
Abstract
Evidence suggests disclosing an autism diagnosis is associated with reduced stigmatization for autistic adults. However, it is unknown whether this is true for autistic adolescents. We used a vignette-and-questionnaire design to study stigmatizing attitudes with adolescents (aged 11–12 and 14–16 years, total N = 250) in a UK school. We investigated the effect of disclosing that a fictional adolescent had an autism diagnosis on stigmatizing attitudes of peers by testing the effect of disclosure of diagnosis on the social and emotional distance pupils wanted to maintain from the autistic adolescent. We also tested the effect of disclosure on peers’ assessment of the adolescent’s responsibility for their own behaviour. We checked to see if the effects were moderated by gender and age-group. Disclosing autism did not affect the social and emotional distance peers wanted to maintain from the autistic adolescent, but was associated with significant reduction in personal responsibility attributed to the adolescent’s behaviour. Boys attributed more personal responsibility to the autistic adolescent than girls, but this gender effect was reduced when autism was disclosed. These findings suggest that disclosing autism to other pupils may be of limited use in reducing stigmatization by peers in UK schools.
Autism spectrum disorder (ASD, hereafter referred to as autism) is a neurodevelopmental condition, characterized by difficulties with social communication and interaction, and patterns of repetitive behaviours and intense interests (American Psychiatric Association, 2013). Autistic adolescents experience high rates of bullying and social isolation (Humphrey & Lewis, 2008), poorer friendship quality, and lower social network status compared to their typically developing peers (Locke, Ishijima, Kasari, & London, 2010). This is especially problematic as peer relationships become particularly important in adolescence (Brown & Larson, 2009), and positive peer relationships are crucial for successful inclusion of autistic pupils at school (Humphrey & Lewis, 2008).
Labelling and stigma
Stigmatization is here defined as the process by which a person is labelled as undesirably different from the common group and experiences discrimination and loss of status as a result of being linked to negative stereotypes (Link & Phelan, 2001). Stigmatization leads to both individual and structural discrimination, as well as self-stigmatization, puts the stigmatized person at greater risk for mental and physical health problems, and negatively affects motivation and performance (Barreto, 2014). Adolescents with a diagnosis of autism are victimized more frequently than their typical peers (Zeedyk, Rodriguez, Tipton, Baker, & Blacher, 2014), and autistic children and their parents experience avoidance and negative attitudes from others (Gray, 2002).
It is still a matter for debate whether disclosing autism leads to better outcomes for the autistic person, although medical policy and charity information emphasize the importance and value of diagnosis for improved outcomes (Russell, 2016). Increased or decreased stigma is a possible consequence of diagnosis and disclosure. Labelling theory predicts that publicly labelling a person with a disorder will increase the stigmatization they experience (Scheff, 1966). Corrigan (2007) suggests that a clinical diagnosis may increase the application of stereotypes and so increase stigmatization. For a variety of conditions, it is unclear whether a diagnostic label improves or damages children and adolescents’ self-concept (O’Connor, Kadianaki, Maunder, & McNicholas, 2018). Regarding autism, adolescent pupils report that they feel ‘marked’ by their diagnosis and are concerned that diagnosis has altered how they are viewed by others (Jones, Gallus, Viering, & Oseland, 2015). Others feel that disclosing the diagnosis makes it harder for them to fit in (Humphrey & Lewis, 2008). Young people aged 9–16 years report wanting to distance themselves from the label of autism, and most could not report any benefit of having their diagnosis (Calzada, Pistrang, & Mandy, 2012).
However, parents in the latter study reported that although they were concerned about stigma resulting from their child’s diagnosis, they believed disclosing was useful for improving others’ understanding of (and adjusting to) their child’s difficulties and could stop others from blaming their child for atypical behaviours (Calzada et al., 2012). A label of autism might be able to decrease the stigmatization of a child by providing a neurological explanation for their atypical behaviour (Farrugia, 2009). The ‘problem behaviour’ is no longer considered the fault of the child, so the personal responsibility attributed to the child is decreased. Attribution theory proposes that the degree to which an observer believes a person to be responsible for their negative behaviour affects the observer’s emotional and sympathetic response to that person, which can in turn affect stigmatization (Weiner, 1993). There may be other benefits to disclosing; for example, autistic children may have more consistent social support at school when their diagnosis is fully disclosed to teachers and pupils (Ochs, Kremer-Sadlik, Solomon, & Sirota, 2001). In one study with autistic teenagers, participants reported that having a diagnostic label of autism had been important in constructing a positive sense of self, by legitimizing their differences and by providing a sense of common identity with other people who had autism (Mogensen & Mason, 2015). Having a diagnosis was experienced as positive if the autistic adolescent felt it improved self-understanding and gave them control in their life. Generally, disclosing a stigmatized identity can improve a person’s feelings of authenticity, as it frees them from the pressure of secrecy and trying to ‘pass’ as having a non-stigmatized identity (Newheiser & Barreto, 2014). Indeed, some autistic people conceive of autism as a complex difference to support rather than cure, regarding autism as a positive identity (Kapp, Gillespie-Lynch, Sherman, & Hutman, 2013). Similarly, they are less interested in normalizing autism than non-autistic people, in association with their relatively low stigma towards autism (Gillespie-Lynch, Kapp, Brooks, Pickens, & Schwartzman, 2017).
