
Abstract
The global impact of dementia on social, political, economic, and health systems is of contemporary concern. As the world’s population ages, differentially, across countries in the Global North and Global South, dementia research and care have become embedded in primary mandates for action within the agendas of governments and health research and service organisations. Using notions of social problem construction and sociologies of legitimacy, this article seeks to explore dementia as Zeitgeist that has captured imaginations but as such is contingent and therefore precarious building an edifice that may be limited and may occlude dangers for people living with dementia. This article argues for an applied sociological approach that recognises precarity and seeks to embed a sustainable praxis-focused axiology at macro, meso, and micro levels in respect of approaches to dementia.
Introduction
The global impact of dementia on social, political, economic, and health systems is much rehearsed. As the world’s population ages, albeit differentially, across countries in the Global North and Global South, dementia has become embedded in primary mandates for action within the agendas of domestic governments, for example, the UK Department of Health (DoH; 2015), and international health organisations, such as Alzheimer’s Disease International (ADI; 2013) and the World Health Organization (WHO; 2015).
This article explores the development of dementia as a Zeitgeist or global issue of the moment, demanding significant channelling of economic and human resource. It analyses dementia through the concept of social problem construction, incorporating a global level. Our contention is that, while such consideration has great potential for enhancing the lives of people with dementia and their carers, and intersects with population, poverty, security, and migration, it constructs fear and distancing that potentially generates the ‘othering’ of those living with dementia (Lacan, 1988), while also deflecting attention from other global health and social challenges. While social constructionist and critical approaches to dementia have been articulated previously (Hampson and Morris, 2017; Harding and Palfrey, 1997; Sabat and Harré, 1992), the novelty of this article lies in the focus on dementia as a socio-political Zeitgeist for health and social care systems. The concept of dementia as a Zeitgeist forms a useful distraction that allows neoliberal globalisation to maintain its grip on the politico-economic world of social health, and gaining purchase and legitimation through an isomorphic convergence in socio-health responses as a means of ensuring continuity of dementia ‘industries’. However, as a Zeitgeist, dementia – constructed in today’s socio-political context – is also an ephemeral and precarious representation that will, in time, be replaced, thus evoking possible dangers for people living with dementia, their families, and those organisations and services that have been created to meet their needs. Thus, such an understanding of dementia adds urgency to developing genuinely person-centred understandings that can survive changes in Zeitgeister.
After briefly reviewing the ways that dementia has been portrayed throughout the WHO, Alzheimer Disease International (ADI) and country reports critiquing international responses and demands, representations of the scale of the ‘problem’ of dementia will be explored. Subsequently, this article will present a revised and novel understanding of the social problem construction model taking into account globalisation and processes of legitimation, through convergence and homogeneity. This model will be applied to the ways in which dementia has been represented by interest groups since the turn of the millennium. It will be argued that dementia represents a socio-global Zeitgeist that has both positive and negative consequences for global, and individual, wellbeing.
The representations of dementia and consequent demands resulting from these will be shown, by comparison with Ebola, Zika, and HIV/AIDS, to act as distractions that may primarily prevent other global issues from receiving adequate attention. This situation acts to construct our current axiological foci in health, which in turn allows neoliberal capitalism to retain its grip on social, health, and medical service provision (see Latimer, 2018). Thus, many contemporary nations and big pharmaceutical industries may have vested interests in maintaining the emphasis on dementia while it remains potentially profitable or functionally useful to do so through the development of employment and health industry. Our analysis will show, however, that the development of a Zeitgeist suggests that in time it may be replaced and is, therefore, precarious and contingent. This is similar to Kuhn’s (1962) thesis of paradigm shifts in respect of scientific thought, but social problem construction perhaps serves us better in understanding issues more directly affecting human life and its organisation, and may offer a more historically congruent picture (Spector and Kitsuse, 1987). The role of the social representations will be considered, examining how these are employed and what that means for other socio-global Zeitgesiter.
