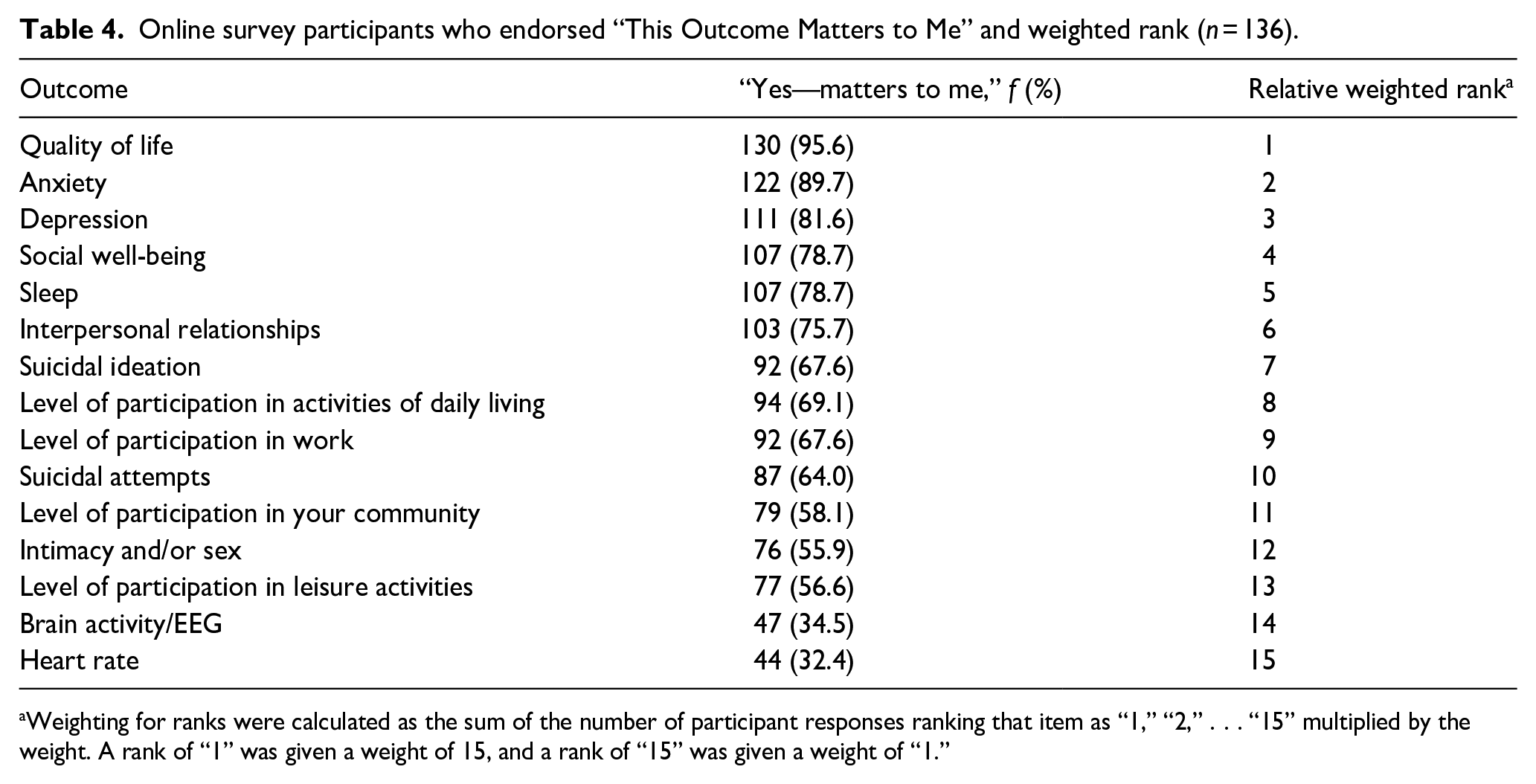
Weighting for ranks were calculated as the sum of the number of participant responses ranking that item as “1,” “2,” . . . “15” multiplied by the weight. A rank of “1” was given a weight of 15, and a rank of “15” was given a weight of “1.”