Several studies have used vignettes to examine whether disclosing a condition has an impact on others’ perceptions. Vignettes usually consist of text describing a fictional person or situation that participants respond to, often by questionnaire, and are a popular way of investigating stigmatizing attitudes. Including a label of autism in a vignette of a person with typical autistic characteristics tends to decrease stigmatization by adult observers, so the label of autism can protect the autistic person from stigma. For example, college students’ attitudes are more positive towards a peer when labelled with ASD compared to when only typical ‘autistic behaviours’ are described (Matthews, Ly, & Goldberg, 2015; Sasson & Morrison, 2019).
The literature on how labelling affects stigmatization for children and adolescents is mixed. Adults perceived an autistic child more positively when autism was disclosed, compared to when the child displayed typical autistic behaviours but did not have an autism label (Chambres, Auxiette, Vansingle, & Gil, 2008). The label had an overall protective effect, but adult participants evaluated the labelled child as being more emotionally disturbed. By contrast, Butler and Gillis (2011) found that labelling a student with Asperger’s disorder had no effect on college students’ desire for social distance from them. Overall, previous research seems to suggest that disclosing autism to adults can reduce stigmatization, but it may have an associated cost for the autistic person, as observers may consider them to be less capable and more emotionally disturbed.
Adults may stigmatize a child less when a diagnostic label of autism is applied, but there is less evidence that children and adolescents do the same. In addition, since 7–12 year olds displayed more stigma towards a child displaying typical ‘autistic behaviours’ than adults did in the absence of a label, it is not self-evident that strategies that affect adult attitudes would similarly affect those of young people (Harnum, Duffy, & Ferguson, 2007). We have identified three studies that examined children’s perceptions of an autistic peer, with and without a label of autism. Campbell (2007) found that adding a label of autism as well as providing explanatory information about autism improved how 13 year olds perceived a hypothetical peer. A similar result was found for 8–12 year olds (Campbell, Ferguson, Herzinger, Jackson, & Marino, 2004). However, Swaim and Morgan (2001) found no difference in the behavioural intentions of 8–12 year olds towards an autistic child when both label and explanatory information were provided. These three studies used slight variants of an explanatory vignette that included the following quote: ‘I have autism, which means that there’s something wrong with my brain’, which has been criticized for ‘not be[ing] the best way to decrease stigma’ (Gillespie-Lynch et al., 2015), and may have unduly influenced participants.
It remains unclear whether the effects detected in these studies were due to the application of the label, or whether results were affected by the inclusion of this sentence. Furthermore, all three studies were carried out with US samples, and it is unknown if results are generalizable beyond that setting. The United States is more highly medicalized than the United Kingdom, tending to frame deviance, particularly in childhood, as a medical problem (Malacrida, 2004; Rafalovich, 2013). Diagnostic labels, such as autism, may therefore be more meaningful and familiar to pupils in the United States, so disclosure could be more beneficial in reducing stigma than it is for UK pupils. However, a more medicalized understanding of autism (as opposed to a diversity-oriented framing) may engender greater desire for social distance. Our goal was to examine the effect of disclosure among adolescents living in the United Kingdom, with the primary hypothesis that adolescents would stigmatize the autistic adolescent less when autism was disclosed than when it was not.
Disclosure has been studied at various developmental stages, but we are not aware of any studies which have compared how older and younger adolescents’ attitudes vary in response to disclosure of autism. Early adolescence (ages 11–14 years) shows the highest prioritization of popularity and status, with young adolescents prioritizing popularity over friendships and empathy for other peers (LaFontana & Cillessen, 2010). Younger adolescents may therefore be more likely to be sensitive to deviations from the norm and therefore more likely to stigmatize an ostracized adolescent. There may also be a difference between the way older and younger adolescents react to the disclosure of a diagnostic label. Older adolescents may see the label of autism and the person separately (Fondelli & Rober, 2017), and be more concerned about the impact of stigma on peers (Berger, Hasking, & Martin, 2017). Disclosing a label might be more influential in reducing stigmatization by older adolescents than for younger adolescents.
In addition, observer gender is known to affect stigmatization of a disabled person. Studies tend to find that adult women stigmatize autistic people less than men do (Chambres et al., 2008; Gillespie-Lynch et al., 2015), although there is some conflicting evidence for this finding (Matthews et al., 2015; Nevill & White, 2011). Women may be less likely to endorse stereotypes (Carter, Hall, Carney, & Rosip, 2006), and girls report more positive cognitive attitudes and behavioural intentions towards an autistic peer (Campbell, 2007). To shed further light on this, we also examined whether the effect of disclosing autism was greater for the older age-group, and for girls.