Dementia in contemporary society
Dementia is presented to us in a variety of ways. From earlier clinically focused descriptions of a disease characterised by neurophysiological change and damage, or a syndrome illustrated by deterioration in memory, spatial and temporal organization, and cognitive debilities (Blessed et al., 1968; Kitwood, 1997), we have moved into biographical film and televisual media portrayals of individual experiences with dementia, such as Iris, the 2001 BBC Films portrayal of the life of writer Iris Murdoch, and Still Alice the 2015 US fictional production relating the life of a linguistics professor. This shift, from a primarily biomedical focus towards the lived experience of dementia has widened the scope of exploration. Previously when one considered dementia, it was through a lens of loss – the loss of one’s self, one’s mind, and one’s personhood, but this is being challenged recognising that Dementia does not represent the loss of self rather an adaption to representation of who we are. Sabat and Harré (1992) argue that the sense of self is lost, not through the individual themselves but in their interaction with others, arguing that as the individual’s ability to communicate declines, the recognition of what makes them who they are declines and instead all people see is a dementia ‘sufferer’. It is this external viewing of the individual which perpetuates an increasing vulnerability but also the declining sense of self. Take, for example, an active and driven individual used to a busy working environment who would be seen as proactive and positive in their life. That individual is unlikely to lose that aspect of their self because of a diagnosis of dementia but this activity is likely to be re-categorised as meaningless ‘wandering’ once they have a diagnosis.
Not only has the construction of the individual experience of loss changed but so too has the focus individual and their families towards communities and wider society. Downs (2000) argues that one’s experience of dementia is influenced not only by bio-physical changes but also by wider sociological factors such as culture, ethnicity, and social class. These wider sociological factors have led to organisations such as the Joseph Rowntree Foundation, Dementia Action Alliance, and the Alzheimer’s Society, to challenge the degree to which people with dementia are integrated within their local community, through initiatives such as Dementia Friends, Dementia Friendly Communities, and Dementia Friendly Societies. On an international scale, agendas such as the Global Action against Dementia (World Health Organization (WHO), 2017) recognise the importance of prioritising care over cure; public awareness; and accessibility to services, equity, and research in an effort to broaden the general global approach to dementia. A refocus from biomedical and residential care towards the importance of living well within the community illustrates a shifting emphasis from a deficit model towards an asset-based approach.
Contemporary discourses about dementia are not as polarised as often indicated. While there has been an historical, somewhat linear process of development spanning the biomedical, psychological, social/biographical, and latterly dementia-friendly accounts, when we read about, hear reports of, and see dementia, we are faced with a composite view stemming from our experiences (Parker and Ashencaen Crabtree, 2014). In earlier work, we identified the different media involved in the ways in which dementia is perceived at professional and individual levels, recognising the ways in which it is responded to professionally and personally reflects back on the constructions and experiences of others (Parker, 2003).
The various discourses by which dementia is portrayed, while fascinating and socio-culturally important for the organisation and delivery of services and expressions of care as well as understanding, are beyond the scope of this article. For the purposes of the current discussion, we need to acknowledge the prevalence of the bio-medical understandings of dementia and the psycho-behavioural manifestations associated with it. Biomedical positions often inform the personal experiences and biographies of many families, friends, and people living with dementia. The critique of these constructions provides a rich cultural repository for critique and approaching dementia through a different lens (see Martin and Bartlett, 2007). We focus, in this article, on the received understandings of dementia recognising that it is the combined set of discourses that underpin people’s responses and reactions to it as a ‘social problem’.
The idea that dementia, and people’s responses to it from their various personal and social positions, is socially constructed is not new as we discuss below. However, this article sets those constructions within a context that responding is a temporal imperative; it has come of age and demands a global response. Our contention is that while the human imperative is clear, the anxiety created by its position as Zeitgeist creates significant dangers and leaves responses subject to populist problem identification and makes global responses precarious.
The scope of the ‘problem’
The 2015 figures suggest that there are 46.8 million people globally living with dementia (ADI, 2015), a figure which is estimated to triple to 152 million by 2050 (WHO, 2018). The rate of new cases is rising by 9.9 million worldwide per year, equating to one every 3.2 seconds (ADI, 2015), although Schrijvers et al. (2012) question whether the incidence of dementia is in fact decreasing proportionately to global population. However, this rise in new cases is not evenly spread throughout the world. Indeed, 58% of people with dementia are in low- and middle-income countries, with the fastest growth in numbers of people with dementia occurring in Asia (especially China, India, South Asia, and other Western Pacific countries), and this figure is estimated rise to 68% by 2050 (ADI, 2015).