Open-ended responses from online survey participants and focus group participants resulted in additional outcomes being identified that were important when improving mental health, including levels of societal discrimination which were felt to impact mental health acceptance of self and self-esteem, co-occurring rates of PTSD and other mental health diagnoses, standard of living (e.g. rates of autistic individuals in poverty, homeless, and/or sub-par standard of living), and other objective measures of stress (e.g. cortisol) or aging (e.g. hormones associated with aging and menopause). Many respondents also indicated that it would be helpful for researchers to allow autistic research participants to define their own goals and outcomes.
Top mental health priorities
Through the iterative methods described above, a list of top mental health priorities were compiled, and are presented in Table 5.
Top mental health priority topics and questions.
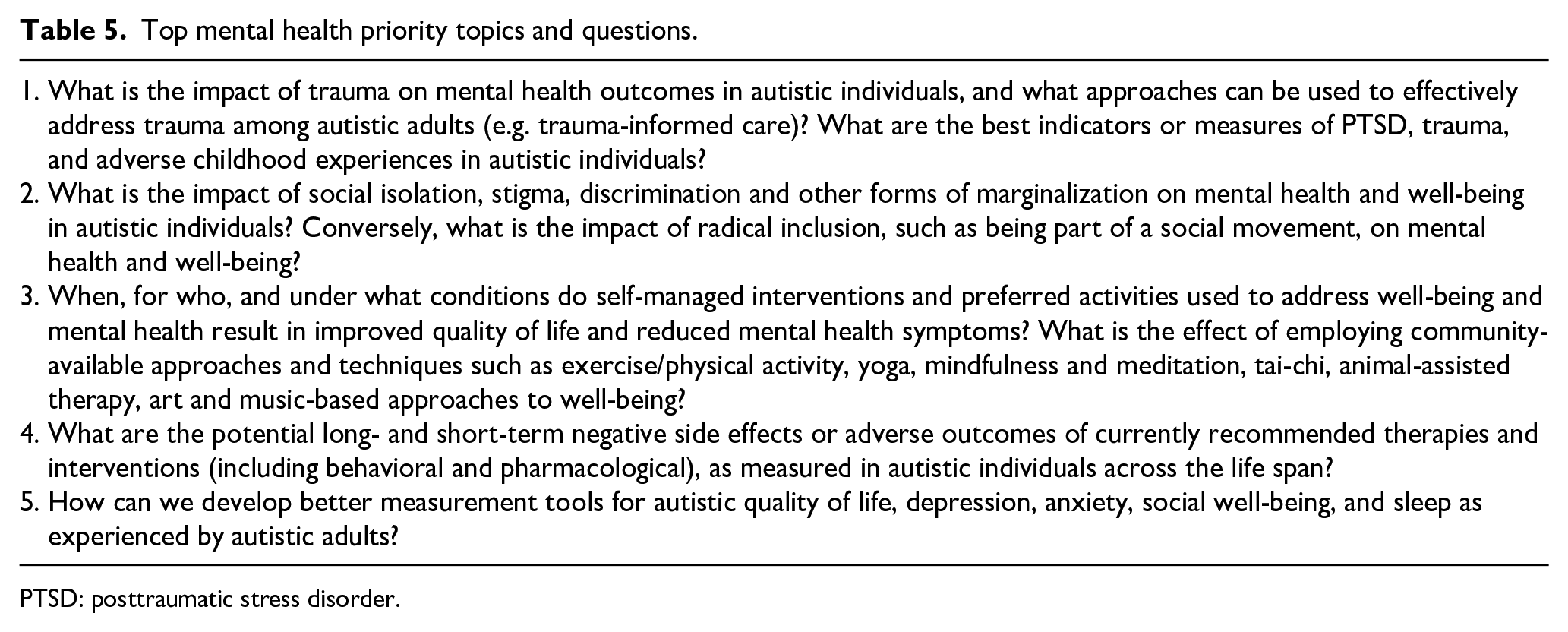
PTSD: posttraumatic stress disorder.