The issue of whether an autistic adolescent should disclose to peers is of high importance. Can disclosing autism reduce stigmatizing attitudes that peers may harbour towards an adolescent with autistic behaviours? Or could disclosure negatively affect how the adolescent is perceived? It is crucial to ascertain if disclosing autism is helpful in reducing stigmatization of pupils in order to provide concrete recommendations to parents, teachers and autistic pupils themselves.
This study aimed to assess whether the disclosure of the label of autism affected the stigmatization of an autistic adolescent by their peers, compared to a baseline of stigmatization due to presence of behaviours typical of autism. Given that our primary hypothesis was that adolescents would stigmatize the autistic adolescent less when autism was disclosed, we expected to see decreased social distance, decreased attribution of personal responsibility and decreased negative affect in the disclosure condition compared to the non-disclosure condition.
Methods
Design
Ethical approval was obtained from the University of Exeter. The study had two between-participant label conditions: Disclosure and No Disclosure. Participants read three vignettes describing three fictional adolescent boys, including their background, interests and behaviours. The vignettes were also read aloud to the class. The first vignette described a neurotypical adolescent (i.e. without characteristics of a neurodevelopmental condition), the second an adolescent with behaviour typical of autism and the third an adolescent with behaviour typical of attention deficit hyperactivity disorder (ADHD) (both according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013)). All three vignettes were designed to include the positive attributes and strengths of the child (e.g. the autistic child was described as funny, focused and actively pursuing his interests) in addition to describing their weaknesses. Our focus in this study was the second vignette, which described an autistic child and either included or did not include the label of autism, according to condition (see Supplemental material, Appendix 1 for vignette). Data from the study are freely available online (www.ukdataservice.ac.uk).
Vignettes were accompanied by stock photographs of three adolescent boys, licenced from Shutterstock. The pairing of vignette and photograph was counterbalanced between classes to prevent spurious effects due to the photograph itself. One class was given a reordered workbook, with the ADHD vignette appearing before the autism vignette, to test for order effects.
The label of autism was disclosed by including the disclosure sentence: ‘Alex has autism spectrum disorder, also known as autism’ in the autism vignette. The remaining classes received the same autism vignette without the disclosure sentence. Classes were randomly assigned to disclosure conditions, with all children in the same class receiving the same condition. Approximately half the participants were assigned to the ‘Autism disclosure’ condition (n = 115) and half to the ‘Autism non-disclosure’ condition (n = 135).
Following the presentation of each vignette, participants answered questionnaires about their attitudes and feelings towards the fictional adolescents, plus brief personal attributes, via an anonymous self-report booklet (Supplemental material, Appendix 2).
Setting and participants
Participants were 250 students across two age-groups (11–12 years, Mage = 11.2, SD = 0.4, and 14–16 years, Mage = 14.5, SD = 0.5) attending a secondary school in the South West England. 7.9% of the student population were from minority ethnic origins (UK average: 29.1%, but 7.9% is typical of the regional demographics), and 12.2% received free school meals, an indicator of pupils’ family economic status (UK average: 12.9%; Department for Education, 2017). The school was recruited by opt-in procedure through contacting all secondary schools in the area who had expressed an interest in participating in research.
The vignette study was carried out as part of the school’s ‘Impact Days’, annual extracurricular educational activities days to enrich the educational environment. Data were collected from 116 students (aged 11–12 years) on the Impact Day for Year 7 students in October 2017 and from 134 students (aged 14–16) on the Impact Day for Year 10 students in February 2018. Year 7 participants were asked not to discuss the study between the two data collection points. Data were collected on a class-by-class basis, for classes of between 20 and 30 pupils. All students within Years 7 and 10 were eligible for participation. Consent for participation in the study was gathered first by prior parental opt-out and, second, by an opt-in mechanism by the adolescent on the day of the study, with 0.8% of pupils deciding not to participate.
Sufficient sample size for the moderation analysis was determined with an a priori power analysis on G*Power, using a linear multiple regression test. Based on the assumptions α = 0.05, power = 0.90, medium effect size (f2 = 0.15) and five predictors (three variables and two interactions), the sufficient total sample size to detect the hypothesized effect of moderation by age and gender was 138.
Materials
The vignettes used were developed by the authors from materials used by Harnum et al. (2007), Ohan and Visser (2009), and Swaim and Morgan (2001). All materials used in the study were piloted with a separate group of adolescents and teachers to confirm that the content was appropriate for the participants. Feedback from special educational needs-staff confirmed that the vignettes were realistic in their depictions of adolescents with neurodevelopmental disorders.
Measures
Participants self-reported their age, gender and if they had any additional support needs (ASNs). Social distance, personal responsibility and negative emotional affect are all reliable and often-used ways of assessing stigma towards others (Link, Yang, Phelan, & Collins, 2004). Higher scores in these three dimensions reflect higher stigmatization of the vignette adolescents. The scales used in the study were developed from existing scales to make them appropriate for a UK adolescent population. Supplemental material, Appendix 2, gives the adapted scales and demographic questions in full.