Increased prevalence and incidence rates may on one hand represent a success story in human technologies of health care (Nettleton, 2013). The global demographic of ageing populations with decreasing birth rates results, however, in increasing numbers of older and often more dependent people, increasingly with dementia (Ferri and Prince, 2005; Prince et al., 2013). Dementia is also recognised as affecting an increasing number of younger people (Pritchard and Rosenorn-Lanng, 2015). This results in huge economic and care resource demands. A cynical view of Western hegemony might suggest that dementia, rising more in developing countries, would not be seen as such a huge and immediate social and health problem to tackle. This is not the case, however, not because of altruistic sentiment and concern for international development but resulting from dementia’s potential as a business opportunity.
The costs related to dementia may be higher than perceived, however, owing to inconsistent diagnosis. It is estimated that only 50% of incidences are diagnosed in high-income countries and less than 10% in low- and middle-income countries (ADI, 2016). In others, there is a concerted effort to improve diagnosis and therefore target resources more effectively as a means of consolidating costs and ensuring appropriate care is provided as soon as possible (ADI, 2016).
International reactions to dementia
The global imperatives for health and social care arising from dementia are clear, as are the economic challenges (ADI, 2015). The World Alzheimer’s Disease Report in 2015 estimated the costs of dementia at $818 billion, an increase of 35% since the previous estimation of $604 billion (ADI, 2010). The annual and economic cost of dementia is expected to increase to $1 trillion by 2018, a figure which has been suggested to be the equivalent of being the 18th largest economy in the world, exceeding the market values of Apple and Google (ADI, 2015). These costs include those stemming from family care and informal caregiving which are also rising, and it is suggested that by 2030, the cost of dementia will reach $2 trillion (ADI, 2015, 2016). A negative consequence of the focus on the cost of dementia is a perpetuation of fear and stigma associated with the disease (Latimer, 2018), especially in the current climate of reducing social care budgets and increasing concerns regarding how long-term social care of older people will be funded.
The latest world report focuses on improving healthcare for people with dementia (ADI, 2016), a shift from the previous reports (ADI, 2014) which concentrated on risk reduction and developing healthy lifestyles through public health initiatives. This, over time, will reduce global economic costs and no doubt develop corporate responses that will construct alternative means of income generation from this global issue (see also, Parker and Ashencaen Crabtree, 2014). However, the current population patterns have caused concerns that have mobilised an array of health, social, and politico-economic responses as to whether or not this focus on population change represents less of a cause for concern (Dorling, 2014).
(Global) social problem construction
Bond (1992) recognised how the medicalization of dementia informed its social construction. Challenging this was crucial in developing models that focused on the person. This has become a well-trodden area that recognises a dialectical interplay between multiple factors, including the social and political, to form our constructions of dementia (Adams, 1998; Hampson and Morris, 2017; Harding and Palfrey, 1997; Innes, 2009; Wearing, 2013). Bosco et al’.s (2019) rigorous systematic review of research into dementia and its social construction through time found that various conceptualisations exert significant influence on its representation and how it is responded to. They identified the importance of understanding the social construction of dementia for developing new and improved ways of responding to dementia. To state that dementia represents a social construction or a socially constructed problem does not, in any way, detract from its experienced, lived reality or the potentially devastating impact of diagnosis or experience as an individual with dementia, a friend, or carer (Åsberg and Lum, 2010; Behuniak, 2011). Indeed, it sets dementia within a human context of shared perspectives and concerns.
Dementia is socially constructed, as we note above, through the ways in which social actors approach and engage with dementia and are confronted by socio-cultural representations of it as an experience or phenomenon within the world; that is how societies organise services, treat, communicate with and about people with dementia, and how families and communities act (Bosco et al., 2019; Hashmi, 2009; Parker, 2003, 2005). This creates meanings that become an assumed, taken-for-granted part of social actors’ repertoires. Those meanings are not, of course, recreated anew at every point but build on the collective responses and experiences of those actors involved (Atkinson, 2015; Blumer, 1971; Harding and Palfrey, 1997).
Accepting that dementia may be construed as a (global) social problem given its prevalence, incidence, and the socio-political responses to it, it is important to consider the processes by which a social problem becomes recognised as such (Blumer, 1969; Schneider, 1985; Spector and Kitsuse, 1987). Social problem construction has many facets and has developed across wide areas (see Best and Harris, 2013). Common aspects of problem construction relate to the recognition of a phenomenon that is interpreted and communicated to others. If accepted as a ‘problem’ by others, however, it does not mean that social action will necessarily be taken; social problems are contingent (Best, 2002; Spector and Kitsuse, 1987). In respect of dementia, the global assumption or taken-for-grantedness of its problematic status was built on growing acceptance of such over time combined with the demographic evidence and economic demands resulting from increased recognition at an active policy and practice level. To maintain its social problem status, it needs to both reinforce and be reinforced by governmental and corporate responses. This, again, is contingent on recognition and acceptance and its relative weight against other issues that may have global reach or an impact on key economic interests of powerful nations. Not only is this contingent on economic interests, it is likely to change and develop over time according to newly recognised problems and the unforeseen consequences of social and political actions. Thus, it cannot be taken-for-granted that recognised resources will continue to be allocated to dementia care, making the ADI (2016) report on cost-effectiveness of care all the more important.