Discussion
This 2-year project aimed to involve the autistic adult community in defining and prioritizing specific desired outcomes and interventions for health research that directly affects their QoL. We ascertained that autistic adults in our project believed gaps existed in evidence supporting desired interventions, and that outcomes were not aligned with the needs of the community. The three large priority areas identified were mental health, access to healthcare, and gender and sexual health; this article describes the mental health priorities. We urge researchers, clinicians, research funders and policymakers to consider the desired outcomes and priorities, and to align their work to meaningfully engage the autistic community as partners in the development of future research and practice. In the past 5 years, research and initiatives to co-develop research to identify and address priorities, such as those by Cassidy and colleagues (unpublished) for an upcoming INSAR Mental Health Policy Brief on suicide, as well as work by Autistica (Cusack & Sterry, 2019), highlight the importance of engaging a variety of stakeholders in the research process. This and other priority-setting work is essential for meaningful research and practice that is relevant to autistic individuals.
The first mental health priority identified by stakeholders in our project reflects the extent to which trauma is experienced and addressed across the lifespan. Autistic adults described this in many ways, but it was clear that cumulative, repeated negative experiences with others in a variety of environments (homes, schools, workplaces, healthcare settings, communities) resulted in a range of poor mental health outcomes. Terms such as “bullied,” “discriminated against,” “stigmatized,” and others were frequently used in conjunction with trauma. Existing research has identified that bullying victimization among autistic adolescents is as high as 46% in the United States (Sterzing et al., 2012). Bullying is strongly related with anxiety in autistic adolescents, as reported by parents (e.g. Weiss et al., 2015), and although bullying results in cumulative risks to these children (Hebron et al., 2017), little work has investigated these outcomes among autistic adults. In adult samples with serious mental illness, a new construct called “verbal violence” has been used (e.g. Karni-Vizer & Salzer, 2016), and may have relevance to this priority area. In addition, work by Kerns and colleagues on adverse childhood experiences in autism shows promise for translation into adult research (e.g. Kerns et al., 2015). In our project, autistic adults not only desired prevalence rates of trauma, but specifically requested that research inform better ways to assess trauma and PTSD, and evaluate approaches to provide trauma-informed care for autistic individuals.
Related to the experience of trauma was the priority of increasing societal awareness of autistic ways of being, and promotion of inclusivity and respect for neurodiversity. The feeling of societal exclusion, and conversely, inclusion and radical inclusion, was a primary discussion point among our Year 2 meeting participants. The concepts related to belonging, “finding one’s tribe,” and feeling a part of a community were important aspects of mental health. The negative mental effects of “camouflaging” and “masking” in society are described in recent research, and support the need for considering societal approaches for promoting autistic identity (e.g. Cage et al., 2018; Cage & Troxell-Whitman, 2019). Broadly, societal acceptance and inclusion were also identified as a top priority by Gotham et al. (2015), as expressed by stakeholders in that study.
The impact of interacting with providers with little to no training in addressing their needs led many autistic adults to request more research on approaches and interventions that could be self-initiated or managed, or were accessible in their communities. These interventions specifically do not require a “gatekeeper” to access them (e.g. a medical provider), and would allow for self-management. Some of these interventions which autistics desired evidence for included the effect of self-selected exercise and physical activity for depression (Cooney et al., 2013), tai-chi or yoga, mindfulness meditation, or animal-assisted therapy (e.g. Jones et al., 2019). Of these desired priority interventions, only mindfulness meditation has been preliminarily evaluated in autistic adults (e.g. Sizoo & Kuiper, 2017; Spek et al., 2013).
Another self-initiated intervention, medical marijuana or cannabinoids, was identified as a research priority. Although this intervention has begun to be evaluated in autistic children (e.g. Schleider et al., 2019), some adverse effects have been noted (e.g. Aran et al., 2019). Future research is requested by the autistic adult community regarding the safety and efficacy of these interventions for improving mental health outcomes.
Autistic participants in our focus groups also requested more research on psychological approaches that have evidence supporting their use, such as CBT, as long as those interventions were adapted for and evaluated with autistic adults. CBT was among the top 10 interventions identified by online survey respondents, as well. Of interest is that the emerging literature supports the use of CBT with autistic adults as an effective intervention for mental health outcomes (e.g. Hesselmark et al., 2014; Russell et al., 2013).