Social Distance Scale
The Social Distance Scale was used to assess how willing the participants would be to interact with the autistic adolescent in the vignette, with items such as ‘I don’t want Alex to join my class’. Participants responded to eight items on a 5-point scale (1 = Strongly disagree to 5 = Strongly agree); higher scores reflect the desire for more social distance from the adolescent. Internal reliability was high, Cronbach’s α = 0.90. The scale was developed from the Social Distance Scale adapted by Crandall (1991), Shared Activities Questionnaire (Morgan, Walker, Bieberich, & Bell, 1996) and Openness Scale (Harnum et al., 2007).
Personal Responsibility Scale
This scale was used to measure how responsible participants thought the adolescent in the vignette was for their own behaviour, with items such as ‘Alex is acting this way on purpose’. The scale has four items, answered on a 5-point scale (1 = Strongly disagree to 5 = Strongly agree) with higher scores indicating higher perceived responsibility. It had acceptable reliability, α = 0.63. The scale was adapted from the Perceived Responsibility Questionnaire (Campbell, 2007).
Negative Affect Scale
Affective attitudes towards the adolescent in the vignette were assessed by the Negative Affect Scale. This scale has six items (e.g. ‘I feel irritated by Alex’), answered on a 5-point scale as before (1 = Strongly disagree to 5 = Strongly agree). Higher scores indicate more negative affective attitudes. Internal reliability was good, α = 0.86. The scale was developed from the Openness Scale (Harnum et al., 2007) and the Positive and Negative Affect Scale (Watson, Clark, & Tellegen, 1988).
Preliminary analyses
Analyses were conducted using Stata 15. No outliers were found for the Social Distance, Personal Responsibility, or Negative Affect scales. 3.2% of data were missing for these three outcome scales. Missing data points were replaced by prorating.
Measured variables were compared for the autistic vignette and the neurotypical vignette using paired t-tests. The differences between the measured variables were significant in all three tests, with participants desiring more social distance from the autistic adolescent, t(249) = −1.95, p = 0.05, attributing less personal responsibility to the autistic adolescent, t(248) = 8.92, p < 0.001, and feeling more negatively about the autistic adolescent, compared to the neurotypical adolescent, t(249) = −2.33 p = 0.02.
Differences between the distributions of baseline characteristics of participants (Table 1) in the disclosure/non-disclosure conditions for the autism vignette were examined by chi-square tests. No significant differences (at p < 0.05) in distribution were found for age-group, gender, or ASN.
Baseline characteristics, with mean values and standard deviations of measured variables.
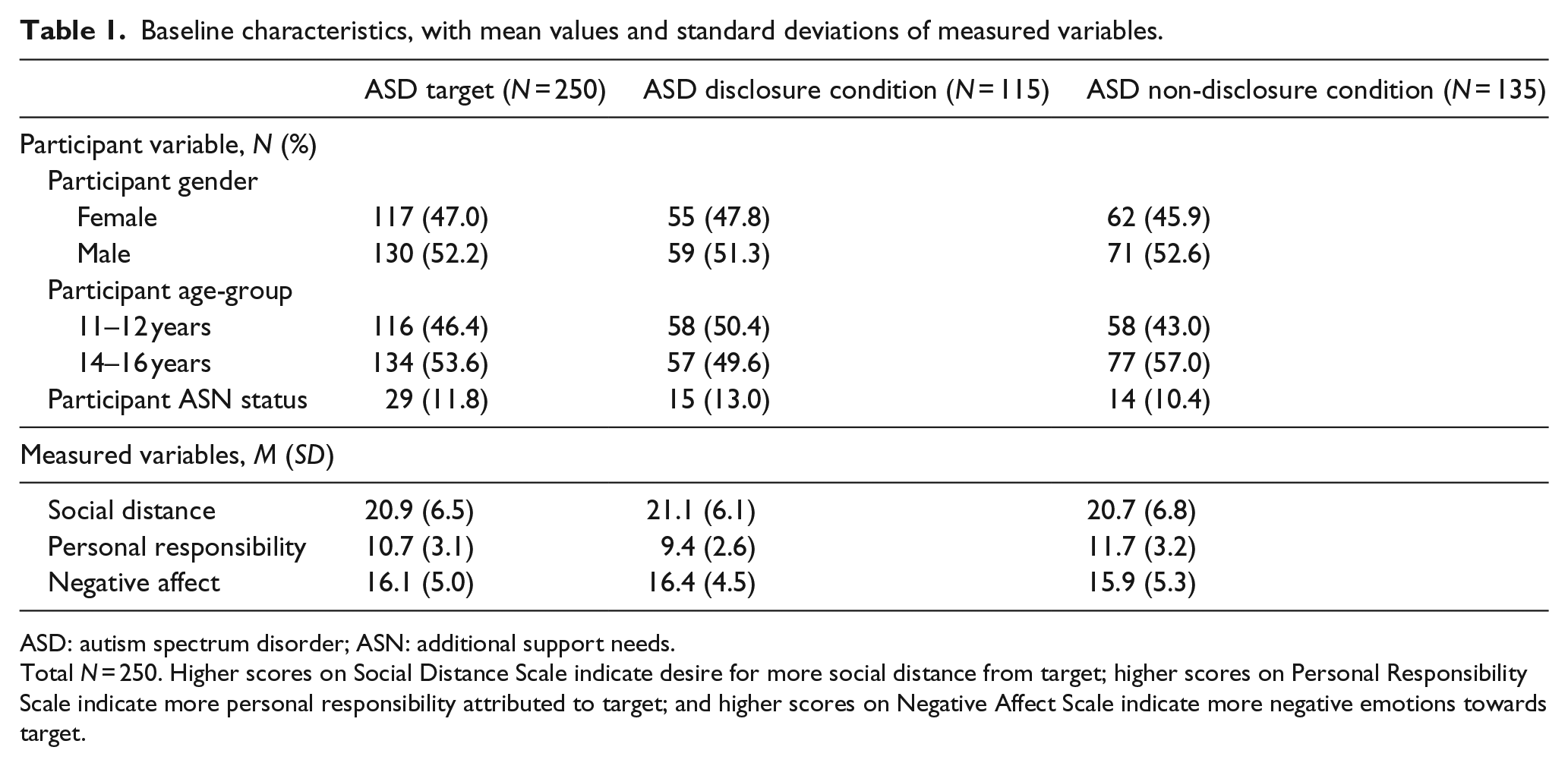
ASD: autism spectrum disorder; ASN: additional support needs.