Our understanding of social problem construction owes much to Blumer’s (1969) theory of symbolic interactionism, Berger and Luckmann’s (1966) social constructionism, and Spector and Kitsuse’s (1987) constructionist approach. Blumer’s original model was based on the idea that people attribute meaning to social phenomena and entities through negotiation of the social processes of symbolic communication which takes place internally and interpersonally. It is a labelling or naming process, something that is very powerful in conveying and constructing meanings and has a ritual element to it.
Becker’s (1963) deviance theory, and subsequent iterations of it as labelling theory (Lemert, 1967), add richness to this understanding notwithstanding critiques from conflict theorists and some feminist scholars (Best, 2002). In the case of dementia, which could itself be constructed as deviance, and thus indicating that it is not so much the bio-psychological aspects that matter but the ways in which the general public, family members, and people with dementia themselves respond to dementia that construct its meanings as a social problem (Åsberg and Lum, 2010). If we add the position of marginalised groups, patients and victimisation and recognise the place of structure as additional forces within this context, labelling offers some understanding.
The social problem of dementia has been perpetuated through the use of language, for example, referring to individuals as ‘demented’, which has assumed an almost exclusive pejorative meaning. In this, the individual is largely reduced to this one negative aspect, which allows further victimisation and the stripping of personhood and citizenship (Åsberg and Lum, 2010). Other research describes a person living with dementia, responding to the categorisation of ‘demented’ as ‘horrendous’, argued that it implies ‘something which is not even human’ (Sabat et al., 2011: 265). Language and stories about dementia in film, theatre, literature, and documentaries contribute to the social and cultural constructions of dementia and reinforce these in popular consciousness (Zelig, 2014). Language is also recognised as important in clinical approaches to dementia (Wray, 2017), but is seen as an important aspect of participative and inclusive research (Waite et al., 2019). In our earlier research concerning daily practices, we noted how the containment, care, holding, and containing practices demarcated the problematic ‘other’ from those working in care-giving or ‘containment’ positions. Symbolically, this protected non-dementia society from the deviant, fear-inducing ‘other’ (Parker, 2005, 2007), and permitted the denial of structural responsibilities through labelling, and reduction of care costs by pushing the ‘deviant’ onto their families, mainly women. Thus, what could have begun as a private health concern or a perceived minor failing in memory or orientation becomes recognised by others who label it as ‘odd’ (deviant), and once this becomes accepted, it may have wide impact on how the person is perceived and treated. When a person is provided with label of dementia, it often becomes the predominate factor which defines and categorises them, and they are perceived as confused and therefore vulnerable. This in turn affects engagement, the person with dementia becomes someone who needs to be protected from being defined by their weakness and vulnerability (Parker, 2007), which would lead to a lack of voice and citizenship. This lack of voice and citizenship perpetuates the social divide and stigma associated with dementia. The turn to ‘living well’ with dementia may also become embedded in popular consciousness and lose some of its current challenge and rather be seen as a normative expression that directs certain ways of responding to people living with dementia or working with those people (Clare et al., 2014; Smith and Simkhada, 2019).
Lemert (1967) identified both primary and secondary deviance. While minor deviations from the ‘rules’ of ‘normal’ or accepted behaviour are fairly common, such as forgetting names or where the shops are, they become transformed into deviance when labels are applied and secondary deviance when those stigmatising labels are internalised, accepted, and acted upon as a self-identity (see Goffman, 1963). This kind of stigmatisation is akin to Kitwood’s concept of malignant social psychology (Kitwood, 1997; Kitwood and Bredin, 1992) which may be reflected in the anxieties of those in the early stages of dementia recognising they are assuming the mantle of dementia and its stigmatising or ‘othering’ features (Maki and Yamaguchi, 2014). This fear may delay the accessing of professional support and early diagnosis. Thus, the stigma associated with the disease simply perpetuates fear and continued stigma, as people hide their diagnosis for fear of being ostracised. This is a similar trend to other healthcare diseases, such as cancer and HIV (Taber et al., 2015).