Autistic individuals also desired research on the short- and long-term side effects of prescribed medications and social-behavioral interventions, particularly those applied in childhood, that were seen as traumatic. When considering the bulk of pediatric autism interventions implemented in childhood, few evaluate the adverse effects as reported by the autistic individuals themselves. Although most other fields would consider adverse effects in any intervention (medical, social-behavioral, other), autism research rarely describes adverse events with the exception of pharmacological research involving children (e.g. Cai et al., 2018).
In our open-ended and closed-ended questions of outcomes and health, individuals frequently brought up QoL and social well-being as the most important, with other similar manifestations of well-being such as sleep, depression, and anxiety being among the top preferred outcomes that were desired for research to address. QoL has recently been a focus of research among autistic adults (Bishop-Fitzpatrick et al., 2017; Kim, 2019; Park et al., 2019; van Heijst & Geurts, 2015) and validation of measures capturing QoL among autistics are in development.
Our priority-setting work was ongoing at the same time as other priority-setting work in other countries (Cusack & Sterry, 2019; Cassidy et al., unpublished). These other groups have identified somewhat similar research priorities, although the Autistica’s Top 10 (Cusack & Sterry, 2019) were broad research priorities (not just on health), and the University of Nottingham research priorities were specific to suicide. Autistica’s report details that the top priority was addressing mental health—which aligns with what our project identified (Cusack & Sterry, 2019). Our findings detailed the specific topics that autistic adults identified as relevant when considering mental health research. Another overlap in priorities from these other groups and our work center on the specific outcomes of interest to the autism community. The Autistica Priority 4 centers on the importance of understanding and addressing anxiety for autistic individuals; we found anxiety to be the second most important outcome to address, endorsed by approximately 90% of our survey respondents. Similarly, the Nottingham Mental Health research group priorities identified the need to better understand the relationship between sleep and suicide. Our stakeholders also identified sleep as one of the most important health outcomes to address. Overall, priority-setting activities are an important part of the research process. Our work, and that of others, contribute to a shared research agenda and open the door to common actions that researchers, stakeholders, practitioners, and funders can take to address community-identified needs.
Limitations and conclusions
This project is one of the first to attempt to identify autistic priorities for research through stakeholder-driven approaches in the United States. However, there were several notable limitations that limit our understanding of these priorities. First, although we attempted to reach across the entire spectrum and invite people to participate in a variety of ways, we do not feel that we sufficiently included the following underrepresented groups: racial and ethnic minorities on the spectrum, or individuals who may not have been able to self-report online or through the focus group due to lack of access, technology, transportation, or communication. Although non-speaking individuals may have participated in our online survey (only 21.3% of respondents preferred to communicate through verbal/spoken language), we did not have an option for caregivers of autistic adults who may not have been independent in reading and answering the questions to participate, and the survey was not trialed for those with screen readers. Future research is needed to target recruitment of these underrepresented groups in collaboration with key stakeholders from those communities. It is likely that these individuals may have different priorities, possibly due to the nature of “compounded disparities,” in which being a member of more than one group experiencing disparities places one at greater risk for poor health outcomes (e.g. Yee et al., 2016). As noted in our methods, we aimed to include individuals across the lifespan in the priority-setting activities. However, we did not conduct analyses to evaluate differences between those in different life stages. Future work could further identify how priorities for research outcomes and available interventions differ across age groups.
Other limitations include the possibility that representatives of a vocal minority were more likely to be involved in our priority-setting activities. We do not believe this was the case, however, because not all individuals, such as those who participated in our focus groups, had heard of the project, the survey, or been involved in advocacy work in the autism community. Most individuals in our focus groups expressed similar needs for research to focus on aspects of well-being and QoL that were present in survey responses. Finally, our sample included a higher ratio of females to males than is generally expected, based on autism prevalence estimates. However, there is some evidence to suggest that females are underdiagnosed, and additionally, females and non-binary individuals are typically underrepresented in autism research; we therefore feel the inclusion of female and non-binary voices in the discussion of priorities is a strength of this work. Generalizability should be carefully assigned to the sample we included, which were those able to independently contribute their perspectives through online, written, or spoken approaches and who were sufficiently well connected to learn about the opportunity to participate.