Total N = 250. Higher scores on Social Distance Scale indicate desire for more social distance from target; higher scores on Personal Responsibility Scale indicate more personal responsibility attributed to target; and higher scores on Negative Affect Scale indicate more negative emotions towards target.
A factor analysis of the items for the three outcome scales was performed to test whether these scales represented the same construct (of stigma). The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.91, above the recommended value of 0.6, and Bartlett’s test of sphericity was significant, χ2(153) = 2143.7, p < 0.001. All 18 items were therefore included in the factor analysis. Factor analysis showed that all items from the social distance and negative affect scales loaded strongly onto the first factor, with all items from the personal responsibility scale loading onto a second factor. The two factors were used as outcome measures in the remaining analysis. The first extracted stigma factor was named social and emotional distance and the second was personal responsibility.
Analyses
Unadjusted regression analysis was carried out to investigate the relationship between independent variable and dependent variables. The model was run twice with disclosure condition as the independent variable and the two stigma constructs identified by factor analysis (social and emotional distance and personal responsibility) modelled separately as dependent variables.
As a sensitivity analysis, participants with ASN were excluded to test whether the main effect of disclosure on stigmatization was affected. In a second analysis, participants who had received reordered workbooks were excluded to check for potential ordering effects. No differences in results were found, so all participants were retained in subsequent analyses.
Multivariable regression analysis was performed, adding age-group and gender of participants as covariates. The unadjusted regression was executed before the multivariable analysis since label disclosure was the key variable of interest. Moderation analysis was carried out to test for interaction between the main predictor of disclosure and age-group or gender on stigma, to determine whether age or gender moderated any reduction in stigma associated with disclosure of autism. Only Label × Gender and Label × Age-Group interactions were included in the model, as the effect of label condition was our principal focus. p < 0.05 was considered statistically significant throughout.
Results
Distribution of participant characteristics and mean values and standard deviations for all measures are presented in Table 1.
In unadjusted analysis, disclosure of autism was not a significant predictor of social and emotional distance, t(248) = 0.11, p = 0.91. Disclosure was a significant predictor of personal responsibility, t(248) = −6.16, p < 0.001, with disclosure explaining around 13% of the variance (R2 = 0.13). Adolescents who were not told that the vignette adolescent was autistic believed them to have more personal responsibility for their behaviour.
Age-group and gender were added as covariates in a multivariable regression analysis, label disclosure was still not a significant predictor of social and emotional distance (SED), and disclosure remained a significant predictor of personal responsibility. Table 2 shows the results of this analysis for factors social and emotional distance and personal responsibility (PR). The 14–15 year olds in this study reported wanting significantly more social and emotional distance than 11–12 year olds, regardless of disclosure (Table 2). Older adolescents attributed less personal responsibility to the autistic peer than younger adolescents. Girls believed the autistic peer to be less responsible for their behaviour than boys regardless of disclosure, but girls and boys did not differ on the social and emotional distance they wanted to maintain from the autistic adolescent.
Multivariable regression analysis for social and emotional distance (SED) and personal responsibility (PR).