These theoretical understandings of dementia explicate clearly the potentially life changing effects of dementia on individuals, families, and communities. They show how people can be excluded from full citizenship, and provide a rationale for the importance of tackling dementia at a psycho-social as well as biomedical level (Bartlett et al., 2018; Bosco et al., 2019; Hampson and Morris, 2017; Kontos et al., 2017). However, the social problem construction may be much wider than a focus on these intra and interpersonal impacts and permeates the realm of organisational responses, clearing the way for economic exploitation of the emerging markets created by health and welfare needs.
Earlier studies framed the object of attention in social problem construction in national or local terms. These could, of course, transcend national barriers as seen in continuing applications of Cohen’s (1972) work on moral panics, but were generally locally bounded as indeed was this seminal study of fighting between rival youth gangs in Britain. Mass global communication and information sharing allows the frame to be extended and ‘glocalised’, accepted as a social problem spanning the world but acknowledging the local variants of its manifestation and responses to it (Drees, 2015). This has both positive and negative aspects. Global energies can be devoted to finding appropriate and effective ways of responding to the identified problem both locally and globally. However, this can lead to the dominance of market approaches that seek primarily to profit from the social problem and, therefore, operate paradoxically to ensure its continuance unless and until a further profitable social problem gains purchase. It may reinforce the hegemony of global capitalism and, indeed, the ways in which the Global North approaches dementia care.
How dementia has become a global social problem can be seen by its history, in its developmental context from Western history and medicine. There have been three precarious phases of recognition, demonstrating the contingency of social problems (see Figure 1). Indeed, it is only latterly that the phenomenon has gained traction as a social problem:
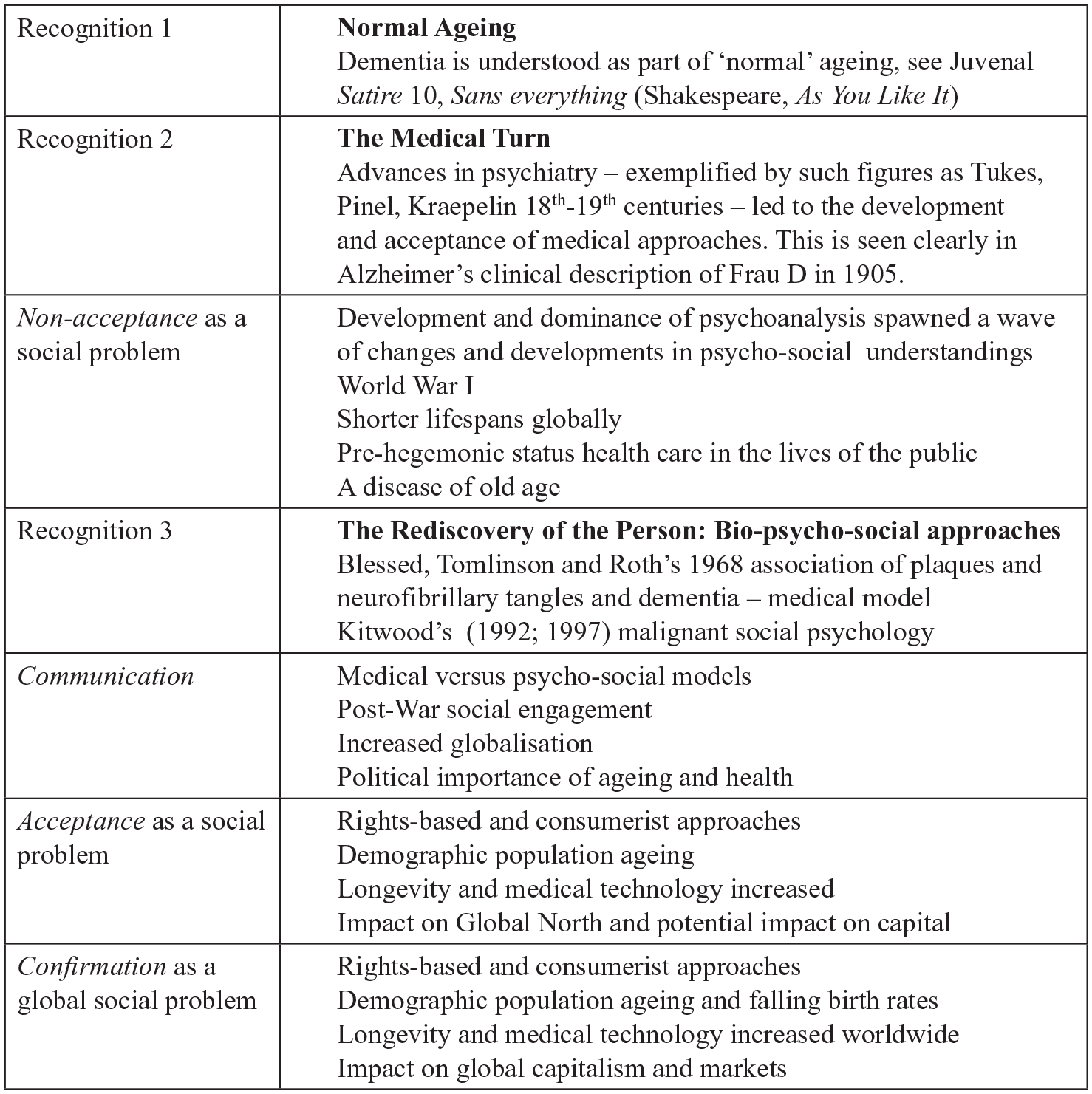
Phases of recognition of dementia as a social problem.
The confirmation of dementia as constituting a global social problem rests not only on benign concern to alleviate the issues arising from dementia across cultures and nations but also on the involvement of global capitalism and a neoliberal market economy that seeks to maximise profit from the increased demands of a population that has growing awareness and fear of the issue. Thus, publicity of dementia as a growing and much feared disease and a drain on global economic resources stimulates a market that demands more effective action, treatments, and care services. The maintenance of the global social problem depends on the privileged position constructed as a result. Through such social problems, the Global North retains its hegemonic status in health and social care.
Contingency and precarity