In sum, our priority-setting activities broadly found that one priority area for future research was mental health. Within the area of mental health, autistic adults expressed a desire for research to focus on improving QoL and social well-being outcomes, as defined by them, and called for approaches that addressed societal barriers such as stigma and discrimination against autistics that led to exclusion, bullying, and other forms of trauma. In addition, participants and stakeholders in our project desired research that evaluated approaches for improving mental health that generally were community-available, and did not require a gatekeeper (medical professional). Usually, these approaches could be self-initiated, and were not in-and-of-themselves approaches that aimed to change characteristics of their autistic identity. When preferences were expressed for more medical-model approaches, such as pharmacological approaches, cannabinoids, or cognitive-behavioral approaches, the stakeholders expressed a desire for those interventions to be evaluated for short- and long-term side effects, and for those approaches to be adapted and delivered by autistic peers to ensure they were relevant and appropriate to the needs of the community.
Supplemental Material
Appendix_120119 – Supplemental material for Listening to the autistic voice: Mental health priorities to guide research and practice in autism from a stakeholder-driven project
Supplemental material, Appendix_120119 for Listening to the autistic voice: Mental health priorities to guide research and practice in autism from a stakeholder-driven project by Teal W Benevides, Stephen M Shore, Kate Palmer, Patricia Duncan, Alex Plank, May-Lynn Andresen, Reid Caplan, Barb Cook, Dena Gassner, Becca Lory Hector, Lisa Morgan, Lindsey Nebeker, Yenn Purkis, Brigid Rankowski, Karl Wittig and Steven S Coughlin in Autism
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of their Autistic Adults and other Stakeholders Engage Together (AASET) Community Council (CC) members. The following CC members are contributors to various project activities: Daria Tyrina, Amy Gravino, Liane Holiday-Wiley, Jamie Marshall, Bill Peters, and Cyndi Taylor. In addition, the authors are thankful for the time and energy that all stakeholders contributed to attending and participating in the various project activities.
Authors’ note
Portions of this project and the results have been presented in various venues, but the content as presented has not been submitted for publication to any other journal.
Author contributions
T.W.B. and S.M.S. conceptualized the idea for the project; obtained funding; organized and planned all aspects of the project including the design and interpretation of data gathered from the Year 1 and Year 2 meetings, survey, and focus groups; and prepared and edited the manuscript as written. K.P. organized and collected data for the focus groups, contributed to data analysis of all the survey and focus groups, participated in the Year 1 and Year 2 meetings, and significantly revised the manuscript. P.D. and A.P. contributed to the design of all project activities including the survey, focus groups, Year 1 and Year 2 meetings, organization and administration of project activities, and approval of the final manuscript as written. M.-L.A., R.C., B.C., D.G., B.L.H., L.M., L.N., Y.P., B.R., and K.W. contributed to the decision-making for development of the survey, interpretation of de-identified data, participation in the Year 1 and/or Year 2 meetings, and revision and approval of the manuscript as written, and are alphabetized based on last name. S.S.C. contributed to the design and development of the survey instrument, statistical expertise in analysis and in significant revision, and approval of the manuscript as written.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the funder did not play a role in the design, data analysis, or interpretation of this study. The grant program officer participated in the Year 2 meeting as a panelist, but did not participate in the implementation or analyses of any project activity, nor did Patient-Centered Outcomes Research Institute (PCORI) or the grant officer participate in the interpretation of the data.
Ethical compliance
All components of the project were reviewed by the institutional review board (IRB) of the first author, although not all components were deemed human subjects research. An IRB Authorization Agreement existed for the reliance of the second author’s IRB on the first author’s IRB. All procedures involving human subjects data were conducted in accordance with the ethical standards of the institution and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained for face-to-face focus groups.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project, Autistic Adults and other Stakeholders Engage Together (AASET), was funded through a Patient-Centered Outcomes Research Institute (PCORI®) Eugene Washington PCORI Engagement Award (EAIN# 4208). The views presented in this presentation are solely the responsibility of the authors and do not necessarily represent the views of the PCORI, its Board of Governors, or Methodology Committee.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.