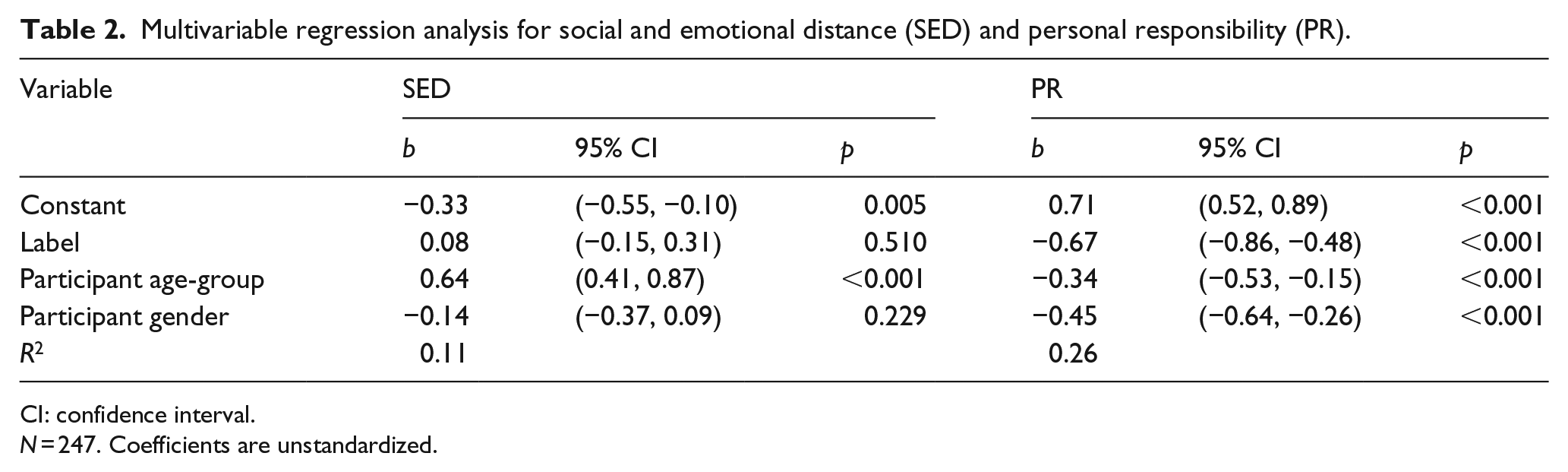
CI: confidence interval.
N = 247. Coefficients are unstandardized.
Moderation analysis
Moderation analysis was carried out to test for interaction between the main predictor of disclosure and age-group or gender on personal responsibility. There was a significant interaction between label and gender for personal responsibility, b = 0.39, 95% confidence interval (CI) (0.01, 0.77), p = 0.04. Disclosure was associated with a bigger reduction in personal responsibility for males, b = −0.855, t(246) = −6.48, p < 0.001, than for females, b = −0.467, t(246) = −3.37, p = 0.001 (see Figure 1). While the gender difference of higher personal responsibility for males than females was significant for the non-disclosure condition, b = −0.626, t(246) = −4.81, p < 0.001, it did not reach significance for the disclosure condition, b = −0.238, t(246) = −1.69, p = 0.09. Disclosing the label therefore reduced the gender difference in ratings. Including age-group, gender and interactions improved the fit of the regression model, explaining 27% of the variance in the outcome of personal responsibility.
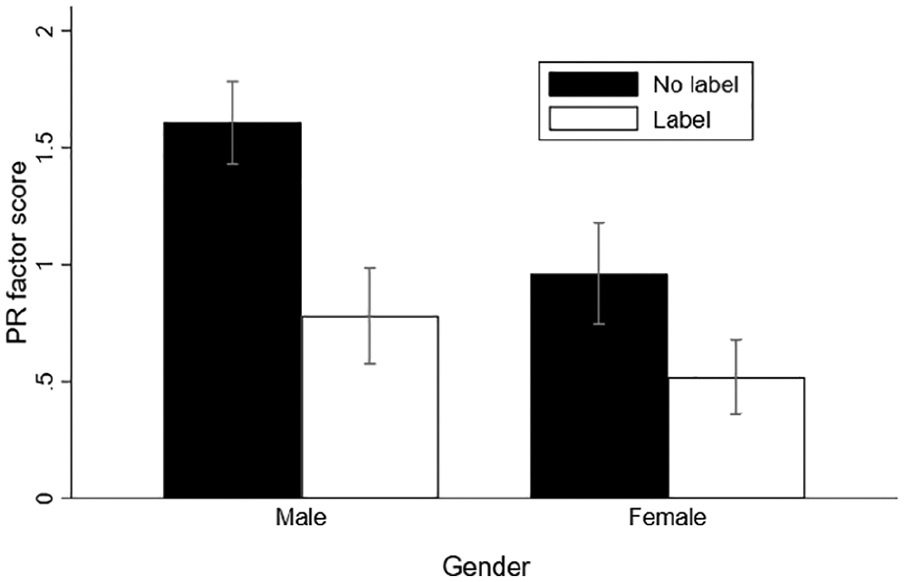
Mean personal responsibility (PR) factor score by gender and label disclosure condition. PR factor has been rescaled for clarity. Error bars are based on 95% confidence intervals.
In analysis of whether age moderated the effect of disclosure on attribution of responsibility, the effect of the interaction term was nonsignificant, b = 0.01, 95% CI (−0.36, 0.39), p = 0.95.