As noted earlier, however, social problems are contingent and other problems may take their place as concerns, fears and interests change and develop. These contingencies depend on dialectic interplays of complex social forces and, to an extent, on capturing the Zeitgeist. We may ask, for instance, why Ebola, which has been around 40 years, or the more recent rise in cases of Zika have not assumed similar status as global social problems (Cowling and Yu, 2014; European Centre for Disease Prevention and Control, 2014). Perhaps, we may assume that because they affect, predominantly, low-income countries in the Global South, that there is little profit for ‘Big pharma’, and because it has not affected many people in the Global North, it has not held the attention of those with power to provide it with social problem status. Should Ebola or Zika develop across the Global North, the fear factor will again most likely be employed to forge marketised responses to it as a global social problem (Hughes and Poletti-Hughes, 2016). It might be argued that Big Pharma’s withdrawal from dementia research belies this analysis. Nicholls (2018) outlines the withdrawal of a number of big pharma companies from dementia drug trials using beta-site amyloid precursor protein cleaving enzymes (BACE) inhibitors given the lack of evidenced for their efficacy and the low returns on investment. However, she is clear that this has not halted the search for drug therapies. Indeed, in the UK, the Medical Research Council, Alzheimer’s Society, and Alzheimer’s Research UK have provided 250 million to fund the UK Dementia Research Institute’s bio-medical and drug research (De Strooper, 2018); Rafols et al. (2014) add some insight here into the changing operations of Big Pharma to work alongside others in drug creation rather than as single entity research organisation.
It can be argued that HIV/AIDS gained global social problem status in the 1980s during which thousands of people were affected. At first when HIV/AIDS was demonised as a deviant disease, affecting those who were ‘othered’ from mainstream, or taken-for-granted and accepted society, little was done except for moral warnings and stern advice. When its impact widened to affect traditionally non-stigmatised groups or individuals, research quickly determined the efficacy of retroviral medicines which offered the possibility of a more ‘normal’ life and lifespan for those having contracted the virus (Broder, 2010). Infected individuals were no longer deviant others and the mystique of impurity associated with the other diminished (Douglas, 1966). HIV/AIDS lost its Zeitgeist status. While HIV/AIDS still affects many millions, it has lost much of its former position and is no longer treated as a global social problem demanding immediate social, political, and economic attention despite affecting millions worldwide (United Nations, 2004). This may be partly due to the availability of retroviral drugs and the slowing infection rate in the Western world, but this ignores the plight of many in the Global South including also more developed countries such as South Africa who have restricted access to medicines and care. This, we argue, demonstrates that global social problem construction is contingent on its impact on the West and on global capital, whether or not it captures the Zeitgeist.
Also, those affected by specific conditions represent a precariat that may receive attention and services or not depending on their timely status or otherwise, and also in terms of their socio-economic utility value. Grenier et al. (2017: 318) highlight dementia as ‘failed’ and ‘frailed’ old age that demarcates the boundaries between ‘them and us’, the ‘frail and the non-frail’, which results in differential resource allocation characterising the fourth age of life (Jones, 2017). This reinforces calls for a more secure basis for care and citizenship for people with dementia removed from the vagaries of politico-economic power.
Currently, dementia has a powerful economic dimension not only as a ‘cost’ to nations globally, but also as a means of developing a wide multi-million pound research industry, provision, training, and development of care staff and the development potential of pharmacological products. This is further supported in the UK by the classification of many of the care tasks required as ‘social’ care rather than ‘health’ care (Alzheimer’s Society, 2014). The projected costs of dementia care in the UK for 2015 are £26.3 billion of which two-thirds (17.4 billion) represent unpaid family care (mainly women) and privately funded care. This not only raises political and moral questions in societies but also demonstrates the importance of dementia as a topical social problem that may, in part, be maintained by the economic imperatives of governments and business to ensure costs are deflected onto families from an already stretched NHS and local government system (Jordan and Drakeford, 2012; Pascall, 2012). The costs of privately funded care ensure also that social care providers are employed, and that a marketised approach is reinforced and health-related businesses become dependent on that care model.
DiMaggio and Powell’s (1983) thesis of isomorphic convergences provides additional understanding of some of the ways in which corporate health markets are exploited by an unholy alliance of health organisation and global social health problem, in this case dementia. They recognised a tendency in large organisations for like-minded businesses to converge around isomorphic constructions of product or service. For instance, should a developing nation wish to show it is working at the level of developed, high-income country, it will copy the practices and be expected to mimic them by those with power, demonstrating its membership of an increasingly exclusive club that adopts the taken-for-granted approach to the problem as the ‘right’ approach. In practice, of course, such convergences do not represent hermetically sealed developments within a country’s social and health care organisations, local practices, and differences do operate. However, they reflect a trend that demonstrates how the hegemony of Western neoliberalism maintains a global social problem for maximising profit from the development and promotion of certain services and responses to dementia.
However, the public and private costs of dementia create employment opportunities and tax revenue for the Government and for research industries. What has been accepted as a social problem becomes a rationale for industry development, continued employment, and tax revenue. The contingent nature of these developments, however, raises a worrying question in terms of sustained care especially post-displacement when a distinct Zeitgeist vies for attention as a global social problem. Unfortunately, it is not only the elusive myth of the discovery of a ‘cure’ that is likely to shift dementia from its primacy.
The focus on dementia also exacerbates a fear reaction and a process of ‘othering’ in which the person with dementia is necessarily excluded and made liminal, and this allows those with political power and capital to distance themselves from responsibility, by pointing to the deviance of dementia, if they deem necessary. The person with dementia is neither person of the world nor completely removed but seen as impure and tainted and to be feared and avoided (Grenier et al., 2017). Therefore, the construction of care rituals and liturgies of policy acts as a protective sheath removing the deviant from positions of feared contamination. Active ageing policies and public health initiatives, often expressed through popular media, add to the embedding of these constructions (Parker and Ashencaen Crabtree, 2014, 2020). However, the fear associated with dementia and the notion of disadvantage attaching to the person by association with the feared other may also present a danger to the current global focus on dementia (Parker, 2005, 2007). The potential for avoidance exerts a strong pull towards other less fear-provoking issues.
While the above analysis focuses on some of the dangers and precarity of the attention focused on dementia, it is not meant to reflect negativity and cynicism. There are many international organisations working to enhance quality of life, and share good practices, novel, and appropriate interventions such as the pan-European group: Alzheimer Europe (2013), Interdem (2018), and the globally reaching Alzheimer’s Disease International (ADI, n.d.-b) which promote global sharing and enhancing local responses. These represent important global responses to the growing awareness of the issues raised by increasing prevalence and incidence of dementia. However, it is crucial to acknowledge the contingent nature of global social problems and to ensure that people with dementia, their families and care organisations developed to assist are not diminished by a shift in problem recognition.