Discussion
This study tested whether disclosing that an adolescent has autism, without providing any additional explanatory information, could decrease stigmatization by other adolescents, and whether age-group and gender moderated the effect of label disclosure. Our primary hypothesis was that adolescents would stigmatize the autistic peer less when autism was disclosed, and we expected to see decreased social and emotional distance, and decreased attribution of personal responsibility in the disclosure condition compared to the non-disclosure condition. Results suggest that disclosure of autism reduced attributions of personal responsibility, but did not significantly affect the social and emotional distance that adolescent pupils wanted to maintain from the autistic peer. There was an interaction between gender and disclosure, with boys attributing less personal responsibility to the autistic adolescent for their ‘autistic behaviours’ than girls did when autism was not disclosed. However, when autism was disclosed, this gender difference was reduced.
Effect of disclosure
Attributions of personal responsibility may have decreased due to disclosure because participants identified autism as a medical label, which led to the autistic peer being placed in a ‘sick role’ (Parsons, 1951). Disclosing a child’s neurodevelopmental diagnosis reduces perceived responsibility and instead transfers responsibility to the child’s brain, in effect creating a neurological explanation for the child’s behaviour (Farrugia, 2009). This can be helpful for improving, for example, peers’ relationships with such pupils, as a peer who ‘is’ a problem becomes viewed as a peer who ‘has’ a problem (Ford & Russell, 2016). Disclosing might motivate an observer to exempt a peer from normal expectations of behaviour and so reduce the responsibility they attribute to the peer. Providing any explanation for non-normative behaviour may itself reduce stigma, whether it is medical in nature or not. Unlike this study, the only other study investigating personal responsibility in the context of manipulating autism disclosure with adolescent participants found that disclosure had no effect on perceived responsibility (Campbell, 2007).
No difference was seen in social and emotional distance as a result of disclosure. This corroborates results seen with children aged 8–12 years, which found that adding a label and explanatory information had no effect on children’s attitudes or behavioural intentions (Swaim & Morgan, 2001). In contrast, other research found that disclosing autism did reduce children’s desired social distance and improved their emotional response to the autistic peer (Campbell, 2007; Campbell et al., 2004).
Several US studies have looked at the effect of disclosing the label of autism in addition to explanatory information about autism that did not problematize it (Iobst et al., 2009; Matthews et al., 2015). These studies found improved acceptance when a label and explanatory information were disclosed. Perhaps, disclosing a label alone, as in the current study, is ineffective in changing social and emotional distance. The explanatory information may be crucial if adolescents lack understanding of autism as a condition. Sasson and Morrison (2019) suggest that greater knowledge about autism on the part of the rater leads them to feel more positively towards a person labelled with autism. Perhaps, if an observer does not have prior knowledge or is not provided with an explanation of autism, disclosing the label has no effect on social and emotional distance.
Unexpectedly, disclosure reduced perceived responsibility, but did not improve social and emotional distance. This is surprising because reduced perceived responsibility is often associated with more positive perceptions, compared to one who is seen as responsible for their behaviour (e.g. Feldman & Crandall, 2007). Attribution theory (Weiner, 1993) suggests that more sympathy is felt towards a person perceived to have less personal responsibility for their own negative behaviour, and emotional response and social support are improved as a result. The type of explanation an observer makes for others’ behaviour could, however, have an impact on social distance and affect: a meta-analysis of how medicalization of mental disorders affects stigma found that medical explanations for mental disorders tended to reduce blaming of people with mental disorders, but found that this did not affect desired social distance from such people (Kvaale, Haslam, & Gottdiener, 2013).
Stigma is a multidimensional construct incorporating a number of factors, and these separate aspects of stigma do not necessarily agree (Jorm & Wright, 2008), so perhaps different aspects of stigma are affected differently by labelling. Perceptions of a person as being ‘sick’ rather than ‘weak’, that is, less personally responsible for their condition, may be just as stigmatizing (Wright, Jorm, & Mackinnon, 2011), so perhaps aiming to reduce personal responsibility through a medical or diagnostic explanation is not an effective way of changing more practical aspects of stigmatization (e.g. social distance).
Age
The 14–15 year olds in this study reported wanting significantly more social and emotional distance from the autistic adolescent than 11–12 year olds. This concurs with other studies, such as Tonnsen and Hahn (2016), who also found that affective and behavioural attitudes towards autism worsened with age for adolescents. Horn (2003) found that 14–15 year olds are more likely than 16–17 year olds to judge social exclusion as wrong and to prefer social order in their peer groups. This age effect may partly explain why the older age-group in this study wanted to maintain more social and emotional distance from the autistic adolescent.
Gender
Girls believed the autistic adolescent was less responsible for their own behaviour than did boys. Previous research found a similar gender effect for attribution of responsibility: male students perceived a male peer with depression as more responsible for their behaviour than female students (Dolphin & Hennessy, 2014). Girls may have attributed less responsibility because, it is argued, adolescent girls may be better at perspective-taking; although evidence for this gender difference is inconsistent, it is suggested to be particularly marked in middle adolescence (Van der Graaff et al., 2014). Perhaps girls are more attentive to contextual explanations for behaviour and so attribute less responsibility to the autistic adolescent.
However, in this study, there was no effect of gender on social and emotional distance, suggesting that girls did not have more positive feelings or behavioural intentions towards the autistic adolescent in the vignette, regardless of whether the label was present or not. This was contrary to our hypothesis, but Nevill and White (2011) similarly found no gender differences on social distance with adult participants. One explanation for the lack of improved social and emotional distance for girls is that the adolescents presented in the vignettes were all male. Perhaps, a gender effect for social and emotional distance would be seen if multiple vignettes describing peers of different genders were used, since children and pre-adolescents tend to favour their own gender (e.g. Dijkstra, Lindenberg, & Veenstra, 2007), although this same-gender preference is thought to decline in early adolescence (Maccoby, 1998).
Gender moderated the effect of label disclosure on personal responsibility. Boys showed a bigger reduction in attributions of responsibility as a result of label disclosure. They had less positive attitudes than girls when the label was undisclosed, but when it was disclosed, this gender difference was reduced. A similar gender moderation effect has been previously observed in adult attitudes towards an autistic child (Chambres et al., 2008): women rated the child less severely than men when autism was not disclosed, but both men and women rated the child positively when it was disclosed. Perhaps, disclosing autism to men and boys is particularly beneficial for an autistic child.
Limitations and future research
The data used for this analysis were collected in a vignette study, so may not be reflective of how participants would feel or act in a real-life situation (Hughes & Huby, 2002). Another limitation of this and previous similar studies (Campbell, 2007; Campbell et al., 2004; Swaim & Morgan, 2001) is that only perceptions towards a male target were assessed. The gender of the autistic child might affect participant attitudes and gender effects, as children may stigmatize peers of the same gender less than those of a different gender (e.g. Bell & Morgan, 2000). The findings of this study may not generalize to how autistic girls are stigmatized, especially given there may be a separate female autism phenotype and stereotype (Bargiela, Steward, & Mandy, 2016). The generalizability of the results is also restricted by the sample as all participants were from the same school, so school-specific effects, such as the lower-than-average ethnic diversity of the school population compared to UK norms, cannot be accounted for. However, the proportion of ethnic minorities in the school is typical of the geographic area of the United Kingdom where the study was conducted. Data were collected from the two age-groups at two different time points, so there may have been contamination of the sample at the second collection point. The vignettes were read aloud to the class, so students may have communicated non-verbally to express their personal attitudes.
One area for future research with adolescents would be to utilize more diverse vignettes, for example, manipulating the gender of the peer in the vignette. The autistic behaviours of the adolescent could be manipulated, as in Butler and Gillis (2011), for example, varying whether more visible or disruptive behaviours are described. The proportion of variance in stigmatization explained by the factors included in this study is fairly low, indicating that a large proportion is unexplained. As the vignette described boys, it is not clear whether our findings can be generalized to girls. Future research should examine whether accounting for other factors such as knowledge of autism (e.g. autism training; Obeid et al., 2015; Someki, Torii, Brooks, Koeda, & Gillespie-Lynch, 2018), vignette gender and vignette behaviour can improve how stigmatization of autism is understood.
The study also has a number of strengths. The original data analysed in this study had a sample typical of secondary schools in the United Kingdom in terms of socioeconomic distribution, attending a mainstream school. The vignettes used improved on those previously used with children, as they portrayed the vignette adolescents in a positive light. Our findings suggest how disclosure of an autism diagnosis may play out among adolescent peers in UK schools. Such information has ramifications about whether to disclose for teachers, parents and autistic adolescents themselves.
Conclusion
Within this study, there is no clear indication that disclosure to peers can reduce stigmatization, in contradiction of our primary hypothesis. Since disclosure was found to reduce attribution of responsibility, perhaps disclosure is more useful in changing peers’ attitudes if the autistic adolescent has more visible typical ‘autistic behaviours’. Previous research suggests that it may be the ‘autistic behaviours’ displayed that have the most impact on stigmatization (e.g. Gillespie-Lynch et al., 2015), and our findings suggest disclosing autism may have limited impact in mitigating this. It is, however, important to note that disclosure may have benefits which have not been investigated in this study, such as feelings of authenticity for the stigmatized individual (Newheiser & Barreto, 2014).
Supplemental Material
AUT887625_Supplemental_material – Supplemental material for Is disclosing an autism spectrum disorder in school associated with reduced stigmatization?
Supplemental material, AUT887625_Supplemental_material for Is disclosing an autism spectrum disorder in school associated with reduced stigmatization? by Rhianna White, Manuela Barreto, Jean Harrington, Steven K Kapp, Jennie Hayes and Ginny Russell in Autism
Footnotes
Acknowledgements
The authors thank Lindsay Harrington of Pudsey Grangefield School for her help in developing materials used in this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Wellcome Trust (grant ref. 108676/Z/15/Z). The funders had no role in development of the work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.