Ways forward
In our analysis, we have sought to engage axiologically with the issues as we see them, as an overt value base is central to applied sociology. An engaged sociology or anthropology, drawn from a pedagogy of the oppressed (Freire, 1970), rejects the role of the researcher as ‘objective’ observer but sees her or him as reflexively involved as an actor and thereby politically embedded, and we acknowledge our position in this analysis. It is important in understanding and stating one’s position as a social actor within the complexities of social problems, so that we pursue arguments and analysis for social problem construction, maintenance, and resolution. It is from this perspective that we can begin to explore a way forward that promotes the needs of people while addressing the dangers inherent within the present contingent way in which dementia, as a global issue is confronted.
There are three immediate levels at which the problem construction operates; a personal/individual and familial one (the micro), a service level/national policy position (the meso), and global political ones (the macro). These three levels are not entirely distinct and interact with one another, and it is important to recognise the needs for action at all levels.
At a macro level, dementia as a global Zeitgeist allows the pursuit of fair policies, acknowledgement of the differential needs and experiences of low-, middle-, and high-income countries, and the search for treatments and social interventions that are meaningful to those receiving them and their families. However, it also allows the development of multinational corporate businesses to enhance capital growth from the growing recognition and fear of dementia. Important to global capitalism is the ability to accumulate resource and income. This brings dangers to the pursuit of ways of responding fairly and appropriately to acknowledged problems. They must be cost effective or, indeed, maximise income for those underwriting the search for problem resolution. The fickle interests of capitalism will follow the rule of profit above others, and the need for overt moral economics is central to a sustained search for effective ways of working effectively with dementia over time, especially important given the unequal distribution of resources of capital expenditure and gain. A critique of the global problem construction of dementia is therefore central to identifying a greater focus on the human dimensions such as the impact on individuals and families, the development of social and health approaches to care-giving, and the construction of person-centred social policies.
The meso level of service and care organisation provision requires a research and value-driven approach, one that develops its strategies and practices according to the local or national need, while drawing on wider or global understandings as well. Dementia needs to be seen within its cultural contexts and responded to accordingly rather than relying uncritically on an imposition of Western medical knowledge. If autochthonous knowledge and practice is given value, it will allow for a continuation of appropriate care services when and if dementia loses its zeitgeist status, when a different global problem takes centre stage. However, the Global North also needs to recognise the inequalities in resource and expenditure as important while dementia retains its primary positioning to demand a redistribution of wealth to ensure continuities of care.
It is important to reduce the fear and ‘othering’ that takes place if individual people with dementia or their families and others looking after them are to be included rather than being made separate and set on a dais of illness and disease that demands obeisance and rejection because of its assumed impurity and contagion by association (Douglas, 1966; Parker, 2005). At the micro level, it is the stories of people themselves spoken from within a range of cultural and social contexts that help illuminate local meanings. If it is the macro, at state, nation, or global levels that are influencing the ways in which services respond and individuals understand dementia, this may not fully acknowledge the (auto) biographical experiences of those at the heart. Therefore, it is these person-centred, humanising processes that are required within the education systems for those engaged in health and social care. Incorporating these person-centred humanised processes require careful consideration, especially the ways of incorporating the individual voice that promotes a focus on the retaining of personhood despite a diagnosis of dementia rather than perpetuating a biomedical discourse of vulnerability and decline. This requires educational processes which challenge and question individual values, understanding and thinking about dementia away from a biomedical towards a biopsychosocial cultural examination. Simultaneously, this focus needs to be brought into health and social care practices, business ethics, and policy. Without this shifting emphasis, people with dementia remain excluded or ‘othered’ and economic concerns predominate.
Critical approaches to service provision, knowledge construction, and globalised responses to significant issues such as dementia offer a means of developing alternative understandings and practices and demand close questioning of taken-for-granted assumptions in global response, policy, the practices of services, and individual responses. The concept of Zeitgeist adds urgency to the need to refocus attentions in dementia care and research. It illustrates the fickle approach that has been pursued and requires a shift to ensure that the person is genuinely positioned as the focus of care, support, and research. By focusing on the socio-political and cultural constructions of dementia, a critical gerontological perspective can offer new understandings and ways of challenging short-term approaches that increase precariousness for those living with dementia and those working with them.
Footnotes
Authors’ note
Clare Cutler is now affiliated with Wessex Institute for Health Research and Development, University of Southampton, UK.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.